Embed Size (px)
Citation preview
STIFF NECK
Pain or discomfort when trying to turn or move the neck.
Definition:
1. Postural2. Atlanto-axial3. Spasmodic Torticollis4. Hysterical Torticollis5. Stiff neck as a result of
muscles
TYPES:
Secondary to auditory and visual
disturbances.
1. Postural
Due to torticollis which is still present.
2. Atlanto-axial rotation fixation
Condition in which the head becomes persistently turned to one side.
Patients experience repeated attacks of painless rotation or lateral flexion of the head.
Gradual onset from age 40. Most common movement= rotation to the left side.
MOBILISATION DOES NOT PLAY A ROLE IN THE MANAGEMENT OF THESE PATIENTS.
3. Spasmodic torticollis
Repeated movements while the patient moves
the head to one side
4. Hysterical torticollis
Post traumatic,Post viral and;torticollis
5. Stiff neck as result of muscles
HISTORYPainless contracture of 1 of
sternocleidomastoid muscles
Neck fixates in side flexion-towards affected side + rotation away from it.
Lack of treatment= patient developing a permanent postural
deformity + facial asymmetry
InjuryOsteoarthritisRheumatoid arthritisPinched nerveFibromyalgiaMuscle spasmMeningitis
Causes: Identified by means of X-ray, MRI or CT
DEPENDANT ON CAUSE
Include: Non-steroidal anti-inflammatory drugs
to relieve pain. A cervical collar to keep the neck still so
that muscles can rest. Limitation of activities that could strain the
neck. Physiotherapy
Treatment:
Massage Ice or heat therapies.Maintaining a good postureAdvice for at home:Patient should sleep on a firm mattress and designed neck pillow or without a pillow.
Treatment Continued:
Onset of a sudden, sharp pain near the midline of the cervical spine on the affected side that appears as a result of an unguarded movement and that is accompanied immediately by an inability to return the head to a straight position.
Acute Cervical Locking (“locked joint”)

Occurs mainly in adolescence Sudden onset Snapping sound is heard Sudden uncontrolled movement Patient may be awakened by the pain Most common between C2/3 Synovial pinching Localised to mid-cervical area Severe, sharp pain with proximal referral if the
patient should try to move out of the position. Noticeable lateral flexion, slight
flexion/rotation away from pain-commen protective deformity.
Characteristics:
CAUSE
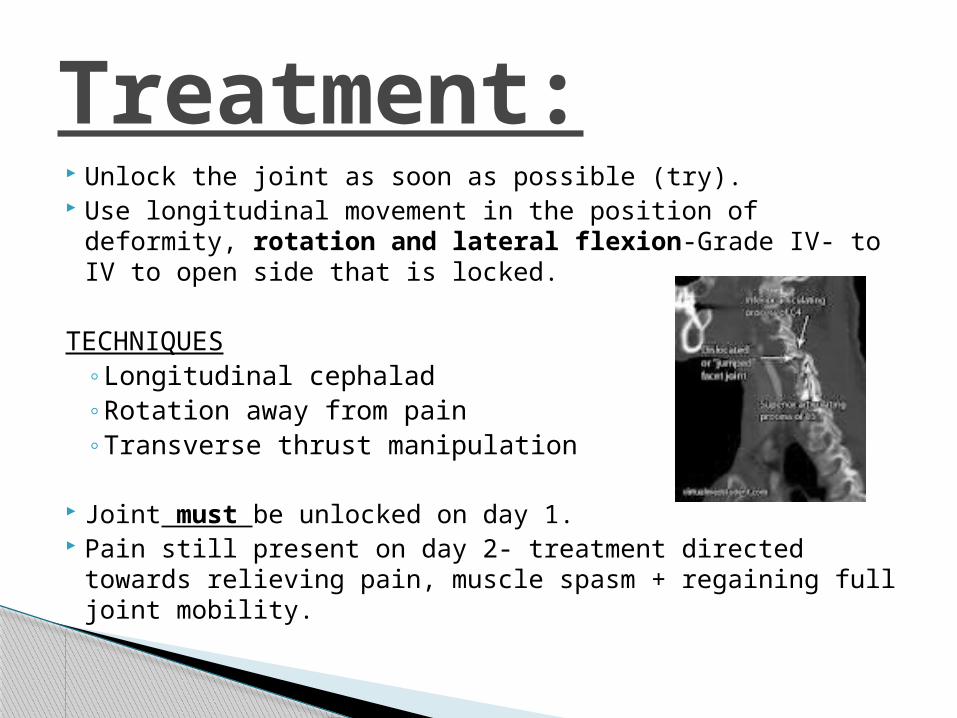
Unlock the joint as soon as possible (try). Use longitudinal movement in the position of deformity,
rotation and lateral flexion-Grade IV- to IV to open side that is locked.
TECHNIQUES◦ Longitudinal cephalad◦ Rotation away from pain◦ Transverse thrust manipulation
Joint must be unlocked on day 1. Pain still present on day 2- treatment directed towards
relieving pain, muscle spasm + regaining full joint mobility.
Treatment:
Mostly affects◦ Atlanto-occipital◦ Atlanto-axial
Traumatic onset:
Bump against the head
Patient has unilateral sub-occipital pain + movement
towards painful side. Lateral flexion and rotation feels stiff.
History
MAITLAND MOBILISATIONS
If not unlocked on day 1◦ Manipulation◦ Strengthening◦ Reduce muscle spasm.
Treatment:
Gradual onset No specific movement May awake with locked neck Any level between C2-C7 Disc Neck pain Worst pain-medial, scapulae area (Clowards area’s) Deep pain Noticeable flexion, lateral flexion away from
pain Extension, lateral flexion and rotation towards the
painful side is stiff but not blocked
Discogenic locked neck
Prolonged poor posture Repetitive neck movements Slouching Heavy lifting with poor technique Poor posture during sleeping Neck joint stiffness A sedentary lifestyle muscle weakness or tightness a lifestyle or occupation involving large amounts of
sitting (particularly at a computer or driving), bending, slouching or heavy lifting
Prolonged repetitive movements stretch tissue in the neck over time, predisposing the facet joint to injury.
May originate from traumatic hyperextension injuries e.g. whiplash
Causes:
Non-steroidal anti-inflammatory medications Corticosteroid injections into facet joints Physiotherapy:
◦ Intermittend constant traction (ICCT)◦ Transverse movement◦ Unilateral PA◦ Rotation and lateral flexion◦ Longitudinal caudad◦ Grade I, II and IV-◦ TENS◦ ice/heat modalities
Treatment:
Literature clearly highlighted the success of manipulations and Maitland’s mobilisation techniques, as well as the combination of the two in treating acute cervical locking.
The preferred techniques are described as well as importance placed on accurate assessment of patients before treatment
There is also a clear explanation of the differences between acute cervical locking and cervical spondylosis.
Literature: Acute Cervical Locking

Assessment Variable Acute Cervical Joint Lock
Spondylosis
Age of occurrence late adolescence usually over 35
Typical history sudden onset associatedwith a quick movement butno trauma
gradual onset that maybe related to minortrauma
Common protective deformity
rotation and lateral flexionaway from the side of painwith slight flexion
rotation and lateral flexionaway from the sideof pain with significantflexion
Area of pain local cervical (C4 to C6area) near the midline onthe affected side awayfrom which the head istilted
more lateral (C4 to C7area), may spread to ipsilateralscapulae, andoften referred to ipsilaterallimb and to occipitalarea
McCoy, K. 2009. Stiff Neck: A Look At Possible Causes.www.EverydayHealth.comRetrieved on 16 July 2012
Sprague, R. B. 1983. The Acute Cervical Joint Lock. Journal of the American Physiotherapy Association 63: 1439-1444.
Kirpalani, D. and Mitra, R. 2008. Cervical Facet Joint Dysfunction: A Review. Division on the Physical Medicine and Rehabilitation 89:770-773.
References:










![FUZZING IN 2014 - · PDF filemov eax, [edx] WRITE Trying to perform r/w operations on illegal or restricted memory locations Attempt to write to an ... 即使有些绕过技术](https://img.pdfslide.tips/doc/110x75/5a788dfb7f8b9a7b698cb35d/fuzzing-in-2014-eax-edx-write-trying-to-perform-rw-operations-on-illegal-or.jpg)