31
Chapter 6 Shoulder Dystocia
Jason Marcus Definition A delivery that needs additional
obstetric manoeuvres to deliver the shoulders, after gentle
downward traction on the fetal head has failed, because the fetal
anterior shoulder is impacted against the maternal pubic symphysis.
Risk Factors
Increased maternal BMI
Diabetes
Assisted delivery
Previous shoulder dystocia
Post-dates pregnancy
Fetal macrosomia
Risk factors have poor predictive value, but the more risk
factors there are, the greater the chance of shoulder dystocia.
Diagnosis
Failure of the shoulders to deliver with the standard amount of
maternal effort and
moderate traction on the fetal head.
Retraction of the fetal head against the perineum, called the
turtle sign. The earlier the
diagnosis is made the better the chances of a positive outcome
for mother and baby.
Management It is important to remain calm and to act quickly.
The HEELPERR mnemonic has been devised as a clinical tool to
provide a structured framework in managing shoulder dystocia. It
does not serve as an algorithm but as an aid to memory about what
to do. The sequence of the manoeuvres has not yet been
systematically reviewed. The baby needs to be delivered within 5
minutes.
32
H Call for Help Be sure to state that youre dealing with a
dystocia and not just saying you need help. It would be beneficial
to also call for someone who is competent in neonatal
resuscitation.
E Patients buttocks to the Edge of the bed E Evaluate for
Episiotomy To make space when performing the entry manoeuvres but
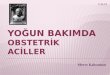
it does not reduce the dystocia L Lift the Legs (McRoberts
manoeuvre) Flex and abduct maternal legs so that the thighs rest on
the maternal abdomen. P SupraPubic pressure
Pressure is applied over the fetal anterior shoulder by an
assistant while maintaining downward traction on the fetal head. If
possible, ask the assistant to apply the pressure in the direction
that the baby is facing so as to push the impacted shoulder
forward
E Entry manoeuvres Attempt to rotate the anterior shoulder
forward into the oblique diameter and under the pubic symphysis. If
this does not help, attempt rotation of the shoulders by applying
pressure posteriorly on the anterior shoulder and anteriorly on the
posterior shoulder. If unsuccessful attempt rotation in the
opposite direction.
R Remove the posterior arm This may help in decreasing the
bisacromial diameter. Flex the fetal elbow and deliver the arm by
sweeping the arm over the anterior fetal chest wall. Be mindful of
potentially causing a fractured humerus.
R Roll the patient Roll the patient onto all-fours which may
help dislodge the impaction by means of gravity
Radical manoeuvres may need to be considered if the preceding
measures fail. Seek expert, experienced advice. The importance of
documenting the sequence of events is extremely important, along
with effective communication with the parents after what is a very
traumatic event for all. It remains paramount to be extremely
vigilant in all births and to be familiar with the various
manoeuvres so that the management of such an unpredictable
emergency can ensure a positive outcome for mother and baby.