Embed Size (px)
Citation preview

11
以實證醫學觀點探討藥物交互作用之影響
Clopidogrel with PPI
臨床藥師 : 邱 春 吉

22
OutlineOutline
BackgroundBackground
– ClopidogrelClopidogrel 、、 PPIPPI
– Drug interactionDrug interaction
Clinical ScenarioClinical Scenario
EBM EBM : : 5 A5 A
– AskAsk 、、 Acquire Acquire 、、 AppraisalAppraisal 、、 Apply Apply 、、 AA
uditudit
ConclusionConclusion

33
Drug-Drug interaction
Severity Documentation Summary
Clopidogrel-Omeprazole
Major Excellent May result in increased risk for thrombosis

44
Summary Severity Reliability Rating
PPI may diminish the therapeutic effect of clopidogrel
Major Good

55

66
Significance Onset Severity Documentation
4 Delayed Moderate Possible
Effect : The antiplatelet activity of clopidogrel may be decreased by certain PPI

77
The FDA is aware of published reports that clopidogrel (marketed as Plavix) is less effective in some patients than it is in others Differences in effectiveness may be due to – (1). genetic differences in the way the body metabolizes
clopidogrel– (2). using certain other drugs with clopidogrel can
interfere with how the body metabolizes clopidogrel.

88

99
ScenarioScenario This is a 58 years female patient who had history This is a 58 years female patient who had history
of DM & HTN and followed up at our Meta OPD. of DM & HTN and followed up at our Meta OPD.
This time, she suffered from chest pain for 2 days. This time, she suffered from chest pain for 2 days.
Due to Due to persisted chest painpersisted chest pain, she was sent to ER. , she was sent to ER.
( 2009/06/18 ). ( 2009/06/18 ).
At ER, EKG At ER, EKG revealedrevealed ST depression over V2-V4ST depression over V2-V4
and and elevated cardiac enzymeelevated cardiac enzyme..
Under the impression of Under the impression of NSTEMINSTEMI,, dual antiplatelet dual antiplatelet
and and heparinheparin were applied. were applied.
Then he was admitted to CCU for further care.Then he was admitted to CCU for further care.

1010Coronary Care Unit

1111NEJM Volume 352(24), 16 June 2005

1212 Lancet 2003
Ⅱa

1313
In CV perspective, Dual therapy is better than monotherapy
In CV perspective, Dual therapy is better than monotherapy

1414

1515

1616
Steps for Minimizing Gastrointestinal Bleeding
J Am Coll Cardiol, 2008; 52:1502-1517
PPI remains the treatment of choice to prevent GI bleeding!

1717
Cytochrome P450 2C19 playing a major role in
the bioactivation of clopidogrel
NEJM 2009;360:363-75
Carriers of a reduced-function CYP2C19 allele

1818
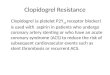
Metabolism of PLAVIX and Omeprazole: Metabolism of PLAVIX and Omeprazole: Potential for Drug–Drug InteractionsPotential for Drug–Drug Interactions
OmeprazoleOmeprazoleOmeprazoleOmeprazole
PLAVIX PLAVIX active active
metabolitemetabolite
PLAVIX PLAVIX active active
metabolitemetabolite
PLAVIX PLAVIX (Inactive Prodrug)(Inactive Prodrug)
PLAVIX PLAVIX (Inactive Prodrug)(Inactive Prodrug)
Decreased Decreased amount of amount of
PLAVIX PLAVIX metabolitemetabolite
Decreased Decreased amount of amount of
PLAVIX PLAVIX metabolitemetabolite
OmeprazoleOmeprazoleOmeprazoleOmeprazoleOmeprazoleOmeprazole(Inactive Prodrug)(Inactive Prodrug)OmeprazoleOmeprazole(Inactive Prodrug)(Inactive Prodrug)
PLAVIX PLAVIX (Inactive Prodrug)(Inactive Prodrug)
PLAVIX PLAVIX (Inactive Prodrug)(Inactive Prodrug)
LIVERLIVERLIVERLIVER
PLAVIX PLAVIX PLAVIX PLAVIX
+ + + +
Gilard M et al. J Am Coll Cardiol. 2008;51:256–60Gilard M et al. J Am Coll Cardiol. 2008;51:256–60
CYP2C19

1919
Diagrammatic representation of Diagrammatic representation of interactioninteraction
studied

2020
CYP2C19 Inducers and InhibitorsCYP2C19 Inducers and Inhibitors

2121
EBM 5 stepsEBM 5 steps
Ask
– 將病人的問題寫成 PICOAcquire
– 找資料來回答問題Appraisal
– 嚴格評讀文獻Apply
– 是否可應用到病人身上Audit – 是否可自我評估以上四個步驟的表現 自我評估以上四個步驟的表現
與施行效率與施行效率

2222
Ask an answerable question ?Ask an answerable question ?
Do Do proton pump inhibitorsproton pump inhibitors decrease decrease
thethe clinical benefit clinical benefit of of clopidogrelclopidogrel
following acute coronary syndrome ?following acute coronary syndrome ? Does concomitant treatment with a Does concomitant treatment with a
proton pump inhibitorproton pump inhibitor and and clopidogrelclopidogrel
after a myocardial infarction after a myocardial infarction increaseincrease the the
risk of risk of recurrent myocardial infarction recurrent myocardial infarction ??

2323
PICO : Therapy PICO : Therapy
Patient / Problem58 years female patient / NSTEMI (ACS)
Intervention Clopidogrel with PPI
Comparison Clopidogrel with placebo
OutcomeRisk of CV (recurrent MI), death or rehospitalization for ACS

2424
EBM 5 stepsEBM 5 stepsAsking
– 將病人的問題寫成 PICO
Acquire
– 找資料來回答問題Appraisal
– 嚴格評讀文獻Apply
– 是否可應用到病人身上Audit – 是否是否可自我評估以上四個步驟的表現 自我評估以上四個步驟的表現
與施行效率與施行效率

2525
Searching for the best Searching for the best available evidenceavailable evidence
DatabasesDatabases
Hierarchy of evidenceHierarchy of evidence
Searching strategiesSearching strategies

2626
searching evidencesearching evidence
medical database internet search engine
prefiltered unfiltered Google
YahooUpToDate
EBM-R
ACP Journal Club
Cochrane Library
Medline
PubMed
Searching for the Best EvidenceSearching for the Best Evidence

2727
Evidence-based textbooks: UpToDate, Clinical Evidence
Evidence-based journal abstrcts, Synopsis of CDSR, ACP Journal Club
Systematic Reviews: The Cochrane Library, PubMed Clinical Queries
Prefiltere
d
Studies
Syntheses
Synopses
Summaries
Systems
5S Levels
Original journal article: PubMedUnfiltered
The levels of organisation of evidence from research
Computerized decision support

2828
Searching strategiesSearching strategiesPrimary Term Synonym 1 Synonym 2
P NSTEMI ACS
I clopidogrel AND proton pump inhibitor
clopidogrel AND PPI
clopidogrel AND omeprazole
C clopidogrel AND placebo
O Re-infarction Recurrent myocardial infarction
CV mortality or morbidity
Limits: humans , english, full text , 2008 - 2009

2929

3030
Key words :
ACS AND clopidogrel AND propton pump inhibitor AND reinfarction
NSTEMI AND clopidogrel AND PPI AND recurrent MI
Clopigogrel AND proton pump inhibitor
Clopidogrel AND omeprazole
Limits :
humans , english, full text , 2008 - 2009

3131
EBM DatabasesEBM Databasesdatabases results
EBM ReviewsCochrane Database of Systematic Reviews
ACP Journal Club
Database of Abstracts of Reviews of Effects
Cochrane Central Register of Controlled Trials
3
Cochrane Library 2
MD Consult 5
Dynamed 44
Essential Evidence Plus 22
PubMed Clinical Queries 3

3232
標題:標題: Influence of omeprazole on the
antiplatelet action of clopidogrel
associated with aspirin
文獻:文獻: J Am Coll Cardiol 2008;51:256–60
實證等級:實證等級: IbIb
建議等級:建議等級: AA
搜尋到的第一篇文章標題及文獻等級搜尋到的第一篇文章標題及文獻等級

3333

3434
EBM 5 stepsEBM 5 stepsAsking
– 將病人的問題寫成 PICO
Acquire
– 找資料來回答問題
Appraisal
– 嚴格評讀文獻Apply
– 是否可應用到病人身上Audit – 是否是否可自我評估以上四個步驟的表現 自我評估以上四個步驟的表現
與施行效率與施行效率

3535

3636
Critical appraisalCritical appraisal
VValidity / Reliability alidity / Reliability
IImportance / Impactmportance / Impact
PPractice / Applianceractice / Appliance

3737

3838

3939

4040
JAMA 1993
vol 270(21)
2598-2601

4141
J Am Coll Cardiol 2008;51:256–60

4242
MethodsPatients and study protocol
We conducted a prospective, double-blind, placebo-controlled, randomized trial.
patients were randomized to 2 treatment groups: associated 20 mg/day omeprazole or placebo, for 7 days.
Platelet reactivity
Blood samples were collected on sodium citrate on Day 1 and 7 in both groups.
Laboratory physicians performed VASP phosphorylation analysis blinded to treatment group.

4343
Hierarchy of evidenceHierarchy of evidence
Syntheses
Studies
filter
unfilter

4444
Oxford Center for Evidence-based Medicine Oxford Center for Evidence-based Medicine Levels of EvidenceLevels of Evidence and and Grades of Recommendations
Grade of Recommendation
Level of Evidence
Therapy/Prevention, Aetiology/Harm
A
1a1a SR (with homogeneity*) of RCT
1b Individual RCT (with narrow Confidence Interval)
1c1c All or none
BB
2a2a SR (with homogeneity*) of cohort study
2b2b Individual cohort study (include low quality RCT; e.g., <80% follow-up)
2c2c “Outcomes” Research
3a3a SR (with homogeneity*) of case-control studies
3b3b Individual Case-Control Study
CC 44 Case-series (and poor quality cohort and case-control studies)
DD 55 Expert opinion without explicit critical appraisal, or based on physiology bench research or “first principles”

4545
J. Am. Coll. Cardiol. 2008;51;256-260
Omeprazole
( n=70 )
Placebo
( n=70 )
Analyzed (n=64)
Analyzed (n=60)
Randomization ( n=140)

4646
J. Am. Coll. Cardiol. 2008;51;256-260
83.9% 83.2%
51.4%
39.8%Platelet Reactivity Index
VASP : vasodilator stimulated phosphoprotein

4747
J. Am. Coll. Cardiol. 2008;51;256-260
omeprazoleplacebo
Platelet Reactivity Index
- 43.3%
- 32.6%

4848
ConclusionsAspirin–clopidogrel antiplatelet dual therapy is widely prescribed worldwide
PPIs frequently associated to prevent gastrointestinal bleeding.
In this randomized study, omeprazole significantly decreased the effect of clopidogrel on platelet as tested by VASP phosphorylation.
The clinical impact of these results remains uncertain but merits further investigation.
Recommend not adding systematically a PPI treatment to the antiplatelet dual therapy without formal indication.

4949
Critical Appraisal Skills Programme Critical Appraisal Skills Programme RCT:CASP (1)RCT:CASP (1)
Are the results of the study Are the results of the study valid / reliablevalid / reliable ? ? Screening Questions Yes No
Did the study ask a clearly focused question? vvWas this a randomised controlled trial (RCT)
and was it appropriately so?vv
Were participants appropriately allocated to
intervention and control groups?vv
Were participants, staff and study personnel
‘blind’ to participants’ study group?vv
Were all of the participants who entered the
trial accounted for at its conclusion? Intension to treat ? followed up complete ? (140-124)
vv

5050
Critical Appraisal Skills Programme RCT:CASP (1)
Are the results of the study Are the results of the study valid / reliablevalid / reliable ? ?
Screening Questions Yes No
Were the participants in all groups followed
up and data collected in the same way?vv
Aside from the experimental intervention, were the groups treated equally ?
vv
Were the groups similar at the start of the trial ?
vv
Did the study have enough participants to
minimise the play of chance? (n=120, 80% statistical power and 5% alpha risk) (124/140)
vv

5151
Critical Appraisal Skills Programme RCT:CASP (2)
What were the results ? Importance / ImpactImportance / Impact
Screening Questions Yes NoHow large was the treatment effect ? (ARI , NNH)
vv
How precise are these results? (CI , p value) vv
Outcome ARI RR NNHEER CER EER - CER EER/CER 1/ARI
95% CI
EER : Experimental Event Rate CER : Control Event Rate ARI : Absolute Risk Increase RR : Relative Risk NNH : Number Needed to Harm CI : Confidence Interval

5252
Critical Appraisal Skills Programme RCT:CASP (3)
Will the results help me in caring for my patients ? Practice / AppliancePractice / Appliance
Screening Questions Yes No
Were all clinically important outcomes considered ?
vv
Can the results be applied to my patient care
?vv
Are the likely treatment benefits worth the potential harms and costs ?
vv

5353
EBM 5 stepsEBM 5 stepsAsking
– 將病人的問題寫成 PICO
Acquire
– 找資料來回答問題Appraisal
– 嚴格評讀文獻
Apply
– 是否可應用到病人身上Audit – 是否是否可自我評估以上四個步驟的表現 自我評估以上四個步驟的表現
與施行效率與施行效率

5454
Clinical ApplicationClinical Application
這個研究之有效且重要的證據能實際應用到我們照顧的病人這個研究之有效且重要的證據能實際應用到我們照顧的病人病人類似性 病人類似性 ((coronary stent implantationcoronary stent implantation))診療環境之合理可行性診療環境之合理可行性病人從治療中可預防危險病人從治療中可預防危險結合實證醫學的結果、臨床專業經驗結合實證醫學的結果、臨床專業經驗– 給予病人建議給予病人建議結合病人價值觀結合病人價值觀– 幫助病人做出最後的決定幫助病人做出最後的決定
證據之外推
Grade of Recommendation
Level of Evidence
Therapy
A1a Systemic review of RCTs
1b Single RCT
1c ‘All-or-none’

5555
EBM 5 stepsEBM 5 stepsAsking
– 將病人的問題寫成 PICO
Acquire
– 找資料來回答問題Appraisal
– 嚴格評讀文獻Apply
– 是否可應用到病人身上Audit – 是否可自我評估以上四個步驟的表現 自我評估以上四個步驟的表現
與施行效率與施行效率

5656
Evaluation performance Evaluation performance measurement measurement
評估表現與施行效率評估表現與施行效率 Self – Evaluation (自我評估) Evaluation (Audit) by Expert or peer (專家監督或同儕彼此評估) Audit by organization Audit by third party (NHI, Insurance) Audit by computer

5757
Step 5: EvaluationStep 5: EvaluationSelf-evaluation: Step 1Self-evaluation: Step 1
步驟 1 :在提出臨床問題方面 1. 我有提出任何臨床問題嗎? 2. 我提出的問題結構是否完整? 3. 是否知道自己設定的問題類型?

5858
Step 5: EvaluationStep 5: EvaluationSelf-evaluation: Step 2Self-evaluation: Step 2
步驟 2 :在搜尋最佳證據方面1. 我知道在我的臨床領域中現有的最佳證據 來源嗎?2. 我是否擁有搜尋所需的軟硬體及獲得最佳 證據的管道?

5959
Step 5: EvaluationStep 5: EvaluationSelf-evaluation: Step 3Self-evaluation: Step 3
步驟 3 :在文獻評讀方面1. 對我而言,應用研究證據之評讀指引變的 更簡單嗎?2. 我可以更正確、更有效率的使用一些審慎 評估度量工具 ( 如: NNT) ?

6060
Step 5: EvaluationStep 5: EvaluationSelf-evaluation: Step 4Self-evaluation: Step 4
步驟 4 :在整合證據與病患的價值觀方面1. 我盡力將審慎評估之結果融入治療中嗎?2. 為了適用於我的病人,我在調整一些嚴格 評讀的度量值 ( 機率、 NNT等 ) 方面越來越 精準及有效率?

6161
標題:標題: Risk of Adverse Outcomes Associated With Concomitant Use of Clopidogrel and Proton Pump Inhibitors Following Acute Coronary Syndrome
文獻: 文獻: JAMA. 2009;301(9):937-44
實證等級:實證等級: II bII b
建議等級:建議等級: BB
搜尋到的第二篇文章標題及文獻等級搜尋到的第二篇文章標題及文獻等級

6262
JAMA. 2009;301(9):937-944

6363
Context
– Prior studies reported that omeprazole decreases the platelet inhibitory effects of clopidogrel.
– Yet the clinical significance of these findings is not clear.
Objective
– To assess outcomes of patients taking clopidogrel with or without a proton pump inhibitor (PPI) after hospitalization for acute coronary syndrome (ACS).
Design, Setting, and Patients
– Retrospective cohort study of 8205 patients with ACS taking clopidogrel after discharge from 127 Veterans Affairs hospitals between October 1, 2003, and January 31, 2006.

6464
Hierarchy of evidenceHierarchy of evidence
Syntheses
Studies
filter
unfilter

6565
Oxford Center for Evidence-based Medicine Oxford Center for Evidence-based Medicine Levels of EvidenceLevels of Evidence and and Grades of Recommendations
Grade of Recommendation
Level of Evidence
Therapy/Prevention, Aetiology/Harm
A
1a1a SR (with homogeneity*) of RCT
1b Individual RCT (with narrow Confidence Interval)
1c1c All or none
BB
2a2a SR (with homogeneity*) of cohort study
2b Individual cohort study (include low quality RCT; e.g., <80% follow-up)
2c2c “Outcomes” Research
3a3a SR (with homogeneity*) of case-control studies
3b Individual Case-Control Study
CC 44 Case-series (and poor quality cohort and case-control studies)
DD 55 Expert opinion without explicit critical appraisal, or based on physiology bench research or “first principles”

6666JAMA. 2009;301(9):937-944
CER EER

6767
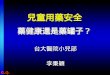
JAMA. 2009;301(9):937-944
Clopidogrel without PPI
Clopidogrel with PPI
Proportion of death or recurrent ACS
Period since discharge

6868
Conclusion (1)
This study found that concomitant use of
clopidogrel and PPI after hospital discharge
for ACS is associated with a higher risk of
adverse outcomes ( recurrent ACS )
compared with clopidogrel use without PPI.
These findings, coupled with prior studies,
suggest that concomitant PPI use may
attenuate the benefits of clopidogrel use after
ACS.

6969
Conclusion (2)
Pending further studies to confirm these
results and prospectively assess
cardiovascular outcomes for patients taking
clopidogrel plus PPI vs clopidogrel without PPI
The results of this study may suggest that PPIs
should be used for patients with a clear
indication for the medication, rather than routine
prophylactic prescription.
JAMA. 2009;301(9):937-944

7070
標題:標題: A population-based study of the drug
interaction between proton pump
inhibitors and clopidogrel
文獻: 文獻: CMAJ 2009 ;180(7):713-28
實證等級:實證等級: III bIII b
建議等級:建議等級: BB
搜尋到的第三篇文章標題及文獻等級搜尋到的第三篇文章標題及文獻等級

7171
CMAJ 2009; 180(7):713-28

7272

7373
Hierarchy of evidenceHierarchy of evidence
Syntheses
Studies
filter
unfilter

7474
Oxford Center for Evidence-based Medicine Oxford Center for Evidence-based Medicine Levels of EvidenceLevels of Evidence and and Grades of Recommendations
Grade of Recommendation
Level of Evidence
Therapy/Prevention, Aetiology/Harm
A
1a1a SR (with homogeneity*) of RCT
1b Individual RCT (with narrow Confidence Interval)
1c1c All or none
BB
2a2a SR (with homogeneity*) of cohort study
2b2b Individual cohort study (include low quality RCT; e.g., <80% follow-up)
2c2c “Outcomes” Research
3a3a SR (with homogeneity*) of case-control studies
3b Individual Case-Control Study
CC 44 Case-series (and poor quality cohort and case-control studies)
DD 55 Expert opinion without explicit critical appraisal, or based on physiology bench research or “first principles”

7575
31-90 daysWithin 30 days
91-180 days
Cases 734 (with recurrent MI): patients who died or readmitted for MI within 90 days after discharge following AMI
Controls 2057 (without recurrent MI): patient were at risk but were not readmitted because of MI before the index date
CMAJ 2009 180(7); 713-28

7676
EER 0.264 CER 0.206 OR 1.27
EER 0.063 CER 0.061 OR 1.02
EER 0.202 CER 0.145 OR 1.40
CMAJ 2009 180(7);713-28
Recurrent MI No recurrent MI
EER 0.050 CER 0.052 OR 0.94

7777
CMAJ 2009 180(7);713-28
Recurrent MI No recurrent MI

7878
Pantoprazole not associated with Pantoprazole not associated with increased risk of increased risk of recurrent myocardial recurrent myocardial
infarctioninfarction
PantoprazoleCMAJ 2009 180(7);713-28

7979
Conclusion (1)
In summary, patients taking clopidogrel following
acute myocardial infarction, the concomitant use of
a proton pump inhibitor that inhibits cytochrome
P450 2C19 ( omeprazole, lansoprazole or
rabeprazole ) was associated with an increased risk
of recurrent myocardial infarction.
This effect, which was not seen with pantoprazole
(inhibits cytochrome P450 2C9) therapy,
presumably reflects inhibition of the metabolic
bioactivation of clopidogrel.

8080
Conclusion (2) Pending further data regarding the clinical
significance of drug interactions.
Concomitant treatment with clopidogrel and proton
pump inhibitors should be minimized when possible.
If a proton pump inhibitor is required, pantoprazole
should be used preferentially in patients who are
also receiving clopidogrel.
Ranitidine or another H2-receptor antagonist
may be an appropriate alternative for patients who
require acid-lowering therapy.

8181
ACP Journal Club
Source Reference :
A population-based study of the drug interaction between proton pump inhibitors and clopidogrel
CMAJ 2009;180:713-8
Issue : Volume 151(2), August 2009, pp JC2-13

8282
ACP Journal ClubIssue: Volume 151(2), August 2009, pp JC2-13

8383
ACP Journal Club
AbstractAbstractQuestionQuestion– In older patients discharged from hospital after In older patients discharged from hospital after
acute MI , does acute MI , does concomitant use of a proton-concomitant use of a proton-pump inhibitor with clopidogrel lead to adverse pump inhibitor with clopidogrel lead to adverse eventsevents ? ?
ConclusionConclusion– concomitant use of a proton-pump inhibitor concomitant use of a proton-pump inhibitor
with clopidogrel was associated with with clopidogrel was associated with increased increased risk for readmission or death from MIrisk for readmission or death from MI within 90 within 90 days of initial discharge.days of initial discharge.

8484
Drug-Drug interaction
Severity Documentation Summary
Clopidogrel-Omeprazole
Major Excellent May result in increased risk for thrombosis

8585

8686
Warning :Warning : Concurrent use of Concurrent use of clopidogrelclopidogrel and and omeprazoleomeprazole may may
result in result in increased risk for thrombosis.increased risk for thrombosis.
Onset : Onset : Delayed Delayed
Severity : Severity : Major Major
Documentation : Documentation : Excellent Excellent
Probable Probable
Mechanism : Mechanism : decreased platelet inhibitory decreased platelet inhibitory effecteffect of clopidogrel by omeprazole of clopidogrel by omeprazole
MicroMedex

8787
Clinical Management Clinical Management
– the the clinical implications remain uncertainclinical implications remain uncertain
– the addition of the addition of proton pump inhibitorproton pump inhibitor therapy therapy
to to clopidogrel clopidogrel plus aspirin should be carefully plus aspirin should be carefully
considered and considered and onlyonly when when clearly indicatedclearly indicated..
– Consider using a Consider using a histamine-2 receptor histamine-2 receptor
antagonistantagonist in patients who required acid-in patients who required acid-
lowering therapy. lowering therapy.
– If a proton pump inhibitor is required, If a proton pump inhibitor is required,
pantoprazolepantoprazole may be preferred. may be preferred.
MicroMedex

8888
Summary Severity Reliability Rating
PPI may diminish the therapeutic effect of clopidogrel
Major Good

8989

9090

9191
55
Until further information is available, FDA recommends the following:
Clopidogrel能降低血栓風險可繼續使用 使用Clopidogrel時, 能同時使用PPI嗎 ? 依據病人之病情由醫師評估是否須同時給予PPI
同時給予 omeprazole時需特別審慎
Conclusion

9292
Until further information is available Until further information is available FDA recommendsFDA recommends
Healthcare providers should Healthcare providers should continue to continue to
prescribeprescribe and patients should and patients should continue to takecontinue to take
clopidogrelclopidogrel as directed. as directed.
Because Because clopidogrelclopidogrel has demonstrated has demonstrated
benefits in benefits in preventing blood clotspreventing blood clots that could that could
lead to a heart attack or stroke. lead to a heart attack or stroke.
Healthcare providers shouldHealthcare providers should re-evaluatere-evaluate the the
need for need for startingstarting or or continuingcontinuing treatment with treatment with
aa PPIPPI in patients in patients taking clopidogreltaking clopidogrel..

9393
Pharmacist’s comments
Concomitant use of clopidogrel and PPI Concomitant use of clopidogrel and PPI associated with a higher risk of recurrent MI.associated with a higher risk of recurrent MI.
The clinical impact remains uncertain.The clinical impact remains uncertain. Pending further data regarding the clinical Pending further data regarding the clinical
significance of drug interactions.significance of drug interactions. PPIs should be used for patients with a clear PPIs should be used for patients with a clear
indication.indication. If a proton pump inhibitor is required, If a proton pump inhibitor is required,
pantoprazole may be preferred. pantoprazole may be preferred. Ranitidine or another H2-receptor antagonist Ranitidine or another H2-receptor antagonist
may be an appropriate alternative.may be an appropriate alternative.

9494
Apply these results to our patient
藥品名稱 劑量 用法 途徑Aspirin 100 mg/cap 1pc QD PO
Clopidogrel 75 mg/tab 1pc QD PO
Heparin sodium 25000 u/5ml/vial
20000 u in 500 ml D5S, run 16 cc/hr
IVF
Rosuvastatin 10 mg/tab ½ pc QD PO
Carvedilol 25 mg/tab ½ pc BID PO
Actrapid HM 100 iu/ml, 10 ml/vial
8 u TID SC
Pantoprazole 40 mg/tab 1pc QD PO

9595
保衛康治潰樂 保栓通
去 學 術 化 術 語

9696
Evidence-Based Clinical Evidence-Based Clinical DecisionsDecisions
LiveUpdateResearch
evidences
Pt’s preferences and actions
Clinical states and environmental resources
Clinical expertises Clinical expertises & experience& experience
以病人為中心的安全醫療照護
Modified from R Brain Haynes et al.: Evid. Based Med. 2002;7;36-38.
Evidence is never enough

9797
謝謝謝謝 ! ! 請多指請多指教教 !!
Chiu Chun Chi

9898
N Engl J Med 2009;360:354-62.

9999
Cytochrome P-450 Polymorphisms and Response to Clopidogrel
Carriers of at least one CYP2C19 reduced-function allele (approximately 30% of the study population) had a relative reduction of 32.4% in plasma exposure to the active metabolite of clopidogrel, as compared with noncarriers (P<0.001).
Carriers also had an absolute reduction in maximal platelet aggregation (MPA) in response to clopidogrel that was 9 percentage points less than that seen in noncarriers (P<0.001).NEJM 360;4 january 22, 2009

100100
Cytochrome P-450 Polymorphisms and Response to Clopidogrel
NEJM 360;4 january 22, 2009
Death from cardiovascular causes, MI , stroke