Embed Size (px)
DESCRIPTION
~ Antimicrobial Resistance Rate Epidemiology Study Team. Line of Reference. MIC (mg/L). MIC (mg/L). Mean Model-Predicted Log 2 MIC. Censoring Boundary. Mean Observed Log 2 MIC. - PowerPoint PPT Presentation
Citation preview

1 Significant pairwise comparisons based on a Bonferroni overall significance level of α = 0.10. 2 Parameter estimates for the interactions were examined by plots of parameter estimates for
each combination of the two categorical variables.
Background. Recent reports describing emerging non-susceptible (NS)
Streptococcus pneumoniae (SP) isolates to levofloxacin (LEV) have become
the focus of examination. N American SENTRY Program data (1997-2001)
were analyzed to determine independent variables (ivs) predictive of MIC in
hospitalized patients with SP blood isolates.
Methods. MIC for LEV vs. patient-specific (e.g., age, specimen type, medical
service category, infection risk factors) & hospital-specific (e.g., bed count,
geographical (geo) region, study year (yr) ivs were analyzed using
multivariable general linear modeling (GLM) for censored data with backwards
stepwise elimination (at p > 0.1). Tree-based modeling was used to identify
important ivs, breakpoints in continuous ivs, and possible interactions for
inclusion into the GLM model.
Results. LEV MIC50, MIC90, MIC range & % NS for isolates (n=383, from 28
hospitals) were: 1.0, 1.0, 0.25 to >4.0, 0.3. Significant ivs associated with
percent increases in the geometric mean of MIC included: geo region
(p<0.0001; Canada, Midwest, Southwest relative to Northeast; 17-23%), study
yr (p<0.0001; other study yrs relative to 1997; 30-45%), and medical service
category (p<0.012; acute care relative to medicine; 15%). Significant
interactions were hospital duration by bed count (p=0.059) and age by primary
diagnosis (p=0.007). This model explained 44% of the variance in MIC.
When examining the performance of the model for predicting MIC for isolates
within individual hospitals by study yr, observed vs. fitted mean MIC were
highly correlated (weighted Spearman R = 0.92).
Conclusions. Despite the narrow range in MIC distribution, a moderate
proportion of variability in MIC was explained by these hospital- and patient-
specific ivs. Identification of additional ivs, such as prior antibiotic exposure by
isolate or institutional usage, would probably be needed to explain more of this
variability. These data might be used to tailor empiric treatment and to
prospectively curtail the growing incidence of NS SP to LEV and other
fluoroquinolones.
Relationships Between Susceptibility of Streptococcus pneumoniae Against Levofloxacin & Hospital- & Patient-Specific Variables:Report From the Antimicrobial Resistance Rate Epidemiology Study Team (ARREST Program)
SM Bhavnani1,2, JP Hammel1, A Forrest2, PG Ambrose1, RN Jones3
1Cognigen Corporation, Buffalo, NY; 2SUNY at Buffalo, NY; and 3The JONES Group, North Liberty, IA
77
INTRODUCTION
• The Antimicrobial Resistance Rate Epidemiology Study Team (ARREST
Program) was established as a collaborative effort between scientists
from The JONES Group and Cognigen Corporation in order to use
surveillance data and analytic techniques to better understand factors
predictive of antimicrobial resistance.
• Data from surveillance programs such as the SENTRY Antimicrobial
Surveillance Program have proven to be a valuable resource and have
been used to alert the scientific and medical communities to problems of
antimicrobial resistance.
• In response to the growing prevalence of antimicrobial-resistant
S. pneumoniae, this analysis was undertaken to determine independent
variables predictive of MIC in hospitalized patients with S. pneumoniae
blood isolates.
GLM Model Results
• Canada, Midwest, and Southwest U.S. were associated with 17-23%
increases in mean MIC in comparison to the Northeast U.S.
• Study years after 1997 had a higher mean MIC than 1997 by 30-45%.
• Isolates from acute care patients had mean MIC values which were 15%
higher than those from patients on medicine services.
• Significant two-way interactions included duration of hospital stay prior
to pathogen isolation*hospital bed count, and primary diagnosis*patient
age.
• The model explained a moderate proportion of the variability in MIC
between patients (R2 = 44%).
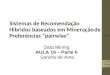
• However, when fit by institution as shown in Figure 2, model-predicted
mean MIC within hospitals was strongly correlated with observed mean
MIC averaged over all study years (Spearman correlation = 0.92). A
high correlation was also seen when averages were computed for
institution by year (Spearman correlation = 0.83).
Data Collection
• Patient- and institution-specific and susceptibility data for
S. pneumoniae blood isolates (one per patient) collected from North
American hospitals participating in the SENTRY Antimicrobial
Surveillance Program (1997-2001) were queried for analysis.
Primary Outcome
• The primary outcome variable was the in vitro activity of levofloxacin
against S. pneumoniae which was measured by the minimum inhibitory
concentration (MIC).
• Observed values of MIC included left- and right-censored values of the
form 0.5 (or 0.25 for 1997) and >4, respectively.
• A log2 transformation of MIC was used to achieve approximate normal
error distributions.
• Using NCCLS interpretive criteria, MIC values were classified as
susceptible (2), intermediate (4), and resistant (>4).
Independent Variables
• Patient-specific variables included age, sex, specimen type, medical
service category, infection risk factors, primary diagnosis, duration of
hospital stay prior to pathogen isolation, nosocomial infection, and
residence in an ICU.
• Additional independent variables included study year and institution-
specific variables (hospital bed count, geographic region, and formulary
demographics).
Tree-Based Modeling
• Using S-Plus 6.0.1 for Unix, tree-based modeling was carried out to
identify subgroups that manifested impressive differences in MIC using
recursive partitioning.
• Potential two-way interactions between independent variables for
inclusion in regression modeling were identified.
Multivariable General Linear Modeling (GLM) for Censored Data
• Using SAS 8.2, GLM for censored data was carried out.
• Continuous independent variables were categorized into subgroups
(using breakpoints to define interpretable subgroups of sufficient size) to
account for potential nonlinear relationships.
• The model was constructed using backward stepwise elimination
(p>0.10).
• The proportion of error variance explained by the model (denoted as R2)
was used to measure model precision.
• A Spearman correlation measure was used to assess the strength of
association between model-predicted and observed MIC means within
institutions, across all study years and within study years.
METHODS
• 383 S. pneumoniae blood isolates from 28 hospitals were collected.
• 7 and 5 hospitals were located in the Midwest and Northeast
regions of the U.S.
• All other regions had 4 hospitals each.
• The variability in observed MIC was narrow with an estimated standard
deviation of 0.60 on the log2 scale and a range of observed MIC values
from 0.25 to >4 (Figure 1).
• There were 67 (17%) left-censored observations (with MIC values of
0.25 or 0.5) and one right-censored observation.
• Proportions of isolates by categories of each independent variable are
summarized in Table 1.
• Based on the results for the tree-based model, two-way interactions
were selected for consideration in the multivariable GLM.
RESULTS
Figure 1: MIC Histogram of All S. pneumoniae Blood Isolates (N=383)
Table 2: Parameter Estimates from the GLM Model for Censored Data
Table 1: Proportion of Isolates by Selected Independent Variables
• These data demonstrate a significant increase in the MIC of levofloxacin to
S. pneumoniae over the study period.
• The use of GLM tailored censored data allowed for prediction of MIC and
estimation of the likelihood of non-susceptibility based on patient- and
institution-specific factors.
• Given the independent variables evaluated, a moderate proportion of
variability in the MIC at the patient level was explained. As part on our on-
going efforts, the impact of additional patient and institution-specific
variables on model-precision will be evaluated, including prior antimicrobial
usage.
• This type of model can be further applied to identify subgroups of patients at
increased risk for infection arising from organisms with increased MIC.
Prospective identification of such risk factors and appropriate intervention
may then arrest further progression of increasing MIC values.
CONCLUSIONS
ABSTRACT
• As shown by the Line of Reference, the observed MIC distribution shifts
to the right as the model-predicted MIC increases.
• Isolates in the lower third of the model-predicted MIC distribution were
all susceptible with an extremely low estimated probability of non-
susceptibility by a fitted normal curve.
• Isolates in the middle third were all susceptible with only a low
probability of non-susceptibility, though the observed mean MIC was
higher than that of the lower third.
• Only one of the isolates in the upper third was non-susceptible. The
probability of non-susceptibility as estimated by a fitted normal curve
was low.
• The percent of isolates from Canada, the Midwest, and the Southwest
U.S., combined, represented 35%, 41%, and 60% of the lower, middle,
and upper third subgroups based on the model-predicted MIC values.
Specifically, these percentages for isolates from Canada were 18%,
14%, and 23%, respectively.
Figure 2: Mean Model-Predicted MIC vs. Mean Observed MIC at the
Institution Level
Figure 3: Histograms of Observed MIC for Isolate Subgroups Falling in
the Lower, Middle and Upper Third of Model-Predicted MIC
Figure 3a: Lower Third (n=127)
Figure 3b: Middle Third (n=128)
Figure 3c: Upper Third (n=128)
N %Patient Age
<18 71 18.519-40 88 2341-60 104 27.261-75 76 19.8>75 44 11.5
Medical ServiceAcute Care 30 7.8Medicine 200 52.2Pediatrics 38 9.9Surgery 30 7.8Other 85 22.2
Primary DiagnosisCardiopulmonary 188 49.1Genitourinary 9 2.3GI/Abdom/Liver 13 3.4Immunocompromised 28 7.3Infection 19 5Neurologic 18 4.7Trauma 5 1.3Other 103 26.9
Duration of Hospital Stay Prior to Pathogen Isolation<=1 day 318 832-5 days 45 11.76-10 days 9 2.311-20 days 6 1.621-30 days 2 0.5>30 days 3 0.8
Hospital Bed Size<=400 116 30.3401-900 215 56.1901-1350 46 12>1350 6 1.6
Geographic RegionCanada 71 18.5Northeast 105 27.4Midw est 86 22.5Southeast 34 8.9Southw est 41 10.7West 46 12
Variable Category (N = 383)
Fre
quen
cy
<=0.25 or <=0.5uncensored>4
0
50
100
150
200
250
0.25 0.5 1 2 4mean AUC = 0.68MIC (mg/L)
Mean MIC = 0.68
Rel
ativ
e F
requ
ency
(%
)
<=0.25 or <=0.5uncensored>4
0
20
40
60
80
100
0.25 0.5 1 2 4
Rel
ativ
e F
requ
ency
(%
)
0
20
40
60
80
100
0.25 0.5 1 2 4
Re
lativ
e F
requ
en
cy (
%)
0
20
40
60
80
100
0.25 0.5 1 2 4
MIC (mg/L)
Line of Reference
Variable Category Estimate Standard Error P-Value Significant Pairs1
Intercept -0.7707 0.1297
Study Year <0.0001 1997 < other study years
1997 0
1998 0.3793 0.0712
2000 0.324 0.0808
2001 0.538 0.1189
Geographic Region <0.0001Northeast, Southeast, West <
Canada, Midw est
Canada 0.3019 0.0913 West < Southw est
Northeast 0
Midw est 0.2926 0.0785
Southeast -0.0216 0.1016
Southw est 0.2208 0.0991
West -0.1447 0.1109
Medical Service 0.012 Medicine < Other
Acute Care 0.2007 0.1038
Medicine 0
Pediatrics -0.0991 0.1255
Surgery 0.0882 0.1108
Other 0.1909 0.0715
Primary Diagnosis * Patient Age2 0.007
Prior Duration of Hospital Stay * Bed Count2 0.059
Mean Observed Log2(MIC)
Me
an
Mo
de
l-pre
dic
ted
Lo
g2
(MIC
)
-1.2 -0.8 -0.4 0.0
-1.2
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
0.2Weighted Spearman R = 0.92
-1.2 -0.8 -0.4 0.0
-1.2
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
0.2
-1.2
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
0.2
Mean Observed Log2 MIC
Mea
n M
od
el-P
redi
cte
d L
og2
MIC
Censoring Boundary
For more information, please contact:Sujata M. Bhavnani, Pharm.D.
Cognigen Corporation395 Youngs Road, Buffalo, NY, [email protected]
716-633-3463, ext. 273