Embed Size (px)
Citation preview

RHEUMTOID ARTHRITIS
台中榮民總醫院臨床藥學科鄭鴻基主任

前言 -1 類 風 濕 性 關 節 炎 ﹙ Rheumatoid
Arthritis , RA﹚是一種慢性的全身性、發炎性的自體免疫疾病。而所謂自體免疫疾病,就是病人本身免疫系統的功能過度活躍,導致不但會攻擊外來的異物,也會去侵犯自身的正常的組織器官而產生自體組織器官的損傷。

前言 -2 特徵:無化膿性增生性滑膜炎,經過一段時間後會導致關節軟骨破壞,及漸進破壞性關節炎。另外也會侵犯全身各個組織器官,使病患的活動受阻礙,甚至最後必須藉助別人的幫助才能維持正常作息。 RA至目前為止仍無法完全治癒。因此,對於 RA病人成功的處理方法,除了需要對疾病的病理、生理及進展過程有正確的認知外,還需確認個別的治療目標,了解不同的治療方式及其潛在的效力和毒性。

流行病學目前全球大約有 1﹪~2﹪的人口患此疾病。然而 RA並不是老人的專利,它可以在任何年齡出現,約有 70﹪的病人是介於 30至 60歲之間,而以 40歲為其高峰。一般而言女性與男性的罹患比例是 3: 1,但是這種差異在年老者並不存在。而台灣每千人有四人罹患類風濕性關節炎,其中以生育年齡的女性最易發生。

RA的流行病學英國 1990-1991 年男性和女性類風濕性關節炎

USA -Arthritis
1985 - 3 千 5 百萬 關節炎病患1995 - 4 千萬 關節炎病患2020 - 5 千 9 百萬 關節炎病患
第二大無法就業原因第二大無法就業原因估計每年對經濟影響有估計每年對經濟影響有 650650億美元億美元

病理機轉類風濕性關節炎的病因至今仍然不明,只知其大概的病理機轉( Fig1)為:當外來的類風濕因子( RF)去刺激滑膜腔內的macrophage釋放 出 第 一 介 白 質 ( IL1 ) , 而 刺 激 T-lymphocyte,使之活化並產生兩條免疫路徑。其中一條路徑為,活化的 T-lymphocyte會釋放出化學趨化物質( chemical mediator ),進而刺激macrophage 對 RF的吞噬作用。另一路徑為,活化的 T-lymphocyte會釋放出第二介白質( IL2 ),進而產生一連串的發炎反應,最後導致軟骨關節的破壞。








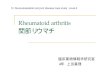
Figure 1F. A working classification of chronic polyarthritis.
A working classification of chronic polyarthritis. It is important to classify each patient because of differences in prognosis between the various syndromes. RF+, RF , and RF± refer to results of tests for IgM rheumatoid factor. Adult juvenile rheumatoid arthritis (AJRA) and remitting seronegative symmetrical synovitis with pitting edema (RS3PE) are examples of subsets of seronegative
polyarthritis (SP). Nodules, vasculitis, sicca syndrome, and Felty syndrome may develop in subsets of patients with rheumatoid arthritis (RA). Palindromic rheumatism (PR), nodulosis (N), and seronegative symmetric synovitis of the wrists (S3) are recognizable syndromes included in the
ambiguous category of RF±.


Approximately 80% of adult patients with chronic polyarthritis treated at referral center clinics are consistently RF+. Most develop radiographic evidence of bony erosions within the first 2 years of disease (Figure 2). Subsets of this group develop extra-articular features as well, such as nodules (Figure 3), vasculitis, sicca features, and Felty syndrome.
DIAGNOSIS > Rheumatoid Arthritis

Figure 2. Radiograph of right hand showing bony erosions.
Radiograph of right hand showing bony erosions at the proximal interphalangeal and metacarpophalangeal joints.

( Fig4 ): PIP erosion 與 MCP erosion的位置圖。

Figure 3. Flexion deformities in rheumatoid arthritis.
Flexion deformities in rheumatoid arthritis. Rheumatoid nodules have developed at sites of trauma over the proximal interphalangeal joints of the third and fourth fingers.


Figure 4. Joint damage is both irreversible and cumulative.
Joint damage is both irreversible and cumulative. Although inflammation often gradually subsides over time it does not go away completely.

Irreversible loss of function due to structural damage to cartilage, bone, tendon, and capsule is cumulative (damage = inflammation X intensity X time). Irreversible damage can occur relatively rapidly (in several months).

Table 3. Remission of rheumatoid arthritis*
1. Duration of morning stiffness <15 min
2. No fatigue
3. No joint pain
4. No joint tenderness or pain on motion
5. No swelling in joints or tendon sheaths
6. ESR <30 mm/h for women, <20 mm/h for men
*American College of Rheumatology definition. Five of six criteria must exist for at least 2 months.ESR erythrocyte sedimentation rate.

緩解期的徵兆類風濕性關節炎是種慢性疾病。 美國風濕病學學會 (ACR) 對類風濕性關節炎之緩解所下的定義,可參考下列的徵兆。如果你在至少連續二個月的期間內,出現了以下所述五種以上的徵兆,那麼這就可能指出你的類風濕性關節炎正處於緩解期: ‧ 早上時關節感到僵硬,但持續不到十五分鐘
‧ 不會有疲倦感‧ 關節並不會疼痛‧ 關炎無觸痛感或移動時不會感到疼痛‧ 關節或肌腱鞘等處並無軟組織腫脹的情形‧ 女性紅血球沈降速率 (ESR) 小於 30mm/hr ,而男性小於 20mm/hr


類風濕性關節炎的診斷標準為何?
人常會將類風濕性關節炎和風濕性關節炎混為一談,其實這是兩種不同的疾病。因為風濕性關節炎發病通常是急劇的,關節紅腫疼痛得厲害;類風濕性關節炎大多發病緩慢,關節不會紅腫但呈腫脹僵硬、多發性,同時病因不明。

類風濕性關節炎的診斷標準為何?
類風濕性關節炎是屬於一種關節炎症為主的慢性反覆發作的全身性疾病。初期時,關節會疼痛、腫脹和功能有障礙,和風濕性關節炎一樣;但晚期時關節會僵硬和畸形,可能導致殘廢。
類風濕性關節炎到目前為止,未發現一定的病因,病變大致在關節滑膜,其次是槳膜、心臟、肺部或是皮膚、眼部、血管等組織器官,而且一旦發病,時輕時重且多發性。

類風濕性關節炎的診斷標準為何?
診斷類風濕性關節炎,均是引用美國風濕病學會制定的標準,其內容如下:1. 早晨僵硬的時間超過一個小時以上。2. 醫生觀察到三個或三個以上關節部位的組織 有腫脹的情況。3. 手腕、掌指間關節腫脹超過六週。4. 對稱性關節﹝如身體兩側相同關節﹞同時腫 脹或先後發病。5. X光檢查出手部或手腕關節軟骨周圍骨質稀 疏改變。6. 類風濕因子呈陽性。7. 類風濕結節。

類風濕性關節炎的診斷標準為何?
如果上述情況 1~4 的情況必須持續六週;具備以上4種或4種以上的條件,就可以診斷為類風濕性關節炎。
若能真正了解此疾病的診斷標準,就可預防因為醫生或病人誤治或誤診而引起不必要的後果。


Normal cortical & trabecular bone

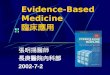
Figure 8. The natural radiographic history of a pocket erosion.
The natural radiographic history of a pocket erosion with successful suppression of inflammation. A, Normal cortical and trabecular bone. B, The earliest detectable lesion is a break in the bony cortex followed by C, loss of spongy bone to produce a pocket erosion. Rarely, these pockets are filled in with new bone and disappear. D, Most often, they become recorticated with the reformed cortical bone outlining the erosive pocket.




骨關節炎診斷與評估空間變窄並有骨贅的形成

類風濕性關節炎的診斷與評估正常和罹患 R A的手部 X 光片

Table 2. The 4 R s: role of the generalist in treatment of rheumatoid arthritis and seronegative polyarthritis
Refer patient to rheumatologist early before irreversible damage has occurred
Reinforce the basic program of rest and exercise and monitor the patients drug program
Return the patient periodically to the rheumatologist for reassessment of prognosis and treatment program
Review the goals of the therapeutic program with the patient annually; if goals are not being met consider obtaining a second opinion

Table 4. Six steps to successful therapy for seropositive rheumatoid arthritis 1. Accurate diagnosis and prognosis
2. Precise assessment, initial and serial, using clinical, radiographic, and laboratory variables
3. Explain pathophysiology and basic program to patient
4. Use whatever drugs it takes to control synovitis
5. Monitor serially for drug effectiveness and for side effects with gradual dose reduction after sustained remission
6. Never completely withdraw therapy from a patient in remission

Education, counseling, physical therapy, changes in
lifestyle
Fast-acting non-steroidal anti-inflammatory drugs
Slow-acting anti-inflammatory drugs
Systemic corticosteroids
Cytotoxic therapy
ExperimentalSurgery Local corticosteroid
injections
Pyramidal schema of the treatment of RA


Sawtooth Paradigm

Strategies of combining antirheumatic drug
Time
Step-down bridge
Time
Time Time
Step-up
Overlap and Switch Parallet



NSAIDs

NSAID-Gastropathy: U.S. Mortality Data for Several Selected Disorders in 1997
20,197
16,685 16,500
10,503
5,3384,441
1,437
0
5,000
10,000
15,000
20,000
25,000
Cause of Death
No
. o
f D
ea
ths
Wolfe et al. N Engl J Med 1999;340:1888-1899
=33

一般常用的 NSAIDS
商品名 Relifex Voltaren Naprosyn Brufen Cinopal Indocid Profenid Surgam Tilcotil Feldene Mobic
製造廠 美占史克 汽巴嘉基 中化 Kaken 氰胺 默克 Rhone-poulenc 龍壽 / 赫斯特 羅氏 Pfizer 百靈佳
化學名稱 nabumetone diclofenac naproxen ibuprofen fenbufen indomethacin ketoprofen tiaprofenic acid tenoxicam piroxicam Meloxicam

Selective vs Specific
COX-1Selective
(Ratio > 1)
Equipotent forCOX-1 and COX-2
(Ratio = 1)
COX-2
Selective(Ratio < 1)
AspirinIndometha
cinSulindac
PiroxicamNaproxenDiclofenacIbuprofen
NabumetoneEtodolac
Meloxicam*Nimesulide
**
*Meloxicam Boerhinger-Ingelheim
**Nimesulide Various
COX-2
Specific(Ratio< < 1)
Celecoxib ~1/400
Rofecoxib (VIOXX)
~1/1000

BUTAZOLIDIN
Salicylic
Propionic AnthranilicAcetic
oxicamscarboxilic
acidspyrazolones
phenylacetic acid
efficacyWHY SO MANY ?
ASPIRIN 1898 Indoleacetic acid
non-acetyl
safety
Nabumetone
IbuprofenKetoprofenNaproxen
Tolmetin
Mefenamic acid
Diclofenac
PiroxicamMeloxicam
DOLOBIDSulindacEtodolac
TRILISATEDISALCID
pyrolacetic acidIndomethacin
NSAIDs

112/04/08
HypothesisCOX-2 Specific Inhibitors
will be anti-inflammatory and analgesic without thetypical side effects
of NSAIDs.





Prostaglandins and Renal
Function
Prostaglandins and Renal
Function The relative roles and importance of COX-1 and COX-2 in the kidney are not well understood.
The deleterious renal effects of NSAIDs in patients at risk are well established.
The renal profile of each COX-2 inhibitor, approved or investigational, has yet to be fully established.
The relative roles and importance of COX-1 and COX-2 in the kidney are not well understood.
The deleterious renal effects of NSAIDs in patients at risk are well established.
The renal profile of each COX-2 inhibitor, approved or investigational, has yet to be fully established.

Goals of Arthritis TherapyGoals of Arthritis Therapy Achieved by conventionalGoal NSAIDs
Relieve pain/inflammation yes
Minimize risk of therapy no
Retard disease progression no
Prevent work disability unknown
Enhance quality of life and functional independence yes/no
Achieved by conventionalGoal NSAIDs
Relieve pain/inflammation yes
Minimize risk of therapy no
Retard disease progression no
Prevent work disability unknown
Enhance quality of life and functional independence yes/no

Two Forms of CyclooxygenaseTwo Forms of Cyclooxygenase
Produces prostanoids that mediate homeostaticfunctions
Constitutively expressed
Especially important in:– Gastric mucosa; small
and large bowel mucosa– Kidney– Platelets– Vascular endothelium
Produces prostanoids that mediate homeostaticfunctions
Constitutively expressed
Especially important in:– Gastric mucosa; small
and large bowel mucosa– Kidney– Platelets– Vascular endothelium
Cyclooxygenase-1 (COX-1)Cyclooxygenase-1 (COX-1)
Produces prostanoids that mediate inflammation, pain, and fever
Induced mainly at sites of inflammation by cytokines
Constitutive expression in:– Brain– Kidney (mainly animal data)
Produces prostanoids that mediate inflammation, pain, and fever
Induced mainly at sites of inflammation by cytokines
Constitutive expression in:– Brain– Kidney (mainly animal data)
Cyclooxygenase-2 (COX-2)Cyclooxygenase-2 (COX-2)
DuBois et al. FASEB J. 1998; 12: 1063–1073DuBois et al. FASEB J. 1998; 12: 1063–1073

Diagrammatic Representations of the COX-1 and COX-2 Structure
As Determined by X-Ray Crystallography
Kurumbail et al. Kurumbail et al. Nature.Nature. 1996; 384: 644-648 1996; 384: 644-648
COX-1 COX-2
Hydrophilic “side pocket”
Hydrophobicchannel
N-terminal N-terminal
Hydrophobicchannel
Bulky isoleucineat position523 closeshydrophilic“side pocket”
Smallervaline at
523 openshydrophilic
“side pocket””
Arginineat 120
C-terminalcontainingactive sites
C-terminalcontainingactive sites
Arginineat 120

COX / Substrate Interaction
COX-1
N-terminal
Arginineat 120
C-terminalcontainingactive sites
Arach
idon
ic Acid PG
Kurumbail et al. Kurumbail et al. Nature.Nature. 1996; 384: 644-648 1996; 384: 644-648

Classical NSAID: Non-specific binding to COX-1 and COX-2
Terminal Carboxylic Acid Plays an Important RoleCOX-1
N-terminal
Carboxylicgroup
of NSAIDforms
“salt bridge”with
Arginineat 120
C-terminalcontainingactive sites
Arach
idonic Acid
NSAID(flurbiprofen)phenyl group
binds tohydrophobic
channel
COX-2
N-terminal
Carboxylicgroup
of NSAIDforms“salt
bridge”with
Arginineat 120
C-terminalcontainingactive sites
Arach
idonic Acid
NSAID(flurbiprofen)phenyl group
binds tohydrophobic
channel
Kurumbail et al. Kurumbail et al. Nature.Nature. 1996; 384: 644-648 1996; 384: 644-648

Celecoxib: A “Purpose Designed” Specific COX-2
Inhibitor
Penning et al. Penning et al. J Med ChemJ Med Chem. 1997; 40: 1347. 1997; 40: 1347
Polar sulfonamidegroup to bind to hydrophilic “side pocket”
Methylphenyl group to bind tohydrophobic channel
No terminal acidgroup to bind to Arg120 in COX-1
3
NN
H C
CF3
S
NH2
OO
OO

Specific COX-2 Inhibitor Binding to COX-2
Exploitation of the “Side Pocket”
COX-2
Hydrophilic “side pocket”
N-terminal
C-terminalcontainingactive sites
Arg 513,Hist 90 – forms hydrogen bonds with oxygen in sulfonamide side chain
Specific COX-2 inhibitor – phenyl group binds tohydrophobic channel
Arach
idonic Acid
Arg 120
Kurumbail et al. Kurumbail et al. NatureNature 1996; 384: 644-648 1996; 384: 644-648

NSAIDs: Unmet Medical Need
Widely used for chronic treatment of arthritis and pain
Significant side-effects: Gastric and intestinal toxicity (serious
events in 2 to 4% per year) Decreased renal function in renally
compromised patients Reduced platelet function (bleeding
events rare; platelet effects may contribute to morbidity and mortality of GI bleeding)

PharmacokineticsCelecoxib
Absorption 75% bioavailability food enhances bioavailability by 7-
20% Distribution
97% bound to plasma proteins Protein binding is independent of
drug concentration 3% unbound with linear kinetic profile
Karim A et al. Pharm Res 1997;14(supp11):S-617.Data on File: Searle

Pharmacokinetics Celecoxib
Metabolism hepatic metabolism by cytochrome
P450 2C9 inactive metabolites
Excretion 57% fecal 29% of excretion is the carboxylic
acid metabolite in the urine <1% unchanged drug in the urine
Karim A et al. Pharm Res 1997;14(supp11):S-617.Data on File: Searle

Metabolism of Celecoxib
CelecoxibCelecoxib
CFCF33
NNNN
SOSO2 2 NHNH22
P450 2C9P450 2C9
HydroxylationHydroxylation
CFCF33
NNNN
Glucuronide of theGlucuronide of theAcid MetaboliteAcid Metabolite
(urinary)(urinary)
SOSO2 2 NHNH22
Glucuronide-OOCGlucuronide-OOC
CFCF33
NNNN
SOSO2 2 NHNH22
Inactive AlcoholInactive AlcoholMetaboliteMetabolite
HOHHOH2 2 CC
CFCF33
NNNN
SOSO2 2 NHNH22
HOOCHOOC
OxidationOxidation
Inactive AcidInactive AcidMetabolite (major)Metabolite (major)
HH3 3 CC
ConjugationConjugation

No effect on drugs studied:No effect on drugs studied:
– MethotrexateMethotrexate
– LithiumLithium
– GlyburideGlyburide
– WarfarinWarfarin
– PhenytoinPhenytoin
– TolbutamideTolbutamide
Drug-Drug InteractionsDrug-Drug Interactions

Incidence of GI Symptoms (>2%)Incidence of GI Symptoms (>2%)North American Controlled Arthritis TrialsNorth American Controlled Arthritis Trials
Celecoxib
AdverseEvent
Placebo 100 mgBID
200 mgQD
200 mgBID
NSAID
n 1864 1779 453 1914 2098
AbdominalPain
2.8 3.4 2.0 5.2 8.2†
Dyspepsia 6.2* 8.7 4.6 9.9 12.0‡
Diarrhea 3.8** 5.0 3.5 6.6 6.1
Nausea 4.2 3.6 2.4 3.7 5.6§
Flatulence 1.0*** 2.1 2.2 2.3 3.7ƒ
* placebo < celecoxib, p=0.004** placebo < celecoxib, p=0.008*** placebo < celecoxib, p=0.003
† celecoxib < NSAID, p=0.21‡ celecoxib < NSAID, p<0.001§ celecoxib < NSAID, p=0.002ƒ celecoxib < NSAID, p=0.003
Data on File: Searle

0.00
0.05
0.10
0.15
0.20
0.25
0 7 14 21 28 35 42 49 56 63 70 77 84Days
Cu
mu
lati
ve P
rob
ab
ility
NSAIDsn=2,427Celecoxibn=3,216Placebon=1,136
GI DiscomfortAbdominal Pain, Nausea, or
Dyspepsia
NSAIDs compared to Celecoxib, p<0.01Placebo compared to Celecoxib, p=NS
Data on File: Searle

Rate of Severe UGI Events
Patient Years Rate# of Patients Exposure # of Events (% per year)
NSAIDs 2,768 535 9 1.7%
Celecoxib 6,376 1,020 2 0.2%50-800mg/day
Placebo 1,864 208 0 –
Open-Label 4,499 5,002 9 0.18%Celecoxib
Non-UsersRodriguez et al 16,672 1,000,000 1,012 0.1%McDonald et al 73,792 220,540 510 0.23%Gutthann et al 5,770 385,000 385 0.1%Singh et al 411 1,035 3 0.29%
Rodriguez et al. Arch Int Med 1998; 158:33-39. McDonald et al. BMJ 1997; 315: 1333-1337.Gutthann et al. Epidemiology 1997; 8 (1): 18-24. Singh G et al. Am J Med 1998; 105 (1B): 31S-38S. Data on File: Searle

Withdrawal Rates for Adverse Events6 Month Study (-041)
00
55
1010
1515
2020
2525
00 22 44 66 88 1010 1212 1414 1616 1818 2020 2222 2424
Diclofenac SR 75mg BIDDiclofenac SR 75mg BID
Celecoxib 200mg BIDCelecoxib 200mg BID
%
% p
atie
nts
wit
hd
raw
np
atie
nts
wit
hd
raw
n
WeeksWeeksGeis GS et al. Geis GS et al. Arthritis & RheumArthritis & Rheum 1998;41(9) Suppl:1699A. 1998;41(9) Suppl:1699A. Data on File: Searle (Study 041)Data on File: Searle (Study 041)
p=0.001p=0.001

Celecoxib Allergic Reactions
Placebo(n= 1864)
Celecoxib(N=4146)
NSAID (n= 2098)
Rash 2.1 %2.1 % 2.2 %2.2 % 1.8 %1.8 %
Pruritus 1.7 %1.7 % 1.5 %1.5 % 1.2 %1.2 %
Urticaria 0.3 %0.3 % 0.5 %0.5 % 0.6 %0.6 %
Skin Disorder 0.3 %0.3 % 0.2 %0.2 % 0.6 %0.6 %
Searle: Data on file

112/04/08
CELEBREX™ (celecoxib):A COX-2 Specific Inhibitor
Phase III trials show that the promise of science and technology has been kept
Potent anti-inflammatory/analgesic effects
COX-1 sparing at clinical doses Unlike conventional NSAIDs, treatment
with celecoxib is no longer a “double-edged sword”

CORTICOSTEROIDS




類風濕性關節炎 藥物的選擇
全身性皮質類固醇研究顯示,全身性皮質類固醇能減緩疾病的進展。雖然只有服藥時才能出現這種效力,但就減輕關節的損傷來說,長期來說這或許能帶來好處。低劑量皮質類固醇是用來:‧ 等待緩解時,抑制疾病的進展;‧ 儘量縮減疾病在短時間內的活動力,比如說在疾 病突然惡化時;‧ 服藥時,控制多餘的症狀並改善關節的功能。






類風濕性關節炎 藥物的選擇
DMARD 如果 NSAID仍舊無法控制住類風濕性關節炎患者
的病情,那麼他們就可以 接受疾病改變抗風濕藥物 (DMARD) 的治療。這種藥物治療的目的,主要是用來緩解病情,並達到對該疾病的最大控制。大多數的 DMARD 均能減緩類風濕性關節炎的進展,並預防關節出現額外的惡化情形。總而言之,DMARD 的作用緩慢,得花上一到六個月才能發揮效力。

類風濕性關節炎 藥物的選擇
是否選擇DMARD 會受下列因素影響: ‧(病患)服用的方便性
‧ 追蹤檢查的需要‧ 毒性風險‧ 醫師對病患預後的判斷‧ 效力顯現的時間(有些DMARD得花上六個月才會發揮效用,但大多數的病患只花二到三個月的時間就享受到它的好處了。)‧ 醫師對病患是否遵守服藥原則的判斷‧ 藥物治療與追蹤檢查的花費

Azathioprine
Imuran 50mg/tab; 50mg/amp

Indications Use Adjunct with other agents in prevention of
rejection of solid organ transplants; also used in severe active rheumatoid arthritis unresponsive to other agents; other autoimmune diseases (ITP, SLE, MS, Crohn's disease)
Pregnancy Risk Factor D Lactation Excretion in breast milk unknown/not
recommended Contraindications Hypersensitivity to
azathioprine or any component of the formulation; pregnancy

Warnings/Precautions Chronic immunosuppression increases
the risk of neoplasia; has mutagenic potential to both men
and women and with possible hematologic toxicities;
use with caution in patients with liver disease, renal impairment; monitor hematologic function closely

Adverse Reactions Dose reduction or temporary withdrawal allows
reversal >10%: CNS: Fever, chills GIl: Nausea, vomiting, anorexia, diarrhea Hema: Thrombocytopenia, leukopenia, anemia Miscellaneous: Secondary infection 1% to 10%: Derma: Rash Hema: Pancytopenia Hepatic: Hepatotoxicity <1%: Hypotension, alopecia, maculopapular rash, aphthous stomatitis, arthralgias, which
include myalgias, rigors, retinopathy, dyspnea, rare hypersensitivity reactions

Drug Interactions Increased toxicity: Allopurinol may increase
serum levels of azathioprine's active metabolite (6-MP). Decrease azathioprine dose to 1/3 to 1/4 of normal dose.
Ethanol/Nutrition/Herb Interactions Herb/Nutraceutical: Avoid cat's claw, echinacea (have immunostimulant properties).

Mechanism of Action Azathioprine is an imidazolyl
derivative of 6-mercaptopurine; antagonizes purine metabolism and may
inhibit synthesis of DNA, RNA, and proteins; may also interfere with cellular metabolism and inhibit mitosis

Pharmacodynamics/Kinetics
Distribution: Crosses placenta Protein binding: ~30% Metabolism: Extensively by hepatic xanthine
oxidase to 6-mercaptopurine (active) Half-life elimination: Parent drug: 12
minutes; 6-mercaptopurine: 0.7-3 hours; End-stage renal disease: Slightly prolonged Excretion: Urine (primarily as metabolites)

Usual Dosage-1 I.V. dose is equivalent to oral dose (dosing
should be based on ideal body weight): Children and Adults: Solid organ transplantation: Oral, I.V.: 2-5
mg/kg/day to start, then 1-2 mg/kg/day maintenance
Adults: Rheumatoid arthritis: Oral: 1 mg/kg/day for 6-8 weeks; increase
by 0.5 mg/kg every 4 weeks until response or up to 2.5 mg/kg/day

Usual Dosage-2 Dosing adjustment in renal impairment: Clcr 10-50 mL/minute: Administer 75% of
normal dose daily Clcr<10 mL/minute: Administer 50% of normal
dose daily Hemodialysis: Slightly dialyzable (5% to 20%) Administer dose posthemodialysis: CAPD
effects: Unknown; CAVH effects: Unknown

precautions Monitoring Parameters CBC, platelet counts, total
bilirubin, alkaline phosphatase Dietary Considerations May be taken with food. Patient Information Take as prescribed (may take in
divided doses or with food if GI upset occurs). Rheumatoid arthritis: Response may not occur for up to 3 months; do not discontinue without consulting prescriber.
Organ transplant: Azathioprine will usually be prescribed with other antirejection medications.
Do not get pregnant while taking this medication; use appropriate contraceptive measures. Breast-feeding is not recommended.

Cyclophosphamide
Endoxan 50mg/tab; 200mg/vial

Indications Nononcologic: Prophylaxis of rejection for
kidney, heart, liver, and bone marrow transplants, severe rheumatoid disorders, nephrotic syndrome, Wegener's granulomatosis, idiopathic pulmonary hemosideroses, myasthenia gravis, multiple sclerosis, systemic lupus erythematosus, lupus nephritis, autoimmune hemolytic anemia, idiopathic thrombocytic purpura (ITP), macroglobulinemia, and antibody-induced pure red cell aplasia

Pregnancy Risk Factor D Precautions Dosage adjustment needed for
renal or hepatic failure; use with caution in patients with bone marrow suppression.
Cyclophosphamide preparation should be performed in a Class II laminar flow biologic safety cabinet. Personnel should be wearing surgical gloves and a closed front surgical gown with knit cuffs. Appropriate safety equipment is recommended for preparation, administration, and disposal of antineoplastics.
If cyclophosphamide contacts the skin, wash and flush thoroughly with water.

Adverse Reactions-1>10%: Dermatologic: Alopecia (40% to 60%) but hair
will usually regrow . Hair loss usually begins 3-6 weeks after the start of therapy.
Endocrine & metabolic: Fertility: May cause sterility; interferes with oogenesis and spermatogenesis; may be irreversible in some patients; gonadal suppression (amenorrhea)
GI: Nausea and vomiting occur more frequently with larger doses, usually beginning 6-10 hours after administration; anorexia, diarrhea, mucositis, and stomatitis are also seen

Adverse Reactions-2 GU: Severe, potentially fatal acute hemorrhagic
cystitis or urinary fibrosis, believed to be a result of chemical irritation of the bladder by acrolein, a cyclophosphamide metabolite, occurs in 7% to 12% of patients and has been reported in up to 40% of patients in some series. Patients should be encouraged to drink plenty of fluids (3-4 L/day) during therapy, void frequently, and avoid taking the drug at night. With large I.V. doses, I.V. hydration is usually recommended. The use of mesna and/or continuous bladder irrigation is rarely needed for doses <2 g/m2.

Adverse Reactions-3 Hematologic: Thrombocytopenia and
anemia are less common than leukopenia
Onset: 7 days Nadir: 10-14 days Recovery: 21 days

Overdosage/Toxicology Overdosage/Toxicology Symptoms
of overdose include myelosuppression, alopecia, nausea, and vomiting. Treatment is supportive.

Drug Interactions-1CYP2B6, 2D6, and 3A3/4 enzyme
substrate Decreased effect: Digoxin: Cyclophosphamide may decrease
digoxin serum levels Increased toxicity: Allopurinol may cause increase in bone
marrow depression and may result in significant elevations of cyclophosphamide cytotoxic metabolites

Drug Interactions-2 Increased toxicity: 1. Anesthetic agents: Cyclophosphamide
reduces serum pseudocholinesterase concentrations and may prolong the neuromuscular blocking activity of succinylcholine; use with caution with halothane, nitrous oxide, and succinylcholine
2. Chloramphenicol results in prolonged cyclophosphamide half-life to increase toxicity
3. Cimetidine inhibits hepatic metabolism of drugs and may decrease or increase the activation of cyclophosphamide

Drug Interactions-3 Increased toxicity: 1. Doxorubicin: Cyclophosphamide may
enhance cardiac toxicity of anthracyclines 2. Phenobarbital and phenytoin induce
hepatic enzymes and cause a more rapid production of cyclophosphamide metabolites with a concurrent decrease in the serum half-life of the parent compound
3. Thiazide diuretics: Leukopenia may be prolonged

Mechanism of Action Cyclophosphamide is an alkylating
agent that prevents cell division by cross-linking DNA strands and decreasing DNA synthesis. It is a cell cycle phase nonspecific agent. Cyclophosphamide also possesses potent immunosuppressive activity. Cyclophosphamide is a prodrug that must be metabolized to active metabolites in the liver.

Pharmacodynamics/Kinetics
Absorption: Oral: Well absorbed Distribution: Well; Vd: 0.48-0.71 L/kg; crosses
placenta; crosses into CSF (not high enough to treat meningeal leukemia)
Protein binding: 10% to 56% Metabolism: Hepatic into its active components:
acrolein, 4-aldophosphamide, 4-hydroperoxy- cyclophosphamide, and nor-nitrogen mustard
Bioavailability: >75%; Half-life elimination: 4-8 hours Time to peak, serum: Oral: ~1 hour Excretion: Urine (<30% as unchanged drug, 85% to
90% as metabolites)

Usual DosageChildren: SLE: I.V.: 500-750 mg/m2 every month;
maximum dose: 1 g/m2 JRA/vasculitis: I.V.: 10 mg/kg every 2
weeks Children and Adults: Oral: 50-100 mg/m2/day as continuous
therapy or 400-1000 mg/m2 in divided doses over 4-5 days as intermittent therapy

Usual DosageChildren and Adults: I.V.: Single Doses: 400-1800 mg/m2 (30-50 mg/kg)
per treatment course (1-5 days) which can be repeated at 2-4 week intervals
MAXIMUM SINGLE DOSE WITHOUT BMT is 7 g/m2(190 mg/kg) SINGLE AGENT THERAPY
Continuous daily doses: 60-120 mg/m2 (1-2.5 mg/kg) per day
Autologous BMT: IVPB: 50 mg/kg/dose x 4 days or 60 mg/kg/dose for 2 days; total dose is usually divided over 2-4 days
Nephrotic syndrome: Oral: 2-3 mg/kg/day every day for up to 12 weeks when corticosteroids are unsuccessful

Methotrexate
MTX 2.5mg/tab; 50mg/2ml; 20mg, 1gm/vial

INDICATIONS Use Treatment of trophoblastic
neoplasms; leukemias; psoriasis; rheumatoid arthritis (RA), including polyarticular-course juvenile rheumatoid arthritis (JRA); breast, head and neck, and lung carcinomas; osteosarcoma; sarcomas; carcinoma of gastric, esophagus, testes; lymphomas

Pregnancy Risk Factor D
Lactation Enters breast milk/contraindicated

Contraindications Contraindications Hypersensitivity to
methotrexate or any component of the formulation; severe renal or hepatic impairment; pre-existing profound bone marrow suppression in patients with psoriasis or rheumatoid arthritis, alcoholic liver disease, AIDS, pre-existing blood dyscrasias; pregnancy

Warnings/Precautions May cause photosensitivity type reaction Reduce dosage in patients with renal or
hepatic impairment, ascites, and pleural effusion.
Use with caution in patients with peptic ulcer disease, ulcerative colitis, or pre-existing bone marrow suppression.
Monitor closely for pulmonary disease; use with caution in the elderly..

Warnings/Precautions Methotrexate given concomitantly
with radiotherapy may increase the risk of soft tissue necrosis and osteonecrosis.
Safety and efficacy in pediatric patients have been established only in cancer chemotherapy and polyarticular-course JRA.

Warnings/Precautions Because of the possibility of severe toxic
reactions, fully inform patient of the risks involved.
May cause hepatotoxicity, fibrosis and cirrhosis, along with marked bone marrow depression.
Death from intestinal perforation may occur. Use caution when used with other hepatotoxic
agents (azathioprine, retinoids, sulfasalazine).

Warnings/Precautions Toxicity from methotrexate or any
immunosuppressive is increased in the elderly.Must monitor carefully.
For rheumatoid arthritis and psoriasis, immunosuppressive therapy should only be used when disease is active and less toxic; traditional therapy is ineffective.
Recommended doses should be reduced when initiating therapy in the elderly due to possible decreased metabolism, reduced renal function, and presence of interacting diseases and drugs.

Overdosage/Toxicology Hydration and alkalinization may be used to
prevent precipitation of MTX or MTX metabolites in the renal tubules.
Generally, neither peritoneal nor hemodialysis have been shown to increase elimination.
However, effective clearance of methotrexate has been reported with acute, intermittent hemodialysis using a high-flux dialyzer.
Leucovorin should be administered intravenously, never intrathecally, for overdoses of intrathecal methotrexate.

Drug Interactions -1
Decreased effect: Corticosteroids: Reported to
decrease uptake of MTX into leukemia cells. Administration of these drugs should be separated by 12 hours. Dexamethasone has been reported to not affect methotrexate influx into cells.
Decreases phenytoin, 5-FU activity

Drug Interactions-2
Increased toxicity: Live virus vaccines vaccinia
infections Vincristine: Inhibits MTX efflux from
the cell, leading to increased and prolonged MTX levels in the cell; the dose of VCR needed to produce this effect is not achieved clinically

Drug Interactions-3 Increased toxicity: Vincristine: Inhibits MTX efflux from the
cell, leading to increased and prolonged MTX levels in the cell; the dose of VCR needed to produce this effect is not achieved clinically
Organic acids: Salicylates, sulfonamides, probenecid, and high doses of penicillins compete with MTX for transport and reduce renal tubular secretion. Salicylates and sulfonamides may also displace MTX from plasma proteins, increased MTX levels

Drug Interactions-4 Increased toxicity: Ara-C: Increases formation of the
Ara-C nucleotide can occur when MTX precedes Ara-C, thus promoting the action of Ara-C
Cyclosporine: CSA and MTX interfere with each others renal elimination, which may result in increased toxicity

Drug Interactions-5 Increased toxicity: NSAIDs: Should not be used during
moderate or high-dose methotrexate due to increased and prolonged methotrexate levels (may increase toxicity); NSAID use during treatment of rheumatoid arthritis has not been fully explored, but continuation of prior regimen has been allowed in some circumstances, with cautious monitoring
Hepatotoxic agents (azathioprine, retinoids, sulfasalazine) may increase the risk of hepatotoxic reactions

Ethanol/Nutrition/Herb Interaction
Ethanol: Avoid ethanol (may be associated with increased liver injury).
Food: Methotrexate peak serum levels may be decreased if taken with food. Milk-rich foods may decrease MTX absorption. Folate may decrease drug response.
Herb/Nutraceutical: Avoid echinacea (has immunostimulant properties).

Mechanism of Action -1 An antimetabolite that inhibits DNA synthesis
and cell reproduction in malignant cells Cytotoxicity is determined by both drug
concentration and duration of cell exposure; extracellular drug concentrations of 1 x 10-8 M are required to inhibit thymidylate synthesis; reduced folates are able to rescue cells and reverse MTX toxicity if given within 40 hours of the MTX dose

Mechanism of Action-2 Folates must be in the reduced form (FH4) to
be active Folates are activated by dihydrofolate
reductase (DHFR) DHFR is inhibited by MTX (by binding
irreversibly), causing an increase in the intracellular dihydrofolate pool (the inactive cofactor) and inhibition of both purine and thymidylate synthesis (TS)

Pharmacodynamics/Kinetics-1
Onset of action: Antirheumatic: 3-6 weeks; additional improvement may continue longer than 12 weeks
Absorption: Oral: Rapid; well absorbed at low doses (<30 mg/m2), incomplete after large doses; I.M. injection: Complete

Pharmacodynamics/Kinetics-2
Distribution: Penetrates slowly into 3rd space fluids (eg, pleural effusions, ascites), exits slowly from these compartments (slower than from plasma); crosses placenta; small amounts enter breast milk; does not achieve therapeutic concentrations in CSF; must be given intrathecally if given for CNS prophylaxis or treatment; sustained concentrations retained in kidney and liver
Protein binding: 50%

Pharmacodynamics/Kinetics-3
Metabolism: <10%; degraded by intestinal flora to DAMPA by carboxypeptidase; hepatic aldehyde oxidase converts MTX to 7-OH MTX; polyglutamates are produced intracellularly and are just as potent as MTX; their production is dose and duration dependent and are slowly eliminated by the cell
Half-life elimination: Low dose: 3-10 hours; High dose: 8-12 hours
Time to peak, serum: Oral: 1-2 hours; Parenteral: 30-60 minutes
Excretion: Primarily urine (44% to 100%);

Usual Dosage(Children)-1
Dermatomyositis: Oral: 15-20 mg/m2/week as a single dose once weekly or 0.3-1 mg/kg/dose once weekly
Juvenile rheumatoid arthritis: Oral, I.M.: Recommended starting dose: 10 mg/m2 once weekly (at higher doses, gastrointestinal side effects may be decreased with I.M. administration); 5-15 mg/m2/week as a single dose or as 3 divided doses given 12 hours apart

Usual Dosage(Adults)-1
Rheumatoid arthritis: Oral: 7.5 mg once weekly OR 2.5 mg every 12 hours for 3 doses/week;
not to exceed 20 mg/week Bone marrow suppression is increased at
dosages >20 mg/week; absorption and GI effects may be improved with I.M. administration at higher end of dosage range

Usual Dosage(Adults)-2
Psoriasis: Oral: 2.5-5 mg/dose every 12 hours for 3 doses given weekly or Oral, I.M.: 10-25 mg/dose given once weekly
Ectopic pregnancy: I.M./I.V.: 50
mg/m2 single-dose without leucovorin rescue

Usual Dosage(Elderly)
Rheumatoid arthritis/psoriasis: Oral: Initial: 5 mg once weekly; if
nausea occurs, split dose to 2.5 mg every 12 hours for the day of administration; dose may be increased to 7.5 mg/week based on response, not to exceed 20 mg/week

Dosing adjustment in renal impairment
Clcr 61-80 mL/minute: Reduce dose to 75% of usual dose
Clcr 51-60 mL/minute: Reduce dose to 70% of usual dose
Clcr 10-50 mL/minute: Reduce dose to 30% to 50% of usual dose
Clcr<10 mL/minute: Avoid use

HD & PD Hemodialysis: Not dialyzable (0%
to 5%); supplemental dose is not necessary
Peritoneal dialysis: Supplemental dose is not necessary

Dosage adjustment in hepatic impairment:
Bilirubin 3.1-5 mg/dL or AST >180 units: Administer 75% of
usual dose
Bilirubin >5 mg/dL: Do not use

Methotrexate Dosing Schedules
Dose Route Frequency
Conventional
15-20 mg/m2P.O. Twice weekly
30-50 mg/m2P.O., I.V. Weekly
15 mg/day for 5 days P.O., I.M. Every 2-3 weeks
Intermediate
50-150 mg/m2I.V. push Every 2-3 weeks
240 mg/m2* I.V. infusion Every 4-7 days
0.5-1 g/m2* I.V. infusion Every 2-3 weeks
High
1-12 g/m2* I.V. infusion Every 1-3 weeks
*Followed with leucovorin rescue - refer to Leucovorin monograph for details.

Administration
Specific dosing schemes vary, but high dose should be followed by leucovorin calcium 24-36 hours after initiation of therapy to prevent toxicity
Renal toxicity can be minimized/prevented by alkalinizing the urine (with sodium bicarbonate) and increasing urine flow (hydration therapy)

Monitoring Parameters Monitoring Parameters For prolonged
use (especially rheumatoid arthritis, psoriasis) a baseline liver biopsy, repeated at each 1-1.5 g cumulative dose interval, should be performed; WBC and platelet counts every 4 weeks; CBC and creatinine, LFTs every 3-4 months; chest x-ray

Patient Information-1 Avoid alcohol to prevent serious side effects. Avoid intake of extra dietary folic acid,
maintain adequate hydration (2-3 L/day of fluids unless instructed to restrict fluid intake) and adequate nutrition (frequent small meals may help).
You may experience nausea and vomiting (small frequent meals may help or request antiemetic from prescriber); drowsiness, tingling, numbness, or blurred vision (avoid driving or engaging in tasks that require alertness until response to drug is known);

Patient Information-2 Mouth sores (frequent oral care is necessary); loss of hair; permanent sterility; skin rash;
photosensitivity (use sunscreen, wear protective clothing and eyewear, and avoid direct sunlight).
Report black or tarry stools, fever, chills, unusual bleeding or bruising, shortness of breath or difficulty breathing, yellowing of skin or eyes, dark or bloody urine, or acute joint pain or other side effects you may experience.

Pregnancy/breast-feeding precautions
Do not get pregnant while taking this medication; use appropriate barrier contraceptive measures. The drug may cause permanent sterility and may cause birth defects.
Do not breast-feed.

Sulfasalazine
SalicylazosulfapyridineDosage Forms Tablet: 500 mg Tablet, enteric coated: 500 mg

Use Management of ulcerative colitis; enteric coated tablets are also used for rheumatoid arthritis (including juvenile rheumatoid arthritis) in patients who inadequately respond to analgesics and NSAIDsUse - Unlabeled/Investigational Ankylosing spondylitis, collagenous colitis, Crohn's disease, psoriasis, psoriatic arthritis, juvenile chronic arthritisPregnancy Risk Factor B/D (at term)
USE

Pregnancy & Lactation Pregnancy Implications Sulfonamides are excreted
in human breast milk and may cause kernicterus in the newborn. Although sulfapyridine has poor bilirubin-displacing ability, use with caution in women who are breast-feeding.Lactation Enters breast milk/use caution (AAP recommends use "with caution")Contraindications Hypersensitivity to sulfasalazine, sulfa drugs, salicylates, or any component of the formulation; porphyria; GI or GU obstruction; children <2 years of age; pregnancy (at term)

Warnings/Precautions
Use with caution in patients with renal impairment; impaired hepatic function or urinary obstruction, blood dyscrasias, severe allergies or asthma, or G6PD deficiency; may cause folate deficiency (consider providing 1 mg/day folate supplement). Chemical similarities are present among sulfonamides, sulfonylureas, carbonic anhydrase inhibitors, thiazides, and loop diuretics (except ethacrynic acid). Use in patients with sulfonamide allergy is specifically contraindicated in product labeling,

Adverse Reactions>10%: Central nervous system: Headache (33%) Dermatologic: Photosensitivity Gastrointestinal: Anorexia, nausea, vomiting,
diarrhea (33%), gastric distress Genitourinary: Reversible oligospermia (33%) <3%: Dermatologic: Urticaria/pruritus (<3%) Hematologic: Hemolytic anemia (<3%), Heinz
body anemia (<3%)

Mechanism of Action
Acts locally in the colon to decrease the inflammatory response and systemically interferes with secretion by inhibiting prostaglandin synthesis

Drug Interactions-1Azathioprine, mercaptopurine, sulfasalazine: May
increase the risk of myelosuppression (due to TPMT inhibition).
Cyclosporine concentrations may be decreased; monitor levels and renal function
Digoxin's absorption may be decreased Folic acid's absorption may be decreased
Hypoglycemics: Increased effect of oral hypoglycemics (rare, but severe); monitor blood sugar

Drug Interactions-2
Methotrexate-induced bone marrow suppression may be increased
NSAIDs and salicylates: May increase sulfonamide concentrations
Thiazide diuretics: May increase the incidence of thrombocytopenia purpura
Warfarin and other oral anticoagulants: Anticoagulant effect may be increased; decrease dose and monitor INR closely

Pharmacodynamics/Kinetics Absorption: 10% to 15% as unchanged drug from small
intestine Distribution: Small amounts enter feces and breast milk
Metabolism: Via colonic intestinal flora to sulfapyridine and 5-aminosalicylic acid (5-ASA); following absorption, sulfapyridine undergoes N-acetylation and ring hydroxylation while 5-ASA undergoes N-acetylation
Half-life elimination: 5.7-10 hours Excretion: Primarily urine (as unchanged drug,
components, and acetylated metabolites)

Dosage Oral-1 Children 6 years: Juvenile rheumatoid arthritis:
30-50 mg/kg/day in 2 divided doses; Initial: Begin with 1/4 to 1/3 of expected maintenance dose; increase weekly; maximum: 2 g/day typically

Dosage Oral-2 Adults: Enteric coated tablet: Ulcerative colitis: Initial: 1 g 3-4 times/day,
2 g/day maintenance in divided doses; may initiate therapy with 0.5-1 g/day
Rheumatoid arthritis: Initial: 0.5-1 g/day; increase weekly to maintenance dose of 2 g/day in 2 divided doses; maximum: 3 g/day (if response to 2 g/day is inadequate after 12 weeks of treatment)

Dosing interval in renal impairment
Clcr 10-30 mL/minute: Administer twice daily
Clcr<10 mL/minute: Administer once daily
Dosing adjustment in hepatic impairment: Avoid use

Administration
GI intolerance is common during the first few days of therapy (administer with meals).Dietary Considerations Since sulfasalazine impairs folate absorption, consider providing 1 mg/day folate supplement.

Patient Information-1 Do not crush, chew, or dissolve coated tablets. Do not take on an empty stomach or with
antacids. Maintain adequate hydration (2-3 L/day of
fluids unless instructed to restrict fluid intake) to prevent kidney damage.
Increased dietary iron may be recommended. You may experience nervousness or dizziness (use caution when driving or engaging in hazardous activities until response to drug is known).

Patient Information-2 You may experience photosensitivity (use
sunscreen, wear protective clothing and eyewear, and avoid direct sunlight). Orange-yellow color of urine, sweat, tears is normal and will stain contact lenses and clothing. Report rash, persistent nausea or anorexia, or lack of improvement in symptoms (after 1-2 months). Pregnancy/breast-feeding precautions: Inform prescriber

Hydroxychloroquine
Dosage Forms Tablet, as sulfate: 200 mg [base 155
mg]Plaquenil®

USE Use Suppression and treatment of acute attacks of
malaria; treatment of systemic lupus erythematosus and rheumatoid arthritisUse - Unlabeled/Investigational Porphyria cutanea tarda, polymorphous light eruptionsPregnancy Risk Factor CLactation Enters breast milk/compatibleContraindications Hypersensitivity to hydroxychloroquine, 4-aminoquinoline derivatives, or any component of the formulation; retinal or visual field changes attributable to 4-aminoquinolines

Warnings/Precautions
Use with caution in patients with hepatic disease, G6PD deficiency, psoriasis, and porphyria; long-term use in children is not recommended; perform baseline and periodic (6 months) ophthalmologic examinations; test periodically for muscle weakness

Adverse Reactions-1CNS: Irritability, nervousness, emotional changes,
nightmares, psychosis, headache, dizziness, vertigo, seizures, ataxia, lassitude
Derm: Bleaching of hair, alopecia, pigmentation changes (skin and mucosal; black-blue color), rash
Endocrine and metabolic: Weight loss GI: Anorexia, nausea, vomiting, diarrhea, cramping Hematologic: Aplastic anemia, agranulocytosis,
leukopenia, thrombocytopenia, hemolysis (in patients with glucose-6-phosphate deficiency)

Adverse Reactions-2 Ocular: Disturbance in accommodation,
keratopathy, corneal changes/deposits (visual disturbances, blurred vision, photophobia - reversible on discontinuation), macular edema, atrophy, abnormal pigmentation, retinopathy (early changes reversible - may progress despite discontinuation if advanced), optic disc pallor/atrophy, attenuation of retinal arterioles, pigmentary retinopathy, scotoma, decreased visual acuity, nystagmus
Otic: Tinnitus, deafness

Overdosage/Toxicology
Symptoms of overdose include headache, drowsiness, visual changes, cardiovascular collapse, and seizures followed by respiratory and cardiac arrest. Treatment is symptomatic. Urinary alkalinization will enhance renal elimination.

Drug Interactions Chloroquine and other 4-aminoquinolones
may be decreased due to GI binding with kaolin or magnesium trisilicate
Increased effect: Cimetidine increases levels of chloroquine and probably other 4-aminoquinolones
Ethanol/Nutrition/Herb Interactions Ethanol: Avoid ethanol (due to GI irritation).

Mechanism of Action
Interferes with digestive vacuole function within sensitive malarial parasites by increasing the pH and interfering with lysosomal degradation of hemoglobin; inhibits locomotion of neutrophils and chemotaxis of eosinophils; impairs complement-dependent antigen-antibody reactions

Pharmacodynamics/Kinetics Onset of action: Rheumatic disease: May require
4-6 weeks to respond Absorption: Complete Protein binding: 55% Metabolism: Hepatic Half-life elimination: 32-50 days Time to peak: Rheumatic disease: Several months Excretion: Urine (as metabolites and unchanged
drug); may be enhanced by urinary acidification

DOSE Dosage Note: Hydroxychloroquine
sulfate 200 mg is equivalent to 155 mg hydroxychloroquine base and 250 mg chloroquine phosphate.
Oral: Children: JRA or SLE: 3-5 mg/kg/day divided 1-2
times/day;avoid exceeding 7 mg/kg/day

DOSE-2Adults: Rheumatoid arthritis: 310-465 mg/day to
start taken with food or milk; increase dose until optimum response level is reached; usually after 4-12 weeks dose should be reduced by 1/2 and a maintenance dose of 155-310 mg/day given
Lupus erythematosus: 310 mg every day or twice daily for several weeks depending on response; 155-310 mg/day for prolonged maintenance therapy

PRECAUTIONS Administration Administer with food or
milkMonitoring Parameters Ophthalmologic exam, CBCDietary Considerations May be taken with food or milk.

Patient Information-1 It is important to complete full course of
therapy which may take up to 6 months for full effect.
May be taken with meals to decrease GI upset and bitter aftertaste. Avoid alcohol.
You should have regular ophthalmic exams (every 4-6 months) if using this medication over extended periods.

Patient Information-2 You may experience dizziness, headache,
nervousness, or lightheadedness (use caution when driving or engaging in tasks requiring alertness until response to drug is known);
Increased sensitivity to sunlight Report vision changes, rash or itching,
persistent diarrhea or GI disturbances, change in hearing acuity or ringing in the ears, chest pain or palpitation, CNS changes, unusual fatigue, easy bruising or bleeding, or any other persistent adverse reactions.

Penicillamine
Dosage Forms Capsule: 125 mg, 250 mg Tablet: 250 mg

USE Use Treatment of Wilson's disease, cystinuria,
adjunct in the treatment of rheumatoid arthritis; lead, mercury, copper, and possibly gold poisoning. (Note: Oral DMSA is preferable for lead or mercury poisoning); primary biliary cirrhosis; as adjunctive therapy following initial treatment with calcium EDTA or BALPregnancy Risk Factor DLactation Enters breast milk/contraindicated

ContraindicationsHypersensitivity to penicillamine or any
component of the formulation; renal insufficiency; patients with previous penicillamine-related aplastic anemia or agranulocytosis; concomitant administration with other hematopoietic-depressant drugs
(eg, gold, immunosuppressants, antimalarials, phenylbutazone); pregnancy

Warnings/Precautions Cross-sensitivity with penicillin is possible;
therefore, should be used cautiously in patients with a history of penicillin allergy.
patients should be warned to report promptly any symptoms suggesting toxicity; approximately 33% of patients will experience an allergic reaction; since toxicity may be dose related, it is recommended not to exceed 750 mg/day in elderly.

Adverse Reactions-1 >10%: Dermatologic: Rash, urticaria, itching (44% to
50%) GI: Hypogeusia (25% to 33%) Neuromuscular & skeletal: Arthralgia 1% to 10%: CV: Edema of the face, feet, or lower legs CNS: nervous system: Fever, chills GI: Weight gain, sore throat GU: Bloody or cloudy urine Hema: Aplastic or hemolytic anemia, leukopenia
(2%), thrombocytopenia (4%)

Drug Interactions Decreased effect with iron and zinc salts, antacids
(magnesium, calcium, aluminum) & food Decreased effect/levels of digoxin Increased effect of gold, antimalarials,
immunosuppressants, phenylbutazone (hematologic, renal toxicity)
Ethanol/Nutrition/Herb Interactions Ethanol: Avoid or limit ethanol.
Food: Penicillamine serum levels may be decreased if taken with food. Do not administer with milk. Iron and zinc may decrease drug action.

Mechanism of Action Chelates with lead, copper, mercury and
other heavy metals to form stable, soluble complexes that are excreted in urine; depresses circulating IgM rheumatoid factor, depresses T-cell but not B-cell activity; combines with cystine to form a compound which is more soluble, thus cystine calculi are prevented

Pharmacodynamics/Kinetics
Absorption: 40% to 70% Metabolism: Hepatic, small amounts Protein binding: 80% to albumin Half-life elimination: 1.7-3.2 hours Time to peak, serum: ~2 hours Excretion: Primarily urine (30% to
60% as unchanged drug)

DOSE Dosage Oral: Rheumatoid arthritis: Children: Initial: 3 mg/kg/day ( 250
mg/day) for 3 months, then 6 mg/kg/day ( 500 mg/day) in divided doses twice daily for 3 months to a maximum of 10 mg/kg/day in 3-4 divided doses
Adults: 125-250 mg/day, may increase dose at 1- to 3-month intervals up to 1-1.5 g/day

ADMINISTRATION Dosing adjustment/comments in
renal impairment: Clcr<50 mL/minute: Avoid use
Administration Administer on an empty stomach (1 hour before meals and at bedtime). Patients unable to swallow capsules may mix contents of capsule with fruit juice or chilled pureed fruit.

Monitoring Parameters Urinalysis, CBC with differential, platelet count,
liver function tests; weekly measurements of urinary and blood concentration of the intoxicating metal is indicated (3 months has been tolerated)
CBC: WBC <3500/mm3, neutrophils <2000/mm3 or monocytes >500/mm3 indicate need to stop therapy immediately; quantitative 24-hour urine protein at 1- to 2-week intervals initially (first 2-3 months); urinalysis, LFTs occasionally; platelet counts <100,000/mm3 indicate need to stop therapy until numbers of platelets increase

Dietary Considerations Dietary Considerations Should be taken at
least 1 hour before a meal on an empty stomach. Iron and zinc may decrease drug action; increase dietary intake of pyridoxine. For Wilson's disease, decrease copper in diet and omit chocolate, nuts, shellfish, mushrooms, liver, raisins, broccoli, and molasses.
For lead poisoning, decrease calcium in diet.

Patient Information-1 Take this medication exactly as directed;; do not
take with milk or milk products. Avoid or limit alcohol and excess intake of vitamin A.
It is preferable to take penicillamine on empty stomach (1 hour before or 2 hours after meals). Maintain adequate hydration (2-3 L/day of fluids unless instructed to restrict fluid intake).
Wilson's disease: Avoid chocolate, shellfish, nuts, mushrooms, liver, broccoli, molasses.
Lead poisoning: Decrease dietary calcium.

Patient Information-2 Cystinuria: Take with large
amounts of water. Pregnancy/breast-feeding
precautions: Do not get pregnant while taking this medication; use appropriate contraceptives. Do not breast-feed.

CyCLOSPORINE
Neoral cap 50mg; 100mg/capSolution 100mg/ml;50ml/bot
INJ 50mg/ml/amp

Pharmacology
Selectively and reversibly inhibits
T-lymphocyte activation without
causing myelosuppression
Blocks interleukin-2 (T-cell growth
factor) production

Cyclosporine Cyclosporin A, Sandimmune, CsA, CyA
History Approved by FDA in 1983 Chemistry
- Fungal metabolite
- Cyclic Polypeptide (11 amino acids) with
a high MW
- Neutral and hydrophobic (nonpolar) product

Pharmacokinetics Absorption : slow, variable and incomplete (30%), peak conc. at 2-4 hrs ↑ abs. with time, ↓ abs. from T-tube Distribution : widely distributed throughout the body primarily in liver, pancreas, and lung highly protein bound (mainly RBC) not dialyzed

Pharmacokinetics
Metabolism : extensively metabolized by the liver
(cytochrome p-450 enzyme)
Elimination :
primarily excreted via biliary

Dosage & Administration
Oral --- 5 ~ 18 mg/kg/day initially in 1-2 doses, mix with chocolate milk or fruit juice in a glass container
I.V. --- 2 ~ 6 mg/kg/day over 2-6 hrs infusion IV dose = 1/3 oral dose dilute 50mg CsA in 20-100ml 0.9% NaCl or 5%
D/W use glass container only use NTG IV set

Parameters to Monitor
CsA trough level --- 100 ~ 200 ng/ml (whole blood, TDx)
Renal function --- I/O, BUN / Cr Hepatic Function --- LFTs, Bilirubin

UseProphylaxis of organ rejection in kidney,
liver, and heart transplants, has been used with azathioprine and/or corticosteroids; severe, active rheumatoid arthritis (RA) not responsive to methotrexate alone; severe, recalcitrant plaque psoriasis in nonimmunocompromised adults unresponsive to or unable to tolerate other systemic therapy

Use Unlabeled/Investigational Short-term, high-dose
cyclosporine as a modulator of multidrug resistance in cancer treatment; allogenic bone marrow transplants for prevention and treatment of graft-versus-host disease; also used in some cases of severe autoimmune disease (ie, SLE, myasthenia gravis) that are resistant to corticosteroids and other therapy; focal segmental glomerulosclerosis
Pregnancy Risk Factor C

ContraindicationsHypersensitivity to cyclosporine or any
component of the formulation. Rheumatoid arthritis and psoriasis: Abnormal renal function, uncontrolled hypertension, malignancies. Concomitant treatment with PUVA or UVB therapy, methotrexate, other immunosuppressive agents, coal tar, or radiation therapy are also contraindications for use in patients with psoriasis.

Warnings/Precautions
Dose-related risk of nephrotoxicity and hepatotoxicity; monitor renal function and adjust dose appropriately.
Use caution with other potentially nephrotoxic drugs (eg, acyclovir, aminoglycoside antibiotics, amphotericin B, ciprofloxacin).
Increased risk of lymphomas, other malignancies, infection. May cause hypertension.

Warnings/Precautions
Psoriasis: Patients should avoid excessive sun exposure; safety and efficacy in children <18 have not been established
Rheumatoid arthritis: Safety and efficacy for use in juvenile rheumatoid arthritis have not been established

Side Effects
Nephrotoxicity # Hypertention * # Neurologic changes* (tremor, numbness) Hirsutism* Gum hyperplasia* Electrolyte disturbance (↑K,↓Mg,↑uric acid )
Infection
(bacteria, viral, fungal) Hepatoxicity* Convulsions Thrombocytopenia & hemolytic anemia Lymphoma*
Note: * dose-dependent
# difficult to differentiate CsA toxicity from renal rejection)

Efficacy Comparison







ENBREL 恩博 (etanercept) Dimeric fusion protein
Human p75, Soluble, extracellular domain of tumor necrosis factor-α (TNFα) linked to Fc portion of IgG1
934 amino acid Molecular weight: 150 kD Recombinant DNA technology Produced by Chinese Hamster Ovary (CHO) cell line Pharmacotherapeutic group: selective
immunosuppressant agent New Generation of Biotechnology Agents-
Biological Response Modifier (BRM)





ENBREL Pharmacokinetics
Pharmacokinetics C max :48 hours
Bioavailability :76%
Vd: 7.6 l
Half-life: 70 hours
Clearance: 0.066 l/hr
No difference between men and women
MTX has no effect on the pharmacokinetics of Enbrel
No increase concentration of Enbrel in renal and hepatic impairment

ENBREL Usage
Dose Adult (18-64 y/o): 25mg, sc, twice weekly
Child (4-17): 0.4mg/kg, sc, twice weekly
No dose adjustment for elderly patients ( 65y/o), renal and hepatic ≧impairment
Notes No special routine examination
Major adverse effects: inject site reaction
Stop ENBREL when Infection

ENBREL (etanercept) 恩博ENBREL的療效對病人的利益 可恢復患者日常生活能力 實現患者的願望 保存患者關節的功能

ENBREL (etanercept) 恩博ENBREL的使用方式 成人 :25mg 皮下注射 ,一星期二次 小孩 :0.4mg/kg,皮下注射 ,一星期二次 不需特殊的實驗室檢查 適應症 :
類風濕性關節炎 幼年型類風濕關節炎 牛皮癬關節炎

ARHEUMA 雅努麻 ®
(Leflunomide)ARHEUMA 雅努麻 ®
(Leflunomide)
Immuno-modulatorDMARD for Rheumatoid
Arthritis
LOTUS Pharm.Co. Ltd.

ArheumaTM
20mg/Tab. 適應症 :治療成人類風濕性關節炎,並減緩於 X 光所顯現之關節磨損與關節間隙狹窄等結構性損害。

Outlines Mechanism of Arheuma Pharmacokinetics Contraindications Warning Precautions Drug Interactions Side Effects Dosage and Administration

Mechanism of Arheuma Inhibiting the amplification of T, B
cell Anti-inflammatory effects
Reducing the production of PGE2 Increasing the producing of IL-1
receptor antagonist in human synovial fibroblasts and articular chondrocytes
Suppressing the activation of NFkB


Pharmacokinetics I Major active metabolite: A77 1726 (M1) Absorption :
No food interaction BA : 80% Peak level of M1 : 6-12 hours after dosing
Distribution : Low Vd : (Vss=0.13 L/kg) Extensively bound (>99.3%) to albumin Linear pharmacokinetics
ARAVATM Prescribing Information US, 1998.

Pharmacokinetics II Metabolism : M1 Elimination
Excretion of radiolabeled A77 1726: approximately 43% in urine, 48% in feces
Clearance : 31 mL/hr T 1/2 : 2 weeks (biliary recycling) Accelerate elimination with:
cholestyramine activated charcoal

Pharmacokinetics III Special populations
Smoking : have a 38% increase in clearance Chronic Renal Insufficiency
M1 is not dialyzable (CAPD or hemodialysis) Free fraction of M1 are almost doubled Caution
Hepatic Insufficiency : is not recommended 輕度腎臟功能不全之病患不需要調整劑量。 65 歲以上之病患不需要調整劑量。
Weber & Harnisch 1998 Rheumatol Eur 27(Suppl 2):110.

Contraindication
Hypersensitivity to leflunomide or any other components of Arheuma
Women who are or may become pregnant

Immunosuppression potential/ Bone marrow supression
Hepatotoxicity Pre-existing hepatic disease
Significant hepatic impairment or evidence of infection with hepatitis B or C
Skin reactions Malignancy
Warnings

Precautions Need for Drug Elimination Laboratory Tests :
Hematologic Monitoring (WBC, Hb, platelet) Liver Enzyme Monitoring (AST,ALT,Serium
albumin) 服藥前及用藥後的前六個月, 每隔四週測,之後每隔 6-8 週監測
Pregnancy : X Nursing Mothers (excreting to human
milkunknown) 治療期間使用有效避孕方式 , 只要活性代謝物 M1 之血漿濃度高於
0.02mg/l 不可懷孕 男性病患應注意:
可能有男性引起的胎兒毒性,服藥期間應使用有效的避孕方法。

Drug Interactions Warfarin did not affect M1 protein
binding M1 會取代 ibuprofen 、 diclofenac 與的
protein binding 。這些藥物游離態的部分僅增加 13% 至 50% ,但不具有臨床意義
M1 inhibits CYP 450 2C9, which is responsible for the metabolism of phenytoin, tobutamide, warfarin, NSAIDs
Rifampin : M1 peak levels increases(~40%)

如何預防類風濕關節炎 類風濕關節炎是一種以關節炎症為主的全
身性的疾病,好發的對象以女性多於男性、成人多於兒童,雖然目前確實的病因不明,不過,預防勝於治療,平常就應該具備預防類風濕關節炎的概念。
(一)常常運動、鍛鍊體魄:例如早上起床後能做做體操、練氣功、打太極拳或散步;因為有運動就能增強抵抗力,日常生活裏也就較不易生病。

如何預防類風濕關節炎 (二)避免受到風寒、防止潮濕環境:盡可能
要受涼、淋雨或受潮,例如不要穿已濕的衣服、鞋子或襪子,不要住太過潮濕的地方,不要暴飲冰水等等。
(三)避免過度疲勞:除了飲食有節之外,應當盡量讓自己不要太過勞累,使身體產生疾病,懂得適度的工作和休閒。

如何預防類風濕關節炎 ( 四 ) 保持心情的愉悅:有時候類風濕關節炎
的患者是因心理上或精神上受到刺激、過度悲傷才罹患此症的,所以懂得調節自己的心情是很重要的。
(五 )預防和控制感染:在病歷上像患有扁桃腺炎、鼻竇炎或是齲齒等感染後,也會有類風濕關節炎,所以應預防受到一些疾病感染,並早期治癒。

Algorithm for the aggressive treatment of rheumatoid at an early stage
ACTIVE DISEASE
EARLY DISEASELATE DISEASE
LOCALISED
SynovectomyIntra-articularJoint surgeryj
GENERALISEDGOOD PROGNOSIS
Hydroxychloroquine Sulfasalazine
PARTIAL RESPONSE orLOSS OF EFFICACY
Add other agents toExisting drug therapy
NO RESPONSETO THERAPY
Age < 65 Age > 65
Methotrexate or IM gold
RESPONSE TO THERAPY
Maintenance therapy with IM gold
Oral corticosteroid (low dose)
NO RESPONSE TO THERAPY
CyclosporinAzathioprineExerimental therapies
POOR PROGNOSIS
Pulse corticosteroid therapy
Pulse corticosteroid therapy