Embed Size (px)
Citation preview

8/16/18
1
Chronic Venous Insufficiency
Kimberly Giberga MSN APRN FNP-C RPhS2018
Financial Disclosure
� Unfortunately, I have no financial obligations to disclose.
Objectives
• Describe Venous Anatomy• Describe the pathophysiology of Venous Disease• Describe symptoms and physical exam findings
associated with chronic venous insufficiency• Discuss complications associated with Chronic
Venous Insufficiency• The provider will learn to differentiate arterial vs
venous symptoms of vascular disease• Discuss diagnostic tests used to diagnose venous
disease• The provider will learn different therapies used to
treat vein disease.
Case Study
� 44 yo female presents complaining of leg fatigue and aching at end of 12+ hour shifts.
� PT complains of ‘charley horse’ style cramping always in right medial calf that wakes her from sleep.
� Often massages legs at night to relieve fatigue enough to sleep.
� Daily pain 5-6/10.� Denies edema, all labs WNL, + 30lbs overweight,
+hx of asthma controlled through inhalers, mild htncontrolled trough compliant medication use.
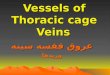
Prevalence
0
5
10
15
20
25
Vein D
isease
Coronary Hea
rt…PAD
CHFStro
ke
Cardiac A
rrythmias
millions
Risk Factors
• Heredity• Woman• Multiple Pregnancies• Careers with prolonged standing or prolonged
sitting• Age• Obesity• Height• Smaller risk factors: Chemotherapy, surgical
changes, injury

8/16/18
2
Venous Anatomy
� Deep veins include the iliac, tibial, femoral and popliteal veins.
� These veins are either intermuscular or intramuscular in the legs
� Superficial veins include the Great Saphenous and Small Saphenous veins and Accessory Veins
� Superficial to the deep muscular fascia
Deep Veins
The Muscle Pump
Venous Valves
• Typically bicuspid• Throughout the veins up to every 2 cm, more in
areas of higher pressure, • Have 2 main jobs:
• Maintain normal venous pressure 20-30mm Hg, even through changes in venous pressure from muscular contraction,
• Prevent retrograde flow

8/16/18
3
Pathophysiology of Venous Disease
ValvularDysfunction Venous Reflux Venous
hypertension
Changes in enzyme and
collagen expression by
vein cell
Variations in vein wall thickness
decrease in muscle in vein
wall
Venous dilation abnormal vascular
permeability and edema.
InflammationLipodermatosclerosis
Venous ulcersHyperpigmantation
Symptoms of Venous Insufficiency
• Heaviness• Swelling• Pain with prolonged standing or sitting• Need to elevate the legs through the day or stop and
rest the legs• Leg Fatigue• Itching• Burning• Sores• Weeping blisters• Cramping• Bulging Veins• Restless Legs
Physical Exam Findings
• Peripheral Edema• Lymphedema• Stasis Dermatitis• Erythema• Induration• Superficial
Thrombophlebitis• Hyperpigmentation• Venous Ulcers• Excoriation• Vesicles• Corona Phlebectasia• Telangectasia• Varicosities• Venous Eczema• Atrophie Blanche• Lipodermatosclerosis
• May be no Findings
Complications of Venous Insufficiency
� Ulcers� Lipodermatosclerosis� Lymphedema
Physical Exam Findings
Lipodermatosclerosis (note inverted champagne bottle shape)
Hyperpigmentation (middle) and Venous ulcer (above) Venous Ulcers (left) Venous eczema, lipodermatosclerosis
(center) Atrophie Blanche with Corona Phlebectasia (right)

8/16/18
4
Stasis Dermatitis (both images)
Lymphedema
Stemmer’s Sign
� Stemmer's sign is a thickened fold of skin at the base of the second toe or second finger that can be gently pinched and lifted. The presence of this sign is most often an early diagnostic indication of primary lymphedema; however, it can also develop later in secondary lymphedema.
Vein Disease Scoring
• Most Common is CEAP scoring but other scoring systems show how this impacts patients daily life.
Diagnostic Tests
• Venous ultrasound is gold standard• This is different from a DVT rule out• Most vein centers want to do their own• A good reflux study should include
• DVT rule out• Size and reflux of superficial veins including
accessories• Size of visible perforator veins• Size and reflux associated with varicosities
• Studies can be limited by • body habitus, acute DVT’s, and
Lipodermatosclerosis

8/16/18
5
Treatment
• Conservative therapy• Elevation• Compression socks• Exercise
• Pharmacologic Therapy• Surgical Treatment• Treatment may include ablation of the Saphenous
Veins and perforator veins related to ulcers• Ultrasound Guided Sclerotherapy• Phlebectomy• Insurance
Compression Therapy
• 2 types• Sequential Compression Devices• Compression socks 20-30mmHg /30-40mm Hg graded
Sequential Compression Devices
• Many insurance Companies cover this for peripheral lymphedema.
• Used daily.• Gives patient control.• Caution in your neuropathy, diabetic ulcer
patients.• 18-25mmHg For Diabetic patients with
neuropathy or mixed PVD
Compression Socks or Wraps
¡ Should be worn during the day only• Strong Cautions for people with mixed arterial/venous
disease• 80% of lower extremity ulcers are venous but you need to be
sure.• ABI 0.9-0.6 sufficient for compression therapy with
precautions.• Caution in your neuropathy, diabetic ulcer patients.• 18-25mmHg For Diabetic patients with neuropathy or mixed
PVD• 60-70% Noncompliance with compression therapy
• Measure and fit patient
Pharmacologic Therapy
• Not the mainstay of treatment in the US• Diuretics should not be used to treat peripheral edema
caused by venous insufficiency unless CHF or renal failure present.
• Pentoxifylline 800mg tid –effective for improved healing of ulcers metanalysis
• Escin (horse chestnut seed extract) — Horse chestnut seed extract (HCE) at a dose of 300 mg (standardized to 50 mg of escin [aescin], the active compound) BID similar reduction in symptoms and edema as wearing compression stockings
• Other medications with very small studies:• ASA 300mg QD, Stanozolol, Prostacyclin analogues, etc.
• Other medications not avilable in the US: • Micronized Purified Flovonoid Faction: mix of Diosmin
and hesperidin,• Hydroxyethylrutoside
When to refer
• Most vein centers want to see the patient sooner rather than later!
• Hyperpigmentation, ulcers, lipodermatosclerosis, venous eczema, stasis dermatitis, atrophie blanche and any inflammatory changes all are considered severe classifications of venous disease and should all be referred –If you can see signs of vein disease you should refer it out.
• Bleeding varicosities• Lack of response to conservative therapy• If you are considering a venous reflux study –send
it out.

8/16/18
6
Treatment
� 1. Conservative Therapy� 2. Ablation of superficial veins� 3. Ablation of perforator veins� 4. Sclerotherapy� 5. Microphlebectomy
Conservative Therapy
� NSAID’s, Elevation, Compression� May be an insurance requirement to be completed
under treating provider� Patients with Disease of hands/back may have
trouble with donning/removing compression� Alternative Velcro wraps � Sequential Compression Device
Ablations
� Ablations of the Saphenous veins� Radiofrequency or Laser� Goal is to shut down the vein permanently� Outpatient procedure followed by ultrasound� Local anesthesia sufficient� No down time� Complications DVT, EHIT
Ablation of Perforators
� Perforator Veins ‘perforate’ the muscle to connect deep veins to superficial veins.
� Refluxing perforators are often the cause of localized pain, varicosities and ulcerations.
� Local anesthesia� No Down time� 50% Success rate standard� Repeat us for follow-up� Risk DVT, failure to ablate
Sclerotherapy
� Injection of foam sclerosant into vein.� Local or no anesthesia� Outpatient� Risks non-closure, DVT, closing non-pathologic
veins
Phlebectomy
� Again, outpatient. Local anesthesia.� Suitable for large superficial varicosities.� Usually done after ablations.� Small superficial incisions in skin.� No down time to 1-2 days downtime or more
depending on procedure itself and person’s lifestyle.� Risk surgical scarring, segments left may develop
phlebitis.

8/16/18
7
Venous Disease Arterial Disease
� Increased gradual pain at the end of the day.
� Pain may get worse with rest
� Relief with leg elevation� Medial ankle ulcers� No change in pulses� No change in capillary
refill� Hemosiderin Staining
� Intermittent claudication� Pain subsides with rest� Relief with a dependent
limb� Toe Ulcers most common� Decreased pedal pulses� Decreased capillary refill� Pallor with elevation,
dusky in dependent position
Reviewing Arterial vs. Venous disease Case Study
� 60 yo female presents with left lateral leg ulcer x 9 months, followed by wound care, hyperbaric use ulcer has improved and worsened, but not healed.
� Pt was previously treated for chronic venous insufficiency.
� US shows duplicate GSV with reflux and abnormal perforator veins behind ulcerations.
Case Study Continued
� PT was treated, both duplicate GSV and perforator veins were ablated.
� At 1 month follow-up pt ulcer had almost healed.� 3 months later pts ulcer had healed and she had lost
40lbs.
Case Study
� 44 yo female presents complaining of leg fatigue and aching at end of 12+ hour shifts.
� PT complains of ‘charley horse’ style cramping always in right medial calf that wakes her from sleep.
� Often massages legs at night to relieve fatigue enough to sleep.
� Daily pain 5-6/10.� Denies edema, all labs WNL, + 30lbs overweight, +hx
of asthma controlled through inhalers, mild htncontrolled through compliant medication use.
Case Study Cont.
� Physical exam normal few telangiectasias, few corona phlebectactica right perimalleollar area.
� Fingerpoint are of tenderness right medial leg� Reflux study shows abnormal perforator vein located
under area of tenderness, >1.0s reflux in Great Saphenous vein below knee
Case Study Cont.
� Conservative therapy trial.� 6 weeks pt reports no ‘charley horse’ type cramping
in legs, decreased leg fatigue.� PT does not want to continue wearing compression
socks.� Ablation is done on the R Great Saphenous Vein,
perforator is shut down. � 2 years since, no muscle cramps in the right leg.
Daily pain resolved. Mild leg fatigue at end of day occasionally.

8/16/18
8
Thank you! Resources
• Compression Socks: • www.Juzo usa.com• Cep socks: www.cepcompression.com
• American College of Phlebology: www.phlebology.com
• Kim Giberga MSN APRN FNP-C RPhS• [email protected]
Works CitedAlguire, P. C., & Scovell, S. (n.d.). Overview and Management of chronic venous insufficiency. Retrieved August 02, 2016, from https://www.uptodate.com/contents/overview-and-management-of-lower-extremity-chronic-venous-disease?source=machineLearning&search=venous insufficiency prevalence&selectedTitle=1~150§ionRank=1&anchor=H2#H2
Bergan, J. J., Schmid-Schönbein, G. W., Smith, P. D., Nicolaides, A. N., Boisseau, M. R., & Eklof, B. (2006). Chronic Venous Disease. New England Journal of Medicine N Engl J Med, 355(5), 488-498. doi:10.1056/nejmra055289
Home. (2013). Retrieved August 02, 2016, from https://nationaleczema.org/
Jacob, M., Badier-Commander, C., Fontaine, V., Benazzoug, Y., Feldman, L., & Michel, J. (2001). Extracellular matrix remodeling in the vascular wall. Pathologie Biologie, 49(4), 326-332. doi:10.1016/s0369-8114(01)00151-1
Johns Hopkins Medicine, based in Baltimore, Maryland. (n.d.). Retrieved August 02, 2016, from
Works Cited Cont.
Sansilvestri-Morel, P., Rupin, A., Badier-Commander, C., Kern, P., Fabiani, J., Verbeuren, T. J., & Vanhoutte, P. M. (2001). Imbalance in the Synthesis of Collagen Type I and Collagen Type III in Smooth Muscle Cells Derived from Human Varicose Veins. J Vasc Res Journal of Vascular Research, 38(6), 560-568. doi:10.1159/000051092
Santiforestmonastery.Com Human Anatomy Pictures. (n.d.). Retrieved August 02, 2016, from http://www.santiforestmonastery.com/
Travers, J., Brookes, C., Evans, J., Baker, D., Kent, C., Makin, G., & Mayhew, T. (1996). Assessment of wall structure and composition of varicose veins with reference to collagen, elastin and smooth muscle content. European Journal of Vascular and Endovascular Surgery, 11(2), 230-237. doi:10.1016/s1078-5884(96)80058-x
Whiteley, M. S. (2011). Understanding venous reflux: The cause of varicoses veins and venous leg ulcers. Guildford, UK: Whiteley Pub.




![divine [id] - didhbgt€¦ · Web view2018/07/20 · Hamel-Desnos C., Desnos P., Allaert F-A, Kern P. Thermal ablation of saphenous veins is feasible and safe in patients older than](https://img.pdfslide.tips/doc/110x75/5f3e01b9ba1fa24146718712/divine-id-didhbgt-web-view-20180720-hamel-desnos-c-desnos-p-allaert.jpg)