Embed Size (px)
Citation preview
Acute kidney injury
R3 李岳庭 / F1 王奕淳 / VS 林景坤97.10.29
Brenner and Rector's The Kidney, 8th ed P.972-976
高雄長庚腎臟科 Journal reading
Questions
AKI 何時需要洗腎 ?AKI 要怎麼洗 ?HD 跟 CVVHD 哪一個比較好 ?HD QD 會不會比 TIW 好 ?CVVHD 多洗比較好 ?有沒有其他的洗法 ?Mortality 如何 ?
General Comments
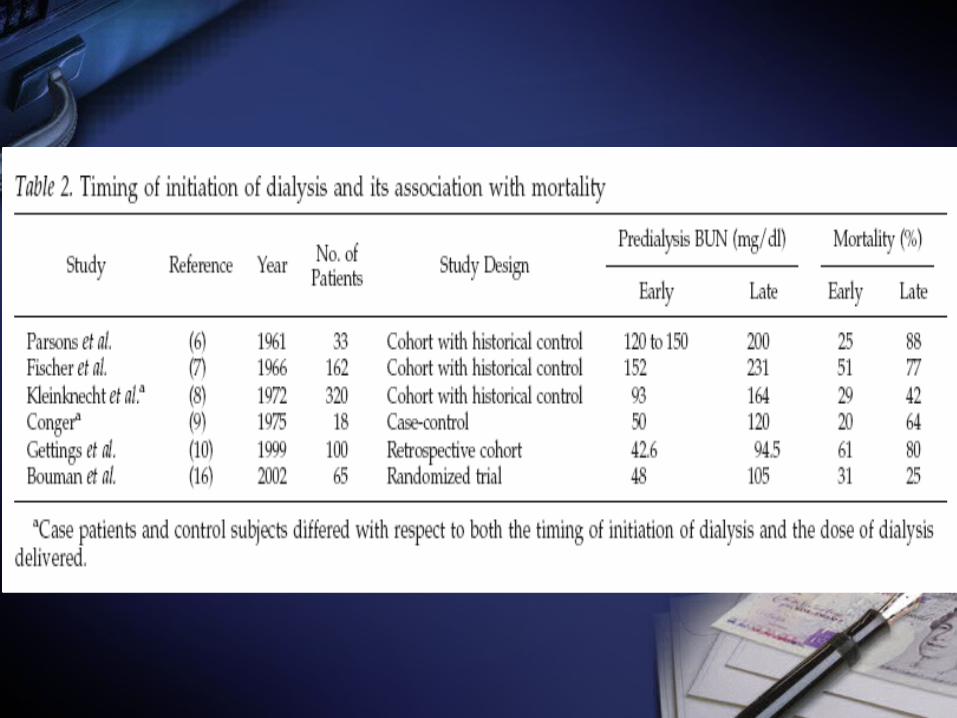
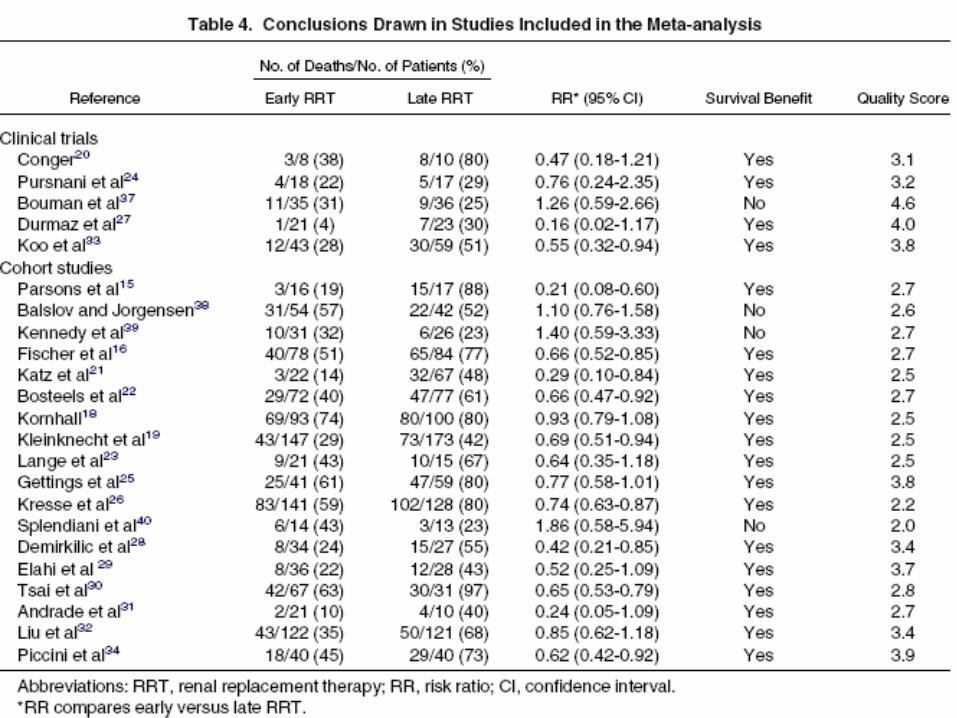
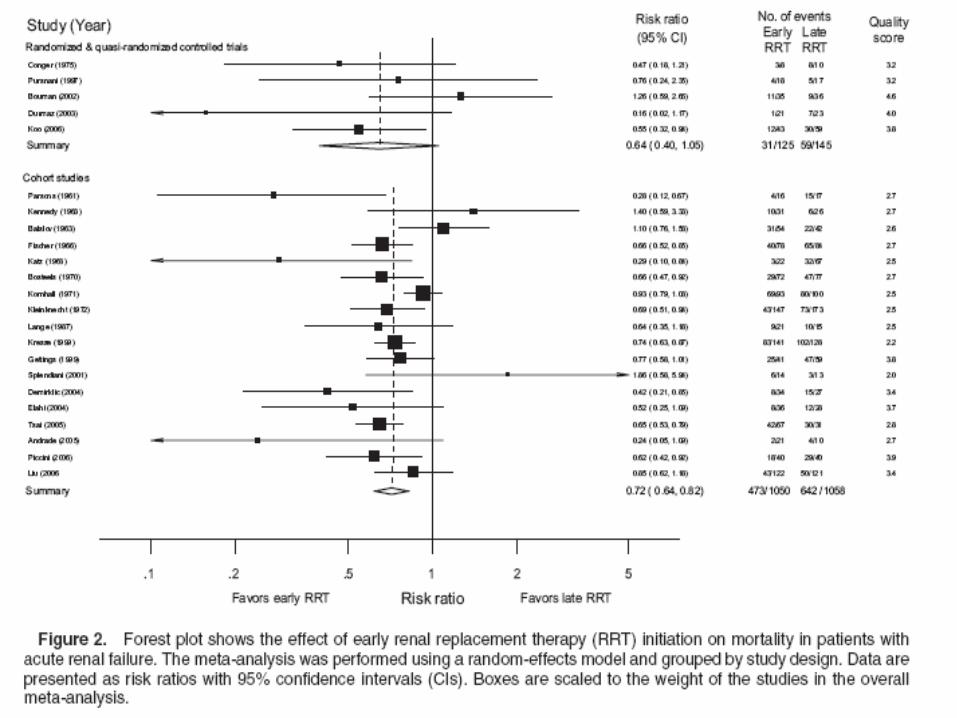
Dialysis does not hasten recovery from AKI. Early dialysis therapy improved prognosis for patients with AKI have not been confirmed.
Once the patient is established on dialysis, the optimal dose of dialysis is controversial. The standards for dialysis adequacy using intermittent hemodialysis in ARF are not defined.
Acute Intermittent Hemodialysis
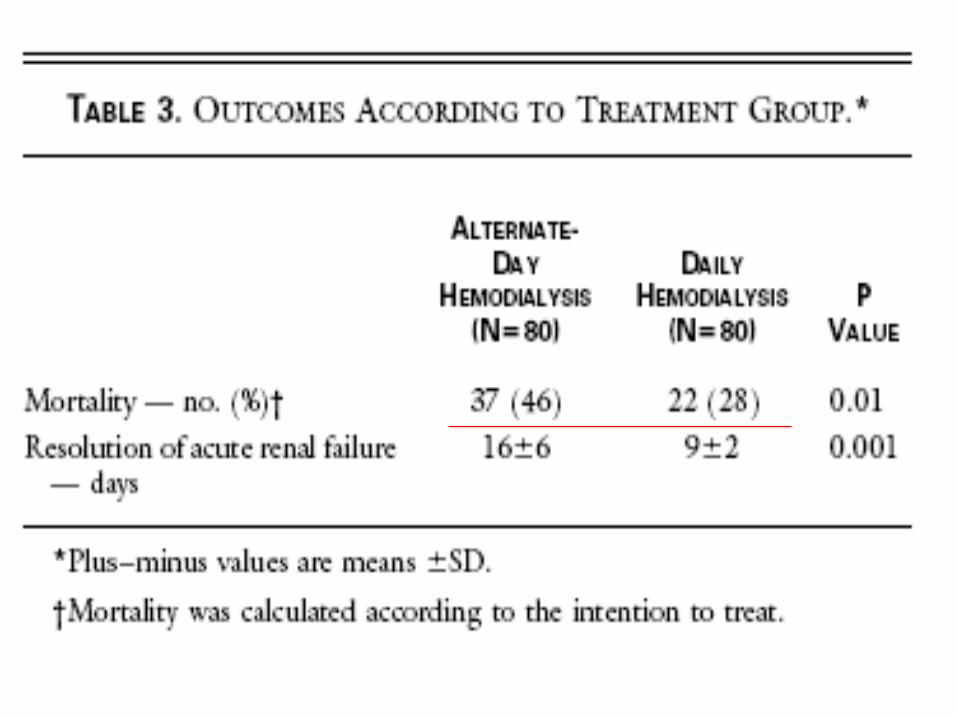
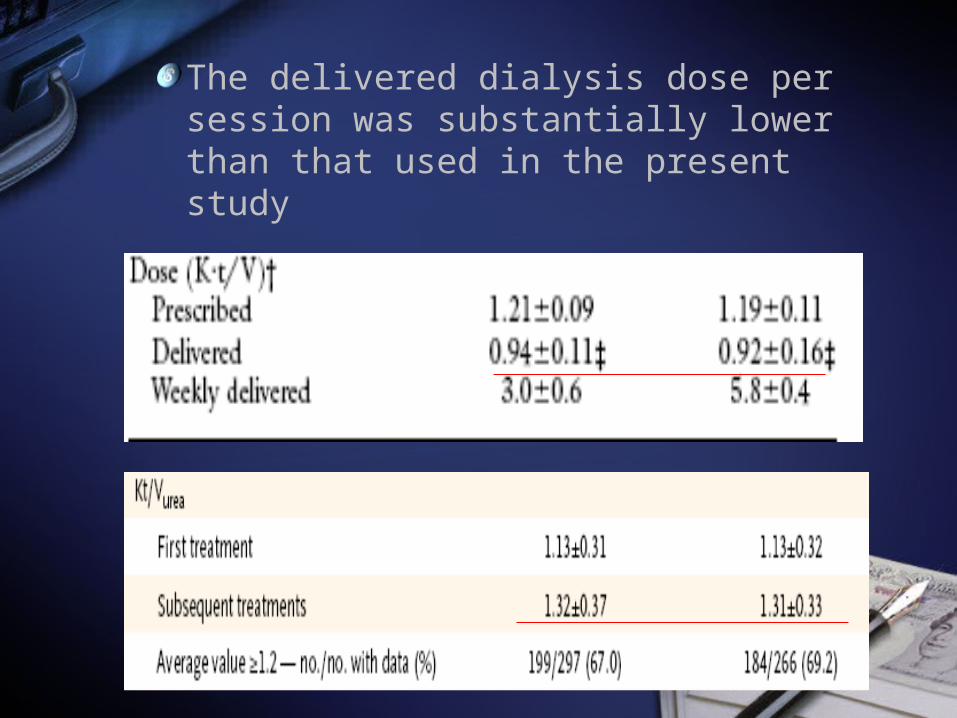
The delivered dialysis dose per session was substantially lower than that used in the present study
Continuous Renal Replacement Therapy
Continuous venovenous hemodialysis (CVVHD)Continuous venovenous hemofiltration (CVVH)Continuous venovenous hemodiafiltration (CVVHDF)
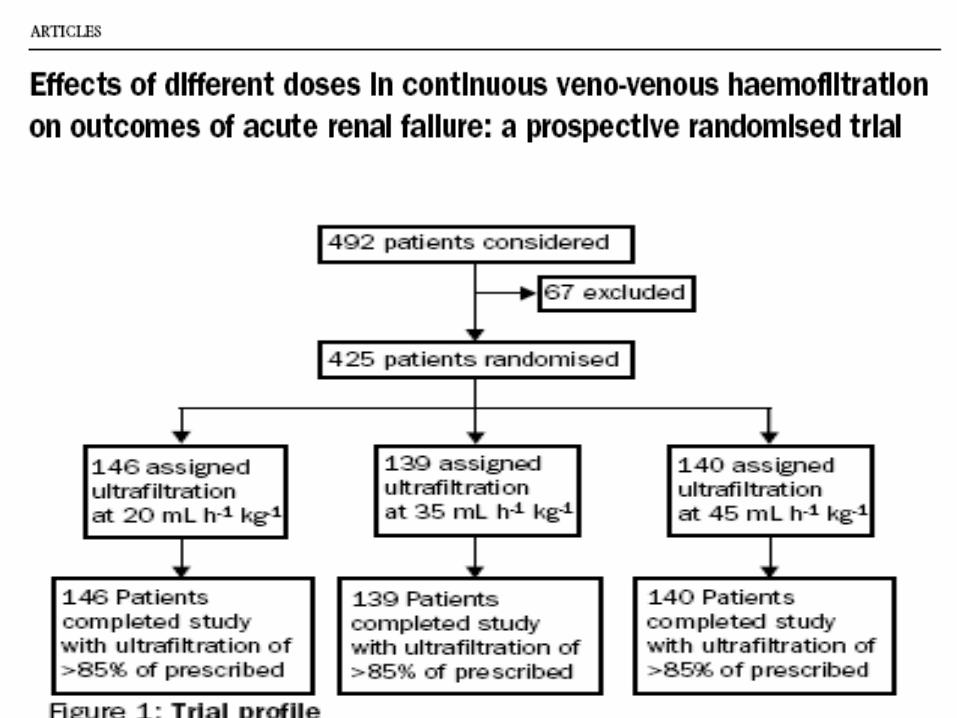
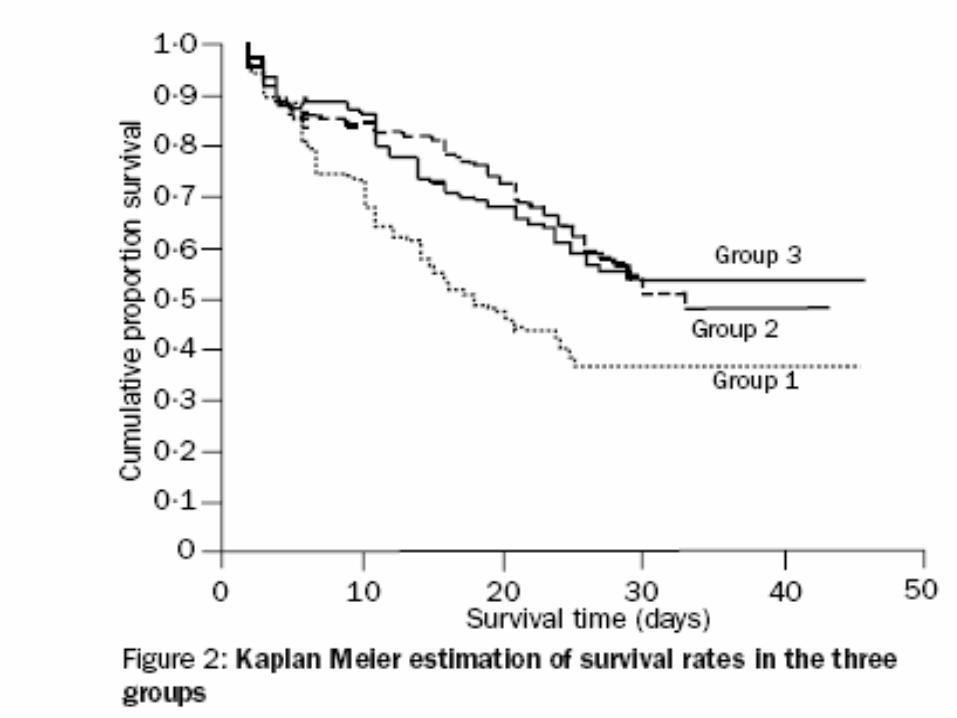
RCT with ultrafiltration rate of 35/mL/kg/hr or above is associated with improved outcomes when compared to 20 mL/kg/hr
Effects of different doses in continuous veno-venous haemofiltration on outcomes of acute renal failure: a prospective randomised trial. Lancet 2000; 356:26-30.
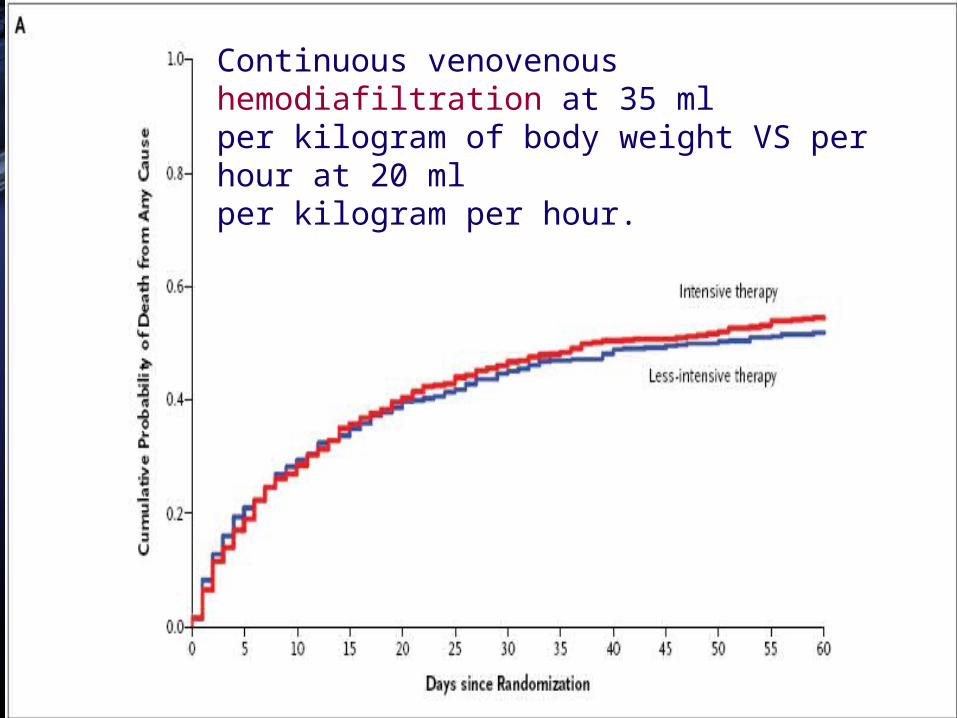
Continuous venovenous hemodiafiltration at 35 mlper kilogram of body weight VS per hour at 20 mlper kilogram per hour.
Q: Continuous forms of renal replacement therapy offer any survival advantage over acute intermittent hemodialysis?
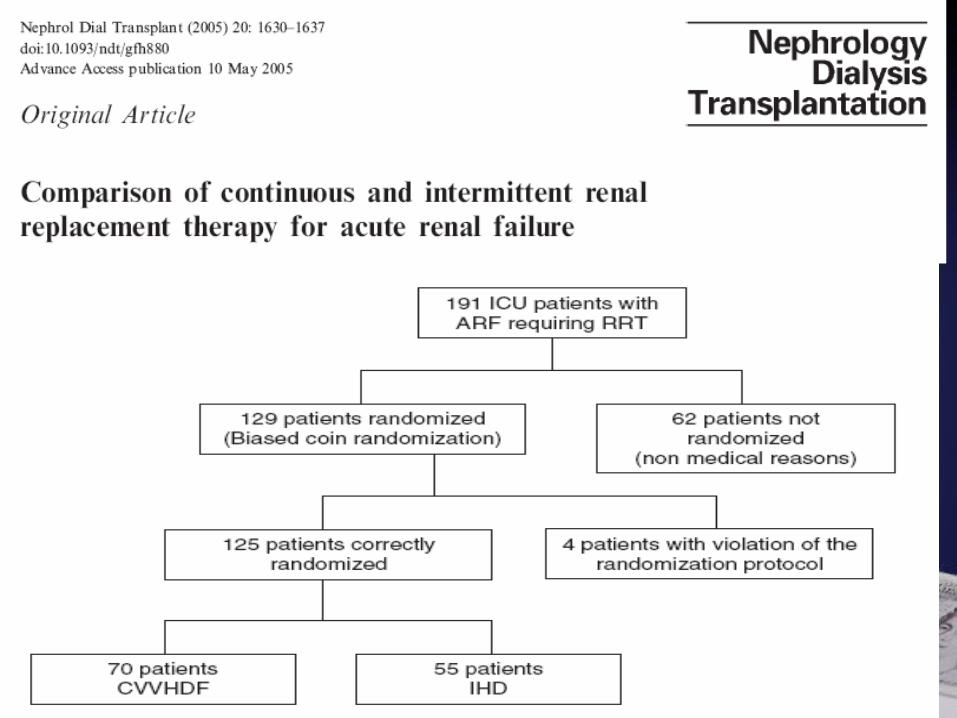
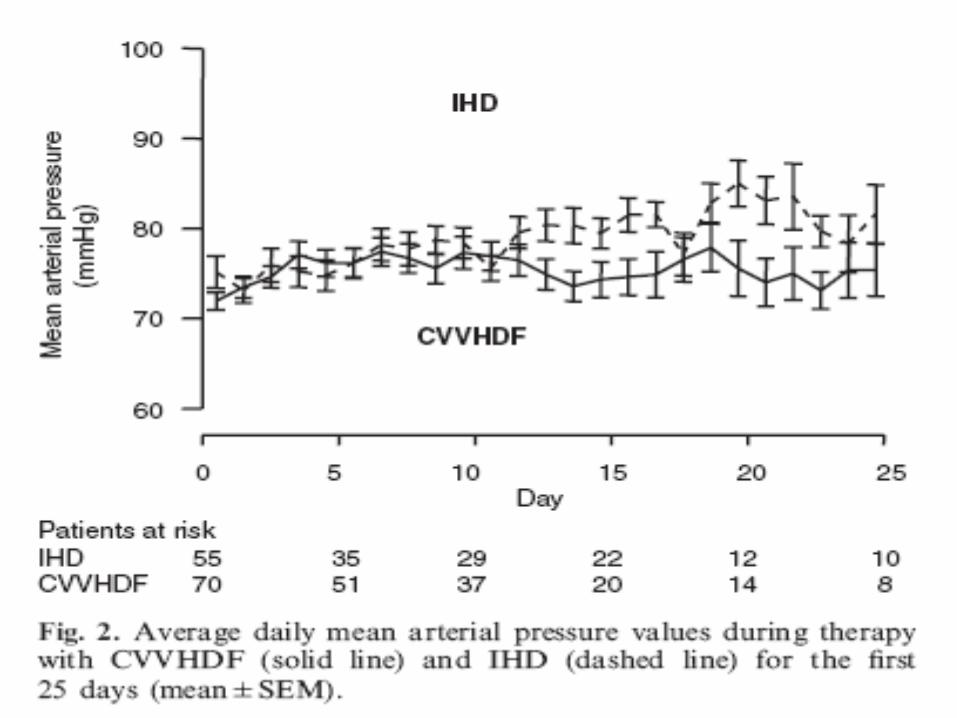
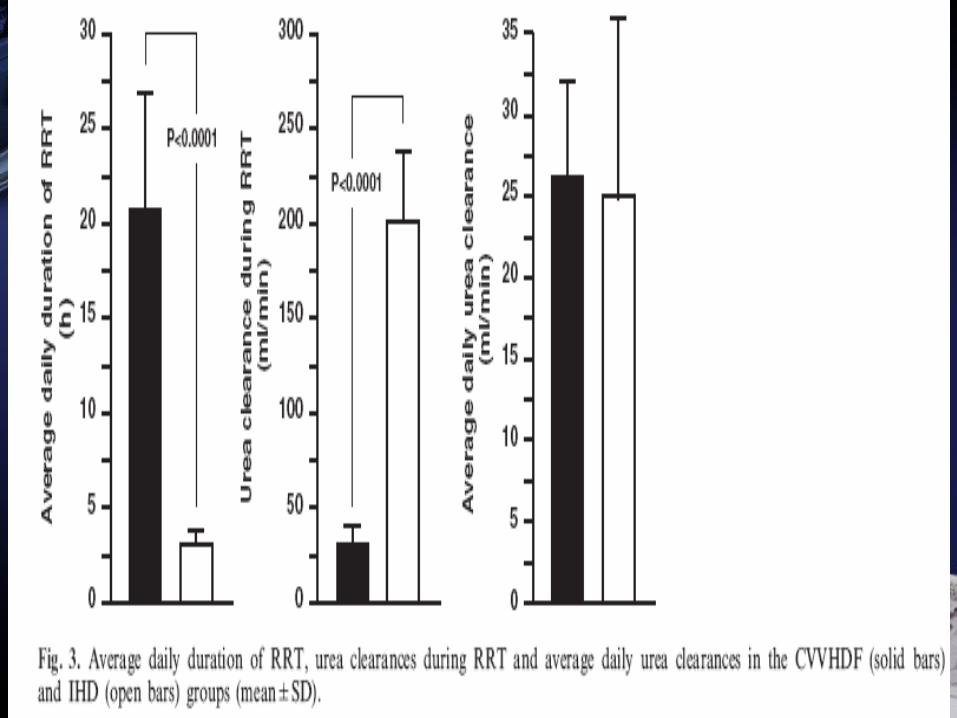
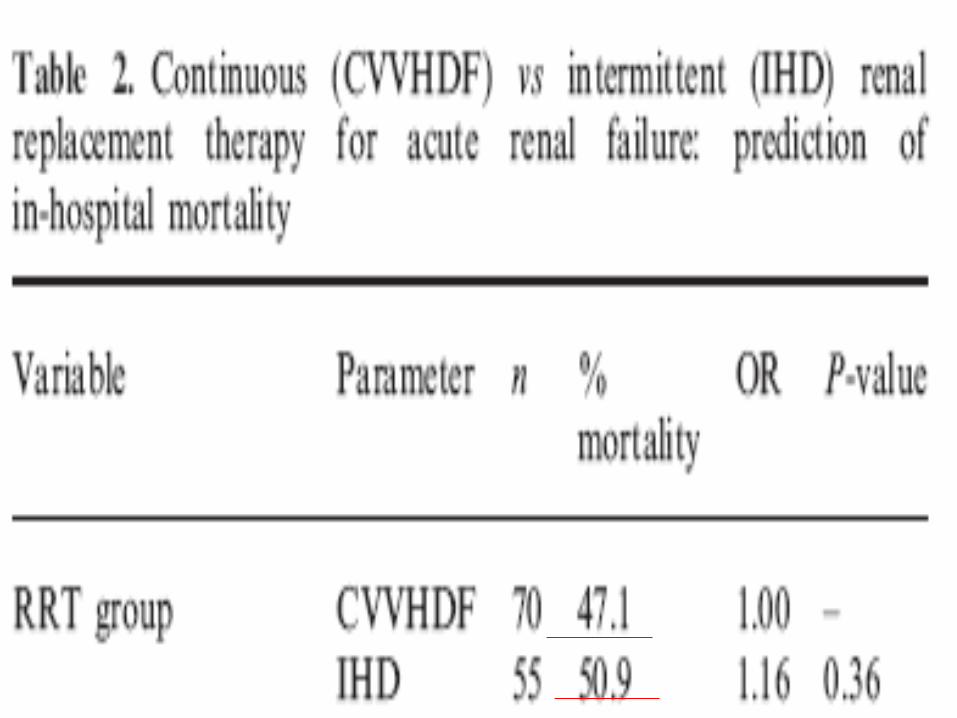
No significant difference between continuous techniques and intermittent hemodialysis with regard to overall mortality
Increasing use of slow continuous therapies will likely continueEspecially in the hemodynamically unstable and catabolic patient
Alternative approach
Slow, low-efficiency daily dialysis for prolonged periods of up to 12 hours a day.
Sustained low-efficiency daily diafiltration (SLEDD-f)for critically ill patients requiring renal replacement therapy: towards an adequate therapyNephrology Dialysis Transplantation. 19(4):877-884, April 2004
This hybrid technique typically requires
blood flows of less than 175 mL/min dialsylate flows less than 330 mL/min adequate solute and volume controlless anticoagulation.
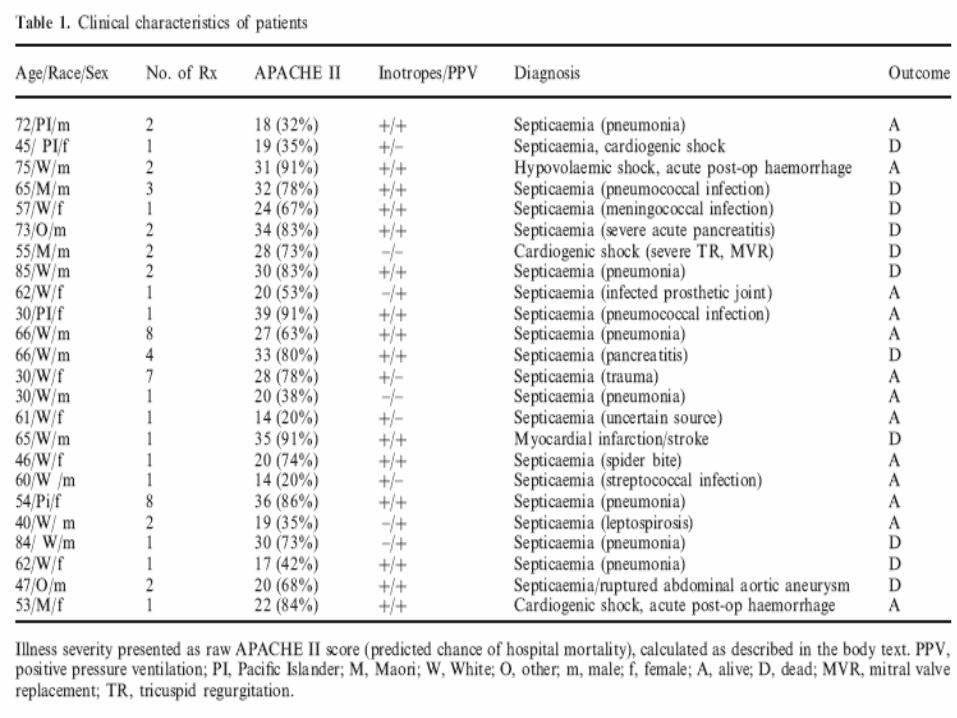
There were no episodes of intradialytic hypotension or other complications. Observed hospital mortality was 46%,not significantly different from the expected mortality as determined from the APACHE II illness severity scoring system.
OUTCOME
The mortality rate among patients with intrinsic AKI approximates 50%Changed little over the past 3 decade
Lack of improvement in outcome
Reduction in the percentage of isolated AKIIncrease in AKI complicating the multiple-organ dysfunction syndrome
A study of 6000 general ICU patients found significant association between early degrees of AKI as assessed by RIFLE score and mortality.
RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis. Crit Care 2006; 10:R73-R83.
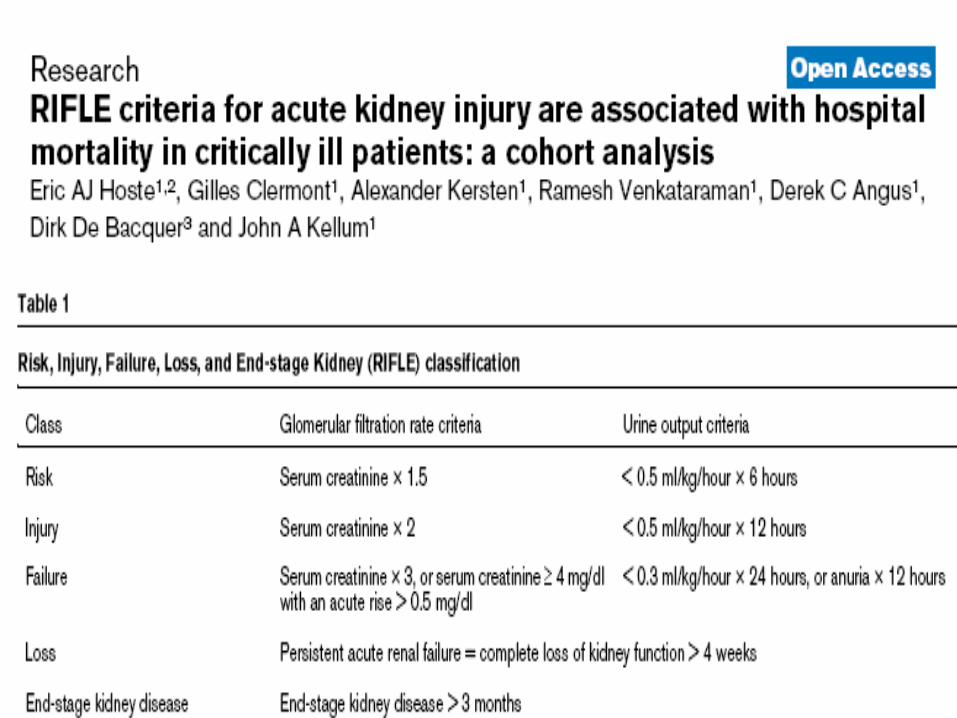
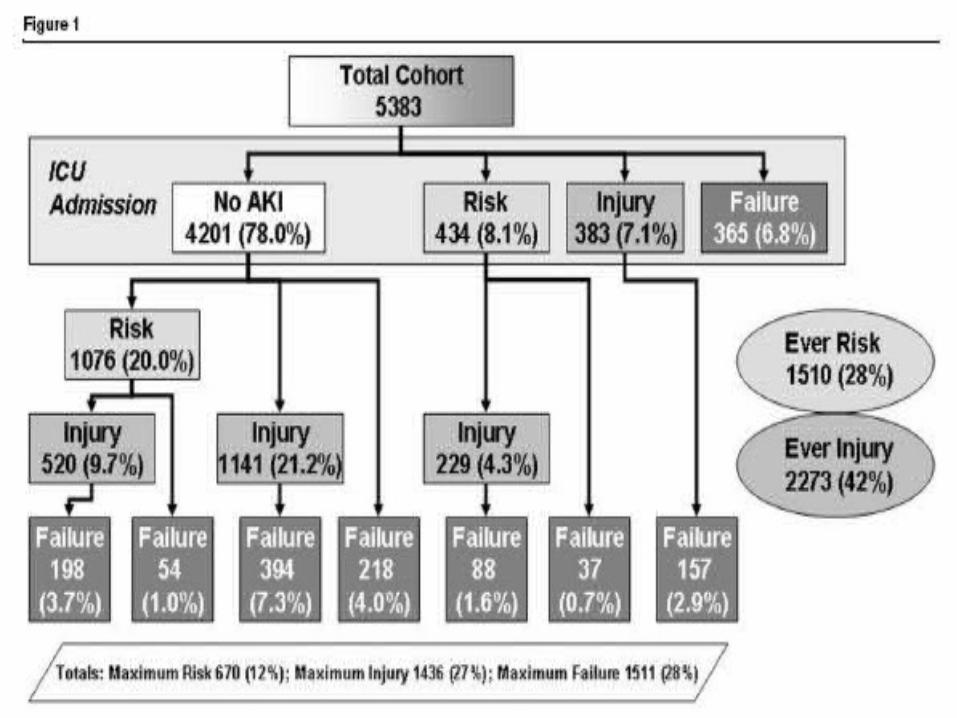
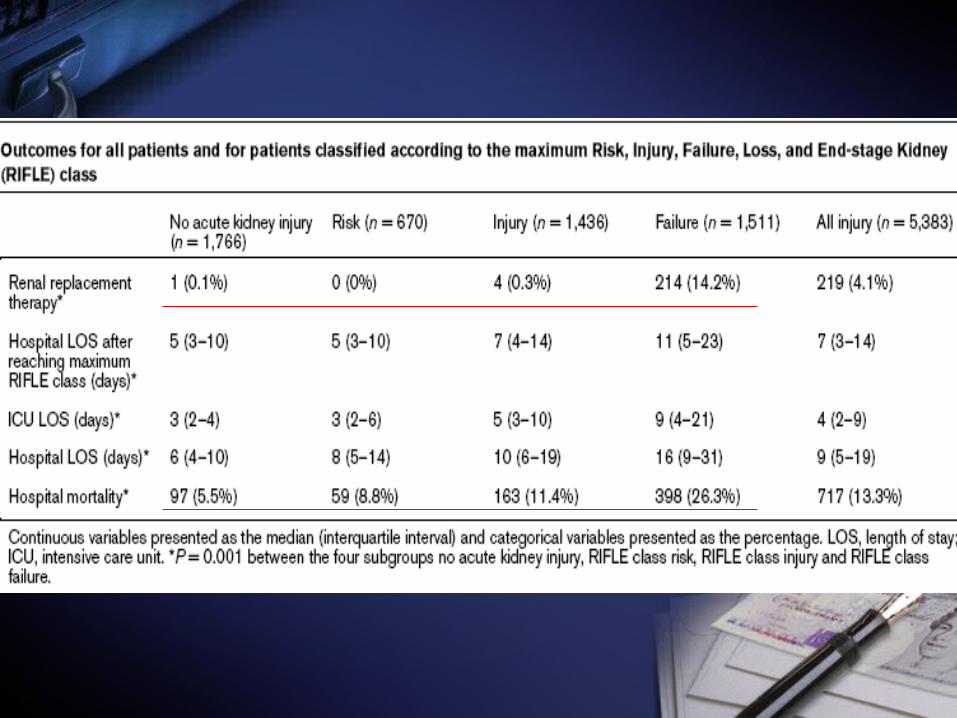
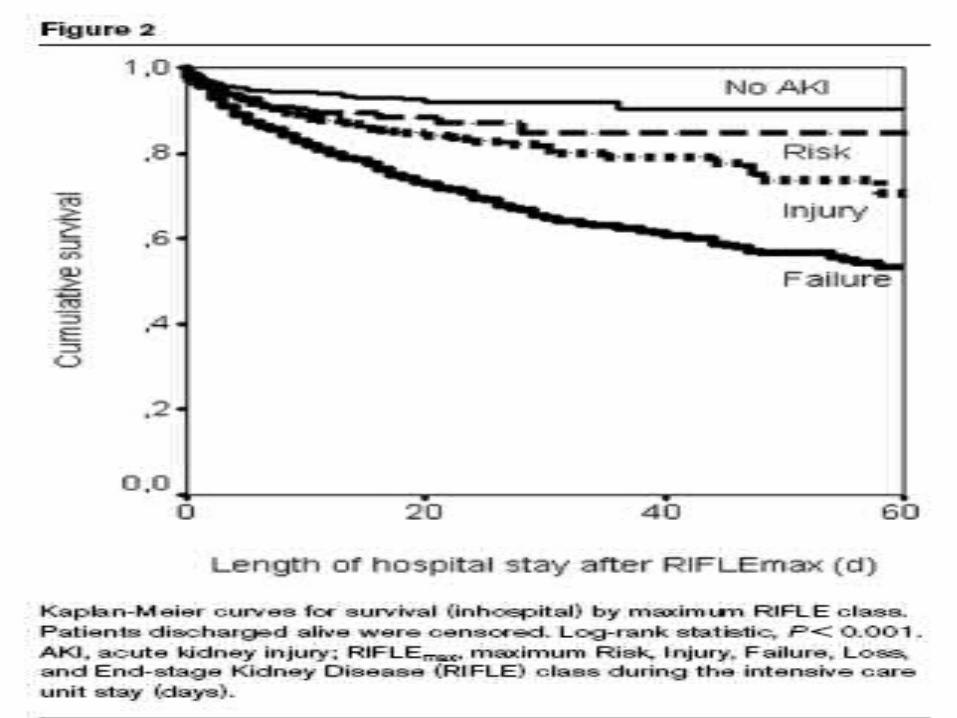
RIFLE classes injury and failure are independently associated with increased risk for in-hospital dead.
Questions
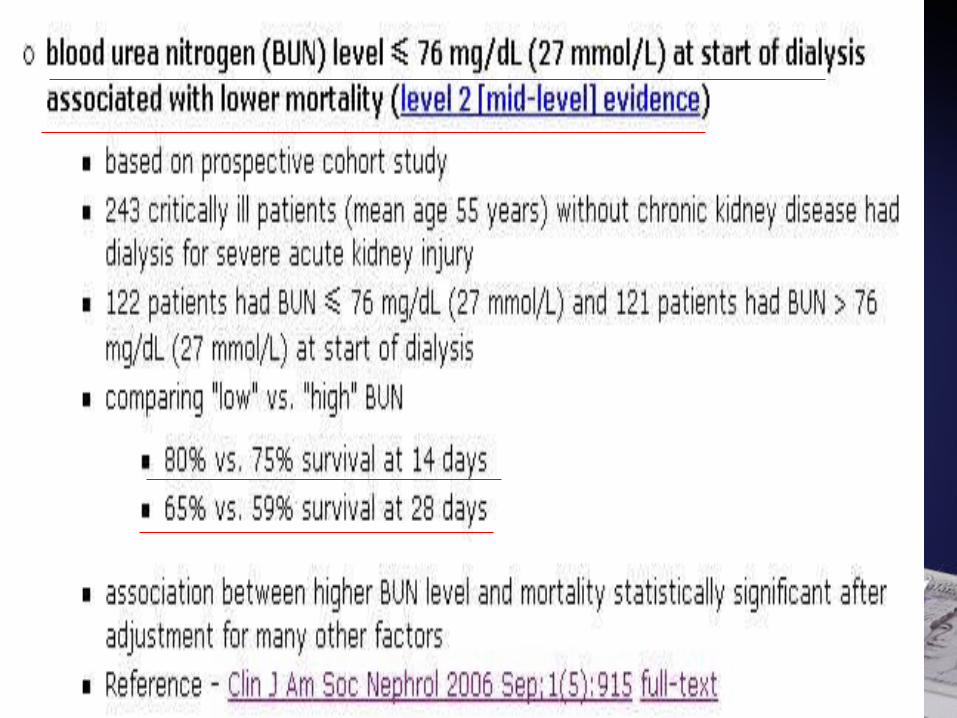
AKI 何時需要洗腎 ? BUN<76?AKI 要怎麼洗 ? ?HD 跟 CVVHD 哪一個比較好 ? 一樣HD QD 會不會比 TIW 好 ? 一樣CVVHD 多洗比較好 ? 一樣有沒有其他的洗法 ? SLEDDMortality 如何 ? RIFILE
Take home message
Early initiation of RRT in patients with ARF might be associated with improved survival.No significant difference between continuous techniques and intermittent hemodialysis with regard to overall mortality
Intensive renal support in critically ill patients with acute kidney injury did not decrease mortality.RIFLE classes injury and failure are independently associated with increased risk for in-hospital dead.
Take home message
Open discussion