-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
1/65
KIDNEYS AND ADRENAL
GLANDS
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
2/65
I. Introduction/General Information
A. Kidneys
1. Paired2. Located between T-12 & L-3/L-4
3. Between iliac crests & lower ribs
4. Right normally more inferior than left
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
3/65
Relationship of the Kidneys to
Vertebra and Ribs
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
4/65
Coronal Section, Right Kidney4. Normal adult kidney
measures:
superior inferior: 10 12 cm
medial lateral: 5 6 cm
anterior posterior: 3 4 cm
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
5/65
Introduction/General Information, cont
6. Portions of kidneys lie in six regionsof the abdomen
1. right & left hypochondriac
2. epigastric
3. right & left lumbar
4. umbilical
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
6/65
Organs of the Urinary System Kidneys
Ureters
Urinarybladder
Urethra
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
7/65
Introduction/General Information, cont
B. Adrenal Glands
1. Small, difficult to see
2. Triangular glands
a. under ribs
b. not well capsulated
c. usually anterior & medial to kidney
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
8/65
Introduction, cont
3. In Epigastric region
4. ~ T-12 to L-1/L-2
5. Right usually moresuperior than left
Why?
Left Adrenal gland
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
9/65
Introduction/General Information, cont
C. Sonographic applications
1. Poorly functioning kidney
2. Cystic vs solid or complex mass3. Post Renal Transplant
Evaluation
a. Cystic mass: may indicate fluid is
not being absorbedb. Signs of rejection
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
10/65
Sonographic applications, continued
4. Congenital anomalies
5. Perirenal abscesses, adenopathy
6. Presence/absence of kidney
7. Ectopic kidney
8. Adrenal mass or cyst:
a. Difficult to visualize
b. Unless neonate or in utero
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
11/65
II. Detailed Anatomy
A. Kidneys1. Paired, retroperitoneal
structures2. Immediately adjacent
to vertebral bodies3. Left: more superior
~ T-12 to upper L-4
4. Right: more inferior~ L-1 to lower L-4
Kidneys, in situ
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
12/65
Position of the Kidneys
P
A
Transverse Sectionthrough R/L Kidneys
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
13/65
Detailed Anatomy of Kidneys, cont
5. Not held by ligaments
-May be displaced 2.5 cm by
respiration6. Upper pole lies more
posterior thanlower pole (on L.S.)
-due to lumbar curve S
I
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
14/65
Detailed Anatomy of Kidneys, cont
7. Adjacent structures, Right kidney:
a. liver, GB
b. descending of duodenum, hepaticflexure
c. right adrenal, IVCd. right crus of diaphragm, psoas,
quadratus lumborum muscles
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
15/65
Right Kidney: Relationships
Note:
Liver
Gallbladder
Duodenal bulb
IVC
A
P
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
16/65
Right Kidney: Relationships
Note:
Liver
Descendingduodenum
Psoas muscle
Quadratus lumborummuscle
IVC
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
17/65
Detailed Anatomy of Kidneys, cont
8. Adjacent structures, Left kidney:
a. spleen, tail of pancreas, left adrenal
b. ascending duodenum,gastroesophageal junction,transverse
colon, jejunum
c. psoas & quadratus lumborum m.
d. aorta, left crus of diaphragm
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
18/65
Left Kidney: Relationships
Note:
Tail of pancreas
Splenic flexure ofcolon
Aorta
Psoas and quadratuslumborum muscles
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
19/65
Detailed Anatomy, cont
9. Diaphragm lies superior &
posterior
10.Transversus abdominislies inferior
11. Separated from abdomen
proper byparietal peritoneum
12. Surrounded by fattycapsule
S
I
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
20/65
Detailed Anatomy of Kidneys, cont
13. Internal anatomy seen on ultrasound
a. Renal cortex
b. Renal medulla (pyramids)
c. Renal columns (of Bertin)
d. Renal pelvis
e. Papillae (apices of pyramids)f. Calyces (if dilated)
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
21/65
Coronal Section, Right Kidney
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
22/65
Detailed Anatomy of Kidneys, cont
14. Pancreas & duodenum are indirect contact
a. pancreatic cancers & duodenal
ulcers can affect the kidney
b. all other organs in indirect
contact, intraperitoneal
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
23/65
Detailed Anatomy of Kidneys, cont
15. Posteriorly, right kidney separatedfrom pleura only by
diaphragm
a. Why??
b. Kidney cancer can spread tolung, vice versa
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
24/65
Detailed Anatomy of Kidneys, cont
16. Fasciae:
a. Supportive C.T. layers
b. Fascia transversalis:
1. at lateral border of kidney
2. splits into prerenal &retrorenal layers
3. forms perirenal fascia (aka:Gerotas fascia)
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
25/65
Position of the Kidneys on the Posterior
Abdominal Wall
Note:
FasciatransversalisPrerenal fasciaRetrorenal fascia
Perirenal(Gerotas)fascia
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
26/65
Detailed Anatomy of Kidneys, cont
c. Retrorenal layer
1. blends with fascia of psoasmajor & quadratuslumborum
muscles
2. also with C. T. thatbinds vertebral column
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
27/65
Fascial Coverings: Retrorenal Layer
Figure 23.2a
Retrorenallayer
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
28/65
Detailed Anatomy of Kidneys, cont
d. Prerenal layer
1. extends medially
2. anterior to renal vessels,aorta & IVC
3. blends with layer from otherside
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
29/65
Fascial coverings: Prerenal Layer
Figure 23.2a
Prerenal layer
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
30/65
Detailed Anatomy of Kidneys, cont
e. Fatty capsule lies between the
layersf. Infections may spread via fascial
sheath
-- especially bacterial infections i.e., perinephritis
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
31/65
Fatty Capsule
Figure 23.2a
Fatty Capsule(Perirenal fat)
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
32/65
Detailed Anatomy of Kidneys, cont
17. Kidney maintains position by intra-abdominal pressure &
fasciae
a. Allows mobility during respiration
b. Allows abdominal palpation oflower pole in some patients
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
33/65
Detailed Anatomy of Kidneys, cont
18. Two layers of renal fascia
a. fuse at upper pole
b. separate at lower polec. if fat decreases, mobility
increases:
1. kidney may move betweenfascial planes
2. pelvic kidney
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
34/65
Detailed Anatomy of Kidneys, cont
d. Adrenals have own fasciae, will
not movee. Kidney may be removed without
disturbing adrenal gland
f. Pathological result:
1. kidney may descend
2. cause kink in ureter
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
35/65
Detailed Anatomy of Adrenals
B. Adrenal Glands1. ~ T-12 to L-1 or L-2
2. Located in epigastricregion
3. Right adrenal liesmore superior
a. Related to visceralsurface of liver
b. IVC & right crus liemedial L. Adrenal Gland, in situ
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
36/65
Detailed Anatomy of Adrenals, cont
c. Right kidney lies
posterior, inferior
& slightly lateral
1. Has linear,
pyramidal, orelongated shape
2. One limb extendsalong medialaspect
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
37/65
Detailed Anatomy of Adrenals, cont
4. Left adrenal
a. Lies posterior & medial to
cardiac sphincter, spleen, medial to tailof pancreas
b. aorta & left crus lie medial
c. left kidney lies posterior, inferior, &lateral
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
38/65
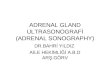
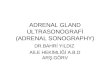
Adrenal Gland In Situ Coronal Section / Adrenal Gland
Human Adrenal Gland
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
39/65
Detailed Anatomy of Adrenals, cont
d. More triangular in shape
e. One limb may extend alongmedial aspect of left kidney
f. Fourth part of duodenum is
caudad
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
40/65
Detailed Anatomy, cont
C. Blood supply1. Renal arteries:
a. arise from abdominal aortab. Divide into 2 or 3 branches
before
entering kidney
c. If 3 branches, may form:1. vascular fork
2. may constrict ureter
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
41/65
Renal Arteries with Vascular Fork Note the
numerous
branches ofthe renalartery priorto entering
the kidneyhilus
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
42/65
Detailed Anatomy, cont
d. R. renal artery courses from aorta
posteriorto IVC into hiluse. Left renal artery course is
from
aorta directlyto hilusf. May see 2 or 3 pairs of renal
arteriesg. Gonadal arteries:
1. may arise from renal artery
2. usually arise from aorta
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
43/65
Origin of Renal, Gonadal Arteries Note the
rightgonadal
arteryarising fromthe aorta,thenbranching
to form theinferiorcapsularartery.
R and LRenalArteries
GonadalArteries
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
44/65
Variations in Renal Arteries The
presence of
multiplerenalarteriesrepresents
persistenceof fetalvessels
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
45/65
Detailed Anatomy, cont
2. Renal Veinsa. Right renal vein enters IVC
directlyb. Left renal vein passes anterior
to aorta, posteriortoSMA, then into IVC
c. Venous pattern complex
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
46/65
Variations in Renal Veins
Note theduplication in
the Left RenalVein
Branchessurround aorta
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
47/65
Pathway of Renal Vessels
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
48/65
Detailed Anatomy, cont
d. On the left side:
1. anastomosis of veins2. from left adrenal, pampiniformplexus
of testis, perirenal fat,ureter
e. Surgery may permit spread ofinfection
f. Malignancies frequently spread viarenal vein
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
49/65
Detailed Anatomy, cont
3. Adrenal glands
a. Blood supply intensiveb. Superior adrenal artery arises
from inferior phrenic artery
c. Middle suprarenal artery arisesfrom aorta
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
50/65
Detailed Anatomy, cont
d. Inferior suprarenal artery arisesfrom renal artery
e. Only one vein drains each gland
1. right drains directly into IVC2. left drains into left renal
vein
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
51/65
Origin of Adrenal ArteriesNote the
superiorarteryarising from
the phrenic a.,the middleartery from theaorta, and
theinferiorartery
from thesuperiorcapsular arteryviathe R. renalartery
SuperiorAdrenal
Artery MiddleAdrenalArteryInferior
AdrenalArtery
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
52/65
Detailed Anatomy, cont
D. Lymphatics
1. Renal lymphatic channels
follow veins2. Most drain into para-
aortic nodes
a. Lie inferior at ~ L-3 or L-4
b. Near bifurcation of aorta
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
53/65
Detailed Anatomy, continued
E. In neonate kidney, note:a. Large size of adrenal vs
kidney
b. Lobulation of kidney (plastinatedspecimen)
c. Increased amount of perirenalfat
d. Paraganglia along aorta1. precursor to aortic nodes
2. degenerate in childhood
Lobulated FetalKidneys
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
54/65
Detailed Anatomy, cont
E. Innervation
1. Sensory nerve fibers of kidney &
ureter join spinal cord at T-11 to L-2
2. Passage of calculi causes peristaltic
action of ureter
a. Muscle spasms cause pain in regionssupplied by T-11 to L-2
nerves
b. Pain may refer to testis or anterior thigh
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
55/65
III. Gray-scale anatomyA. U/S can differentiate renal
pyramids,
cortex, columns, calyces, pelvis
1. Pyramids appear echodense regionswithin parenchyma
a. Apex of pyramid = papilla
b. Apex points toward pelvis
2. Cortex, columns less dense than liver
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
56/65
IV. Renal PathologyA. Malpositioned (ectopic) kidney
1. Kidneys migrate cephalad during
development2. Ptosis (Gr. falling): kidney has
sunk from its usual site in fossa3. Pelvic Kidney:
a. lies in floor of pelvic cavityb. may be hypoplastic,
distorted
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
57/65
Pelvic Kidney
Note the
paths ofthe renalartery andrenal veinin pelvickidneys
Ectopic Kidneys
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
58/65
Malpositioned Kidney, continued
2. If kidney not identified in renal fossa,scan lower abdomen
& pelvis
3. If reniform mass is observed in abdomenor pelvis, check renal
fossa
4. If pelvic or ectopic kidney seen in
pregnancy, C-section advised5. Crossed kidneys usually seen
inpediatric age group
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
59/65
Renal Pathology, continued
B. Hypoplasia
1. Kidney small, with poorfunction
2. Appears distorted withincreased lobulation
3. Differentiation fromdiseased kidneymay be difficult
Renal Hypoplasia
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
60/65
Renal Pathology, continued
4. Differentiation from true renal agenesismay be difficult
a. In agenesis, fossa may contain
bowel (simulates hypoplasia)b. Both may result in hypertrophy
of
contralateral kidney
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
61/65
Renal Pathology, continued
C. Duplication/Fusion:
1. May be a duplex
collecting system or twoseparate components
2. If complete separationoccurs, upper pole ureter
may form ureterocele:
Duplex/FusedCollection Systems
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
62/65
Renal Pathology, continued
a. Leads to obstruction &
hydronephrosis
b. May have septations
c. Appears as triangular,sonolucent sac inupper aspect of
kidney
Hydronephrosis
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
63/65
Renal Pathology, continued
3. Horseshoe Kidneya. Most common fusion anomaly
b. Usually fused at inferior polec. The isthmus may simulate
aretroperitoneal mass
d. May be confused with para-aortic
lymph nodese. Look for malrotated pelvis
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
64/65
Abnormal Kidney Structures
Note the
fusedlower poleandrotated
pelves
PancakeKidney
HorseshoeKidney
Malrotated
Kidneys
-
7/31/2019 BIOL226Lec10 Kidney,Adrenal
65/65
Renal Pathology, continued
Renal and Adrenal Diseases: In Patho