Embed Size (px)
Citation preview

대한혜담도연구회지 1997; 2: 168-172
Adenosquamous Carcinoma of the Pancreas: Differentiation from Pancreatic Pseudocyst
Seung Jae Myung, M.D. , Yeun Suk Kim, M .D ., Seung Yong Kim, M .D.
=국문초록=
Hong Ja Kim, M.D. , Jeong Su Kim, M.D., Dong Wan Seo, M .D .,
Sung Koo Lee, M.D. , Myung Hwan Kim, M.D., and Young 11 Min, M.D.
Department of Intemal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
가성낭종과 구별이 어려웠던 훼장 선편평상피암 1여|
울산대학교 의과대학 서울중앙병원 내과학교실
명승재·김연석·김승용·김흥자·김정수
서동완·이성구·김명환·민영일
혜장의 선평편상피암은 드문 형태의 춰l장암으로 이의 생물학적 행태와 임상적 양상은 훨씬
흔한 종류인 쉐장선암입니다 선암이나 순수한 평편상피암과 유사한 것으로 알려지고 있다. 저자등은 초기에 쉐장가성낭종과의 감별이 힘들었던 드문 형태의 춰l장 선편펑상피암 1예를
경험하였기에 문헌고찰과 함께 보고하는 바이다.
중심단어 선편평상피암, 춰l장, 궤장가성냥종, 낭성변성
extravasation of contrast to the mass have also been
INTRODUCTION reported.5-6 We report here an unusual case of adeno
squamous carcinoma of the pancreas which has ini-
Adenosquamous carcinoma of the pancreas is a rare tially brought some difficulties in differentiating from
form of pancreatic cancer. 1•2 Its bi이ogical behavior pancreatic pseudocyst.
and c\inical features are known to be similar to the
much more common ductal adenocarcinoma or to
pure squamous cell carcinoma, another rare form of
pancreatic malignancy.3.4 However, the unusual mani
festations of cancer with cystic degeneration and
연락처 명송재, 서울시 송파구 풍납동 388-1 , 서울중앙병원 소화기 내과
168
CASE REPORT
A 64-year-old man was admitted to our hospital
with a two-week history of epigastric pain. The
patient complained that the pain was dull and
continuous radiating to his back. He was a social

Seung Jae Myung, et al: Aden∞quamous Carcinoma of the Pancreas: Differentiation from Pancreatic Pseudocyst 169
drinker and denied use of any kind of drug medi- mild tenderness over the epigastrium, but no rebound
cation. There was no history of abdominal trauma or tenderness or guarding was present. There was no
diabetes mellitus. No fever, chills, jaundice, or weight hepatosplenomegaly or palpable mass. Laboratory
loss was reported. Family histoη was unremarkable. tests incIuded white blood count 8,100 cellsjmm3, On physical examination, the patient was thin and hemoglobin 13.6 gjdl, amylase 263 UjL (60-210 UjL) ,
not in the state of acute distress. He complained of and Iipase 461 UjL (66-220 UjL). Liver function test
and tumor markers (CAI9-9 and CEA) were within
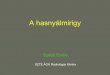
Fig. 1. Abdominal CT scan showing 3- to 4-cm sized ovoid cyst-like lesion in the region of the pan-creatic head.
the norrnal Iimit.
An abdominal CT scan revealed a 3- to 4-cm sized
ovoid and cyst-Iike lesion in the region of the pan
creatic head (Fig. 1). The pancreatic duct was mildly
dilated, however, the parenchyma of the pancreatic
body and tail showed no specific abnorrnal findings.
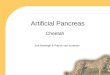
Endoscopic retrograde balloon pancreatography (ERP)
showed about a 2 cm segmental narrowing of the
main duct at the head portion of the pancreas and
mild upsπeam dilatation (Fig. 2A). In the pancreatic
head, round contrast pooling in communication with
the main duct was noted (Fig. 2A). Brush cytology
revealed no malignant cells but many sheets of ductal
Fig 2. A. Endoscopic retrograde balloon pancreatogram (ERP) showing segmental narrowing (arrow) and mild upstream dilatation of the main pancreatic duct and round pooling of the contrast at some distance (arrow head).
B. Magnetic resonance cholangiopancreatography revealing pancreatic ductal change similar to the findings on ERP and round cystic lesion in the pancreatic head.

170 대한혜담도연구회지 제 2 권 제 2 호 1997
epithelial cells. Magnetic resonance cholangiopancrea
tography showed pancreatic ductal change similar to
the findings on ERP and a round lesion with cystic
character in the pancreatic head (Fig. 2B).
The clinical features and radiological fmdings were
felt most consistent with a pancreatic pseudocyst and
benign stricture secondary to chronic pancreatitis, although a cystic tumor or ductal carcinoma could not
be ruled out. A pancreatic stent was inserted to relieve
the stasis in the pancreatic duct, and supportive care
including NPO and total parenteral nutrition was com
menced. Even after four weeks of medical therapy,
the patient still complained about the persistence of
abdominal pain. Follow-up ERP showed no change of
the ductal narrowing in the main pancreatic duct but
the cyst-like lesion in the region of the pancreatic
head showed enlargement on follow-up CT scan.
Cytologic findings from needle biopsy of the pan
creatic head were interpreted as adenosquamous carci
noma.6•7 The patient underwent pylorus preserving
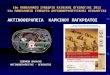
pancreatoduodenectomy and a 3.5 x 3 X 2.8 cm sized
poorly demarcated mass with a cystic cavity was
resected (Fig. 3). Upon histological examination, the
tumor was composed mainly of nests of malignant
squamous cells with areas of adenocarcinoma which
was compatible with adenosquamous carcinoma of the
pancreas (Fig. 4) πle postoperative course was un-
Fig 3. Macroscopic appearance of the adenosquamous carcinoma of the pancreatic head. Poorly demarcated firm infiltrating mass with cystic change was noted
Fig 4. Photomicrograph of the transitional zone where adenocarcinoma and squamous cell carcinoma are seen m contact.

Seung Jae Myung, et al: Aden∞quamαIS Carcinαna of the Pancreas: Differentiation from p,외1σ'eatic Pseudocyst 171
eventful and the patient was doing well at 4-month creatic duct. Pain relief and the resolution of the
follow up. pseudocyst were expected. lO,11 Even after four weeks
of medical treatment, the patient ’s symptoms had not
DISCUSSION been improved. Follow up ERP showed no change of
Adenosquamous carcinoma of the pancreas, often
called adenoacanthoma, is a rare variant of nonendo
crine pancreatic cancer. 1,2 까le collective incidence of
this malignancy has been estimated at 1 - 4 % of
pancreatic malignancies,3-4,8 even though higher rates 1,9 of 9-11 % have been reported in Japan.'" Some au-
thors have suggested that pure squamous cell carcino
ma behaves more aggressively,8 however, literature
review shows no significant differences in age pre
valence, sex ratio, distribution of cancer in the pan
creas, neoplastic behavior, or prognosis among adeno
squamous carcinoma, ductal cell carcinoma, and pure 2-5 squamous cell carcinoma of the pancreas.
Our patient was initially managed under the diag
nosis of chronic pancreatitis with pseudocyst because
of his pain compatible with pancreatitis and the ele-
vated pancreatic enzymes. Radiologic fmdings sup
ported our first conclusion. Segmental narrowing of
the main pancreatic duct suggesting benign stricture
was detected on ERP. The lesion in the pancreatic
head was almost purely cystic and it did not exhibit
a definite mass on CT (Fig. 1). Brush cytology
revealed no malignant cells, a1though a sufficient
number of cells had been taken. However, there also
were several fmdings that were not consistent with
chronic pancreatitis. The parenchyma of the pancrea
tic body and tail did not show the changes of chronic
inflammation, such as swelling, fluid collection, or
calcification on CT scan. The dilated main duct was
rather smooth on ERP as well . A cystic tumor and
malignant neoplasm were also suspected, but clinical
features and radiological findings were not compatible
with both conditions.
The patient was managed by stenting of the pan-
ductal stricture, and abdominal CT scan showed
enIargement of the previously noted cyst-like lesion.
πle cytologic findings from the needle biopsy sug
gested adenosquamous carcinoma of the pancreas,
which was confirmed by surgical resection of the
tumor.
Aside from having a rare type of pancreatic tumor,
this patient exhibited very unusual features which led
us to an erroneous initial diagnosis. This case showed
extravasation of ERP contrast into a tumor cavity due
to cystic change, as well as ductal communication to
the cystic portion of the tumor. These findings can
occur in a cystic neoplasm with ductal communication
or in a pseudocyst associated with pancreatitis or
tumor. Extravasation of the contrast to the ductal cell
carcinoma is possible,12 however, pooling of the
contrast at some distance from the main duct or round
accumulation of the contrast shown in our case is an
uncommon finding. πlese findings are quite unusual
for adenosquamous carcinoma of the pancreas as well, 5,6 although a few similar cases had been reported. J ,U Our
case and previous cases suggest that this rare pan
creatic malignancy can be misdiagnosed as pancrea
titis with pseudocyst. In adenosquamous carcinoma of
the pancreas, ductal communication with cancer may
be expected since this rare malignancy may arise from
the malignant degeneration of squamous metaplasia of
pancreatic ductal epithelium.1
In summary, we report a case of adenosquamous
carcinoma of the pancreas with unusual manifestation.
lnitially, a cyst-like lesion in the region of pancreatic
head was diagnosed as pancreatic pseudocyst asso
ciated with chronic pancreatitis. Our case emphasizes
that this rare pancreatic tumor can be difficult to
differentiate from a benign condition, such as pan-

172 대한쉐담도연구회지 · 제 2 권 제 2 호 1997
creatic pseudocyst, thus mislead the physician into
arriving at an initial misdiagnosis.
Key Word: Pseudocyst, Pancreas, Adenosquamous
carcmoma
REFERENCES
1. Ishikawa 0 , Matsui Y, Aoki 1, Iwanaga T, Terasawa
T, Wada A: Adenosquamous carcinoma of the
pancr않s: A c\inicopathologic study and report of three
cases. Cancer 1980; 46: 1192-6.
2. Makiyama K, Takuma K, Zea-Iriarte WL, lkuno N, Kawatomi M, Mori N, et al: Adenosquamous
carcinoma of the pancr않s. J Gastroenterol 1995; 30
798-802.
3. Cubilla AL, Fitzgerald PJ: Morphological pattems of
primary nonendocrine human pancreas carcinoma.
Cancer Rest 1975; 35: 2234-48.
4. Chen J, Baitkun SI: Morphological study of 391 cases
of exocrine pancreatic tumors with special reference
to the c\assification of exòcrine pancreatic carcinoma
J Pathol 1985; 146: 17-29
5. Beyer KL, Marshall JB, Metzler MH, Pou\ter JS, Seger RM, Diaz-Arias AA: Squamous cell carcinoma
of the pancr않s : Report of an unusual case and review
of the literature. Dig Dis Sci 1992; 37: 312-8.
6. Wi \czynski SP, Vanente PT, Atkinson BF: Cyto
diagnosis of adenosquamous carcinoma of the pan
creas: Use of intraoperative fine needle aspiration.
Acta Cytol 1984; 28: 733-6.
7. Smit W, Mathy JP, Donaldson E: Pancreatic cytology
and aden∞quamous carcinoma of the pancr않S. Patho
logy 1993; 25: 420-2.
8. Baylor SM, Berg JW: Cross-c\assification and survival
characteristics of 5,000 cases of cancer of the pan
creas. J Surg Oncol 1973; 5: 335-58.
9. Yamaguchi K, E띠oji M. Adenosquamous carcinoma
of the pancreas: A c\inicopathologic study. J Surg
Oncol 1991; 47: 109-16
10. Catalano MF, Geenen JE, Schmalz MJ, Johnson GK, Dean RS, Hogan WJ: Treatment of pancreatic
pseudocysts with ductal communication by trans
papillary pancreatic duct endoprosthesis. Gasσointest
Endosc 1995; 42: 214-8
11. Ponchon T, Bory RM, Hede\ius F, Roubein LD, Paliard P, Napoleon B, et al: Endoscopic stenting for
pain relief in chronic pancreatitis: results of a stan
dardized protoc이 . Gastrointest Endosc 1995; 42:
452-6.
12. Siegel JH: Endoscopic retrograde ch이angiopancreat
ography: Technique, diagnosis, and therapy. New
York: Raven Press, 1992: 155-6.