Embed Size (px)
Citation preview
Adrenergic DrugsLEARNING OBJECTIVES
Define adrenergic receptors and the drugs acting on them Describe the structural requirements of a sympathomimetics acting on α and β subtypes Classify sympathomimetics and describe their preparation method Describe the importance of specificity of the receptor environment based on optical isomers of
ephedrine Define sympatholytics and their utility Classify sympatholytics, their uses and actions
22.1 INTRODUCTION
Adrenergic drugs are those chemical agents that exert their principal pharmacologic and therapeutic effects by acting at peripheral sites to either enhance or reduce the activity of components (adrenaline) of the sympathetic division of the autonomic nervous system. In general, those substances that produce effects similar to stimulation of sympathetic nervous activity are known as sympathomimetics, adrenomimetics, or adrenergic stimulants. Those that decrease sympathetic activity are referred to as sympatholytics, antiadrenergic, or adrenergic blocking agents.
Adrenergic receptors: In the adrenergic system there are two main types of receptors: α and β. There are two types of α-adrenoreceptors, α1 and α2. The α1-adrenoreceptors subserve smooth muscle stimulant functions, adrenergic sweating, and salivation. The α2-adrenoreceptors serve to inhibit the pre-synaptic release of noradrenaline and the post-synaptic activation of adenylate cyclase (and, hence, inhibit post-synaptic responses). The β-adrenoreceptors are subdivided into β1 and β2 adrenoreceptors, and perhaps more. β1-adrenoreceptors effect cardiac stimulation and lipolysis; β2-adrenoreceptors subserve adrenergic smooth muscle relaxation (vasodilatation, bronchodilatation, and intestinal and uterine relaxation) and glycolysis.
22.2 SYMPATHOMIMETIC DRUGS
Peripheral actions and uses of sympathomimetics are discussed below.
22.2.1 α-Adrenoreceptor Agonists
α-Agonists cause arteriolar and venous constriction and, hence, have an action to increase blood pressure. This vasopressor action is used to support blood pressure in hypotensive states, such as in orthostatic hypotension, carotid sinus syndrome, shock, and during spinal anaesthesia.
The systemic vasoconstrictor effects are also employed in the management of a variety of serious allergic conditions, such as giant urticaria, serum sickness, angioneurotic oedema, and anaphylaxis.
The α-agonists are applied topically to induce local vasoconstriction in nasopharyngeal, scleroconjunctival, and otic blood vessels in acute conditions of rhinitis, coryza, nasopharyngitis, sinusitis, conjunctivitis, and hay fever.
By inhalation, α-agonists may be used to suppress bronchial congestion in allergic and asthmatic conditions.
Structural requirements: The structural requirements for α-agonist activity are a phenylethylamine skeleton to which at least two hydroxyl groups are attached; the optimal positions are ring 3- and side chain L-2, but ring 4- and L-2 and ring 3, 4-dihydroxy compounds are active.

22.2.2 β1-Adrenergic Agonists
The β1-receptors are located in the heart. The β1-agonists increase the heart rate, enhance atrioventricular conduction, and increase the strength of the heartbeat. These effects are achieved in part through the activation of the adenylyl cyclase system and intermediation of 3’,5’-cyclic adenosine monophosphate (cAMP). They may be administered by intracardiac injection to restore the heartbeat in cardiac arrest and heart block with syncopal seizures. Sometimes, β1-agonists also are used for their positive inotropic actions in the treatment of acute heart failure and in cardiogenic or other types of shock, in which contractility often is diminished.
22.2.3 β2-Selective Adrenergic Agonists
The β2-receptors are located in the lung and uterus. The β2-agonists relax smooth muscle and induce hepatic and muscle glycogenolysis, also by activating the adenylyl cyclase system and increasing the intracellular levels of cAMP. Thus, they dilate the bronchioles, arterioles in vascular beds which are invested with β2-receptors and veins, and they relax the uterus and intestines.
Some β2-agonists are used as bronchodilators in the treatment of bronchial asthma, emphysema, and bronchitis. They are also used to relax the uterus and delay delivery in premature labour, and to treat dysmenorrhoeal problem.
Structural requirements: The structural requirements include an L-β-OH group, which is essential to both β1 and β2 activity. N-Alkyl substitution enhances both the activities, while isopropyl and t-butyl confer optimal activity. A ring hydroxyl group at the 3- or 4-position is required; the 3-OH appears to be more favourable for β2- and the 4-OH for β1-activity.
22.2.4 Classification of Sympathomimetics
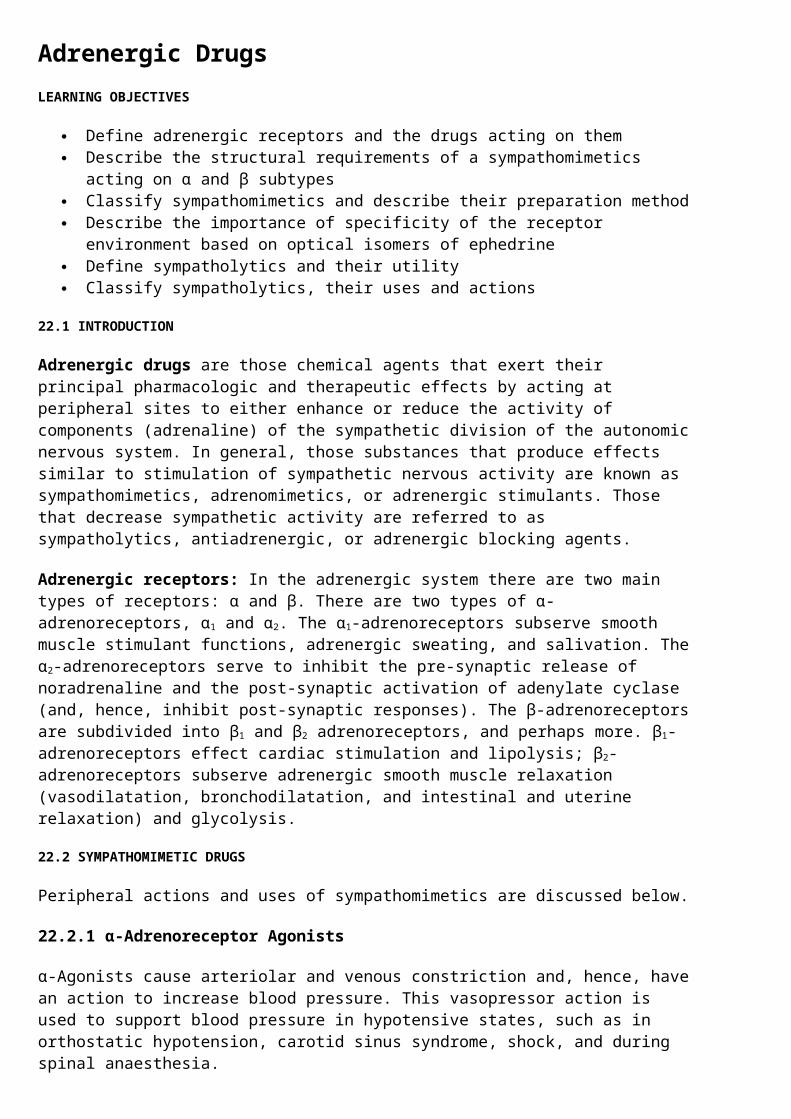
1. Phenylethanolamine derivatives
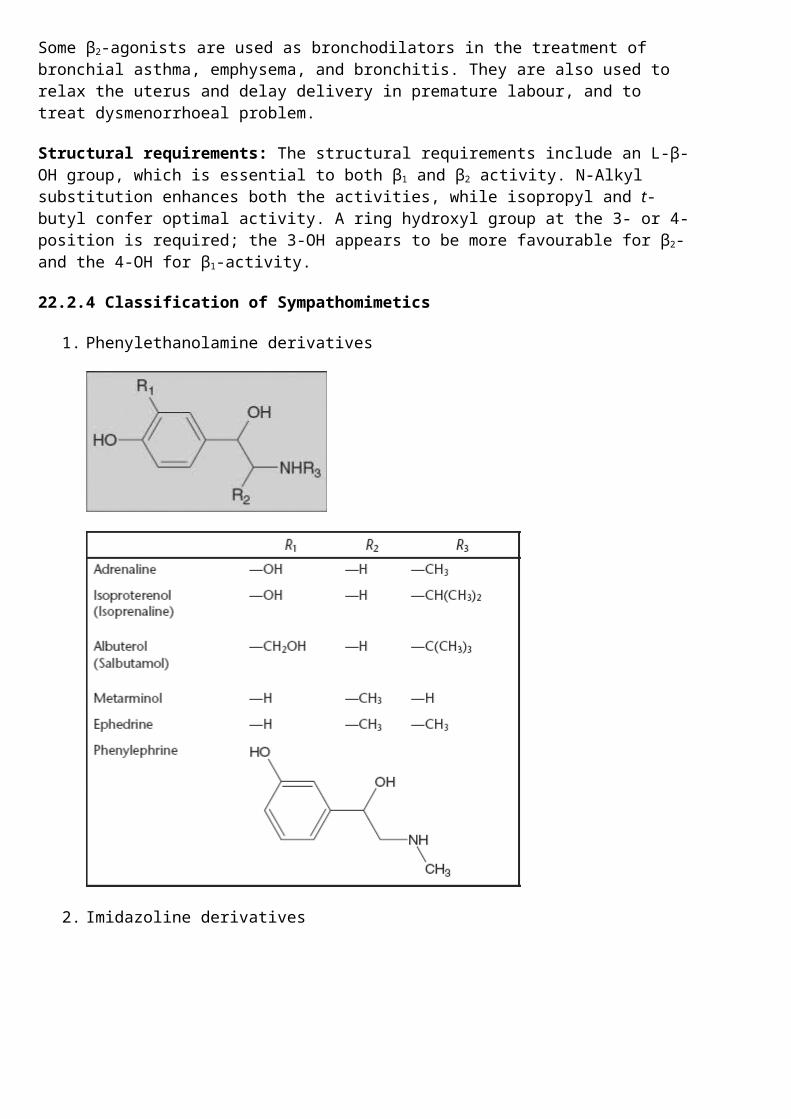
2. Imidazoline derivatives
RXylometazoline
Oxymetazoline
Naphazoline
22.2.5 Phenylethanolamine Derivatives
Adrenaline (-)-3,4-Dihydroxy-α-[(methylamino)methyl] benzyl alcohol
It possesses all of strong α1-, α2-, β1-, and β2-agonist activities. It is the drug of choice in the management of allergic emergencies such as anaphylaxis, angioneurotic oedema, urticaria, and serum sickness.
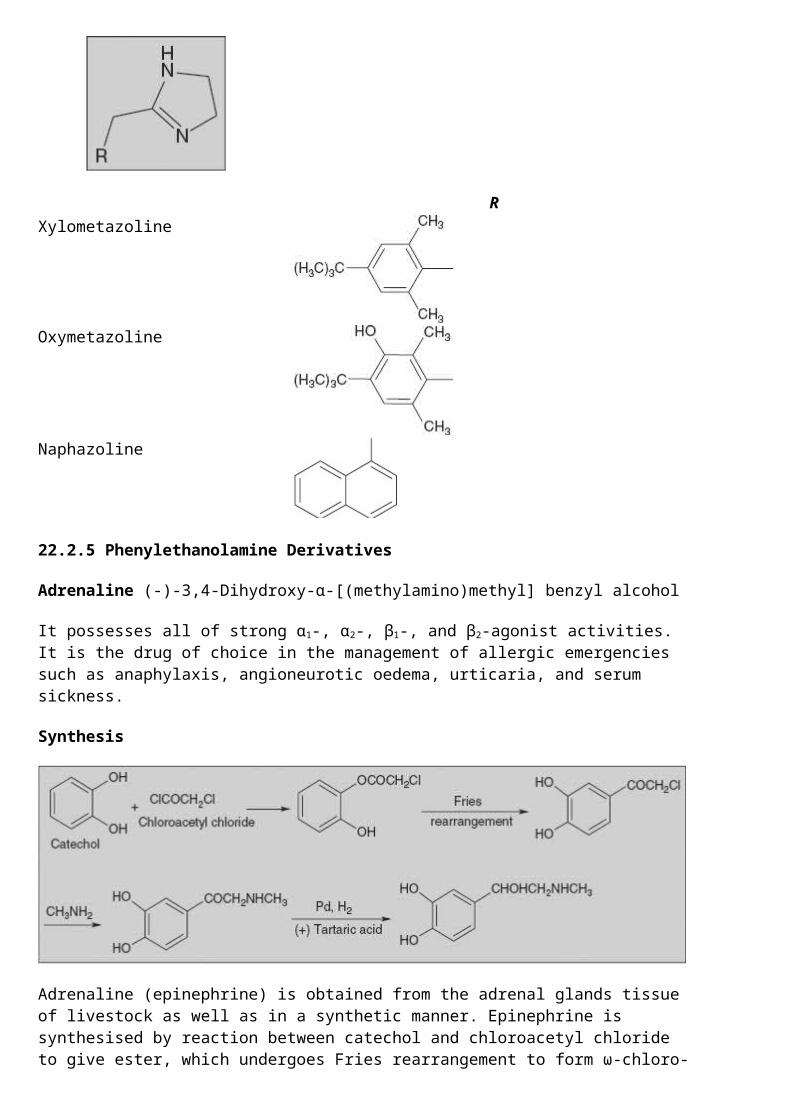
Synthesis
Adrenaline (epinephrine) is obtained from the adrenal glands tissue of livestock as well as in a synthetic manner. Epinephrine is synthesised by reaction between catechol and chloroacetyl chloride to give ester, which undergoes Fries rearrangement to form ω-chloro-3,4-dihydroxyacetophenone. Reaction of this with excess of methylamine gives ω-methylamino-3,4-dihydroxyacetophenone. Reduction of this gives D,L-epinephrine, which is separated into isomers using (-) tartaric acid.
Epinephrine was isolated and identified in 1895 by Napoleon Cybulski, a Polish physiologist. In May 1896, William Bates reported the discovery of a substance produced by the adrenal gland in the New York Medical Journal.
Isoprenaline: 3, 4-Dihydroxy-α-[(isopropylamino)methyl]benzyl alcohol
Preparation: By the synthetic procedure given for adrenaline using isopropylamine in place of methylamine
It has strong β1- and β2-agonist activity but lacks α-activity. Its primary use is in the treatment of bronchial asthma.
Salbutamol: 4-Hydroxy-3-hydroxymethyl-α-[(tert-butylamino)methyl] benzyl alcohol.
Synthesis
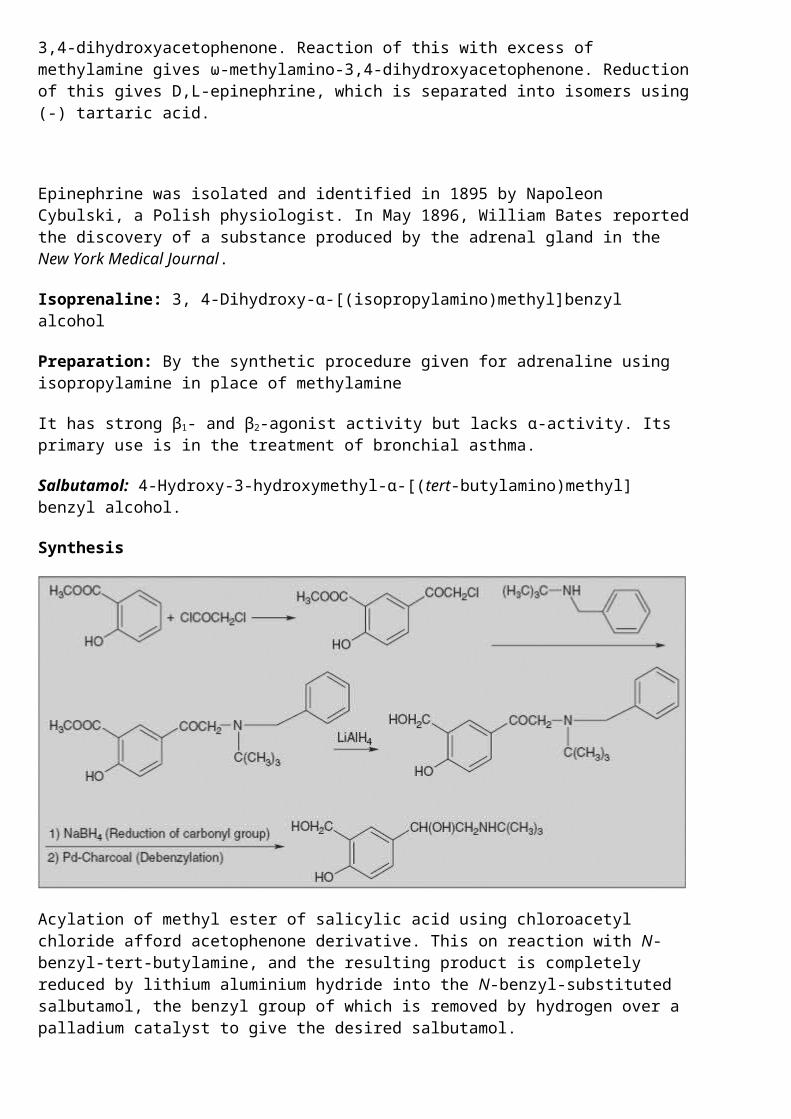
Acylation of methyl ester of salicylic acid using chloroacetyl chloride afford acetophenone derivative. This on reaction with N-benzyl-tert-butylamine, and the resulting product is completely reduced by lithium aluminium hydride into the N-benzyl-substituted salbutamol, the benzyl group of which is removed by hydrogen over a palladium catalyst to give the desired salbutamol.
The therapeutic action and uses of salbutamol are similar to those of isoprenaline.
Metarminol (-)-α-1-Aminoethyl-3-hydroxy benzyl alcohol
Reaction of 4-hydroxy propiophenone with benzyl chloride gives O-benzyl derivative, which on treatment with butyl nitrite undergoes nitrosation reaction at the α-position. Stepwise reduction of the nitrosoketone leads to amino alcohol metarminol.
Phenylephrine (-)-3-Hydroxy-α-[(methylamino)methyl] benzyl alcohol
It is synthesised by an analogous scheme of making epinephrine; however, instead of using ω-chloro-3,4-dihydroxyacetophenone, ω-chloro-3-dihydroxyacetophenone is used.
It has a strong α-agonist and negligible β-agonist activity. It is used in the treatment of paroxysmal supraventricular tachycardia and to support blood pressure.
Ephedrine (-)-Erythro-α-[1-(methylamino)ethyl] benzyl alcohol
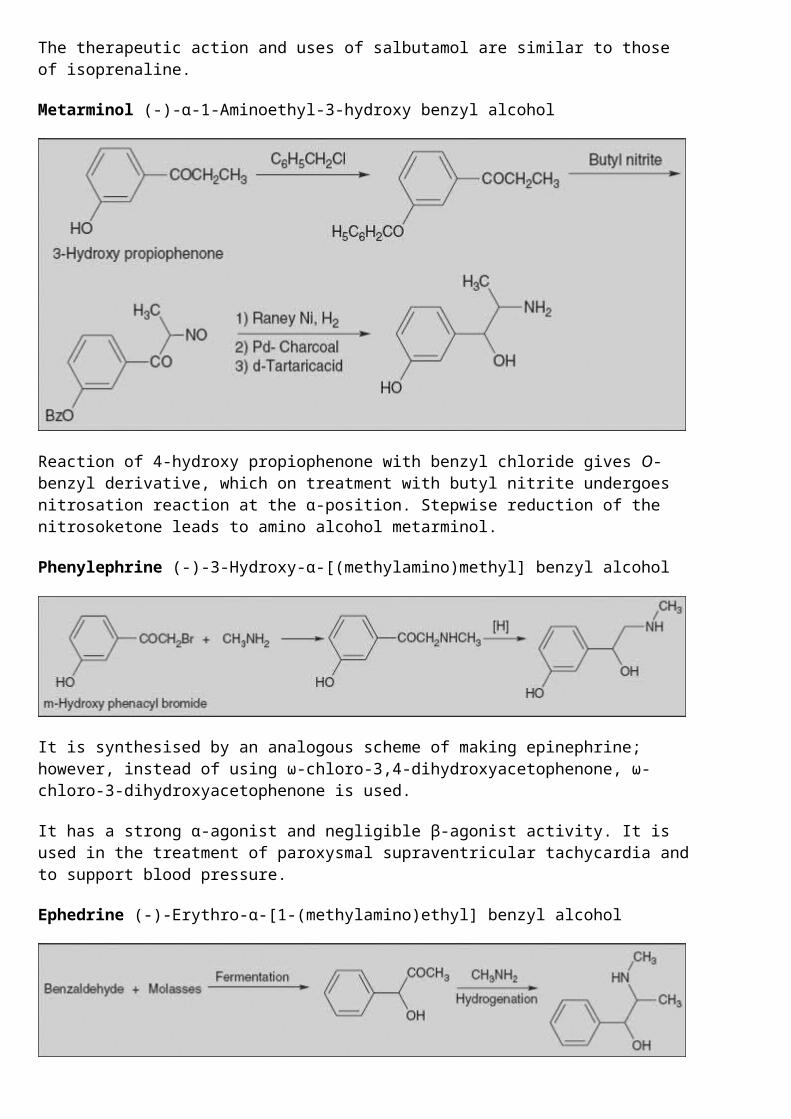
The method consists of the fermentation of glucose by yeast carboligase in the presence of benzaldehyde, which during the process turns into (-)-1-phenyl-2-ketopropanol. This is reduced by hydrogen in the presence of methylamine, to give the desired ephedrine.
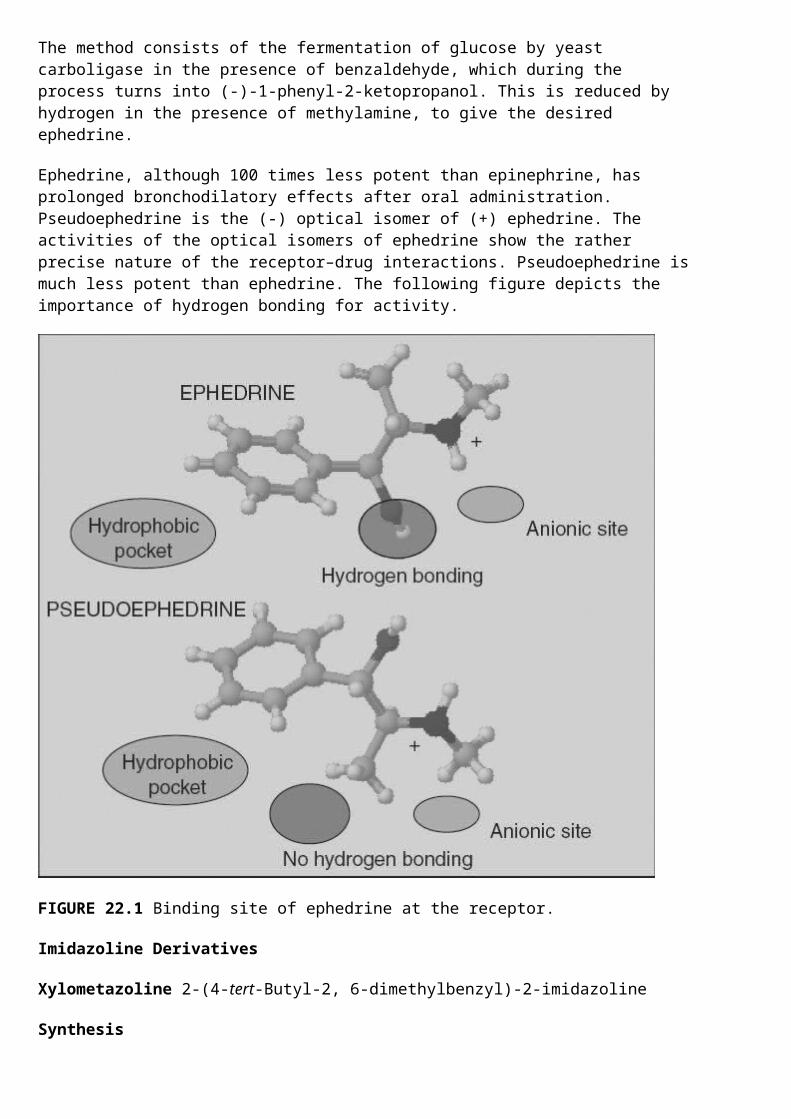
Ephedrine, although 100 times less potent than epinephrine, has prolonged bronchodilatory effects after oral administration. Pseudoephedrine is the (-) optical isomer of (+) ephedrine. The activities of the optical isomers of ephedrine show the rather precise nature of the receptor–drug interactions. Pseudoephedrine is much less potent than ephedrine. The following figure depicts the importance of hydrogen bonding for activity.
FIGURE 22.1 Binding site of ephedrine at the receptor.
Imidazoline Derivatives
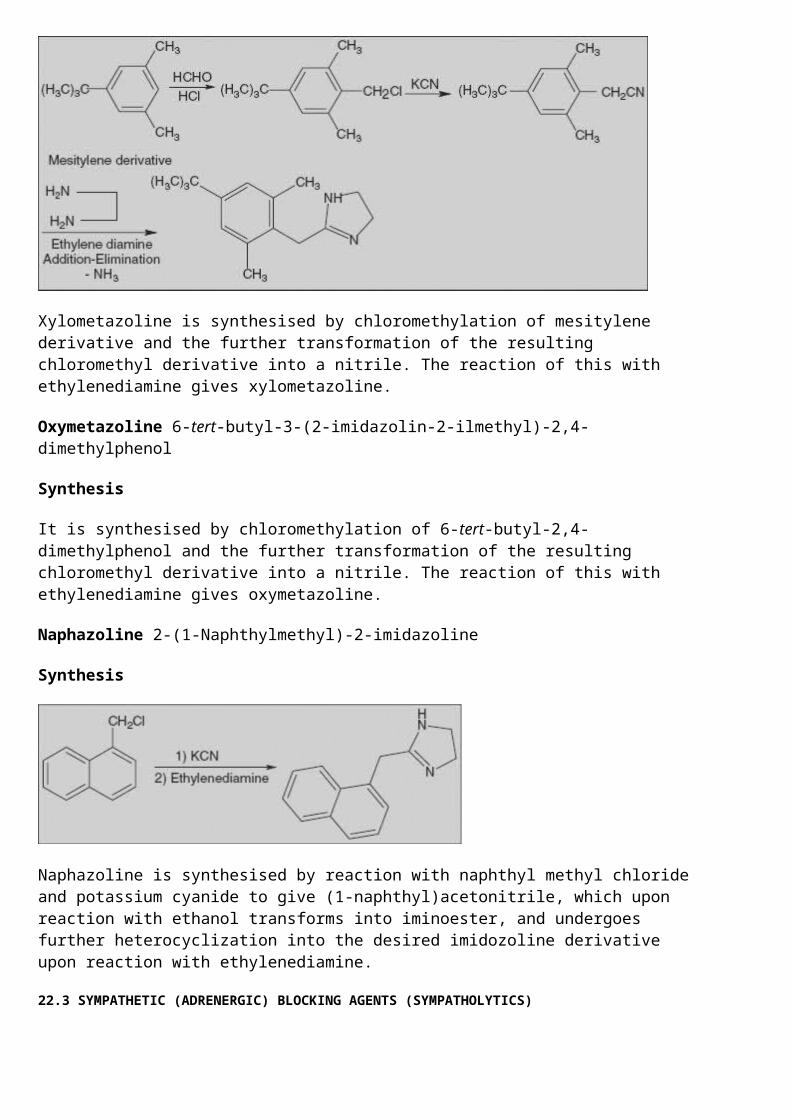
Xylometazoline 2-(4-tert-Butyl-2, 6-dimethylbenzyl)-2-imidazoline
Synthesis
Xylometazoline is synthesised by chloromethylation of mesitylene derivative and the further transformation of the resulting chloromethyl derivative into a nitrile. The reaction of this with ethylenediamine gives xylometazoline.
Oxymetazoline 6-tert-butyl-3-(2-imidazolin-2-ilmethyl)-2,4-dimethylphenol
Synthesis
It is synthesised by chloromethylation of 6-tert-butyl-2,4-dimethylphenol and the further transformation of the resulting chloromethyl derivative into a nitrile. The reaction of this with ethylenediamine gives oxymetazoline.
Naphazoline 2-(1-Naphthylmethyl)-2-imidazoline
Synthesis
Naphazoline is synthesised by reaction with naphthyl methyl chloride and potassium cyanide to give (1-naphthyl)acetonitrile, which upon reaction with ethanol transforms into iminoester, and undergoes further heterocyclization into the desired imidozoline derivative upon reaction with ethylenediamine.
22.3 SYMPATHETIC (ADRENERGIC) BLOCKING AGENTS (SYMPATHOLYTICS)
Adrenergic blocking agents are drugs that produce their pharmacologic effects primarily by preventing the release of noradrenaline from sympathetic nerve terminals.
These drugs produce their effects by stabilization of the neuronal membrane or the membranes of the storage vesicles. This stabilization makes the membranes less responsive to nerve impulses, thereby inhibiting the release of noradrenaline into the synaptic cleft.
22.3.1 Classification, Action, and Uses
α-Adrenergic Antagonists
1. Non-selective α-antagonists: Examples: Phenoxybenzamine, Phentolamine, Tolazoline
This class produces α1 and α2 blockade. Antagonism of α1-adrenergic impulses to the arterioles decreases vascular resistance, thus tending to lower the blood pressure, and causes a pink warm skin and nasal and scleroconjunctival congestion. α-Antagonism causes tachycardia, palpitations, and increased secretion of renin. They are used in the treatment of peripheral vascular disorders such as Raynaud’s disease, acrocyanosis, frostbite, acute arteriolar occlusion, causalgia, and pheochromocytoma.
2. Selective α-antagonists: Theoretically, α1-blockers (prazosin and terazosin) should be useful for the same disorders as are the non-selective α-blockers, but they are approved only for the treatment of hypertension.
Selective α2-antagonists include yohimbine and rauwolscine, but there are presently no therapeutic application of α2-blockade.
β-Adrenergic Antagonists
1. Non-selective β-antagonists: Drugs such as Propranolol, Nadolol, Pindolol, and Timolol suppress both β1- and β2-adrenoreceptor-mediated responses almost equally. Blockade of myocardial β1-receptors causes sinoatrial bradycardia, decreased force of myocardial contraction, slowing of atrioventricular conduction, and increased atrioventricular refractoriness.
Uses
o β-Blockers are of prophylactic value in the treatment of stable angina pectoriso The effect to decrease sinoatrial rate is also used to suppress tachycardia in
thyrotoxicosis and pheochromocytomao The effect to decrease atrioventricular nodal conduction is employed in the chronic
management of paroxysmal supraventricular tachycardiao All available β-antagonists are used in the treatment of hypertensiono β-Antagonists have usefulness in the prophylaxis of migraine headache
2. Selective β1-antagonists: Examples: Acebutolol, Atenolol, Metoprolol, Practolol, and Tolamol
Selective β1-antagonists can be used for all the purposes listed under the non-selective blockers. Advantages to selective β1-blockade are lesser effect on bronchiolar airway resistance and diminished effect to increase insulin-induced hypoglycaemia.
3. Partial agonist β-antagonist: Examples: Oxprenolol, Acebutolol, and Pindolol
It also causes some stimulation of β-adrenoreceptors. This partial agonism acts as buffer to lessen the seriousness of the various adverse effects attributable to β-blockade.
22.3.2 Synthesis of α-adrenergic Blockers
Phenoxybenzamine N-(2-Chloroethyl)-N-(1-methyl-2-phenoxyethyl)benzylamine
Phenoxybenzamine is synthesised by reacting phenol with propylene chlorohydrin, which forms 1-phenoxy-2-propanol, the chlorination of which with thionyl chloride gives 1-phenoxy-2-propylchloride. Reacting this with 2-aminoethanol leads to formation of 1-phenoxy-2-(2-hydroxyethyl)aminopropane. Alkylation of the secondary amino group gives N-(2-hydroxyethyl)-N-(1-methyl-2-phenoxyethyl)benzylamine, the hydroxyl group of which is chlorinated using thionyl chloride, giving phenoxybenzamine.
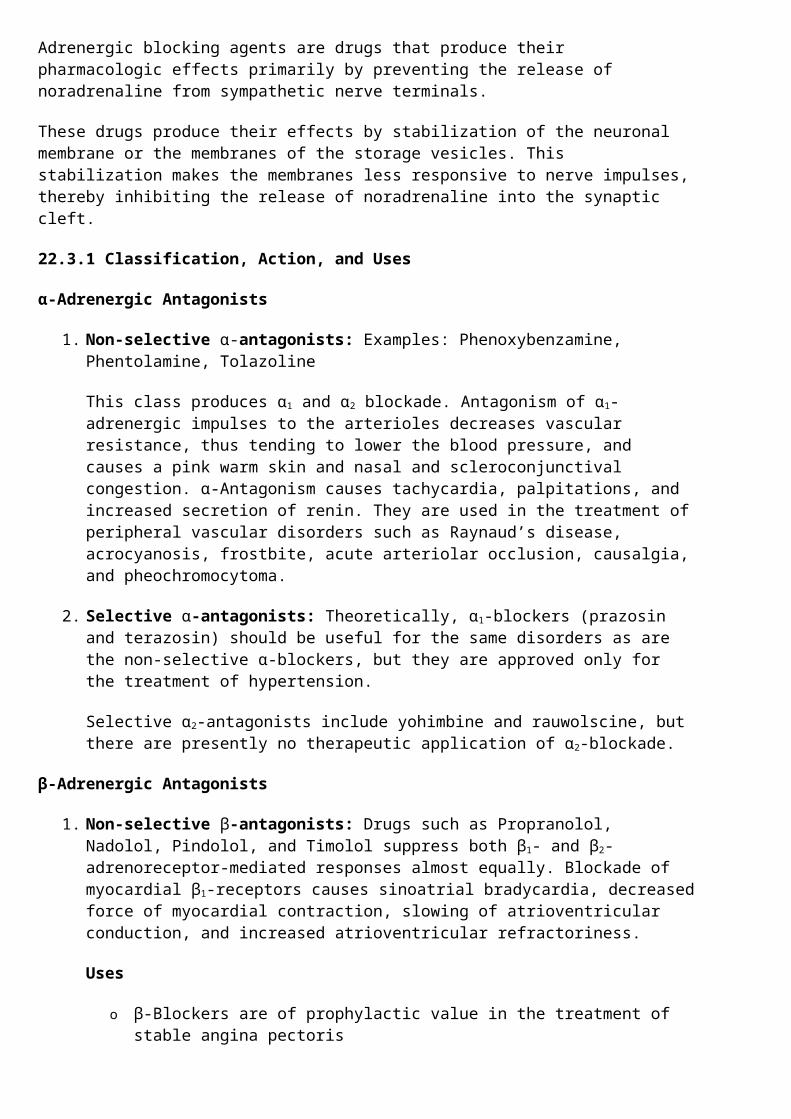
Phentolamine 3-[[(4,5-Dihydro-1H-imidazol-2-yl)methyl](4-methyl-phenyl)amino]phenol
Chlormethylation of diphenylamine is followed by further transformation of the resulting chloromethyl derivative into a nitrile. The reaction of this with ethylenediamine gives phentolamine.
Tolazoline 2-Benzyl-2-imidazoline

Tolazoline is synthesised by the heterocyclation of the ethyl ester of iminophenzylacetic acid with ethylenediamine, which forms the desired tolazoline.
(Synthesis of prazosin and terazosin was discussed in Chapter 16 on ‘Antihypertensive Agents’.)
(For synthesis of β-Adrenergic blockers, refer to Chapter 16 on ‘Antihypertensive Agents’.)
22.4 NEWER DRUGS
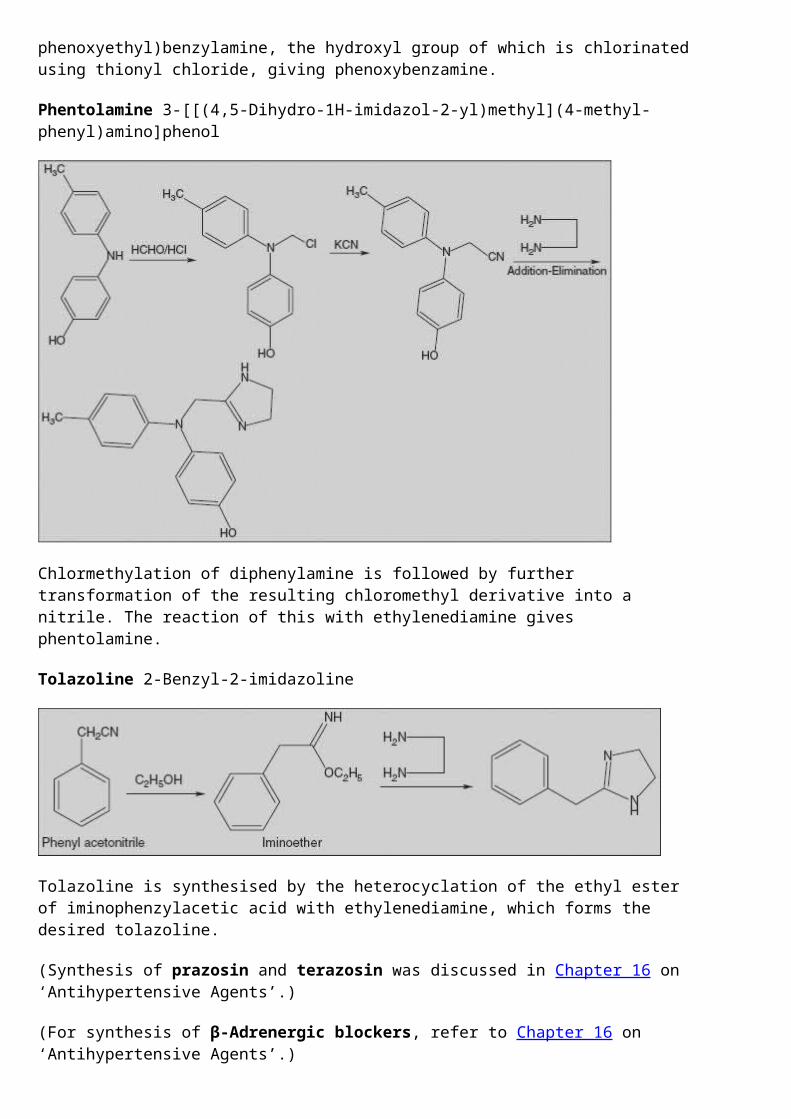
Clenbuterol 1-(4-Amino-3,5-dichlorophenyl)-2-(tert-butylamino)ethanol
It is a drug prescribed to sufferers of breathing disorders as a decongestant and bronchodilator. Clenbuterol is a β2-adrenergic agonist with some similarities to ephedrine, but its effects are more potent and longer lasting as a stimulant and thermogenic drug.
Salmeterol 2-(Hydroxymethyl)-4-{1-hydroxy-2-[6-(4-phenylbutoxy)hexylamino]ethyl}phenol
It is a long-acting β2-adrenergic receptor agonist drug that is currently prescribed for the treatment of asthma and chronic obstructive pulmonary disease (COPD).
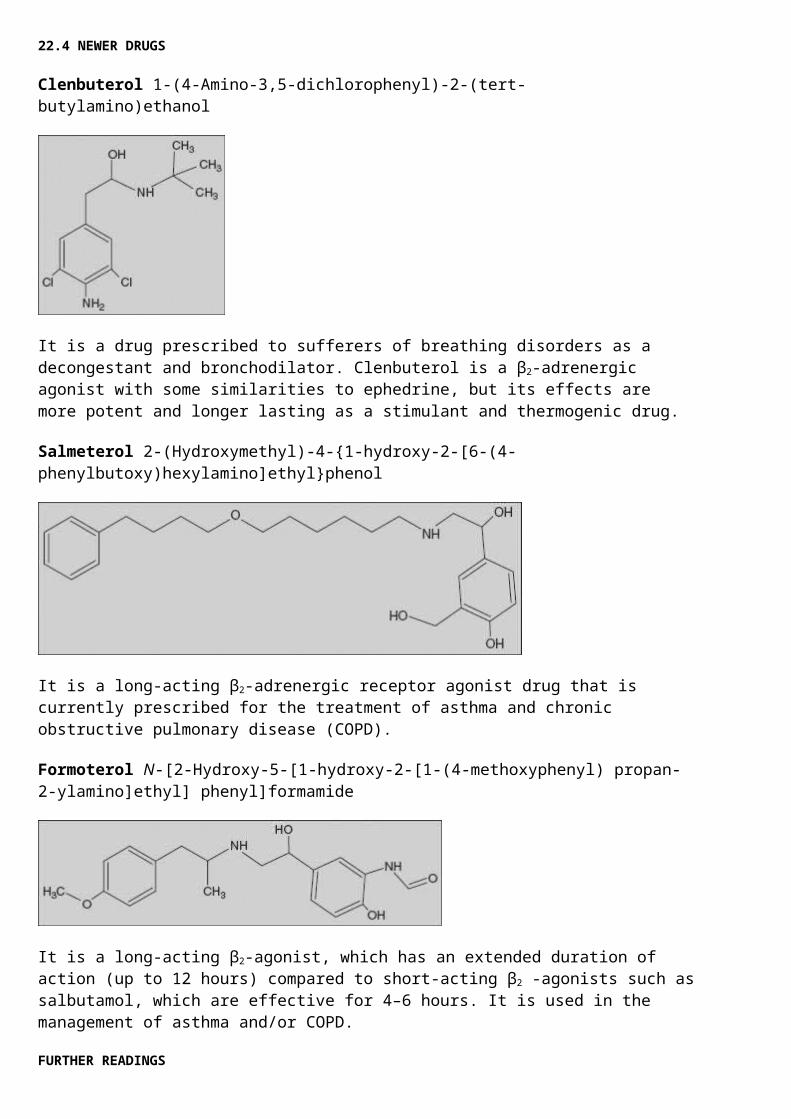
Formoterol N-[2-Hydroxy-5-[1-hydroxy-2-[1-(4-methoxyphenyl) propan-2-ylamino]ethyl] phenyl]formamide
It is a long-acting β2-agonist, which has an extended duration of action (up to 12 hours) compared to short-acting β2 -agonists such as salbutamol, which are effective for 4–6 hours. It is used in the management of asthma and/or COPD.
FURTHER READINGS
1. Choudhary, M. Iqbal, 1996. Progress in Medicinal Chemistry, Taylor & Francis (UK).
2. Silverman, Richard B., 2004. The Organic Chemistry of Drug Design and Drug Action, Elsevier.
MULTIPLE-CHOICE QUESTIONS
1. β-Adrenergic blockers are not used for 1. Migraine headache2. Hypertension3. Angina pectoris4. Supra-ventricular bradycardia
2. Pindolol is a (an) 1. α1-Agonist2. β1-Agonist3. β1-Partial agonist antagonist4. α1-Partial agonist antagonist
3. Propanolol is useful for 1. Asthma2. Ventricular tachycardia3. Anaesthesia4. Atropine poison
4. The β1-receptors are located in 1. Heart2. Lungs3. Kidney4. Adrenal gland
5. Orthostatic hypotension is treated with 1. β-Blockers2. β-Agonists3. α-Blockers4. α-Agonists
6. Drug of the following class is useful in the treatment of asthma: 1. β1-Blockers2. β1-Agonists3. α1-Blockers4. α1-Agonists
7. The adrenergic agent obtained by fermentation procedure is 1. Propanolol2. Adrenaline3. Ephedrine4. Phenylephrine
8. 3, 4-Dihydroxy-α-[(isopropylamino)methyl]benzyl alcohol is
1. Adrenaline2. Propanolol3. Phenylephrine4. Isoprenaline
9. 3-[[(4,5-Dihydro-1H-imidazol-2-yl)methyl](4-methyl-phenyl)amino]phenol is 1. Phentolamine2. Tolazoline3. Naphazoline4. Phenoxybenzamine
10. Salbutamol is synthesised starting from 1. Phenyl acetonitrile2. Methyl salicylate3. 4-Hydroxy propiophenone4. Mesitylene derivative
QUESTIONS
1. Classify sympathomimetics and discuss their therapeutic uses.2. With the structure of epinephrine, discuss the design of agonists and antagonists based on the
structural modification.3. Write the synthetic scheme for salbutamol, isoprenaline, phentolamine, and ephedrine.4. Classify antiadrenergic drugs with structural examples.5. Write a short note on the therapeutic uses of β-blockers.
SOLUTION TO MULTIPLE-CHOICE QUESTIONS
1. d; 4. b; 7. c; 10. b.2. c; 5. d; 8. d; 3. b; 6. b; 9. a;