-
to
People and Plants Initiative,
Division of Ecological Sciences,
UNESCO, 7 Place de Fontenoy,
75352 Paris CEDEX 07 SP, France.
This series of working papers
is intended to provide information and
to generate fruitful
discussion
on key issues
in the sustainable
and equitable use
of plant resources.
Please
send comments
on this paper
and suggestions
for future
issues
1
-
Published in 1993 by the United Nations Educational, Scientific
and Cultural Organization,7 Place de Fontenoy, 75352 Paris CEDEX 07
SP.
Printed by UNESCO Presse on chlorine-free recycled paper.
Series editor: Alison SempleDesign and layout: Ivette
FabbriSuggested citation: Cunningham, A.B. (1993). African
medicinal plants: setting priorities at the interface between
conservation and primary health care. People and Plants working
paper 1. Paris. UNESCO.
Author's address:A.B. Cunningham84 Watkins Street - White Gum
Valley, Fremantle 6162Western Australia - Australia
The designations employed and the presentation of material
throughout this publication do notimply the expression of any
opinion whatsoever on the part of UNESCO concerning the legal
statusof any country, territory, city, or area of its authorities,
or concerning the delimitation of its frontiersor boundaries. The
opinions expressed in this paper are entirely those of the author
and do notcommit any Organization.
-
Sustainable management of traditional medici-nal plant resources
is important, not onlybecause of their value as a potential source
ofnew drugs, but due to reliance on traditionalmedicinal plants for
health. The vast majority(70-80%) of people in Africa consult
traditionalmedical practitioners (TMPs) for healthcare.With few
exceptions, traditional medicinalplants are gathered from the wild.
Althoughreliance on TMPs may decline in the long termas alternative
healthcare facilities becomeavailable, increasing demand for
popular herbalmedicines is expected in the foreseeable future.Over
the same period, certain vegetation typesthat were sources of
supply of traditional med-icines will drastically decline due to
forestclearance for agriculture, afforestation of mon-tane
grasslands, uncontrolled burning and live-stock grazing. Exclusion
from core conserva-tion areas adversely affects TMPs who
previ-ously gathered medicinal plants in those sites.In addition,
supplies of herbal medicines toTMPs are affected by competing
resource usessuch as timber logging, commercial harvestingfor
export and extraction of pharmaceuticals,and use for building
materials and fuel. Thiscreates a growing demand for fewer
resources,in some cases resulting in local disappearanceof favoured
and effective sources of tradition-al medicine and reduced species
diversity.
The most vulnerable species are popular,slow growing or slow to
reproduce, or specieswith specific habitat requirements and a
limit-ed distribution. Although in theory, sustainable
use of bark, roots or whole plants used as herbalmedicines is
possible, the high levels of moneyand manpower required for
intensive manage-ment of slow growing species in multiple-species
systems are unlikely to be found in mostAfrican countries. The
cultivation of alterna-tive sources of supply of popular, high
conser-vation priority species outside of core conser-vation areas
is therefore essential. However,commercial cultivation of such
species is not asimple solution and at present is unlikely to
beprofitable due to the slow growth rates formost tree species and
low prices paid for tra-ditional medicines. These slow growing
speciesare a priority for ex situ conservation and strictprotection
in core conservation areas. By con-trast, the high price paid for
some species doesmake them potential new crop plants for
agro-forestry systems (e.g. Warburgia salutaris,Garcinia kola, G.
afzelii, G. epunctata) or agri-cultural production (e.g.
Siphonochilusaethiopicus). Pilot studies on these species
areneeded.
Priority areas for cooperative actionbetween healthcare
professionals and conser-vationists are rapidly urbanizing regions
witha high level of endemic taxa, particularly westAfrica
(Guineo-Congolian region), specificallyCte dIvoire, Ghana, and
Nigeria; east Africa(Ethiopia, Kenya, Tanzania);
south-easternAfrica (South Africa, Swaziland). The mostthreatened
vegetation types are Afro-montaneforest and coastal forests of the
Zanzibar-Inhambane regional mosaic.
African medicinal plantsSETTING PRIORITIES AT THE INTERFACE
BETWEEN CONSERVATION AND PRIMARY HEALTHCARE
Abstract
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
ContentsAbstract ContentsIntroduction
The role of traditional medical practitionersCustomary controls
on medicinal plant gatheringDynamics of the commercial trade
Domestic tradeInternational trade
The impact of the trade in medicinal plantsSustainable supplies
of traditional medicinesSustainability of chewing stick
harvestingSupplying international trade
The real price of tradeThe reasons for concernFocus of
management effortConditions for cultivation as an alternative
source of supply
Key issuesConservation strategyPolicy recommendations
International and national policySharing the costsConservation
methods
In-situ conservationBuffer zones and ex-situ conservation
Buffer zonesTraditional medical practitionersConservation
through commercial cultivationBotanical gardens and field gene
banksOther recommendations
Education and trainingResearch and monitoring
AcknowledgementsPersonal communicationsReferencesAppendix 1:
African medicinal plants observed in trade Appendix 2: Plant
species mentioned in text
!
"#
-
African medicinal plants: setting priorities at the
interfacebetween conservation and primary healthcare
"
If there is to be any real improvement in thehealth of the
under-served populations of theworld, then there will have to be
full utiliza-tion of all available resources, human and mate-rial.
This is fundamental to the primary health-care approach.
Traditional medical practition-ers constitute the most abundant and
in manycases, valuable health resources present in thecommunity.
They are important and influentialmembers of their communities who
should beassociated with any move to develop health ser-vices at a
local level.
Akerele (1987)
First the unukane (Ocotea bullata) trees werekilled by
ring-barking for sale in the cities. Nowthe same is happening to
igejalibomvu (Curtisiadentata) and umkhondweni (Cryptocarya
myr-tifolia) trees. Soon they will be gone as welland we will have
to buy the barks from theherb traders.
Herbalist, Nkandla forest, Natal, South Africa, 1987
The populations of developing countriesworldwide continue to
rely heavily on the useof traditional medicines as their primary
sourceof healthcare. Ethnobotanical studies carriedout throughout
Africa confirm that native plantsare the main constituent of
traditional Africanmedicines (Adjanohoun et al . , 1980;Adjanohoun
et al., 1984; Adjanohoun et al.,1985; Adjanohoun et al., 1986;
Adjanohoun etal., 1988; Ake Assi, 1988; Ake Assi et al.,1981;
Hedberg, et al., 1982; Hedberg et al.,1983a; Hedberg et al., 1985b;
Kokwaro, 1976;Oliver Bever, 1987). With 70-80% of Africaspopulation
relying on traditional medicines, theimportance of the role of
medicinal plants inthe healthcare system is enormous.
Medicinalplants are now being given serious attention,as is
evidenced by the recommendation givenby the World Health
Organization in 1970(Wondergem et al., 1989) that proven
tradi-tional remedies should be incorporated withinnational drug
policies, by recent moves towardsa greater professionalism within
Africanmedicine (Last and Chavunduka, 1986) and alsoby the
increased commercialization of phar-
Introduction
maceutical production using traditionalmedicinal plants with
known efficacy(Sofawara, 1981).
Little attention however, has been paid tothe socio-economic and
conservation aspects ofmedicinal plant resources, probably due to
therelatively small volumes involved and the spe-cialist nature of
the informal trade in them.However, the management of traditional
med-icinal plant resources is probably the most com-plex African
resource management issue fac-ing conservation agencies, healthcare
profes-sionals and resource users. As pressure isincreasing on
diminishing medicinal plant sup-plies, constructive resource
management andconservation actions must be identified, basedupon a
clear understanding of the surroundingmedicinal plant use.
This study seeks to respond to three cen-tral questions:(1) What
are the causes behind the depletion
of wild populations of medicinal plantspecies in Africa?
(2) Which species are of particular concernand should be given
priority for positiveaction?
(3) What can be done to ensure the effectiveconservation of all
medicinal plantspecies?
An explanation of the present situation in thefirst section
(Medicinal plant use in Africa)illustrates the urgent need for
action. Theactions required to alleviate problems and anassessment
of priorities for medicinal plant con-servation and resource
management are dis-cussed in the second section (Policy
prioritiesin conservation and primary healthcare).The study is
based on research and literaturesurveys, correspondence with other
researchers,field visits to establish contact with
traditionalmedical practitioners (TMPs) and herbalists andvisits to
Cte dIvoire, Malawi, Mozambique,Swaziland, Zambia and Zimbabwe in
1990.
I have chosen not to make distinctionsbetween plant species with
symbolic or psy-chosomatic uses and those with active ingredi-ents
in this study, the main issue being whetheror not a species is
threatened.
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
Medicinal plant use in Africa
$$
In contrast with western medicine, whichis technically and
analytically based, tradition-al African medicine takes a holistic
approach:good health, disease, success or misfortune arenot seen as
chance occurrences but are believedto arise from the actions of
individuals andancestral spirits according to the balance
orimbalance between the individual and the socialenvironment
(Anyinam, 1987; Hedberg et al.,1982; Ngubane, 1987; Staugard, 1985;
WHO,1977). Traditionally, rural African communitieshave relied upon
the spiritual and practical skillsof the TMPs (traditional
medicinal practition-ers), whose botanical knowledge of
plantspecies and their ecology and scarcity areinvaluable.
Throughout Africa, the gathering ofmedicinal plants was
traditionally restricted toTMPs or to their trainees (Photo 1).
Knowledgeof many species was limited to this groupthrough spiritual
calling, ritual, religious con-trols and, in southern Africa, the
use of alter-native (hlonipha) names not known to outsiders.
Hedberg et al., (1982) observed that thenumber of traditional
practitioners in Tanzaniawas estimated to be 30 000 - 40 000 in
com-parison with 600 medical doctors (Table 1) (MPand TMP : total
population ratios were notgiven). Similarly, in Malawi, there were
an esti-mated 17 000 TMPs and only 35 medical doc-tors in practice
in the country (Anon., 1987).
Economic and demographic projections formost African countries
offer little grounds foroptimism. A shift from using traditional
medi-cines to consulting medical doctors, even if theyare
available, only occurs with socio-economicand cultural change,
access to formal education(Kaplan, 1976) and religious influences
(e.g.through the African Zionist movements, whichforbid the use of
traditional medicines by theirfollowers, substituting the use of
ash and holywater instead; Sundkier, 1961). Access to west-ern
biomedicine, adequate education andemployment opportunities
requires economicgrowth. Unfortunately, most African countries
are affected by unprecedented economic deteri-oration. Per
capita income has reportedly fall-en by 4% since 1986, whilst
Africas foreigndebt is three times greater than its export
earn-ings. In Zambia, government spending on edu-cation has fallen
by 62% in the last decade, andthat on essential pharmaceutical
drugs by 75%from 1985 to 1989 (Zimbabwe Science News,1989). At the
same time, the African popula-tion has grown by 3% per annum,
increasingthe difficulty of adequate provision of Western-type
health services. For this reason, there is aneed to involve TMPs in
national healthcaresystems through training and evaluation
ofeffective remedies, as they are a large and influ-ential group in
primary healthcare (Akerele,1987; Anyinam, 1987; Good, 1987).
Sustainableuse of the major resource base of TMPs - med-icinal
plants - is therefore essential.
The sustainable use of medicinal plants wasfacilitated in the
past by several inadvertent orindirect controls and some
intentional manage-ment practices.
Taboos, seasonal and social restrictions ongathering medicinal
plants, and the nature ofplant gathering equipment all served to
limitmedicinal plant harvesting. In southern Africa(and probably
elsewhere) before metalmachetes and axes were widely available,
plantswere collected with a pointed wooden diggingstick or small
axe, which tended to limit thequantity of bark or roots gathered.
For exam-ple, traditional subsistence harvesting ofCassine
papillosa bark causes relatively littledamage to the tree (Figure
1). Pressure on med-icinal plant resources has remained low
inremote areas and in countries such asMozambique and Zambia where
the commer-cial trade in traditional medicines has onlydeveloped to
a limited extent due to the small
-
African medicinal plants: setting priorities at the
interfacebetween conservation and primary healthcare
#
Photo 1.Trainee diviner
(twasa) with a small
quantityof Boophane
disticha(Amaryllidacea
e) bulbs for local
use.
size of major urban centres. Examples of fac-tors which have
limited pressure on specieswhich would otherwise be vulnerable to
over-exploitation include:
(1) Taboos against the collection of med-icinal plants by
menstruating women in SouthAfrica and Swaziland; it is believed
that thiswould reduce the healing power of the plants(Scudder and
Conelly, 1985).
(2) The tendency in southern Africa forwomen to practise as
diviners, while men prac-tise as herbalists (Berglund, 1976;
Staugard,1985). This limits the number of resource users.
(3) The perceived toxicity of some medi-cinal species which
reduced their use in thepast: the level of toxicity is sometimes
givenmythical proportions. Synadenium cupulare forexample, is
considered so toxic that birds fly-ing over the tree are killed;
special ritual prepa-rations are made in west Africa before the
barkof Okoubaka aubrevillei is removed (Good,1987).
(4) The traditional use of a wooden bat-ten for removal of bark
from Okoubaka aubre-villei - under no circumstances may a macheteor
other metal implement be used (Good, 1987).
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
%
For any society to institute intentionalresource management
controls, certain condi-tions have to be fulfilled:
(1) the resource must be of value to thesociety;
(2) the resource must be perceived to bein short supply and
vulnerable to over-exploita-tion by people;
(3) the socio-political nature of the soci-ety must include the
necessary structures forresource management.
Intentional resource management controlshave endured in Africa
in various forms andfor various reasons and some have affected
theabundance and availability of medicinalspecies. The widespread
practice in Africa ofconserving edible wild fruit-bearing trees
fortheir fruits or shade also ensures availability ofsome
traditional medicines as several are mul-tiple-use species. For
example the following sixtrees are conserved for their fruit:
Irvingiagabonensis and Ricinodendron heudelotii inwest Africa
(barks are used for diarrhoea anddysentery); from southern Africa
Trichiliaemetica (enemas), Parinari curatellifolia (con-stipation
and dropsy), Azanza garkeana (chest
pains), and Sclerocarya birrea (diarrhoea).Albizia
adianthifolia, used for enemas, is con-served for its shade.
Protection of vegetation at grave sites, forreligious and
spiritual reasons, is a commonfeature in many parts of Africa
(includingKenya, Malawi, South Africa and Swaziland)and an
important means through which bioticdiversity is maintained outside
core conserva-tion areas. In south-eastern Africa during
thenineteenth century, specific Zulu regimentswere called up
annually to burn fire-breaksaround the grave sites of Zulu kings:
thesewoodland or forested sites were considered tobe a sanctuary
for game animals (Webb andWright, 1986). An important feature of
vege-tation conservation around grave sites is thatthis practice is
maintained even under high pop-ulation densities and tremendous
demand forarable land, for example in Malawi. The prac-tice might
possibly be strengthened through theburial of prominent leaders in
conservationareas.
Religious beliefs have also helped to ensurecareful harvesting
of Helichrysum kraussii, anaromatic herb known as impepho in Zulu
whichis widely burnt as an incense in Natal. Diviners
!"!#$% !&'% ()$( !&$"*"+&%'% (%!(!$"!!)!), !&
& "(%#$ (&(!,&$ "
&'($)* $+$&$,& -+$&$,& )./.).(.
! "#!! $%&'&()*
+)+(+,%+- . /0#! 1(%*#
2+3&41%5 66# 6!"6/ +7*#
8
%'+9+3+%: * *0 ))4*0
&%+(9(&-&: #"#/ 0!!!! ;+7(+(31&*0
-
African medicinal plants: setting priorities at the
interfacebetween conservation and primary healthcare
0
are careful not to rip the plant out by its roots(Cooper,
1979).
In Swaziland and South Africa, taboos alsorestrict the seasonal
(summer) collection ofAlepidea amatymbica roots,
Siphonochilusaethiopicus and Agapanthus umbellatus rhi-zomes. In
each case, collection is restricted tothe winter months after seed
set as summergathering is believed to cause storms and light-ning.
In Zimbabwe, clearance has to be obtainedfrom ancestral spirits
before entering certainforests where Warburgia salutaris occurs.
Ineach of the above cases (excepting Agapanthusumbellatus), the
species concerned are popular,scarce and effective. These
intentional conser-vation practices may be due to the
century-oldhistory of trade in these plants in the southernAfrican
region.
Government legislation has played a large-ly ineffective role in
controlling the use of med-icinal plants in Africa. Under colonial
admin-istration, religious therapy systems practised bydiviners
were equated with witchcraft and leg-i s l a t e d a g a i n s t a
l m o s t e v e r y w h e r e(Cunningham, 1990; Gerstner, 1938;
Staugard,1985). In South Africa (and possibly other partsof Africa)
during the colonial era, there werealso attempts to prohibit the
sale of traditionalmedicines within urban areas, such as theefforts
made by the Natal PharmaceuticalSociety in the 1930s in Durban,
South Africa.Apart from having the temporary effect of dri-ving
informal sector plant sellers and TMPs
underground, this kind of legislation has beenineffective in
reducing traditional medicine use.Attempts to suppress traditional
medicine arenot, however, solely restricted to the colonialera: in
post-independence Mozambique, forexample, diviners involved in
symbolic ormagico-medicinal aspects of traditional medi-cine were
sent to re-education camps in aneffort to do away with
obscurantism(Adjanohoun et al., 1984).
Although forest legislation in most Africancountries generally
recognizes the importanceof customary usage rights (including
gatheringof dead-wood for fuel, felling poles and gath-ering latex,
gums, bark resins, honey and med-icinal plants) conservation land
or certain plantspecies are often set aside for strict
protection(Schmithusen, 1986). In South Africa, forexample,
forestry legislation was promulgatedin 1914 for the protection of
economicallyimportant timber species such as Ocotea bul-lata.
Specially protected status has been givensince 1974 to all species
within the familiesLiliaceae, Amaryllidaceae and Orchidaceae dueto
their prominence in the herbal medicinetrade.
At best, this legislation has merely sloweddown the rate of
harvesting. Extensive exploita-tion within forest reserves still
occurs in SouthAfrica. One of the main reasons for this is
thatlegislation for core conservation areas (CCAs)in the past has
concentrated on a holdingaction to maintain the status quo and
neglected
Figure 1. Assessment of debarking damage to Cassine papillosa
(Celastraceae) trees in an area where subsistence harvesting rather
than commercialexploitation is taking place (Cunningham, 1988a)
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
1
to provide local communities with viable alter-natives to
collecting customary plants.
--
If effective action is to be taken to dealwith the
over-exploitation of medicinal plants,there has to be a clear
understanding of thescale and complexity of the problem.
--
Africa has the highest rate of urbanizationin the world, with
urban populations doublingevery 14 years as cities grow at 5.1%
each year(Huntley et al., 1989). In rural areas through-out Africa,
wild plant resources fulfill a widerange of basic needs and are a
resource baseharvested for informal trade or barter, whereasin
urban areas, a much smaller range of speciesand uses is found. In
rural areas of theMozambique coastal plain for example, 76 edi-ble
wild plant species are used (Cunningham,1988a) but only five
species are sold in urbanmarkets in Maputo. Urbanization results in
thisgeneral reduction in the number of species andthe quantities of
certain wild plant resourcesused as people enter the cash economy,
andalternative foods, utensils and building materi-als become
available. However, informal sec-tor trade in two categories of
wild plantresources continues to be very important inmany cities:
fuelwood (alternative energysources such as electricity, gas and
paraffin arenot available or affordable; Eberhard, 1986;Farnsworth,
1988) and medicinal plants.
The range of commercially sold medicinalspecies in southern
Africa remains wide despiteurbanization (over 400 indigenous
species inNatal, South Africa, for example; Cunningham,1990).
Little attention has been paid to the cul-tural, medical, economic
or ecological signifi-cance of the herbal medicine trade, yet
tradi-tional medicine sellers are a feature of everyAfrican city
(ECP/GR, 1983). Cities are con-centrated centres of demand drawing
in tradi-tional medicines from outlying rural areas andacross
national boundaries. Despite the differ-ences in volume and range
of species used, par-allels can be drawn between the trade in
med-icinal plants and that in fuelwood:(1) high proportions of
people use medicinal
plants (70-80%) and fuelwood (60-95%)(Leach and Mearns,
1988);
(2) high urban demand can undermine the
rural resource base by causing the deple-tion of favoured but
slow growing speciessuch as Combretum (fuelwood, Botswana;Kgathi,
1984) and Warburgia salutaris(bark medicines, Zimbabwe);
(3) harvesting is a strenuous and labour inten-sive activity
with financial returns, carriedout by rural people with a low level
of for-mal education and poor chance of formalemployment;
(4) supplies may be drawn from a long dis-tance away - from
200-500 km for fuel-wood in many African cities (Leach andMearns,
1989) and as far as 800-1200 kmfor certain medicinal plants in west
Africasuch as Entada africana and Swartziamadagascariensis or
Synaptolepis kirkii insouthern Africa (Cunningham, 1988a).
The herbal medicine trade is characterized bytwo features.
First, from being almost solely anactivity of traditional
specialists, medicinalplant collection has now shifted to involve
com-mercial harvesters in the informal sector, and(in South Africa
at least) formal sector traders(Table 2) who supply the large urban
demand.Women, rather than men, are increasinglyinvolved as
non-specialist sellers of traditionalmedicines, and this general
pattern is seenthroughout Africa. In rural areas and small
vil-lages, male and female TMPs practise fromtheir homes. In larger
villages, herbalists (main-ly men) dispense from a small quantity
of tra-ditional medicines that they have gatheredthemselves. In
towns, larger quantities of mate-rial are sold, some of which are
bought fromcommercial harvesters, and in cities or largetowns,
large quantities of plant material are sup-plied by commercial
harvesters and soldthrough increasing numbers of informal
sectorsellers (mainly women) to urban herb tradersor herbalists for
self-medication. Men drop outof non-specialist sales as it becomes
an increas-ingly marginal activity, and only persist as sell-ers of
animal material. Second, demand for tra-ditional medicines is
highly species specific andalternatives are not easily provided due
to thecharacteristics of the plant or animal material,their
symbolism, or the form in which they aretaken. These large urban
areas dictate prices,which are kept low because of rising
unem-ployment, over-supply and cheap labour. Thusnothing is paid
towards the replacement of thewild stocks.
In the stressful environment which is afeature of many urban
areas in Africa, it isnot surprising that demand has increased
fortraditional medicinal plant and animal mate-rials which are
believed to have symbolic orpsychosomatic value.
-
African medicinal plants: setting priorities at the
interfacebetween conservation and primary healthcare
!
;
C?
>5,1)&%51
)> 532- 15F1 2353 3+, +'+5%+( G%)G%1 1 7G)%+ +1 + G%7+% 3+(3
5+%
7+1&%
3(7+3&4%41)>745+(G(+1G51+%&1423+%-)+17+((%&7'%
)> 3 7)1 G)G&(+% 1G51 +55)&1 >)% 7&53 )> 3
5)77%5+( %+4 ) &%'+ +%+1 31
+GG(1J&+(()532-15F1)=+7'J&>)%K+7G( +4
9'+5+:+% 37)1
5)77)(1)(41G51+(3)&-3)3%1G51+%&145)&
%24 L 4C,)% 3 7)1 G)G&(+% 1)&%51 )> 532- 15F1 +%
+4
+4(115)77)(&14532-15F12%
+4 +7%)))(
+4 2% 3 '+11 )> + 532- 15F A5)+- 4&1%B 9+&-+%4
*/:
7(+%(1)&3%3++>%)7+1+7G()>**!G)G(%,241K1G51941-&134
' >)&% ()5+( +71: +55)&4 >)% *"M )> +((
&1+- +4 3 7+I)% )> 3 5)77%5+( 1+(1
3 7+I)% )> +(( 31 %1G)41 4G4 ) ')&-3 7+%+( %+3% 3+ 5)((5-
37
1(,1 %%1G5, )> 1= )> 1(7 3 (, )% 3% 4&5+)+( 1+&1
9;-&% 6: 3
1G51 &14 2% 1)F)4&+ 9
+4 9/MN /0 G)G(:N 2+G+
9 9*0MN6*:N1+29 +4 96MN!*:N+4
)2'%'% 9!
9"0MN00:
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
%&
14
14
.
>+@@
.
5)%+3
5)%+34
)37'
.
.
(5
-(&5)%4)41
-(&5)%4)41
'&%+4
)3%+(F+()41
G+(7+%
I+)%3=
5)(+7'+7
)37'
>+@@
G31)1-7
91%:
1%)(1
%%G1
4)5)1+)(
%1%G
)37'5
)&+'+
,)+5+7
,)+5+7
3++9:
)4C,)%96:
3++9:
3++9:
3++9:
3++9:
L4C,)%
+7%))$
3++96/:
+7'+9:
+7'+9:
3++9:
+=++9#:
+7%))9/:
L4C,)%96:
L4C,)%96:
3++9:
+7%))+
+4+-+15+%9":
%51 O9''2!:N6OF11G%15)77NO9)*":N#OE+G%15)77N
/O9;*":N"O9++(+) */:
.2. &').). $)$'.- 2(=).-2.($
-
African medicinal plants: setting priorities at the
interfacebetween conservation and primary healthcare
"
12.8% sold to France, 1.9% to Italy, 1.5% toUSA, 1% to Belgium
and 1.2% sold locally orto South Africa (Nott, 1986).
Unfortunately, thelow prices paid for the plants do not
coverreplacement or resource management costs, andas such, major
importers demanding high vol-umes of plant material are
contributing to thedecline of medicinal plant species in
Africa.
$$
Commercial gathering of traditional medicinesin large countries
with small urban populations(e.g. Mozambique, Zaire and Zambia) is
limit-ed and cases of over-exploitation are rare.Harvesting by TMPs
continues usually to beselective and on a small scale, and
traditionalconservation practices, where they exist, wouldbe
expected to be retained. In African coun-tries with high rural
population densities andsmall cities (e.g. Rwanda), gathering is
alsoexpected to be small scale, and where a speciesis popular and
supplies are low due to habitatdestruction and agricultural
expansion, the treewill suffer a death of a thousand cuts
ratherthan one-off ring-barking due to commercialharvesting (see
Photo 3).
The emergence of commercial medicinalplant gatherers in response
to urban demand formedicines and rural unemployment has result-ed
in indigenous medicinal plants being con-sidered as an open access
or common proper-
ty resource instead of a resource only used byspecialists. The
resultant commercial, large-scale harvesting has been the most
significantchange, although seasonal and gender relatedrestrictions
have also altered. Rural traditionalmedical practitioners and the
hereditary chiefswho traditionally regulate resource manage-ment
practices admit that ring-barking andover-exploitation by
commercial gatherers arebad practices that undermine the local
resourcebase. In Natal (South Africa) it appears thatrestrictions
placed by traditional communityleaders and enforced by headmen and
tradi-tional community policemen have reducedcommercial
exploitation of local traditionalmedicinal plant resources. With
culturalchange, increased entry into the cash economyand rising
unemployment however, these con-trols are breaking down.
Ring-barking or uprooting of plants is thecommonest method of
collection used by com-mercial gatherers (Photo 6). Where urban
pop-ulations (and resultant commercial trade in tra-ditional
medicines) are relatively small, buthigh rural population densities
and an agricul-tural economy have cleared most natural veg-etation,
tree species such as Erythrina abyssini-ca and Cassia abbreviata,
which are popularand accessible, have small pieces of barkremoved
(Photos 3 and 4), rather than a one-off removal of trunk bark
(Photos 5 and 6).
In South Africa, where the taboo againstgathering of traditional
medicines by menstru-ating women was widespread in the past,
urbanherbalists now no longer place importance onthis when buying
plants from urban markets,
Photo 2.Medicinal
plant sellerat a marketin Abidjan,
CtedIvoire,
showing thedominance
of fresh leafmaterial as
a sourceof herbal
medicines.
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
or in some cases, treat the plants to magicallyrestore their
power. Strict seasonal restrictionsare still placed on the
gathering of Siphonochilusaethiopicus rhizomes in South Africa
andSwaziland, but commercial collection ofAlepidea amatymbica
rhizomes now takes placeon misty days in summer (although
harvest-ed material is stored away from the homesteadfor fear of
lightning). Even where seasonalrestrictions are still in place,
demand can exceedsupply. Siphonochilus natalensis for example,had
disappeared from its only known localityin Natal before 1911 as a
result of trade betweenLesotho and Natal (South Africa)
(Medley-Wood and Evans, 1898).
It is clear that medicinal plant species gath-ered for
commercial purposes represent themost popular and often most
effective (physi-ologically or psychosomatically) herbal reme-dies.
From historical records (Gerstner, 1938,1939; Medley-Wood, 1896) it
is clear that themajority of species that were popular in thepast
are still popular today. Examples in south-ern Africa include
Erythrophleum lasianthum,Cassine transvaalensis, Alepidia
amatymbica
and Warburgia salutaris. Commercially soldspecies thus represent
a short list of the med-icinal plants used nationally, since many
speciesthat are used to a limited extent in rural areasare not in
demand in the urban areas. Alsoimportant from a resource management
pointof view, is that in virtually all African coun-tries, it is
not the limited, selective harvestingby specialist TMPs that
represents the problem.In most cases, non-sustainable use of
favouredspecies results from commercial harvesting tosupply an
urban demand for traditional medi-cines, after clearing for
agricultural or urbanassociated development has already takenplace.
The widespread commercial harvestingand sale of the same genera and
speciesthroughout their distribution range is signifi-cant (e.g.
Solanum fruits, Erythrophleum bark,Abrus precatorius seeds,
Myrothamnus flabel-lifolius stems and leaves and Swartzia
mada-gascariensis roots) (Appendix 1).
Medicinal plant gatherers are familiar withwhich species are
becoming difficult to find,either because of limited geographical
distrib-ution, habitat destruction or over-exploitation.
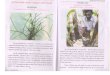
Photos 3 to 6. Declining rural resource base under
non-commercial demand, but limitedsupplies (3) Erythrina abyssinica
(Fabaceae), Malawi (death from a thousand cuts)and (4) Cassia
abbreviata (Fabaceae), Zimbabwe, (5) Large pieces of Warburgia
-
African medicinal plants: setting priorities at the
interfacebetween conservation and primary healthcare
#
sustainable rate of harvest. Low stocks are like-ly to produce
small sustainable yields, particu-larly if the target species is
slow growing andslow reproducing. Large stocks of species witha
high biomass production and short time toreproductive maturity
could be expected to pro-duce high sustainable yields, particularly
ifcompetitive interaction is reduced by thin-ning. The impact of
gathering on the plant isalso influenced by factors such as the
part ofthe plant harvested and harvesting method.
Demand for fast growing species with a widedistribution, high
natural population density andhigh percentage seed set can be met
easily, par-ticularly where leaves, seeds, flowers or fruitsare
used (Photo 7). The common sale and useof medicinal plant leaves as
a source of med-icine in Cte dIvoire and possibly other partsof
west Africa (Photo 2) is therefore highly sig-nificant as it
differs markedly from the highfrequency of roots, bark or bulbs at
markets in
Their insights, coupled with botanical and eco-logical knowledge
of the plant species involved,provide an essential source of
information fora survey of this type. In this survey, it was
notconsidered constructive to distinguish betweenplant species with
symbolic uses and those withactive ingredients. The important
question hereis whether the species are threatened or
not,because:(1) species that have a purely symbolic value
are nevertheless important ingredients oftraditional medicines
for their psychoso-matic value and are as effective as place-bos
are in urban-industrial society;
(2) the majority of traditional medicines havenot been
adequately screened for activeingredients and a number of species,
forexample Rapanea melanophloes in south-ern Africa, while being
primarily used forsymbolic purposes, also have active ingre-dients.
Conservation efforts must thereforebe directed at all species
vulnerable toover-exploitation.
For any resource, a relationship exists betweenresource capital,
resource population size and
salutaris (Canellaceae) bark from Namaacha on the Swaziland
border commerciallygathered for sale in Maputo, Mozambique, (6)
Curtisia dentata (Cornaceae) tree in Afro-montane forest, South
Africa, debarked for sale in Durban, a city 100 km away.
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
%
the southern African region (Photo 7).Throughout Lesotho,
Malawi, Mozambique,Swaziland, Zambia, Zimbabwe, and particular-ly
South Africa, herbal material that is dried(roots or bark), or has
a long shelf-life (bulbs,seeds and fruits) dominates herbal
medicinemarkets (see Appendix 1). In contrast, six sell-ers in
Abidjan, Cte dIvoire, primarily soldleaf material (20-41 spp.),
followed by roots(1-16 spp.), bark (0-8 spp) and whole plants(0-3
spp.). This situation was typical of the 111traditional medicine
sellers in Abidjan, apartfrom those bringing material from Burkina
Fasoand Mali, who sell more root and bark mater-ial. The situation
with chewing stick sellers inCte dIvoire and other parts of west
Africa issomewhat different however, as stems and rootsare the
major plant parts used, with consequenthigher impact on favoured
species.
Despite limited information on the popu-lation biology of
medicinal plants, it is possi-ble to classify target plant species
according todemand, plant life-form, part used, distributionand
abundance (Cunningham, 1990). The largecategory of traditional
medicinal plants whichare under no threat at all are the cause of
lit-tle concern to TMPs or to conservation biolo-gists. For these
species, demand easily meetssupply. From a conservation viewpoint,
on anAfrica-wide scale, there are two categories ofmedicinal plants
that are of concern:(1) Slow growing species with a limited
dis-
tribution which are the focus of commer-cial gathering where
demand exceeds sup-ply. Harvesting expands to areas progres-sively
further afield, where rising pricesfor the target species are
incentives to col-lect. This results in the species beingendangered
regionally and causes wide-spread depletion of the rural resource
base
of TMPs. Examples of this includeWarburgia salutaris in east and
southernAfrica and Siphonochilus aethiopicus inSwaziland and South
Africa. Endemicspecies with a very localized distributionare a
particular problem, for example:(a) Ledebouria hypoxidoides, which
is
endemic to the eastern Cape region(South Africa). Herbalists
wereobserved removing the last bulbs fromthe locality near
Grahamstown (F.Venter, pers. comm.).
(b) Mystacidium millari, also endemic toSouth Africa, which is
threatened dueto harvesting and commercial sale asa traditional
medicine in the nearbycity of Durban, South Africa(Cunningham,
1988a).
(2) Popular species which are not endangeredbecause they have a
wide distribution, butwhere habitat change through
commercialharvesting is cause for concern. Trichiliaemetica and
Albizia adianthifolia forexample, are not a high priority for
con-servation in southern Africa, although theyare a popular source
of traditional medi-cines. What is of concern however, is
thatring-barking in conserved forests iscausing canopy gaps and
changing the for-est structure, which can lead to an influxof
invasive exotic species. This is impor-tant for local habitat
conservation.
Both categories are of particular concern in pro-tected area
management, as core conservationareas will ultimately come under
pressure fromharvesting for favoured species if they are dif-ficult
to obtain elsewhere.
Information on the quantities of tradition-al medicines being
harvested or sold is sparse,
3))0
45+(G(+1
>)%1+(++ 7+%F
&(+2+) '+%F
+4%))7+%+(
+1+1)&%5
)>3%'+(7451
-
African medicinal plants: setting priorities at the
interfacebetween conservation and primary healthcare
0
whether for the local trade in traditional medi-cines, or for
export and extraction of active ingre-dients. Apart from placing
the quantities requiredfrom cultivation into perspective, the
informa-tion available is of little relevance unlessexpressed in
terms of impact on the species con-cerned. In South Africa,
harvesting from wildpopulations of certain species is on a scale
thatgives cause for concern amongst conservation
organizations and rural herbalists, and a listingof priority
species is available (Cunningham,1988a) (Box 2). The same applies
to some chew-ing stick species, such as Garcinia afzelii in
westAfrica. The only quantitative data on the vol-ume of plant
material sold comes from Natal(South Africa), where medicinal
plants areordered by urban based herb traders in standard-size
maize bags (Table 4).
-%+(%7
-%+(%7
-%+(%7
-%+(%7
)
"
"
#
#"
)
$
+"
,-
.
,/"
!01!2
!""
,"
3"
)
#--
"
&
)"
*"
$
3"
)
#
9 .:,& "!#..$'% ( &""!%&&,6 &.$1":,& 6*
&"&%$%;721" ','(. )$'.- ?'($2$*
+2&&'&
(=
3&'3+()
'=+
&4&=+
+3&-+&
3+3+=)
;&(2+7
)()&
+7&
+7&
7+7(()
&F&7'(
)'3)&
+G3G3+F3&'+()&
-2,&
3+3+1
+=+&
3+4(+-&&
+3)-2&
'1(+
3&3&(&&7
3)J)&
2+=1
3&5&
&F+&
;-)7
3)42&7
+=7+7++
')(+
8+=+-)7+7')7,&
3&'3&'3&&
(&=
(&-&3(&-&&7
+F2+1
+'+'+=+&
32+-&&7
&7+
+3(&7
""
6#
**
6
00#
/*
/
#/
#6#
0@
0@
#
#!
#!
60
6"
/
6/
6**
6*#
6/0
6/6
6#
6##
6#!
6#
6
66*
660
66#
666
666
66!
6"
66
6!*
6!
*
0
'&('
'&('
%))
17
'+%F
'&('
'&('
%))9(:H
(+,1P17
%))
'+%F
23)(G(+
'+%F
'+%F
%))
(+,1P17
'&('
'+%F
%))
%))
'&('
'+%F
%))9(:H
'+%F
%))
'&('
'+%F
17
'+%F
(+,1P17
23)(G(+
'&('
'+%F
>%&
'+%F
@ , 1G51O,,, +4,/
@@ # +4 H %))9(:O%))9(-)&'%:
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
1
66
Chewing sticks are obtained from wild popula-tions of indigenous
plants, apart from the infre-quent sale of exotic species such as
Azadirachtaindica and Citrus sinensis (Appendix 1).Garcinia afzelii
is considered to be threatenedby this trade (Ake Assi, 1988b;
Gautier-Beguin,pers. comm.). In Nigeria, Okafor (1989) reportsthat
Randia acuminata chewing sticks are stillcollected from primary and
secondary forestwithin 3 km of villages, but that the distance
isincreasing, which indicates that the resource isbeing depleted.
At a single depot, for example,Okafor (1989) recorded that five
commercialchewing stick collectors assembled 1144 bun-dles of
chewing sticks, made up of seven or eightsplit stems one metre long
per bundle. What ishighly significant from a resource
managementviewpoint, and has not been taken into accountpreviously,
is that whilst peeled twigs are usedas chewing sticks from most
species, split stemsand roots are the source of the
commerciallysold chewing sticks. Among the 27 species usedin Ghana,
for example, high impact harvestingof stem wood or root material
from only sevenspecies accounted for 88% of chewing sticksused. The
low impact use of peeled twigs aschewing sticks accounted for the
other 12 % ofsticks used and for the remaining 20 species(Ake Assi,
1988b). Impact on those sourcespecies which are cut down or
up-rooted to sup-ply urban demand is therefore high.
Few data are available on the quantities of rawmaterial
harvested for the pharmaceutical trade,or the environmental impact
of harvesting. It isclear however that large quantities of
materialare collected from the wild and that harvestingcan be very
destructive. The same can apply toplant material collected for
screening purpos-es. Juma (1989) offers the example of
Maytenusbuchananii: 27.2 tons of plant material werecollected by
the American National CancerInstitute (NCI) from a conservation
area in theShimba Hills (Kenya), for screening purposesas a
potential treatment for pancreatic cancer.When additional material
was required fouryears after the first harvesting in 1972,
regen-eration was so poor that collectors struggled toobtain the
additional material needed.
No studies are known to have been carriedout on the social or
environmental conse-quences of harvesting, for example:(1) the
75-80 t of Griffonia simplicifolia seed
exported each year to Germany from
Ghana (Abbiw, 1990);(2) the medicinal plant material exported
from
Cameroon to France (Voacanga africanaseed (575 tons); Prunus
africana bark (220tonnes), Pausinystalia johimbe bark (15 t)(United
Republic of Cameroon, 1989).
However, Ake-Assi (pers. comm.) reports thatcommercial gatherers
in Cte dIvoire chopdown Griffonia simplicifolia vines andVoacanga
africana and Voacanga thouarsiitrees in order to obtain the fruits.
Concern hasbeen expressed about a similar situation inIndonesia,
where Rifai and Kartawinata (1991)point out that:
Export of medicinal plants has been goingon for many years, and
the demand in the inter-national market keeps increasing. One
bigSwiss pharmaceutical company, for example,has requested eight
tons of seeds of Voacangagrandifolia and are willing to pay a high
price.This species is rare and has light seeds. To sat-isfy the
above request, all available seeds inthe forest will perhaps have
to be harvested,leaving nothing for regeneration. Similarly,
fivetons of rhizomes of a rare Curcuma (temabadur) has been sought
by a West German phar-maceutical company, and 100 kg year-1 of
pilicibotii (fine hairs of Cibotium barometz) by aFrench firm. It
can be imagined how manyplants of these species will have to be
destroyedshould such requests be satisfied.
If the international companies involved inthis trade are to
operate in a responsible man-ner, then this situation needs to
change to oneof commercial cultivation and sustainable use.
$$
The categories of medicinal plant species thatare most
vulnerable to over-exploitation can beidentified by combining the
insights of herbalmedicine sellers with knowledge on plant biol-ogy
and distribution (Cunningham, 1990).However, due to the number of
species involvedand the limited information on biomass, pri-mary
production and demography of indige-nous medicinal plants, no
detailed assessmentof sustainable off-take from natural
populationsis possible. Even if these data were available,their
value would be questionable due to theintensive management inputs
required for man-aging sustainable use of vulnerable species
incases where demand exceeds supply.
Unsustainably high levels of exploitationare not a new problem,
although the problemhas escalated in regions with large urban
areasand high levels of urbanization since the 1960s.
-
African medicinal plants: setting priorities at the
interfacebetween conservation and primary healthcare
!
Prior to 1898, local extermination of Mondiawhitei had been
recorded in the Durban area ofSouth Africa due to collection of its
rootswhich found a ready sale in stores. By 1900,Siphonochilus
natalensis (an endemic speciesn o w c o n s i d e r e d s y n o n y
m o u s w i t hSiphonochilus aethiopicus; Gibbs-Russell et
al.,1987) had disappeared from its only knownlocalities in the
Inanda and Umhloti valleys dueto trade to Lesotho. This occurred
despite a tra-ditional seasonal restriction on harvesting
thisspecies. By 1938, all that could be found ofWarburgia salutaris
in Natal and Zululand waspoor coppices, every year cut right down
tothe bottom (Gerstner, 1938). Most botanicaland forestry records
reflect the impact of com-mercial collection of Ocotea bullata bark
dueto the importance of this species for timber.Oatley (1979) for
example, estimated that lessthan 1% of 450 trees examined in
Afro-mon-tane forest in South Africa were undamaged,and in the same
region, Cooper (1979) esti-mated that 95% of all Ocotea bullata
trees hadbeen exploited for their bark, with 40% ring-barked and
dying. The situation would appearto be similar in Kenya, where
Kokwaro (1991)records that some of the largest Warburgia salu-taris
and Olea welwitschii trees have been com-pletely ring-barked and
have died. InZimbabwe, due to the high demand and limit-ed
distribution of this species, the situation isworse, and all that
remains of wild Warburgiasalutaris populations are a few coppice
shoots
(S. Mavi pers. comm., 1990). In Cte dIvoire,Garcinia afzelii is
considered threatened due toharvesting for the chewing stick trade
(AkeAssi, 1988b). Destructive harvesting ofGriffonia simplicifolia,
Voacanga thuoarsii andVoacanga africana fruits for the
internationalpharmaceutical market is also of concern (L.Ake-Assi,
pers. comm., 1989). In Sapoba ForestReserve, Nigeria, despite
traditional restrictionson bark removal, Hardie (1963) observed
howthe trunk of a large Okoubaka aubrevillei tree(a very rare
species in west Africa) was muchscarred where pieces of bark had
beenremoved. There appears to be nothing pub-lished on the current
status of this species.Botanical records are also scanty for
bulbousor herbaceous species, where little remains toindicate
former occurrence after the plant hasbeen removed. It would
therefore be useful tocarry out damage assessments for species
suchas:(1) Okoubaka aubrevillei, Garcinia afzelii, G.
epunctata, and G. kola in Cte dIvoire ,Ghana, and Nigeria;
(2) Warburgia salutaris in Kenya, Tanzaniaand Zimbabwe;
(3) assessments of the impact of Prunusafricana and
Pausinystalia johimbe barkharvesting in Cameroon and Madagascar,and
fruit harvesting of Griffonia simplici-folia, Voacanga thuoarsii
and Voacangaafricana for the international pharmaceu-tical
market.
Figure 4. The seven-point scale used in field assessment of bark
damage. All assessments represent the degree of bark removal below
head height (2 m), which is marked by the dotted line and arrow in
the figure (Cunningham, 1988a).
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
9'+5+:
+%+%1G51)55&%%-37)&+1+%+)%321)
4C,)% 23)1 %))1 +% &14 %+4)+( 745 +(1) 41 )
' ,1-+4
>>22
(3)&-3()5+(),%KG()+))> 9%534+5+:
9%1%54 ) (71) )&5%)G1N &14 +1 + (&5F 53+%7 +4 >)%
+
A12)( ( 1)7+53B: +4 G)11'( ) "
9(+-((+5+:9+(1)+ (7441%'&)&14+1+ (&5F53+%7
)G%,) >%)7'-2+1>&( 9G+%5&(+%(237):4& )
3 A5()143+4B13+G)> 3 (+,1:7+)55&%+4&7'%1)>
9;+'+5+: 9%))1 &14 ) %+ 4+%%3)+
+4+'4)7+(G+1:3+,45(4+%)&4&1+F+4&)47+4
>)% 7'% ) 1G51 +% 3%+4 ' 3 3%'+( 745 %+4
+ 311+-4& ) 3 ()23&7+G)G&(+)41+4 %(+,
( 17+(( 1=)> 3&%'+G)G&(+)
;;
Forests also contain a high number of medicinalplant species,
yet represent a small (and declin-ing) proportion of total land
area in the easternsection of Africa and trees are often subject
to
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
""&&>>22??''..
)5+( ),%KG()+) )> 1)7 1G51 ) 3+5+
1(+4 '& +1 3 )%5)&-31
5)(41 &G1 1)7+53 +4 +1 + 1&>> >)%
3+4+531
" 9G+5+: &14 >)% 5)&-31
+45)(41
)
9%5+ 55)%4- ) ()5+( 3%'+(11 )
3+1 41+GG+%4 >%)7 F)2 ()5+(1
)&14+()()I++&%1%,2+=(+4
%%,,4422
AA'',,((..)),,..((----..,,22((22((==
$
9)15)%+5+:
# 1G51 9F)2 ()5+((+17&2+2+: &14
>)% 1)7+53 +(71 +4 ) %+ ,%+( 41
+1
)5+(),%KG()+))>
" 9;+'+5+:+4+&4>4
1G51F)2()5+((+1F+F)71+7%--G%)'
(7
00&&''$$:://))22 9&-3+7!:
..BB$$22(($$22(($$::..4422,,--
) 9
-
African medicinal plants: setting priorities at the
interfacebetween conservation and primary healthcare
#
..((--((==..))..--
+" 9+((+5+:&14>)%5)&-31
5)(41+1+1&>>>)%3+4+5319G)24%4'+%F
7K423'+%F >%)7
9;+'+5+:
)
9)% 12)(( &44%1 )> 5+( >)%
531 5)7G(+1+4 >)%7+-5+(G&%G)11
, 9(+3+5+: '+%F &14 '
4,%1 )-3% 23 1+G) %53 1G51
1&53 +1& + &'&(+2& 7K
) + ' ( 3 7 ) % G % 4 % + 7 1
5(+%(
3" 9+&%+5+: &14 >)% 17')(5 G&%
G)11 ) 7+F + G%1) A17(( +4 '5)7
&G)G&(+%B
3 9+&%+5+: &1+1+'),
# 9)%+5+:%45)()&%4'+%F&14
>)% 7+-5+( G&%G)11 1 &F)2 +4
FG ,%15%
9(+1%+5++: &1 &G&'
(134
6
9%)+5+: '+%F &14 )
%+71%&+(G+1+(1) >)% &'%5&()11
5 9+5+%4+5+: &1) %5)%44
9%534+5+: ) + 1G51
1G5>5 &1 )77) 1+54&7 5+G1
)41-&134'3%'+(11+14>>%)3
1G519+47+)3%GG31&14>)%17
')(5G&%G)11:
5" 9(+5+: '&('1 &14 )
G%G+%7+1
%+4)+( 745+( G(+1 )3% 5+
-)%1 +% -, &-3+7 **'N !
+%5&(+%( )2)%3 +%
9 + & 5 & ( + 5 + : + 4 )
9+-%+5+: 475 ) 1)&3+1% >%5+
945(-:
Commercial gatherers of medicinal plant mate-rial, whether for
national or international trade,are poor people whose main aim is
not resourcemanagement but earning money.
Cultivation as an alternative to over-exploitation of scarce
traditional medicinalplants was suggested over 50 years ago in
SouthAfrica for scarce and effective species such asAlepidea
amatymbica (Gerstner, 1938) andWarburgia salutaris (Gerstner,
1946). Until twoyears ago, no large scale cultivation had
takenplace. There are two main reasons for this, andboth apply
elsewhere in Africa:(1) lack of institutional support for
production
and dissemination of key species for cul-tivation;
(2) the low prices paid for traditional medic-inal plants by
herbal medicine traders andurban herbalists.
If cultivation is to be a success as an alterna-tive supply to
improve the self-sufficiency ofTMPs and take harvesting pressure
off wildstocks, then plants have to be produced cheap-ly and in
large quantity. Any cultivation forurban demand will be competing
with materi-al harvested from the wild that is supplied ontothe
market by commercial gatherers who haveno input costs for
cultivation. Prices thereforeincrease with scarcity due to
transport costs,search time and the long-distance trade. At
pre-sent, low prices (whether for local or interna-tional
pharmaceutical trade) ensure that fewspecies can be marketed at a
high enough priceto make cultivation profitable. Even fewer ofthe
potentially profitable species are in the cat-egory most threatened
by over-exploitation.
At present, cultivation of herbs and medi-cinal plants is
chiefly restricted to temperateareas (Staritsky, 1980) and with the
exceptionof India (Kempanna, 1974) and Nepal (Malla,1982), few
tropical countries have investigat-ed the potential of cultivating
medicinal plantson a commercial scale. Cultivation of herbs
andmedicinal plants is widespread in easternEurope, but even where
cultivation is welldeveloped, such as in the Russian
Federation,about half of the supplies are gathered fromwild
populations (Staritsky, 1980). In all caseswhere cultivation has
taken place, whether inEurope, Asia or Africa, plants have been
grownfor profit or a high level of resource returns
and provide acceptable alternative resourcesoutside increasingly
fragmented core conserva-tion areas to stop over-exploitation of
favouredspecies inside them.
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
%
(e.g. multiple use species for fruits, shade andmedicinal
properties) and are either fast grow-ing species, or plants where a
sustainable har-vest is possible (e.g. resins (Bosweilia),
leaves(Catha edulis).
With few exceptions, prices paid to gath-erers are very low,
taking no account of annu-al sustainable off-take. In many cases,
medic-inal plants are also an open access, rather thana limited
access or private resource. To makea living, commercial medicinal
plant gathererstherefore mine rather than manage theseresources. If
cultivation of tree species is to bea viable proposition as an
income generatingactivity then either:(1) the flood of cheap
bark/roots mined from
wild stocks is reduced through better pro-tection of conserved
forests in order tobring prices to a realistic level; or,
(2) wild populations will have to decline fur-ther before
cultivation is a viable option.
Cultivation for profit is therefore restricted toa small number
of high priced and/or fast grow-ing species (Box 3).
Although some of these species are threat-ened in the wild (e.g.
Garcinia afzelii andWarburgia salutaris), low prices ensure that
fewslow growing species are cultivated. With thedeclining economic
state of many African coun-tries, it is unlikely that subsidized
productionof these species is likely to occur, and collec-tion of
seed or cuttings for establishment offield-gene banks (for
recalcitrant fruitingspecies) and seed banks must therefore be
seenas an urgent priority.
Strong support and commitment are nec-essary if cultivation is
to succeed as a meansof meeting the requirements of
processingplants for pharmaceuticals (whether for localconsumption
or export) or urban demand forchewing sticks and traditional
medicinal plants.If cultivation does not take place on a
largeenough scale to meet demand, it merelybecomes a convenient bit
of window dress-ing, masking the continued exploitation ofwild
populations. The regional demand for wildScilla natalensis
(Liliaceae) in Natal, SouthAfrica is 300 000 bulbs yr-1, all at
least 8-10years old. On a 6-year rotation under cultiva-tion at the
same planting densities as Gentry etal., (1987) used for Urginea
maritima, 70 hawould be required (Cunningham, 1988a). Dueto their
slow growth rates, the rotational arearequired for tree species
would be far greater,with total area dependent on demand.
The success of cultivation also depends onthe attitude of TMPs
to cultivated material, andthis varies from place to place. In
Botswana,TMPs said that cultivated material was unac-ceptable, as
cultivated plants did not have thepower of material collected from
the wild (F.Horenburg, pers. comm.). Discussions withsome 400 TMPs
in South Africa over a twoyear period showed general acceptance of
cul-tivated material as an alternative. Similarly,TMPs in the
Malolotja area of Swazilandaccepted cultivation as a viable
alternative. Inboth countries there is a tradition of
growingsucculent plant species near to homesteads toward off
lightning. Similarly, in Ghana, plantsof spiritual significance
such as Datura metel,
&))-)(+
%)7)+
2&=.&=):2'(2$
? ."8&(&$"!#&%' "' $ (0
.&,'$"!#"%)&"'''"*,&1,"&%% ,$&)$ '"+&%)""$
& $%")( " &(.&%.)$(&1!#."&%' (!(.,& *#$(
&&!&&%( &&!& &)$""+
).
5
-
African medicinal plants: setting priorities at the
interfacebetween conservation and primary healthcare
0
Pergularia daemia, Leptadenia hastata andScoparia dulcis are
tended around villages.Therefore, although little is known about
atti-tudes to cultivation of medicinal plants in westAfrica, it is
possible that TMPs would be infavour of cultivation of alternative
supplysources.
An interesting model is provided inThailand where a project for
cultivation ofmedicinal plant of known efficacy has been ini-tiated
in about 1000 villages and traditionalhousehold remedies, with
improved formulae,are produced as compressed tablets packed infoil
and distributed to drug co-operatives setup through a Drug and
Medical Project Fundin more than 45 000 villages as well as
incommunity hospitals (Desawadi, 1991).Wondergem et al. 1989; WHO,
1977) havealready drawn on the Thailand experience inmaking
recommendations regarding primaryhealthcare in Ghana.
;;""
>>2244..
+" 9+((+5+:@
" 9G+5+:
#"" 9;+'+5+:
44>>22,,((--
9>)% ()5+(7+%F+4 >)%KG)% ))&3>%5+:
+" 9+((+5+:@
" 9G+5+:
&/ 9(+5+:
)
1 9
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
1
Figure 6. The main African phytochoria (afterWhite, 1983)
showing one highconservation priority area and focal priority areas
for action onmedicinal plant conservation .I. Guineo-Congolian
regional
centre of endemism. II. Zambezian regional centre
of endemism.III. Sudanian regional centre of
endemism. IV. Somalia-Masai regional centre of
endemism.V. Cape regional centre of endemism. VI. Karoo-Namib
regional centre of endemism. VII. Mediterranean regional centre of
endemism.VIII. Afromontane archipelago-like centre of endemism
(including IX, Afroalpine archipelago-like region ofextreme
floristic impoverishment, not shown separately).
X. Guinea-Congolia/Zambezia regional transition zone.XI.
Guinea-Congolia/Sudania regional transition zone.XII. Lake Victoria
regional mosaic. XIII. Zanzibar-Inhambane regional mosaic. XIV.
Kalahari-Highveld regional transition zone. XV. Tongaland-Pondoland
regional mosaicXVI. Sahel regional transition zone. XVII. Sahara
regional transition zone. XVIII. Mediterranean/Sahara regional
transition zone.
Figure 7.The relative size anddistribution of majorurban centres
in sub-Saharan Africa(after Udo, 1982).
-
African medicinal plants: setting priorities at the
interfacebetween conservation and primary healthcare
!
Policy priorities forconservation and primary
healthcare
88
In order to ensure the effective conservation ofAfrican plants
which have medicinal value, therecommendations recognize the
importance ofthe following two issues:(1) the destruction of
natural habitat through
agricultural expansion, logging, planta-tions, dam construction,
urban associateddevelopment, etc.;
(2) the over-exploitation of particular plantspecies to satisfy
demand e.g. Warburgiasalutaris in South Africa, Swaziland
andZimbabwe.
The conservation strategy for African medici-nal plants must
address the problem at two lev-els: recommendations which have
socio-eco-nomic effects must be incorporated at the pol-icy level
and recommendations for conserva-tion methodology must be addressed
at thenational and local levels. The recommendationscover the
following areas:(1) international and national policy;(2) in-situ
and ex-situ conservation methods;(3) education and research.
22
Policies made at both the international andnational level will
have substantial effects onthe success of an overall conservation
strategythrough the easing of wealth inequalitiesbetween nations.
International policies such as
trade and tariff agreements, GATT and EECsubsidized imports all
aim to make tradingbetween wealthier and poorer nations easier:
inaddition, international aid and financial supportby such bodies
as the World Bank plays animportant role. At the national level,
policiesaffecting agricultural expansion, plantations,urban and
industrial developments, education,employment, healthcare, the
provision of socialservices and funding affect the potential
suc-cess of any conservation strategy.The policy making process
should:(1) recognize the international and national
price paid for habitat destruction, includ-ing the loss of
medicinal plant resourcesand a reduced quality of healthcare;
(2) ensure that commodity prices at both thenational and
international levels are real-istic enough to reflect the cost of
resourcereplacement;
(3) ensure that incentives exist for the sus-tainable management
of medicinal plantresources;
(4) encourage equitable financial partnershipagreements and
incentive packages to con-serve biological diversity; tropical
zonecountries with the richest biological wealthhave the poorest
economic wealth withwhich to conserve those resources (debtswaps go
some way to ameliorate this dis-crepancy);
(5) provide the framework for greater incen-tives such as
security of land tenure toencourage longer term investment in
sus-tainability;
(6) recognize the relationship between socialservices and
dependence on naturalresources as a means of generating income.
International conservation agencies, in con-junction with
governments and NGOs, need todetermine a mechanism whereby
those
-
African medicinal plants: setting priorities at the interface
between conservation and primary healthcare
"G(+ %1)&%51
3%)&-3G%),4-1&GG)% )3)')+11
>%)7 4,()G-5)&%1
3+,171>%)73%5)-)3+ G)G(
%&%+(5)77&1)>3+,4+(4+4
G%)>)&4F)2(4-)>3G%)G%1+45)()-)>
()5+(()55&%%-G(+1+4%()37>)%7+)>
3%>))417451>&('&(4-7+%+(1
+4 )3%G%)4&51)2,%7&53
)> 31 F)2(4-1'-()1233 %+1>)%7+)
)>()5+(5)1171+4 ()5+(5&(&%1,%
3+%,1-)> ) 5&(,+4G(+115%+1-(
5)77)5+&14'()11)>3+'+5%+1 ()5+(
&1+43-%)2-47+41)>%+4)-%7
5)1%,+))>G(+%1)&%51+43 F)2(4-
+11)5+42337144>)%3'>)>3
()5+(G)G(+4 >)% 3% G)+(&1)()5+(
5)77&1 )3%G(+51
34,%1)>%+4)+(G(+%1)&%5
7++-7G%+551%&13%)&-3+ 1G5%&7>%)7
A5&(,+)B3%)&-3) -+3%-A2(4BG(+1+(()>
2353+%5(&443)G(+4(+1
+GG%)+53
3)')+115+2)%F)-3%23()5+(G)G()
1&4+4%5)%43&11)>G(+%1)&%514>
5+11)>),%3+%,1-)> )5&(,+4G(+1>4
1&1++'(3+%,1-73)41+4,1-+
+(%+,11&53+15&(,+)
3)G(+4(+1+,1'&(4-1&GG)%
>)%3)')+11>%)74,()G-5)&%123)
2)%F23()5+(G)G()11&1%(+4)3
5)1%,+))>')3G(+%1)&%51+4%+4)+(
5)()-5+(F)2(4-G+%5G+1)%-+=
G+%5G+)%2)%F13)G1&4%+F415&11)+4
+4,1)%,11)>(4G%)I51+4G%),4(%+&%
)3)')+%+4)+(5)()-5+(F)2(4-+4
1&1++'(G(+%1)&%5&113)G43++
2)%F)> 3)')+112)%F-)3111&1
4>>%5)&%1+4%-)15+'4,()G4
)K53+->)%7+)13+%KG%5+4
5)((+')%+)>(4G%)I51
Contents