Embed Size (px)
Citation preview

Aksiyal Spondiloartrit Konsepti;Klasifikasyon Kriterleri ve Erken
Tanı için Sevk Stratejileri
Dr. Servet Akar
İzmir Katip Çelebi Üniversitesi Tıp Fakültesi
Romatolojide Son II Yıl10-13 Nisan 2014 /Swissotel Grand Efes, İzmir

Tanı vs Sınıflama
Tanı kriterleri Sınıflama kriterleriTanı koymaya çalışan hekimlerce kullanılır Tanısı zaten konulmuş olan hastalara uygulanır
Test/parametrenin değeri hastalık prevalansına bağlıdır (pretest olasılık)
Tüm hastalar zaten tanı aldığı için hastalık prevalansı önemli değildir
Amaç bireysel hastaya tanı koymaktır Klinik veya deneysel çalışmalarda amaç araştırıcıların homojen bir hasta grubunu değerlendirmesi ve ortak dili konuşuyor olmasıdır
Olabildiğince çok hastayı tanıyabilmek için “duyarlılığı” yüksek olmalıdır
Yanlış tanıdan kaçınabilmek için “özgünlüğü”yüksek olmalıdır
Tanısal güvenilirlik “esnek” olmalıdır (kesin, olası, muhtemel vb)
Evet veya hayır diye cevaplanabilir
Bireysel hastalara uygulanır Bir grup hastaya uygulanır
Rudwaleit M et al. Arthritis & Rheum 2005:1000-1008

İçerik
• Aksiyal SpA (vaka tanımlama) ve temel kavramlar
• Sevk; kim için ve niye
– Toplumsal hastalık yükü
– Etkin sevk (refere) stratejisi var mı

Spondiloartrit-SpA (Spondiloartropati)
•Ankilozan Spondilit
•Reaktif artrit
•Psöriatik artrit
•İnflamatuvar barsak hasta-
lıkları ile ilişkili artritler
•Belirlenemeyen SpA
•Juvenil SpA
Klinik
Genetik
Radyolojik
HLA B27, ARTS1

AS için Modifiye New York (1984) Sınıflandırma Kriterleri*
Klinik Kriterler:1. Üç ay veya daha uzun süren, dinlenme ile geçmeyip, egzersiz
ile düzelen bel ağrısı ve tutukluğu2. Lomber omurga hareketlerinde, sagittal ve frontal planlarda
kısıtlılık3. Göğüs ekspansiyonunun yaş ve sekse göre düzeltilmiş normal
değerlere göre kısıtlanması
Radyolojik Kriterler:1. Bilateral grade 2-4 sakroiliit2. Unilateral grade 3-4 sakroiliit
Kesin AS: Bir radyolojik kriter ve klinik kriterlerden biriOlası AS: Tek başına üç klinik kriter veya bir radyolojikkriter
*van der Linden S, et al 1984

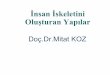
AS Tanısında Gecikme

AS Tanısında Gecikme
Feldtkeller E, et al. Rheumatol Int 2003;23:61–66Feldtkeller E, et al. Curr Opin Rheumatol 12 (2000) 239-247
İlk BelirtiYaşı
İlk TanıYaşı
Erkekler (N=920)Kadınlar (N=476)
00 10 20 30 40 50 60 70
20
40
80
60
100Hast
a (%)
Almanya’da AS tanısında ~ 9 yıllık gecikme
Yaş (yıl)

Radyografik sakroiliit
• İnflamasyonu göstermiyor!
• Sonuçlarını (?) gösteriyor!


71 hastanın verileri “paper patients”
Kronik bel ağrısı ve SpA ilişkili bazı bulguları var
%96 radyografik sakroiliiti yok
20 ASAS uzmanınca değerlendirilmiş
SpA vs SPA değil şeklinde sınıflamaları istenmiş
33 SpA, 15 SpA değil ve 23 sınıflanamaz
MRI verileri sonrası 15 hastanın (%21) sınıflaması değişmiş
36 SpA, 19 SpA değil (MR OR 45)

Aksiyal SpA için ASAS sınıflama kriterleri
≥ 3 ay bel ağrısı ve semptom başlangıç yaşı <45 yaş hastalarda
Görüntülemede sakroiliit*
+
≥ 1 SpA bulgusu**
HLA B27
+
≥ 2 diğer SpA bulgusu**
veya
*Görüntülemede sakroiliit:
-MRI’da SpA ilişkili sakroiliiti
şiddetle düşündüren aktif
(akut) sakroiliit
-Modifiye New York kriterlerine
göre kesin radyografik
sakroiliit
** SpA bulguları:
-İnflamatuvar bel ağrısı
- Artrit
-Entezit (topuk)
-Üveit
-Daktilit
-Psöriazis
-Crohn hastalığı/Ülseratif kolit
-NSAID’a iyi yanıt
-Ailede SpA öyküsü
-HLA B27
-Artmış CRP
Sensitivite %82.9Spesifisite %84.4
+LR 5.3-LR 0.20
Görüntüleme koluSensitivite %66.2Spesifisite %97.3
Pretest olasılığı %60 olan romatoloji kliniğinde:Kriterleri karşılayan hastada
Posttest olasılık %89Karşılamayan hastalardaPosttest olasılık %23.5



Aksiyel Spondiloartrit
Bel/sırt ağrısıBel/sırt ağrısı
Radyolojik sakroiliit
Bel/sırt ağrısıSindesmofitler
Preradyolojik dönem
Aksiyel farklılaşmamış SpA
Radyolojik dönem
AS (Modifiye New York Kriterleri)
1984
Zaman (yıl)
Rudwaleit, et al. Arthritis Rheum 2005;52:1000-8
X

Aksiyel Spondiloartrit
Bel/sırt ağrısıBel/sırt ağrısı
Radyolojik sakroiliit
Bel/sırt ağrısıSindesmofitler
Non-radyografik AksiyelSpA
Radyolojik dönem
AS (Modifiye New York Kriterleri)
1984
Zaman (yıl)
Rudwaleit, et al. Arthritis Rheum 2005;52:1000-8
Radyografik sakroiliitkriterini (henüz!) karşılamayan
hastalar)

Bel/sırt ağrısıBel/sırt ağrısı
Radyolojik sakroiliit
Bel/sırt ağrısıSindesmofitler
Evre 1? Evre 2? Evre 3?

(Predominant) axSpA=• nr-axSpA• AS (radyografik axSpA)Her ikisi de psoriazis ve/veya IBH ile ilişkili olabilirPrimer veya sekonder axSpA denilmiyor:(Ps ve/veya IBH ile birlikte axSpA)
(Predominant) perSpA=• PsA veya Ps ile birlikte perSpA• IBH ile birlikte perSpA• ReA• Undiferansiye perSpA

ASAS kriterlerini karşılamayan ancakpotansiyel olarak axSpA olarak tanı
konulabilecek hastalar

ASAS kriterlerini karşılamayan ancakpotansiyel olarak perSpA olarak tanı
konulabilecek hastalar

Aksiyal SpA farklı bir antite midir?
GESPİC:• 10 yıl semptom süresi olan 236 AS ve• 5 yıl semptom süresi olan 226 modifiye
ESSG nonradyografik aksiyal SPA’lı hasta
• Tüm klinik özellikleri (HLA B27 dahil) gruplar arasında farklı değildir


Kimi niçin refere (sevk) edelim?
• Aksiyal ve periferik SpA hastaların ayrı ayrı
sınıflanması avantajlı?
• Preradyografik evresindeki hastalarda
yapılan klinik çalışmalar başlanmış

• DMARD’lar etkili değil
– TNF öncesi vs sonrası
• Aktivite, fonksiyon, mobilite, artrit, entezit ve AFR
• MRI aktivitesi baskılanabilir
• Kısa hastalık süresi ve iyi fonksiyon iyi yanıt belirteçleri

Kimi niçin refere (sevk) edelim?
• Bel ağrısı genel popülasyonda çok sık ve çoğunlukla non-spesifik ama çoğu kez birinci basamağa veya romatoloji dışı uzmanlıklara gidiyorlar
• Bel ağrısı olanlarda aksiyal SpA sıklığı %5
olarak tahmin edilmekte(y)di(r)
Underwood et al. 1995:1074
• Yakın dönemde Çin’de kronik bel ağrısı prevalansı %7.2
• Kronik bel ağrısı olanlarda axSpA sıklığı %11.7• Tahmini toplumda axSpA prevalansı %0.8
Liao ZT et al. Scand J Rheumatol 2009:455




Birinci basamakta gerçekten durum ne?Kronik (>2 ay <10 yıl) ve genç başlangıçlı (16-45 yaş) bel ağrısıhastalarında (Ortopedi pratiği!!!)

<45 yaş ve >2 ay <10 yıl süreli bel ağrısı olan hastalarda(n=950) IBP hangi özellikleri axSpA tanısı ile dahafazla ilişkili

Birinci basamakta IBP hastalarında durum ne?
SpA sıklığı %33 (30/92) ve
Bunların %50 AS

Hangi özellikleri olan hastaları sevk edelim?

Kronik bel ağrılı hasta
İnflamatuvar bel ağrısı LR 3 .7
AS/Aksiyel uSpA > % 90
Yüksek akut faz reaktanları LR 2 .5
Topuk ağrısı (entezit) LR 3 .4
Periferal artrit LR 4 .0
Daktilit LR 4 .5
Akut ön üveit LR 7 .3
Olası aile öyküsü LR 6 .4
NSAII’lara iyi yanıt LR 5 .1
HLA-B27 (beyazlarda) LR 9 .0
Kesin sakroiliit (X-ray) LR 20
MRI (STIR) SI eklem (& ) LR 9 .0
5% AS/Axial uSpA
Underwood & Dawson.
Brit J Rheumatol 1995
3.7 x 5.1 x 9.0 x 9.0
LR çarpımı >> 200
Rudwaleit, Khan & Sieper. Arthritis Rheum. 2005; 52:1000-1008.
AS/Aksiyel uSpA’lerin Bazı Klinik Özelliklerinin Likelihood Ratio larına göre Tanı

Hangi özellikleri olan hastaları sevk edelim?
NATURE REVIEWS | RHEUMATOLOGY VOLUME 8 | MAY 2012 | 265
However, fulfillment of one, two or all three of these fea-
tures was not required. As imaging of SIJ is sometimes
performed in primary care, physicians could also refer
patients of the target population if sacroiliitis was indi-
cated by any already available imaging modality (including
radiography, CT, scintigraphy and MRI), but the ordering
of such imaging tests was not encouraged.
Overall, 350 patients of the target population were
referred and a diagnosis of axSpA was made in 45.4%.
AxSpA was diagnosed in 34.2% who were referred using
a single parameter, but this value increased to 62.6% of
patients who met at least two referral parameters. If IBP
was the only referral parameter, axSpA was diagnosed
in 27% of patients, and if HLA-B27 was the only param-
eter, axSpA was diagnosed in 46%. Suspected sacroili-
itis on imaging as the only referral parameter yielded a
diag nosis of axSpA in only 26% of patients. Among the
patients diagnosed with axSpA, 50.3% were classified as
having AS and 49.7% nonradiographic axSpA.37 This first
proof-of-concept study therefore confirmed that a refer-
ral strategy can be effective. The study also confirmed
the expected superiority of HLA-B27 testing over IBP
regarding the yield of diagnosis of axSpA: 1 in 3.7 patients
referred with IBP, and 1 in 2.1 patients with a positive
HLA-B27 test were diagnosed with axSpA. The overall
higher than expected rate of positive diagnoses in this
study might reflect preselection of patients by the refer-
ring physicians, in that patients in whom SpA was already
strongly con sidered, but not diagnosed, were presumably
preferentially referred.
In a second small study from Austria,45 345 general
practitioners received a folder explaining the Calin cri-
teria for IBP and were asked to refer patients younger than
45 years who fulfilled the criteria. Of 92 referred patients,
a diagnosis of SpA was made in 30 (33%). Neck pain and
reduced cervical spine sagittal movement was negatively
associated with SpA, whereas HLA-B27 positivity and an
elevated CRP level contributed to a diagnosis of axSpA.45
National multicenter study
In a national multicenter study coordinated in Germany,38
we aimed to confirm the data from the monocenter
study37 in a broader setting (Table 2). This study, referred
to as MASTER (multicentre AS survey trial to evaluate
and compare referral parameters in early SpA) included
259 physicians across the country who referred patients
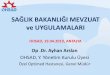
Chronic low back pain (> 3 months)Age at onset ≤45 years
HLA-B27 positiveor
Refer to rheumatologist for further evaluation
In ammatory back pain■ Morning stiffness >30 min■ Pain at night or ear ly morning■ Improvement by exercise
Sacroiliitis on imaging(only if imaging is already available)■ Radiography or CT■ MRI■ Scintigraphy
Figure 2 | Proposed referral strategy for axial
spondyloarthritis for primary care physicians. Patients who
present with chronic low back pain and age of onset
≤45 years can be sent to a rheumatologist for assessment
if they have inflammatory back pain or are HLA-B27 positive.
Adapted with permission from the BMJ Group © Sieper, J. &
Rudwaleit, M. Ann. Rheum. Dis. 64, 659–663 (2009).
Table 1 | Comparison of clinical and laboratory SpA features relevant for axial SpA
Parameter Sensitivity* %
Specificity* %
Sensitivity %(best representative estimate)
Specificity %(best representative estimate)
Positive likelihood ratio‡
In ammatory back pain 38–95 76–100 75 76 3.1
Heel pain (enthesitis) 16–52 89–96 37 89 3.4
Peripheral arthritis 26–62 91–100 40 90 4.0
Dactylitis 12–27 96–99 18 96 4.5
Anterior uveitis 10–22 97–100 22 97 7.3
Psoriasis 1–17 96 10 96 2.5
IBD 2–7 99 4 99 4.0
Positive family histor y for AS, reactive
arthritis, IBD, psoriasis, anterior uveitis
7–36 93–100 32 95 6.4
Response to NSAIDs 64–77 75–85 77 85 5.1
Elevated acute phase reactants (CRP) 38–69 67–100 50 80 2.5
HLA-B27 83–96 91–96 90 90§ 9.0
MRI of sacroiliac joints 54–93 83–100 90 || 90 || 9.0
* For the details of the primary literature please refer to Supplementary reference list (Supplementary Table 1 online). ‡Positive likelihood ratio refers to sensitivity/ (1-specificity); in most Western European populations this ratio ranges between 5–10%, corresponding to a specificity of 90–95%. §The specificity
figure depends on the background prevalence in the population. ||No gold standard is available to assess the true sensitivity of sacroiliitis on MRI in axial SpA. The reported specificities depend largely on type of control group, technical performance, and interpretation of MRI findings. Abbreviations: AS, ankylosing spondylitis; CRP, C-reactive protein; IBD, inflammatory bowel disease; SpA, spondyloarthritis. Adapted with permission from the BMJ Group © Rudwaleit, M. et al.
Ann. Rheum. Dis. 63, 535–543 (2004).
FOCUS ON SPONDYLOARTHRITIS
© 2012 Macmillan Publishers Limited. All rights reserved


HLA-B27 ile vs IBP ile tarama
• Duyarlılık (90% v 75%),
• Özgüllük (90% v 75%),
• axSpA tanısı için daha az sayıda hasta (1/3 v 1/7)
Ancak maliyeti ve sık olarak kullanılmıyor
Görüntüleme vs IBP ile tarama
• Duyarlılık (90% v 75%),
• Özgüllük (90% v 75%),
Ancak yorumlama uzmanlı gerektiriyor
Birinci basamak çekmesin ama varsa kullansın (!)


Tek bir tarama bulgusu ile refere etme dahakullanışlı olabilir! MASTER çalışması


• Known extra-articular manifestations



Semptom süresi uzadıkça refere edilenhastalarda daha yüksek oranda AS tanısıkonulabiliyor

ORIGINAL ARTICLE
Comparison of rates of referral and diagnosisof axial spondyloarthr itis before and after an ankylosingspondylitis public awareness campaign
Andrew A. Harrison &Chr istoffel Badenhorst &
Sandra Kirby &Douglas White &Josie Athens &
Simon Stebbings
Received: 13 October 2013 /Revised: 24 January 2014 /Accepted: 20 February 2014# Clinical Rheumatology 2014
Abstract The objective of this research is to measure the
effect of anational ankylosing spondylitis (AS) public aware-
ness campaign on numbers of referrals for suspected AS and
numbers of cases diagnosed with axial spondyloarthritis
(SpA). A television advertising campaign was conducted by
Arthritis New Zealand in 2011 to raise public awareness of
AS. A retrospectiveanalysiswasmadeof referralsreceivedby
the three rheumatology services 3 months before the cam-
paignstartedand 3 monthsafter thecampaignended. Theage,
gender, number of referrals for suspected AS and number of
referrals resulting in a diagnosis of axial SpA were recorded.
Independent analysis showed that the awareness campaign
reached 82 % of theprimary target audience. In the3 months
after theawarenesscampaign, therewasasignificant increase
in referrals for suspected AS compared with the 3 months
before the campaign (54 vs. 88, 63 %, p=0.0056). Referrals
for other conditions did not change. The number of referrals
resulting in adiagnosisof axial SpA also increased (27 vs. 44,
63 %, p=0.0576). The mean agesof thepatients referred and
of those diagnosed with axial SpA did not change. The
male/female ratio was 1:1 among the referrals for suspected
AS and 2:1 in referrals diagnosed with axial SpA, beforeand
after the campaign. The Arthritis New Zealand AS public
awareness campaign was associated with a significant in-
crease in referrals to rheumatology services for suspected
AS and an increase in the diagnosis of axial SpA in clinics.
Keywords Ankylosingspondylitis . Axial spondyloarthritis .
Publicawareness . Referral rates . Servicedelivery
Introduction
Ankylosing spondylitis(AS) isapotentially disabling chronic
inflammatory disease predominantly affecting the spine and
sacroiliac joints that is associated with very significant nega-
tive effects on quality of life [1]. The clinical outcome is
variable and unpredictable, but the severity of the disease is
defined by the course within the first 10 years of the onset of
symptoms[2]. Theopportunity to interveneat thisearly stage
of diseaseisoften hampered by failureto distinguish ASfrom
more common causes of back pain [3], which can result in a
delay between the onset of symptoms and diagnosis of up to
11 years [4].
The delay may be exacerbated by the perception amongst
health professionals that spinal limitation and radiographic
changes are necessary for the diagnosis of AS, a perception
re-enforcedby themodifiedNew York criteria[5], whichhave
been used for classification in themajority of theASliterature
in the last three decades [6]. These criteria define a group of
patients with relatively late-stage disease due to the require-
ment for radiographic sacroiliitis. More recently, the ASAS
criteria [7] for axial spondyloarthritis (axial SpA) have been
A. A. Harrison (* )
Department of Medicine, University of Otago, Wellington, New
Zealand
e-mail: [email protected]
C. Badenhorst : S. Stebbings
Department of Medicine, University of Otago, Dunedin, New
Zealand
S. Kirby
Arthritis New Zealand, Wellington, New Zealand
D. White
Rheumatology Department, Waikato Hospital, Hamilton, New
Zealand
J. Athens
Preventiveand Social Medicine, University of Otago, Dunedin, New
Zealand
Clin Rheumatol
DOI 10.1007/s10067-014-2551-0


262 | MAY 2012 | VOLUME 8 www.nature.com/ nrrheum
Endokrinologikum
Berlin, Jägerstrasse 61,
10117 Berlin, Germany
(M. Rudwaleit).
Department of
Medicine, Charité
University Medicine,
Campus Benjamin
Franklin,
Hindenburgdamm 30,
12203 Berlin, Germany
(J. Sieper).
Correspondance to:
M. Rudwaleit
martin.rudwaleit@
endokrinologikum.com
Referral strategies for early diagnosis of axial spondyloarthritisMartin Rudwaleit and Joachim Sieper
Abstract | The spectrum of HLA-B27-associated inflammatory spine diseases is referred to as axial
spondyloarthritis (axSpA). AxSpA encompasses established ankylosing spondylitis (AS) but also
nonradiographic axSpA, and can be classified according to the Assessment of SpondyloArthritis international
Society classification criteria for axSpA. Specific and effective therapy for axSpA includes education,
physiotherapy, NSAIDs and biologic agents, as appropriate. Patients with axSpA, however, are often diagnosed
late in the course of the disease. As specific therapy is available, the effective identification of those
individuals who are likely to have axSpA among patients with chronic back pain in primary care and their
subsequent referral to a rheumatologist for establishing a correct diagnosis is worth pursuing. Candidate
referral parameters that can easily be applied to patients with chronic back pain and age at onset ≤45 years
(the target population) include inflammatory back pain (IBP) and positivity for HLA-B27. Following diagnostic
work-up by a rheumatologist, these referral parameters, either alone or in combination, have led to the
diagnosis of as many as 33–45% of patients within this target population with axSpA, 41–62% of whom had
undiagnosed AS. Thus, educating primary care physicians on the value of IBP and HLA-B27 testing within
this target population, and referral to a rheumatologist if one of these parameters is positive, is a promising
approach to reduce the long delay in diagnosing patients with axSpA.
Rudwaleit, M. & Sieper, J. Nat. Rev. Rheumatol. 8, 262–268 (2012); published online 10 April 2012; doi:10.1038/ nrrheum.2012.39
Introduct ionAnkylosing spondylitis (AS) is the prototype subgroup of
spondyloarthritis (SpA)—a group of disorders character-
ized by similar clinical manifestations, a common genetic
basis, and similar treatment options.1,2 Radiographic
sacroiliitis has been considered a hallmark of AS and is
present in at least 90% of patients with established disease.
Radiographic sacroiliitis is also a requirement for the fulfill-
ment of the modified New York criteria for AS established
in 1984, which are widely used as classification and diag-
nostic criteria in clinical practice.3 Making a diagnosis of
AS, however, is often delayed by 6–8 years, mainly because
definite evidence of sacroiliitis on plain radiographs is
not readily observed during the early stages of disease.4
Moreover, in early disease the patient’s posture does not
usually indicate AS. Although chronic low back pain is
often the first and predominant symptom of AS, back pain
is commonly observed in the general population, and only
approximately 5% of individuals with such pain are con-
sidered to have AS or axial SpA (axSpA).5,6 Referral strate-
gies for primary care physicians could, therefore, be useful
to channel those patients with chronic back pain who are
most likely to have early axSpA to rheumatologists.
The concept of axial SpA MRI has revolutionized the imaging of sacroiliitis. Active
inflammation of the sacroiliac joints (SIJ), with or without
signs of structural damage, can be accurately visual-
ized by MRI, particularly when plain radiographs of SIJ
seem normal or equivocal.7,8 Sacroiliitis on MRI images,
together with clinical manifestations such as inflamma-
tory back pain (IBP), arthritis, enthesitis, uveitis, associ-
ated psoriasis or inflammatory bowel disease, response of
back pain to NSAIDs, positivity for HLA-B27 and a posi-
tive family history for SpA, have been incorporated into a
diagnostic algorithm,9 a diagnostic probability approach
based on likelihood ratios,4,10 and the Assessment of
SpondyloArthritis international Society (ASAS) clas-
sification criteria for axSpA.11,12 According to the ASAS
criteria, a patient with chronic back pain and age at onset
≤45 years can be classified as having axSpA if sacroiliitis
is observed on plain radiographs or, alternatively, by MRI
in the presence of at least one further clinical SpA feature
(referred to as the imaging arm). Patients can also be clas-
sified as having axSpA using a ‘clinical arm’ in which the
patient must be positive for HLA-B27 and have at least two
additional SpA features (Box 1).12
The term axSpA has been used to describe the entire
spectrum of SpA that has predominant axial involvement,
irrespective of the presence of structural damage on plain
radiographs.4 Accordingly, axSpA comprises established
AS at one end and an early stage of axSpA (referred to as
‘nonradiographic axSpA’) at the other end (Figure 1). A
substantial proportion of patients with nonradiographic
Competing interests
M. Rudwaleit declares associations with the following
companies: Abbott, Chugai Pharmaceutical Co. (a subsidiary of
Roche), MSD, Pfizer and UCB. J. Sieper declares associations
with the following companies: Abbott, Bristol–Myers Squibb,
Merck, Pfizer, Roche and UCB. See the article online for full
details of the relationships.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved
262 | MAY 2012 | VOLUME 8 www.nature.com/ nrrheum
Endokrinologikum
Berlin, Jägerstrasse 61,
10117 Berlin, Germany
(M. Rudwaleit).
Department of
Medicine, Charité
University Medicine,
Campus Benjamin
Franklin,
Hindenburgdamm 30,
12203 Berlin, Germany
(J. Sieper).
Correspondance to:
M. Rudwaleit
martin.rudwaleit@
endokrinologikum.com
Referral strategies for early diagnosis of axial spondyloarthritisMartin Rudwaleit and Joachim Sieper
Abstract | The spectrum of HLA-B27-associated inflammatory spine diseases is referred to as axial
spondyloarthritis (axSpA). AxSpA encompasses established ankylosing spondylitis (AS) but also
nonradiographic axSpA, and can be classified according to the Assessment of SpondyloArthritis international
Society classification criteria for axSpA. Specific and effective therapy for axSpA includes education,
physiotherapy, NSAIDs and biologic agents, as appropriate. Patients with axSpA, however, are often diagnosed
late in the course of the disease. As specific therapy is available, the effective identification of those
individuals who are likely to have axSpA among patients with chronic back pain in primary care and their
subsequent referral to a rheumatologist for establishing a correct diagnosis is worth pursuing. Candidate
referral parameters that can easily be applied to patients with chronic back pain and age at onset ≤45 years
(the target population) include inflammatory back pain (IBP) and positivity for HLA-B27. Following diagnostic
work-up by a rheumatologist, these referral parameters, either alone or in combination, have led to the
diagnosis of as many as 33–45% of patients within this target population with axSpA, 41–62% of whom had
undiagnosed AS. Thus, educating primary care physicians on the value of IBP and HLA-B27 testing within
this target population, and referral to a rheumatologist if one of these parameters is positive, is a promising
approach to reduce the long delay in diagnosing patients with axSpA.
Rudwaleit, M. & Sieper, J. Nat. Rev. Rheumatol. 8, 262–268 (2012); published online 10 April 2012; doi:10.1038/ nrrheum.2012.39
IntroductionAnkylosing spondylitis (AS) is the prototype subgroup of
spondyloarthritis (SpA)—a group of disorders character-
ized by similar clinical manifestations, a common genetic
basis, and similar treatment options.1,2 Radiographic
sacroiliitis has been considered a hallmark of AS and is
present in at least 90% of patients with established disease.
Radiographic sacroiliitis is also a requirement for the fulfill-
ment of the modified New York criteria for AS established
in 1984, which are widely used as classification and diag-
nostic criteria in clinical practice.3 Making a diagnosis of
AS, however, is often delayed by 6–8 years, mainly because
definite evidence of sacroiliitis on plain radiographs is
not readily observed during the early stages of disease.4
Moreover, in early disease the patient’s posture does not
usually indicate AS. Although chronic low back pain is
often the first and predominant symptom of AS, back pain
is commonly observed in the general population, and only
approximately 5% of individuals with such pain are con-
sidered to have AS or axial SpA (axSpA).5,6 Referral strate-
gies for primary care physicians could, therefore, be useful
to channel those patients with chronic back pain who are
most likely to have early axSpA to rheumatologists.
The concept of axial SpA MRI has revolutionized the imaging of sacroiliitis. Active
inflammation of the sacroiliac joints (SIJ), with or without
signs of structural damage, can be accurately visual-
ized by MRI, particularly when plain radiographs of SIJ
seem normal or equivocal.7,8 Sacroiliitis on MRI images,
together with clinical manifestations such as inflamma-
tory back pain (IBP), arthritis, enthesitis, uveitis, associ-
ated psoriasis or inflammatory bowel disease, response of
back pain to NSAIDs, positivity for HLA-B27 and a posi-
tive family history for SpA, have been incorporated into a
diagnostic algorithm,9 a diagnostic probability approach
based on likelihood ratios,4,10 and the Assessment of
SpondyloArthritis international Society (ASAS) clas-
sification criteria for axSpA.11,12 According to the ASAS
criteria, a patient with chronic back pain and age at onset
≤45 years can be classified as having axSpA if sacroiliitis
is observed on plain radiographs or, alternatively, by MRI
in the presence of at least one further clinical SpA feature
(referred to as the imaging arm). Patients can also be clas-
sified as having axSpA using a ‘clinical arm’ in which the
patient must be positive for HLA-B27 and have at least two
additional SpA features (Box 1).12
The term axSpA has been used to describe the entire
spectrum of SpA that has predominant axial involvement,
irrespective of the presence of structural damage on plain
radiographs.4 Accordingly, axSpA comprises established
AS at one end and an early stage of axSpA (referred to as
‘nonradiographic axSpA’) at the other end (Figure 1). A
substantial proportion of patients with nonradiographic
Competing interests
M. Rudwaleit declares associations with the following
companies: Abbott, Chugai Pharmaceutical Co. (a subsidiary of
Roche), MSD, Pfizer and UCB. J. Sieper declares associations
with the following companies: Abbott, Bristol–Myers Squibb,
Merck, Pfizer, Roche and UCB. See the article online for full
details of the relationships.
REVIEWS
© 2012 Macmillan Publishers Limited. All rights reserved

TEŞEKKÜRLER