Embed Size (px)
Citation preview

82
An Interesting Cause of Acute Neck-Chest Pain and Dyspnea: Spontaneous PneumomediastinumAni Gelişen Boyun-Göğüs Ağrısı ve Nefes Darlığının İlginç Bir Nedeni: Spontan Pnömomediastinum
ÖZETSpontan pnömomediastinum mediastende hava varlığı olarak tanımlanabilir ve nadir görülen bir
klinik tablodur. Oluşum mekanizması belirsizdir ancak oluşumu için alveolar ve intrabronşiyal basınç artışı sorumlu tutulmaktadır. Spontan pnömomediastinumun en sık tetikleyicileri akut astım atağı, diyabetik ketoasidoz, sigara, esrar veya kokain kullanımı, tüplü dalış, uçakla seyahat, aşırı egzersiz, aşırı kusma veya öksürüktür. Göğüs-boyun ağrısı ve nefes darlığı başlıca semptomlardır. Şüpheli olgularda tanı çoğunlukla akciğer grafisiyle konabilir veya toraks BT ile doğrulanabilir. Tedavi yaklaşımı; oksijen, analjezikler ve hastanın yakın takibidir. Tedavi yüz güldürücüdür ve tekrarlama düşüktür. Tansiyon pneumomediastinum, tansiyon pnömotoraks veya mediastinit saptanırsa cerrahi tedavi gerekebilir.
Çalışmamızda spontan pnömomediastinum tanısı alan iki olguyu sunmayı amaçladık. Birinci olgu 17 yaşında bir erkekti. Yaklaşık 2 metre derinlikteki denize dalıştan 8 saat sonra acil servise nefes darlığı, non-prodüktif öksürük, göğüs-boyun ağrısı şikayetleri ile başvurdu. İkincisi olgu ise, akut nefes darlığı ve göğüs ağrısı ile başvuran 20 yaşındaki bir kadındı. Anamnezde 2 gün önce şiddetli öksürük atağı geçirdiği öğrenildi. Her iki hastada akciğer grafisi ve toraks BT'de pnömomediastinum ve cilt altı amfizemi saptandı. Hastalar konservatif tedavi uygulama ve takip amaçlı hastaneye yatırıldı. Kontrol akciğer grafileriyle takip sonrası sorunsuz taburcu edildiler.
Dispne, akut boyun ve göğüs ağrısı ile acil servise başvuran olgularda spontan pnömomediastinum akla getirilmelidir. Literatürde nadir olmasına rağmen bu durum, tüpsüz dalış veya şiddetli öksürük sonrası bile gelişebilir.
Anahtar kelimeler: spontan, pnömomediastinum, dalış, öksürük
ABSTRACTSpontaneous pneumomediastinum can defined as the presence of air in the mediastinum and it is a
rare clinical entity. The formation mechanism is unclear but rise of alveolar and intrabronchial pressure is blamed for its formation. The most frequent triggers of spontaneous pneumomediastinum are acute asthma attack, diabetic ketoacidosis, smoking marijuana or cocaine, scuba diving, traveling by plane, excessive exercise, excessive vomiting or cough. Chest-neck pain and dyspnea are the main symptoms. Diagnosis can be confirmed mostly by chest radiography or thorax CT for suspected cases. The treatment of choice is oxygen, analgesics and monitoring the patient. It has a satisfactory outcomes and the recurrence is low. Surgical tretament may be necessary if tension pneumomediastinum, tension pneumothorax or mediastinitis determined.
We report two cases with spontaneous pneumomediastinum. First one was an 17-year-old boy who presented emergency service with dyspnea, non-productive cough, chest-neck pain 8 h after the diving about 2 meter depth under the sea. Second one was a 20-year-old woman presented emergency service with acute dyspnea and chest pain. She was complained severe cough 2 days ago in her history. In both patients chest radiography and thorax CT revealed pneumomediastinum and subcutaneous emphysema. The patients admitted to the hospital for conservative treatment and follow up. They were discharged without any problems after follow up with control chest radiography.
If patients refer to emergency department with dyspnea, acute neck and chest pain, spontaneous pneumomediastinum should be remembered. Although rare in the literatüre, this condition can develop while diving tubeless or with severe coughing.
Keywords: spontaneous, pneumomediastinum, diving, cough
AUTHORS / YAZARLAR
Fazlı YanıkDepartment of Thoracic Surgery, Trakya University School of Medicine, Edirne, Turkey
Yekta Altemur KaramustafaogluDepartment of Thoracic Surgery, Trakya University School of Medicine, Edirne, Turkey
Yener YorukDepartment of Thoracic Surgery, Trakya University School of Medicine, Edirne, Turkey
CASE REPORT / OLGU SUNUMU 2017
Corresponding Author / İletişim içinAssist. Prof. Fazlı Yanık, MDTrakya University School of Medicine, Department of Thoracic Surgery, Edirne, TurkeyE-mail: [email protected] of submission: 27.02.2017 / Date of acceptance: 07.08.2017

83
Introduction
Spontaneous pneumomediastinum can defined as the presence of air in the mediastinum and it is a rare clinical entity which usually occurs in the absence of pulmonary disease. It mostly affects young males, with a male:female ratio of 8:1, and presents a diagnostic challenge. The formation mechanism is unclear but alveolar and intrabronchial pressure rise is blamed for it’s formation. Especially acute asthma attack, diabetic ketoacidosis, smoking marijuana or cocaine, scuba diving, traveling by plane, excessive exercise, excessive vomiting or cough can cause of it. Shallow water breath hold diving is extremely rare for sponaneos pneumomediastinum. Chest pain and neck pain are the main symptoms. Diagnosis can be confirmed mostly by chest radiography or thorax CT for suspected cases. The treatment of choice is oxygen, analgesics and monitoring the patient. It has a satisfactory outcomes and the recurrence is low. Surgical tretament may be necessary if tension pneumomediastinum, tension pneumothorax or mediastinitis determined (1-3). We present two cases of spontaneous pneumomediastinum diagnosed in emergency service with acute chest–neck pain and dyspnea.
Case 1 An 17-year-old adolescent boy presented
emergency service with dyspnea, non-productive cough and pleuritic chest pain radiating to both sides of his neck beginning 8 h after he had been jumping from a pontoon and diving about 2 meter depth under the North Aegean sea. Meanwhile he tried to breath-hold in shallow water for as long as possible. He repeated this about 2 times over an hour. There was no reported loss of consciousness, seizure or neurologic complaints upon surfacing or afterwards. On physical examination, the patient was conscious, oriented and cooperative. Blood pressure was 110/60 mm Hg, and oxygen saturation was measured 98% by pulse oxymeter on room air. Pulse was 78 beats/min, and respiration rate was 18 breaths/min. ECG, blood count, C-reactive protein, troponin T, troponin I and blood gas analysis were within normal limits. He has no respiratory distress. Palpation of bilateral neck revealed anterolateral crepitus depending on the
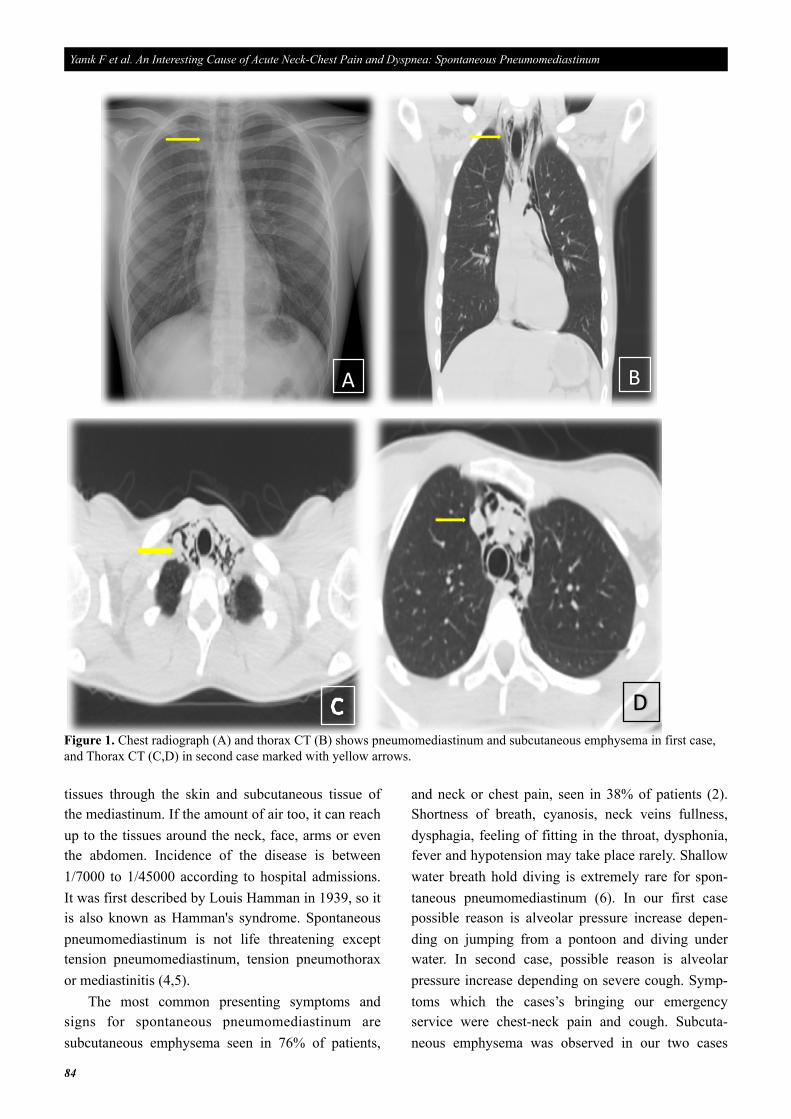
subcutaneous emphysema and auscultation of heart and lungs was unremarkable. Other system exami- nations were unremarkable too. Chest radiography and thorax CT (Computerized tomography of the thorax) showed pneumomediastinum and subcuta- neous emphysema on the both side of the neck (Figure 1). The case was admitted to the hospital for observation and symptomatic relief. He was treated conservatively with 100% oxygen via nasal mask for 24 h, and given paracetamol for pain control. Next day, he was asymptomatic and pneumomediastinum had resolved. He was discharged after two days, and 10 days later control chest radiography was normal.
Case 2
A 20-year-old girl presented with acute dyspnea and chest pain. She complained severe cough 2 days ago in her history. On physical examination, the patient was conscious, oriented and cooperative. Blood pressure was 120/70 mm Hg, and oxygen saturation was measured 96% by pulse oxymeter on room air. Pulse was 68 beats/min, and respiration rate was 14 breaths/min. ECG, blood parameters were within normal limits. She has no respiratory distress. Palpation of bilateral neck revealed anterolateral crepitus depending on the subcutaneous emphysema and auscultation of heart and lungs was unremar- kable. Other systems examinations were normal. Chest radiography and thorax CT revealed pneumomediastinum and servical subcutaneous emphysema. She was hospitalized and treated conservatively with 100% oxygen via nasal mask for 24 h, and given paracetamol for pain control. Two days later she was asymptomatic and pneumo- mediastinum had resolved. She was discharged after three days of follow up and 10 days later control chest radiography was normal.
Discussion
Pneumomediastinum can be categorized as spontaneous or traumatic. Traumatic pneumo- mediastinum is caused by blunt or penetrating trauma to the chest, or iatrogenic injury, such as produced by mechanical ventilation or thoracic surgery. Generally, the air starting proceeding from the damaged area (terminal alveoli, bronchi, trachea, esophagus) to the
Euras J Fam Med 2017;6(2):82-86
84
tissues through the skin and subcutaneous tissue of the mediastinum. If the amount of air too, it can reach up to the tissues around the neck, face, arms or even the abdomen. Incidence of the disease is between 1/7000 to 1/45000 according to hospital admissions. It was first described by Louis Hamman in 1939, so it is also known as Hamman's syndrome. Spontaneous pneumomediastinum is not life threatening except tension pneumomediastinum, tension pneumothorax or mediastinitis (4,5).
The most common presenting symptoms and signs for spontaneous pneumomediastinum are subcutaneous emphysema seen in 76% of patients,
and neck or chest pain, seen in 38% of patients (2). Shortness of breath, cyanosis, neck veins fullness, dysphagia, feeling of fitting in the throat, dysphonia, fever and hypotension may take place rarely. Shallow water breath hold diving is extremely rare for spon- taneous pneumomediastinum (6). In our first case possible reason is alveolar pressure increase depen- ding on jumping from a pontoon and diving under water. In second case, possible reason is alveolar pressure increase depending on severe cough. Symp- toms which the cases’s bringing our emergency service were chest-neck pain and cough. Subcuta- neous emphysema was observed in our two cases
Yanık F et al. An Interesting Cause of Acute Neck-Chest Pain and Dyspnea: Spontaneous Pneumomediastinum
A B
DFigure 1. Chest radiograph (A) and thorax CT (B) shows pneumomediastinum and subcutaneous emphysema in first case, and Thorax CT (C,D) in second case marked with yellow arrows.

85
with both radiological and physical examination.Diving-related diseases include decompression
sickness, baro-sinusitis, perforated tympanic mem- brane, temporo-mandibular joint dysfunction, arterial gas embolism, and hyperbaric-triggered migraine. Pulmonary airleaks may result from pulmonary barotrauma sustained during scuba or compressed air diving, with rupture of the terminal alveoli secondary to increased intrathoracic pressure. Air tracks along the peri-bronchial vascular sheaths towards the hilum of the lung and spreads through the tissue plane, causing subcutaneous emphysema, pneumoperi- toneum, pneumothorax, and even pneumopericar- dium. The incidence of diving-related pneumo- mediastinum is unclear (7). Despite the lack of scuba diving in our first case we believe that the same mechanism occurs for pneumomediastinum. Other diving-related diseases not followed in the case.
Diagnosis of pneumomediastinum is largely based on clinical findings and imaging. In most cases, it can be demonstrated on routine chest radiography, although the diagnosis may be missed up to 30% of cases, especially when it is not obvious. Thorax CT increases the chance of diagnosis and provides additional information about any additional patho- logy. Esophagogram may also help for the cases considered in the diagnosis of esophageal rupture. Electrocardiography may reveal reduced voltage, ST segment changes or axis deviations in some cases (8). Vivek et al. (1) reported 62 adult consecutive spon- taneous pneumomediastinum cases in a retrospective study. Forty-seven of patients (76%) were hospi- talized for a median duration of 2.5 day. Additional diagnostic procedures were defined in 27 patients (44%) and included contrast esophagography, bronchoscopy, and esophagogastroduodenoscopy. Pneumothorax was seen in 32% of cases but less than one-third of these patients underwent chest tube thoracostomy. For our two cases chest radiograph and physical examination was suspicious. Definitive diagnosis was reached with thorax CT. Electro- cardiography changes were not detected. Our first case was discharged after the second day and the other one was discharged after the third day when the air is completely resorbed.
When spontaneous pneumomediastinum diag-
nosis is established, the patient should be hospitalized and monitored for 24-36 hours to prevent potential complications. Treatment includes analgesic, continuous oxygen therapy and antibiotherapy if mediastinitis identified. In the presence of tension pneumomediastinum and tension pneumothorax air decompression with opening pretracheal cervical fascia or applying tube thoracostomy can be life-saving. Also importantly, patients who have esophageal perforation or mediastinitis in the setting of spontaneous pneumomediastinum require urgent and aggressive medical or surgical treatment (9,10). Only continuous oxygen therapy and paracetamol was sufficient for our cases’ treatment and control chest radiography 10 days later was normal. We did not determinate esophageal perforation or medias- tinitis in our cases.
The detection of spontaneous pneumomedias- tinum requires a high suspicion and should be considered in all cases with acute neck or chest pain who are presenting to the emergency departments or primary health care institutions. The most frequent triggers of spontaneous pneumomediastinum are asthma, vomiting, coughing, breath-holding and intense sport activities, but it is rarely associated with free shallow water diving (11). These patients should avoid diving, severe coughing, breath-holding, intense sport activities and manoeuvres creating forced expiration to lessen the risk of barotrauma.
Conclusion
Spontaneous pneumomediastinum is a rare entity whose etiology is not clear but probably alveolar barotrauma accused. It usually heals with oxygen and analgesic treatment. Surgical intervention may be necessary if tension pneumomediastinum, tension pneumothorax or mediastinitis determined. The cases who admitted emergency department with acute neck-chest pain and dyspnea this pathology should be remembered. Although rare in the literature this condition can develop while diving in even shallow waters or severe coughing.
Euras J Fam Med 2017;6(2):82-86
86
Yanık F et al. An Interesting Cause of Acute Neck-Chest Pain and Dyspnea: Spontaneous Pneumomediastinum
1. Vivek NI, Avni YJ, Jay HR. Spontaneous pneumomediastinum: analysis of 62 consecutive adult patients. Mayo Clin Proc 2009;84(5):417–21.
2. Damore DT, Dayan PS. Medical causes of pneumomediastinum in children. Clin Pediatr (Phila) 2001;40(2):87-91.
3. Kannappa Shankar Pani Y, Hart G, Yeo W. Spontaneous pneumomediastinum: a rare entity but not to be missed. Intern Med J 2017;47(6):709-10.
4. Dionísio P, Martins L, Moreira S, Manique A, Macedo R, Caeiro F, et al. Spontaneous pneumomediastinum: experience in 18 patients during the last 12 years. J
Bras Pneumol 2017;43(2):101-5.
5. Takada K, Matsumoto S, Hiramatsu T, Kojima E, Watanabe H, Sizu M, et al. Management of spontaneous pneumomediastinum based on clinical experience of 25 cases. Respir Med 2008;102(9):1329–34.
6. Chapdelaine J, Beaunoyer M, Daigneault P, et al. Spontaneous pneumomediastinum: are we over investigating?. J Pediatr Surg 2004;39(5):681-4.
7. Oh ST, Kim W, Jeon HM, Kim JS, Kim KW, Yoo SJ, et al. Massive pneumoperitoneum after scuba diving. J Korean Med Sci 2003;18(2):281-3.
8. Kaneki T, Kubo K, Kawashima A, Koizumi T,
Sekiguchi M, Sone S. Spontaneous pneumomediastinum in 33 patients: yield of chest computed tomography for the diagnosis of the mild type. Respiration 2000;67(4):408-11.
9. Ralp-Edwards AC, Pearson FG. Atypical presentation of spontaneous pneumomediastinum. Ann Thorac Surg 1994;58(6);1758-60.
10. Potz BA, Chao LH, Ng TT, Okereke IC. Clinical significance of spontaneous pneumomediastinum. Ann Thorac Surg 2017;104(2):431-5.
11. Shah S, Thomas S, Gibb E. Pneumomediastinum after shallow water diving. J Emerg Med 2009;36(1):76-7.
References





























