Embed Size (px)
Citation preview

Ananda Allan
Senior Health Intelligence Analyst
‘The Quality Outcomes Framework (QOF):
Can it be used for more than just paying GPs?’
‘The Quality Outcomes Framework (QOF):
Can it be used for more than just paying GPs?’
Ananda AllanSenior Health Intelligence Analyst
NHS Dumfries & Galloway
Ananda AllanSenior Health Intelligence Analyst
NHS Dumfries & Galloway

Ananda Allan
Senior Health Intelligence Analyst
Today’s talk will cover…Today’s talk will cover…
• What is the QOF?• What else can QOF be used for?
– Our understanding of patient populations
– Comparing disease registers– Geographical distribution of disease– Referral and Admission patterns
• What is the QOF?• What else can QOF be used for?
– Our understanding of patient populations
– Comparing disease registers– Geographical distribution of disease– Referral and Admission patterns

Ananda Allan
Senior Health Intelligence Analyst
About the QOFAbout the QOF• Started 2004 as part of new GP contract• “A voluntary system of financial
incentives… rewarding contractors (GPs) for good practice through participation in an annual quality improvement cycle”
• Pays GPs for:– looking after patients with specific chronic
illnesses – qualitative practice improvement measures
• 134 indicators overall in 2010/11 • 20 conditions across 80+ clinical indicators
• Started 2004 as part of new GP contract• “A voluntary system of financial
incentives… rewarding contractors (GPs) for good practice through participation in an annual quality improvement cycle”
• Pays GPs for:– looking after patients with specific chronic
illnesses – qualitative practice improvement measures
• 134 indicators overall in 2010/11 • 20 conditions across 80+ clinical indicators

Ananda Allan
Senior Health Intelligence Analyst
1. Patient Populations: accurate count of the full
practice lists…
1. Patient Populations: accurate count of the full
practice lists…• There are different ways of counting
D&G patients:– NRS (was GROS) estimate June 2010:
148,190– CHI residents May 2010: 154,184– CHP (QOF) headcount July 2010: 155,381
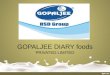
• There may not be much difference between CHI residents and CHP (1,200) but these patients belong to only 3 practices!
• There are different ways of counting D&G patients:– NRS (was GROS) estimate June 2010:
148,190– CHI residents May 2010: 154,184– CHP (QOF) headcount July 2010: 155,381
• There may not be much difference between CHI residents and CHP (1,200) but these patients belong to only 3 practices!

Ananda Allan
Senior Health Intelligence Analyst
700
470150
N.B. For those of you who are wondering why this doesn’t add up to 1,200… we have 200 patients living in D&G registered with an English GP in Longtown!

Ananda Allan
Senior Health Intelligence Analyst
This is important because:
This is important because:
• We can now calculate accurate GP practice activity rates using the CHP headcounts, thanks to the QOF
• Prior to the QOF, GP populations were not regularly published
• Publishing these figures nationally has forced transparency
• We can now calculate accurate GP practice activity rates using the CHP headcounts, thanks to the QOF
• Prior to the QOF, GP populations were not regularly published
• Publishing these figures nationally has forced transparency

Ananda Allan
Senior Health Intelligence Analyst
2. Disease Registers2. Disease Registers• Prior to the release of the QOF we
had two sources for disease prevalence:– Individual disease registers/audits
•Limited number of diseases and focus on acute activity: diabetes, stroke, renal failure, cancer audits
– Continuous Morbidity Recording (CMR)•70 ‘spotter’ practices producing age-
specific rates (evolved into PTI)– Or… write out to every practice and ask!
• Prior to the release of the QOF we had two sources for disease prevalence:– Individual disease registers/audits
•Limited number of diseases and focus on acute activity: diabetes, stroke, renal failure, cancer audits
– Continuous Morbidity Recording (CMR)•70 ‘spotter’ practices producing age-
specific rates (evolved into PTI)– Or… write out to every practice and ask!

Ananda Allan
Senior Health Intelligence Analyst
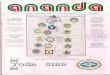
2788
61415834
0
1000
2000
3000
4000
5000
6000
7000
CMR Age-Specific Rates 2002applied to Board Population 2004
(All ages)
Local Diabetic Register (includes under 18s)
July 2004
QOF disease registerfor Diabetes (18+)
March 2005
Comparing Local Diabetes Register with CMR
Estimates…
Comparing Local Diabetes Register with CMR
Estimates…
Now SCI-DC Diabetes Register Co-ordinates with EMIS nightlyNow SCI-DC Diabetes Register Co-ordinates with EMIS nightly

Ananda Allan
Senior Health Intelligence Analyst
QOF disease prevalence figures are not without
problems…
QOF disease prevalence figures are not without
problems…Condition Prevalence Condition Prevalence
Stroke 2.3% Dementia 0.9%Palliative Care 0.2% CVD Risk 1.0%
New Depression 18+ 8.7% COPD 2.3%Mental Health 0.8% Chr Kidney Dis 18+ 3.0%
Learning Disability 18+ 0.4% CHD 5.1%Hypothyroidism 3.5% Cancer 1.9%
High Blood Pressure 14.8% Atrial Fibrillation 1.7%Heart Failure 0.9% Asthma 5.8%Epilepsy 18+ 0.7% Obesity 16+ 7.6%
Diabetes 17+ 4.7%
Condition Prevalence Condition Prevalence
Stroke 2.3% Dementia 0.9%Palliative Care 0.2% CVD Risk 1.0%
New Depression 18+ 8.7% COPD 2.3%Mental Health 0.8% Chr Kidney Dis 18+ 3.0%
Learning Disability 18+ 0.4% CHD 5.1%Hypothyroidism 3.5% Cancer 1.9%
High Blood Pressure 14.8% Atrial Fibrillation 1.7%Heart Failure 0.9% Asthma 5.8%Epilepsy 18+ 0.7% Obesity 16+ 7.6%
Diabetes 17+ 4.7%
The denominator is still ALL ages; The denominator is still ALL ages; overlap?overlap?

Ananda Allan
Senior Health Intelligence Analyst
3. Mapping the geographical burden of
disease
3. Mapping the geographical burden of
disease• Will QOF disease prevalence follow
patterns of area deprivation?• Can we add value to existing GIS
analysis?
• Will QOF disease prevalence follow patterns of area deprivation?
• Can we add value to existing GIS analysis?

Ananda Allan
Senior Health Intelligence Analyst
Different in Urban areas?

Ananda Allan
Senior Health Intelligence Analyst
4. Correlating Disease Prevalence to Acute Activity
4. Correlating Disease Prevalence to Acute Activity• Some studies make an a priori assumption
that disease prevalence correlates with emergency admissions
• It has been shown that recorded prevalence of COPD accounts for 21.9% of admission variance (the APHO estimated prevalence was an even better predictor, accounting for 45.1%) (Calderón-Larrañaga et al, Thorax 2011)
• However, local correlations have been disappointingly inconclusive
• Some studies make an a priori assumption that disease prevalence correlates with emergency admissions
• It has been shown that recorded prevalence of COPD accounts for 21.9% of admission variance (the APHO estimated prevalence was an even better predictor, accounting for 45.1%) (Calderón-Larrañaga et al, Thorax 2011)
• However, local correlations have been disappointingly inconclusive

Ananda Allan
Senior Health Intelligence Analyst
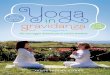
R2 = 0.0005
R2 = 0.0235
0%1%2%3%4%
5%6%7%8%9%
0 4 8 12 16 20 24 28
Indirectly Standardised Referral Rates per 1,000 Population (Age/Sex/SIMD09v2)
QO
F P
reva
lence
Coronary Heart Disease
Diabetes
R2 = 0.0005
R2 = 0.0235
0%1%2%3%4%
5%6%7%8%9%
0 4 8 12 16 20 24 28
Indirectly Standardised Referral Rates per 1,000 Population (Age/Sex/SIMD09v2)
QO
F P
reva
lence
Coronary Heart Disease
Diabetes
New Referral Rates to Cardiology
and Diabetes & Endocrinology vs. QOF Prevalence
New Referral Rates to Cardiology
and Diabetes & Endocrinology vs. QOF Prevalence
New Referrals New Referrals ≈ ≈ Incidence … Incidence … ≠ Prevalence?≠ Prevalence?

Ananda Allan
Senior Health Intelligence Analyst
R2 = 0.0729
0%1%2%3%4%
5%6%7%8%9%
0 2 4 6 8 10 12 14
Indirectly Standardised Emergency Admission Ratesper 1,000 Population (Age/Sex/SIMD09v2)
QO
F P
reva
lence
Coronary Heart Disease
R2 = 0.0729
0%1%2%3%4%
5%6%7%8%9%
0 2 4 6 8 10 12 14
Indirectly Standardised Emergency Admission Ratesper 1,000 Population (Age/Sex/SIMD09v2)
QO
F P
reva
lence
Coronary Heart Disease
Emergency Admission Rates for All Heart Disease
vs. QOF CHD Prevalence
Emergency Admission Rates for All Heart Disease
vs. QOF CHD Prevalence

Ananda Allan
Senior Health Intelligence Analyst
Conclusions from the published papers…
Conclusions from the published papers…
1. Bankart et al,Emerg Med J
(2011)[2 PCT England]
High Emg Adm = closer to hospital, small list size, older (removed CHD prevalence), white ethnicity, female, deprivation, not seeing own GP
2. Purdy et al, Public Health (2011) [All England]
High Emg Adm = deprivation, CHD prevalence, smoking but not QOF quality of care factors for CHD
3. Purdy et al, J Health Serv Res Policy (2011) [All England]
High Emg Adm = deprivation, Asthma and COPD prevalence, smoking, urban, closer to hospital, bed availability
4. Calderón-Larrañaga et al, Thorax (2011) [All England]
High Adm = deprivation, COPD QOF and undiagnosed prevalence, smoking, lower flu jabs, worse GP access/staffing

Ananda Allan
Senior Health Intelligence Analyst
So…So…• Too many other factors to use
prevalence in isolation?• Small rural board = insufficient
sample?• Under-diagnosis skewing figures (e.g.
COPD)?• Despite the results… Examining
outliers has led to new case-finding
• Too many other factors to use prevalence in isolation?
• Small rural board = insufficient sample?
• Under-diagnosis skewing figures (e.g. COPD)?
• Despite the results… Examining outliers has led to new case-finding

Ananda Allan
Senior Health Intelligence Analyst
In conclusion…In conclusion…• QOF has given added value to other
health information• What we really need is:
– Age/Sex breakdown of QOF prevalence– Knowledge of co-morbidity (overlap)
• QOF Calculator not designed to extract this (and does not hold this)
• We will continue to explore…
• QOF has given added value to other health information
• What we really need is: – Age/Sex breakdown of QOF prevalence– Knowledge of co-morbidity (overlap)
• QOF Calculator not designed to extract this (and does not hold this)
• We will continue to explore…

Ananda Allan
Senior Health Intelligence Analyst
AcknowledgmentsAcknowledgments
• Dr Andrew Carnon, Consultant in Public Health Medicine
• Carolyn Hunter-Rowe, Senior Health Intelligence Analyst
• Dr Andrew Carnon, Consultant in Public Health Medicine
• Carolyn Hunter-Rowe, Senior Health Intelligence Analyst