-
8/19/2019 articulo cesar.pdf
1/8
Inuence of temporomandibular joint discdisplacement on
craniocervical posture
and hyoid bone position
Jung-Sub An,a Da-Mi Jeon,a Woo-Sun Jung,b Il-Hyung Yang,c Won
Hee Lim,d and Sug-Joon Ahne
Seoul, Korea
Introduction: The purpose of this study was to evaluate
craniocervical posture and hyoid bone position in or-
thodontic patients with temporomandibular joint (TMJ) disc
displacement. Methods: The subjects consisted
of 170 female orthodontic patients who consented to bilateral
magnetic resonance imaging of their TMJs.
They were divided into 3 groups based on the results of magnetic
resonance imaging of their TMJs: bilateral
normal disc position, bilateral disc displacement with
reduction, and bilateral disc displacement without reduc-
tion. Twenty-
ve variables from lateral cephalograms were analyzed with 1-way
analysis of variance toinvestigate differences in craniocervical
posture and hyoid bone position with respect to TMJ disc
displacement status. Pearson correlation coefcients were
calculated to analyze the relationships between
craniofacial morphology and craniocervical posture or hyoid bone
position. Results: Subjects with TMJ disc
displacement were more likely to have an extended craniocervical
posture with Class II hyperdivergent patterns.
Themost signicant differences werefound between patients with
bilateral normal disc position and bilateral disc
displacement without reduction. However, hyoid bone position in
relation to craniofacial references was not
signicantly different among the TMJ disc displacement groups,
except for variables related to the mandible.
Pearson correlation coefcients indicated that extended
craniocervical posture was signicantly correlated
with backward positioning and clockwise rotation of the
mandible. Conclusions: This suggests that craniocer-
vical posture is signicantly inuenced by TMJ disc displacement,
which may be associated with hyperdivergent
skeletal patterns with a retrognathic mandible. (Am J Orthod
Dentofacial Orthop 2015;147:72-9)
Disc displacement of the temporomandibular joint(TMJ) is a
common temporomandibular disorder(TMD)1 and refers to an abnormal
positional rela-
tionship between thearticular disc and thecondyle, fossa,and
articular eminence.2 TMJ disc displacementgenerally progresses
from a reducing to a nonreducing state andmay lead to TMJ clicking,
crepitus, and in some cases,pain and jaw movement
limitations.2-4 Common causesof TMJ disc displacement include
trauma andparafunctional habits, such as clenching and
bruxism.4
Various imaging techniques are available for evalua-tion
of the TMJ, such as transcranial radiography,arthrography,
tomography, computed tomography,
and magnetic resonance imaging (MRI).5 Among them, MRI is
the only modality that directly depicts the discand is the gold
standard in determining articular disc po-sition relative to the
condyle and articular eminence
because of its high diagnostic accuracy.6 In addition,
italso offers other advantages, such as noninvasiveness,lack of
soft tissue distortion, minimal pain, minimal
risk potential, and lack of ionizing radiation exposure.7
Approximately 30% of asymptomatic adults and 82%of symptomatic
patients have some f orm of TMJ discdisplacement, as
determined by MRI.6
Previous studies have investigated the
relationship between TMJ disc displacement and dentofacial
charac-teristics in orthodontic patients, reporting that
patients
with TMJ disc displacement have decreased posteriorfacial
height as well as backward positioning and clock-
wise rotation of the mandible.8,9 Since craniocervical
posture and hyoid bone position can be associated with
dentofacial morphology, both of these featurescould be signicantly
inuenced by TMJ disc
From the Dental Research Institute and Department of
Orthodontics, School of Dentistry, Seoul National
University, Seoul, Korea.a Postgraduate
student. b Researcher.cAssistant professor.dAssociate
professor.e Professor.
All authors have completed and submitted the ICMJE Form for
Disclosure of
Potential Conicts of Interest, and none were reported.
Address correspondence to: Sug-Joon Ahn, Dental Research
Institute and
Department of Orthodontics, School of Dentistry, Seoul
National University,
101 Deahak-ro, Jongno-Gu, Seoul 110-768, Korea; e-mail,
[email protected].
Submitted, April 2014; revised and accepted, September 2014.
0889-5406/$36.00
Copyright 2015 by the American Association of Orthodontists.
http://dx.doi.org/10.1016/j.ajodo.2014.09.015
72
ORIGINAL ARTICLE
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-mailto:[email protected]:[email protected]://dx.doi.org/10.1016/j.ajodo.2014.09.015http://dx.doi.org/10.1016/j.ajodo.2014.09.015mailto:[email protected]://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 articulo cesar.pdf
2/8
displacement.10,11 However, the associations between
TMJ disc displacement and craniocervical posture orhyoid bone
position have not yet been fully investigated. Although the
effects of TMD on
craniocervical posture and hyoid bone position have been
investigated, the results remain controversial.Several studies have
reported an association between
TMD and craniocervical posture,12-16 but others donot
support the connection between T MD andcraniocervical
posture or hyoid bone position.17-20 Thepurpose of this study was
to investigate therelationships between TMJ disc displacement
andcraniocervical posture, and between TMJ discdisplacement and
hyoid bone position, using MRI. The
null hypothesis was that no signicant relationships would
be found between TMJ disc displacement andcraniocervical posture,
or between TMJ discdisplacement and hyoid bone position.
MATERIAL AND METHODS
Female subjects were recruited from patients whoconsented
to bilateral MRI of their TMJs. All subjectshad a primary complaint
of malocclusion, and routinelateral cephalograms were taken in
natural head position
with an Asahi CX-90SP II (Asahi Roentgen, Kyoto,
Japan). Natural head position was determined by having the
sub-
jects look straight into a mirror in a standing
position.21 Achain plumb line was suspended in front of the
cassetteto indicate a true vertical line. The MRI images were
takento evaluate TMJ status mainly because of TMJ symptomsincluding
TMJ sounds, pain, masticatory muscle tender-ness, limited
mandibular movement, and locking. Exclu-
sion criteria were (1) age less than 17 years, (2)
any systemic disease, (3) history of orthodontic treatment,(4)
history of facial cosmetic or orthognathic surgery,(5) history of
trauma involving the TMJ, (6) juvenile rheu-matoid arthritis, (7)
history of TMJ treatment, (8) airway
obstruction, (9) oral habits, (10)TMJ discdisplacementof a
greater severity on the unilateral side, and (11) partial
TMJ disc displacement or TMJ disc displacement withpartial
reduction. This research protocol was approved
by the institutional review board of the Seoul
National University Dental Hospital (CRI11040).
Radiologists with MRI experience with the TMJ inter-preted
the images blinded to the clinical information.According to disc
position, TMJ disc status was dividedinto 3 categories as
follows.
1 Normal disc position.In theclosed-mouthposition,the
intermediate zone of the disc was interposed betweenthe condyle
and the posterior slope of the articulareminence, with the anterior
and posterior bandsequally spacedon eitherside of thecondylar
loadpoint.
2 Disc displacement with reduction. The disc was ante-riorly
displaced relative to the posterior slope of thearticular eminence
and the head of the condyle in theclosed-mouth position, but the
disc was reduced on
mouth opening.3 Disc displacement without reduction. The disc
wasanteriorly displaced relative to the posterior slopeof the
articular eminence and the head of thecondyle, and the disc was not
reduced on mouthopening.
The position and shape of the articular disc of theTMJ were
carefully evaluated according to the classica-tion criteria. We
excluded patients with a unilaterally
different disc displacement status because the possibleskeletal
morphologies associated with unilateral discdisplacement would be
obscured by averaging of the
right and left landmarks used to determine their loca-tion, and
unilaterally different disc displacement statusmay asymmetrically
inuence craniocervical posture orhyoid bone position, which is
dif cult to measure in
lateral cephalometric analysis.22 From the
originally selected patients, only those with bilateral normal
discstatus (BN), bilateral disc displacement with reduction(DDR),
and bilateral disc displacement without reduction
(DDNR) were included in this study.One investigator (S-J.A.),
who was blinded to the
clinical information and the disc position, traced alllateral
cephalograms. Eighteen landmarks were recorded
on each radiograph using a digitizer with a desktopcomputer, and
25 variables were calculated from these
landmarks: 9 variables for craniocervical posture, 7for hyoid
bone position, and 9 for craniofacialmorphology (4 for vertical and
5 for sagittal craniofacialmorphologies). The positions and
denitions of thelandmarks are shown in Figure 1, and the
locations of the reference planes are shown in Figure
2. Measure-ments for craniocervical posture, hyoid bone
position,
and craniofacial morphology are shown in Figures 3,
4,and 5, respectively.
Lateral cephalograms of 20 randomly selected sub-
jects were measured again to test the magnitude of
mea-surement errors. The intraclass correlation coef cientsfor
the reliability of tracing, landmark identication,
and analytic measurements were greater than
0.98. Descriptive statistics were calculated for all vari-
ables. The differences in the cephalometric variablesfor
craniocervical posture, hyoid bone position, and
craniofacial morphology with respect to the TMJ discdisplacement
status (BN, DDR, and DDNR) were tested
with 1-way analysis of variance. Scheff e multiple
com-parisons were performed at a signicance level of 0.05to analyze
between-group relationships. To investigate
An et al 73
American Journal of Orthodontics and Dentofacial
Orthopedics January 2015 Vol 147
Issue 1
-
8/19/2019 articulo cesar.pdf
3/8
the correlations between craniofacial morphology and
craniocervical posture or hyoid bone position,
Pearsoncorrelation coef cients were calculated.
RESULTS
A total of 170 female subjects were included in thisstudy (Table
I). Their age range was 17.0 to 50.8 years(mean age, 24.5 6 5.7
years). There were no signicantdifferences in age distribution
among the 3 study groups
(data not shown).Table II presents the differences in
craniocervical
posture, hyoid bone position, and craniofacialmorphology with
respect to TMJ disc displacement sta-tus (BN, DDR, and DDNR).
Signicant differences werefound in craniocervical posture between
the BN and
DDNR groups (Table II). Subjects with DDNR had larger
angles between the craniofacial reference planes and thecervical
vertebrae (FH/CVT, NL/CVT, FH/OPT, and NL/OPT) than did the
subjects with BN, indicating that sub-
jects with DDNR had extended craniocervical
posturecompared with those with BN. Although the subjects
with DDR demonstrated intermediate values, there was
no signicant difference in craniocervical posture be-tween the
BN and DDR groups, or between the DDRand DDNR groups. Angles
between the cervical vertebraeand the true horizontal plane
(HOR/CVT and HOR/OPT)
or the mandibular plane (MP/CVT and MP/OPT) werenot signicantly
different among the 3 groups. Cervical
curvature (OPT/CVT) also did not vary signicantly among the
different TMJ disc displacement groups.
Among the variables for hyoid bone position,
only measurements related to the mandible were
signicantly
inuenced by TMJ disc displacement status. Subjects with
DDNR had a decreased hyoid angle (Go/Hy/Me)compared with those with
BN or DDR (BN 5
DDR. DDNR). In addition, the hyoidale to the most
pro-trusive point of retrognathion distance (Hy-RGn)decreased as
TMJ disc displacement status increased
inseverityfromBNtoDDNR(BN. DDR. DDNR). However,
distances between craniocervical landmarks or referenceplanes
and the hyoid bone (Hy-Ba, Hy to NSL, Hy to NL,
Hy-cv3ia, and Hy to cv3ia-RGn) did not show
signicantdifferences according to TMJ disc displacement
status(Table II).
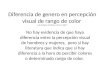
Fig 2. Craniocervical reference planes used in this
study:
1, nasion-sella line (NSL,planethroughnasion and sella);
2 , true horizontal plane (HOR, true horizontal plane
pass-
ing through sella); 3 , Frankfort horizontal plane (FH,
plane
through porion and orbitale); 4 , nasal line (NL,
line
through the posterior nasal spine and anterior nasal
spine); 5 , mandibular plane (MP, line through
gonion
and menton); 6 , cervical vertebrae tangent (CVT,
line
through cv2tg and cv4ip); 7 , odontoid process
tangent
(OPT, line through cv2tg and cv2ip).
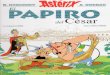
Fig 1. Landmarks used in this study:1, nasion;2 ,
sella;3 ,
orbitale; 4 , porion; 5 , basion;
6 , anterior nasal spine; 7 ,
posterior nasal spine; 8 , Point A;9 , Point
B;10 , pogonion;
11, menton; 12 , gonion; 13 , RGn (most
protrusive point of
retrognathion); 14 , hyoidale (Hy, most superior and
ante-
rior point on the body of the hyoid bone); 15 ,
cv2tg
(tangent point of the superoposterior extremity of the sec-
ond cervical vertebra); 16 , cv2ip (most
posteroinferior
point on the second cervical vertebra);17 , cv3ia (most
an-
teroinferior point on the third cervical vertebra);
18 , cv4ip
(most posteroinferior point on the fourth cervical
vertebra).
74 An et al
January 2015 Vol 147 Issue
1 American Journal of Orthodontics and Dentofacial Orthopedics
-
8/19/2019 articulo cesar.pdf
4/8
As previously reported, subjects with TMJ discdisplacement have
a retrognathic mandi ble with a hy-perdivergent skeletal
pattern (Table II).8,9 Our study
showed that increased ANB, and decreased SNB and Nperpendicular
to pogonion (PNP), are specic sagittal
craniofacial morphologies in subjects with TMJ discdisplacement.
In addition, these skeletal characteristics
became more severe as TMJ disc displacementprogressed from
BN to DDNR. However, variables
representing maxillary position (SNA and Nperpendicular to point
A [ANP]) were not signicantly different among the 3 groups.
Subjects with DDNRhad a hyperdivergent skeletal pattern: eg,
increased
Frankfort-mandibular plane angle (FMA), decreasedposterior
facial height (PFH), and decreased facial heightratio (FHR)
compared with those with BN or DDR. In
contrast to sagittal craniofacial morphology,
verticalcraniofacial morphology did not vary signicantly be-tween
the BN and DDR groups (Table II).
Correlations between craniofacial morphology andcraniocervical
posture or hyoid bone position are
presented in Table III. Generally, craniocervical
posture
(FH/CVT, NL/CVT, FH/OPT, and NL/OPT) was signi-cantly correlated
with variables representing sagittal(ANB, SNB, and PNP) and
vertical (FMA and FHR)craniofacial morphologies, and subjects with
extendedcraniocervical posture had a retrognathic mandible
with a hyperdivergent skeletal pattern. However,
cervical
curvature (OPT/CVT) was not signicantly correlated with
craniofacial morphology.
The hyoid angle (Go/Hy/Me) and the distance be-
tween the hyoidale and the most protrusive point of
ret-rognathion (Hy-RGn) were signicantly correlated with
craniofacial morphologic variables (Table III). Both values
decreased as the skeletal pattern became more hy-
perdivergent (increased FMA and decreased FHR) and asthe
mandible was located more posteriorly (increasedANB and decreased
SNB and PNP).
DISCUSSION
The relationships between TMJ status and craniocer- vical
posture have not been fully addressed, specically in
orthodontic patients. This may be due to the
Fig 4. Variables of the hyoid bone position (all are
linear
measurements except for Go/Hy/Me): 1, linear distance
between the hyoidale and basion (Hy-Ba); 2 ,
perpendic-
ular distance between the hyoidale to nasion-sella line
(Hy to NSL); 3 , perpendicular distance between the
hyoi-
dale to nasal line (Hy to NL); 4 , linear distance
between
the hyoidale and RGn (Hy-RGn); 5 , linear distance
be-
tween the hyoidale and cv3ia (Hy-cv3ia);6 ,
perpendicular
distance between the hyoidale and cv3ia-RGn plane (Hy
to cv3ia-RGn, positive when the Hy is located below the
cv3ip-RGn plane); 7 , hyoid angle, angle of
Go-Hy-Me
(Go/Hy/Me, the angle is larger when the hyoidale is
located above the mandibular plane).
Fig 3. Variables of craniocervical posture (all are
angular
measurements): 1, true horizontal plane to cervical
verte-
brae tangent angle (HOR/CVT); 2 , Frankfort
horizontal
plane to cervical vertebrae tangent angle (FH/CVT);
3 ,
nasal line to cervical vertebrae tangent angle (NL/CVT);
4 , mandibular plane to cervical vertebrae tangent
angle
(MP/CVT); 5 , true horizontal plane to odontoid
process
tangent angle (HOR/OPT); 6 , Frankfort horizontal
plane
to odontoid process tangent angle (FH/OPT); 7 ,
nasal
line to odontoid process tangent angle (NL/OPT);
8 ,
mandibular plane to odontoid process tangent angle
(MP/OPT); 9 , the cervical curvature,
downward-opening
angle between odontoid process tangent and cervical
vertebrae tangent (OPT/CVT, positive when the cv4ip is
located on the left side of odontoid process tangent).
An et al 75
American Journal of Orthodontics and Dentofacial
Orthopedics January 2015 Vol 147
Issue 1
-
8/19/2019 articulo cesar.pdf
5/8
methodologic problems of previous studies, such asinadequate
sample sizes and subjective criteria for clas-sifying TMJ
status.12,13,17,18,23 In this study, we used alarge sample size
(170 subjects) including a control
group (BN TMJs). In addition, the subjects wereobjectively
classied with MRI of their TMJs, not withsubjective signs and
symptoms. Furthermore, thesubjects were carefully controlled. Only
subjects withthe same TMJ disc displacement conditions
bilaterally
were included. Men were excluded to prevent skewingthe
cephalometric measurements with sex-related dif-
ferences. To prevent growth-related size differences,only female
patients over the age of 17 years wereselected.24
This study showed an association between TMJ discdisplacement
and craniocervical posture. Subjects with
DDNR had increased FH/CVT, NL/CVT, FH/OPT, and
NL/OPT compared with those with BN (Table II).Although
there were no signicant differences in the an-gles between the BN
and DDR groups, or between the
DDR and DDNR groups, there was a tendency towardincreased
angles between the craniofacial referenceplanes and the cervical
vertebrae as TMJ disc displace-
ment progressed from BN to DDNR. This means thathead or cervical
posture can change according to TMJdisc displacement status. Since
neither angle betweenthe cervical vertebrae and the true horizontal
plane(HOR/CVT and HOR/OPT) or the cervical curvature(OPT/CVT) was
signicantly different among the 3 discdisplacement statuses, head
posture may rotate above
the second vertebra without changes in cervical
vertebralposition in relation to the true horizontal plane.Although
direct comparison was not possible, our nd-ings are similar
to those of previous studies reporting
that patients with TMD have a more extended
craniocer- vical posture than the control group, without
signicantdifferences in cervical curvature,12 and that there are
nosignicant differences in the curvature of the cervical
vertebrae between the third and seventh vertebrae
aftercomparing cervical vertebral alignment bet ween sub-
jects with TMD and volunteers without TMD.19
Despite changes in head posture, the positional
rela-tionships between the cervical vertebrae and themandibular
plane (MP/CVT and MP/OPT) did not showsignicant differences among
the 3 TMJ groups. This
might be because mandibular position is
signicantly associated with TMJ disc displacement status.
Subjects
with TMJ disc displacement generally had an
increasedmandibular plane angle with extended craniocervicalposture
(Table II). Because both cervical vertebrae andthe mandible are
rotated clockwise in relation to the
craniofacial reference planes in subjects with TMJ
discdisplacement, there may be no signicant differences
in relationships between the cervical vertebrae and
themandibular plane.
The association between TMJ disc displacement andextended
craniocervical posture can be explained in 2
ways. The rst possibility is that extended
craniocervicalposture may inuence TMJ disc displacement.
Previousstudies have reported that abnormal craniocervicalposture
is an etiologic factor of TMD, postulating thatas the cranium
rotates backward, the mandibular denti-tion will be located more
posteriorly in relation to themaxillary dentition; in turn, the
mandible will be
advanced to obtain occlusal support.12,13 Increasedmuscular
activity that develops as a result will lead
todisc displacement.12,13 Although the subjects with TMJdisc
displacement had a more extended craniocervicalposture in this
study, they had a more posteriorly
Fig 5. Variables of craniofacial morphology: 1,
Frankfort
horizontal plane to mandibular plane angle (FMA);
2 ,
anterior facial height (AFH, linear distance between na-
sion and menton); 3 , posterior facial height (PFH,
linear
distance between sella and gonion); 4 , ANB angle;
5 ,
SNA angle; 6 , SNB angle; 7 , N
perpendicular to Point A
(ANP); 8 , N perpendicular to pogonion (PNP);
9 , facial
height ratio (FHR, ratio of posterior facial height [3 ]
to
anterior facial height [2 ]).
Table I. Number and age distribution of subjects with
BN, DDR, and DDNR
Group BN DDR DDNR Total
Subjects, n (%) 53 (31.2) 55 (32.4) 62 (36.5) 170 (100)
Age (y)
Mean 23.7 6 6.6 25.1 6 5.4 24.6 6 5.3 24.5 6 5.7
Range 18.3-50.8 17.3-42.0 17.0-41.0 17.0-50.8
76 An et al
January 2015 Vol 147 Issue
1 American Journal of Orthodontics and Dentofacial Orthopedics
-
8/19/2019 articulo cesar.pdf
6/8
located mandible than did subjects with BN (Table II);this
differs from previous studies.
The second possibility is that TMJ disc displacement
may induce extended craniocervical posture. Previousstudies have
reported that the severity of TMJ discdisplacement increases as the
sagittal skeletal classica-tion changes from skeletal Class III to
skeletal Class II,and the vertical skeletal classication changes
from hy-podivergent to hyperdivergent.8,9,25 As a result,
subjects
with skeletal Class II or hyperdivergent deformities
have
a high possibility of severe TMJ disc displacement. Inaddition,
experimentally induced TMJ discdisplacement leads to signicant
impairment of
vertical and horizontal mandibular growth, and theamount
of vertical or horizontal skeletal changegradually increased as TMJ
disc displacement increased
in severity in animal studies.26,27 Because TMJ
discdisplacement frequently occurs during puberty, itseems that TMJ
disc displacement can lead to aretrognathic mandible with a
hyperdivergent skeletal
pattern; this in turn may reduce upper airway
space with the same craniocervical posture.28 Therefore,
extended craniocervical posture associated with TMJdisc
displacement may result from protective responsesto maintain upper
airway space. This hypothesis is sup-
ported by our ndings, indicating that extended
cranio-cervical posture is positively related to a
hyperdivergentand Class II skeletal pattern (Table III). de Farias
Netoet al16 also postulated that in the patients with TMD,altered
mobility of the articular disc limits the biome-chanics of mouth
opening and triggers compensatory extension of the cervical
vertebrae to prevent compres-
sion of the upper airway. However, the cause-and-effect
relationships are not clear because the results
were derived from cross-sectional data.Interestingly, TMJ
disc displacement did not signi-
cantly inuence the positional relationships of the
hyoid bone to the craniofacial references and the cervical
vertebrae, but it signicantly inuenced the
positionalrelationships of the hyoid bone to the mandible (Go/
Hy/Me and Hy-RGn) (Table II). Subjects with TMJ
discdisplacement, and specically those with DDNR, had a
smaller hyoid angle (Go/Hy/Me) and a shorter hyoidaleto the most
protrusive point of retrognathion distance
Table II. Comparisons of cephalometric variables among
the BN, DDR, and DDNR groups
Variable BN DDR DDNR Signi cance z Multiple
comparisons
Craniocervical posture
HOR/CVT () 98.7 6 6.9 99.5 6 5.8 99.6 6 5.9 NS
FH/CVT () 96.6 6 8.2 98.3 6 6.3 100.3 6 7.1 *
BN\ DDNR NL/CVT () 96.1 6 8.7 98.3 6 6.4 99.6 6
6.9 * BN\ DDNR
MP/CVT () 67.3 6 8.8 67.6 6 7.0 64.7 6 8.5 NS
HOR/OPT () 93.6 6 7.4 94.9 6 7.1 94.7 6 6.4 NS
FH/OPT () 91.5 6 8.5 93.7 6 7.3 95.4 6 7.4 *
BN\ DDNR
NL/OPT () 91.0 6 8.8 93.7 6 7.2 94.7 6 7.1 *
BN\ DDNR
MP/OPT () 62.2 6 8.6 63.0 6 7.9 59.8 6 8.5 NS
OPT/CVT () 5.1 6 2.8 4.6 6 2.9 4.9 6 2.5 NS
Hyoid bone position
Hy-Ba (mm) 76.3 6 5.6 77.0 6 6.0 75.1 6 6.1 NS
Hy to NSL (mm) 107.0 6 6.4 108.2 6 7.6 108.4 6 6.4 NS
Hy to NL (mm) 60.7 6 5.2 61.8 6 6.0 62.6 6 5.7 NS
Hy-RGn (mm) 38.4 6 5.7 35.5 6 5.5 32.3 6 5.5 y
BN . DDR . DDNR
Hy-cv3ia (mm) 36.2 6 3.8 36.5 6 3.0 35.2 6 3.4 NS
Hy to cv3ia-RGn (mm)
1.56
6.1 0.06
5.0 0.56
5.9 NSGo/Hy/Me () 154.3 6 18.0 151.0 6 14.8 143.4 6 15.1
* BN 5 DDR . DDNR
Vertical craniofacial morphology
FMA () 28.9 6 7.0 30.6 6 6.7 35.5 6 7.0 y BN
5 DDR\ DDNR
FHR (ratio) 0.63 6 0.06 0.62 6 0.05 0.59 6 0.06 y
BN 5 DDR . DDNR
AFH (mm) 132.8 6 5.5 133.7 6 6.5 133.3 6 6.0 NS
PFH (mm) 83.7 6 7.6 82.6 6 6.6 77.9 6 6.7 y
BN 5 DDR . DDNR
Sagittal craniofacial morphology
ANB () 2.4 6 4.5 5.1 6 2.4 7.7 6 2.8 y
BN\ DDR\ DDNR
SNA () 81.1 6 3.1 81.6 6 3.2 81.4 6 2.8 NS
SNB () 78.7 6 4.9 76.5 6 2.9 73.8 6 3.6 y BN
. DDR . DDNR
ANP (mm) 1.7 6 3.0 2.3 6 2.8 1.5 6 3.2 NS
PNP (mm) 1.32 6 10.43 6.32 6 6.65
14.05 6 7.73 y BN . DDR . DDNR
NS , Not signicant.
*P \
0.05;
y
P \
0.001;
z
Scheff e multiple comparisons were used to analyze the
intergroup difference at the level of
a 50.05.
An et al 77
American Journal of Orthodontics and Dentofacial
Orthopedics January 2015 Vol 147
Issue 1
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 articulo cesar.pdf
7/8
(Hy-RGn) than did the subjects with BN, whereas the dis-tances
between the hyoid bone and the craniofacial ref-erences (Hy-Ba, Hy
to NSL, and Hy to NL) or the cervical
vertebrae (Hy-cv3ia), and the relationship between the
hyoid bone and the craniocervical reference (Hy tocv3ia-RGn),
were not signicantly different among the
3 TMJ disc displacement groups. The relationship be-tween the
hyoid bone and the mandible can be explained
by the compensatory response of the hyoid bone to
pre-serve upper airway space. It seems that the position
of the hyoid bone may not signicantly change duringthe
protective process, which maintains the pharyngealairway space and
swallowing functions against back-
ward positioning and clockwise rotation of the
mandibleassociated with TMJ disc displacement. As a result, the
subjects with TMJ disc displacement have backwardpositioning and
clockwise rotation of the mandible
with a relatively stable hyoid bone position, which
may
change the positional relationships of the hyoid boneto the
mandible signicantly. This hypothesis is partly supported by
previous research that found no signicant
differences in hyoid bone positions between
subjects with and without TMD.19 Other research regardingTMJ
disc displacement status with MRI also documentedthat the position
of the hyoid bone was not signicantly
different between subjects with a normal disc positionand
those with disc displacement.20
Generally, the facial prole is important in the diag-nosis and
treatment planning for orthodontic patients.This study showed that
TMJ disc displacement can
inuence craniocervical posture, although the cause-and-effect
relationship remains unclear. As a result,in subjects with TMJ disc
displacement, the retro-gnathic prole is compromised by extending
their
craniocervical posture despite the backward positioningand
rotation of the mandible. Recently, the importance
of the soft tissue paradigm has been emphasized, and anormal
soft tissue proportion is considered a primary
treatment goal in orthodontic or
surgical-orthodontictreatment.29-31 Because craniocervical
posture isdirectly related to the soft tissue prole of the
face,this study suggests that clinicians should
carefully evaluate relationships between the
craniocervicalposture and the facial prole in patients
withpotential TMJ disc displacement before orthodontic
treatment.This study has the following limitations. The
causal
relationships between TMJ disc displacement and cra-
niocervical posture, or between TMJ disc displacementand the
hyoid bone position, are not clear becauseour results were derived
from cross-sectional data. In
addition, these results are based on lateral cephalo-grams with
static posture; hence, they do not showthe function associated with
mandibular kinetics.
Further studies with longitudinal data are needed to
clarify the relationships of intra-articular distance,mandibular
kinematics, and mandibular loading with
craniocervical posture. This would be helpful for thediagnosis
and treatment planning of patients withTMJ disc displacement.
Table III. Correlations between craniofacial morphology
and craniocervical posture or hyoid bone position
Variable
Correlation
FMA FHR AFH PFH ANB SNA SNB ANP PNP
Craniocervical posture HOR/CVT () 0.241y NS 0.196*
NS 0.240y 0.169* 0.332y 0.153* 0.334y
FH/CVT () 0.381y 0.247y 0.270y NS 0.399y 0.205y
0.499y 0.316y 0.591y
NL/CVT () 0.256y 0.192* 0.262y NS 0.315y
0.248y 0.454y 0.193* 0.416y
MP/CVT () 0.547y 0.556y NS 0.512y NS NS
NS NS NS
HOR/OPT () 0.258y 0.154* 0.153* NS 0.242y
0.168* 0.333y NS 0.325y
FH/OPT () 0.396y 0.256y 0.234y NS 0.399y 0.207y
0.501y 0.290y 0.578y
NL/OPT () 0.283y 0.208y 0.231y NS 0.326y 0.253y
0.467y 0.178* 0.422y
MP/OPT () 0.498y 0.519y NS 0.468y NS NS
NS NS NS
OPT/CVT () NS NS NS NS NS NS NS NS NS
Hyoid bone position
Hy-Ba (mm) NS 0.152* 0.247y 0.281y 0.162*
0.162* 0.257y NS 0.174*
Hy to NSL (mm) NS NS 0.341y 0.289y NS 0.281y
NS NS NS
Hy to NL (mm) 0.237y NS 0.247y NS 0.236y
NS 0.161* NS 0.267y
Hy-RGN (mm) 0.519y 0.388y NS 0.396y 0.584y
NS 0.421y NS 0.562y
Hy-cv3ia (mm) 0.181* 0.191* 0.165*
0.278y NS NS NS NS NS
Hy to cv3ia-RGn (mm) NS NS NS NS 0.174* NS NS NS
NS
Go/Hy/Me () 0.385y 0.358y 0.168* 0.447y 0.324y
NS 0.339y 0.151* 0.367y
NS , Not signicant.
*Pearson correlation is signicant at the .05 level;
y Pearson correlation is signicant at the .01 level.
78 An et al
January 2015 Vol 147 Issue
1 American Journal of Orthodontics and Dentofacial Orthopedics
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 articulo cesar.pdf
8/8
CONCLUSIONS
This study was performed to evaluate the relation-
ships between TMJ disc displacement and craniocervicalposture,
and between TMJ disc displacement and hyoid
bone position, in adult orthodontic patients. The
sub- jects with TMJ disc displacement were more likely tohave
an extended craniocervical posture with Class II hy-perdivergent
patterns. In contrast, hyoid bone position
was relatively stable irrespective of TMJ disc
displace-
ment status. Therefore, the null hypothesis of our
study was partially rejected. Extended craniocervical
posture was signicantly correlated with backward
positioningand clockwise rotation of the mandible. This study
sug-gests that craniocervical posture is signicantly inu-enced by
TMJ disc displacement, which may be
associated with a hyperdivergent skeletal pattern with
a retrognathic mandible.
REFERENCES
1. Liu MQ, Chen HM, Yap AU, Fu KY. Condylar remodeling
accompa-
nying splint therapy: a cone-beam computerized
tomography
study of patients with temporomandibular joint disk
displacement.
Oral Surg Oral Med Oral Pathol Oral Radiol 2012;114:259-65.
2. Dolwick MF, Katzberg RW, Helms CA. Internal
derangements of
the temporomandibular joint: fact or ction? J Prosthet
Dent
1983;49:415-8.
3. Murakami S, Takahashi A, Nishiyama H, Fujishita M,
Fuchihata H.
Magnetic resonance evaluation of the temporomandibular
joint
disc position and conguration. Dentomaxillofac Radiol 1993;
22:205-7.
4. Okeson JP. Management of temporomandibular disorders
and
occlusion. St Louis: Elsevier/Mosby; 2013.
5. Westesson PL. Reliability and validity of imaging
diagnosis of
temporomandibular joint disorder. Adv Dent Res
1993;7:137-51.
6. Tasaki MM, Westesson PL, Isberg AM, Ren YF, Tallents
RH. Classi-
cation and prevalence of temporomandibular joint disk
displace-
ment in patients and symptom-free volunteers. Am J Orthod
Dentofacial Orthop 1996;109:249-62.
7. Nebbe B, Major PW. Prevalence of TMJ disc displacement
in a pre-
orthodontic adolescent sample. Angle Orthod 2000;70:454-63.
8. Nebbe B, Major PW, Prasad N. Female adolescent facial
pattern
associated with TMJ disk displacement and reduction in disk
length: part I. Am J Orthod Dentofacial Orthop 1999;116:
168-76.
9. Kwon HB, Kim H, Jung WS, Kim TW, Ahn SJ. Gender
differences indentofacial characteristics of adult patients with
temporomandib-
ular disc displacement. J Oral Maxillofac Surg
2013;71:1178-86.
10. Solow B, Sandham A. Cranio-cervical posture: a factor
in the
development and function of the dentofacial structures. Eur
J
Orthod 2002;24:447-56.
11. Adamidis IP, Spyropoulos MN. Hyoid bone position and
orienta-
tion in Class I and Class III malocclusions. Am J Orthod
Dentofacial
Orthop 1992;101:308-12.
12. Huggare JA, Raustia AM. Head posture and
cervicovertebral and
craniofacial morphology in patients with craniomandibular
dysfunction. Cranio 1992;10:173-7.
13. Nicolakis P, Nicolakis M, Piehslinger E, Ebenbichler
G, Vachuda M,
Kirtley C, et al. Relationship between craniomandibular
disorders
and poor posture. Cranio 2000;18:106-12.
14. D'Attilio M, Epifania E, Ciuffolo F, Salini V, Filippi
MR, Dolci M,
et al. Cervical lordosis angle measured on lateral
cephalograms;
ndings in skeletal Class II female subjects with and withoutTMD:
a cross sectional study. Cranio 2004;22:27-44.
15. Munhoz WC, Marques AP, Siqueira JT. Radiographic
evaluation of
cervical spine of subjects with temporomandibular joint
internal
disorder. Braz Oral Res 2004;18:283-9.
16. de Farias Neto JP, de Santana JM, de Santana-Filho VJ,
Quintans-
Junior LJ, de Lima Ferreira AP, Bonjardim LR. Radiographic
mea-
surement of the cervical spine in patients with
temporomandibular
dysfunction. Arch Oral Biol 2010;55:670-8.
17. HackneyJ, Bade D, Clawson A. Relationship between
forward head
posture and diagnosed internal derangement of the
temporoman-
dibular joint. J Orofac Pain 1993;7:386-90.
18. Visscher CM, De Boer W, Lobbezoo F, Habets LL, Naeije
M. Is there
a relationship between head posture and craniomandibular
pain?
J Oral Rehabil 2002;29:1030-6.
19. Andrade AV, Gomes PF, Teixeira-Salmela LF. Cervical
spine align-ment and hyoid bone positioning with temporomandibular
disor-
ders. J Oral Rehabil 2007;34:767-72.
20. Matheus RA, Ramos-Perez FM, Menezes AV, Ambrosano
GM,
Haiter-Neto F, Boscolo FN, et al. The relationship between
tempo-
romandibular dysfunction and head and cervical posture. J
Appl
Oral Sci 2009;17:204-8.
21. Solow B, Tallgren A. Natural head position in standing
subjects.
Acta Odontol Scand 1971;29:591-607.
22. Ahn SJ, Lee SP, Nahm DS. Relationship between
temporomandib-
ular joint internal derangement and facial asymmetry in
women.
Am J Orthod Dentofacial Orthop 2005;128:583-91.
23. Olivo SA, Bravo J, Magee DJ, Thie NM, Major PW,
Flores-Mir C.
The association between head and cervical posture and
temporo-
mandibular disorders: a systematic review. J Orofac Pain
2006;20:
9-23.
24. Lee SJ, An H, Ahn SJ, Kim YH, Pak S, Lee JW. Early
stature predic-
tion method using stature growth parameters. Ann Hum Biol
2008;35:509-17.
25. Ahn SJ, Baek SH, Kim TW, Nahm DS. Discrimination of
TMJ inter-
nal derangement by lateral cephalometric analysis. Am J
Orthod
Dentofacial Orthop 2006;130:331-9.
26. Bryndahl F, Eriksson L, Legrell PE, Isberg A.
Bilateral TMJ disk
displacement induces mandibular retrognathia. J Dent Res
2006;
85:1118-23.
27. Legrell PE, Isberg A. Mandibular height asymmetry
following
experimentally induced temporomandibular joint disk
displace-
ment in rabbits. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod
1998;86:280-5.
28. Isberg A, Hagglund M, Paesani D. The effect of age and
gender onthe onset of symptomatic temporomandibular joint disk
displace-
ment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
1998;85:
252-7.
29. Prof t WR, Fields HW, Sarver DM. Contemporary
orthodontics. St
Louis: Elsevier/Mosby; 2013.
30. Yu YH, Kim YJ, Lee DY, Lim YK. The predictability of
dentoskeletal
factors for soft-tissue chin strain during lip closure. Korean
J
Orthod 2013;43:279-87.
31. Toureno L, Kook YA, Bayome M, Park JH. The effect of
western
adaptation of Hispanic-Americans on their assessment of
Korean
facial proles. Korean J Orthod 2014;44:28-35.
An et al 79
A i J l f O th d ti d D t f i l O th di J 2015 V l 147 I 1
http://refhub.elsevier.com/S0889-5406(14)00867-1/sref1http://refhub.elsevier.com/S0889-5406(14)00867-1/sref1http://refhub.elsevier.com/S0889-5406(14)00867-1/sref1http://refhub.elsevier.com/S0889-5406(14)00867-1/sref1http://refhub.elsevier.com/S0889-5406(14)00867-1/sref2http://refhub.elsevier.com/S0889-5406(14)00867-1/sref2http://refhub.elsevier.com/S0889-5406(14)00867-1/sref2http://refhub.elsevier.com/S0889-5406(14)00867-1/sref2http://refhub.elsevier.com/S0889-5406(14)00867-1/sref2http://refhub.elsevier.com/S0889-5406(14)00867-1/sref3http://refhub.elsevier.com/S0889-5406(14)00867-1/sref3http://refhub.elsevier.com/S0889-5406(14)00867-1/sref3http://refhub.elsevier.com/S0889-5406(14)00867-1/sref3http://refhub.elsevier.com/S0889-5406(14)00867-1/sref3http://refhub.elsevier.com/S0889-5406(14)00867-1/sref3http://refhub.elsevier.com/S0889-5406(14)00867-1/sref4http://refhub.elsevier.com/S0889-5406(14)00867-1/sref4http://refhub.elsevier.com/S0889-5406(14)00867-1/sref5http://refhub.elsevier.com/S0889-5406(14)00867-1/sref5http://refhub.elsevier.com/S0889-5406(14)00867-1/sref5http://refhub.elsevier.com/S0889-5406(14)00867-1/sref6http://refhub.elsevier.com/S0889-5406(14)00867-1/sref6http://refhub.elsevier.com/S0889-5406(14)00867-1/sref6http://refhub.elsevier.com/S0889-5406(14)00867-1/sref6http://refhub.elsevier.com/S0889-5406(14)00867-1/sref6http://refhub.elsevier.com/S0889-5406(14)00867-1/sref7http://refhub.elsevier.com/S0889-5406(14)00867-1/sref7http://refhub.elsevier.com/S0889-5406(14)00867-1/sref8http://refhub.elsevier.com/S0889-5406(14)00867-1/sref8http://refhub.elsevier.com/S0889-5406(14)00867-1/sref8http://refhub.elsevier.com/S0889-5406(14)00867-1/sref8http://refhub.elsevier.com/S0889-5406(14)00867-1/sref9http://refhub.elsevier.com/S0889-5406(14)00867-1/sref9http://refhub.elsevier.com/S0889-5406(14)00867-1/sref9http://refhub.elsevier.com/S0889-5406(14)00867-1/sref10http://refhub.elsevier.com/S0889-5406(14)00867-1/sref10http://refhub.elsevier.com/S0889-5406(14)00867-1/sref10http://refhub.elsevier.com/S0889-5406(14)00867-1/sref11http://refhub.elsevier.com/S0889-5406(14)00867-1/sref11http://refhub.elsevier.com/S0889-5406(14)00867-1/sref11http://refhub.elsevier.com/S0889-5406(14)00867-1/sref12http://refhub.elsevier.com/S0889-5406(14)00867-1/sref12http://refhub.elsevier.com/S0889-5406(14)00867-1/sref12http://refhub.elsevier.com/S0889-5406(14)00867-1/sref13http://refhub.elsevier.com/S0889-5406(14)00867-1/sref13http://refhub.elsevier.com/S0889-5406(14)00867-1/sref13http://refhub.elsevier.com/S0889-5406(14)00867-1/sref14http://refhub.elsevier.com/S0889-5406(14)00867-1/sref14http://refhub.elsevier.com/S0889-5406(14)00867-1/sref14http://refhub.elsevier.com/S0889-5406(14)00867-1/sref14http://refhub.elsevier.com/S0889-5406(14)00867-1/sref14http://refhub.elsevier.com/S0889-5406(14)00867-1/sref15http://refhub.elsevier.com/S0889-5406(14)00867-1/sref15http://refhub.elsevier.com/S0889-5406(14)00867-1/sref15http://refhub.elsevier.com/S0889-5406(14)00867-1/sref16http://refhub.elsevier.com/S0889-5406(14)00867-1/sref16http://refhub.elsevier.com/S0889-5406(14)00867-1/sref16http://refhub.elsevier.com/S0889-5406(14)00867-1/sref16http://refhub.elsevier.com/S0889-5406(14)00867-1/sref17http://refhub.elsevier.com/S0889-5406(14)00867-1/sref17http://refhub.elsevier.com/S0889-5406(14)00867-1/sref17http://refhub.elsevier.com/S0889-5406(14)00867-1/sref17http://refhub.elsevier.com/S0889-5406(14)00867-1/sref18http://refhub.elsevier.com/S0889-5406(14)00867-1/sref18http://refhub.elsevier.com/S0889-5406(14)00867-1/sref18http://refhub.elsevier.com/S0889-5406(14)00867-1/sref19http://refhub.elsevier.com/S0889-5406(14)00867-1/sref19http://refhub.elsevier.com/S0889-5406(14)00867-1/sref19http://refhub.elsevier.com/S0889-5406(14)00867-1/sref20http://refhub.elsevier.com/S0889-5406(14)00867-1/sref20http://refhub.elsevier.com/S0889-5406(14)00867-1/sref20http://refhub.elsevier.com/S0889-5406(14)00867-1/sref20http://refhub.elsevier.com/S0889-5406(14)00867-1/sref21http://refhub.elsevier.com/S0889-5406(14)00867-1/sref21http://refhub.elsevier.com/S0889-5406(14)00867-1/sref22http://refhub.elsevier.com/S0889-5406(14)00867-1/sref22http://refhub.elsevier.com/S0889-5406(14)00867-1/sref22http://refhub.elsevier.com/S0889-5406(14)00867-1/sref23http://refhub.elsevier.com/S0889-5406(14)00867-1/sref23http://refhub.elsevier.com/S0889-5406(14)00867-1/sref23http://refhub.elsevier.com/S0889-5406(14)00867-1/sref23http://refhub.elsevier.com/S0889-5406(14)00867-1/sref24http://refhub.elsevier.com/S0889-5406(14)00867-1/sref24http://refhub.elsevier.com/S0889-5406(14)00867-1/sref24http://refhub.elsevier.com/S0889-5406(14)00867-1/sref25http://refhub.elsevier.com/S0889-5406(14)00867-1/sref25http://refhub.elsevier.com/S0889-5406(14)00867-1/sref25http://refhub.elsevier.com/S0889-5406(14)00867-1/sref26http://refhub.elsevier.com/S0889-5406(14)00867-1/sref26http://refhub.elsevier.com/S0889-5406(14)00867-1/sref26http://refhub.elsevier.com/S0889-5406(14)00867-1/sref27http://refhub.elsevier.com/S0889-5406(14)00867-1/sref27http://refhub.elsevier.com/S0889-5406(14)00867-1/sref27http://refhub.elsevier.com/S0889-5406(14)00867-1/sref27http://refhub.elsevier.com/S0889-5406(14)00867-1/sref28http://refhub.elsevier.com/S0889-5406(14)00867-1/sref28http://refhub.elsevier.com/S0889-5406(14)00867-1/sref28http://refhub.elsevier.com/S0889-5406(14)00867-1/sref28http://refhub.elsevier.com/S0889-5406(14)00867-1/sref29http://refhub.elsevier.com/S0889-5406(14)00867-1/sref29http://refhub.elsevier.com/S0889-5406(14)00867-1/sref29http://refhub.elsevier.com/S0889-5406(14)00867-1/sref29http://refhub.elsevier.com/S0889-5406(14)00867-1/sref30http://refhub.elsevier.com/S0889-5406(14)00867-1/sref30http://refhub.elsevier.com/S0889-5406(14)00867-1/sref30http://refhub.elsevier.com/S0889-5406(14)00867-1/sref31http://refhub.elsevier.com/S0889-5406(14)00867-1/sref31http://refhub.elsevier.com/S0889-5406(14)00867-1/sref31http://refhub.elsevier.com/S0889-5406(14)00867-1/sref31http://refhub.elsevier.com/S0889-5406(14)00867-1/sref31http://refhub.elsevier.com/S0889-5406(14)00867-1/sref31http://refhub.elsevier.com/S0889-5406(14)00867-1/sref31http://refhub.elsevier.com/S0889-5406(14)00867-1/sref31http://refhub.elsevier.com/S0889-5406(14)00867-1/sref30http://refhub.elsevier.com/S0889-5406(14)00867-1/sref30http://refhub.elsevier.com/S0889-5406(14)00867-1/sref30http://refhub.elsevier.com/S0889-5406(14)00867-1/sref29http://refhub.elsevier.com/S0889-5406(14)00867-1/sref29http://refhub.elsevier.com/S0889-5406(14)00867-1/sref28http://refhub.elsevier.com/S0889-5406(14)00867-1/sref28http://refhub.elsevier.com/S0889-5406(14)00867-1/sref28http://refhub.elsevier.com/S0889-5406(14)00867-1/sref28http://refhub.elsevier.com/S0889-5406(14)00867-1/sref27http://refhub.elsevier.com/S0889-5406(14)00867-1/sref27http://refhub.elsevier.com/S0889-5406(14)00867-1/sref27http://refhub.elsevier.com/S0889-5406(14)00867-1/sref27http://refhub.elsevier.com/S0889-5406(14)00867-1/sref26http://refhub.elsevier.com/S0889-5406(14)00867-1/sref26http://refhub.elsevier.com/S0889-5406(14)00867-1/sref26http://refhub.elsevier.com/S0889-5406(14)00867-1/sref25http://refhub.elsevier.com/S0889-5406(14)00867-1/sref25http://refhub.elsevier.com/S0889-5406(14)00867-1/sref25http://refhub.elsevier.com/S0889-5406(14)00867-1/sref24http://refhub.elsevier.com/S0889-5406(14)00867-1/sref24http://refhub.elsevier.com/S0889-5406(14)00867-1/sref24http://refhub.elsevier.com/S0889-5406(14)00867-1/sref23http://refhub.elsevier.com/S0889-5406(14)00867-1/sref23http://refhub.elsevier.com/S0889-5406(14)00867-1/sref23http://refhub.elsevier.com/S0889-5406(14)00867-1/sref23http://refhub.elsevier.com/S0889-5406(14)00867-1/sref22http://refhub.elsevier.com/S0889-5406(14)00867-1/sref22http://refhub.elsevier.com/S0889-5406(14)00867-1/sref22http://refhub.elsevier.com/S0889-5406(14)00867-1/sref21http://refhub.elsevier.com/S0889-5406(14)00867-1/sref21http://refhub.elsevier.com/S0889-5406(14)00867-1/sref20http://refhub.elsevier.com/S0889-5406(14)00867-1/sref20http://refhub.elsevier.com/S0889-5406(14)00867-1/sref20http://refhub.elsevier.com/S0889-5406(14)00867-1/sref20http://refhub.elsevier.com/S0889-5406(14)00867-1/sref19http://refhub.elsevier.com/S0889-5406(14)00867-1/sref19http://refhub.elsevier.com/S0889-5406(14)00867-1/sref19http://refhub.elsevier.com/S0889-5406(14)00867-1/sref18http://refhub.elsevier.com/S0889-5406(14)00867-1/sref18http://refhub.elsevier.com/S0889-5406(14)00867-1/sref18http://refhub.elsevier.com/S0889-5406(14)00867-1/sref17http://refhub.elsevier.com/S0889-5406(14)00867-1/sref17http://refhub.elsevier.com/S0889-5406(14)00867-1/sref17http://refhub.elsevier.com/S0889-5406(14)00867-1/sref16http://refhub.elsevier.com/S0889-5406(14)00867-1/sref16http://refhub.elsevier.com/S0889-5406(14)00867-1/sref16http://refhub.elsevier.com/S0889-5406(14)00867-1/sref16http://refhub.elsevier.com/S0889-5406(14)00867-1/sref15http://refhub.elsevier.com/S0889-5406(14)00867-1/sref15http://refhub.elsevier.com/S0889-5406(14)00867-1/sref15http://refhub.elsevier.com/S0889-5406(14)00867-1/sref14http://refhub.elsevier.com/S0889-5406(14)00867-1/sref14http://refhub.elsevier.com/S0889-5406(14)00867-1/sref14http://refhub.elsevier.com/S0889-5406(14)00867-1/sref14http://refhub.elsevier.com/S0889-5406(14)00867-1/sref13http://refhub.elsevier.com/S0889-5406(14)00867-1/sref13http://refhub.elsevier.com/S0889-5406(14)00867-1/sref13http://refhub.elsevier.com/S0889-5406(14)00867-1/sref12http://refhub.elsevier.com/S0889-5406(14)00867-1/sref12http://refhub.elsevier.com/S0889-5406(14)00867-1/sref12http://refhub.elsevier.com/S0889-5406(14)00867-1/sref11http://refhub.elsevier.com/S0889-5406(14)00867-1/sref11http://refhub.elsevier.com/S0889-5406(14)00867-1/sref11http://refhub.elsevier.com/S0889-5406(14)00867-1/sref10http://refhub.elsevier.com/S0889-5406(14)00867-1/sref10http://refhub.elsevier.com/S0889-5406(14)00867-1/sref10http://refhub.elsevier.com/S0889-5406(14)00867-1/sref9http://refhub.elsevier.com/S0889-5406(14)00867-1/sref9http://refhub.elsevier.com/S0889-5406(14)00867-1/sref9http://refhub.elsevier.com/S0889-5406(14)00867-1/sref8http://refhub.elsevier.com/S0889-5406(14)00867-1/sref8http://refhub.elsevier.com/S0889-5406(14)00867-1/sref8http://refhub.elsevier.com/S0889-5406(14)00867-1/sref8http://refhub.elsevier.com/S0889-5406(14)00867-1/sref7http://refhub.elsevier.com/S0889-5406(14)00867-1/sref7http://refhub.elsevier.com/S0889-5406(14)00867-1/sref6http://refhub.elsevier.com/S0889-5406(14)00867-1/sref6http://refhub.elsevier.com/S0889-5406(14)00867-1/sref6http://refhub.elsevier.com/S0889-5406(14)00867-1/sref6http://refhub.elsevier.com/S0889-5406(14)00867-1/sref5http://refhub.elsevier.com/S0889-5406(14)00867-1/sref5http://refhub.elsevier.com/S0889-5406(14)00867-1/sref4http://refhub.elsevier.com/S0889-5406(14)00867-1/sref4http://refhub.elsevier.com/S0889-5406(14)00867-1/sref3http://refhub.elsevier.com/S0889-5406(14)00867-1/sref3http://refhub.elsevier.com/S0889-5406(14)00867-1/sref3http://refhub.elsevier.com/S0889-5406(14)00867-1/sref3http://refhub.elsevier.com/S0889-5406(14)00867-1/sref2http://refhub.elsevier.com/S0889-5406(14)00867-1/sref2http://refhub.elsevier.com/S0889-5406(14)00867-1/sref2http://refhub.elsevier.com/S0889-5406(14)00867-1/sref1http://refhub.elsevier.com/S0889-5406(14)00867-1/sref1http://refhub.elsevier.com/S0889-5406(14)00867-1/sref1http://refhub.elsevier.com/S0889-5406(14)00867-1/sref1