-
7/28/2019 Articulo Dr. Dawson (1)
1/9
N e w d e f i n i ti o n f o r r e l a t in g o c c l u s i o n
t o v a r y i n g c o n d i t i o n s o ft h e t e m p o r o m a n
d i b u l a r j o i n t
P e t e r E . D a w s o n , D D S aCenter For Advanced Dental
Study, St. Petersburg, Fla.C e n t r i c r e l a t i o n i s t h e
a c c e p t e d t e r m f o r d e f i n i n g t h e c o n d y l a r
a x i s p o s i t i o n o f i n t a ct ,c o m p l e t e l y s e a
te d , p r o p e r l y a l i g n e d c o n d y l e - d i s k a s s
e m b l i e s . H o w e v e r , s o m e s t r u ct u r-a l l y d e
f o r m e d t e m p o r o m a n d i b u l a r j o i n t s m a y f u
n c t i o n c o m f o r t a b ly , e v e n t h o u g h t h e yd o n
o t f u l f i ll th e r e q u i r e m e n t s f o r c e nt r i c r
e l a ti o n . A w i d e r a n g e o f te m p o r o m a n d i b u
-l a r d i s or d e r s f r o m p a r t ia l t o c o m p l e t e d
i s k d e r a n g e m e n t s w i t h o r w i t h o u t r e d u c t
i o nm a y a d a p t t o a c o n f o r m a t i o n t h a t p e r m
i t s t h e jo i n t s t o c o m f o r t a b l y a c c e p t m a x
i m a lc o m p r e s s i v e l o a d i n g b y t h e e l e v a to r
m u s c l e s . T h e r e h a s b e e n n o a c c e p t e d t e r m
i n o l o g yt o d e f in e t h e c o n d i t io n o r p o s i t i
o n o f s u c h jo in t s . Th e p u r p o s e o f t h i s a r t i
c l e i s tod e f i n e a n e w t e r m , a d a p t e d c e n t r i
c p o s t u r e, a n d t o e x p l a i n i t s ra t i o n a l e a n
d h o w i t isd e t e r m i n e d . V e r i f i c a ti o n o f s u
c c e s s f u l a d a p t a t i o n i s a n i m p o r t a n t s t e
p i n d i a g n o s i s,b e c a u s e i t r u le s o u t s t r u c
t u r a l in t r a c a p s u la r d i s o r d e r s a s a s o u r c
e o f o r o f a c ia l p a ina n d e s t a b l i s h e s r e s p o
n s i b l e g u i d e l i n e s f o r i n i t i a t i o n o f o c c
l u s a l t r e a t m e n t o r p r o s t h e t i cd e n t i s tr y
. I t al s o e s t a b l i s h e s a m u c h n e e d e d t e r m i
n o l o g y f o r m o r e s p e c i f i c d e s c r i p t i o no f
t e m p o r o m a n d i b u l a r j o i n t p o s i t i o n a n d c
o n d i t i o n f o r c l i n i c a l r es e a r c h o n t h er e
la t io n s h ip b e t w e e n o c c lu s i o n a n d t h e t e m p
o r o ma n d ib u la r j o in t s . ( J PROSTHET
DENT1995;74:619-27.)
Confusion about the relationship between dentalocclusion and the
temporomandibula r joints (TMJs) hasbeen evident in the literature
for many years. Manyauthors advocate that condyle position is
critical to theequilibrium of the ma sticatory system at maximal
inter-cuspationYTM Others have argued that little or no
rela-tionship exists between faulty occlusion and temporoman-dibula
r disorders. 2~
In c ontrast to published information that occlusion is nota
factor in temporoman dibu lar disorders (TMDs), a reviewof the
literature suggests that such a conclusion is not to-tally
supported, because the information is routinelydevoid of specific
details about the position or the conditionof the temporomandibular
joints in relation to occlusalcontacts.20-2t F urt her confusion
results from the u se o f thesingle ter m "TMD" to denote a whole
constellation of signsor s ymptoms with no specificity of the type
of intracapsu-lar deformation or whethe r any s tructural
deformation haseven occurred.
It is important to determine the type of
intracapsulardeformation or change in TMJ structu res before
attempt-ing to determine the optimal relationship between
thetemporomandibularjoints and maximal intercuspation ofthe teeth.
B ecause the position of the condylar axis can be
aDirector.Copyright 9 1995 by The Editorial Council of THE
JOU~AL OVPROSTHETIC DENTISTRY.0022-3913/95/$5.00 + 0.
10/1/67765
altered by these changes , this article att empt s to clarify
therationale for positioning healthy condyle-disk assembliesin
centric relation and suggests more definitive terminol-ogy and
rationale for positioning temporomandibularjointsthat have
undergone intracapsular deformation and struc-tural change.
This article suggests three categories for
condyle-fossarelationships: centric relation, adapted centric
posture,and treatment position. These categories will be
defined,explained, and related to maximal intercuspation of
theteeth.C E N T R I C R E L A T I O N
Centric relation is defined in this article as the
preciselocation of the horizontal condylar axis when
properlyaligned condyle-disk assemblies are completely seated
intheir respective bony sockets. Because the position of
thehorizontal condylar axis determines the maxillo-mandib-ular
relationship during jaw closure, any variation incondyla r position
will change the closing arc of the mandi-ble and th us affect the
initial contact of the mandibularteeth against the maxillary teeth.
If maximal intercuspaltooth con tact is not coincident with the
completely seatedposition of both condyles, the condyles mus t be
displacedto achieve complete jaw closure into maximal
intercuspa-tion. Numerou s electromyographic studies reported
thatocclusal interferences to centric relation disrupt the
coor-dination of mas ticato ry muscle function. 25-3~
The most important criterion for centric relation is the
DECEMBER 1995 THE JOURNAL OF PROSTHETI C DENTISTRY 61 9
-
7/28/2019 Articulo Dr. Dawson (1)
2/9
T H E J O U R N A L O F P R O S T I t E T IC D E N T I S T R Y D
A W S O N
. , :
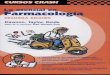
Fig. 1. In coordinated muscle function, triad of strong
el-evator muscles pulls condyles up slippery posterior slopesof
eminentiae. Inferior lateral pterygoid muscles releaseand stay
released th rough complete closure if no occlusalinterferences to
centric relation occur.
complete release of the lateral pterygoid muscles duringjaw
closure. 2 During jaw closure in intact TMJs thecondyle-disk
assemblies are pulled up t he eminent iae by atriad of stro ng
elevato r muscles (Fig. 1). To ensure a coor-dinated ne uromus
culatu re function, the release of inferiorlateral pterygoid muscle
contraction must allow thecondyles to slide up to the apex of force
positions,n~ at whichpoint th e medial pole of each condyle-disk
assemble wouldbe stopped by bone. This buttressed bone stop occurs
atthe height of concavity in the medial thir d of each fossa(Fig.
2). This relationship would then be considered theideally aligned
or completely seated condyle-disk assem-bly.
The condyles mus t be free to move down and up the pos-terior
slope of the eminence during function. The functionof the massete r
and internal pterygoid muscles shouldkeep th e condyles loaded 2
against the eminentiae in allexcursive movements (Fig. 3) and in
centric relation. Fol-lowing this philosophy, it may be more
descriptive to saythat centric relation is the most superior
position that theproperly aligned condyle-disk assemblies can
achieveagainst the eminentiae. This position would appear to
bephysiologic, because it results mechanically from coordi-nated
release function, which completely seats the condyle-disk
assemblies if no occlusal inclines interfere. Thesignificance of
this uppermost position is that only at thisbone-braced
relationship is the coordinated activity of theinferior lateral
pterygoid muscles achieved through com-plete closure. Ligament
bracin g is not a factor, because thecondyles can be displaced down
and back from centric re-lation before the ligaments reach their
functional limita-
tions. This "uppermost" position is a departure from theconcept
of"most retruded." To equate centric relation withthe "retruded
position" is still common in the literature,which, although it may
be confusing, is acceptable ifachieved by coordinated masticatory
muscles. I t should notbe considered centric relation if the
condyles are forcedaway from the eminent iae to a more retruded
position thanthe one achieved by the coordinated muscle function.
Un-fortunately, in patients under going dental procedures
thetechnique of pushing the jaw back to record centric relationis
still too prevalent.
The reason we advocate preciseness in l(~cating centricrelation
is because of the common clinical observation thateven the most
minute deflection from the bone-bracedcondyle position may activate
uncoordinat ed contraction ofthe lateral pterygoid muscles in
opposition to elevatormuscle contraction. Our observations of this
uncoordi-nated muscle activity suggests that it can result in
myo-fascial pain i f disrup tive occlusal contact is prolonged. It
isreasonably assumed th at prolonged isometric contractionof
antagonistic muscles can result in myogenous pain,particularly in
the smaller lateral pterygoid muscles,which are at a
disadvantage.
The trigger that activates lateral pterygoid contractioncan be
inconspicuous. The exquisit e sensitivi ty of peri-odontal and
interdenta l proprioceptive sensors can triggerpainful reflex
muscle patterns from deflective occlusal in-terferences tha t are
easily missed by clinicians who do notrecognize their impor tance
or the importance of verifyingthe accuracy ofcentric relation
before starting any occlusalcorrection procedures (Fig. 4).
In most, if not all, of he published studies th at downplaythe
role of occlusion, no att empt has been reported to pre-cisely
locate and verify an acc urate centric relation. If
thisverification is not done, any conclusions drawn regardingthe
relationship between correct occlusion and properlypositioned
temporo mandibul ar joints are highly suspect.
The mandible is in centric relation if four criteria
arefulfilled:1. The disk is properly aligned on both condyles.2.
The condyle-disk assemblies are at the highest pointpossible
against the posterior slopes of the eminentiae.3. The medial pole
of each condyle-disk assembly is braced
by bone.4. The inferior lateral pterygoid muscles have
releasedtheir contraction and are passive.If all four of these
criteria are fulfilled, he althy temporo-
mandibu lar joints in centric relation can accept all of
theloading that the elevator muscles can apply, because all ofthe
force is directed through avascular, noninnervatedstru ctures tha t
were designed to be load-bearing. 3236 If theupwa rd slide of the
condyle-disk assemblies is stopped bybone, no resistance should be
required from the inferiorlateral pterygoid muscles once the
condyles are completelyseated; therefore upward loading should not
alter their
620 V O L U M E 7 4 N U M B E R 6
-
7/28/2019 Articulo Dr. Dawson (1)
3/9
DAWSON THE JOURNAL OF PROSTHETIC DENTISTRY
Fi g. 2. The condyle-disk assemblies slide up convex posterior
slopes of eminentiae untilmedial poles (solid arrow) are stopped by
buttres sed bone at medial third of fossae. Circleindicates upper
most position at which medial pole braces aga inst bone (with disk
inter-posed). Lat eral two thirds of roof of fossa is thin and n ot
beari ng area.
Fig . 3. No muscles are in a position to distr act condyles. Whe
the r occlusal contac t is onanterior teeth only or posterior teeth
only, all elevator muscles combine to direct thecondyles
antero-superiorly in centric relation (A) and also keep th em
loaded agai nst em-inentiae as they travel up and down the slopes
in function (B).
passive state during closure or activate their contractioneven
during strong clenching. So unless the muscles aretriggered by a
disruptive occlusal contact that occursbefore maximal closure is
complete, the coordinated re-lease of he inferior lateral pterygoid
muscle should remainconsistent with elevator muscle contraction
during the re-petitive clenching posture associated with
swallowing.
When both condyle-disk assemblies are completelyseated in
centric relation, their medial poles should be at
the highest point of concavity of that part of each fossa.From
where the medial poles are stopped by bone the fos-sae walls curve
downward on three sides so that from acorrect centric relation, the
condyles cannot travel for-ward, backward, or medially without
moving downward(Fig. 5). The un der sta nding of this apex of force
position isextremely impor tant to our concept of centric relation.
I tmeans tha t failure to completely seat condyles when har
-monizing an occlusion invariably results in a muscle-
D E C E ~ m~ R x g gs 6 2 1
-
7/28/2019 Articulo Dr. Dawson (1)
4/9
THE JOURNAL OF PROSTHETIC DENTISTRY DAWSON
Fig. 4. Load testing conducted at suspected centric rela-tion
hinge position with torquing action start ing with gen-tle loading
first, then increasing pressure from light to veryfirm. Any sign of
tension or tend erness in either joint in-dicates that centric
relation has not been achieved. Fingersmust be placed on posterior
half of mandible duringmanipulation.
braced condyle instead of a bone-braced condyle. It alsomeans t
hat wheneve r the condyles go to their more upwardcentric relation
position during function, the closing forcesare directed more on
the most posterior teeth, whichbecome pivotal to the upward moving
condyles (Fig. 6).
Contra ry to some opinions tha t centric relation is not
afunctional position, that observation has not been sup-ported by
extensive researc h at the University of Florida isor in studies
that show that the retruded position is usedfrequently in
swallowing. 37 If the idea t hat the condyles dogo repeatedly to
centric relation is doubted, it would onlybe necessary to observe
the facets of wear on the teeth ofa numb er of patients. Casts mo
unted correctly in centricrelation routinely show that if wear
facets are present, thefacets always extend to centric relation on
tooth inclinesthat interfere with centric relation.
A study of condyle/fossa anatomic condition makes itevident that
the medial wall of the fossa braces against themedial pole of he
condyle disk assembly when the condylesare in centric relation.
This fact is why centric relation isthe midmost position of the
mandible (Fig. 7). Thus fromcentric relation it is not possible for
eithe r condyle-disk as-sembly to move horizontally toward the
midline. I f such amovement occurs, it is an indication t hat the
condyles werenot completely seated in centric relation at the start
ofmovement. From centric relation the orbiting condylemust move
downward as it moves medially.
A D A P T E D C E N T R I C P O S T U R EMany TMJs function with
complete comfort and appar-
ent normalcy, even though they have undergone deforma-tion
caused by disease, trauma, or remodeling and there-fore
automatically c annot fulfill all of our criteria for cen-tric
relation. Some TMJs click or exhibit other signs ofintracapsular
disorder, but they do not prevent patientsfrom functioning in an
acceptable and comfortable man-ner. Determining whether a deformed
TMJ can functionacceptably with comfort and with a reasonable
degree ofstability is one of the m ost impo rtant decisions in the
di-agnostic process.
The author defines adapted centric posture as the rela-tionship
of the mandible to the maxilla that is achievedwhen deformed
temporom andibular joints have adapted tothe degree that they can
comfortably accept firm loadingwhen completely seated at the most
superior positionagainst the eminentiae.
Like centric relation, adap ted centric posture is a hori-zontal
axial position of the condyles. It occurs irrespectiveof vertical
dimension or toot h contact. It is also a midmostposition, because
even if the disk is totally displaced, themedial pole of the
condyle adapts to the concavity of thefossa and maintains contact
against its medial incline.
The mandible is in adapted centric posture if four crite-ria are
fulfilled:1. The condyles are comfortably seated at the
highestpoint against the eminentiae.2. The medial pole of each
condyle is braced by bone. (Thedisk may be partially interposed.)3.
The inferior lateral pterygoid muscles have released
contraction and are passive.4. The condyle-to-fossa
relationships occur at a manage-able level of stability.The
consequences of adaptive changes in the temporo-
mandi bular articulation may be positive or negative withregard
to symptoms. The same adaptive changes that re-sult in reduction of
symptoms may simult aneously produceserious and progressive
deformation ofintracap sular struc-tures and dama ge to collateral
structures eleswhere. Teethand supporting structures can be
especially affected bystruc tural changes of the TMJs. We note that
excessiveocclusal wear or hypermobility of teeth is routinely
ob-served as disharmony between the TMJs and the
occlusionprogresses. 3s Our clinical observation is consistent:
unsta-ble TMJs result in unstable occlusions.
Adapted centric posture m ay be achieved in a variety
ofintracapsular deformations. The progression from ahealthy, intact
TMJ to one that is deformed and hasadapted may include stages that
produce pain and dys-function as the adaptation process takes
place. The pro-gression of deformation ma y occur with little or no
intra-capsular pain. Diagnosis made on the basis of symptomsonly is
insufficient and may lead to false assumptionsabout the source of
pain in patients with TMD.
622 VOLUME74 NUMBER6
-
7/28/2019 Articulo Dr. Dawson (1)
5/9
DAWSON THE JOURNAL OF PROSTHETIC DENTISTRY
Fig. 5. Medial pole of each condyle-disk assembly is braced
against uppermo st roof ofconcavity at medial third of each fossa.
From t hat seated position condyles cannot moveforward, backward,
or medialward without t raveling downward (circle represents
medialpole position). Because an terio r face of each condyle disk
assembl y ( l ine wi th three arrows)is against eminence in centric
relation, no forward translat ion is possible without down-ward
movement.
Proper diagnosis requires an orderly evaluation ofintra-capsular
struct ures, not jus t to see wheth er deformation ispresent but to
determine t he specific stage of deformationresponsible for the
discomfort. The clinical experience ofthe author has shown that in
most patients with so-calledTMD, the discomfort is far more likely
to be myogenousrather than intracapsular, even when some
deformationhas occurred within the intracapsular structures. This
di-agnosis cannot be determin ed on the basis
ofepidemiologicpercentages. It must be determined by specific
testing ofeach individual patient to determine whether any
intrac-apsula r stru ctures are disordered, and, if they are
de-formed, to determine whether they have adapted to amanageab le
level of comfort and stability. A combinationof history, load
testing, auscultation, and palpation canusually lead to a
diagnosis, but some type of imaging ma ybe needed for
specificity.
Some of the most common intracap sular conditions thatmay permi
t an a dapted centric posture are (1) lateral poledisk derangements
, (2) complete disk derangements withformation of a pseudo-disk,
(3) complete disk displacementwith perforation, and (4) other
partial disk derangementsand asymptomatic clicking TMJs.L a t er a
l p o l e d i s k d e r a n g e m e n t s
Piper's classification of intra capsul ar disorders
distin-gnishes between lateral pole disk derangements andderang
ement s in which the disk is displaced off both thelateral and
medial poles of the condyle. If the disk is not
displaced off the medial pole, it is possible to achieve
com-plete seating ofthe condyle with no discomfort. This is
trueeven when a lateral pole click has progressed to closed lockof
the lateral half of the disk. I f the intraca psular defor-mation
is intercepted at these stages, it has been our clin-ical
experience that stability of the articulation can beachieved if
harmon y is established be tween the occlusionand the completely
seated condyle-disk assemblies.
The experience of the author also suggests that lateralpole disk
derang ements can be treated as normal joints ifthe medial pole
disk alignment is acceptable and if adaptedcentric posture can be
veri fied by load tes ting. 39 In my ex-perience the key to success
is in main taini ng coordinatedmusculature function through
elimination of all occlusalinterferences to a verified adapted
centric posture.C o m p l e t e d i sk d e r a n g e m e n t s w i
t h f o r m a t i o no f a p s e u d o d i s kIn the early stages
of a complete disk displacement it isthe experience of the a uthor
tha t a period exists duringwhich pain is a symptom. Considerable
pain may resultfrom compression of the vascular and richly
innervatedretrodiskal tissue by the condyle (Fig. 8). If this
compres-sion occurs, adapted centric posture cannot be
achievedbecause the TMJ will not accept loading without some
de-gree of discomfort. Although not predictable, the retrodis-kal
tissue is sometimes converted to a fibrous connectivetissue
pseudo-disk. We have observed such pseudo-diskformation in cadaver
specimens, in open-joint microsur-
DECEMBER 1995 62 3
-
7/28/2019 Articulo Dr. Dawson (1)
6/9
THE JOURNAL OF PROSTHETIC DENTISTRY DAWSON
A
, ~ l [ [ / [ [ i l F i g . 7 . M e d i a l p o l e b r a c i n
g in l i n e w i t h m e d i a l p t e r y g o i dt i i[IIr m u s c
l e c o n t r a c ti o n e s t a b l i sh e s midmosto s i t i o n
a t c e n t r i c: ~ ~ ~ ~ re la tio n. T hi s m i dm o st p os i t
i o n is c on si s te nt ly s m u lt a-' n e o u s w i t h u p p e
r m o s t p o s it io n .
! ~ f i l l
F i g . 6 . B e c a u s e c o nd y le s m u s t d i sp l ac e d
o w n w a r d t o a c- ~ xc o m m o d a t e i n t e r c u s p a l p
o s i ti o n t h a t i s f o r w a r d o f c e n t ri cr e l a t io
n ( A ), m o s t p o s t e r i o r t o o t h t h a t i n t e r f e
re s b e c o m e sp i v o t a l p o i n t w h e n c o n d y l e s a
r e p u l l e d u p i n t o c e n t r i c r e - F i g . 8 . I n e a
r l y s t a g e s o f c o m p l e t e d i s k d e r a n g e m e n t
,l a t io n . B , I n f e r i o r l a t e r a l p t e r y g o i d m
u s t r e m a i n a c t i v e l y c o n d y l e l o a d s o n t o v
a s c u l a r , r e t r o d i s k a l t i s s u e , w h i c h i sc
o n t r a c t ed w h e n e v e r t e e t h a r e i n t e r c u s p
a te d , r i c h ly i n n e r v a t e d . W h e n t h i s s t r u c
t u r a l m i s a l i g n m e n t o c-
c u r s, T M J c a n n o t a c c e p t l o a d i n g w i t h o u
t p a i n .g e r y , a n d o n m a g n e t i c r e s o n a n c e i
m a g e s . I f t h i s f o r m a t i o no c c u r s, i t i s p o s
s i b l e t h a t b l o o d v e s s e l s a n d t h e i r a c c o m
p a -n y i n g s e n s o r y n e r v e s w i ll e v a c u a t e t h
e b e a r i n g a r e a , a n dt h e f i b r o u s e x t e n s i o
n o f t h e o r i g i n a l d i s k w i ll e v e n t u a l l y b ea
b l e t o a c c ep t l o a d i n g w i t h n o d i s c o m f o rt .
I t m a y t h e n b ep o s s ib l e t o a c h i e v e a n a d a p t
e d c e n t ri c p o s t u r e t h a t a p p e a r st o b e a s s t
a b l e a s a n i n t a c t c o n d y l e - d i s k a l i g n m e n
t .C o m p l e t e d is k d i s p l a c e m e n t w i t h p e r f o
r a t io n
T h e m o s t l i k e l y p r o g r e s s i o n f r o m a c l o
se d - lo c k , a n t e r i o rd i s p l a c e m e n t o f t h e d
i s k i s to p r o c e e d t h r o u g h a p a i n f u ls t a g e o
f c o m p r e s s i o n o f t h e r e t r o d i s k a l t i s s u e
s , w h i c h b e -c o m e l e s s p a i n f u l a s t h e c o n d
y l e p e r f o r a t e s t h e s e n s i t i v e
v a s c u l a r t i s su e s a n d b e g i n s t o l o ad a g a
i n s t b o n e . A s t h es o f t - t i s s u e p e r f o r a t i
o n e x p a n d s , a c o m p l e t e b o n e - t o - b o n ec o n
t a c t m a y r e s u l t t h a t p e r m i t s l o a d i n g w i t
h n o i m p i n g e -m e n t a g a i n s t i n n e r v a t e d s t
r u c tu r e s . A t t h i s s t a g e i t is p os -s i b le t o v
e r i f y a n a d a p t e d c e n t ri c p o s t u r e b y t h e a
b s e n c e o fd i s c o m f o r t w h e n t h e c o n d y l e s a
r e l o a d e d .
T h e t y p i c a l s e q u e n c e o f e v e n t s t h a t w e
h a v e e x p e r i e n c e da f t e r t h e r e t r o d i s k a l
t i s s u e i s p e r f o r a t e d i s a p r o g r e s s i v ef l
a t t e n i n g o f b o t h t h e c o n d y l e a n d e m i n e n c
e . T h e o s t e o a r -t h r i t i c d e f o r m a t i o n s t a
r t s a t t h e a r t i c u l a r c a r t i l a g e , c a u s-i n g
a l o s s o f h e i g h t o f t h e c o n d y le . B e c a u s e t
h e p e r f o r a t i o n
62 4 VOLUME 74 NUMBER 6
-
7/28/2019 Articulo Dr. Dawson (1)
7/9
DAWSON THE JOURNAL OF PROSTH ETIC DENTISTRY
and disk dera ngeme nt d isrupts the flow of synovial
fluid,nourishment to the articular surfaces is compromised.Thus the
osteoarthritic joint is not completely stable.Although the condyle
will continue to lose height as itsbearing surface breaks down, the
deformation can usuallybe slowed to a manage able condition by
reestablishing co-ordinated muscle function and reducing muscle
hyperac-tivity. Any discomfort in this type of problem is
invariablymyogenous. It can be readily resolved by restoring
har-mony between the occlusion and the completely seatedTMJs, even
though they have undergone deformation.
It is the author's contention that patients with
slowlyprogressing osteoarthritis can be made as comfortable
aspatients with intact TMJs if occlusal harmony is estab-lished
with adapted centric posture. If both condyles canaccept loading
with no discomfort, relief of myofascial painis highly predictable
if all occlusal interferences to thebone-braced condyle position
are completely eliminated.Typically, it is necessary to adjust the
occlusion periodi-cally as condylar height is lost, but it does not
create aman agem ent problem if patients are informed of this
needin advance. In my clinical experience minimal correctionsto the
occlusion are all t hat is needed at 9- to 12-month in-tervals to
maintain comfort in the masticatory muscula-ture.O t h e r p a r t
i a l d i s k d e r a n g e m e n t s a n da s y m p t o m a t i c
c l i c k i n g T M J s
Reciprocal clicking is a sign that some degree of defor-mation
has occurred in the diskal ligaments. The varia-tions in
deformation of the ligaments and the disk appearunlimited. However,
many clicking and deformed jointshave a dapted sufficiently so that
they can comfortably ac-cept loading. If a structur al analysis
shows that the condi-tion is reasonably stable, adapted centric
posture may beachieved, even though the disk is deranged and a
click ispresent. The key to successful treatm ent of adapted TMJsis
the complete seating of both condyles so that the inferiorlateral
pterygoid muscles can release their contractionduring closure all
the way to maximal intercuspation.T R E A T ME N T P O S I T I O
N
Three general types ofintr acapsular disorders result inpain or
discomfort when the temporo mandibul ar joints areloaded.1. In
complete displacement of he disk, disk displacementis almost always
anterior to the condyle, which resultsin compression of the
vascular, innervated, ret rodiskalstructures. If the disk is not
reducible and compressionofretrodi skal tissue causes discomfort,
it is necessary todetermine a tre atment position for the condyle
for thepurpose of developing an adapted centric posture thatcan
even tually acce pt loading.2. Retrodiskal inflammation and ede ma
usually occurs asa result of trau ma and ma y or may not be
associated
with disk displacement. When the retrodiskal tissuesare swollen
and painful, t he condyles cannot completelyseat to either centric
relation or adapted centric posturewithout compressing these
structures. A treatme nt po-sition that reduces the compressive
force and allows theinflamma tion to subside should be determined.
Antiin-flammatory medication and soft diet are recommendedin
combination with the use of a trea tme nt position thatis protruded
enough to prevent compression of retro-diskal tissue. The condyles
should be permitted toretu rn to centric relation or adapted
centric posture assoon as the edema is reduced, which is usually a
mat-ter of a few days.3. Pathologic conditions and struc tural or
functional dis-orders that affect the ability of the int racaps
ular struc-tures to accept loading can result from a variety
ofcauses. The basic rule is, "If the TMJs ca nnot acceptloading
with complete comfort...find out why."
Differential diagnosis must first confirm tha t the sourceof
pain is within the i ntraca psular structure s an d not iso-lated i
n muscle. Load testing is the most effective way tomake that
determination. Masticatory muscle pain iscommon when int racapsu
lar pathosis is present, becausethe muscles tend to protect the
painful joint from overload.Attemp ting to treat mastica tory
muscle problems withoutknowledge of the specific type of intracaps
ular problem isinappropriate. Appropriate treatment combines an
at-tempt to resolve the intra capsul ar problem while
simulta-neously establishing equilibrium within the total
mastica-tory system. If this procedure requires harmonization ofthe
occlusion with a t empor ary trea tmen t position for thejoints,
that decision should be based on determining theoptimal treatment
position first.Not all pathologic deformation results in pain on
loading.It is sometimes possible to load condyles with advancedbone
disease, but the condition may be too unstable towarrant treatment
procedures that are irreversible. Acomplete diagnosis including
history, palpation, load test-ing, Doppler auscultation, range and
path of motion test-ing, and appropriate imaging should be used to
determinea specific diagnosis. 2, 39 Blood studies, surgical
exploration,or both may be needed in some cases. It is not the
purposeof this article to outline all the protocols for diagnos ing
thewide range of diseases tha t may be encountered. Advance-ments
in diagnostic tests and imaging capabilities make itdifficult for
structural disorders to hide from an astute di-agnostician.D e t e
r m i n a t i o n o f t r e a t m e n t p o s i t i o n
The need for a trea tmen t position can be determined af-ter it
has been verified that neither centric relation oradapted centric
posture can be achieved. Two objectivesexist in determining the
most favorable trea tmen t positionfor the condyles: (1) relief of
pain, and (2) eventual stabi-lization of he condyles in either
centric relation or adaptedcentric posture.
DECEMBER 1~5 625
-
7/28/2019 Articulo Dr. Dawson (1)
8/9
T H E J O U R N A L O F P R O S T H E T I C D E N T I S T R Y D
A W S O N
I t m a y b e d i f fi c u l t t o d e t e r m i n e w h e t h e
r a t r e a t m e n t p o -s i t i o n is n e c e s s a r y i f l a
t e r a l p t e r y g o i d m u s c l e c o n t r a c t i o ni s n
o t r e l e a s e d . T h e p a i n o f m u s c l e s p a s m o r p
r o l o n g e d h y -p e r c o n t r a c t i o n m a y m a k e i t
t o o d i f f i cu l t t o a c h i e v e co m -f o r t a b l e s e
a t i n g o f t h e c o n d y l e s , e v e n w h e n n o i n t r a
c a p s u -l a r d i s o r d e r is p r e s e n t . U n l e s s a n
a c t i v e i n t r a c a p s u l a r d i s-o r d e r is o b v i o
u s, a n a t t e m p t s h o u l d b e m a d e t o d e p r o g r a
ml a t e r a l p t e r y g o i d c o n t r a c t i o n b e fo r e a
s s u m i n g t h a t t h eT M J s a r e t h e p r i n c i p a l s
o u r c e o f t h e p a i n . I t i s s u g g e s t e dt h a t t h
i s d e p r o g r a m m i n g i s b e s t d o n e b y c o m p l e t
e l y se p -a r a t i n g a l l p o s t e r i o r t o o t h c o n t
a c t b y u s i n g a s m o o t h , f l a t,a n t e r i o r b i t e
p l a n e . S u c h a p e r m i s s i v e s p l i n t a ll o w s t
h em u s c l e s t o m o v e t h e m a n d i b l e i n c o o r d in
a t e d f u n c t io n t h a ti s u n d i s t u r b e d b y d e f l
ec t i v e t o o t h c o n t a c t s . I f t h e p e r m i s -s i v
e s p l i n t p e r m i t s r e l e a s e o f l a t e r a l p t e r
y g o i d m u s c l e c o n -t r a c t i o n a n d a l l o w s t h
e c o m p l e t e s e a t i n g o f t h e c o n d y l e s t oc e n
t r i c r e l a t i o n o r a d a p t e d c e n t r i c p o s t u
re , u s e o f a t r e a t -m e n t p o s i t i o n w i l l n o t b
e n e c e s s a r y . T h e r e l i e f o f o c cl u so -m u s c l
e p a i n o c c u r s q u ic k l y , m o s t o f t e n w i t h i n
h o u r s w h e na l l o c c l u s al i n t e r f e r e n c e s a r
e e l i m i n a t e d . I f t h e p e r m i s s i v es p l i n t d
o e s n o t r e s u l t i n r e l i e f o f a l l d is c o m f o r
t w h e n t h ec o n d y l e s a r e l o a d - t e s t e d , a n i
n t r a c a p s u l a r d i s o r d e r is s u s -p e c t e d , a n
d f u r t h e r t e s t i n g i s i n o rd e r t o d e t e r m i n
e w i t hs p e c i fi c i t y t h e t y p e o f s t r u c t u r a l
d i s o r d e r t h a t i s p r e s e n t .T h e t r e a t m e n t
p o s i t i o n t h a t i s s e l e ct e d s h o u l d b e s p e ci
f i cf o r t h e t y p e o f d i s o r d e r t h a t i s d i a g n
o s e d .
S U M M A R YL a c k o f d e f i n i t i v e t e r m i n o l o g
y t o c l a r if y d i f f e r e n t p o s i-
t i o n s a n d c o n d i t i o n s o f t h e t e m p o r o m a
n d i b u l a r j o i n t s h a sc a u s e d c o n f u s i o n i n
t h e l i t e r a t u r e a n d h a s c o m p l i c a t e ds c i e
nt i fi c d i s c u s s i o n r e g a r d i n g t h e r e l a t i o
n s h i p o f t h eT M J s t o o c c l u s i o n .
U s e o f t h e n o n s p e c i f i c t e r m T M D i s in a d e
q u a t e f o rd e s c r i b i n g s p e c i fi c d i s o r d e r s
o f t h e m a s t i c a t o r y s y s t e m .T h e t e r m T M D d
o e s n o t s pe c i fy w h e t h e r a d is o r d e ri n v o l v e
s d e f o r m a t i o n o f i n t r a c a p s u l a r s t r u c t u
r e s , d o e s n o ts p e c if y w h e t h e r a d i s o r d e r i
s p r i m a r i l y a m a s t i c a t o r ym u s c l e p r o b l e
m w i t h o r w i t h o u t i n t r a c a p s u l a r d e f o r m a
-t io n , d o e s n o t s p e ci f y w h e t h e r a d e f o r m e
d T M J h a s a d a p t e ds u f f i c ie n t l y to a c c e p t l
o a d i n g w i t h o u t d i s c o m f o r t , d o e s n o ts p e
c if y w h e t h e r a n a d a p t e d T M J i s s t a b l e or u n
s t a b l e , a n dd o e s n o t s p e c i fy t h e t y p e o f d e
f o r m a t i o n o r p a t h o s i s w i t he n o u g h c l a r i
t y to b e m e a n i n g f u l i n d e t e r m i n i n g a n o p t
i m a lt r e a t m e n t p o s i t i o n f o r T M J s t h a t c a
n n o t a c c e p t l o a d in g .
I t is t h e a u t h o r ' s b e l i e f t h a t u n c o o r d i
n a t e d , h y p e r a c t i v e ,m a s t i c a t o r y m u s c l
e s a r e t h e p r i m a r y s o u r c e o f r e p e t i t iv e ,t
e n s i v e , a n d c o m p r e s s i v e fo r c es a g a i n s t t
h e T M J s a n d t h et e e t h a n d o t h e r m a s t i c a t o
r y s y s t e m s t r u c t u r e s . I t i s t h ea u t h o r ' s
b e l i e f t h a t a n a l y s i s o f t h e c a u s e s f o r m a
s t i c a t o r ym u s c l e p a i n o r d y s f u n c t i o n m u
s t i n c l u d e a c c u r a t e d e s c r i p -t i o n o f t h e
r e l a t i o n s h i p o f t h e o c c l u s io n t o t h e p o s
i t i o n a n dc o n d i t i o n o f t h e T M J s .
R E F E R E N C E S
1. Rami~ord SP, Ash MM . Occlusion. 4th ed. Phi ladelphia: WB
Sau ndersCo, 1983:76.2. Dawson PE. Evahia t ion, diagnosis and t re
atm ent of occ]usal problems.2nd ed. St Louis: CV Mosby Co,
1989:28-39.3. Celenza FV, Na sedkin JN. Occlusion, the state of the
ar t . Chicago:Quintessen ce Publ ish ing Co Inc, 1978:31-46.4.
Gilboe D. Centric rela tion as th e tre at m en t position. J
PROSTI-IETDENT1983;50:685-9.5. Wil l iamson EH . Larainographic
study o f ma ndibu lar condyle posi tionwh en reco rding cen tric
relation. J PROSTHETDENT 1978;39:561-4.6 . G ibbs CH, L undeen HC,
M ahan PE , e t a l . Movemen t s o f t he m ola rteeth a nd m and
ibula r condyles dur ing chewing [Abstract]. J De nt
Res1980;59:915.7. Lucia VO. A tec hniq ue for reco rding cen tric
relation. J PaOSTKETDENT1964;14:492-505.8. Gra nge r ER. Cen tric
relatio n. J PROSTHET DENT 1952;2:160-71.9. O keson JP. Ma nage men
t of temp orom andibu lar disorders an d occlu-sion. 3rd ed. St
Louis: Mosby-Year Book, 1992:110-1.10. Guiche t NF. Biologic a ws
governing unct ions ofmuscles tha t move themand ible. Par t 1:
Occlusal programming. J P rosthe t Dent 1977;37:648-56 .Long JH Jr.
Locating ce ntric relatio n wi th a lea f gauge. J PROSTHETDENT
1973;29:608-10.Woelfel JB. A new device for accurately recording
centric relation. JPROSTHET DENT 19 86;5 6:71 6-27 .McHorr is WH. O
cclusal adjustm ent via selective cut t ing of natu ralteeth. Pa r
t I . Int J Per iodont Rest Den t 1985;5:8-25.L aur i t zen AG.
Func t iona l ana lys i s t echn ique in t h e n a tu r a l den t i
ti on :atla s of occlusal analysis. C olorado Springs: HAH
Publications, 1974.Schuyler CH. F und am enta l pr inciples in the
correct ion of occlusal dis-harmon y, natu ral and ar ti ficial . J
Am D ent Assoc 1935;22:1193-202.Lytle JD. The clinicians in dex of
occlusal disease: definition, recogni-t ion and man agem ent . Int
J P er iodont Rest Dent 1990;10:102-23.Beyron H. Opt im al
occlusion. De nt C l in Nor th Am 1969;13:537-54.Lund een HS, Gibbs
CH. Advances in occlusion. Boston: Joh n W right ,1982.Man n AW,
Pankey L D. Or a l r ehab i li t a t ion . Pa r t I : Use o f t he
P - M in -s t r ume n t i n t r ea tm en t p l ann ing and in r es
to r ing the l ower pos te r io rtee th. J PROSTHET DENT 1960
;10:135-5 0.20. Greene CS. Orthodont ics andtem porom
andibulardisorde rs. Den t Cl inNor th A m 1988;32:529-38.21. Lipp
MJ. Tem porom andibular symp toms and occlusion: a review of hel i
terature a nd the concept. N Y State De nt J 1990:56:58-66.22.
Dworkin SF, Ha nson Huggins K, Le Resche LH, et al . Epidemiology
ofsigns and symp toms in temp orom andibu lar disorders: cl inical
signs incases and controls. J Am D ent Assoc 1990;120:273-81.23.
Goodman P, G reene CS, Laskin DM. Response of pat iente wi th
myo-fasclal pain-dysfunction synd rom e to mock equilibration. J Am
D entAssoc 1976;92:755-8.24. Adler RC. W hat do a leech and a han
dpiece have in common? J CranioPractice 1993;11:1.25. Ramijord SP.
Dysfunctional temporom andibu lar oint and muscle pain.J PROSTHET
DENT 1961;11 :353-74.26. Bakk e M, Moller E . Distor tion ofm axim
um elevator activity by uni lat -eral tooth contact . Scand J Den t
Res 1980;80:67.27. Ri ise C, S heikholeslam A. The inf luence of
exper ime ntal inter fer ingocclusal contacts on postural act ivi
ty of the anter ior temporal andma ssete r muscles in young adul
ts. J O ral Rehabi l 1982;9:419-25.28. Wil l iamson EH, Lund qnist
DO. Anter ior guidance: i t s ef fect on elec-t romyographic act
ivi ty of the tem poral an d ma ssete r muscles. J PRos-THET DENT
1983;49:816 -23.29 . Hann am AG, DeCow RE , Sco tt JD , Wood WW. T
he r e l a t i onsh ipbetwee n denta l occlusion, muscle ac t ivi
ty and associated jaw move-me nt in m an. A rch Oral Biol
1977;22:25-32.30. M aha n PE, Wilkinson TM, Gibbs CH, Ma uder l i
A, Brannon LS. Supe-r ior and in fer ior bell ies of the latera l
pterygoid EM G act ivi ty at b asicjaw posi t ions. J Prosthe t
Dent 1983;50:710-8.31. Schae fer P. Stal la rd RE, Zander HA.
Occlusal inter ferences and mas-tication: an electrom yograp hic
stu dy . J PROSTHET DENT 1967;1 7:438-49 .
11 .12 .13 .14 .15 .16 .17 .18 .19 .
62 6 VOLUME 74 NVMBE R
-
7/28/2019 Articulo Dr. Dawson (1)
9/9
D A W S O N T H E J O U R N A L O F P R O S T H E T I C D E N T
I S T R Y
32. Zola A. Morphologic limiting factors in the temp
oromandibular oint. JPROSTHET DENT 1963;13:732-40.33. Sicher H. The
temporomand ibular oint. In: Sarnot BG, editor. 2nd ed.Springfield,
Ill: Charles Thomas Publisher, 1964.34. Mansour RM, Reynik RJ. In
vivo occlusal forces and moments: forcesmeasured in t erminal hinge
position and associated moments. J DentRes 1975;54:114-20.35. Smi
th DM, McLochlan KR, McCall WD. A numerica l model of
tem-poromandib ular join t loading. J Dent Res 1986;65:1046-52.36.
Hylander WL. The human mandible: leverorlink. Am J Phi p Anthro-pol
1975;43:227-42.37. Gra f H, Zander HA. Tooth contact pat ter ns in
mast ication. J PEOSTHETDENT 1963;13:1055-66.
38. Schellhas KP, Piper MA, Omlie MR. Facial skeleton remodel
ing due totemporomandibular joint degeneration: an imaging study of
100patient s. Am J Neuroradiol 1990;11:541-51.39. Dawson PE, Pipe r
MA. Temporomand ibula r disorders and orofacialpain. Seminar
Manual. St Petersburg: Center for Advanced DentalStudy,
1993:130-45.Reprint requests to:DR. PETER E. DAWSON1 1 1
SECONDAVE., NESurrE 1109ST. PETERSBURG, FL 33701
B o u n d v o l u m e s a v a i la b l e to s u b s c r i b e r
sBound volumes of THE JOURNALOF PROSTHETICDENTISTRYare available to
subscribers
(only) for the 1995 issues from the publ isher at a cost of
$72.00 ($85.00 internati onal) forVol. 73 (Janua ry-J une ) and
Vol. 74 (July-December). Shipping cha rges are included. Eac hbound
volume contains a subject and a utho r index, and all advertising
is removed. Copiesare sh ipped within 30 days after publication of
the las t issue in the volume. The bindingis durable buckram with
the journal name, volume number, an d yea r stamped in gold onthe
spine. Volumes 71 and 72 are also available. Payment must accompany
all orders.Contact Mosby- Year Book, Inc., Subscription Services,
11830 Westline Ind ustri al Drive,St. Louis , MO 63146-3318, USA;
phone (800)453-4351, or (314)453-4351.S u b s c r i p t i o n s m u
s t b e i n fo r c e t o qu a l if y . B o u n d v o l u m e s a r
e n o t a v a i l a b l e i n
p l a c e o f a r e g u l a r JO UR NA L s u b s c r i p t i o n
.
D E C E M B E R 1 ~ 5 627