Embed Size (px)
Citation preview

Hemoglobin, 36(2):157–160, (2012)Copyright © Informa Healthcare USA, Inc.ISSN: 0363-0269 print/1532-432X onlineDOI: 10.3109/03630269.2012.658129
SHORT COMMUNICATION
ASSOCIATION OF Hb NEW YORK WITH Hb E AND α0-THALASSEMIA
IN A CHINESE WOMAN IDENTIFIED BY SEBIA CAPILLARYS2 SYSTEM
Dong-Zhi Li, Jian-Ying Zhou, Xing-Mei Xie, and Can Liao
Prenatal Diagnostic Center, Guangzhou Maternal & Neonatal Hospital, Guangzhou Women &Children Medical Center, Guangzhou Medical College, Guangzhou, Guangdong, People’sRepublic of China
� We describe a Chinese woman who was assumed to be heterozygous for both Hb E[β26(B8)Glu→Lys] and α0-thalassemia (α0-thal) by a high performance liquid chromatography(HPLC) method, but was later also shown to be a Hb New York [β113(G15)Val→Glu] heterozy-gote by the Sebia CapillaryS2 system. This study suggested that a single test is never sufficient toallow the correct diagnosis of an abnormal hemoglobin (Hb). We also emphasize the importance ofa correct diagnosis of interactions between α- and β-thalassemias.
Keywords Hemoglobin (Hb) variant, Hb E, Hb New York
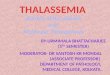
A Chinese couple screened positive during our prenatal thalassemiascreening program at the mother’s early gestation. The husband had a clas-sic α-thalassemia (α-thal) trait (RBC 5.8 × 1012/L, Hb 13.7 g/dL, MCV 65.1fL, MCH 23.0 pg, Hb H bodies [+], Hb A 97.6%, Hb A2 2.4%). The 28-year-old mother had a mild anemia (RBC 4.9 × 1012/L, Hb 10.7 g/dL, MCV 62.0fL, MCH 22.2 pg and Hb H bodies [−]). Hemoglobin (Hb) analysis usinghigh performance liquid chromatography (HPLC) (Bio-Rad Laboratories,Hercules, CA, USA) showed a Hb E [β26(B8)Glu→Lys] trait (Hb A win-dow 64.4%, Hb A2 + E 25.3% and Hb F 2.7%) in the mother (Figure 1a).Single-tube multiplex gap-polymerase chain reaction (gap-PCR) was used todetect the three common deletional α-thalassemias (– –SEA, –α3.7 and –α4.2),
Received 30 October 2011; Accepted 2 December 2011.Address correspondence to Dr. Can Liao, Prenatal Diagnostic Center, Guangzhou Women & Chil-
dren Medical Center, Jinsui Road 9, Zhujiang New Town, Guangzhou, Guangdong 510623, People’sRepublic of China; Tel./Fax: +86-20-38076078; E-mail: [email protected]; [email protected]
157
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Way
ne S
tate
Uni
vers
ity o
n 11
/26/
14Fo
r pe
rson
al u
se o
nly.

158 D.-Z. Li et al.
(a)
(b)
FIGURE 1 Chromatograms of Hb analysis in the patient. (a) VARIANT IITM (Bio-Rad Laboratories)HPLC pattern. (b) Sebia CapillryS2 pattern.
and both of the partners were shown to be carriers of the – –SEA deletion.This was the mother’s first pregnancy. At 11 weeks of the gestation, prena-tal diagnosis was performed using chorionic villus sampling. The fetus wasdiagnosed as homozygous α-thal (– –SEA/– –SEA), and the pregnancy wasterminated immediately.
Accidentally, the blood sample from the mother was sent to be testedin a program aimed at comparing two methods of analysis in thalassemiascreening: HPLC and the Sebia CapillryS2 system (Sebia, Paris, France). TheHb patterns investigated using the capillary electrophoresis system showedanother Hb variant that automatically positioned in zone 11 with regard tothe Hb A fraction (Figure 1b). The on-board Hb library within this zone listsonly one variant: Hb New York [β113(G15)Val→Glu]. This was confirmedby DNA sequencing (Figure 2). Thus, the mother was a compound heterozy-gote for Hb New York and Hb E complicated by an α-thal. Surprisingly, a lowpercentage (3.2%) of a Hb with a mobility similar to that of Hb A was foundby the Sebia CapillryS2 system. The underlying cause for it was not explored.The woman denied having ever received a transfusion. An additional verysmall peak (0.2%) was also shown, which might be a degraded product.
Hb E is the most common Hb variant in Southeast Asia and Hb NewYork is also relatively common in the Chinese population. However, a
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Way
ne S
tate
Uni
vers
ity o
n 11
/26/
14Fo
r pe
rson
al u
se o
nly.

Association of Hb New York With Hb E and α0-Thal 159
FIGURE 2 Partial DNA sequencing of the β-globin gene. The GTG>GAG mutation is at codon 113 andcorresponds to the Val→Glu substitution of Hb New York.
combination of the two variants is not common in our experience. Iden-tification of Hb E is important, because the double heterozygous state forHb E and β-thalassemia is clinically characterized as β-thal major. In HPLC,Hb E migrates with Hb A2. The Sebia CapillryS2 system is capable of dis-tinguishing Hb E from Hb A2 (1). In this case, the Hb A2 percentage wasincreased (4.1%), which might be explained by the β-thalassemic nature ofthe Hb E mutation; the Hb E percentage was lower than that of Hb New Yorkbecause the βE chain was synthesized at a reduced rate due to its creation ofan abnormal splicing within exon 1 of β-globin gene (2).
Although Hb New York is a common β chain variant in our region, a testfor it is not included in the prenatal screening program. The initial screenfor a thalassemia trait in our local practice is the MCV value generated byautomated blood cell counters. Using a cut-off value of MCV<80 fL, prac-tically all the thalassemic individuals can be identified. However, subjectswho are heterozygotes for Hb New York are asymptomatic with normal Hband MCV levels. Most of these individuals would be omitted, and a few areincidentally identified when they coinherit α- or β-thal. In the latter situa-tion, the samples manifested as simple α- or β-thal heterozygotes on HPLCas this variant elutes in the Hb A window in the Bio-Rad Laboratories sys-tem, indeed, the phenotype of the two groups appears to have no significantdifference (3).
The chance of discovering a coexisting α-thal in a β-thal carrier dependson the individual’s ethnic background. This chance is 5.7% in our popula-tion (4). It is well known that routine screening testing, such as MCV andHb A2 levels, cannot distinguish double heterozygotes for α- and β-thal fromthe pure β-thal heterozygotes. In many laboratories, Hb H inclusion bod-ies are used for the detection of α-thal trait. However, this procedure haslimited sensitivity. As in this case, if there is a concomitant β-globin genemutation such as Hb E, the proportion of Hb H inclusion bodies wouldbe reduced, which might confound the diagnosis of the underlying α-thal.Most often, DNA diagnosis is necessary for differentiation. The diagnosis
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Way
ne S
tate
Uni
vers
ity o
n 11
/26/
14Fo
r pe
rson
al u
se o
nly.

160 D.-Z. Li et al.
of this double heterozygous state is important for genetic counseling since,unlike the typical β-thal carriers, these individuals will be at-risk of having off-spring with homozygous α0-thal if they have a partner who is also an α0-thalheterozygote.
Declaration of Interest: The authors report no conflicts of interest. Theauthors alone are responsible for the content and writing of this article.
REFERENCES
1. Higgins TN, Khajuria A, Mack M. Quantification of Hb A2 in patients with and without β-thalassemiaand in the presence of Hb S, Hb C, Hb E, and Hb D Punjab hemoglobin variants: comparison of twosystems. Am J Clin Pathol. 2009;131(3):357–362.
2. Orkin SH, Kazazian HH Jr, Antonarakis SE, Ostrer H, Goff SC, Sexton JP. Abnormal RNA processingdue to the exon mutation of βE-globin gene. Nature. 1982;300(5894):768–769.
3. Lee AC, Ma ES, Chan AY, Szeto SC, Chan LC. Double heterozygosity for Hb New York [β113GTG>GAG; Val→Glu] and β0-thalassemia mutations manifests as a thalassemia trait. PediatrHematol Oncol. 2008; 25(3):227–231.
4. Li D, Liao C, Li J, Xie X, Huang Y, Zhong H. Detection of α-thalassemia in β-thalassemia carriersand prevention of Hb Bart’s hydrops fetalis through prenatal screening. Haematologica. 2006;91(5):649–651.
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Way
ne S
tate
Uni
vers
ity o
n 11
/26/
14Fo
r pe
rson
al u
se o
nly.