Embed Size (px)
Citation preview

Case Report
Autopsy case of amebic granulomatous meningoencephalitiscaused by Balamuthia mandrillaris in Japanpin_2816 418..423
Yoshimi Bando,1 Tetsuyuki Takahashi,2 Hisanori Uehara,2 Teruyoshi Kagegi,3 Shinji Nagahiro3 andKeisuke Izumi2
1Division of Pathology, Tokushima University Hospital, Departments of 2Molecular and Environmental Pathology and3Neurosurgery, Institute of Health Biosciences, The University of Tokushima Graduate School, Tokushima, Japan
Balamuthia mandrillaris is a free-living ameba that causesamebic encephalitis. Herein, we report an autopsy case ofBalamuthia encephalitis proven with polymerase chainreaction (PCR) and immunohistochemistry from paraffin-embedded brain biopsy specimens. A 68-year-old Japanesemale presented at a hospital with progressive right hemi-paresis approximately 3 months before his death. An open-brain biopsy specimen showed diffuse meningitis withmassive coagulative necrosis. The perivascular spacescontained numerous lymphocytes, histiocytes and giantcells, although the etiology was not determined. The patientdeteriorated into coma and died from cerebral herniation.Autopsy revealed abundant trophozoites and cysts in thesubarachnoid and Virchow-Robin’s spaces. Electron-micrographs of the amebic cysts showed a characteristictriple-walled envelope. The amebas were identified as Bala-muthia mandrillaris based on immunohistochemical analy-sis from the autopsy and biopsy specimens. Primer setsdesigned to amplify approximately 200 bp bands of mito-chondrial 16S rRNA gene of Balamuthia by PCR producedpositive results from the biopsy specimens but negativeresults from the autopsy specimens. In summary, PCR toamplify shorter segments of DNA may be of diagnosticvalue in detecting suspected cases of balamuthiasis informalin-fixed, paraffin-embedded specimens. Increasedawareness and timely diagnosis of Balamuthia encephalitismight lead to earlier initiation of therapy and improvedoutcome.
Key words: amebic meningoencephalitis, Balamuthia, poly-merase chain reaction
INTRODUCTION
Balamuthia mandrillaris is a free-living ameba that causesfatal granulomatous amebic encephalitis (GAE) in humansand other animals.1 The incidence of B. mandrillaris-inducedGAE in humans has been increasing in recent years, withmore than 120 cases of Balamuthia encephalitis reportedworldwide,2 although there is only a single case in Japan.3
Because of a lack of pathognomonic symptoms and difficultyin recognizing amebas in biopsy tissues, most cases are notdiagnosed or effectively treated. Even in instances whereantemortem diagnosis is made, the patients are generally inan advanced state of the disease.4,5 Only a few cases haverecovered following antimicrobial treatment,6–9 and recoveryis dependent on how early the disease is diagnosed and drugtherapy is initiated. Thus, it is important to establish rapid andaccurate diagnostic methods.
The definitive diagnosis for Balamuthia encephalitis isbased on the detection of amebic trophozoites and cystswithin brain lesions by light microscopy. Although H&E stain-ing is usually sufficient to detect the amebic structures, theyare often difficult to recognize when brain tissues showmassive necrosis. Polymerase chain reaction (PCR) is auseful diagnostic tool for identifying suspected cases of bala-muthiasis.10,11 Using a primer set to amplify 1075 bp seg-ments of the mitochondrial 16S rRNA gene, Balamuthia DNAhas been identified in formalin-fixed tissues, unfixed tissuesand cerebrospinal fluid (CSF).12 In the present study, wedescribe an autopsy case of Balamuthia-induced menin-goencephalitis diagnosed by PCR analysis using paraffin-embedded specimens. We were unable to detect the1075 bp DNA segments of the mitochondrial 16S rRNA geneof Balamuthia in formalin-fixed, paraffin-embedded braintissue specimens. Thus, we tested our samples with newlydesigned primers to amplify shorter DNA segments ofthe 16S rRNA gene of Balamuthia DNA (approximately200 bp).13 Using this approach we identified B. mandrillaris in
Correspondence: Yoshimi Bando, MD, PhD, Division of Pathology,Tokushima University Hospital, 2-50-1 Kuramoto-cho, Tokushima770-8503, Japan. Email: [email protected]
Received 28 June 2011. Accepted for publication 20 January2012.© 2012 The AuthorsPathology International © 2012 Japanese Society of Pathology andBlackwell Publishing Asia Pty Ltd
Pathology International 2012; 62: 418–423 doi:10.1111/j.1440-1827.2012.02816.x
bs_bs_banner

formalin-fixed, paraffin-embedded specimens as a cause ofGAE in the patient. Although DNA from the autopsy samplesof the present case was not amplified, DNA from the biopsysamples was successfully amplified with these primer pairs.We suspect that formalin-induced cross-linking of DNA mayhave interfered with the PCR reaction.
CLINICAL SUMMARY
The patient was a 68-year-old Japanese male who had nevertraveled outside of Japan. He was a farmer and had nohistory of recent water-sports activities. He had a good healthhistory except for transcatheter arterial embolization (TAE)for hepatitis C virus (HCV)-related hepatocellular carcinoma(HCC) 2 years earlier. He presented at a hospital with paresisof his right leg. Computed tomography (CT) scan of the brainshowed a low-density area in the motor region of the leftfrontal lobe. Right hemiplegia appeared over a month and thelesions spread more widely on CT and magnetic resonanceimaging (MRI) (Fig. 1a–c). He was admitted to hospital andopen-brain biopsy was performed for diagnosis of suspectedbrain tumors. A lumbar puncture yielded clear colorless CSFunder an initial pressure of 9.5 cm H20 with a glucose level of68 mg/dL, total protein level of 34 mg/dL and a cell count of77/3 cells/cm3, the majority of which were lymphocytes. Titersof herpes simplex virus (HSV)-IgG were increased to 1:317 inCSF and 1:29 488 in serum. However, HSV-DNA in CSF wasnegative by PCR. Cultures from serum and CSF were nega-tive for bacteria, fungi and mycobacteria. Disturbance ofspeech appeared and the patient deteriorated into coma. CTscan showed low-density lesions spreading more widely overthe left cerebral hemispheres and cerebral herniation. Thera-peutic treatment with aciclovir, g-globulin and corticosteroids
did not result in a favorable response. The patient diedapproximately 3 months after onset of clinical symptoms.
PATHOLOGICAL FINDINGS
Biopsy findings
The leptomeninges were thick and opaque. A biopsy speci-men from the left frontal lobe lesion showed diffuse menin-gitis with massive coagulative necrosis in the subarachnoidspace and Virchow-Robin’s space. Vasculitis with thrombosisand discrete reactive gliosis were present. The perivascu-lar spaces contained numerous lymphocytes, histiocytes,plasma cells and multinucleated giant cells (Fig. 2a,b). Theinfiltrate and necrosis extended into the adjacent cortex. Nobacterial, fungal, or parasitic elements were identified withspecial stains. Immunohistochemical analysis for HSVI andHSVII was negative. The etiology of the meningoencephalitiswas not determined at the time of biopsy.
Autopsy and histological findings
The brain showed obvious softening and swelling with bilat-eral transtentorial herniation and weighed 1500 g (Fig. 3a).Severe hemorrhage and necrosis were noted in the left cere-bral hemisphere (Fig. 3b). Microscopic examination of thebrain revealed extensive fibrinoid necrosis of medium andsmall arteries, with thrombosis of many vessels and perivas-cular infiltrate composed of neutrophils, lymphocytes, plasmacells and histiocytes. No multinucleated giant cells wereseen. Small necrotic vessels were surrounded and infiltratedby trophozoites and cysts of ameba measuring 15–20 mm in
a b c
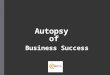
Figure 1 Magnetic resonance imaging (MRI) images of the brain. (a) T1-weighted image showing the low-intensity areas in the motor regionof the left frontal lobe (b) the increased intensity on the T2-weighted image. (c) Coronal T1-weighted image after administration of gadoliniumshowing the heterogeneous enhancing lesion.
Identification of Balamuthia by PCR 419
© 2012 The AuthorsPathology International © 2012 Japanese Society of Pathology and Blackwell Publishing Asia Pty Ltd

diameter (Fig. 3c). The cysts were generally stellate or oval inappearance, with a wrinkled wall. Hemorrhage and necroticlesions with many ameba trophozoites were found in the leftcerebral hemisphere, midbrain, pons and the spinal cord atcervical and thoracic levels.
The liver showed a single small nodule of well-differentiated HCC (1 cm in diameter) and chronic hepatitis.The lungs showed mild bronchopneumonia. Fat necrosisaround the pancreas and a nodule of latent papillary carci-noma of the thyroid were found. There were no detectableamebic trophozoites or cysts in the lung, gastrointestinaltract, liver, or other organs.
Ultrastructural examination of paraffin-embedded braintissue showed triple-walled cysts with a thick inner wall. The
cytoplasmic organelles were compactly arranged. Numer-ous low-density spherical structures were conspicuouslyarranged around electron dense structures (Fig. 3d). Thesefindings exhibited the classical characteristics of the cysts ofBalamuthia.
Immunohistochemistry (IHC) was performed with rabbitantisera made against B. mandrillaris (1:10 000), Acan-thamoeba spp. (1:10 000) and Naegleria fowleri (1:2000)using the ChemMate Envision kit (DakoCytomation,Denmark). Antibodies were supplied by Dr Takuro Endo.Balamuthia antibodies stained the trophozoites and cysts inthe brain tissue autopsy samples. IHC on the biopsy sectionsconfirmed the presence of B. mandrillaris within areas ofcoagulative necrosis (Fig. 2d). Review of the brain biopsy
a
c
b
d
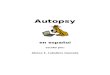
Figure 2 Histological appearance of the open-brain biopsy specimen. (a) Upper part: Subarachnoid space filled by diffuse massiveinflammatory infiltrates; Lower part: Brain parenchyma showing many blood vessels and inflammatory infiltrates. (b) Numerous lymphocytes,histiocytes, plasma cells and multinucleated giant cells infiltrated in the subarachnoid space. (c) A few rounded structures that were interpretedas degenerating amebic forms were seen in the blood vessels walls within areas of coagulative necrosis (arrow). (a–c, H&E) (d) Immunohis-tochemical staining for Balamuthia mandrillaris. Positive staining was seen in the necrotic tissues of the biopsy specimen. Scale bars, 100 mm.
420 Y. Bando et al.
© 2012 The AuthorsPathology International © 2012 Japanese Society of Pathology and Blackwell Publishing Asia Pty Ltd

specimen by H&E stain identified a few rounded structuresthat were interpreted as degenerating amebic forms in theblood vessel walls within areas of coagulative necrosis(Fig. 2c). The results of IHC staining for Acanthamoeba spp.and N. fowleri were negative.
PCR analysis
DNA templates were prepared from formalin-fixed, paraffin-embedded brain tissue using DEXPAT (TaKaRa, Otsu,Shiga, Japan). Initially, B. mandrillaris genus-specific primerswere used for the PCR amplification of the mitochondrial 16SrRNA gene, as previously described.11 Primer sequenceswere: 5′Balspec 16S (5′-CGCATGTATGAAGAAGACCA-3′)and 3′ Balspec 16S (5′-TTACCTATATAATTGTCGATACCA-3′). These primers result in amplification of 1075 bp seg-
ments of DNA. PCR was performed in a volume of 50 mLcontaining 1 ¥ PCR buffer (Applied Biosystems, Carlsbad,CA, USA), 200 mmol/L GeneAmp dNTP mix (Applied Biosys-tems), 3.5 mmol/L MgCl2, 1 mmol/L each primer, 1.25 U Ampli-Taq Gold (Applied Biosystems) and 5 mL DNA template. ThePCR cycling conditions consisted of an initial denaturationstep of 95°C for 5 min, followed by 45 cycles of 95°C for30 s, 52°C for 1 min and 72°C for 1 min, with a final extensionstep of 72°C for 15 min. Amplified DNA was electrophoresedin a 1.8% agarose gel, stained and visualized under UVillumination.
Balamuthia mandrillaris DNA could not be amplified frombiopsy or autopsy tissue samples using the 1075 bp segmentprimer set. Thus, we used the primers designed by Foremanet al.13 to amplify shorter segments of B. mandrillaris andAcanthamoeba spp. The three pairs of B. mandrillarisprimers were: 5′Balspec 16S (5′-CGCATGTATGAAGAAG
a b
c d
Figure 3 (a) Macroscopic appearance of the brain. The brain showed obvious softening and swelling with bilateral transtentorial herniation.(b) Tissue sections revealed severe hemorrhage and necrosis in the left cerebral hemisphere. (c) Histological appearance of the autopsyspecimen. Amoebic trophozoites and cysts were located in the perivascular spaces and invading the blood vessels walls (H&E. Bars, 100 mm).(d) Electron-micrograph of the amoebic triple-walled cysts with numerous low-density spherical structures conspicuously arranged aroundelectron dense structures. Scale bars, 5 mm.
Identification of Balamuthia by PCR 421
© 2012 The AuthorsPathology International © 2012 Japanese Society of Pathology and Blackwell Publishing Asia Pty Ltd

ACCA-3′) and Bal16Sr610 (5′-CCCCTTTTTAACTCTAGTCATATAGT-3′) to amplify 230 bp DNA, Bal16Sf940(5′-TGCACATTTTCGGTTCTAC-3′) and Bal16Sr1170 (5′-GACATACTCCTCATCCTCAAA-3′) to amplify 200 bp DNAand Bal16Sf1150 (5′-TGAGGCGGAGTAAATCTCT-3′) and 3′Balspec 16S (5′-TTACCTATATAATTGTCGATACCA-3′) toamplify 251 bp DNA. The pair of Acanthamoeba castellaniiprimers was: Aca16Sf1160 (5′-AGGAGAAGAAGTCAAATCATTATG-3′) and Aca16Sr1350 (5′-GAGTACAAAGATTGAGAATATATTCA-3′) to amplify 215 bp DNA. Positivecontrol amoebas fixed in 10% formalin/PBS were provided byDr Takuro Endo. Two pairs of Balamuthia-specific primersresulted in successful amplification of Balamuthia DNA fromthe biopsy samples, but not from the autopsy samples(Fig. 4).
DISCUSSION
In the brain, Naegleria causes primary amebic encephalitis(PAM), an acute fulminant illness, whereas Acanthamoebaspp. and B. mandrillaris produce chronic granulomatousamebic meningoencephalitis (GAE).14 To the best of ourknowledge, in Japan there are only a few previouslyreported cases of PAM and GAE,15,16 and only one case ofBalamuthia encephalitis.3 In the present case, the patho-logical features of the biopsy specimens were similar tothose of GAE, although the pathological findings at autopsyshowed extensive hemorrhage and necrotic lesions with noproliferation of multinucleated giant cells. Balamuthia iscapable of infecting both healthy and immunosuppressedhosts.17 In the present case, although autopsy findingsrevealed a small nodule of well-differentiated HCC andHCV-induced chronic hepatitis, the patient was in goodhealth. Thus, the role of liver disease in the development ofthe amebic infection is unclear.
There are a number of potential causes of Balamuthiainfection. Portals of entry of the ameba into the human aresuspected to include breaks in the skin contaminated by soil
with subsequent hematogenous spread, or cysts transportedby air currents to the respiratory tract. In experimentalanimals, the olfactory neuroepithelium has also beenreported as a possible portal of entry.18,19 At autopsy, we didnot find any lesions in the subjects’ nose, eyes, or skin andthe primary site of infection in this patient remains unclear.However, since B. mandrillaris has been found in soil mate-rial,20 the patient may have had contact with polluted soilwhile working.
Balamuthia encephalitis is difficult to diagnose, with themajority of cases diagnosed at postmortem examination. Inthe present case, amebae were not readily apparent onhistological sections of brain biopsy specimens. Furthermore,a thorough examination revealed no identifiable amebic tro-phozoites or cysts using special stains such as the PASreaction. However, immunohistochemical analysis of thebiopsy specimens was positive for Balamuthia. On re-reviewof the biopsy specimens, rare degenerating amebic formsthat had been initially interpreted as histiocytes were retro-spectively identified in the blood vessels walls within areas ofcoagulative necrosis.
Using PCR analysis on formalin-fixed, paraffin-embeddedtissue specimens, we were unable to detect the organismusing the B. mandrillaris genus-specific primers that amplifythe DNA of 1075 bp length.11 However, PCR analysis usingprimers sets to amplify the shorter DNA segments13 fromour biopsy samples resulted in successful amplification ofB. mandrillaris. We were unable to successfully amplify DNAfrom the autopsy samples using any sets of primers, likelydue to the presence of formalin-induced cross-linking of DNAwithin the specimen.
Treatment for amebic encephalitis is problematic and theoptimal antimicrobial therapy has yet to be determined.21
Nevertheless, timely diagnosis of this disease entity mightlead to improved outcome, although it is difficult to make adiagnosis on the basis of the results of routine serologicaland CSF testing. Cultures from clinical samples22 and serumantibody tests23 may help in the diagnosis of Balamuthiainfection. All patients that were previously reported to survive
1 2 3 4 5 6 7 8 9 10 11 12
Figure 4 Polymerase chain reaction (PCR) analysis of formalin-fixed, paraffin-embedded brain tissue showed the presence of BalamuthiaDNA. Lanes 1–3, Balamuthia positive control; Lane 4, Acanthamoeba spp. positive control; Lanes 5–8, DNA from the brain biopsy specimens;Lanes 9–12, DNA from the brain autopsy specimens. Primers: Lanes 1, 5 and 9 with 5′Balspec 16S and Bal16Sr610 to amplify 230 bp DNA;Lanes 2, 6 and 10 with Bal16Sf940 and Bal16Sr1170 to amplify 200 bp DNA; Lanes 3, 7 and 11 with Bal16Sf1150 and 3′ Balspec16S to amplify251 bp DNA; Lanes 4, 8 and 12 with Aca16Sf1160 and Aca16Sr1350 to amplify 251 bp DNA.
422 Y. Bando et al.
© 2012 The AuthorsPathology International © 2012 Japanese Society of Pathology and Blackwell Publishing Asia Pty Ltd

from Balamuthia encephalitis underwent brain biopsy. Thesepatients were diagnosed before death and antimicrobialtherapy was initiated early enough to halt the course of thedisease.6–9 As Balamuthia is virtually indistinguishable fromAcanthamoeba, further differentiation via indirect immunof-luorescence staining using rabbit anti-Balamuthia serum andultrastructural studies is typically required. PCR usingBalamuthia-specific primers to amplify the mitochondrial 16SrRNA gene is also a useful diagnostic tool.
In summary, our data suggest that PCR assays usingprimers to amplify DNA segments of approximately 200 bp inlength may be more suitable for detection of B. mandrillaris informalin-fixed, paraffin-embedded specimens. With greaterawareness that amoebas can cause encephalitis, earlierdiagnosis can be made by immunohistochemistry and PCRanalysis, as well as by recognizing the amebas in histologicalsections of biopsy brain tissue.
ACKNOWLEDGMENTS
We thank Dr Govinda S. Visvesvara (Centers for DiseaseControl and Prevention, Division of Parasitic Diseases,Atlanta, Georgia, USA) for the immunofluorescence test, DrTakuro Endo (Department of Parasitology, National Instituteof Infectious Disease, Tokyo, Japan) for supplying antibodies,Ms Kaoru Saegusa for pathological examination andMs Akiko Akagi for her excellent technical work onelectron-micrographs.
REFERENCES
1 Visvesvara GS, Schuster FL, Martinez AJ. Balamuthia mandril-laris, N. G., N. Sp., agent of amebic meningoencephalitis inhumans and other animals. J Eukaryot Microbiol 1993; 40:504–14.
2 Matin A, Siddiqui R, Jayasekera S, Khan NA. Increasing impor-tance of Balamuthia mandrillaris. Clin Microbiol Rev 2008; 21:435–48.
3 Shirabe T, Monobe Y, Visvesvara GS. An autopsy case ofamebic meningoencephalitis. The first Japanese case causedby Balamuthia mandrillaris. Neuropathology 2002; 22: 213–17.
4 Galarza M, Cuccia V, Sosa FP, Monges JA. Pediatric granulo-matous cerebral amebiasis: A delayed diagnosis. Pediatr Neurol2002; 26: 153–6.
5 Bakardjiev A, Azimi PH, Ashouri N et al. Amebic encephalitiscaused by Balamuthia mandrillaris: Report of four cases.Pediatr Infect Dis J 2003; 22: 447–53.
6 Deetz TR, Sawyer MH, Billman G, Schuster FL, Visvesvara GS.Successful treatment of Balamuthia amoebic encephalitis: Pre-sentation of 2 cases. Clin Infect Dis 2003; 37: 1304–12.
7 Jung S, Schelper RL, Visvesvara GS, Chang HT. Balamuthiamandrillaris meningoencephalitis in an immunocompetentpatient: An unusual clinical course and a favorable outcome.Arch Pathol Lab Med 2004; 128: 466–8.
8 Cary LC, Maul E, Potter C et al. Balamuthia mandrillaris men-ingoencephalitis: Survival of a pediatric patient. Pediatrics 2010;125: e699–703.
9 Martinez DY, Sease C, Bravo F et al. Successful treatment ofBalamuthia mandrillaris amoebic infection with extensive neu-rological and cutaneous involvement. Clin Infect Dis 2010; 51:e7–11.
10 Booton GC, Carmichael JR, Visvesvara GS, Byers TJ, FuerstPA. Genotyping of Balamuthia mandrillaris based on nuclear18S and mitochondrial 16S rRNA genes. Am J Trop Med Hyg2003; 68: 65–9.
11 Booton GC, Carmichael JR, Visvesvara GS, Byers TJ, FuerstPA. Identification of Balamuthia mandrillaris by PCR assaysusing the mitochondrial 16S rRNA gene as a target. J ClinMicrobiol 2003; 41: 453–5.
12 Yagi S, Booton GC, Visvesvara GS, Schuster FL. Detection ofBalamuthia mitochondrial 16S rRNA gene DNA in clinical speci-mens by PCR. J Clin Microbiol 2005; 43: 3192–7.
13 Foreman O, Sykes J, Ball L, Yang N, De Cock H. Disseminatedinfection with Balamuthia mandrillaris in a dog. Vet Pathol 2004;41: 506–10.
14 Martinez AJ, Visvesvara GS. Free-living, amphizoic and oppor-tunistic amebas. Brain Pathol 1997; 7: 583–98.
15 Nakamura T, Kobayashi M, Wada H, Tsunoda Y, Akai K, OmataK. An autopsy case of primary amoebic meningoencephalitis.Adv. Neurol Sci 1979; 23: 500–9. (in Japanese with Englishabstract).
16 Sugita Y, Fujii T, Hayashi I et al. Primary amebic meningoen-cephalitis due to Naegleria fowleri: An autopsy case in Japan.Pathol Int 1999; 49: 468–70.
17 Schuster FL, Visvesvara GS. Free-living amoebae as opportu-nistic and non-opportunistic pathogens of humans and animals.Int J Parasitol 2004; 34: 1001–27.
18 Janitschke K, Martinez AJ, Visvesvara GS, Schuster F. Animalmodel Balamuthia mandrillaris CNS infection: Contrast andcomparison in immunodeficient and immunocompetent mice: Amurine model of ‘granulomatous’ amebic encephalitis. J Neuro-pathol Exp Neurol 1996; 55: 815–21.
19 Kiderlen AF, Laube U. Balamuthia mandrillaris, an opportunisticagent of granulomatous amebic encephalitis, infects the brainvia the olfactory nerve pathway. Parasitol Res 2004; 94: 49–52.
20 Dunnebacke TH, Schuster FL, Yagi S, Booton GC. Balamuthiamandrillaris from soil samples. Microbiology 2004; 150: 2837–42.
21 Schuster FL, Visvesvara GS. Opportunistic amoebae: Chal-lenges in prophylaxis and treatment. Drug Resist Updat 2004; 7:41–51.
22 Jayasekera S, Sissons J, Tucker J et al. Post-mortem culture ofBalamuthia mandrillaris from the brain and cerebrospinal fluid ofa case of granulomatous amoebic meningoencephalitis, usinghuman brain microvascular endothelial cells. J Med Microbiol2004; 53: 1007–12.
23 Schuster FL, Yagi S, Wilkins PP, Gavali S, Visvesvara GS,Glaser CA. Balamuthia mandrillaris, agent of amebic encepha-litis: Detection of serum antibodies and antigenic similarity ofisolates by enzyme immunoassay. J Eukaryot Microbiol 2008;55: 313–20.
Identification of Balamuthia by PCR 423
© 2012 The AuthorsPathology International © 2012 Japanese Society of Pathology and Blackwell Publishing Asia Pty Ltd