Embed Size (px)
Citation preview
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 1/17
Nafeez Zawahir, MD
CME Clinical Director, Medscape, LLC
Disclosure: Nafeez Zawahir, MD, has disclosed no relevant financial relationships.
From Medscape Education Cardiology
Sudden Cardiac Death From A to Z: Focus on Primary
Prevention CMEMichael R. Gold, MD, PhD; Michael J. Mirro, MD; Jeanne E. Poole, MD
CME Released: 11/09/2012; Valid for credit through 11/09/2013
Slide 1.
Michael R. Gold, MD: I am Michael Gold, and I am the chief of Cardiology at the Medical University of South
Carolina and a cardiac electrophysiologist.
Today, I am joined by 2 esteemed colleagues and experts in the field of cardiac arrhythmia who will be discussing
the prevention of sudden cardiac death (SCD): Dr Jeanne Poole from the University of Washington and Dr.
Michael Mirro from the Parkview Health System in Fort Wayne, Indiana.
What we are going to be talking about is the problem of sudden cardiac death. Sudden cardiac death is one of the
leading causes of death in the United States. It has been estimated that up to 1 person per minute dies due to
SCD. As such, this is possibly the largest cause of mortality in the United States and in other Western societies.
We have learned much about identifying patients at risk for SCD, and we have also learned about therapies that
can prevent this problem. Many of these deaths are due to underlying heart failure and coronary artery disease, so
any therapies that help prevent these problems are effective for preventing SCD.
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 2/17
Slide 2.
Therefore, reducing cholesterol, controlling hypertension, and treating heart failure are all effective approaches.
However, in the groups of patients with the highest risk, these approaches are insufficient, and antiarrhythmic
drugs have not been found to be helpful. Accordingly, we have moved towards the implantable cardioverter-defibrillator (ICD), which is very effective for certain subgroups of patients. [1] Despite this being a class I
recommendation and multiple randomized studies showing that the ICD can reduce mortality, and sudden death,
in groups of patients at high risk for SCD, we have been disappointed by the penetration of this therapy in the
community.[2]
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 3/17
Slide 3.
There are a number of issues that are probably contributing to this lower penetration than expected or than is seen
with other drug therapies for SCD. These include confusion as to which groups would benefit most from
preventative medical therapy or ICD therapy, for instance, patients following a myocardial infarction (MI) vs those
patients with diabetic cardiomyopathy; the level of heart failure that patients may have; and concomitant medicaltherapies.
What has further confounded many has been the disconnect between what the guidelines tell us, what clinical
studies have told us, and what Centers for Medicare and Medicaid Services (CMS) coverage is for ICD therapy
payment. This has been further accentuated by investigations by the Department of Justice and other
investigations into billing for the use of many cardiac devices. Unfortunately in some situations, this has led to the
underuse of ICDs when their use is appropriate.
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 4/17
Slide 4.
What we would like to discuss is which patients are at high risk, which patients should receive an ICD; when is the
right time to give an ICD; and then, finally, what would be the appropriate bridging strategies for patients, if they
have not been optimally treated, or if they are in a time period in which an ICD is not yet indicated, because they
have had a recent revascularization or an MI.
Jeanne E. Poole, MD: Welcome to this program, “Sudden Cardiac Death From A to Z: A Focus on Primary
Prevention.” I am Jeanne Poole from the University of Washington in Seattle, Washington, and it is my pleasure to
moderate this session on this important topic, a topic I might add that while being of the utmost concern to health
care providers working in the cardiovascular arena, is also a source of confusion at times with respect to the CMS
guidelines.
We hope to clarify some of these gray areas over the next 15 to 20 minutes. Assisting me in this task is Michael
Mirro from Fort Wayne, Indiana.
Welcome, Mike.
Michael J. Mirro, MD: Jeanne, thank you for the introduction. I am an electrophysiologist in Parkview Health
System in Fort Wayne, Indiana, and I run the Clinical Research Center at that institution, and SCD has been a
particular area of interest for me and the institution for a number of years.
Dr Poole: Can you give us a precise definition of what we mean when we use the term sudden cardiac death?
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 5/17
Slide 5.
Dr Mirro: What we are referring to is the onset of cardiac arrest outside of the hospital. Typically most of these are
witnessed but many are unwitnessed arrests, and the patients have virtually no symptoms prior to the onset of
their hemodynamic collapse, and the arrest is arrhythmic in origin. That is the definition that we use pertaining to
the guidelines and primary prevention. The incidence of SCD is estimated as between 250,000 to 350, 000;however, it is difficult to know precisely based on the fact that reporting is geographically diverse from state to
state.[2,3]
Dr Poole: It remains one of the most important public health problems that we face in the United States.
Dr Mirro: In patients who do not survive the cardiac arrest, the most frequent finding at autopsy is advanced
coronary disease, which, many times was undiagnosed.
Dr Poole: Tragic. When you think about the kinds of patients that are most l ikely to be victims of SCD, what risk
factors place these patients at risk for an arrhythmic event?
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 6/17
Slide 6.
Dr Mirro: The primary risk factor is heart failure. The clinical presence of significant left ventricular systolic
dysfunction is a very important factor, which is now the basis of our guidelines. The ejection fraction determination
has become one of the biggest predictors of SCD in the highest-risk population.
The presence of nonsustained ventricular tachycardia (nsVT) is a predictor. Of course, the presence of more
advanced sustained ventricular tachycardia (sVT), defined as 30 seconds or more of ventricular tachycardia, is
also a predictor. There are other factors that contribute to the risk, and it has been a challenge since the ejection
fraction, as we all know, has quite a bit of variability based on imaging studies: who is performing the study, how it
is interpreted, and whether the patients are on medical therapy. Other technologies have been evaluated, but no
other risk stratification tests have emerged that clearly identifies a subset of patients who are at risk for SCD. [2]
Dr Poole: Ejection fraction and a clinical history of heart failure, particularly moderate heart failure, were the risk
stratifiers that patients had to meet for enrollment into the major clinical trials. I think we can state, unequivocally,
that the randomized clinical trials that evaluated ICD therapy for primary prevention of SCD have established this
therapy modality as lifesaving. It certainly begs the question, why not just place an ICD in all of the patients who
are at similar risk?
Dr Mirro: Yes, that is a great question. Many of these patients have complex illnesses with comorbidities and
many patients have a life expectancy of less than a year. We would not want those patients to receive ICDs. We
also know there is a lot of variation in ejection fraction determination.
If you look at the overall SCD population,, the vast majority of people who suffered a sudden death, as pointed out
in Bob Myerburg's excellent review articles, had preserved ejection fractions. [3,4] It is a public health challenge as to
how we are going to identify these people. The ICD implant guidelines are based on these clinical trials and are
focused on the highest risk patients.[1] Also, CMS coverage decision requires, as you know, a 90-day waiting
period for nonischemic patients.[5]
Dr Poole: You bring up an interesting issue. There has been confusion about guidelines regarding appropriate
patients for implantation of an ICD vs what CMS states in their coverage decisions for reimbursement -- they are
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 7/17
not always in sync with each other. Can you comment about the differences between the guidelines and CMS
reimbursement?
Slide 7.
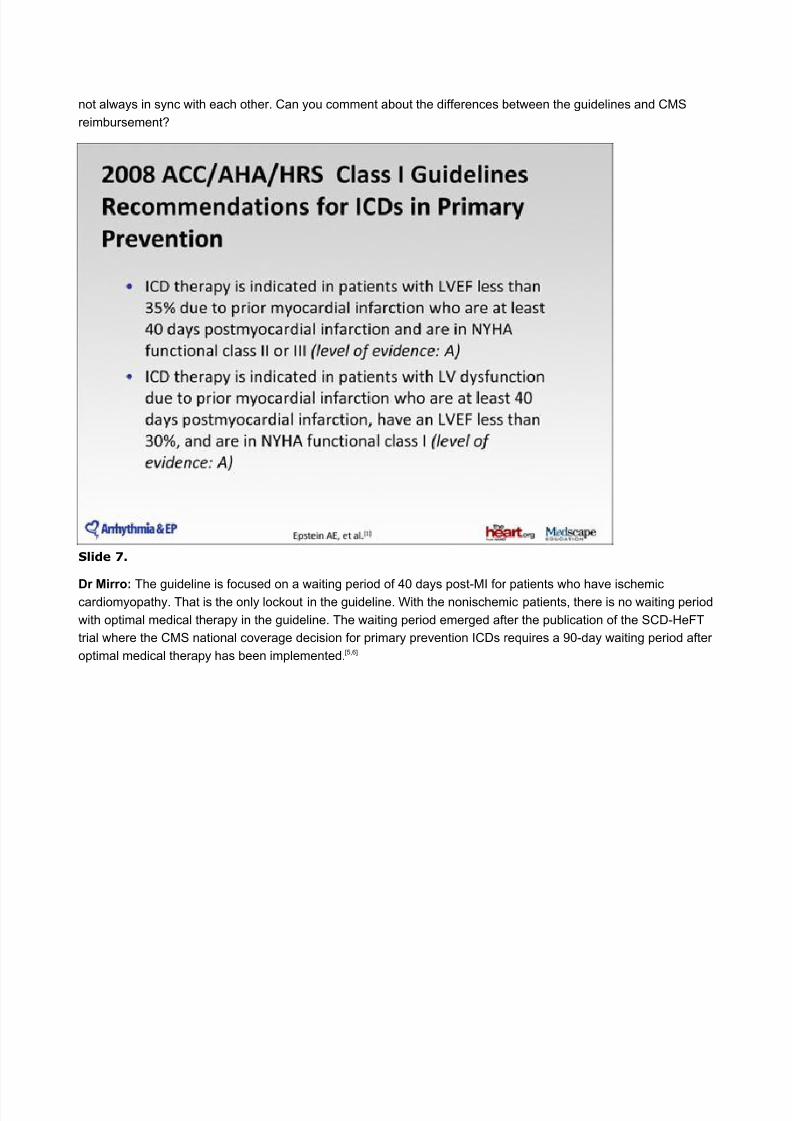
Dr Mirro: The guideline is focused on a waiting period of 40 days post-MI for patients who have ischemiccardiomyopathy. That is the only lockout in the guideline. With the nonischemic patients, there is no waiting period
with optimal medical therapy in the guideline. The waiting period emerged after the publication of the SCD-HeFT
trial where the CMS national coverage decision for primary prevention ICDs requires a 90-day waiting period after
optimal medical therapy has been implemented. [5,6]
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 8/17
Slide 8.
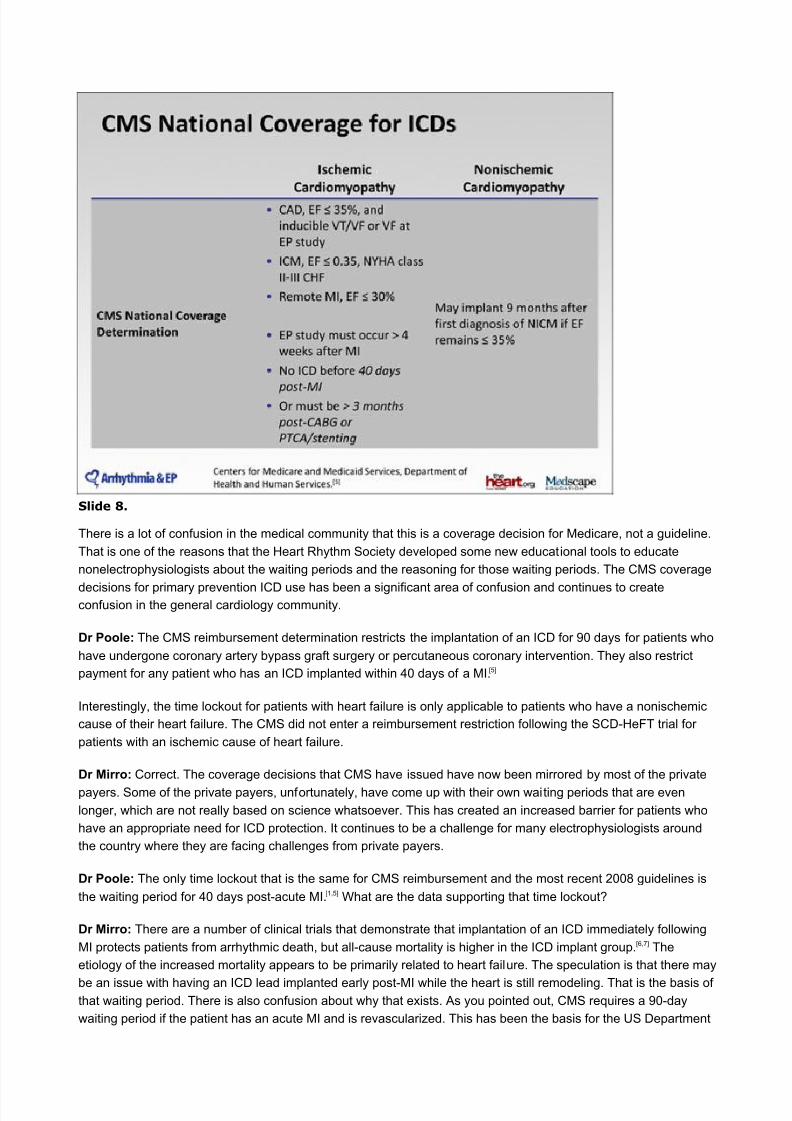
There is a lot of confusion in the medical community that this is a coverage decision for Medicare, not a guideline.
That is one of the reasons that the Heart Rhythm Society developed some new educational tools to educate
nonelectrophysiologists about the waiting periods and the reasoning for those waiting periods. The CMS coverage
decisions for primary prevention ICD use has been a significant area of confusion and continues to createconfusion in the general cardiology community.
Dr Poole: The CMS reimbursement determination restricts the implantation of an ICD for 90 days for patients who
have undergone coronary artery bypass graft surgery or percutaneous coronary intervention. They also restrict
payment for any patient who has an ICD implanted within 40 days of a MI.[5]
Interestingly, the time lockout for patients with heart failure is only applicable to patients who have a nonischemic
cause of their heart failure. The CMS did not enter a reimbursement restriction following the SCD-HeFT trial for
patients with an ischemic cause of heart failure.
Dr Mirro: Correct. The coverage decisions that CMS have issued have now been mirrored by most of the private
payers. Some of the private payers, unfortunately, have come up with their own waiting periods that are even
longer, which are not really based on science whatsoever. This has created an increased barrier for patients who
have an appropriate need for ICD protection. It continues to be a challenge for many electrophysiologists around
the country where they are facing challenges from private payers.
Dr Poole: The only time lockout that is the same for CMS reimbursement and the most recent 2008 guidelines is
the waiting period for 40 days post-acute MI.[1,5] What are the data supporting that time lockout?
Dr Mirro: There are a number of clinical trials that demonstrate that implantation of an ICD immediately following
MI protects patients from arrhythmic death, but all-cause mortality is higher in the ICD implant group. [6,7] The
etiology of the increased mortality appears to be primarily related to heart failure. The speculation is that there may
be an issue with having an ICD lead implanted early post-MI while the heart is still remodeling. That is the basis ofthat waiting period. There is also confusion about why that exists. As you pointed out, CMS requires a 90-day
waiting period if the patient has an acute MI and is revascularized. This has been the basis for the US Department
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 9/17
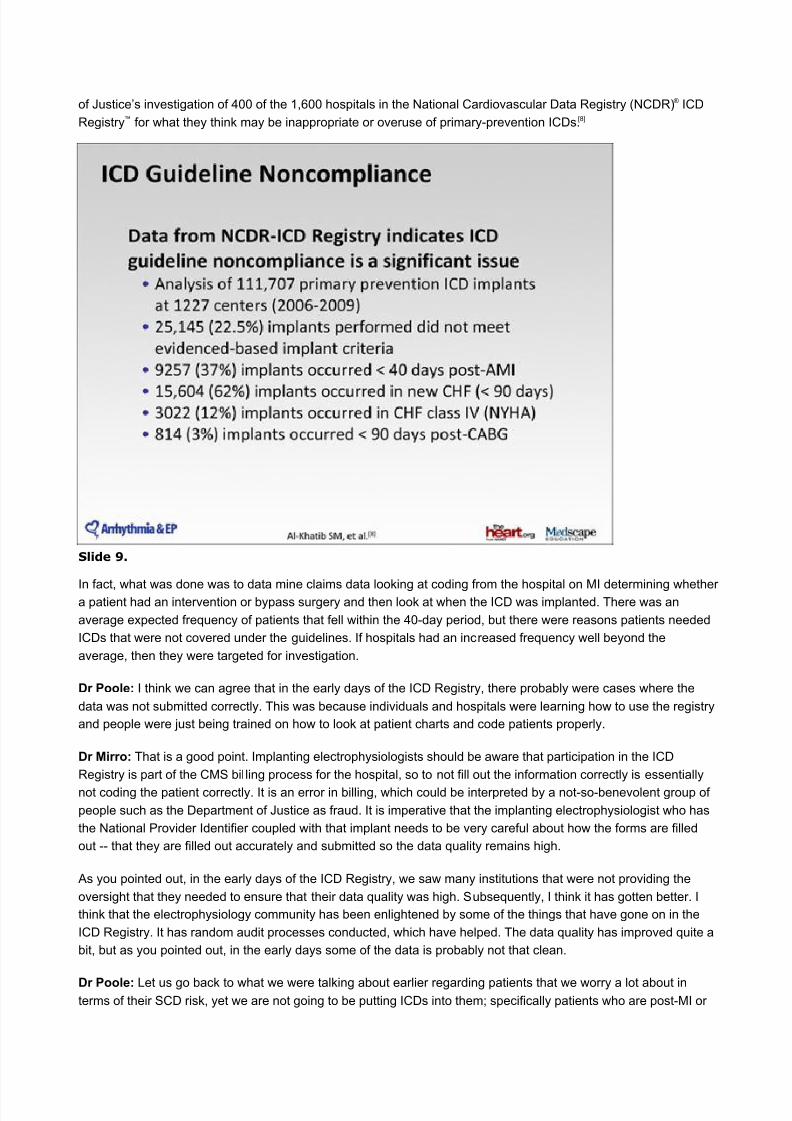
of Justice’s investigation of 400 of the 1,600 hospitals in the National Cardiovascular Data Registry (NCDR) ® ICD
Registry™ for what they think may be inappropriate or overuse of primary-prevention ICDs.[8]
Slide 9.
In fact, what was done was to data mine claims data looking at coding from the hospital on MI determining whethera patient had an intervention or bypass surgery and then look at when the ICD was implanted. There was an
average expected frequency of patients that fell within the 40-day period, but there were reasons patients needed
ICDs that were not covered under the guidelines. If hospitals had an increased frequency well beyond the
average, then they were targeted for investigation.
Dr Poole: I think we can agree that in the early days of the ICD Registry, there probably were cases where the
data was not submitted correctly. This was because individuals and hospitals were learning how to use the registry
and people were just being trained on how to look at patient charts and code patients properly.
Dr Mirro: That is a good point. Implanting electrophysiologists should be aware that participation in the ICD
Registry is part of the CMS bil ling process for the hospital, so to not fill out the information correctly is essentially
not coding the patient correctly. It is an error in billing, which could be interpreted by a not-so-benevolent group of
people such as the Department of Justice as fraud. It is imperative that the implanting electrophysiologist who has
the National Provider Identifier coupled with that implant needs to be very careful about how the forms are filled
out -- that they are filled out accurately and submitted so the data quality remains high.
As you pointed out, in the early days of the ICD Registry, we saw many institutions that were not providing the
oversight that they needed to ensure that their data quality was high. Subsequently, I think it has gotten better. I
think that the electrophysiology community has been enlightened by some of the things that have gone on in the
ICD Registry. It has random audit processes conducted, which have helped. The data quality has improved quite a
bit, but as you pointed out, in the early days some of the data is probably not that clean.
Dr Poole: Let us go back to what we were talking about earlier regarding patients that we worry a lot about interms of their SCD risk, yet we are not going to be putting ICDs into them; specifically patients who are post-MI or
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 10/17
have had recent revascularization. What alternative methods might we consider to take care of these patients
during these waiting periods?
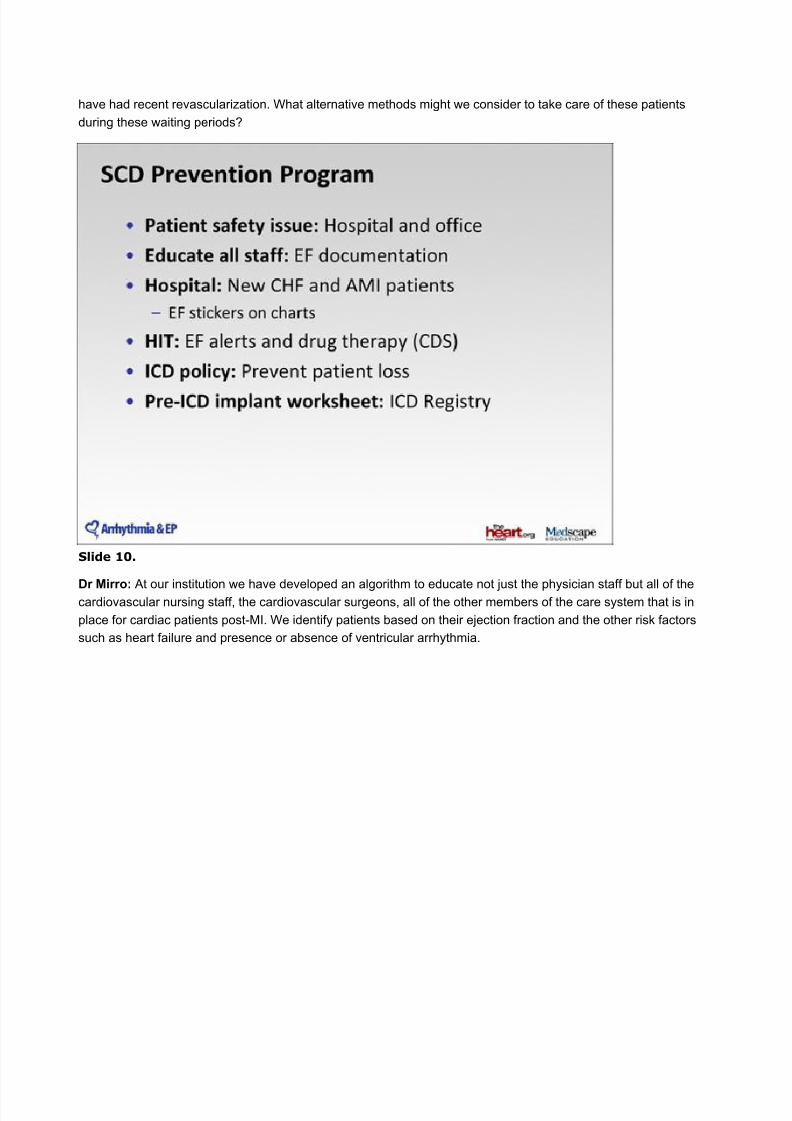
Slide 10.
Dr Mirro: At our institution we have developed an algorithm to educate not just the physician staff but all of thecardiovascular nursing staff, the cardiovascular surgeons, all of the other members of the care system that is in
place for cardiac patients post-MI. We identify patients based on their ejection fraction and the other risk factors
such as heart failure and presence or absence of ventricular arrhythmia.
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 11/17
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 12/17
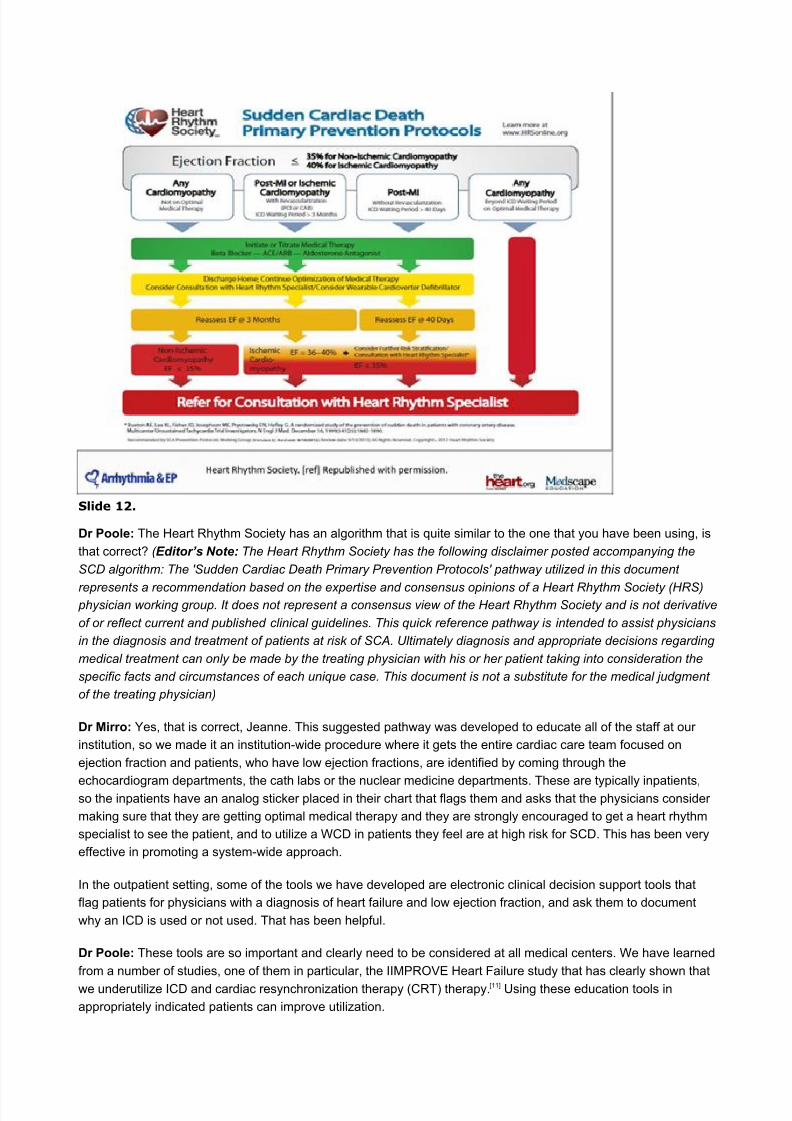
Slide 12.
Dr Poole: The Heart Rhythm Society has an algorithm that is quite similar to the one that you have been using, is
that correct? ( Editor’s Note: The Heart Rhythm Society has the following disclaimer posted accompanying the
SCD algorithm: The 'Sudden Cardiac Death Primary Prevention Protocols' pathway utilized in this document
represents a recommendation based on the expertise and consensus opinions of a Heart Rhythm Society (HRS) physician working group. It does not represent a consensus view of the Heart Rhythm Society and is not derivative
of or reflect current and published clinical guidelines. This quick reference pathway is intended to assist physicians
in the diagnosis and treatment of patients at risk of SCA. Ultimately diagnosis and appropriate decisions regarding
medical treatment can only be made by the treating physician with his or her patient taking into consideration the
specific facts and circumstances of each unique case. This document is not a substitute for the medical judgment
of the treating physician)
Dr Mirro: Yes, that is correct, Jeanne. This suggested pathway was developed to educate all of the staff at our
institution, so we made it an institution-wide procedure where it gets the entire cardiac care team focused on
ejection fraction and patients, who have low ejection fractions, are identified by coming through the
echocardiogram departments, the cath labs or the nuclear medicine departments. These are typically inpatients,so the inpatients have an analog sticker placed in their chart that flags them and asks that the physicians consider
making sure that they are getting optimal medical therapy and they are strongly encouraged to get a heart rhythm
specialist to see the patient, and to utilize a WCD in patients they feel are at high risk for SCD. This has been very
effective in promoting a system-wide approach.
In the outpatient setting, some of the tools we have developed are electronic clinical decision support tools that
flag patients for physicians with a diagnosis of heart failure and low ejection fraction, and ask them to document
why an ICD is used or not used. That has been helpful.
Dr Poole: These tools are so important and clearly need to be considered at all medical centers. We have learned
from a number of studies, one of them in particular, the IIMPROVE Heart Failure study that has clearly shown that
we underutilize ICD and cardiac resynchronization therapy (CRT) therapy. [11] Using these education tools in
appropriately indicated patients can improve utilization.
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 13/17
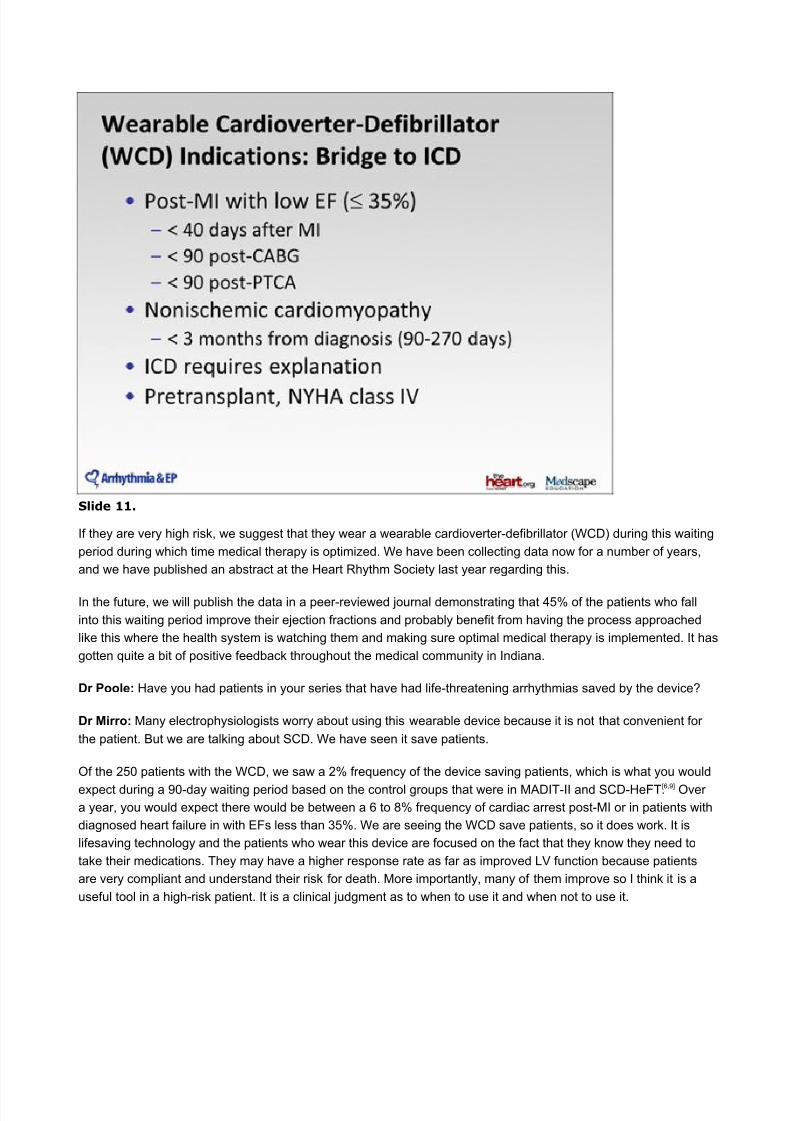
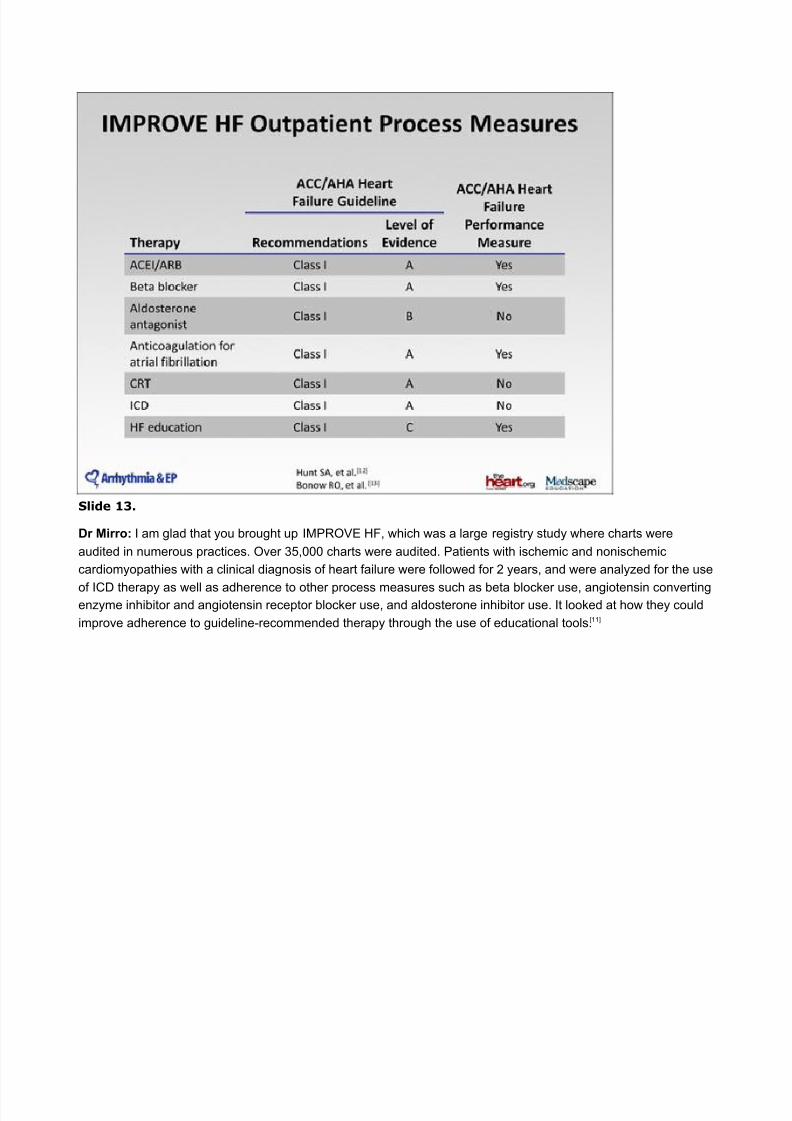
Slide 13.
Dr Mirro: I am glad that you brought up IMPROVE HF, which was a large registry study where charts were
audited in numerous practices. Over 35,000 charts were audited. Patients with ischemic and nonischemic
cardiomyopathies with a clinical diagnosis of heart failure were followed for 2 years, and were analyzed for the use
of ICD therapy as well as adherence to other process measures such as beta blocker use, angiotensin convertingenzyme inhibitor and angiotensin receptor blocker use, and aldosterone inhibitor use. It looked at how they could
improve adherence to guideline-recommended therapy through the use of educational tools.[11]
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 14/17
Slide 14.
The investigators rolled out these tools to these practices and demonstrated that at the beginning of the audit the
use of primary-prevention ICDs was extremely poor, in the range of 40% to 45% on average. It did improve over
time. Over a 2-year period, it improved to about 65%, which, unfortunately, is still a significant underpenetration of
the appropriate use of primary-prevention therapy in these patients.
There is still room for significant improvement, and the use of educational tools such as those the Heart Rhythm
Society has been rolling out has been very helpful to continue to educate the general cardiology community on the
guidelines but also the differences between the guidelines and the CMS coverage decision.
Dr Poole: All of these efforts are critical and hopefully can be embraced by a broader community. We need to do
this in order to continue to address the public health problem of SCD and capture appropriate patients for ICD
therapy. I want to thank you for your time today. Mike, do you have any final pearls of wisdom that we should keep
in mind?
Dr Mirro: It is important that electrophysiologists take a lead at their institutions in developing a system-wide
approach to SCD prevention at the local and grassroots level. Having an energized cardiovascular nursing staff
like the one at our institution is incredibly helpful in screening patients and taking ownership of the patients with
low ejection fractions, in order to ensure that these patients receive proper care. It is key that the
electrophysiologists continue to take a leadership role in this area. It is the best thing for our patients, and it is the
best thing for the medical community.
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 15/17
Slide 15.
Dr Poole: Thank you so much, Mike, for your insights on how to better manage ICD therapy for patients, and
thank you for listening in to this activity. I hope that you found it informative. You may now take the CME posttest
by clicking on the “Earn CME Credit” link. Please also take a moment to complete the program evaluation that
follows. Thank you.
This transcript has been edited for style and clarity.
This article is a CME certified activity. To earn credit for this activity visit:
http://www.medscape.org/viewarticle/771023
Abbreviations
ACC = American College of Cardiology
ACEI = angiotensin converting enzyme inhibitor
AHA = American Heart Association
AMI = acute myocardial infarction ARB = angiotensin receptor blocker
CABG = coronary artery bypass graft
CAD = coronary artery disease
CDS = clinical decision support
CHF = coronary heart failure
CMS = Centers for Medicare and Medicaid Services
CRT = cardiac resynchronization therapy
EF = ejection fraction
EP = electrophysiology
HIT = health information technology
HRS = Heart Rhythm SocietyICD = implantable cardioverter-defibrillator
ICM = ischemic dilated cardiomyopathy
LDL = low-density lipoprotein
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 16/17
LV = left ventricular
LVEF = left ventricular ejection fraction
MADIT-II = Multicenter Autonomic Defibrillator Implantation Trial 2
MI = myocardial infarction
NCDR = National Cardiovascular Data Registry
NICM = nonischemic dilated cardiomyopathynsVT = nonsustained ventricular tachycardia
NYHA = New York Heart Association
PTCA = percutaneous transluminal coronary angioplasty
SCD = sudden cardiac death
SCD-HeFT = Sudden Cardiac Death in Heart Failure Trial
sVT = sustained ventricular tachycardia
VF = ventricular fibrillation
VT = ventricular tachycardia
WCD = wearable cardioverter-defibrillator
References
1. Epstein AE, DiMarco JP, Ellenbogen KA, et al; Writing Committee Members; ACC/AHA Task Force
Members. ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities:
executive summary. Circulation. 2008;117:e350-408. Abstract
2. Fishman GI, Chugh SS, Dimarco JP, et al Sudden cardiac death prediction and prevention: report from a
National Heart, Lung, and Blood Institute and Heart Rhythm Society Workshop Circulation.
2010;122;2335-2348.
3. Myerburg RJ, Junttila MJ. Sudden cardiac death caused by coronary heart disease. Circulation.
2012;125:1043-1052. Abstract
4. Myerburg RJ, Hendel RC. Expanding risk-profiling strategies for prediction and prevention of suddencardiac death. J Am Coll Cardiol. 2010;56:215-217. Abstract
5. Centers for Medicare and Medicaid Services, Department of Health and Human Services. CMS Manual
System, Pub. 100-03 Medicare National Coverage Determinations.
http://www.cms.gov/transmittals/downloads/R29NCD.pdf. Published March 4, 2005. Accessed October 9,
2012.
6. Bardy GH, Lee KL, Mark DB, et al; for the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT)
Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J
Med. 2005;352:225 –-237.
7. Hohnloser SH, Kuck KH, Dorian P, et al; DINAMIT Investigators. Prophylactic use of an implantable
cardioverter-defibrillator after acute myocardial infarction. N Engl J Med. 2004;351:2481-2488. Abstract
8. Al-Khatib SM, Hellkamp A, Curtis J, et al. Non-evidence-based ICD implantations in the United States.JAMA. 2011;305:43-49. Abstract
9. Moss AJ, Zareba W, Hall WJ, et al; Multicenter Automatic Defibrillator Implantation Trial II Investigators.
Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection
fraction. N Engl J Med. 2002;346:877-883. Abstract
10. Heart Rhythm Society. SCD Primary Prevention Protocols. http://www.hrsonline.org/News/Sudden-
Cardiac-Arrest-SCA-Awareness/SCA-Provider-Resources/Primary-Prevention-Protocols. Published 2012.
Accessed October 9, 2012.
11. Fonarow GC, Albert NM, Curtis AB, et al. Improving evidence-based care for heart failure in outpatient
cardiology practices: primary results of the Registry to Improve the Use of Evidence-Based Heart Failure
Therapies in the Outpatient Setting (IMPROVE HF). Circulation. 2010;122:585-596. Abstract
12. Hunt SA, Abraham WT, Chin MH; American College of Cardiology; American Heart Association TaskForce on Practice Guidelines; American College of Chest Physicians; International Society for Heart and
Lung Transplantation; Heart Rhythm Society. ACC/AHA 2005 Guideline Update for the Diagnosis and
8/16/2019 Basi Neurobiologiche Delle Competenze Emotive
http://slidepdf.com/reader/full/basi-neurobiologiche-delle-competenze-emotive 17/17
Management of Chronic Heart Failure in the Adult: a report of the American College of
Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update
the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with
the American College of Chest Physicians and the International Society for Heart and Lung
Transplantation: endorsed by the Heart Rhythm Society. Circulation. 2005;112:e154-235. Abstract
13. Bonow RO, Bennett S, Casey DE Jr, et al; American College of Cardiology; American Heart AssociationTask Force on Performance Measures (Writing Committee to Develop Heart Failure Clinical Performance
Measures); Heart Failure Society of America. ACC/AHA clinical performance measures for adults with
chronic heart failure: a report of the American College of Cardiology/American Heart Association Task
Force on Performance Measures (Writing Committee to Develop Heart Failure Clinical Performance
Measures) endorsed by the Heart Failure Society of America. J Am Coll Cardiol. 2005;46:1144-1178.
Abstract
14. Medtronic, Inc. IMPROVE HF. http://www.improvehf.com/. Accessed October 15, 2012.
Disclaimer
The material presented here does not necessarily reflect the views of Medscape, LLC, or companies that support
educational programming on medscape.org. These materials may discuss therapeutic products that have not beenapproved by the US Food and Drug Administration and off-label uses of approved products. A qualified healthcareprofessional should be consulted before using any therapeutic product discussed. Readers should verify allinformation and data before treating patients or employing any therapies described in this educational activity.
Medscape Education © 2012 Medscape, LLC





























