8/8/2019 Brachial Plexus Neuropathy
1/3
Australas Radio1 1 9 9 1 : 3%379-381
MRI Scanning in Brachial Plexus NeuropathyV E m Y AHERN,M.B.,
B.S.
Registrar, Department of Radiation OncologyY.S. SOO, M.B.
B.S.(HK),D.M.R.D.(Eng),M.A.R.C.R.
StafSSpecialist,DepartmentofRadiologyALLAN D. LANGLANDS, B.Sc.,
F.R.A.C.R., F.R.C.S.(Ed.)
Director, Departmentof Radiation OncologyWestmead Hospital,
Westmead,NSW, Australia
INTRODUCTIONBrachial plexus neuropathy (BPN) occurring
afterradiotherapy for breast carcinoma is uncommon.Distinction
between radiation-induced neuropathy andtumour infiltration of the
plexus is frequently difficult onclinical grounds,
electrodiagnosticstudies or computerised
tomography (CT)canning.We report the use of magnetic resonance
imaging(MRI) to diagnose BPN due to tumour infiltration in apatient
with breast carcinoma.CASE REPORT
In June 1986, a 39 year old woman developed a 3.5cmcarcinoma of
the right breast. There were no lymph nodespalpable nor evidence of
metastatic disease. The patientwas treated by total mastectomy and
axillary clearance.The primary tumour was an infiltrating duct
carcinoma.None of 40 lymph nodes dissected were involved. No
fur-ther treatment was advised. Five months later, a 5 x 3cmmass of
lymph nodes in the right supraclavicular fossa(SCF) was proven by
incision biopsy to be involved withmetastatic breast carcinoma.
There was no clinical evi-dence of disease at other sites. Routine
blood tests, CXRandCT scan of the thorax were normal.
On 21/11/86 the patient commenced chemotherapyconsisting of 3
cycles of novantrone (N) and cyclophos-phamide (C), followed by
6Mev radiotherapy to the rightSCF and internal mammary chain by a
direct anteriorfield. A dose of 50Gy at a depth of 3cm was given in
25fractions over 38 days. Six cycles of cyclophosphamide(C),
methotrexate (M), 5 fluorouracil (F),and prednisone(P) were then
given.By the commencement of CMFP, there was completeremission of
disease.In December 1988, the patient complained of pain inthe
right shoulder and left parastemal area. No abnormali-ty was
detected on physical examination, bone scan, orCT scan of the
thorax.On 10/2/89, she presented with a 3 day history of
pro-gressive swelling of the right arm. There was a fullness ofthe
right SCF but no discrete mass. No metastatic diseasewas clinically
evident. Venography demonstrated throm-bosis of the right
subclavian vein, and the patient was
treated with intravenous heparin, andwarfarin. No under-lying
cause for the thrombosis was demonstrated on a CTOne month later
the patient complained of increasingpain around the right shoulder.
Matted lymph nodes overan area of 5 x 5cm were palpable in the
right SCF.
Multiple lung metastases were seen on chest X-ray.
CMFchemotherapy at intervals of three weeks, was recom-menced on
23/3/89. After a total of 6 cycles ofchemotherapy, the right SCF
mass wa s still palpable andmeasured4 3cm, but the patient no
longerrequiredanal-gesia to control her pain. A chest X-ray
demonstrated sig-nificant reduction in the size of the pulmonary
metastases.Within 2 months, the patient returned with severesharp
pain in the right arm adiating to the right hand, andsubjective
weakness of the fingers of the right hand.On examination, the right
SCF mass had not changedin size or consistency, and there were no
neurologicalabnormalities of the upper limbs. An MRI scan of
thelower cervical and upper thoracic region clearly demon-strated
metastatic disease in the right SCF infiltrating intothe right
brachial plexus region laterally and inferiorly
into the extrapleural space of the right upper lateral
chest(Fig. la,b).She was last seen on 12/2/90, with right arm pain
con-trolled by oralmorphine, and increasing difficulty in hold-ing
objects in the right hand.
scan.
DISCUSSIONRadiation fibrosis affecting the brachial plexus
follow-ing therapy for breast carcinoma can be difficult to
distin-guish from tumour infiltration of the plexus.Kori et a1
(1981) (9) in an analysis of 1(Kfpatients withBPN, defined clinical
criteria for distinguishing the twoentities. Early severe pain,
hand weakness, whole plexusinvolvement and Homers syndrome
suggested malignantBPN. These criteria were not supported in
studies by
Thomas and Colby (1972) or Bagley et a1(1978). (12,2).Radiation
fibrosis is usually assumed to be the cause ifa biopsy of the SCF
is negative for malignancy, the= is noevidence of metastases, and
the patient survives for a pro-tracted period (5).
A d d m for correspondence:Dr. .AhemDepartment of Radiation
OncologyWestmeadHospitalWestmead, NSW 2145 AustraliaSubmitted
forpublication on:6th April, 1990Resubmittedfor publicationon:
14thJanuary, 1 9 9 fAccepted forpublicationon:14thJ u e , 1991
AustralasianRadioIogy, Vol.35, o. ,November.1991 379
8/8/2019 Brachial Plexus Neuropathy
2/3
VERITY AHERN el a/
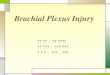
FIGURE I A -Coronal TI weighted image shows an isointense
lobulated ma ss (arrows) in the right brachial plexus region,
indenting on the apical extrapleural space .These cr i te r ia wi l
l not be fu lf i l led f or a l l pa t ients.Negative biopsies were
reported by Cascino et a1 ( 1 983)(4) in 2 patients who underwent
surgical explorations ofthe brachia l p lexus but repea t b iops
ies d i rec ted a t CTabnormalities in the brachial plexus were
positive.Lederman and Wilbourn (1984) (10) found tha t t
heelectrodiagnostic findings of fasciculation and the occur-rence
of myokymia (involuntary muscle movement in anundulating, wavelike
manner) ( 1 ) in radiation-inducedBPN, together with certain
clinical features, were suffi-ciently diagnostic to allow an
accurate differentiation ofthe tw o entities in a majority of
patients.Recently CT scanning of the brachial plexus has
beenclaimed to be the investigation of choice in distinguishing
the causes of BPN, particularly when thin C T cuts andbolus
intravenous enhancement are used (3). With tumourrecurrence, the CT
scan should demonstrate a soft tissuemass rather than a hazing of
the margins of axillary ves-sels or increased density of the
subcutaneous and axillaryfat; (5,3).Prior surgery or radiotherapy
to the affected SCF willalter the CT scan appearances of the SC F
region, m akinginterpretation based on these criteria difficult.A
further limitation of CT scanning interpretation of
(1983): 5 patients with histologically proven metastaticAuwo luc
i un Kudio /o , iy W i / .3.5. N o . 4 . N o w r n h f r . 1 Y Y
I
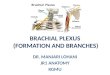
FIGURE IB - The mass shows increased signals in T2 weighted th e
SCF in was recognised by Cascino ersequence, indicative
ofmetastatic disease (a rrows).380
8/8/2019 Brachial Plexus Neuropathy
3/3
MRI SCANNING IN BRACHIAL PLEXUS NEUROPATHY
plexopathy had normal CT scans. This may have beenbecause CT
scans will not identify perineural infiltrationof the plexus by
tumour.The use of MRI in distinguishing radiation inducedBPN from
recurrent tumour in breast cancer has been
reported on only 3 previous occasions (7,8,11).Axial and
sagittal views are considered complemen-tary in defining the extent
and volume of a tissue mass inthe region of the brachial plexus (1
1). On T1 weightedimages, tumour is generally of higher signal
intensity thanradiation fibrosis. The higher intensity of tumour
com-pared to radiation fibrosis is more pronounced on T2images. In
the case reported by Rapoport et a1 1988, themass in the brachial
plexus area was of inhomogeneoussignal intensity on T2 images -
anteriorly the mass wa s ofhigh signal intensity, and posteriorly,
low. Biopsy of theanterior portion was positive for metastatic
breast carcino-ma; the posterior lower intensity portion was
consideredto be radiation fibrosis.We conclude that the physical
symptoms and signs,
and clinical course of radiation induced BPN, may beidentical to
those of disease recurrence. Surgical explo-ration,
electrodiagnostic tests, and CT scanning of theSCF will not always
be helpful in distinguishing the twoentities. MRI scanning may
ultimately prove to be theinvestigation of choice. The distinction
between BPN dueto radiation or malignant infiltration is not
academic, astreatment options exist for breast cancer (the
commonestcause of brachial plexus involvement by tumour).
1.2.
3.4.5.
6.7.
8.
9.10.11.12.
REFERENCESAlbers JW, Allen AA , Bastron JA. Daube JR. Limb
myokymia.Muscle and Nerve 1981; 4: 494-504.Bagley FH , Walsh JW.
Cady B, Salzman FA, Oberfield RA,Pazianos AG. Carcinomatous versus
radiation-induced brachialplexus neumpathy in breast cancer. Cancer
1978; 41: 2154-2157.Ban C, Kissin MW. Radiation-induced brachial
plexus nevOpamyfollowing breast conservation and radical
radiotherapy. Br J Surg1987; 7 4 855-856.Cascino TL, Kori S , Kml
G. Foley KM. CT of thc brachial pkxmin patients with cancer.
Neurology 1983; 33: 1553-1557.Cmke J, Cooke D, Parsofis C. ?he
anatomy a d uaU101mf thebrachial plexus asdemonsrratcdby computed
tomc&aphy.v-ClinicalRadiology 1988; 39: 595.601.Cooke J, Powell
S, ParsonsC. The diagnosis by computed tomogra-phy of brachial
olexus lesions followine radiotheraov for carcinomaof-& breast.
ciinical ~ a d i ~ i ~ ~988;39:ma-.-Glazer HS, Lee JKT, Levitt RG,
Heiken J Ling D,TMtyWG. BalfeDM, Emani B, Wasserman TH,Murphy WA.
Radiation fibrosis:differentiation from m m n t umour by MR maging.
Radiology1985; 156: 721-726.KneelandJB.Kellman GM, MiddletonWD,
ates D, JcmanowiczA, Fm i s zW, Hyde JS. Diagnosis of diease of the
supzlclavicularregion by use ofMR maging. AJR 148: 1549-1551.Kori
SM, Foley KIM, Posner JB. Brachial plexus ksiws n patientswith
cancer: OOcases. Neurology 1981; 31: 45-50.Merman RJ,Wilboum AJ.
Brachial plexopathy: Remmnt canceror radiation? Neurology
1984.34.1331-1335.Rapoport S, Blair DN, McCarthy SM, Desser TS.
Hammers LW,Sostman HD. Branchial plexus - conelation of MR maging
withCT and pathologic findings. Radiology 1988; 167: 161-165.Thomas
EE, Colby MY. Radiation-induced or metastatic brachialplexopathy? A
diagnostic dilemma. JAMA 1972; 222: 1392-1395.
Australasian Radiology. Val.35,No. 4. November,1991 381