Embed Size (px)
Citation preview
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
CARBOHYDRATE CHEMISTRY:-
Formula:- Cn (H2O)n Glucose and mannose are epimers at C2 carbon
Glucose galactose epimers at C4
Enantimomers are mirror images to each other.
α and β cyclic forms of D-glucose known as anomers
C1 is anomeric carbon
Benedict test reducing properties of sugars
Sodium amalgam is used as reducing agent.
Reduction of mono saccharides gives alcohols.
Aldose reductase converts aldehydes to alcohols.
Fructose is converted to sorbitol dehydrogenase (liver)
Monosaccharides gives needle shaped osazones.
Maltose gives sunflower shaped osazones
Lactose gives powderpuff shaped osazones
Maltose (α1-4) (glucose + glucose) – maltose (hydrolysed)
Lactose (βgalactose – βglucose) (β1-4) – lactase (hydrolysed)
Sucrose (glucose-fructose) (α1- β2)
Glucosidic bond- bond between monosaccharides.
Sucrose is hydrolysed by sucrase/invertase
Dextrins are breakdown product of starch
Inulin is a polymer of fructose
Glycogen and starch are polymer of glucose
Inulin is need to assess GFR
Dietary fiber is cellulose (β-glycoside bond)
D-glucoronic acid + N-acetyl glucosamine – Hyaluronic acid
Keratin sulphate keeps cornea transparent
LIPID CHEMISTRY:-
Saturated fatty acids does not contain double bond
Unsaturated fatty acids has double bonds
Linolecic, linolenic and arachidonic acid (PUFA)
Deficiency of EFA – phyrnoderma (toad skin)
Arachidonic acid gives Eicasonoids
Unsaturated fatty acids exists in Cis form
Hydrolysis of triacyl glycerin with alkali produces soaps (saponification)
Vit.E is naturally occuring antioxidant, superoxide dismutase, urase
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
Purity of fatty acid is checked by iodine number
RM number (Reichert-Meissl) – to check purity of butter
Phospholipids – free fatty acids + alcohol + phosphate + nitrogen Base
Lecithin – choline ( nitrogen base) - ( lung surfactant)
Hormones like oxytocin and vasopressin action is mediated by phosphatidyl inositol
Sphinogophospholipid :- cerebonic acid + sphingosine + phosphate + choline =
sphingomyelin.
Phospholipases – A1, A2, C, D
PLA2 (phospholipase A2)– give arachidonic acid
Ganglioside GM2 accmulates in taysachs disease
Cholesterol –C27 H46 O
Cholesterol has ohg group at C3. Double bond between C5-C6
Ergosterol is precussor for vit.D
Zaks test is used to identify the qualitative analysis of cholesterol
Emulsified fats in the intestine forms Micelles
PROTEINS AND AMINO ACID CHEMISTRY:-
kjeldahi’s method is used to find out protein in biological fluids.
the amino acid glycine has H as side chain
alanine has –CH3 (methyl) as side chain.
Cysteine and methionine are sulphur containing aminoacid.
Aspartic acid and glutamic acid are acidic aminoacid
Phenyl alanine, tyrosine, tryptophan –aromatic aminoacid
Alanine is glucogenic aminoacid.
Leucine and lysine – ketogenic aminoacid.
Monosodium glutamate intolerance causes chinese restaurant syndrome
D-penicilamine- used as chelating agent in Wilson’s disease (Accmulation of copper in
brain)
N-acetyl cysteine used in cystic fibrosis and chronic renal failure.
GABA-pentane is used as anticonvulsant
Linear sequence of aminoacid seen in primary structure
α helix and β sheath – secondary structure.3 diminsional arrangement of protein –teritary
2 or more poly peptide chains- quartenary structure
Peptide bond – bond between 2 aminoacid.
Sangers reagent – used to determine aminoacid sequence
Sangers reagent used to determin insulin structure
Biurate is a compound formed by heating urea to 180 degrees . process is biurate reaction
Copper sulphate is used for heatin in biurate reaction
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
Glutathione is involved in transport of amino acfid in intestine and kidney via glutanyl
cycle/meister cycle.
Aspertame – artifical sweetner.
NUCLEIC ACIDS AND NUCLEOTIDES:-
Nucleotides – nitrogen base + pentose sugar + phosphate
Nucleoside – nitrogen base + sugar
Ribose and deoxyribose differs in C2
Purine nucleotide is Adenosin mono phosphate
Pyramide nucleotide is Cyitidine MonoPhosphate, UradineMonoPhosphate
Alopurinol used in the treatment of gout
5- fluorouracil used in the treatment of cancers
Azathioprine is used to suppress immunological rejection during transplantation
The width of double helix of DNA – 20 Å / 2 nm
Each turn of helix contains 10 base pairs
Each turn of helix is 34 Å
2 strands of double helixd are hold by H-bonds
DNA protiens are known as histones
B-DNA proposed by watson and crick in 1953
A-DNA has 11 base pairs per turn.
A and B- DNA are right handed helix
Z-DNA is left handed helix
Z-DNA has 12 base pairs per turn (zigzag)
Formamide destahilses H-bonds, therefore it lowers Tm
Formamide used in recombinant DNA technology
The sugar in RNA kis ribose
RNA is subjected to alkali hydrolysis and DNA cannot
RNA can be identified lby orcinol colour reaction because of ribose
Nucleolus synthesis r-RNA
DNA converts M-RNA converts protein
M-RNA has 7 methyl guicnosine at 5 prime end
The 3 prime kend contains poly- A tail (MRNA)
The stucture of t-RNA resembles clover leaf
the acceptor arm of t-RNA has CCA cap (3prime)
D-arm has dihyrouridine (t-RNA)
TψC arm has T, pseudouridine and C (tRNA)
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
ENZYMES :-
There are 6 cclasses of enzymes
The functional unit of enzyme is holoenzyme
Holoenzyme is made up of apoenzyme (protein part) and co-enzyme (non-protein part).
Increase in concentration of substrate increase enzyme velocity
Km = ½ Vmax
Km = S (substrate concentration) Km-(michaelis-menten constant)
Km is defined as the substrate concentration to produce ½ maximum velocity.
Low Km denotes strong affinity between enzyme and substrate
When enzymes are exposed to C and above temperatures denaturation occurs.
All enzymes are active at neutral PH (7)
The most common aminoacid at active site is serine
INHIBITORS:-
Xanthine oxidase – allopurinol
MAO (mono amino oxidase) – ephedrine, auphetamine
Dihydrofolate reducatse – aminopterin, amethopterin, methotrexate
Acetylcholine esterase – succinyl choline
Dihydropteroate synthase – sulfanilamide
Vit. Kepoxide reductase – dicumorol
HMG co-A reducatse – lorastatin, compactin.
Disulfiran is the drug used in the treatment of alcoholism
Transketolase requires TPP
Streptokinase is used to remove blood clots
Streptokinase converts plasminogen to plasmin
Asperginase is used in treatment of leukemias
Increase amylase – acute pancreatitis
Increase SGPT (serum glutamate pyruvate transaminase) – liver diseases
Increase alkaline phosphatase – rickets and bone diseases
Increase acid phosphatase – prostate carcinoma
Increase aldolase – muscle dystrophy
Increase troponin I – MI (first marker)
Increase CPK1 – BB (brain)
Increase CPK2 – MB (heart)
Increase CPK3 – MM (skeletal muscle)
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
LIPID METABOLISM:-
TG – plasma concentration is 75-150 mg/dl
Cholesterol – plasma concentration is 150-200 mg/dl
Hypercholesteremia - >250mg/dl
Hormone sensitive TG lipase removes fatty acid from C1 or C3 of TAG
glucagon, epinephrine, thyroxine, ACTH – increase cAMP – increase lipolysis.
Insulin – decrease cAMP – decrease lipolysis
Glycerol is metabolized by liver.
FFA from Adipose Tissue are transported to liver by albumin.
Brain, erythrocytes cannot utilize FA
FA activation – cytosol (ATP, Co-A, mg2+) requires 2 ATP
Long chain FA are metabolized in peroxisomes
Tangair’s disease – plasma HDL particles are almost absent
Biosynthesis of FA in liver starts with glycerol and in adipose tissue with glucose and
acetyl Co-A
Glycolipids act as receptors in cell membrane
Absorption of cholesterol from intestine is by diffusion
Cholesterol gives bile salts, vit.D, steroid hormones (sex hormone and corticoids)
Prostaglandin exhibit platelet aggregation, increase cAMP and vasodilation
Obesity gene – leptin
β-oxidation – mitochondria
activation of FA in β-oxidation – cytosol
melanoyl Co-A inhibits – CAT-I, thus inhibits β-oxidation
CAT-I – outer mitochondrial membrane
CAT-II – inner mitochondrial membrane
Medium chain aceyl Co-A dehydrogenase, rate limiting step of β-oxidation.
β-oxidation of palmitate gives 106 ATP
SIDS (sudden infant dead syndrome) – deficiency of medium chain aceyl Co-A
dehydrogenase (M-CAD.)
Methyl melanoic academia – vit.B12 deficiency
Methyl melanoic Co-A – requires Vit. B12
Zellweger syndrome – absence of peroxisomes cerebrohepatorenal syndrome.
Zellweger syndrome – defect in long chain fatty breakdown
α-oxidation – Refsums disease – accumulation of phytanic acid.
ω-oxidation requires – cytochrome P450 , NADPH, O2.
Ketone bodies are synthesized in liver
Ketone bodies are utilized by brain in prolonged starvation
HMG – CoA synthase – rate limiting step in ketone bodies synthesis
Ketone bodies cannot be utilized by liver because of deficiency of thiophorase
Acetone exhaled by lungs – sweetish odur.
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
Detection of ketone bodies in urine – rothers test
Glucagon stimulates ketone bodies synthesis, insulin inhibits
Treatment of keto acidosis – insulin
Fatty acid bio-synthesis – cytosol.
Acetyl Co-A for fatty acid biosynthesis (FAB) obtains from citrate lyase
NADPH in FAB obtained form HMP- pathway and malic enzyme
Acetyl Co-A carboxylase – rate limiting step in FAB
Insulin stimulates FAB –glucagon inhibits
Un-saturated fatty acids synthesized by fatty aceyl Co-A desaturase. Human lacks this
enzyme.
TAG synthesis – adipose tissue
Cerebronic acid + phyngosine = seramide
Seramide + phosphate + choline = sphingomyelin
Phospholipase A1 – cleaves FFA at C1
Phospholipase A2 – cleavesFFA at C2
Phospholipase C - cleaves phosphate and glycerol found in lysozomes of hepatocytes
L-CAT found in lungs
L-CAT activity is associated with apo-A1 of HDL
Sphingomyelinase deficiency niemann’s pick’s desease
Deficiency of seramidase Fauber’s disease
Deficiency of β-galactidase krabbe’s disease
Deficiency of β-glucosidase gauchers disease
Deficiency of α-galactidase fabrys disease
Deficiency of hexosaminidase A – Taysachs disease
Cholesterol biosynthesis, liver- 50%, intestine- 15%
Cholesterol synthesis- cytosol.
HMG- CoA reductase – rate limiting step in cholesterol biosynthesis
Cholesterol formulae :- C27 H46 O
Glucagon – glucocorticoids – decrease cholesterol biosynthesis
Compactin, lorastatin inhibits – HMG Co-A reductase
HMG-CoA reductase also inhibited by bileacids
7-α-hydroxylase – rate limiting step in bileacid biosynthesis
95% of the bile is reabsorbed and return back to liver
Primary bileacids – cholic acid chenodeoxycholic acid.
Conjuation of bile acids done by – glycine , taurine
Deoxycholic acid,lithocholic acid – secondary bile acids
Chenodiol treat for cholilithiasisctiatn of chylomi
Chylomicrons has B48
VLDL has B100
HDL has apoprotein-A
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
Activation of chylomicrons and VLDL requires Apo-CII and Apo-E from HDL
Lipoprotein lipase deficiency – hyperlipoprotenimia type I
Defect in LDL receptors – type IIA
Excess apoB – type IIB
Abnormality in apo-E – type III
Over production of TG – type IV
Defect in HDL receptors – tangier’s disease
OXIDATIVE PHOSPHORYLATION AND ETC:-
Phosphophenol pyruvate is 14.8 cal/mole.
S-adenosyl methionane is 10 cal/mole
cAMP is 12 cal/mole
ATP is 7.3 cal/mole
The inner mitochondrial membrane is impermeable to H+, K+ and Na+
Co-enzyme Q is also known as ubiquione
Complex-I – NADH-co-encyme Q reductase inhibited by – amytal, rotenone,
pricydine-A
Complex III – Co-enzyme Q-cytC reductase inhibited by antimycin A,
BAL (british anti lewisite)
Comple IV – cytochrome oxidase inhibited by cyanide, CO, Na-azide.
otation of -subunit is 12
ATP synthatase has F0 and F1 subunits.
F0 – channel protein C
F1 – central γ subunit, 3α, 3β
Mutation of mitochondrial DNA – oxiphos disease AKA (lebers hereditary optic
neuropathy)
2, A dinitrophenol – uncoupler of oxiphosphorylation
Digomycin inhibits oxidative phosphorylation by binding to ATP synthetase 2 blockes
proton channels
Atractyloside inhibits oxidative phosphorylation by blocking the adequate supply of
ADP.
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
VITAMINS:-
Vit.A:-
Retinol is present in animals in the form of retinylester
Retinal,retinol and retinoic acid are vitamers of vitamin A
β- carotene gives l2 moles of retinal by 1 ’-1 ’ di-oxygenase
retinyl esters are transported by chylomicrons and stored in liver
retinol is transported in circulation by RBP 9retinal binding protein)
rods – dim light vision
cones – bright light
vit-A required for rods
rhodopsin present in rods
rhodopsin = 11-cis retinal + opsin
during walds visual cycle rhodipsin is bleached to metarhodopsin-II which increases C-
GMP an degenerates nerve impulse
Vit-A deficiency night blindness
Serene deficiency of vit-A causes xerophthalmia, characterized of dryness of conjunctiva
and cornea, white triangular plaques, bitot’s spots are seen
Xerophthalmia leads to keratomalacia causing total blindness
Vit. D
Ergosterol (plants) ergocalciferol – vit. D2
Cholecalciferol (animals)- vit.D3
Vit-D synthesis takes place in skin.
1,25- Di-hydroxycholecalciferal is known as calcitriol i.e., active form of vit-D
25- α -hydroxylase and 1-α-hydroxylase requires cyt-p-450, NADPH and O2
Vit.D is essential for bone formation
Vit-D deficiency:- pickets – bowlegs – children; osteomalacia – Adults.
Alkaline phosphatase activity elevated in rickets
Vit-D is more toxic in over doses
Vit-D is transported in the circulation by α2-globulin
1-α-hydroxylase present in kidney and stimulated by PTH
25- α –hydroxylase present in liver
Vit-E:-
Anti sterility vitamin
Also known as tocopherols α,β,γ,δ out of these α-tocopherols more active
Vit-E is transported by VLDL and LDL in the circulation
Normal plasma levels of tocopherols <1mg/dl
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
Vit-E naturally occurring antioxidant and it requires selenium
Vit-E prevents peroxidation reactions of PUFA
ALA-synthase requires vit.E
Vit-K:-
Vit-K also synthesized by intestinal bacteria
Bile salts are essential for absorption of vit- K
Transported to liver by means of LDL
Vit-K is responsible for post transitional modification of 2,7,9,10 clotting factors by
carboxylation of glutamic acid
Carboxylation of glutamic acid is inhibited by dicumarol
Deficiency of vit-K leads to lack of acive prothrobin in circulation
High doses of vit-K causes hemolytic anemia
Vit-C :-
Vit-C is required for collagen formation
Vit-C is co-enzyme for hydroxylation of proline and lysine, where protocollagen is
converted to collagen
Deficiency of vit-C leads to scurvy, delayed wound healing
Vit-B1 :-
co-enzyme – TPP
TPP required for PDH transketolase
Deficiency seen in the people who consume polished rice as a staple food
Elevation of pyruvate in plasma and excrets in urine
Wet-beriberi – edema – systolic increase – diastolic decrease – bouncing pulse.
Dry-beriberi – no edema – neurological manifestations are seen
Decrease transketoplase activity – Wernick’s korsakoff syndrome
Thyamine deficiency more commonly seen in alcoholics.
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
B2 – RIBOFLAVIN:-
Coenzymes – FMN, FAD
Used in oxidation reduction reactions
Deficiency – cheilosis, glosittis, dermatitis
Assessment of glutathione reductase in erythrocytes will be useful in
accessing riboflavin deficiency
NIACIN:-
Coenzyme – NAD, NADP
Pellagra preventive factor
Niacin coenzymes synthesized from tryptophan
Niacin deficiency results pellagra
Pellagra symptoms – diarrhea, dementia, dermatitis – death “HD”
Niacin inhibits lipolysis
Niacin is used in treatment of hyperlipoprotenuria type_IIB. (increased
VLDL, increased LDL)
PYRIDOXINE:- B6
Coenzyme – pyridoxine, pyridoxal pyridoxamine
Pyridoxine used in transamination, decarboxylation, deamination.
Active form is pyridoxal phosphate (PLP) transamination
It is required for the production of the monoamine neurotransmitters
serotonin, dopamine, norepinephrine and epinephrine, as it is the precursor
to pyridoxal phosphate: cofactor for the enzyme aromatic amino acid
decarboxylase. This enzyme is responsible for converting the precursors 5-
hydroxytryptophan (5-HTP) into serotonin and levodopa (L-DOPA) into
dopamine, noradrenaline and adrenaline. As such it has been implicated in
the treatment of depression and anxiety.
DEFICIENCY MANIFESTATIONS:-
1. neurological symptoms
2. excretion of xanthurenic acid in urine
3. drugs isoniazid and penicillamine can cause B6 deficiency.
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
BIOTIN – B7
It is required for carboxylation reactions
Eg.:- 1. acetyl CoA carboxylase
2. propony CoA carboxylase
3. pyruvate carboxylase
PANTOTHENIC ACID:-
also known as coenzyme –A
deficiency – burning feet syndrome
FOLIC ACID:-
it is important for one carbon metabolism
the active form if tetrahydrofloate TH4 or THF
the most common vitamin deficiency
important for the synthesis of nitrogenous bases in DNA and RNA.
Supplemented in pregnancy to prevent neural tube defects
Deficiency of folic acid megaloblastic anemia.
In folic acid deficiency FIGLU excreted in urine.
(FIGLU- formiminoglutamate)
VITAMIN –B12 (COBALAMIN)
The absorption of vit-B12 requires intrinsic factor, intrinsic factor
produced by gastric parietal cells
Absorption of B12 into mucosal cells is Ca+2 dependent
In mucosal cells B12 converts to methyl B12
From the mucosal cells transported in the plasma by transcobalamins
i.e., Tc-I and Tc-II
Methyl –B12 (mucosal cells) – 90% binds to Tc-I and 10% binds to
Tc-II
Vit-B12 stores in liver, as deoxyadenosyl
B12 (storage form of vit B12)
DEFICIENCY:-
Methyl melanoic acidemia
Pernicious anemia
Neurological manifestations (optic neuropathy)
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
Use schilling test to detect deficiency
Vit-B12 deficiency - most common cause is malabsorption sprue .
HAEMOGLOBIN AND PORPHYRINS:-
METABOLISM:-
Heme contains porphyrin molecule known as protoporphyrin IX
Heme contains 4 pyrole rings
The central atom of heme contains Fe
The adult hemoglobin – α2,β2 – HbA1
Fetal hemoglobin – α2 γ2 – HbF
HbA2 – α2 δ2
Glycosylated hemoglobin – Hb A1 C – α2 β2 –glucose (diabetes)
Fetal Hb has more affinity towards O2 than adult – HbF – 100% ;
HbA1 – 95%.
In heme if Fe2+ oxidizes to form Fe3+ known methehemoglobin
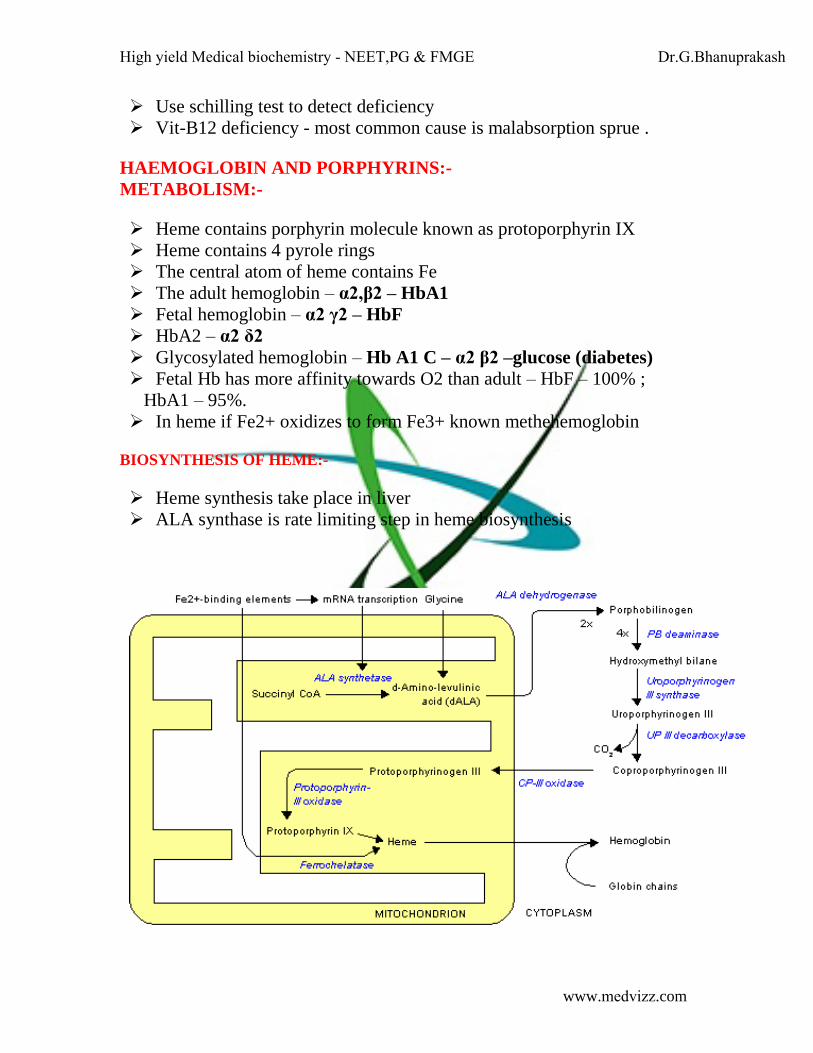
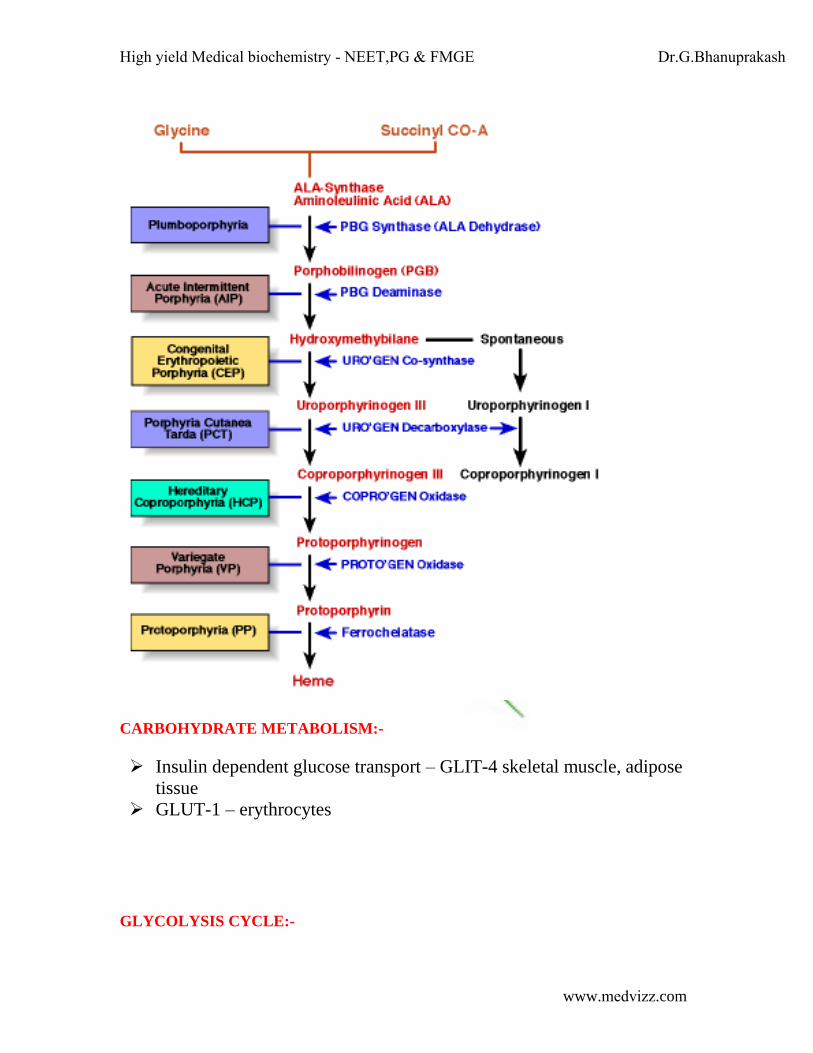
BIOSYNTHESIS OF HEME:-
Heme synthesis take place in liver
ALA synthase is rate limiting step in heme biosynthesis
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
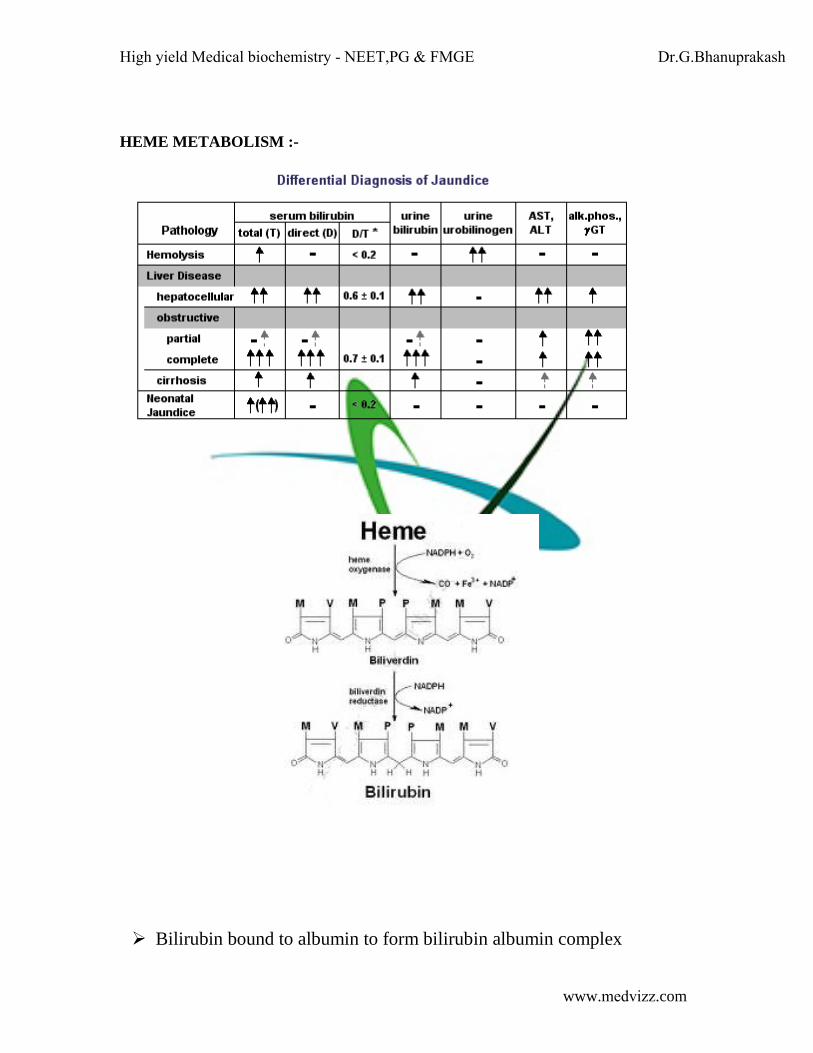
HEME METABOLISM :-
Bilirubin bound to albumin to form bilirubin albumin complex
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
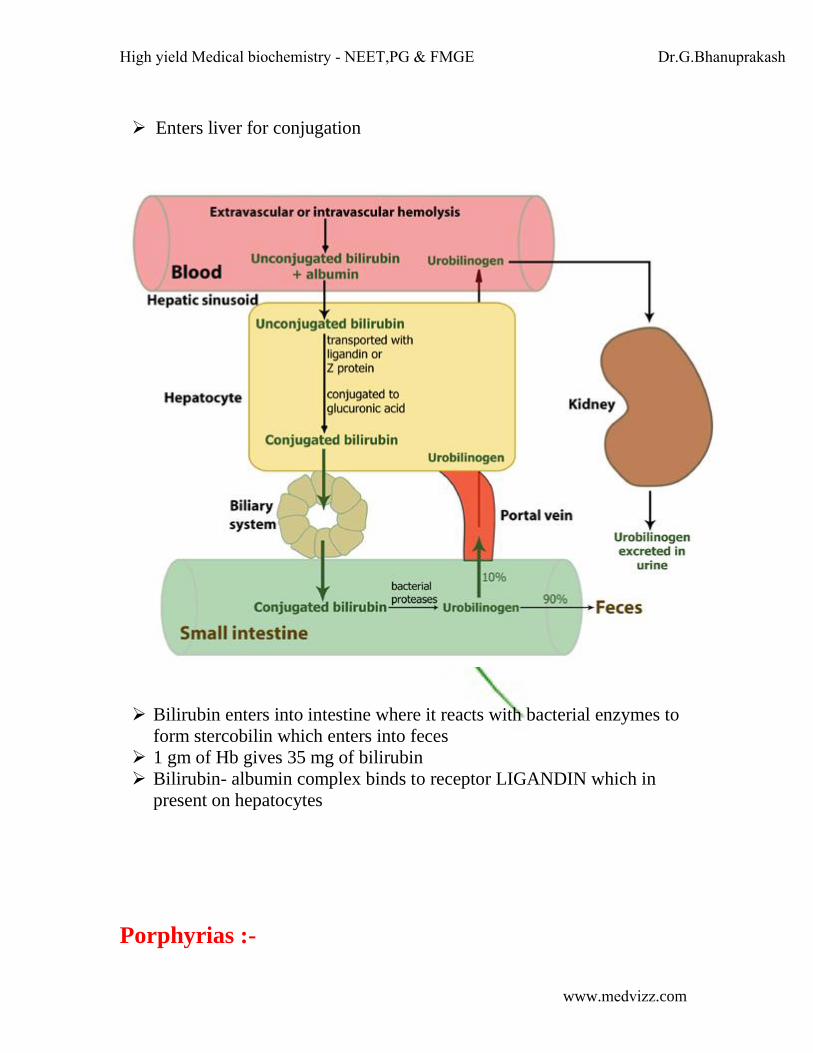
Enters liver for conjugation
Bilirubin enters into intestine where it reacts with bacterial enzymes to
form stercobilin which enters into feces
1 gm of Hb gives 35 mg of bilirubin
Bilirubin- albumin complex binds to receptor LIGANDIN which in
present on hepatocytes
Porphyrias :-
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
CARBOHYDRATE METABOLISM:-
Insulin dependent glucose transport – GLIT-4 skeletal muscle, adipose
tissue
GLUT-1 – erythrocytes
GLYCOLYSIS CYCLE:-
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
Location – cytosol of all most all the cells
Glucokinase – liver, hexokinase – other tissues
Hexokinase – low Km, glucokinase- High Km
(PFK-1) Phosphofructokinase-1 – rate limiting step
Spilitting – aldolase-A . 7 ATP in aerobic glycolysis and 2 ATP in
anerobic
Glycolysis in RBC is always anerobic
IRREVERSIBLE STEPS:-
Hexokinase
PFK-1
Pyruvate kinase ( deficiency hemolytic anemia )
INHIBITORS:-
Glycerol dehyde 3 phosphate dehydrogenase – iodo acetate ,arsenate
Enolase – fluoride
Phospphotriose isomerase - bromohydroxy acetone phosphate
End product of aerobic glycolysis – pyruvate
End product of anaerobic glycolysis – lactate
Glycolysis in erythrocytes is always anaerobic
Number of ATP under aerobic glycolysis 7
Number of ATP under anaerobic glycolysis 2
PFK-1 is regulated by PFK-2
A product of glycolysis – 2,3 BPG combines with hemoglob9in and
unloads O2 to tissues.
Increase 2,3-BPG shifts O2 /Hb dissociation curve to right
Decrease 2,3-BPG shifts O2/Hb dissociation curve to left.
PDH COMPLEX:
Location – mitochondria
Enzyme complexes:-
1. E1 – pyruvate dehydrogenase – TPP
2. E2 – dihydro lipoyl transacetylase – lipoamide ,CoA
3. E3 – dihydro lipoyl dehydrogenase – NAD, FAD
Inhibitors – arsenic poisoning
TCA CYCLE:-
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
Location – mitochondria
Citrate synthase - rate limitin step
NADH produce in :-
1. iso citrate dehydrogenase
2. α-ketoglutarate dehydrogenase
3. malate dehydrogenase
FADH produced by succinate dehydrogenase
GTP produced by succinate thiokinase
INHIBITORS:-
1. Aconitase – fluroacetate
2. Α-keto glutarate dehydrogenase – arsenate
3. Succinate dehydrogenase – malonate
Number of ATP produced from 1 Acetyl Co-A is 10.
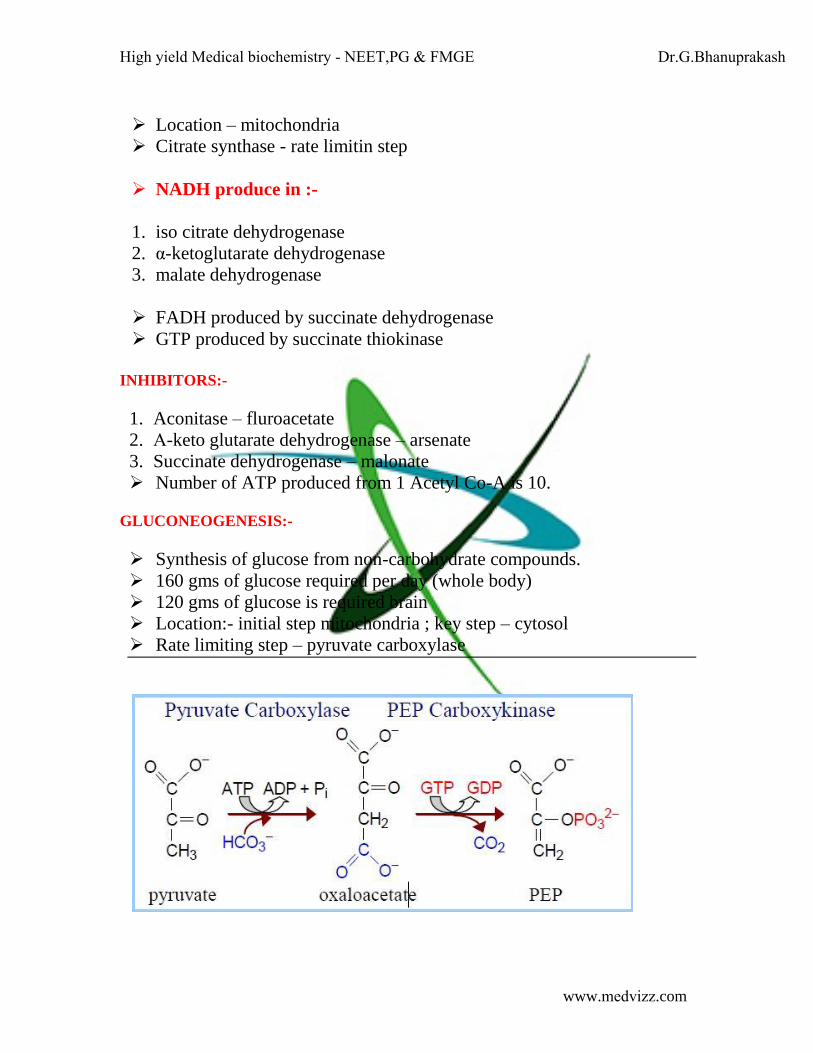
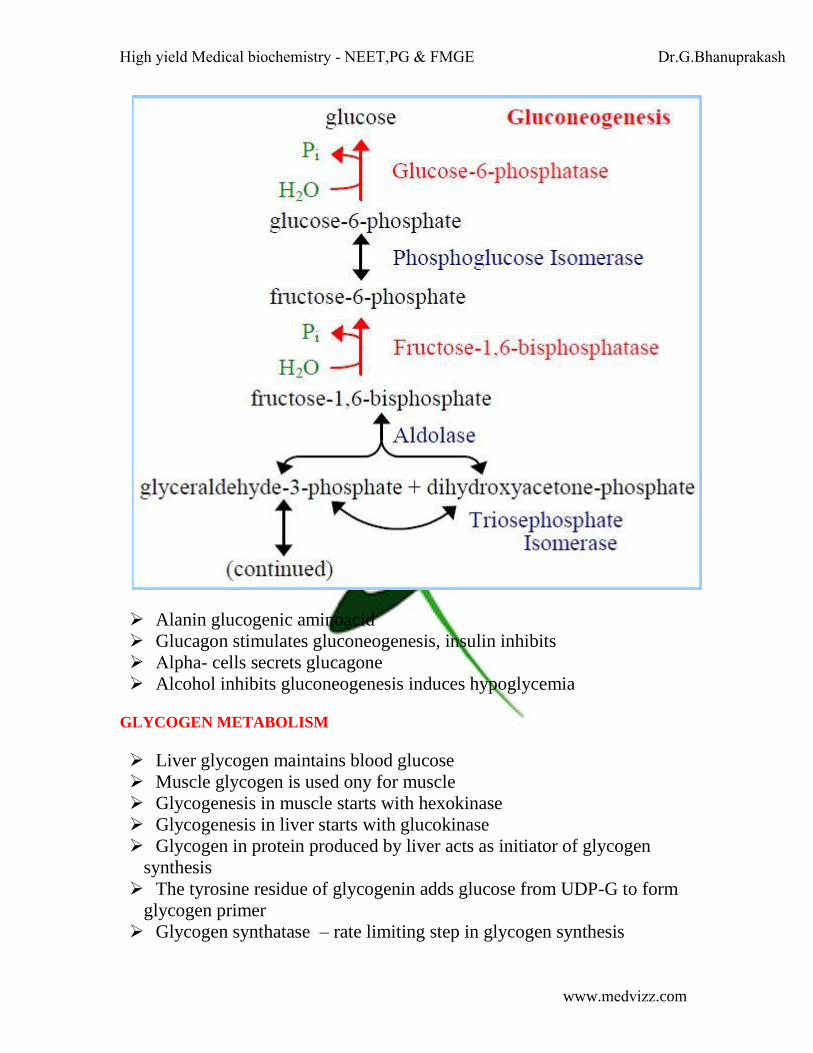
GLUCONEOGENESIS:-
Synthesis of glucose from non-carbohydrate compounds.
160 gms of glucose required per day (whole body)
120 gms of glucose is required brain
Location:- initial step mitochondria ; key step – cytosol
Rate limiting step – pyruvate carboxylase
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
Alanin glucogenic aminoacid
Glucagon stimulates gluconeogenesis, insulin inhibits
Αlpha- cells secrets glucagone
Alcohol inhibits gluconeogenesis induces hypoglycemia
GLYCOGEN METABOLISM
Liver glycogen maintains blood glucose
Muscle glycogen is used ony for muscle
Glycogenesis in muscle starts with hexokinase
Glycogenesis in liver starts with glucokinase
Glycogen in protein produced by liver acts as initiator of glycogen
synthesis
The tyrosine residue of glycogenin adds glucose from UDP-G to form
glycogen primer
Glycogen synthatase – rate limiting step in glycogen synthesis
High yield Medical biochemistry - NEET,PG & FMGE Dr.G.Bhanuprakash
www.medvizz.com
Glycogen phosphorylase breaks glycogen at α1-4 residues.
Glucagons stimulates glycogen breakdown in liver
Epinephrine stimulates glycogen breakdown in muscle
Calcium promotes glycogen breakdown by Ca+2 colmodulin complex
Glucose 6 phosphatase deficiency –Von Girek’s disease
Lysosomal α (1, 4) glucosidase deficiency – Pompe’s disease – heart is
more commonly involved – death occurs due to heart failure.
De-branching enzyme deficiency Anderson’s disease
Muscle glycogen phosphorylase deficiency –MC Ardle’s disease
Liver glycogen phosphorylase Her’s disease
Phosphofructokinase – Taruri’s disease – erythocytes, hemolysis
HMP PATHWAY:-
HMP pathway is only pathway which synthesizes NADPH in RBC
(required for antioxidant reaction)
Rate limiting step – glucose 6 phosphate dehydrogenase
Deficiency of glucose 6 phosphate dehydrogenase – hemolytic anemia
HMP pathway – synthesis of riboses
Transketolase dependent on TPP – decrease TPP – Werick’s
korsakoff syndrome
Glucose 6 phosphate dehydrogenase deficiency is resistant to malaria
Deficiency of xylitol dehydrogenase – essential pentosuria
GLACTOSE METABOLISM:-
CLASSICAL GALACTOSEMIA
Infants
Deficiency of galactose 1-phosphate Transferase uradyl.
Increase galactitol by aldose reductae – cataract diagnosis – elevated
galactose 1-phosphate uridyl transferase
FRUCTOSE METABOLISM:-
Deficiency of fructokinase essential fructosuria
Deficiency of aldolase-B hereditary fructose intolerance
Mucopolysaccharidoses-I – Iduronidase – Hurler’s syndrome
Mucopolysaccharidoses-II – iduronate sulfatase – Hunter’s syndrome
Mucopolysaccharidoses-III – sanfilippo syndrome
β- glucuronidase – sly syndrome (Mucopolysaccharidoses-VII)