Embed Size (px)
Citation preview

CASE REPORT
Esophagus (2010) 7:119–125 © Japan Esophageal Society and Springer 2010DOI 10.1007/s10388-010-0233-9
Daisuke Kobayashi · Masahiko Koike · Yasuhiro Kodera Michitaka Fujiwara · Goro Nakayama · Akimasa Nakao
Carcinosarcoma of the esophagus treated with chemoradiotherapy: report of four cases
Abstract Esophageal carcinosarcoma is a rare neoplasm. Esophagectomy with lymph node dissection has often been performed, although the effi cacy of chemotherapy or radio-therapy is not yet confi rmed. Four cases of esophageal carcinosarcoma who underwent chemoradiotherapy are presented. Complete response of the primary tumor was observed in one case; tumor size decreased in three cases. Two patients have been observed to be disease free, another patient died of metastatic disease, and the other had recur-rence. Six cases of carcinosarcoma treated with chemora-diotherapy were retrieved from the literature and analyzed with the four cases in the current study. Reduction of the tumor was observed in seven of the ten cases. Disease pro-gression or local recurrence was observed in three cases, and another two cases died of metastatic disease. Although chemoradiotherapy seems to be capable of local control, whether it is benefi cial in terms of prolonging survival of patients with this disease remains unknown.
Key words Esophagus · Carcinosarcoma · Chemoradio-therapy
Introduction
Carcinosarcoma of the esophagus is a relatively rare neo-plasm composed of both epithelial carcinomatous and mes-enchymal sarcomatous elements. As in the case of esophageal carcinoma, esophagectomy with regional lymph node dis-section has often been performed to treat carcinosarcoma of the esophagus, although the effi cacy of chemotherapy or radiotherapy has not yet been confi rmed. Given the short-age of patient resources, establishment of a standard therapy
through the process of formal clinical trials may not be feasible. Through review of the literature, the authors have come across several cases where chemotherapy or chemo-radiotherapy was given postoperatively. However, these modalities have rarely been used preoperatively. In the current report, the clinical course and outcome of four cases of esophageal carcinosarcoma treated with chemoradio-therapy are reported. Analysis of these patients may be of value when considering optimal multimodal therapy for this rare disease. Clinicopathological fi ndings were described according to the Guidelines for Carcinoma of the Esopha-gus of the Japanese Society for Esophageal Disease [1], and the stages in each case were classifi ed by Japanese clinical staging system.
Case report
Case 1
A 68-year-old man presented with dysphagia. Barium swallow examination revealed an irregularly elevated mass in the cervical and upper thoracic esophagus. Endoscopic examination revealed a type 2 tumor, and biopsy from the tumor led to diagnosis of carcinosarcoma. A computed tomography (CT) scan revealed lymphadenopathy around the recurrent nerves (lymph node nos. 106recR and 106recL in the Japanese classifi cation), which implied nodal metas-tasis; hence the clinical fi nding of T3N1M0, stage III. Although complete resection was deemed possible through total laryngectomy and esophagectomy, the patient wished to have the larynx preserved. Preoperative chemoradio-therapy was proposed with the aim of achieving suffi cient resection margin through shrinkage of the tumor and was delivered after written informed consent was obtained. The chemotherapy regimen consisted of oral agent S-1 (100 mg/body, days 1–21) and intravenous CDDP (80 mg/body, day 8). Two-portal radiotherapy of 40 Gy in 20 fractions to the upper mediastinum and neck was delivered synchronously during the 4 weeks of chemotherapy. Clinical response in
D. Kobayashi (*) · M. Koike · Y. Kodera · M. Fujiwara · G. Nakayama · A. NakaoDepartment of Gastroenterological Surgery, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya, Aichi 466-8550, JapanTel. +81-52-744-2250; Fax +81-52-744-2252e-mail: [email protected]
Received: October 13, 2009 / Accepted: March 8, 2010

120
the lymph nodes according to the Response Evaluation Criteria in Solid Tumors (RECIST) was partial response (PR). Shrinkage of the primary tumor was also observed (Fig. 1). Subtotal esophagectomy with regional lymph node dissection was performed subsequently (Fig. 2), and the larynx was successfully preserved. Pathological fi ndings revealed only microscopic residual squamous cell carci-noma in the mucosa of the esophagus by hematoxylin and eosin (H&E) staining (Fig. 3), and the tumor was down-staged to pTisN0M0, stage 0. Pathological effect was grade 2. The patient has been disease free for 60 months after initiation of the treatment.
Case 2
A 72-year-old man who had undergone gastrectomy for gastric cancer was examined by screening endoscopy that revealed a type 1 tumor which fi lled the lumen of the
ba
dc
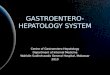
Fig. 1. a Before treatment started, computed tomography (CT) showed tumor fully occupy-ing the intralumen and lymph-adenopathy around the recurrent nerves (arrows). b After the patient underwent chemoradio-therapy, CT revealed esophageal tumor shrinking and that lymph-adenopathy had disappeared (arrows). c Endoscopy showed an irregularly surfaced elevated tumor before treatment. d Shrinkage of the primary tumor was also observed by endoscopy after treatment
Fig. 2. Subtotal esophagectomy with regional lymph node dissec-tion was performed. Macroscopic fi ndings were Ce, 0-1p, 45 × 20mm, T3N1M0, IM0, and stage III. We confi rmed R0, PM0, DM0, EM0, and CurA
Fig. 3. Pathological fi ndings revealed that most of the tumor was replaced by necrotic granulation tissue and that only a small amount of the squamous cell carcinoma cells were present in the mucosa. Hematoxylin and eosin (H&E). ×100

121
ba
dc
Fig. 5. a Before treatment started, CT showed a tumor fully occupying the intralumen and lymphadenopathy around the left recurrent nerve (arrows). b After the patient underwent chemora-diotherapy, CT revealed that the esophageal tumor and lymphade-nopathy had disappeared. c Endoscopy revealed a type 1 tumor that fi lled the intralumen of the cervical esophagus before treatment. d The esophageal tumor disappeared completely after treatment
cervical esophagus. Biopsy led to the diagnosis of carcino-sarcoma by H&E staining (Fig. 4). A barium swallow exami-nation showed an irregularly surfaced mass in the cervical esophagus. CT scan revealed nodal metastasis in the node no. 106recL (around the left recurrent nerve). Clinical fi nd-ings were T3N1M0, stage III. Although curative resection was considered possible through total laryngectomy and esophagectomy, the patient wished preservation of the larynx. He subsequently underwent chemoradiotherapy, which consisted of 5-FU (340 mg/body, day 1–5) and CDDP
Fig. 4. Pathological fi ndings revealed both atypical squamous cells growing proliferously and sarcomatous components by H&E. ×100
(6.5 mg/body, days 1–5) by weekly administration for 4 weeks with a synchronous two-portal radiotherapy of 64 Gy in 32 fractions to the upper mediastinum and neck. After chemoradiotherapy, CT scan and endoscopy revealed com-plete response (CR) in the lymph nodes as well as complete disappearance of the primary tumor (Fig. 5). He underwent additional chemotherapy, which consisted of S-1 (120 mg/body, days 1–21) and CDDP (80 mg/body, day 8) every 5 weeks for 4 months. He has been alive without recurrence for 29 months since the treatment was begun.
Case 3
A 64-year-old man presented with dysphagia. A barium swallow examination showed an irregularly elevated mass in the cervical esophagus. Endoscopic examination revealed a type 0-1p tumor (Fig. 6a), and biopsy from the tumor showed carcinosarcoma. CT scan revealed cervical lymph-adenopathy (no. 101 lymph node by the Japanese Classifi ca-tion), which led to the clinical fi nding of T2N1M0, stage II. Complete resection seemed not to be possible without sac-rifi cing the right recurrent nerve, which calls eventually for total laryngectomy. Again, chemoradiotherapy was selected, and the patient was given 5-FU (250 mg/body, days 1–5) and CDDP (5 mg/body, days 1–5) weekly with synchronous two-portal radiotherapy to the neck. After 3 weeks of treatment and delivery of radiotherapy with 38 Gy in 19 fractions, the patient wished to terminate the therapy and turn to surgery. There was no objective response to the lymph nodes, and the response was graded as stable disease (SD). Partial esophagectomy with regional lymph node dissection and

122
laryngectomy was performed (Fig. 6b). The primary tumor had responded signifi cantly, and histopathological examina-tion by H&E staining revealed that the disease was down-staged to pT1aN1M0, stage I (Fig. 7). Histological response to the preoperative treatment was diagnosed as grade 2. He suffered from necrosis of the trachea as a postoperative complication. Metastases to the liver and bone were detected 4 months after the operation, and the patient died 11 months after surgery.
Case 4
A 74-year-old man presented with dysphagia. Endoscopic examination revealed an elevated tumor that completely fi lled the lumen of the esophagus, and esophageal malignant neoplasm was diagnosed by the subsequent biopsy. CT scan showed no evidence of lymph node swelling or distant metastasis (Fig. 8). Thus, clinical fi ndings were T3N0M0, stage II. Again, the patient rejected total laryngectomy, which was necessary to curatively resect the tumor. The gigantic size of the primary tumor was such that there was diffi culty in deciding on the fi eld for irradiation. An alterna-
tive was to excise the esophageal tumor with a minimal resection margin and to immediately add defi nitive postop-erative adjuvant therapy. He underwent the palliative surgery, and histopathological examination by H&E and immunohistochemical staining of the resected specimen revealed carcinosarcoma (Fig. 9). Chemoradiation therapy, which consisted of 5-FU (300 mg/body, days 1–5) and CDDP (5 mg/body, days 1–5) weekly administration for 4 weeks and synchronous two-portal radiotherapy of 60 Gy in 30 fractions to the residual tumor in the cervical esopha-gus were given to the patient, who subsequently responded completely. However, a CT scan performed 2 months later showed lymph node metastasis located dorsally to the larynx (Fig. 10). He is currently being treated with a second-line chemotherapy that consists of oral agent S-1 (100 mg/body, days 1–21) and CDDP (80 mg/body, day 8) every 5 weeks.
Discussion
Carcinosarcoma of the esophagus is a relatively rare disease that reportedly accounts for 0.5%–2.4% of all esophageal malignant tumors [2,3]. According to the Japanese Society for Esophageal Disease, carcinosarcoma is defi ned as a neo-plasm that is composed of both epithelial carcinomatous and mesenchymal sarcomatous elements [1]. The idea that squamous cell carcinoma cells can differentiate and lead to evolution of nonepithelial cells such as mesenchymal cells within the cancerous lesion has gradually gained general acceptance as an etiology of this rare neoplasm [4,5].
By reviewing the PubMed and Igaku-Chuo-Zasshi (in Japanese) databases, only a small number of articles were found that described more than a single case of carcinosar-coma [1,6]. In most cases, radical esophagectomy with lymph node dissection was considered necessary to cure patients with carcinosarcoma. Chemotherapy or radiotherapy had been given to treat recurrent or unresectable carcinosar-coma of the esophagus, but in only a few cases were these options explored as treatment with curative intent. Tepper reported that preoperative chemoradiotherapy in esopha-geal cancer resulted in signifi cant pathological response and
a bFig. 6. a Before treatment started, endoscopic examination revealed a type 0-1p tumor at the cervical esophagus. b The patient underwent partial esophagec-tomy and laryngectomy. It was apparent macroscopically that the primary tumor had shrunk after chemoradiotherapy
Fig. 7. Pathological fi ndings revealed both atypical squamous cells that formed a sheet-like structure and partly formed a luminal structure and atypical spindle cells by H&E. ×100

123
a bFig. 8. a Endoscopic examination revealed an elevated primary tumor that fi lled the intralumen of the esophagus almost fully. b CT scan showed a huge tumor fi lling the cervical esophagus (arrow) and no obvious lymph-adenopathy or distant metastasis
a bFig. 9. a Pathological fi ndings by H&E staining revealed atypical spindle cells growing prolifer-ously and irregularly. However, epithelial components were not seen in the specimen. b Immuno-histochemical staining revealed AE1/AE3 positivity, which con-fi rmed the epithelial components. a, b ×100
Fig. 10. CT scan performed 2 months after chemoradiation showed lymph node metastasis located dorsally to the larynx (arrows)
downstaging and survival advantage [7]. However, no spe-cifi c observations were made regarding carcinosarcoma. Six cases of primary or recurrent carcinosarcoma treated with chemoradiotherapy were retrieved from the literature and analyzed with the four cases presented in the current study (Table 1). In our three cases, chemoradiation was selected so as to downstage the primary tumor, and in the other case it was undergone to distinguish the remnant tumor. Also, in all four cases, chemoradiation had the aim to avoid total laryngectomy, which is expected to cause deterioration of the quality of the lives of the patients. Three of six cases retrieved from the literature [8–10] underwent chemoradio-therapy because they were considered to not be candidates for surgical therapy for reasons of cardiac or pulmonary complications. One of three other cases had been deemed
unresectable because of direct invasion to the bronchus [11]. In another case, chemoradiotherapy was performed at the remnant metastatic lymph node, which was located in the mediastinum [12]. The reason for preoperative chemo-radiotherapy was uncertain in the remaining case [13]. Reduction of the primary tumor or metastatic site by the treatment was observed in seven of all ten cases; of the ten, CR was obtained in two cases. Disease progression or local recurrence was observed in three cases, and another two cases died of metastatic disease in the absence of local recurrence. It seems that chemoradiation is often useful in providing local control for patients with esophageal carcinosarcoma. In most reported cases, a combination of 5-FU and CDDP was utilized as a chemotherapeutic component. Similarly, we usually selected a combination

124
Tabl
e 1.
Ten
cas
es o
f ca
rcin
osar
com
a of
the
eso
phag
us t
hat
unde
rwen
t ch
emor
adio
ther
apy
Aut
hor
Age
Sex
Loc
atio
nTy
peSi
ze
(mm
)T
NM
Stag
eC
hem
othe
rapy
RT
Red
ucti
on
rate
Ope
rati
onP
atho
logi
cal
effe
ctO
utco
me
(mon
ths)
C
ause
of
deat
h
Ito
[8]
68M
UtC
e1
45T
3N0M
0II
5-F
U/C
DD
P30
Gy
24%
Sub
Gra
de 0
6 m
onth
s, de
adB
rain
infa
rcti
onM
iyak
e [9
]68
MM
t1
60T
3NX
MX
–5-
FU
/CD
DP
71 G
y94
%N
one
–3
mon
ths,
aliv
eSa
nada
[11
]58
MU
t3
75T
4N0M
0II
I5-
FU
/DT
X66
Gy
45%
Byp
ass
–8
mon
ths,
dead
Tum
or-b
ronc
hial
fi st
ula
Kaw
ano
[10]
82M
Mt
Lp
50T
3N0M
0II
5-F
U/C
DD
P60
Gy
CR
Non
e–
12 m
onth
s, de
adM
ulti
ple
met
asta
sis
Kis
him
oto
[12]
67M
Lt
113
0T
3N3M
0II
I5-
FU
/CD
DP
50 G
yP
DSu
b–
4 m
onth
s, de
adL
ymph
nod
e m
etas
tasi
sH
amee
d [1
3]24
MC
e–
––
–C
DD
P11
0 G
yP
DN
one
––
Our
cas
e68
MC
eUt
114
0T
3N1M
0II
IS-
1/C
DD
P40
Gy
80%
Sub
Gra
de 2
60 m
onth
s, al
ive
No
recu
rren
ceO
ur c
ase
72M
CeU
t1
80T
3N1M
0II
I5-
FU
/CD
DP
64
Gy
CR
Non
e–
27 m
onth
s, al
ive
S-1/
CD
DP
No
recu
rren
ceO
ur c
ase
64M
Ce
Lp
30T
2N1M
0II
5-F
U/C
DD
P38
Gy
–P
arG
rade
27
mon
ths,
dead
Liv
er a
nd b
one
met
asta
sis
Our
cas
e74
MC
eUt
143
T3N
0M0
II5-
FU
/CD
DP
60
Gy
–P
ar–
8 m
onth
s, al
ive
S-1/
CD
DP
Lym
ph n
ode
met
asta
sis
Sex:
M, m
ale;
Loc
atio
n: C
e, c
ervi
cal e
soph
agus
; Ut,
uppe
r th
ird
of t
he e
soph
agus
; Mt,
mid
dle
thir
d of
the
eso
phag
us; L
t, lo
wer
thi
rd o
f th
e es
opha
gus;
Size
: len
gth
in m
m; D
TX
, doc
etax
el; R
T,
irra
diat
ion;
Ope
rati
on: S
ub, s
ubto
tal e
soph
agec
tom
y; P
ar, p
arti
al e
soph
agec
tom
y; P
D, p
rogr
essi
ve d
isea
se; C
R, c
ompl
ete
resp
onse
of 5-FU and CDDP, and dose and schedule were modifi ed according to the patient’s condition. For patients who did not tolerate the prolonged hospitalization needed for fractionated delivery of intravenous 5-FU, the drug was replaced by S-1, an oral derivative of tegafur that is known to be active against squamous carcinoma of the head and neck.
Several studies have reported chemoradiotherapy to be effective against carcinoma of the esophagus [14,15], and could be one of the options, along with surgery, as a treat-ment with curative intent. Ota reported that granulocyte-colony stimulating factor G-CSF was detected in both squamous cell carcinoma cells and sarcoma cells and postu-lated that these components originated from a single clone [16]. The current concept referred to earlier that carcinosar-coma could arise from cells of the epithelial origin, our clinical observations, and analysis of the literature all suggest that chemoradiotherapy is active against carcinosarcoma and could be considered as a therapeutic option whenever surgery is not feasible. In this report, multimodal strategy including chemoradiation certainly seemed useful in carci-nosarcoma of cervical esophagus to preserve the laryngeal function. It may provide patients who cannot undergo surgi-cal resection with adequate local control. However, chemo-radiation did not result in ultimate cure even of the responders, sometimes because of metastatic disease outside the fi eld of radiation. These recurrences sometimes occurred early after local control was obtained, and whether the local control contributes to prolongation of survival remains to be elucidated.
References
1. Japanese Society for Esophageal Diseases. Guide lines for the clini-cal and pathologic study on carcinoma of the esophagus. Ninth edition. Esophagus 2003;1:61–88.
2. Xu LT. Clinical and pathological characteristics of carcinosarcoma of the esophagus: report of four cases. Ann Thorac Surg 1984;37:197–203.
3. Iyomasa S. Carcinosarcoma of the esophagus: a twenty-case study. Jpn J Clin Oncol 1990;20:99–106.
4. Iwaya T. Esophageal carcinosarcoma: a genetic analysis. Gastroen-terology 1997;113:973–7.
5. Matsumoto T. Loss of heterozygosity analysis shows monoclonal evolution with frequent genetic progression and divergence in esophageal carcinosarcoma. Hum Pathol 2004;35:322–7.
6. Iascone C. Carcinosarcoma and pseudosarcoma of the esophagus: two names, one disease. Comprehensive review of the literature. World J Surg 1999;23:153–7.
7. Tepper J. Phase III trial of trimodality therapy with cisplatin, fl uo-rouracil, radiotherapy, and surgery compared with surgery alone for esophageal cancer: CALGB 9781. J Clin Oncol 2008;26:1086–92.
8. Ito M. A case of so-called carcinosarcoma of the esophagus. Kouchi-shi Ishi 2002;7:80–4.
9. Miyake M. One case of carcinosarcoma of the esophagus treated with chemoradiotherapy. Jpn J Cancer Clin 2003;49:127–31.
10. Kawano S. A case of carcinosarcoma of the esophagus treated by the chemoradiotherapy. Nippon Syoukakibyou Gakkai Zasshi 2007;104:535–41.
11. Sanada Y. Esophageal carcinosarcoma with intramural metastasis. Dis Esophagus 2006;19:119–31.
12. Kishimoto H. A case of carcinosarcoma of the esophagus. Geka 2002;64:713–6.

125
13. Hameed H. Metastasis of carcinosarcoma of oesophagus to gas-trostomy site. Br J Oral Maxillofac Surg 2009;47:643–4.
14. Herskovic A. Combined chemotherapy and radiotherapy com-pared with radiotherapy alone in patients with cancer of the esoph-agus. N Engl J Med 1992;326:1593–8.
15. Mariette C. Therapeutic strategies in oesophageal carcinoma: role of surgery and other modalities. Lancet Oncol 2007;8:545–53.
16. Ota S. Monoclonal origin of an esophageal carcinosarcoma produc-ing granulocyte-colony stimulating factor: a case report. Cancer (Phila) 1998;73:2102–11.