Embed Size (px)
DESCRIPTION
CP pychia not perfect but can be used as guide
Citation preview

Holy Child School of Davao
E. Jacinto Street, Davao City
College of Nursing
A Case Study on
Schizophrenia – Paranoid type
In Fulfillment of the Requirements in
Nursing Care Management 105
Related Learning Exposure
Psychiatric Nursing Exposure
Submitted to :
Ms. Clara Grace Lising
Mr. Kenneth Sabido
Submitted By :
March 12, 2012

TABLE OF CONTENTS
I. INTRODUCTION……………………………………………………………….A. Goals and Objectives……………………………………………………….B. Spot Map…………………………………………………………………….
II. ANAMNESIS…………………………………………………………………….A. Informants……………………………………………………………………B. NPI……………………………………………………………………………C. Genogram……………………………………………………………………D. Developmental Task………………………………………………………..
III. PHYSICAL ASSESSMENT……………………………………………………
IV. MENTAL STATUS EXAMINATION…………………………………………………………………A. Initial………………………………………………………………………….B. Final………………………………………………………………………….
V. DEFINITION OF TERMS………………………………………………………
VI. ANATOMY AND PHYSIOLOGY………………………………………………
VII. PSYCHODYNAMICS………………………………………………………….A. Etiology
1. Predisposing……………………………………………………………2. Precipitating…………………………………………………………….
B. Symptomatology……………………………………………………………C. Schematic Tracing…………………………………………………………D. Narrative……………………………………………………………………
VIII. MEDICAL MANAGEMENTA. Actual Laboratory/Diagnostic Test………………………………………B. Drug Study…………………………………………………………………
IX. NURSING MANAGEMENTA. Nursing Care Plan…………………………………………………………B. Discharge Plan……………………………………………………………
X. PROGNOSIS…………………………………………………………………XI. REFERENCES………………………………………………………………

Introduction
“Once were thought to be possessed by demons and were feared, tormented, exiled or locked up forever”.
Schizophrenia, also sometimes colloquially called split personality disorder, is a chronic,
severe, debilitating mental illness. With the sudden onset of severe psychotic
symptoms, the individual is said to be experiencing acute schizophrenia. Psychotic
means out of touch with reality or unable to separate real from unreal experiences.
There is no known single cause of schizophrenia. As discussed later, it appears that
genetic factors produce a vulnerability to schizophrenia, with environmental factors
contributing to different degrees in different individuals. Symptoms of schizophrenia may
include delusions, hallucinations, catatonia, negative symptoms, and disorganized
speech or behavior. People with schizophrenia are at increased risk of having a number
of other mental-health conditions, committing suicide, and otherwise dying earlier than
people without this disorder.
There are five types of schizophrenia based on the kind of symptoms the person has at
the time of assessment: paranoid, disorganized, catatonic, undifferentiated, and
residual.
Our patient given name “Mr. Bill” was chosen to be the subject of this case study. He
was diagnosed with Schizophrenia-Paranoid type and manifest symptoms such as
hallucinations and delusions.
Schizophrenia occurs in all societies regardless of class, color, religion or culture. It is found in over one percent of the population over the age of 18 or as many as 51 million people worldwide.It appears between the ages of 15 and 25 with men getting the disease earlier than women according to Schizophrenia.Com, a non-profit online community that provides information, support, and education to people with schizophrenia.Schizophrenia is costly for both families and society. In the US alone, schizophrenia consumes a total of $63 billion a year for direct treatment, societal, and family costs. It is one of the Top 10 causes of disabilities in developed countries, according to the World Health Organization.
In the Philippines, a disability survey made by the National Statistics Office revealed that mental illness (which includes schizophrenia) is the third most common form of disability with a prevalence rate of 88 cases per 100,000 population.

Here in Davao, Dr. Padilla said that the Davao Mental Hospital receives an average of eight to 10 patients a day suffering from schizophrenia.
This case study is an in depth look at patients environment, we study his unique experiences and behaviors to improve some aspects of his behaviors.
This case study would help us manage future pt. with similar disease. And be a reference for future researchers this will also implicates understanding human mind and behavior in general.
This Case study was conducted at Dela Cerna Psychiatric Clinic and Rehabilitation Center at Cabantian Davao City to a 32 years old Psychiatric Pt. in cooperation with his significant others.

A.OBJECTIVES
General Objectives
At the end of the clinical exposure at Dela Cerna Psychiatric Clinic and Rehabilitaion
center for mentally challenge individual at Cabantian Davao City. We the 3rd year nursing
students of Holy Child College of Davao will be able to understand insanity and conduct a
thorough and comprehensive study about “Mr. Bill’s” disease according to data gathered from
series of interview, patients chart and data gathered from extensive research.
Specific Objectives:
1.Organized Patients data for reference of background information.
2. Show families health history, as well as the past and present illness to correlate factors that
can contribute to patients illness.
3. Make Genogram and of patients family and trace factors that can predispose to patients
disease.
4. Trace psychological development of our patient through the use of the different
developmental theories .
5. Give the best definition of the disorder and understand unfamiliar terms
6. To have a good overview of patients over all health status by presenting data gathered from a
thorough physical assessment.
7. To discuss Anatomy and Physiology of system involved
8. Make a diagram showing the pathophysiology of Schizophrenia and its relation to its
symptoms to have idea on how this affects a person.
9. To perform and evaluate the patient’s Mental Status Exam
10. To study appropriate and actual drugs of Patient.
11. To formulate individualized care plan to address needs and problems.
12. Prognose probable outcome of nursing management rendered to patient.

II. ANAMNESIS
A. Personal Data
Patient name is “Z”,33 years old Male and was born on March 17, 1978, He is a Filipino
citizen and was baptized under Catholic Religion. He is single and the eldest to their
family he resides at Prk 1 Alejal Carmen Davao del Norte.His mother is Mrs Y 48 years
old She is a plain housewife while Pt.Z’s Father Mr X, 64 yrs old a retired Principal at
Alejal Elementary School Carmen Davao del Norte.And currently manage their 24 hectar
land at Dujali, Carmen Davao del Norte.Where they grow Rice, Banana and Coconut
trees which is the source of their income.
B. Family History
1. Maternal and Paternal Grand Lineages
Mental Disease was not present on both parties. On the Paternal side, they are just a
small family, with three siblings and 2 of them are professionals, while on the Maternal
side they have a bigger family with 9 siblings The Patient’s Mother was married at the
age of 15 and next to her marry a soldier and has abundant life compare to their other
brothers and sisters.On the Maternal side Chronic unemployment is present, eccentricity
and dependency and also Drug addiction is present.
The Mother claimed that the patient was living in one of his brother in Tanay Rizal in
Manila for 3 years after graduating in college and that they heard that her brother was a
user and a pusher. They believed that the patient was influenced and used drugs when
he stayed there and also her brother was killed in front of the patient by unknown
suspects.
2. Father
The patient’s father Mr. X 64 years old is a kind and loving father he is not strict and a
good provider. He always ensure that his family meet their needs and inculcate the
importance of education to his children. His father also claimed that Patient Z was one

of his favorites. He is also a responsible husband to his wife and believes that in
disciplining it doesn’t mean you have to hurt your child that’s why when his children
commit mistake he just talked to them and instead of hitting .
Patient Z’s Father belong to a middle class society. He taked Bachelor of Science in
Education during College at St. Mary’s College at Tagum City and was able to finished
his education. He worked as a Teacher right after graduation, Although he is already
living in with the patients mother they got married just after graduation.
3. Mother
Mrs Y same with Mr X she is also a loving and caring mother. She is not so strict same
with his husband she is just a high school student when she got married to Mr. X.She did
finished her highschool and did not pursue college education because she wanted to
take care of her children. She had her first baby Pt Z. When she is 14 years old so she
needs to go to school and entrusted Pt. Z to his grandmother. She got married at the
age of 15. According to Mr Y, Mrs X is an affectionate wife she is understanding and
helps his husband at all times.
4. Sibling
Pt. Z has two younger brother and sister. Baby Boy 32 years old is next to him and Baby
Girl 31 the youngest and only girl in the family. Although sibling rivalry is present with Pt
Z and Baby Boy they still care for each other,He helps Baby Boy at all times especially
school works. Baby Girl said that Pt. Z is a strict Brother he often scold her if she come
home late and don’t allow her to go to disco even with the company of their cousins.
Baby Girl doesn’t smoke but drinks occasionally same with Baby Boy
.

C. Personal History
a.Prenatal
Mrs Y is just 14 years old when she conceived Pt. Z. They are not expecting but they are
happy when they heard that she is pregnant.Obstetrical supervision is adequate,she had
her regular check up at her Ob-gyne Dr. Abad at Christ the king Hospital Tagum City.
She had completed her pre natal check up and doses of tetanus vaccine and was able
to take her vitamins.
b.Birth
March 16, 1978 Mrs Y felt pain and starts to labor. She was rushed to Christ the King
Hospital in Tagum City. She was examined and assisted by her Doctor, Dr. Abad,After
39 weeks of conception Mrs Y gave birth to a live Baby Boy on March 17, 1978 3:30 am.
She labored for 2days and 1 night. She gave birth via normal spontaneous vaginal
delivery
c.Infancy
,The patient did not completed his vaccination because during their time the implication
of vaccination is not that strict unlike today. He was only given BCG.vaccine. Patient
was breastfeed for 3months Mrs Y would always cuddle him and feed him everytime he
cries. Because Mrs Y is still studying . she needs to entrust Mr Bill to her mother, They
then decided to bottle feed him with Bona. Every morning before going to school she
would prepare her babies milk. And her mother would take care of him until she comes
home. Her mother said that she feeds the baby when it cries and cuddle him almost all
the time He is the first grandson so he is really well loved. Mrs Y first noticed that he
sprouted his first tooth when he is 3months they had observed that he become irritable
and starts biting behavior and drooling . When both parents are at home they would start
to teach him how to walk, and talk. Pt. Z started to walked when he is 1 year and 3
months and started to talked at 1 .Mrs Y reported his first illness during his first year, he

was admitted for 1 weak at Cainglet Hospital at Panabo under the service of Dr. Boiser
because of typhoid fever.
d. Psychosexual History
At 3 years old they saw that Pt. Z starts to fondle his penis and both parents just ignored
this behavior. Masturbatory practices was not observed by parents. He was circumcised
at age 6 and lowered speech of voice was first observed during his High School year at
age 14.
e. Play Life
Pt. Z preferred to play marble when he was young according to his parents. He often
play with his Brother and sister and also to his peers outside with both sexes. He usually
leads the game but noted also by his peers to be a good follower. He usually played
mostly outside of their house than in their neighborhood. The parents did not noticed any
habit formed by particular games nor playmates. He always make sure that all his
household chores and schoolwork’s are finished and had his snacks before going out to
play.
f. School History
Patient started to enter school at age 7 at Alejal elementary School where his father is
working as a teacher , He graduated with Honors. He had his HighSchool at Carmen
National High school at age 13 he become an active member of the ROTC he attented
numerous seminars about leadership during high School According to patients
classmates he is a good to everyone.His teachers stated that he is not a problem to
them, and he is a responsible and a good leader.According to his parents he doesn’t
want to miss school even without a “Baon” it is ok with as long as he will not miss his
classl. He usually study for 30 minutes to 1 hour everyday.His Favorite subject is Art.

Even in his free time Patient Z would paint on their wall and curved wood. He graduated
with Honors again in High School.He then started his first year in College at University of
Mindanao in Tagum and taked up Bachelor of Science in Criminology, at this time the
patient started to engaged self in alcohol and cigarettes. Then patient decided to transfer
to a new school according to him people in his previous school are bad influence to him.
He finished his course at University of Mindanao in Bolton Davao City at age 22 last
March 5 1999.
g. Religious and Social Adaptability
Patient Z is noted to be friendly he selects his friends and he usually hang out with
intelligent people of their class. He is choosy, shy but if he knows you already he is
friendly. Even thou he is choosy he is still kind to other people its just that he is much
closer to his choosen friends. Patient Z was born and and baptized in the catholic
religion. He is an active member of his church and he would always goes to church
every Sunday. When patient feels down and failured he would usually sit on the corner
and keep it himself.
h. Occupational history
The patient has no current job and reported to worked only as a security guard at age
23 in Manila after graduation for 1 year.Parents don’t know the reason why patient
decided to quit his job. And that he has not saved any money during his work.
i.Marital Status
According to patients significant others he had his first girlfriend in highschool but the
girl’s parent did not liked him and that caused their breakup. Then after graduation he
went to Manila and meet his second girl they become lived in partner in manila for 2
years until the girl decided to live for no known reason.The patient is said to be a
secretive person especially in his lovelife,.And so some of love life and problems about it
are not known to them.

j.Substance used and abused
Patient is reported to abused drugs during his stay at his uncles house who is pusher in
manila. He smoked and drink alcohol regularly during his stay in Manila usually with
people around their place.When he came back in Carmen he would be invited by friends
to drink and when already drunk he usually shout and hunt his younger brother.
k. Coping Strategy
Patient is reported to be secretive in terms of problem, he usually don’t tell anyone when
he is upset. He will be found walking and sitting in there baranggay hall when he is upset
or angry but after an hour he would come back and act normally. When he cames back
from manila he would easily get mad and use his fist when he is angry to someone.
l.Family physical or mental problems
There is no mental problems within the family .But one of the Patients uncle is said to be
a drug user and pusher. And patient is said to be influenced by his uncle. And his uncle
eventually died after being shoot by an unidentified person this happens 6 years ago.
m. Onset of Present illness
The family of Patient believed that his mental illness started after he come back from
Manila. When the patient is 22 years old right after his graduation in college, He decided
to go to Manila because of his dream to enter the Armed Forces of the Philippines, Even
thought all his family tried to stop him and instead work as a policeman in their province
Patient Z still decided to go. April 21, 2000. He lived in Tanay Rizal in one of his
mother’s Older brother. They did not monitor his life with his uncle, all they know is that
he is working as a security guard and that he did enter the AFP but they don’t know what
really happens at AFP. And one of his aunt who lived in quiapo said that on June 16 of
2000 Patient Z visited them and they saw that the patient seems so emaciated, If they
ask how is he he would just answer he is fine Z also told them that he is now living in
with his girlfriend whom she meet a month ago. Then that was the last visit that the

patient did until a one morning of December 2002 a news was reported that somebody
has been killed and that man was the patients uncle and they said that it was a planned
killing because his uncle was a user and a pusher and the patient had disappear, Until
the Patient’s decided to find him with the help of his aunt. Her aunt was a overseas
worker who happened to come back at same year she was married to a soldier and
decided to find him it was almost 5 years since the family has not received any news
from the patient. Untill the patients aunts imbestigator send a good news. He has found
the Pt. in one of the provinces in quezon. According to his description he was wearing a
sack and covered his head with a plastic cellophane and he had a long hair and a beard,
dirty and he is staying on the trees.The aunt decided to bring him to a clinic so he can be
check, they give them food, cut his hair,clean him, and he was given a maintenance .
Then they decided to send him back to alejal where his parents are waiting for him. So
his aunts husband, the soldier, take him to Carmen riding a plane but The patient don’t
want to see the other soldier he seems afraid even with their uniforms. He starts to have
delusion that he is going to be persecuted by those person. So the soldiers wear civilian
clothes just for him to ride the plane and after coming back home at Carmen Davao del
Norte on May 2006 his family take care of him they continue to give him his
maintenance. They claimed improvement and they did not send him to doctor for a
check up for his past condition. According to the patients sister he seems to be anxious
of someone and afraid of people who pass at there house, that wears a black dress a
helmet and rode a motorcycle. He even told his sister not to talked to anyone he don’t
know. His sister told this to her mother but the mother seemed to be in denial when told
that his son is having mental illness and so the mother just ignore this symptoms.
Everyday the patients just stay at their house and don’t go out his brother was in davao
that time working as a security guard.Then one day, there is a disco. And the patients
friend come to there house and invited him. The patient go and took a glass of liquor

then reported to involved in a riot. Behavioral changes are seen everyday, hysterical
behaviors, poor sleep was noted but his parents managed it by giving him herbal
medicines then they brought him in an acupuncture clinic at PORRAS in tagum and they
claimed improvement. But after a months patient starts to talked to self and they
discovered that pt. is taking all his meds at once when scolded by his father he would
answer “kanus.a pman diay ko mahuman ug inum ana” so they brought him back to
PORRAS. They claimed improvement but after 5 months had relapse, Patient smoke 2
packs of cigarette per day, and drinks liquor. On Jan.8 2012 he was reported that he
slapped his cousins face and tend to become violent he verbalized “patyon ko ninyo” He
isolates himself and cries alone; Hence bought to the Davao Mental Hospital on January
20 2012. He was an out patient in Southern Philippines Medical Center prior to DMH on
January 8 2012.under the service of Dr. Lacro and was advised to be back after 2 week
for a follow up check up he was given medications such as Risperidone 2 mg 1 tab Am
and 1 tab HS, Haloperidol 5mg 1 amp IM and akidin 2mg 1 tab BID PRN for
EPS.Admitting Impression, Schizophrenia Paranoid Type and Final Diagnosis was
Schizoprenia Paranoid type.Because of overwhelming number of patients at DMH The
Parents decided to transfer the patient to Dela Cerna Psychiatric Hospital and
Rehabilitation on January 22 2012, 2pm Under the service of his physician Dr. Janet
Perez and Phsychia incharge Dr. ma. Lythia Dela Cerna Cervera. Pt. wearing a blue
shirt and maong shorts also wearing a rosary and accompanied by his parents, he is
crying, Conscious and responsive and a fair affect was noted. Medication are
Risperidone 4 mg ¼ tab Am ¼ tab Hs BPN 2mg 1tab BID, Rivotril 2 mg ¼ tab. Patient
was in Homicidal, Suicidal and escape precaution.
The patient was reported that he did not completed his immunization during childhood
her mother told that the patient at an early age suffer from many childhood diseases
such as Typhoid fever after 1 weak from discharge he was again admittedfor 1 week

under the service of Dr. Boiser because of loose bowel discharge at Cainglet Hospital at
Panabo and with diagnosis of Amoebiasis. And during his 3 years of age he was again
admitted for 1 week at the same Hospital and same attending physician because his
mother noted a yellowish discoloration in his skin he was diagnosed to have hepatitis A.
A. Informants
1. Name: Mr. X
2. Address:Prk 1 Alejal Carmen Davao del Norte
3. Relationship to Patient:Father
4. Length of time knowing the Patient: Since Birth
5. Apparent understanding to present illness of patient: “Nag adik man gud na siya
atong pag adto niya ug manila human cguro frustration pud nga wla xa kasulod sa
AFP mao na ing ana siya”
6. Characteristic and attitude of informant: The father warmly and happily welcomes
us. He is very kind and friendly. He was cooperative and answers all our question.
1. Name: Mrs Y
2. Address:Prk 1 Alejal Carmen Davao del Norte
3. Relationship to Patient: Mother
4. Length of time knowing the Patient: Since Birth
5. Apparent understanding to present illness of patient:” Wala man me kabalo naunsa
na siya nagkalit lang man, naa lang mga istorya nga sa Manila daw kay naga
drugs siya.”

6. Characteristic and attitude of informant: The mother is simple and smiled when she
see us. She is also cooperative when ask about information about his son.
1. Name: Mrs Nena
2. Address:Prk 1 Alejal Carmen Davao del Norte
3. Relationship to Patient:Aunt
4. Length of time knowing the Patient: Since Birth
5. Apparent understanding to present illness of patient: “na troma man gud na siya
kay gepatay akng igsuon sa iya jud atubangan”
6. Characteristic and attitude of informant: The informant was talkative and happily
shares information about the patient.
1. Name: Lea
2. Address:Prk 1 Alejal Carmen Davao del Norte
3. Relationship to Patient: Sister
4. Length of time knowing the Patient:Since Birth
5. Apparent understanding to present illness of patient: “Nasugdan man gud na og
adik-adik mao na ing.ana na kay kana man gud igsuon sa akong mama getudluan
na nila akong kuya.”
6. Characteristic and attitude of informant: The informant was a strong person she
was hesitant at first but eventually open up and shared information about her
brother.

1. Name: Rasec
2. Address:Prk 8 Ising Carmen Davao del Norte
3. Relationship to Patient: Friend
4. Length of time knowing the Patient:Since High School
5. Apparent understanding to present illness of patient: “natingala lang man
nganu na ing. Ana mn siya nga but’an man kaau na siya nga tao wla pud bisyo
atong nag iskwela pa me, ingon nila sa manila daw naadik dawn na siya
human wla niya ma control mao na ing.ana”
6. Characteristic and attitude of informant: Informant was nice and openly shares
information about the patient

Narrative History:
On the paternal side both pts grandparents died of old age. They only have 3 sibling.Ram the
eldest was aborted accidentally when Ning slipped on the floor, then Luz 65 years old a retired
teacher and has hypertension. Then the youngest is the pts father X 63 years old male he dont
have any ailments because he is a sporty person.On the maternal side his Grandparents linda
and Jose are both deceased jose died because of old age while his wife linda died with no
known reason. They have 9 siblings Boy the eldest died at age 18 because of vehicular
accident then next Yna married with no work then Lando died because of a gunshot and is
rereported to be a drug addict.Then next is The pts mother Y 43 years old with no noted
ailments at present. Next to her is Linda with hypertension, Then Nato who died also at age 24
because of a vehicular accident Then Kardo with arthritis and Mario with arthritis also then pila
with hypertension and the eldest is Ben.X and Y has 3 siblings Patient Z eldest and diagnosed
recently with Paranoid schizophrenia Next to her is Ben 32 years old and the Eldest the only
female Lisa 31years old.

D. Developmental Task
Developmental
stage
Task Achieved Not
achieved
Justification
Trust Vs,
Mistrust
(Birth to 18
months)
Autonomy Vs.
Shame and
doubt
(18 months to 3
years)
Initiative Vs.
Guilt
(3 to 5 years old)
Industry Vs.
Inferiority
(6 to 12 years)
Identity Vs. Role
Confusion
( 12 to 18 years)
Intimacy Vs.

Isolation
( 18-35 years)
III. Physical Assessment
Name: Z
Date of Assessment: March 2, 2012
Time of Assessment:2:30 pm
Location of Assessment:Dela Cerna Psychiatric and Rehabilitation Center
Cabantian Davao City.
Vital Signs: BP 100/60milimeter mercury
Wt: 76 kilogram
CR: 79beats per minute
RR: 24 cycles per minute
Temp: 36.5 Degrees Celsius
General Survey:
Our Pt. Z was assessed on March 2, 2012@ 2:30pm. He was siiting on the chair behind
the wall of the convention room. He was conscious, oriented and coherent when asked. He is
cooperative and appears happy. He is wearing a clean white shorts and a blue shirt.
Skin
Patient has fair skin, has good skin turgor,Nails were properly trimmed with no traces of dirt
noted upon inspection, warm to touch skin, No rashes nor inflammation noted.Pt. Temperature
is in normal range.
Head

Pt’s head is normocephalic. Involuntary, Lesions, bleeding and bruises were not seen upon
inspection.Hair is Black and well cut. With no dandruff noted.
Eyes
Eyelids are symmetrical, pink conjunctiva noted. Sclerae is clear and icteric. Iris appears black
on both eyes. She has isocoric pupil of 2mm; Round and reactive to light accommodation. Both
eyes moved in unison with no signs of scratches and discharges on both eyes.
Ears
Externa pinnae are aligned to the outer canthus of each eye and are symmetrical.The shaped of
the pinnae are oval with no discharges noted. Ears are firm and non tender. Signs of lasions,
lacerations, swelling and bruises were not seen upon inspection. She was able to repeat
sentences when softly said behind his ears, which reveals that he has no hearing problems.
Nose
External surface of the nose is smooth and oily. Nasolabial folds are symmetrical. Nostrils are
also symmetrical with no flaring and discharges. Nasal hairs are present upon inspection. Nasal
septum is not deviated. Both nostrils are patent. No signs of tenderness noted. Patient was able
to distinguish the smell of the rubbing alcohol and female Perfume while eyes are closed.
Mouth
Gums and buccal mucosa are pinkish in color. Uvula is positioned in the midline of the soft
palate Tongue is in the midline of the mouth. No signs of inflammation and laceration of the
uvula. Tonsils are not inflamed. Bleeding, ulceration and swellingwere not seen upon
inspection.Patyient was on Diet as tolerated and does not have difficulty in eating and
swallowing.
Neck

The neck of pt. can moved easily without any difficulty, which includes right and left rotation and
hyperextension. Neck properly supports head with no signs of thyroid enlargement and lymph
nodes. No deformities noted.
Chest and lungs
Chest muscle expand during inspiration and relaxation, during expiration are symmetrical and
painless. No presence of scars and lesions. He was not in respiratory distress. Respiratory rate
is 24cycles per minute, rhythm was regular. Breath sounds were clear on both lungs.
Heart
Heart rate is normal and regular in rhythm. Apical pulse is auscultated at fifth intercostals space
left midclavicular line. Heart sound is clear. Murmurs are not noted.
Abdomen
Patient abdomen is globular and not distended upon inspection. Normoactive bowel sound of 16
in one full minute is noted. Tenderness is not noted. No abrasion or scars noted.
Genitourinary
Patient refused to assess genital area. However patient verbalized no pain or difficulty upon
urination and defecation. His total urine output for 8 hours was about 640cc. It is a straw colored
urine. And defecate once a day with clay colored urine.
Upper Extremities
Patients upper limbs and shoulders and arms were symmetrical. No tenderness noted on both
bones of the wrist and fingers. No deformioties and swelling noted. He could freely move her
shoulders. The patient has strong grip when asked to squeeze one of my hands. No structural
deviation noted. And edema was not noted.
Lower Extremities

Both legs of patients are symmetrical and can stretch, flexed, rotate, extend and bend without
any difficulty. No signs of deformities, lesions, and lacerations noted bruises were not seen
upon inspection.
Holy Child College of Davao
College of Nursing
MENTAL STATUS EXAMINATION
Name of Patient:_______________________________ Date:______________________
I. Pre-Examination
A. General Apperance:________________________________________________
B. General Mobility:___________________________________________________
1.Posture & Gait:___________________________________________________
2. Activity: ( ) normoactive ( )Psychomotor retardation
( )hyperactive ( )agitated
3. Facial Expression:_______________________________________________
C. Behavior ( ) friendly ( )impulsive ( )angry
( ) negativistic ( ) evasive ( )seductive
( )withdrawn ( )embarrassed ( )indifferent
D. Doctor- Patient Interaction
( ) cooperative ( ) uncooperative
( ) initially
( ) all throughout
Quality: ( ) warm ( ) distant ( ) dependent

( ) hostile ( ) suspicious ( ) talkative
Others:__________________________________
II. Stream Of Talk
A. Character
( ) spontaneous ( ) deliberate ( ) Pressured ( ) blocking
B. Organization
( ) relevant ( ) loose association ( ) Tangentiality
( ) Irrelevant ( ) flight of ideas ( ) neologism
( ) incorrect ( ) circumstantiality ( ) others
C. Accessibility
( ) good ( ) self absorbed ( ) defensive
( ) fair ( ) mute ( ) inaccessible
III. EMOTIONAL STATE AND REACTIONS
A. Mood
( ) euthymic ( ) depression ( ) euphoria
B. Affect
( ) appropriate ( ) Inappropriate
Quality:
( ) flat ( ) elated ( ) Histrionic
( ) Blunted ( ) labile ( ) angry
( ) hostile ( ) anxious ( ) others_______________________
C. DEPERSONALIZATION and DEREALIZATION
( ) present ( )absent
D. SUICIDAL IDEATION
( ) present ( ) absent

IV. THOUGHT CONTROL
A. PERCEPTION
( ) present ( ) absent
B. DELUSIONS
( ) Present ( ) absent
Type:___________________________________________________________
C. IDEAS OF REFERENCE ( ) present ( ) absent
D. PREOCCUPATIONAL AND RUMINATIONS( ) present ( ) absent
E. DÉJÀ VU and JAMAIS VU ( ) present ( ) absent
V. NEUROVEGETATIVE DYSFUNCTION
A. SLEEP
( ) normal ( ) MNA ( ) DFA
( ) Hypersomnia ( ) EMA ( ) interrupted sleep
B. APPETITE_____________________________________________________
C. DIURAL VARIATION_____________________________________________
D. WEIGHT_____________________________
E. LIBIDO______________________________
VI. GENERAL SENSORIUM AND INTELLECTUAL STATUS
A. ORIENTATION Time:_________ Place:________ Person:_______
Situation:______________________________________
B. MEMORY Remote:_______ Recent:________Immediate:_____
C. ATTENTION SPAN: ( ) Good ( ) Fair ( ) Poor
D. GENERAL INFORMATION___________________________________________
E. ABSTRACT THINKING ABILITY______________________________________
F. JUDGEMENT AND REASONING ( ) unimpaired( ) impaired

VII. INSIGHT:
( ) unimpaired ( ) intellectual
( ) impaired ( ) true
VIII. SUMMARY OF MENTAL STATUS EXAMINATION
A. DISTURBANCE IN
( ) Presentation ( ) Neurovegetative dysfunction
( ) Stream of Talk ( ) General Sensorium and Intellectual status
( ) thought Control ( 0 Emotional state and Reaction
( ) insight
B. DIAGNOSTIC CATEGORY
( ) Functional ( ) psychotic
( ) Organic ( ) non-psychotic
C. DSM III-R DIAGNOSIS
AXIS I_______________________________________________________
AXIS II_______________________________________________________
AXIS III_______________________________________________________
AXIS IV
Psychosocial Stressors_____________________________________
Severity_________________________________________________
AXIS V
Current GAF______________________________________________
Past Year GAF_____________________________________________
________________________ ______________________ _________________
Student Resident Consultant

Holy Child College of Davao
College of Nursing
MENTAL STATUS EXAMINATION
Name of Patient:_______________________________ Date:______________________
IX. Pre-Examination
E. General Apperance:________________________________________________
F. General Mobility:___________________________________________________
1.Posture & Gait:___________________________________________________
2. Activity: ( ) normoactive ( )Psychomotor retardation
( )hyperactive ( )agitated
4. Facial Expression:_______________________________________________
G. Behavior ( ) friendly ( )impulsive ( )angry
( ) negativistic ( ) evasive ( )seductive
( )withdrawn ( )embarrassed ( )indifferent
H. Doctor- Patient Interaction
( ) cooperative ( ) uncooperative
( ) initially
( ) all throughout
Quality: ( ) warm ( ) distant ( ) dependent
( ) hostile ( ) suspicious ( ) talkative
Others:__________________________________
X. Stream Of Talk
D. Character
( ) spontaneous ( ) deliberate ( ) Pressured ( ) blocking

E. Organization
( ) relevant ( ) loose association ( ) Tangentiality
( ) Irrelevant ( ) flight of ideas ( ) neologism
( ) incorrect ( ) circumstantiality ( ) others
F. Accessibility
( ) good ( ) self absorbed ( ) defensive
( ) fair ( ) mute ( ) inaccessible
XI. EMOTIONAL STATE AND REACTIONS
E. Mood
( ) euthymic ( ) depression ( ) euphoria
F. Affect
( ) appropriate ( ) Inappropriate
Quality:
( ) flat ( ) elated ( ) Histrionic
( ) Blunted ( ) labile ( ) angry
( ) hostile ( ) anxious ( ) others_______________________
G. DEPERSONALIZATION and DEREALIZATION
( ) present ( )absent
H. SUICIDAL IDEATION
( ) present ( ) absent
XII. THOUGHT CONTROL
F. PERCEPTION
( ) present ( ) absent
G. DELUSIONS
( ) Present ( ) absent

Type:___________________________________________________________
H. IDEAS OF REFERENCE ( ) present ( ) absent
I. PREOCCUPATIONAL AND RUMINATIONS( ) present ( ) absent
J. DÉJÀ VU and JAMAIS VU ( ) present ( ) absent
XIII. NEUROVEGETATIVE DYSFUNCTION
F. SLEEP
( ) normal ( ) MNA ( ) DFA
( ) Hypersomnia ( ) EMA ( ) interrupted sleep
G. APPETITE_____________________________________________________
H. DIURAL VARIATION_____________________________________________
I. WEIGHT_____________________________
J. LIBIDO______________________________
XIV. GENERAL SENSORIUM AND INTELLECTUAL STATUS
G. ORIENTATION Time:_________ Place:________ Person:_______
Situation:______________________________________
H. MEMORY Remote:_______ Recent:________Immediate:_____
I. ATTENTION SPAN: ( ) Good ( ) Fair ( ) Poor
J. GENERAL INFORMATION___________________________________________
K. ABSTRACT THINKING ABILITY______________________________________
L. JUDGEMENT AND REASONING ( ) unimpaired( ) impaired
XV. INSIGHT:
( ) unimpaired ( ) intellectual
( ) impaired ( ) true
XVI. SUMMARY OF MENTAL STATUS EXAMINATION

D. DISTURBANCE IN
( ) Presentation ( ) Neurovegetative dysfunction
( ) Stream of Talk ( ) General Sensorium and Intellectual status
( ) thought Control ( 0 Emotional state and Reaction
( ) insight
E. DIAGNOSTIC CATEGORY
( ) Functional ( ) psychotic
( ) Organic ( ) non-psychotic
F. DSM III-R DIAGNOSIS
AXIS I_______________________________________________________
AXIS II_______________________________________________________
AXIS III_______________________________________________________
AXIS IV
Psychosocial Stressors_____________________________________
Severity_________________________________________________
AXIS V
Current GAF______________________________________________
Past Year GAF_____________________________________________
________________________ ______________________ _________________
Student Resident Consultant


Definition of Diagnosis
Paranoid Schizophrenia-
Reference:
Paranoid Schizophrenia
Reference:
Paranoid Schizophrenia
Reference:
VI. ANATOMY AND PHYSIOLOGY
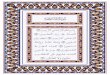
Mesolimbic pathway

Mesolimbic dopaminergic and serotonergic pathways.
The mesolimbic pathway is one of the dopaminergic pathways in the brain. The pathway
begins in the ventral tegmental area of the midbrain and connects to the limbic system via
the nucleus accumbens, the amygdala, and the hippocampus as well as to the medial prefrontal
cortex. The mesolimbic dopamine system is widely believed to be a "reward" pathway, but that
theory is not universally accepted.
Following structures are considered to be a part of the mesolimbic pathway:
Ventral Tegmental Area
The ventral tegmental area (VTA) is a part of the midbrain. It consists of
dopaminergic, GABAergic, and glutamatergic neurons.The VTA communicates with the nucleus
accumbens via the medial forebrain bundle.
Nucleus Accumbens

The nucleus accumbens is found in the ventral striatum and is composed of medium spiny
neurons It is subdivided into limbic and motor subregions known as the shell and core. [2] The
medium spiny neurons receive input from both the dopaminergic neurons of the VTA and the
glutamatergic neurons of the hippocampus, amygdala, and medial prefrontal cortex. When they
are activated by these inputs, the medium spiny neurons' projections release GABA onto
the ventral pallidum. The release of dopamine in this structure drives the mesolimbic system.
Amygdala
The amygdala is a large nuclear mass in the temporal lobe anterior to the hippocampus. It has
been associated with the assignment of emotions, especially fear and anxiety. There are two,
one in each temporal lobe, and their functions may be lateralized.
Hippocampus
The hippocampus is located in the medial portion of the temporal lobe. It is known for its
association with double memory (i.e., bothprocedural and declarative memory).
Bed Nucleus of the Stria Terminalis
Controversy over mesolimbic dopamine function
There is some controversy regarding dopamine’s role in the reward system. Three hypotheses
— hedonia, learning, and incentive salience — have been proposed as explanations
for dopamine’s function in the reward system. The hedonia hypothesis suggests
that dopamine in thenucleus accumbens acts as a 'pleasure neurotransmitter'. Historically, in
the late 1970s, it was found that some drugs of abuse involved dopamine activity, particularly in
the nucleus accumbens, to cause the "high" or euphoric state. However, not all rewards or
pleasurable things involve activation of the reward system, which may suggest that the
mesolimbic pathway may not be just a system that works merely off enjoyable things
(hedonia). Learning, on the other hand, deals with predictions of future rewards and association
formation. Studies have shown that rats that had their ventral tegmental area and nucleus
accumbens destroyed do not lose their learning capabilities, but rather lack the motivation to

work for a reward.Incentive salience (wanting) stands out as a possible role for dopamine as it
regards this molecule as being released when there is a stimulus worth working hard for, thus
making an individual work to get it. This is one of the reasons whydopamine transport has been
extensively studied in the case of ADD and ADHD. It is now widely understood that most people
suffering from some form of attention deficit disorder most likely lack dopamine stimulation. This
also explains why dopamine reuptake inhibitors and stimulants often dramatically improve
symptoms of attention disorders. In self-administration studies, animals have been trained to
give anoperant response (lever press, nose poke, wheel turn, etc.) in order to obtain either a
drug or mate. It has been shown that the animals will continue to perform the required task until
the reward is received, or fatigue sets in.
Clinical significance
Since the mesolimbic pathway is shown to be associated with feelings of reward and desire, this
pathway is heavily implicated inneurobiological theories of addiction, schizophrenia,
and depression. Drug addiction, the loss of control over drug use or the compulsive seeking and
taking of drugs despite adverse consequences, with the four major classes of abused drugs
(psychostimulants, opiates, ethanol, and nicotine) are due to increased dopamine transmission
in the limbic system-each by different mechanisms.Like drug addiction, schizophrenia and
depression have similar structural changes with dopamine transmission.
Psychodynamics

Etiology
Predisposing
Factors
Presen
t
Absent Justification Rationale
Genetics X According to our
interview no one
suffer from mental
illness in the family.
It is widely agreed that
both hereditary and
environmental play an
important factor . Because
genes can be passed
through the next
generation. (Merikangas et
al, 2002: Sulivan, Neale,
and kindler, 2000)
Maternal Factors X The mother has
adequate pre natal
care. She was not
stree and well
nourished during her
conception.
Factors such as hypoxia
and infection, or stress
and malnutrition in the
mother during fetal
development, may result
in a slight increase in the
risk of schizophrenia later
in life.
Age-27 years old He was 27 when
symptoms occur.
Schizophrenia may
developed usually in
middle adulthood.

Gender- Male Client manifested
symptoms such as
delusion,
hallucinations and a
flat affect.
Schizophrenia are
commonly affecting male
than female.
Race- asian X He is born in the
Philippines which is a
tropical country.
People diagnosed with
schizophrenia are more
likely to have been born in
winter or spring (at least in
thenorthern hemisphere),
Precipitating Factor Presen
t
Absent Justification Rationale
Substance Abuse Patient was reported
to use drugs during
his stay in Manila.
A number of drugs have
been associated with the
development of
schizophrenia,
including cannabis, cocain
e, and amphetamines.
[3] About half of those with
schizophrenia use drugs
and/or alcohol excessively
(Pocket Guide for Nurses
Lippincott and Williams 4th
edition)
Environmental Stress X Patients environment
was calm and quiet.
It is widely agreed that
environmental play an

There house is made
of light materials but
all things are fixed.
important role in triggering
illness (Merikangas et al.
2002; Sulivan, Neale, and
Kendler, 2000)
Infections X Patient was
hospitalized but
those illness that
cant trigger his
mental conditions.
A recent study shows that
exposure to influenza and
trend tend to stimulate
faulty firings of
neurotransmitters.
Trauma Patient’s uncle was
shot in front of him
causing trauma. And
pt. has delusion of
persecution.
Refers to traumatic
experiences of a person
that involves loss of
significant person.
(Psychiatric Nursing, 8th
edition)
Biological Factors
a. Endocrine
system
b. Cortisol
c. Neurotransmitt
ers
Patient has mood
problems which a
result of imbalances
in his
neurotransmitters.
The biological model
explores chemical
changes in the body
during depressed states.
Significant abnormalities
can be seen in many body
systems during depressive
illness. (Psychiatric
Nursing 8th edition)
Symptomatology

Signs and
Symptoms
Present Absen
t
Justification Rationale
Positive
Symptoms
Hallucination
Delusion
Negative
Symptoms
Blunted affect
Alogia
Anhedonia
Asociality
avolition

Schematic Tracing

Narrative:

Medical management
Actual laboratory test/ Diagnostic Test
Complete Blood Count
Patient Name: Z Ref # 11903 Date: 01/23/2012 Age:33
Physician Name: Dela Cerna Hospital Sex: M
Routine Normal Value Result Interpretation
Hemoglobin
Hematocrit
White Blood Cells
Neutrophils
Lymphocytes
Monocytes
Eosinophils
Donna P. Gallosa RMT/Ariel P. Guillermo RM Oscar P. Orageda, M.D FPSP
Medtech Pathologist
Urinalysis
Physical Normal value Result Interpretation
Color Straw
Transparency Clear

pH 5.0
Specific Gravity 1.005
ChemicalProtein Negative
Glucose Negative
Microscopic
Pus Cells 0.2/HPF
RBC 0-1/HPF
ECG Result
Buhangin Medical Clinic and Diagnostic Center January 30, 2012
Atrial Ventricular Rate: 78/min PR interval: With in Normal Range
Rhythm: Sinus QRS interval: With in Normal Range
Axis +45 Degree QTinterval: With in Normal Range
Pwave: Upright QRS Complex:With in Normal Range
ST Segment: With in Normal Range
Others:_________________________________________________________________
________________________________________________________________________
Interpretation: Normal Sinus Rhythm
Victorio C. Aguirre MD
Internal Medicine

Discharge Planning
Action/Order Rationale
Medications
Exercise
Treatment
Hygiene
Out patient
Diet
Spirituality
Sexuality

Prognosis
Criteria Poor fair Good Justification
Duration Of Illness
Onset of Illness
Predisposing/
Precipitating factor
Compliance to treatment
regimen
Age
Environment
Family Support
Total

Reference: