Embed Size (px)
Citation preview

Journal of Alzheimer’s Disease 55 (2017) 1039–1053DOI 10.3233/JAD-160701IOS Press
1039
AZD3293: Pharmacokineticand Pharmacodynamic Effectsin Healthy Subjects and Patientswith Alzheimer’s Disease
Gvido Cebersa,1, Robert C. Alexandera,2, Samantha Budd Haeberleina,3, David Hanb,Ronald Goldwaterc, Larry Ereshefskyb, Tina Olssona,3, Naidong Yea,4, Laura Rosena,5,Muir Russelld, Justine Maltbyd, Susanna Eketjalle,∗ and Alan R. Kuglera,6
aAstraZeneca, Neuroscience, Waltham, MA, USAbPAREXEL, Early Phase Clinical Unit, Glendale, CA, USAcPAREXEL, Clinical Pharmacology Research Unit, Harbor Hospital, Baltimore, MD, USAdAstraZeneca, Protein Biomarkers, Personalised Healthcare and Biomarkers, Alderley Park, UKeAstraZeneca Integrated Cardio Metabolic Centre, Cardiovascular and Metabolic Diseases,Innovative Medicines and Early Development Biotech Unit, Karolinska Institutet, Solna, Sweden
Handling Associate Editor: M. Paul Murphy
Accepted 12 September 2016
Abstract. AZD3293 (LY3314814) is a promising new potentially disease-modifying BACE1 (�-secretase) inhibitor inPhase III clinical development for the treatment of Alzheimer’s disease. Reported here are the first two Phase I studies: (1)a single ascending dose study evaluating doses of 1–750 mg with a food-effect component (n = 72), and (2) a 2-week multipleascending dose study evaluating doses of 15 or 50 mg once daily (QD) or 70 mg once weekly (QW) in elderly subjects (Part 1,n = 31), and 15, 50, or 150 mg QD in patients with mild to moderate Alzheimer’s disease (Part 2, n = 16). AZD3293 wasgenerally well tolerated up to the highest doses given. No notable food effects were observed. PK following multiple doses(Part 2) were tmax of 1 to 3 h and mean t1/2 of 16 to 21 h across the 15 to 150 mg dose range. For single doses of ≥5 mg, a ≥70%reduction was observed in mean plasma A�40 and A�42 concentrations, with prolonged suppression for up to 3 weeks at thehighest dose level studied. Following multiple doses, robust reductions in plasma (≥64% at 15 mg and ≥78% at ≥50 mg)and cerebrospinal fluid (≥51% at 15 mg and ≥76% at ≥50 mg) A� peptides were seen, including prolonged suppressioneven with a QW dosing regimen. AZD3293 is the only BACE1 inhibitor for which prolonged suppression of plasma A�with a QW dosing schedule has been reported. Two Phase III studies of AZD3293 (AMARANTH, NCT02245737; andDAYBREAK-ALZ, NCT02783573) are now ongoing.
Keywords: Amyloid-beta peptides, AZD3293, BACE1 protein-human, cerebrospinal fluid proteins, early onset Alzheimer’sdisease, pharmacodynamics, pharmacokinetics, Phase I clinical trials
Current Addresses: 1Independent Consultant, Cambridge,MA, USA. 2Pfizer Inc., Cambridge, MA, USA. 3Biogen Idec, Inc.,Cambridge, MA, USA. 4Millendo Therapeutics, Inc., Ann Arbor,MI, USA. 5Flex Pharma, Inc., Boston, MA, USA. 6Coastal PharmaGroup, Concord, MA, USA.
∗Correspondence to: Susanna Eketjall, PhD, Cardiovascularand Metabolic Diseases, Innovative Medicines and Early Devel-opment Biotech Unit, AstraZeneca, Integrated Cardio MetabolicCentre (ICMC), Karolinska Institutet, Novum, Blickargangen 6,SE-141 57 Huddinge, Sweden. Tel.: +46 553 22977; Fax: +46 831 11 01; E-mail: [email protected].
ISSN 1387-2877/17/$35.00 © 2017 – IOS Press and the authors. All rights reserved

1040 G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor
INTRODUCTION
Alzheimer’s disease and other dementias affectmore than 47 million people and their families world-wide [1], a number which is projected to reach 115million by 2050 [2]. Current treatments are palliative,offering only modest improvements in some symp-toms, and have no effect on disease progression [3,4]. Therapeutic approaches that act on the underly-ing pathophysiology of Alzheimer’s disease have thepotential to slow disease progression.
Pathological, biomarker, genetic, and mechanisticdata suggest that amyloid accumulation, as a resultof changes in production, processing, and/or clear-ance of brain amyloid-� (A�) peptides, plays a keyrole in the pathogenesis of Alzheimer’s disease [5, 6].Consequently, investigating potential disease modifi-cation through modulation of A� concentrations hasbecome one of the highest priority therapeutic targetsin Alzheimer’s disease [4, 7].
Alzheimer’s disease pathology is characterized bycerebral A� accumulation and the formation of amy-loid plaques and neurofibrillary tangles, which areassociated with inflammatory changes and neuro-transmitter loss [5, 8]. The genetics of Alzheimer’sdisease also provides compelling evidence that cere-bral A� accumulation is crucially involved in thepathogenesis of Alzheimer’s disease, with diversechanges in at least five different genes leading toincreased cerebral A� accumulation associated withfamilial Alzheimer’s disease [6, 9]. Genetic muta-tions in the amyloid-� protein precursor (A�PP)have been linked causally to familial early onsetAlzheimer’s disease [10–12], and many of thesemutations are clustered around the �- and �-secretasesites, leading to increased cleavage and production ofthe toxic A� peptide [13–15].
The formation of A� begins with the cleavageof A�PP by the �-site A�PP cleaving enzyme 1(BACE1, or �-secretase), with the soluble N terminalfragment of A�PP (sA�PP�) as a direct product [6].Inhibition of BACE1 at the first step in the process-ing of A�PP to A� peptides is therefore an attractivetarget for therapeutic intervention to stop A� produc-tion and theoretically slow disease progression [5, 9].This hypothesis is supported by studies in transgenicmouse models of Alzheimer’s disease [9, 16–19] andmost compellingly by human genetic associations.Specifically, two mutations in A�PP have been asso-ciated with changes in A�PP cleavage by BACE1.Of these, the Swedish mutation, K670N/M671L,increases A�PP susceptibility to BACE cleavage and
confers early onset Alzheimer’s disease [12], whilethe A673T A�PP variant reduces A�PP susceptibil-ity to BACE cleavage and is associated with a reducedrisk for Alzheimer’s disease in elderly individuals[20]. Based on this amyloid cascade hypothesis,reducing A� accumulation in the brain by inhibit-ing the rate-limiting BACE cleavage enzyme earlyenough in the disease process could be efficacious inAlzheimer’s disease [6].
While early studies with the first generationBACE1 inhibitors were hampered by factors includ-ing poor blood-brain barrier penetration and hERG(human ether-a-go-go related gene) activity [21–23],several second generation BACE1 inhibitors withimproved drug-like properties have now progressedinto clinical trials. Eli Lilly’s LY2811376 was thefirst to report Phase I clinical trial results but wasterminated due to the observation of cytoplasmicinclusions in the retinal epithelium in a chronictoxicology study in rats [24]. LY2886721, also byEli Lilly, was terminated in Phase II due to abnor-mal liver biochemistry [25]. Other BACE1 inhibitorscurrently in clinical development include MK-8931([26]; Merck, Phase III), E2609 ([27], Eisai/Biogen,Phase II), JNJ-54861911 ([28]; Johnson & John-son, Phase II), and CNP520 ([29]; Novartis/Amgen,Phase II) [6, 23, 29].
The novel, potent BACE1 inhibitor AZD3293(LY3314814) is a blood-brain barrier permeable,orally active compound with a slow off-rate fromits target enzyme BACE1, which robustly reducedplasma, cerebrospinal fluid (CSF), and brain A�40,A�42, and sA�PP� concentrations in vitro and in vivoin mouse, guinea pig, and dog (Table 1) [30]. Thein vitro 50% inhibitory concentrations (IC50s) ofAZD3293 for BACE1 and BACE2 are both sub-nanomolar (0.6 and 0.9 nM, respectively), and themean Caco-2 apical to basolateral Papp permeabilityis 34.8 10–6 cm/sec [30].
Here we report the favorable findings of the firstPhase I clinical trials of AZD3293 in healthy sub-jects and patients with mild to moderate Alzheimer’sdisease. AZD3293 was given as an oral solution ofthe camsylate salt with dose and concentration unitsreported as AZD3293 free base equivalents.
Objectives
To investigate the safety/tolerability, pharma-cokinetics (PK), and pharmacodynamics (PD) ofAZD3293 in two well matched and designed Phase Iplacebo-controlled trials: a single ascending dose

G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor 1041
Table 1Selected chemical and nonclinical pharmacokinetic/pharmacodynamic characteristics of AZD3293
Test/Assessment Result*
Chemical/PermeabilityChemical name (IUPAC) (1r,1′R,4R)-4-methoxy-5′′-methyl-6′-[5-(prop-1-yn-1-yl)
pyridin-3-yl]-3′H-dispiro[cyclohexane-1,2′-indene-1′,2′′-imidazol]-4′′-amine
Salt form CamsylateCaco-2 apical to basolateral Papp 34.8 10-6 cm/s
In Vitro Target Potency/Selectivity/MechanismhBACE1 (IC50) 0.6 nMhBACE2 (IC50) 0.9 nMInhibition mechanism Competitive and reversible (off-rate t1/2 = ∼9 h)
In Vivo Target Potency (IC50 for brain A�40 reduction)Mice 0.6 nM (CV 8%)Guinea Pigs 0.9 nmol/L (CV 4%)Dogs 0.8 nmol/L (CV 9%)
Nonclinical PharmacokineticsMale rats at steady state (6 months dosing)
120 mg/kg/day Cmax = 57 �mol/L, AUC = 371 �mol*h/L250 mg/kg/day Cmax = 153 �mol/L, AUC = 1920 �mol*h/L
Male Beagle dogs at steady state (9 months dosing)5 mg/kg/day Cmax = 16 �mol/L, AUC = 224 �mol*h/L20 mg/kg/day Cmax = 81 �mol/L, AUC = 1340 �mol*h/L
∗Data reprinted from Eketjall et al., 2016 [30], with permission from IOS Press. The publication is available at IOS Pressthrough http://dx.doi.org/10.3233/JAD-150834.
(SAD)/food-effect study in young and elderly healthysubjects; and a multiple ascending dose (MAD) studyin elderly healthy subjects and patients with mild tomoderate Alzheimer’s disease.
MATERIALS AND METHODS
Study design
Two Phase I, randomized, double-blind, placebo-controlled studies of AZD3293, SAD/food-effectand MAD, were conducted in healthy subjects andpatients with mild to moderate Alzheimer’s disease.An overview of the SAD/food-effect and MAD studydesigns is provided in Supplementary Figure 1. Inboth studies the primary endpoint was safety andtolerability. Secondary objectives included plasmaPK, plasma biomarkers, and PK/PD relationship inplasma. CSF samples were also collected in the MADstudy, for analysis of PK and PD biomarkers. Basedon selected findings in nonclinical studies, the MADstudy protocol was amended to collect baseline andpost-treatment skin biopsies in Part 2 of the study (seeProcedures).
The SAD/food-effect study was conducted atPAREXEL, Harbor Hospital, Baltimore, MD, USA,from December 2012 to May 2013. The MAD study
was conducted at PAREXEL, Early Phase ClinicalUnit, Glendale, CA, USA, from March 2013 to March2014. Both studies were approved by the indepen-dent Institutional Review Board, Aspire IRB, Santee,CA, USA. The studies were performed in accordancewith the Declaration of Helsinki of 1975 and Interna-tional Conference on Harmonisation/Good ClinicalPractice guidelines. All subjects provided writteninformed consent prior to enrolment into the studies.
Subjects
SAD/food-effect studyYoung (18–55 years) and elderly (55–80 years)
healthy subjects with a body weight of ≥50 to≤100 kg and a body mass index (BMI) ≥19 to≤30 kg/m2, and clinically normal findings on phys-ical examination in relation to age, as judged bythe investigator, were included in the SAD/food-effect study (NCT01739647). Exclusion criteriaincluded a history of previous or on-going psychi-atric disease/condition, neurologic disease, or use ofantipsychotic, antidepressant or anxiolytic drugs.
MAD studyElderly healthy subjects and patients with mild
to moderate Alzheimer’s disease were included in

1042 G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor
the MAD study (NCT01795339). In Part 1, elderlyhealthy subjects aged 55–80 years with a body weight≥50 to ≤100 kg and BMI ≥19 to ≤30 kg/m2 and withclinically normal findings on physical examinationin relation to age were included. Exclusion criteriaincluded a history of previous or on-going psychiatricdisease/condition or neurologic disease, a history ofany malignant disease within the past 5 years, or clin-ically significant illness, medical/surgical procedureor trauma within 4 weeks of the first administrationof investigational product. In Part 2, subjects aged55–85 years with a clinical diagnosis of probableAlzheimer’s disease according to the National Insti-tute of Neurological and Communicative Disordersand Stroke and the Alzheimer’s Disease and RelatedDisorders Association (NINCDS-ADRDA [31]) cri-teria, with manifestation of Alzheimer’s diseasesymptoms at least 6 months before randomization,and a Mini-Mental State Examination [32] scoreof 16–26 were included. Permitted treatments forAlzheimer’s disease included acetylcholinesteraseinhibitors donepezil and rivastigmine or memantine;galantamine was not allowed. Subjects had otherwiseclinically normal findings on physical examination inrelation to age, as judged by the investigator. Exclu-sion criteria included significant disease affecting theCNS other than Alzheimer’s disease, including otherdementias, other significant neurological or majorpsychiatric disease, stroke in the last 3 years, activecardiovascular disease, uncontrolled type 1 or type 2diabetes mellitus or other uncontrolled risk factors forstroke, and a history of any malignant disease withinthe past 5 years.
Procedures
SAD studyIn the SAD study, single oral doses of 1, 5, 15,
50, 150, 450, and 750 mg AZD3293 or placebo wereadministered in a fasted state through gradual esca-lation of dose in 56 young healthy subjects, and onedose of 15 mg or placebo in eight elderly healthy sub-jects. Safety was assessed before and after dosing andduring follow-up (7 to 10 days postdose) by record-ing adverse events (AEs), physical and neurologicalexaminations, Columbia-suicide severity rating scale(C-SSRS [33], Mini-International NeuropsychiatricInterview (MINI [34]), vital signs, ECG, and resultsof clinical safety laboratory tests. AEs were alsorecorded at additional follow up visits at 14–21 daysand 21–24 days after dose. For PK analysis of plasmaAZD3293 and its main metabolite AZ13569724,
blood samples were collected at predose and at reg-ular intervals postdose up to 72 h. Blood samples fordetermination of unbound AZD3293 in plasma werecollected 1.5 h postdose. In urine sampling for PK,there were six urine collection periods up to 72 hpostdose. Plasma and urine sampling collection timepoints are provided in full in Supplementary Table 1and could be modified or extra visits added depend-ing on emerging preclinical data. For plasma PDbiomarker analysis (A�40 and A�42), blood sampleswere collected predose, at regular intervals in the 72 hpostdose and at follow up visits on 7–10, 14–21, and21–24 days postdose (Supplementary Table 1).
Food-effect study
The food-effect study was a randomized, open-label, single-dose, cross-over, food-effect design atone dose level (150 mg). Healthy young subjects(n = 8) were randomized to start with a single doseof AZD3293 in fed (n = 4) or fasting (n = 4) state,and then following a washout period of at least 7days, were crossed to fasting or fed, respectively, toreceive another single dose of AZD3293. Safety wasassessed before and after dosing and during follow-up (7–10 days after dose) by recording AEs, physicaland neurological examinations, C-SSRS, vital signs,ECG, and results of clinical safety laboratory tests.Blood samples for PK analysis of plasma AZD3293and AZ13569724 were collected predose and in the72 h postdose, as described in Supplementary Table 1.
MAD study
In Part 1, healthy elderly subjects were dosed withAZD3293 15 or 50 mg or placebo once on Day 1 fol-lowed by once daily (QD) doses starting on Day 3for 12 days, or AZD3293 70 mg once weekly (QW)on Days 1, 8, and 15. Safety was assessed before andafter dosing and during follow-up (7–10 days post-dose) by recording AEs, physical and neurologicalexaminations, C-SSRS, vital signs, ECG, and resultsof clinical safety laboratory tests.
In Part 1, QD and QW dosing, PK blood andurine sampling for determination of AZD3293 andAZ13569724 were each conducted at multiple timepoints as detailed in Supplementary Table 1. Bloodsampling for PD (A�40 and A�42) and investigative(sA�PP� and sA�PP�) biomarker analysis was per-formed predose, postdose during treatment and onfollow-up visits with QD and QW dosing (Supple-mentary Table 1). Serial CSF samples were collected

G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor 1043
by lumbar puncture for PK and biomarker analysiswith QD and QW dosing of AZD3293 at multipletime points (Supplementary Table 1). Dosing and allother procedures for the QD and QW dosing patientswere identical, with the subgroups differing only withrespect to the timing of lumbar punctures and the finalPK/PD samples.
In Part 2, which was conducted after Part 1, patientswith mild to moderate Alzheimer’s disease received15, 50, or 150 mg AZD3293 or placebo once on Day1 followed by once daily for 12 days. In Part 2,the assessments and study duration were similar toPart 1. Safety was assessed before and after dos-ing and during follow-up (7–10 days postdose) byrecording AEs, physical and neurological examina-tions, C-SSRS, vital signs, ECG, eye examinationsperformed by an ophthalmologist, and results of clin-ical safety laboratory tests. The time points whenblood samples were collected for PK analysis ofplasma AZD3293 and plasma PD biomarkers (A�40and A�42), and CSF sampling was performed forAZD3293 PK and PD biomarkers (A�40 and A�42)are detailed in Supplementary Table 1. In addition,skin biopsies were taken from patients in Part 2 ofthe MAD study on Day –1 (predose) and Day 15(after last day of multiple dosing) to microscopicallyassess any effects on skin pigmentation.
Sample handling and analysis
Similar methods of sample collection and analysiswere used in the SAD/food-effect and MAD studies.These methods are explained in detail in the Supple-mentary Material.
Statistical analysis
Similar approaches to statistical analysis were usedin the SAD/food-effect and MAD studies. The anal-ysis of data was based on different subsets accordingto the purpose of analysis. All randomized subjectswho received at least 1 dose of AZD3293 or placebo,and for whom any postdose data were available wereincluded in the safety analysis set. The PK andbiomarker analyses used an as-treated approach, withthe analysis sets based on all subjects for whom PKor biomarker data, respectively, were available.
In the SAD study, the two age groups wereanalyzed separately. Similarly, in the MAD study,healthy subjects and Alzheimer’s disease patientswere analyzed separately. However, data from bothgroups were included in the PK/PD analysis where
the disease status (healthy subject/Alzheimer’s dis-ease patient) was considered as a covariate. Noformal statistical hypothesis testing was performed.Safety, tolerability, PK, and PD data were summa-rized descriptively.
Due to the investigative nature of the studies,sample size was not based on formal statistical con-siderations. The sample size for each study was basedon experience from previous similar Phase 1 studieswith other compounds to obtain adequate safety, tol-erability, and PK data to achieve the objectives of thestudy whilst exposing as few subjects as possible tostudy medication and procedures.
RESULTS
Patients
SAD/food-effect studyIn total, 72 subjects were randomized into the first
Phase I trial at one study site. Of these, 64 subjectswere randomized into the SAD part of the study and61 completed that study; one subject each from theplacebo and 50 mg dose groups was lost to followup, and one subject in the 450 mg dose group with-drew consent. Eight subjects were randomized intothe food-effect part of the study, of which six sub-jects received treatment as planned in two periods;two subjects discontinued from the food-effect study,one discontinued due to an AE and one discontinueddue to severe non-compliance.
In the SAD study, the mean age was between 32.5and 42.3 years in the young subjects, and between61.0 and 66.2 years in the elderly subjects; the major-ity of subjects were male (58/64), and Black orAfrican American (41/64) or White (22/64). In thefood-effect study, all subjects were males, and White(5/8) or Black or African American (3/8). Overall, thetreatment groups were well balanced and comparablewith regards to demographic characteristics. Demo-graphic and baseline characteristics are summarizedby treatment group in Table 2.
MAD studyIn total, 47 subjects were randomized into the
MAD study at one study site. Of these, 31 healthyelderly subjects were randomized into Part 1 and 16patients with mild to moderate Alzheimer’s diseasewere randomized into Part 2.
In Part 1, there were more male (19/31) than female(12/31) subjects; mean ages across all groups weresimilar, ranging from 61.2 years in the 15 mg dose

1044 G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor
group to 66.0 years in the 70 mg dose group. In Part 2,there were more female (11/16) than male (5/16)patients; mean ages across all groups were similar,ranging from 60.8 years in the 150 mg group to 66.0years in the 15 mg group.
Demographic and baseline characteristics werewell matched across the different treatment sub-groups of the MAD study and are summarized inTable 3.
Safety
SAD/food-effect studyNo safety and tolerability concerns were identi-
fied in the SAD/food-effect study up to the highest
AZD3293 dose given (750 mg). There were no deathsor other serious adverse events (SAEs), and all AEswere resolved at the end of the study. Across alldose groups, the types and frequencies of AEs werecomparable. In the SAD study, the most frequentlyreported AEs were upper respiratory tract infection(3 subjects [9.7%] treated with placebo) and contactdermatitis (1 subject receiving placebo, 2 receivingAZD3293), both of which were considered unrelatedto treatment in all cases (contact dermatitis consid-ered secondary to use of ECG lead in two cases).Dizziness/dizziness postural was reported by threesubjects, and was considered unrelated to treatmentin two cases. In the food-effect study, there were threeAEs reported, each by one subject (14.3%), dizziness,
Table 2Demographic and baseline characteristics of healthy subjects in the SAD/food-effect study of AZD3293 (Safety population)
SAD Food-effect study
150 mg 150 mgPlacebo 1 mg 5 mg 15 mg 50 mg 150 mg 450 mg 750 mg Placebo 15 mg Fed:Fasted Fasted:Fed(n = 14) (n = 6) (n = 6) (n = 6) (n = 6) (n = 6) (n = 6) (n = 6) (n = 2) (n = 6) (n = 4) (n = 4)Young Young Young Young Young Young Young Young Elderly Elderly Young Young
Gender, n (%)Female 0 0 1 (16.7) 1 (16.7) 0 0 0 0 2 (100) 2 (33.3) 0 0Male 14 (100) 6 (100) 5 (83.3) 5 (83.3) 6 (100) 6 (100) 6 (100) 6 (100) 0 4 (66.7) 4 (100) 4 (100)
Age (years), n 14 6 6 6 6 6 6 6 2 6 4 4Mean 39.8 39.3 41.0 42.0 39.2 33.8 32.5 42.3 61.0 66.2 42.5 36.8SD 10.4 12.4 10.2 7.1 11.1 7.3 9.3 10.4 1.4 6.0 1.0 6.9
BMI (kg/m2), n 14 6 6 6 6 6 6 6 2 6 4 4Mean 26.7 25.9 26.5 26.1 25.6 27.2 25.4 27.5 24.3 27.3 27.8 24.5
Race, n (%)White 4 (28.6) 3 (50) 2 (33.3) 3 (50) 0 (0) 1 (16.7) 2 (33.3) 2 (33.3) 2 (100) 3 (50) 2 (50) 3 (75)Black or African American 9 (64.3) 3 (50) 4 (66.7) 3 (50) 6 (100) 5 (83.3) 4 (66.7) 4 (66.7) 0 3 (50) 2 (50) 1 (25)Asian 1 (7.1) 0 0 0 0 0 0 0 0 0 0 0
Ethnicity, n (%)Hispanic or Latino 3 (21.4) 0 0 1 (16.7) 0 1 (16.7) 1 (16.7) 1 (16.7) 1 (50) 0 1 (25) 0Not applicable or Other 11 (78.6) 6 (100) 6 (100) 5 (83.3) 6 (100) 5 (83.3) 5 (83.3) 5 (83.3) 1 (50) 6 (100) 3 (75) 4 (100)
BMI, body mass index; SAD, single ascending dose; SD, standard deviation.
Table 3Demographic and baseline characteristics in the MAD study of AZD3293 (Safety population)
Healthy elderly subjects Patients with mild to moderate Alzheimer’s disease
Placebo 15 mg 50 mg 70 mg Placebo 15 mg 50 mg 150 mg(n = 7) (n = 6) (n = 6) (n = 12) (n = 4) (n = 4) (n = 4) (n = 4)
Gender, n (%)Female 3 (42.9) 3 (50) 2 (33.3) 4 (33.3) 3 (75) 2 (50) 4 (100) 2 (50)Male 4 (57.1) 3 (50) 4 (66.7) 8 (66.7) 1 (25) 2 (50) 0 2 (50)
Age (years), n 7 6 6 12Mean 63.6 61.2 62.3 66.0 64.0 66.0 64.8 60.8SD 5.4 4.9 7.0 5.1 6.2 8.1 3.9 4.5
BMI (kg/m2), n 7 6 6 12Mean 25.4 26.6 23.8 24.7 26.1 23.8 27.9 25.3
Race, n (%)White 3 (42.9) 1 (16.7) 4 (66.7) 2 (16.7) 3 (75) 2 (50) 1 (25) 1 (25)Black or African American 1 (14.3) 4 (66.7) 0 1 (8.3) 0 0 1 (25) 0Asian 3 (42.9) 1 (16.7) 2 (33.3) 9 (75) 1 (25) 2 (50) 2 (50) 2 (50)Native Hawaiian or other Pacific Islander 0 0 0 0 0 0 0 1 (25)
Ethnicity, n (%)Hispanic or Latino 2 (28.6) 0 2 (33.3) 1 (8.3) 1 (25) 1 (25) 1 (25) 1 (25)Not Hispanic or Latino 5 (71.4) 6 (100) 4 (66.7) 11 (91.7) 3 (75) 3 (75) 3 (75) 3 (75)
BMI, body mass index; MAD, multiple ascending dose; SD, standard deviation.

G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor 1045
contact dermatitis, and rash. The subject with rashhad AZD3293 treatment discontinued owing to theAE; the AE was considered mild in intensity andrelated to study drug. AEs assessed as related to studymedication are shown in Supplementary Table 2.
There were no clinically meaningful findings in theclinical laboratory data, vital signs, or ECG results inthe SAD/food-effect study.
MAD studyIn Part 1 of the study (healthy elderly subjects),
there were no SAEs, or treatment discontinuationsdue to AEs. Treatment-related AEs were reported forsubjects taking placebo and across all dose groups;no trend with dose was apparent in the types and fre-quencies of AEs. AEs assessed as related to studymedication are shown in Table 4.
The majority of treatment-related AEs were mild.Two treatment-related AEs of moderate intensitywere reported: headache (1 subject [8.3%] in the70 mg dose group); and orthostatic hypotension (1subject [33.3%] in the placebo group). All treatment-related AEs were resolved at the end of the study.There were no clinically meaningful findings in theclinical laboratory data (including measures of liverfunction), vital signs, or ECG results.
In Part 2 of the study (patients with Alzheimer’sdisease), there were no treatment discontinuationsdue to AEs. One SAE was reported following comple-tion of dosing (ventricular tachycardia), which wasjudged to be due to a previously unreported sporadicprior condition and unrelated to study drug adminis-tration. Three patients experienced treatment-relatedAEs of orthostatic hypotension (Table 4); all weretransient in nature and resolved without treatment.No other treatment-related AEs associated with vitalsigns data and no trends were identified that couldbe attributed to treatment. There were no clinicallymeaningful findings in the clinical laboratory data,including measures of liver function; physical exam-inations; eye examinations, including visual acuityand retinal assessments; or ECG results. There wasalso no evidence of any drug-related effects onmelanin content or melanocyte appearance in skinbiopsies performed on Day 15 in patients participat-ing in Part 2 of the study.
Pharmacokinetics
SAD studyAfter a single oral dose in young and healthy
elderly subjects, plasma AZD3293 mean Cmax
Table 4Summary of adverse events assessed as related to study medication by the investigator in the MAD study of AZD3293 (Safety population)
Healthy elderly subjects Patients with mild to moderate Alzheimer’s diseaseSystem organ class, n (%) Placebo 15 mg 50 mg 70 mg Placebo 15 mg 50 mg 150 mgPreferred term, n (%) (n = 7) (n = 6) (n = 6) (n = 12) (n = 4) (n = 4) (n = 4) (n = 4)
Cardiac disorders 0 0 1 (16.7) 0 0 0 0 0Palpitations 0 0 1 (16.7) 0 0 0 0 0
Eye disorders 0 0 0 1 (8.3) 1 (25) 0 1 (25) 1 (25)Dry eye 0 0 0 0 0 0 1 (25) 0Foreign body sensation in eyes 0 0 0 1 (8.3) 0 0 0 0Vision blurred 0 0 0 0 1 (25) 0 1 (25) 1 (25)
Gastrointestinal disorders 1 (14.3) 0 0 2 (16.7) 0 0 0 0Abdominal distension 0 0 0 1 (8.3) 0 0 0 0Constipation 0 0 0 1 (8.3) 0 0 0 0Dyspepsia 1 (14.3) 0 0 0 0 0 0 0Flatulence 0 0 0 1 (8.3) 0 0 0 0
Musculoskeletal and connective tissue disorders 0 0 1 (16.7) 0 0 0 0 0Myalgia 0 0 1 (16.7) 0 0 0 0 0
Nervous system disorders 1 (14.3) 2 (33.3) 0 2 (16.7) 0 0 0 1 (25)Dizziness 0 0 0 1 (8.3) 0 0 0 0Headache 1 (14.3) 2 (33.3) 0 1 (8.3) 0 0 0 1 (25)
Renal and urinary disorders 1 (14.3) 1 (16.7) 0 1 (8.3) 0 0 0 0Dysuria 0 1 (16.7) 0 1 (8.3) 0 0 0 0Micturition urgency 1 (14.3) 0 0 0 0 0 0 0
Vascular disorders 3 (42.9) 1 (16.7) 0 3 (25) 0 0 0 0Flushing 1 (14.3) 0 0 0 0 0 1 (25) 2 (50)Hot flush 1 (14.3) 1 (16.7) 0 0 0 0 0 0Orthostatic hypotension 2 (28.6) 0 0 3 (25) 0 0 1 (25) 2 (50)
MAD, multiple ascending dose.

1046 G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor
increased from 1.74 ng/mL (1 mg dose) to5520 ng/mL (750 mg dose). The median tmaxfor the 5 mg to 750 mg dose levels ranged from1.1 to 2.5 h. AZD3293 AUC(0-t) values increasedfrom 26.0 h·ng/mL (1 mg dose) to 66500 h·ng/mL(750 mg dose). The mean effective half-life (t1/2)was 11 to 20 h in the young dose groups and24 h in the elderly dose group. Mean total plasmaAZD3293 concentration-time profiles are shown inSupplementary Figure 2.
Mean renal clearance was similar at approxi-mately 1.40 L/h following a single oral dose of 15 mgAZD3293 in young and elderly subjects (see Supple-mentary Material for a description of AZD3293 urinePK).
Plasma AZ13569724 concentration-time profilesand urinary AZ13569724 excretion varied similarlywith respect to both AZD3293 dose and time post-dose but at lower levels to parent AZD3293 (seeSupplementary Material for information).
Food-effect studyIn the food-effect study, statistical assessment of
the effect of food on single doses of 150 mg (fedor fasted) on AZD3293 exposure showed a mod-est decrease in peak exposure (Cmax), but no effecton overall exposure (AUC) (see SupplementaryFigure 3).
MAD studyFollowing multiple dose administration only lim-
ited plasma AZD3293 accumulation was observed(1.5 fold for Cmax) in healthy elderly subjects (Part 1).A summary of plasma AZD3293 PK parameters onDay 10 and Day 14 of once daily administration isprovided in Table 5. Maximum CSF AZD3293 con-centrations were reached at 3 to 4 h.
No accumulation was observed following multipleweekly doses of AZD3293 based upon Cmax-Cminvalues, but a modest increase in AUC was seenbetween the first and third weekly dose. PK param-eters on Day 15 of QW administration are shown inTable 5.
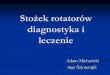
Mean total plasma AZD3293 concentration-timeprofiles on Day 1 and Day 14 are shown in Fig. 1(A, B). In the 50 mg dose group, maximum plasmaAZD3293 concentrations occurred with a mediantmax of 1.5 h on Day 1 and 1.0 h on Day 14. Geo-metric mean AZD3293 AUCtau (AUC0-24 for Day 1)for the 50 mg dose group was 1720 h·ng/mL (range1190–2450 h·ng/mL) for Day 1 and 2820 h·ng/mL
(range 2020–4350 h·ng/mL) for Day 14. Geometricmean t1/2 for the 50 mg dose group was 13.1 h (range10.3–18.3 h) on Day 1 and 14.9 h (11.7–21.6 h) onDay 14.
In patients with Alzheimer’s disease (Part 2),plasma AZD3293 multiple dose PK were compara-ble with those observed in healthy subjects (Table 5).Mean total plasma AZD3293 concentration-time pro-files on Day 1 and Day 14 are shown in Fig. 1(C, D). Maximal plasma AZD3293 concentrationswere achieved at 1 to 3 h and mean t1/2 was 16 to 21 hacross the three doses studied (15, 50, or 150 mg).
Across all dose levels studied, in healthysubjects and patients with Alzheimer’s disease,CSF AZD3293 concentrations were much lower(measured predose on Day 14) compared withplasma AZD3293 concentrations. PK findings forAZ13569724 mirrored those of AZD3293 withincreasing exposure with increasing dose (data notshown).
Pharmacodynamics: Effects on Plasma and CSFAβ Peptides
SAD studyFollowing single doses of AZD3293, both A�40
and A�42 showed robust and dose-dependent reduc-tions. For single doses of 5 mg and above, a ≥70%reduction was observed in mean plasma A�40 andA�42 concentrations over time. Maximum plasmaA�40 suppression was reached at 6 h postdose fornearly all doses of AZD3293, for both young andelderly subjects. Maximum A�42 suppression wasreached within 2 h postdose for nearly all dosesof AZD3293, for both young and elderly subjects.A floor effect was observed with respect to manyplasma biomarker results for the AZD3293 dosegroups, with concentrations being below the lowerlimit of quantitation (LLOQ; threshold values pro-vided in the Supplementary Material). Sustainedsuppression of plasma A�40 and A�42 was observedfor approximately 6 days (147 h) postdose for the450 mg dose and for up to 3 weeks (504 h) postdosefor the 750 mg dose, for both biomarkers. PlasmaA�40 and A�42 suppression was not observed forplacebo subjects.
MAD studyIn Part 1 (healthy elderly subjects), plasma and
CSF A� peptides showed robust reductions follow-ing multiple doses of AZD3293 (15, 50, and 70 mg),

G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor 1047
Table 5Summary of plasma AZD3293 pharmacokinetic parameters, multiple dose, in the MAD study of AZD3293 (PK analysis population)
Healthy elderly subjects Patients with mild to moderate Alzheimer’s disease
Parameter (units) 15 mg (n = 6) 50 mg (n = 6) 70 mg (n = 12) 15 mg (n = 4) 50 mg (n = 4) 150 mg (n = 4)
Day 10 Day 14 Day 10 Day 14 Day 15 Day 10 Day 14 Day 10 Day 14 Day 10 Day 14
Cmax,ss
Geo Mean 65.2 77.1 263 314 415 56.3 67.4 322 361 1460 1520(GCV %) (39.3) (41.7) (44.1) (36.8) (40.1) (50.9) (30.4) (26.7) (22.6) (40.6) (36.2)
Tmax,ss
Median 2.00 2.00 2.00 1.00 1.00 3.00 1.07 2.00 1.50 1.00 1.00(range) (1.00, 4.00) (1.00, 4.00) (1.00, 2.00) (0.50, 2.00) (0.50, 2.03) (1.00, 4.00) (1.00, 2.00) (1.00, 4.00) (1.00, 2.00) (1.00, 1.00) (1.00,2.00)
AUCtau,ss (h·ng/mL)Geo Mean 759 870 2380 2820 4850 674 728 3480 3960 13200 13900(GCV %) (46.8) (37.3) (38.2) (32.5) (21.5) (61.9) (52.1) (36.0) (30.5) (47.7) (43.7)
Cmin,ss (ng/mL)Geo Mean 15.6 18.2 32.1 41.7 0.703 13.2 12.9 65.1 68.8 221 212Mean (GCV %) (54.3) (38.4) (56.0) (35.3) (20.6) (97.6) (93.6) (52.0) (46.4) (80.0) (49.3)
t1/2 (h)Geo Mean 14.4 18.6 10.7 14.9 17.9 14.4 20.6 13.8 17.4 11.2 16.4Mean (GCV %) (7.7) (17.8) (30.5) (24.8) (26.5) (47.7) (17.8) (21.7) (23.3) (19.6) (28.4)
CLss/F (L/h)Geo Mean 19.8 17.2 21.0 17.7 14.4 NA 20.6 NA 12.3 NA 10.8(GCV %) (46.8) (37.3) (38.2) (32.5) (21.5) (52.1) (30.5) (43.7)
Vzss/F (L)Geo Mean 411 464 326 383 373 NA 614 NA 317 NA 255(GCV %) (46.0) (30.4) (52.7) (44.4) (37.2) (41.1) (21.9) (52.9)
Cavg,ss (ng/mL)Geo Mean 31.6 36.2 99.1 117 28.9 28.1 30.3 145 165 551 581(GCV %) (46.8) (37.3) (38.2) (32.5) (21.5) (61.9) (52.1) (36.0) (30.5) (47.7) (43.7)
AUCtau,ss, area under the plasma drug concentration-time curve (AUC) during the dosing interval tau after multiple dose oral administration;Cavg,ss, average plasma drug concentration after multiple dose oral administration; CLss/F, apparent total plasma clearance after multipledose oral administration; Cmax,ss, maximum plasma drug concentration after multiple dose oral administration; Cmin,ss, minimum plasmadrug concentration after multiple dose oral administration; GCV, geometric coefficient of variation; geo mean, geometric mean; NA, notapplicable; PK, pharmacokinetic; SD, standard deviation; t1/2, terminal elimination half life; Tmax,ss, time of maximum drug concentrationafter multiple dose oral administration; Vzss/F, apparent volume of distribution during terminal elimination phase after multiple dose oraladministration.
compared with placebo, which did not recoverduring the sampling period (Fig. 2A–D, showing 15and 50 mg QD data). Similarly in Part 2 (patientswith Alzheimer’s disease), robust plasma and CSFA� peptide reduction was observed at all doses testedcompared to placebo following single and multiple-dose administration (Fig. 2 E–G).
Mean percent change from baseline concentrationsfor plasma and CSF A�40 and A�42 in Parts 1 (dailyand weekly dosing in healthy elderly subjects) and 2(daily dosing in patients with Alzheimer’s disease) ofthe study are presented in Table 6. Here again, plasmabiomarker results for the AZD3293 dose groups fellbelow the LLOQ, suggesting that if biomarker con-centrations could have been determined by moresensitive methods, the mean percent reductionswould have been higher than the values reported.
Pharmacodynamics: Effects on CSFAmyloid-Related Investigative Biomarkers
MAD studyIn Part 1, a dose-dependent sustained decrease in
CSF sA�PP� and broadly dose-dependent increasein CSF sA�PP� was observed with AZD3293 QDdosing (see Supplementary Figure 4). Similarly,a sustained decrease in CSF sA�PP� and increasein CSF sA�PP� were observed with AZD3293when dosed at 70 mg QW (Supplementary Figure 4).Preliminary PK/PD analysis indicated a correlationbetween steady state average CSF AZD3293 con-centrations (for 15 and 50 mg groups) at Day 14 andsuppression of sA�PP� and A�42 (Fig. 3).
Plasma amyloid-related biomarkers are brieflydescribed in the Supplementary Material.

1048 G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor
Fig. 1. Mean total plasma AZD3293 concentration-time profiles at Day 1 and Day 14 following multiple doses of AZD3293 (linear scale):(A, B) in healthy elderly subjects and (C, D) in patients with Alzheimer’s disease.
DISCUSSION
Here we report favorable findings of the first-in-human studies of the potent BACE1 inhibitorAZD3293 involving 103 healthy young and elderlysubjects and 16 patients with mild to moderateAlzheimer’s disease. No safety and tolerability con-cerns were identified up to the highest doses given,which were a single dose of up to 750 mg or multipledaily doses of up to 150 mg for 2 weeks. AZD3293produced prolonged suppression of plasma and CSFA� peptides in healthy subjects as well as inpatients with Alzheimer’s disease, confirming thecentral target engagement and expected mode ofaction of the drug. These observations support thepotential of AZD3293 to alter the pathogenesis ofAlzheimer’s disease in ways that could slow diseaseprogression.
Importantly, no safety issues of special inter-est were identified with AZD3293. No clinicallymeaningful elevation of liver enzymes was noted inhealthy volunteers or patients with Alzheimer’s dis-ease. This is in contrast to LY2886721, which wasvoluntarily withdrawn from clinical development atPhase II owing to liver biochemistry abnormalitiesin a small number of subjects, through a mechanismthat appeared to be unrelated to BACE1 inhibition[25]. Clinical development of other small moleculeBACE1 inhibitors was discontinued early on, includ-ing AZD3839 (AstraZeneca), BI1181181/VTP-37948 (Boehringer/Vitae), HPP854 (High Point),PF-05297909 (Pfizer), and RG7129 (Roche), becauseof a sub-optimal PK profiles, skin reactions, and forundisclosed reasons [6, 29, 35–38].
The plasma half-life of AZD3293 was 11–24 h inthe SAD study, suggesting that a single daily dose

G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor 1049
Fig.
2.M
ean
(±SE
M)
perc
ent
chan
gefr
omba
selin
efo
llow
ing
mul
tiple
dose
sof
AZ
D32
93fo
r:pl
asm
a(A
)A
�40
and
(B)
A�
42an
dC
SFD
ay14
(C)
A�
40an
d(D
)A
�42
inhe
alth
yel
derl
ysu
bjec
ts;a
ndpl
asm
aD
ays
14–1
6(E
)A
�40
and
(F)
A�
42an
d(G
)C
SFD
ay14
A�
pept
ides
inpa
tient
sw
ithA
lzhe
imer
’sdi
seas
e(n
=4
per
dose
).

1050 G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor
Table 6Mean percent change from baseline concentrations for plasma and CSF pharmacodynamic biomarkers (Biomarker population)
Healthy elderly subjects Patients with mild to moderate Alzheimer’s disease
Biomarker Placebo 15 mg 50 mg Placebo 70 mg Placebo 15 mg 50 mg 150 mg(QD, n = 4) (QD, n = 6) (QD, n = 6) (QW, n = 3) (QW, n = 12) (QD, n = 4) (QD, n = 4) (QD, n = 4) (QD, n = 4)
Plasma A�40
Mean (SD), % 21.6 (41.7) –75.3 (5.4) –78.4 (3.5) 15.9 (12.9) –71.5 (10.2) –16.9 (2.4) –74.9 (10.4) –78.7 (3.9) –78.3 (5.9)Timepoint Day 14 Day 14 Day 14 Day 15 Day 15 Day 14 Day 14 Day 14 Day 14
Plasma A�42
Mean (SD), % 25.0 (7.8) –64.3 (25.8)∗ –80.1 (2.8) –10.1 (5.6) –69.0 (26.5) –7.4 (7.0) –77.1 (4.0) –78.1 (6.1) –77.9 (2.4)Timepoint Day 14 Day 14 Day 14 Day 15 Day 15 Day 14 Day 14 Day 14 Day 14
CSF A�40
Mean (SD), % 62.9 (55.1) –51.8 (10.6) –78.0 (5.4) 29.5 (NA) –48.5 (9.6) 0.0 (11.9) –51.1 (11.5) –75.6 (5.9) –89.7 (3.2)Timepoint Day 14 Day 14 Day 14 Day 20 Day 18 Day 14 Day 14 Day 14 Day 14
CSF A�42
Mean (SD), % 39.5 (42.2) –55.2 (8.7) –79.3 (8.8) –18.0 (NA) –52.9 (14.0) 6.3 (15.4) –52.1 (17.8) –75.7 (5.2) –89.8 (2.5)Timepoint Day 14 Day 14 Day 14 Day 20 Day 18 Day 14 Day 14 Day 14 Day 14
A�, amyloid-�; SD, standard deviation; QD, once daily; QW, once weekly. ∗n = 5.
Fig. 3. CSF sA�PP�, sA�PP�, and A�42 percent change frombaseline versus average CSF AZD3293 concentration on Day 14at steady state (Cavg,ss) following 15 and 50 mg AZD3293 dailydosing (mean ± SEM), in healthy elderly subjects.
would provide sufficient drug concentrations in vivo.PK results were similar in young and elderly healthysubjects. Food consumption led to a modest reductionin Cmax and a minimal effect on AUC. PK/PD model-ing of the Phase I data suggests that any effects of foodon AZD3293 exposure would not impact on safety orCSF A� reductions, and therefore that AZD3293 canbe taken with or without food. In the MAD study,similar PK findings were also observed in healthyelderly subjects and patients with Alzheimer’s dis-ease, with tmax of 1.1 to 2.5 h and mean t1/2 of 16 to21 h across the 15 to 150 mg dose range in patientswith Alzheimer’s disease. AZD3293 appears to havea uniquely slow off-rate from BACE1 (t1/2 ∼9 h) asobserved in in vitro studies. It was suggested that theprolonged reduction of A� peptide concentrationswas driven not only by the AZD3293 plasma/brainexposure but also the turnover rate of the BACE1enzyme [30].
Indeed, an interesting observation of the presentstudy was the prolonged suppression of plasma A�peptides by a single dose of AZD3293, for up to3 weeks at the highest dose level studied. SomePhase I studies involving other BACE inhibitors inhealthy subjects have also described sustained reduc-tions in plasma A� that extend beyond the plasmapresence of these compounds, from moderate reduc-tions at around 72–144 h postdose with E2609 andLY2811376 [24, 27] to up to 95% reduction after14 days following a single dose of JNJ-54861911[28]. The sustained effects of AZD3293 on A� ledto the inclusion of QW 70 mg dose groups in theMAD study. Here, results similar to QD dosing atthe 15 mg dose level (for mean change from baselineat Day 14) were seen for the reduction in A� pep-tides compared with placebo. At this time, AZD3293is the only BACE1 inhibitor to have reported pro-longed suppression of plasma A� with a QW dosingschedule.
Similar to effects in plasma, reductions in CSF A�peptides were seen in subjects treated with AZD3293in the MAD study, which further confirmed theexpected mode of action of the drug. In healthyelderly subjects, maximum CSF reductions were seenat the 50 mg dose level, of –78% and –79% for A�40and A�42, respectively, both measured predose onDay 14. Similar CSF reductions in A�40 and A�42(–76% for both) were seen at the 50 mg dose level atthe same time point in patients with Alzheimer’s dis-ease, confirming that PD findings in healthy elderlysubjects translate well into patients with Alzheimer’sdisease. Similar results have also been observed withanother BACE1 inhibitor, MK-8931, which producedsustained mean reductions from baseline in CSFA�40, A�42, and sA�PP� concentrations (up to –84,

G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor 1051
–81, and –88%, respectively) in patients with mildto moderate Alzheimer’s disease [26]. In the MADstudy, reductions in CSF A� peptides were similarbetween AZD3293 15 mg QD and 70 mg QW treat-ment groups (for mean change from baseline at Day14 and Day 18, respectively). Suppression of CSFA� peptides by approximately 50% up to 3 days afterthe last 70 mg QW dose of AZD3293 suggests thata QW dosing regimen may warrant further investi-gation. One could assume that with a daily dosingregimen in cognitively impaired patients, a benefit ofthe prolonged PD effects of AZD3293 would meanthat a single or even several unintentionally misseddoses would have little effect on maintaining steadysuppression of A� concentrations in the brain. Thepossible reason for this prolonged PD effect is theslow off-rate of AZD3293 from the BACE1 enzymediscussed above.
Dose dependent reduction in CSF sA�PP� withAZD3293, an exploratory finding of the presentstudy, provides direct evidence of BACE1 inhibi-tion in the human CNS. In preclinical modeling,the maximum effect of AZD3293 on sA�PP� wasobserved after that on A�40/A�42 [30]. Prelimi-nary PK/PD evaluation in the present study indicateda correlation to Cavg,ss with sA�PP� and A�42,which suggests that measures of amyloid metabolismother than A�42 and A�40 may have significant util-ity in determining PK/PD relationships in BACE1inhibition. These observations are consistent withthe hypothesized mechanism of action of AZD3293and indicate that sustained inhibition of BACE1leads to reduced sA�PP� and A�42 concentrationsand increased flux through the non-pathogenic �-secretase-mediated pathway (sA�PP�). Increasedbrain [39] and CSF [25] sA�PP�, suggestive ofenhanced non-amyloidogenic processing of A�PP,have been observed as a result of BACE1 inhibitionin a preclinical and clinical study, respectively.
In addition to BACE1 inhibitors, studies ofA�-specific therapeutic antibodies have providedevidence to support the therapeutic potential ofA�-directed treatment in Alzheimer’s disease. Mostnotable is the recent delayed-start analysis of pooleddata from the solanezumab EXPEDITION program[40]. The original, Phase III studies (EXPEDITION1 & 2) of solanezumab, in patients with mild tomoderate Alzheimer’s disease, did not reach theirprimary endpoint [41]. However, delayed-start anal-ysis of the pooled data from the entire EXPEDITIONprogram (including data from the open-label exten-sion study EXPEDITION-EXT), which focused on
patients who were defined as ‘mild’ before the startof the placebo-controlled period, provided evidenceto support the A� hypothesis. The pooled analysesshowed that treatment differences at 108 weeks afterrandomization between early-start and delayed-startgroups in both cognition and function were simi-lar to the between-group differences at the end ofthe placebo-controlled period, i.e., the delayed-startgroup did not “catch up”. This difference remainedthrough 132 weeks and suggests a disease-modifyingeffect of A� reduction [40].
Recent evidence in mouse models treated withBACE1 inhibitors with distinct differences in dis-position in periphery and brain adds support to thehypothesis that reduction of A� via BACE1 inhibitionneeds to be carried out in the brain, arguing againstthe peripheral sink hypothesis [4] where reduced A�load in the brain might be achieved through lower-ing of A� peptides in peripheral organs [42]. Animalstudies of AZD3293 confirm that dose- and time-dependent reductions in plasma and CSF A�40, A�42concentrations are also seen in brain tissue [30]. Sim-ilarly, Eli Lilly’s BACE1 inhibitors LY2811376 andLY2886721 also significantly reduced concentrationsof A� and sA�PP� in the PDABPP mouse brain [24,25].
The two successive first-in-man Phase I studiesdescribed here were rationally designed to allow rapidinvestigation of the novel BACE1 inhibitor AZD3293in healthy young and elderly subjects and patientswith mild to moderate Alzheimer’s disease, and theidentification of appropriate doses to be taken for-ward into future trials. The efficiency of the designis highlighted by the speed of the studies, whichtook <16 months from the first subject enrolled intothe SAD study to the last subject visit of the MADstudy. Consequently, AZD3293 has advanced in clin-ical development and is now being evaluated in twoPhase III studies (AMARANTH, NCT02245737; andDAYBREAK-ALZ, NCT02783573). These multi-center, randomized, double-blind, placebo-controlledstudies are testing the disease-modifying potentialof AZD3293 at daily doses 20 or 50 mg for 18 to24 months, in over 4,000 patients with mild cogni-tive impairment due to Alzheimer’s disease and mildAlzheimer’s disease.
CONCLUSION
The BACE1 inhibitor AZD3293 is a promis-ing new potentially disease-modifying treatment for

1052 G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor
Alzheimer’s disease with a uniquely slow off-rateon its enzyme target. AZD3293 provided potentand sustained inhibition of BACE1 and producedprolonged suppression of plasma and CSF A� pep-tides in healthy subjects and patients with mildto moderate Alzheimer’s disease. AZD3293 is theonly BACE1 inhibitor to have demonstrated pro-longed suppression of plasma A� with a QW dosingschedule. No safety and tolerability concerns wereidentified up to the highest single or multiple dosesstudied. Two Phase III studies of AZD3293 (AMA-RANTH, NCT02245737; and DAYBREAK-ALZ,NCT02783573) are now ongoing.
ACKNOWLEDGMENTS
Medical writing services were provided byCatherine Spanswick, PhD, and were funded byAstraZeneca.
These studies were sponsored by AstraZeneca.Authors’ disclosures available online (http://j-alz.
com/manuscript-disclosures/16-0701r1).
SUPPLEMENTARY MATERIAL
The supplementary material is available in theelectronic version of this article: http://dx.doi.org/10.3233/JAD-160701.
REFERENCES
[1] Dementia. Fact sheet number 362 Geneva: World HealthOrganization, March 2015,WHO, http://www.who.int/mediacentre/factsheets/fs362/en/ Accessed September 6, 2016.
[2] Wortmann M (2012) Dementia: A global health priority –highlights from an ADI and World Health Organizationreport. Alzheimers Res Ther 4, 40.
[3] Cole SL, Vassar R (2007) The Alzheimer’s disease beta-secretase enzyme, BACE1. Mol Neurodegener 2, 22.
[4] Karran E, Mercken M, De Strooper B (2011) The amyloidcascade hypothesis for Alzheimer’s disease: An appraisalfor the development of therapeutics. Nat Rev Drug Discov10, 698-712.
[5] Menting KW, Claassen JA (2014) beta-secretase inhibitor;a promising novel therapeutic drug in Alzheimer’s disease.Front Aging Neurosci 6, 165.
[6] Vassar R, Kuhn PH, Haass C, Kennedy ME, Rajendran L,Wong PC, Lichtenthaler SF (2014) Function, therapeuticpotential and cell biology of BACE proteases: Current statusand future prospects. J Neurochem 130, 4-28.
[7] Hardy J, Selkoe DJ (2002) The amyloid hypothesis ofAlzheimer’s disease: Progress and problems on the road totherapeutics. Science 297, 353-356.
[8] Selkoe DJ (1991) The molecular pathology of Alzheimer’sdisease. Neuron 6, 487-498.
[9] Yan R, Vassar R (2014) Targeting the beta secretase BACE1for Alzheimer’s disease therapy. Lancet Neurol 13, 319-329.
[10] Goate A, Chartier-Harlin MC, Mullan M, Brown J, Craw-ford F, Fidani L, Giuffra L, Haynes A, Irving N, James L,Mant R, Newton P, Rooke K, Roques P, Talbot C, Pericak-Vance M, Roses A, Williamson R, Rossor M, Owen M,Hardy J (1991) Segregation of a missense mutation in theamyloid precursor protein gene with familial Alzheimer’sdisease. Nature 349, 704-706.
[11] Hendriks L, van Duijn CM, Cras P, Cruts M, Van Hul W,van Harskamp F, Warren A, McInnis MG, Antonarakis SE,Martin JJ, Hofman A, Van Broeckhoven C (1992) Preseniledementia and cerebral haemorrhage linked to a mutation atcodon 692 of the beta-amyloid precursor protein gene. NatGenet 1, 218-221.
[12] Mullan M, Crawford F, Axelman K, Houlden H, Lilius L,Winblad B, Lannfelt L (1992) A pathogenic mutation forprobable Alzheimer’s disease in the APP gene at the N-terminus of beta-amyloid. Nat Genet 1, 345-347.
[13] Citron M, Oltersdorf T, Haass C, McConlogue L, Hung AY,Seubert P, Vigo-Pelfrey C, Lieberburg I, Selkoe DJ (1992)Mutation of the beta-amyloid precursor protein in famil-ial Alzheimer’s disease increases beta-protein production.Nature 360, 672-674.
[14] Cai XD, Golde TE, Younkin SG (1993) Release of excessamyloid beta protein from a mutant amyloid beta proteinprecursor. Science 259, 514-516.
[15] Suzuki N, Cheung TT, Cai XD, Odaka A, Otvos L Jr,Eckman C, Golde TE, Younkin SG (1994) An increasedpercentage of long amyloid beta protein secreted by famil-ial amyloid beta protein precursor (beta APP717) mutants.Science 264, 1336-1340.
[16] Kawarabayashi T, Younkin LH, Saido TC, Shoji M, AsheKH, Younkin SG (2001) Age-dependent changes in brain,CSF, and plasma amyloid (beta) protein in the Tg2576 trans-genic mouse model of Alzheimer’s disease. J Neurosci 21,372-381.
[17] Roberds SL, Anderson J, Basi G, Bienkowski MJ, Branstet-ter DG, Chen KS, Freedman SB, Frigon NL, Games D, HuK, Johnson-Wood K, Kappenman KE, Kawabe TT, KolaI, Kuehn R, Lee M, Liu W, Motter R, Nichols NF, PowerM, Robertson DW, Schenk D, Schoor M, Shopp GM, ShuckME, Sinha S, Svensson KA, Tatsuno G, Tintrup H, WijsmanJ, Wright S, McConlogue L (2001) BACE knockout mice arehealthy despite lacking the primary beta-secretase activityin brain: Implications for Alzheimer’s disease therapeutics.Hum Mol Genet 10, 1317-1324.
[18] Laird FM, Cai H, Savonenko AV, Farah MH, He K,Melnikova T, Wen H, Chiang HC, Xu G, Koliatsos VE,Borchelt DR, Price DL, Lee HK, Wong PC (2005) BACE1,a major determinant of selective vulnerability of the brainto amyloid-beta amyloidogenesis, is essential for cognitive,emotional, and synaptic functions. J Neurosci 25, 11693-11709.
[19] McConlogue L, Buttini M, Anderson JP, Brigham EF, ChenKS, Freedman SB, Games D, Johnson-Wood K, Lee M,Zeller M, Liu W, Motter R, Sinha S (2007) Partial reductionof BACE1 has dramatic effects on Alzheimer plaque andsynaptic pathology in APP Transgenic Mice. J Biol Chem282, 26326-26334.
[20] Jonsson T, Atwal JK, Steinberg S, Snaedal J, Jonsson PV,Bjornsson S, Stefansson H, Sulem P, Gudbjartsson D, Mal-oney J, Hoyte K, Gustafson A, Liu Y, Lu Y, Bhangale T,Graham RR, Huttenlocher J, Bjornsdottir G, Andreassen

G. Cebers et al. / PK and PD of AZD3293, a Novel BACE1 Inhibitor 1053
OA, Jonsson EG, Palotie A, Behrens TW, Magnusson OT,Kong A, Thorsteinsdottir U, Watts RJ, Stefansson K (2012)A mutation in APP protects against Alzheimer’s disease andage-related cognitive decline. Nature 488, 96-99.
[21] Butini S, Brogi S, Novellino E, Campiani G, Ghosh AK,Brindisi M, Gemma S (2013) The structural evolution ofbeta-secretase inhibitors: A focus on the development ofsmall-molecule inhibitors. Curr Top Med Chem 13, 1787-1807.
[22] Oehlrich D, Prokopcova H, Gijsen HJ (2014) The evolutionof amidine-based brain penetrant BACE1 inhibitors. BioorgMed Chem Lett 24, 2033-2045.
[23] Vassar R (2014) BACE1 inhibitor drugs in clinical trials forAlzheimer’s disease. Alzheimers Res Ther 6, 89.
[24] May PC, Dean RA, Lowe SL, Martenyi F, Sheehan SM,Boggs LN, Monk SA, Mathes BM, Mergott DJ, WatsonBM, Stout SL, Timm DE, Smith Labell E, Gonzales CR,Nakano M, Jhee SS, Yen M, Ereshefsky L, Lindstrom TD,Calligaro DO, Cocke PJ, Greg Hall D, Friedrich S, Citron M,Audia JE (2011) Robust central reduction of amyloid-beta inhumans with an orally available, non-peptidic beta-secretaseinhibitor. J Neurosci 31, 16507-16516.
[25] May PC, Willis BA, Lowe SL, Dean RA, Monk SA, CockePJ, Audia JE, Boggs LN, Borders AR, Brier RA, Calli-garo DO, Day TA, Ereshefsky L, Erickson JA, GevorkyanH, Gonzales CR, James DE, Jhee SS, Komjathy SF, Li L,Lindstrom TD, Mathes BM, Martenyi F, Sheehan SM, StoutSL, Timm DE, Vaught GM, Watson BM, Winneroski LL,Yang Z, Mergott DJ (2015) The potent BACE1 inhibitorLY2886721 elicits robust central Abeta pharmacodynamicresponses in mice, dogs, and humans. J Neurosci 35, 1199-1210.
[26] Forman M, Kleijn HJ, Dockendorf M, Palcza J, Tseng J,Canales C (2013) The novel BACE inhibitor MK-8931dramatically lowers CSF beta-amyloid in patients withmild-to-moderate Alzheimer’s disease. Alzheimers Dement9, P139.
[27] Lai R, Albala B, Kaplow JM, Aluri J, Yen M, Satlin A (2012)First-in-human study of E2609, a novel BACE1 inhibitor,demonstrates prolonged reductions in plasma betaamyloidlevels after single dosing. Alzheimers Dement 8, P96.
[28] Timmers M, Van Broeck B, Slemmon J, De Waepenaert K,Russu A, Bogert J (2015) Profiling the dynamics of CSF andplasma Abeta reduction with JNJ-54861911, an oral BACEinhibitor. Neurodegener Dis 15, 310.
[29] Yan R (2016) Stepping closer to treating Alzheimer’sdisease patients with BACE1 inhibitor drugs. Transl Neu-rodegener 5, 13.
[30] Eketjall S, Janson J, Kaspersson K, Bogstedt A, Jeppsson F,Falting J, Haeberlein SB, Kugler AR, Alexander RC, CebersG (2016) AZD3293: A novel, orally active BACE1 inhibitorwith high potency and permeability and markedly slow off-rate kinetics. J Alzheimers Dis 50, 1109-1123.
[31] McKhann GM, Knopman DS, Chertkow H, Hyman BT,Jack CR Jr, Kawas CH, Klunk WE, Koroshetz WJ, ManlyJJ, Mayeux R, Mohs RC, Morris JC, Rossor MN, Schel-tens P, Carrillo MC, Thies B, Weintraub S, Phelps CH(2011) The diagnosis of dementia due to Alzheimer’s
disease: Recommendations from the National Institute onAging-Alzheimer’s Association workgroups on diagnosticguidelines for Alzheimer’s disease. Alzheimers Dement 7,263-269.
[32] Folstein MF, Folstein SE, McHugh PR (1975) Mini-mentalstate. A practical method for grading the cognitive state ofpatients for the clinician. J Psychiatr Res 12, 189-198.
[33] Columbia-Suicide Severity Rating Scale (Japanese Ver-sion), Columbia University Medical Center, http://www.cssrs.columbia.edu, Accessed September 6, 2016.
[34] Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, JanavsJ, Weiller E, Hergueta T, Baker R, Dunbar GC (1998) TheMini-International Neuropsychiatric Interview (M.I.N.I.):The development and validation of a structured diagnos-tic psychiatric interview for DSM-IV and ICD-10. J ClinPsychiatry 59(Suppl 20), 22-33; quiz 34-57.
[35] Bell J, O’Neill B, Brodney M, Hajos-Korcsok E, Lu Y,Riddell D (2013) A two-part adaptive design to evaluatesafety, pharmacokinetics and pharmacodynamics for mod-ifying beta-amyloid in a first-in-human study. AlzheimersDement 9, P287.
[36] Quartino A, Huledal G, Sparve E, Luttgen M, BuetersT, Karlsson P, Olsson T, Paraskos J, Maltby J, Claeson-Bohnstedt K, Lee CM, Alexander R, Falting J, Paulsson B(2014) Population pharmacokinetic and pharmacodynamicanalysis of plasma Abeta40 and Abeta42 following singleoral doses of the BACE1 inhibitor AZD3839 to healthyvolunteers. Clin Pharmacol Drug Dev 3, 396-405.
[37] BACE Inhibitor BI 1181181 Voluntarily Put on TemporaryClinical Hold for Safety Evaluation, Vitae Pharmaceuticals,http://ir.vitaepharma.com/phoenix.zhtml?c=219654&p=irol-newsArticle&ID=2020814, Accessed September 6,2016.
[38] MacLeod R, Hillert EK, Cameron RT, Baillie GS (2015)The role and therapeutic targeting of �-, �- and �-secretasein Alzheimer’s disease. Future Sci 1, FSO11.
[39] Eketjall S, Janson J, Jeppsson F, Svanhagen A, KolmodinK, Gustavsson S, Radesater AC, Eliason K, Briem S,Appelkvist P, Niva C, Berg AL, Karlstrom S, Swahn BM,Falting J (2013) AZ-4217: A high potency BACE inhibitordisplaying acute central efficacy in different in vivo modelsand reduced amyloid deposition in Tg2576 mice. J Neurosci33, 10075-10084.
[40] Liu-Seifert H, Siemers E, Holdridge KC, Andersen SW, Lip-kovich I, Carlson C (2015) Delayed-start analysis: MildAlzheimer’s disease patients in solanezumab trials, 3.5years. Alzheimers Dement 1, 111-121.
[41] Doody RS, Thomas RG, Farlow M, Iwatsubo T, Vellas B,Joffe S, Kieburtz K, Raman R, Sun X, Aisen PS, Siemers E,Liu-Seifert H, Mohs R (2014) Phase 3 trials of solanezumabfor mild-to-moderate Alzheimer’s disease. N Engl J Med370, 311-321.
[42] Georgievska B, Gustavsson S, Lundkvist J, Neelissen J,Eketjall S, Ramberg V, Bueters T, Agerman K, Jureus A,Svensson S, Berg S, Falting J, Lendahl U (2015) Revisitingthe peripheral sink hypothesis: Inhibiting BACE1 activity inthe periphery does not alter beta-amyloid levels in the CNS.J Neurochem 132, 477-486.