-
8/3/2019 ch 14 part 1
1/10
BACTERIAL SIALADENITIS
Acute Chronic Recurrent Parotitisrare Rare for children &
adults
SG Parotid Submandibular > parotid parotid
ascending infection from mouth -In major glands, usually
non-specific, asocc. with ductobstruction (salivary calculi) &
low grade ascendinginfection
-progressive chronic inflammation of SM complete
replacement of parenchyma by fibrous tissue mistakenfor chronic
sclerosing sialadenitis (a tumor)
Rarely, adult for may follow onfrom childhood type but mostlydue
to persistence ofpredisposing factors (calculi,
duct strictures)
Childhood type:1. Abnormally secretion
rate2. Immature immune
response3. Congenital abnormalities
of ductal system
Clinical features:1. Unilateral or bilateral
2. Recurrent painfulswelling
3. Pus from orifice4. Often resolve
spontaneously by earlyadulthood
bacteria Strep. PyogenesStaph. AureusHaemophilus species
Black-pigmented Bacteroides
Factors 1. salivary flow-Sjogren syndrome-drugs with
xerostomicS/E
2. Postoperativecomplication indebilitated dehydratedpts after
abdominalsurgery
3. Immunocompromized pts4. Acute exacerbation of
chronic sialadenitis
salivary flowDisorder of salivary secretion
Clinicalfeatures
1. Rapid onset2. Swelling3. Pain, fever, malaise4. Redness of
overlying skin5. Pus from duct
1. Unilateral2. Recurrent, tender swelling3. Inflammation of
duct orifice4. Purulent, salty discharge (in acute
exacerbation)
histopathology
1. Vary degrees of ductal dilatation2. Hyperplastic ductal
epi.3. Periductal fibrosis
4. Acinar atrophy, replaced by fibrous tissue5. Chronic
inflammatory infiltration
Sialography :
1. Duct obstruction
2. Glandular tissue
obstruction
3. Ductal dilatation
Cellul
ar
Dilat
edAtrophi
c acini
Fibrosis
with
collage
-
8/3/2019 ch 14 part 1
2/10
VIRAL SIALADENITISMUMPS (EPIDEMIC PAROTITIS)
mumps 1
mumps 2
CYTOMEGALIC INCLUSION DISEASE(SG INCLUSION DISEASE)
Paramyxovirus Cytomegalovirus (herpervirus gp)Acute, contagious
infection, often in minor epidemicsCommonest cause of parotid
enlargement
Commonest of all SG diseaseDiagnosis usually clinicalConfirmed
diagnosis by (within 1st week)
detection of IgM Ab
in serum titer to mumps virus AgImmunity after an attack is
long-lastingRare recurrent infection
Infection is common in humansworldwide
Most 1 infections are asymptomaticCausing severe disseminated
disease inneonates & immunocompromised hosts(transplant, HIV
pts)Maybe assoc. with xerostomia & HIVinfection
Clinically:1. Most common in childhood2. Transmitted by direct
contact with infected saliva &
droplet spread3. Incubation period: 2-3 weeks
4. Prodromal symptoms: fever, malaise5. Sudden onset of painful
swelling of 1 or more SG
-parotid (70%)6. occasional involvement of SM & SL but
rarely w/out
parotid7. enlargement gradually subsides () over 1 week8. virus
present in saliva
-2-3 days before onset-6days after
9. occasional involve of other organs in adults; testes,ovaries,
CNS
10. orchitis (inflamme testes):most common
complication (20%)
Histopathology:1. SG involvement usually an
incidental finding2. Large, doubly contoured owl-eye
inclusion bodies within nucleus or
cytoplasm of duct cells of parotidgland
3. In disseminated disease, similarinclusions are found in
kidneys,liver, lungs, brain & other organs
-
8/3/2019 ch 14 part 1
3/10
SIALADENOSIS (SIALOLIS) HIV-ASSOCIATED SG DISEASE
Non-inflammatory, non-neoplastic, recurrent bilateral swelling
of SGMost common: parotid (due to abnormal of neurosecretory
control)
-A small feature in small # of adults HIV pts-Prevalence higher
in children-xerostomia and/or swelling of major SG, esp
parotid-xerostomia caused by SS-like process associated with
myoepithelial sialadenitis-however, no auto-Ab profile as seen
with SS-HIV-related parotid enlargementdue to:
1. Persistent glandularlymphadenopathy
2. Multiple lymphoepitelialcyst
Reported with:1. Hormonal disturbances
2. Malnutrition3. Liver cirrhosis4. Chronic alcoholism
Various drugs
Histopathology:1. Hypertrophy of serous acinar cells to about 2x
their normal size
Cytoplasm is densely packed with secretory granules
POSTIRRADIATION SIALADENITIS SARCOIDOSIS SIALADENITIS OF MINOR
GLANDSCommon complication of radiotheraphyDirect correlation
btwn-dose of irradiation-severity of damageDamage is often
irreversible, leading to:-fibrous replacement of damaged
acini-squamous metaplasia of ductsIn less severe cases, some degree
of fx mayreturn after several monthsSerous acini are more sensitive
than mucousacini
-May affect parotid & minor salivary glands-Parotid
involvement present as persistent,often painless enlargement-may be
assoc. with involvement of lacrimalglands in Heerfordt syndrome
-often an incidental & insignificant finding-may however be
of diagnosticsignificance, such as in Sarcoidosis &Sjogren
syndrome-Most frequently seen in assoc. withmucous extravasation
cysts & nicotinicstomatitis-Very rarely may present with
multiplemucosal swellings assoc. with cysticdilatation of ducts
& chronic suppuration(stomatitis glandularis)
-most commonly on the lips, probably asan acute exacerbation of
a chronic formassoc. with obstruction or reduction insalivary flow
(cheilitis glandularis)
Clinically Histopathology
-
8/3/2019 ch 14 part 1
4/10
Obstructive&
TraumaticLesions
Obstructive&
TraumaticLesions
SALIVARYCALCULI(SIALOLITHS)
Most common in middle-aged adultsMay form in ducts withinthe
gland, or in mainexcretory ductSubmandibular (79-90%)> parotid
> Sublingual orminor glands (2%)
UnilateralMay be multiple in thesame gland
-when symptomatic, they cause pain &sudden enlargement of
affected gland(esp at meal times when salivaryscrtn)- in flow
predispose to ascendinginfection & chronic sialadenitis-calculi
may be detected by palpation &on radiographs
Form by gradual deposition of Ca saltsaround an initial organic
nidus (whichmay consists of altered salivarymucins with desquamated
cells µorganisms)
NECROTIZINGSIALOMETAPLASIA
UncommonMay be mistaken clinically& histologically
formalignant diseaseMost frequent on hardpalate in middle aged
pts,males
Etiology unknown, butprobably due to:
-most common as deep, crater-like ulcer(mimic malignant
ulcer)-10-12 weeks to healUlcer may be preceded by
induratedswelling
Lobular necrosisSq metaplasiaof ducts & aciniMucous
extravasationInflammatory cell infiltration-Overlying palatal
mucosa:pseudoepitheliomatous hyperplasia-features may be mistaken
for SCC or
mucoepidermoid carcinoma
Sialoliths at the
orifice of
submandibular
Multiple
sialoliths
Duct
metapla
-
8/3/2019 ch 14 part 1
5/10
-ischemia leading toinfarction of Salivarylobules-trauma (eg LA
injection,previous surgery)
MUCOCELES
SJOGREN SYNDROMEChronic autoimmunedisease
1. Primary (Sicca Sydrome)-dry mouth (xerostomia)
-dry eyes (xerophtalmia or keratoconjunctivitis sicca)-more
severe ocular & oral manifestations
Manifestation of keratoconjunctivitis sicca:-dryness of
eyes-conjunctivitis-gritty, burning sensation
2. Secondary-xerostomia
-xerophtalmia-Autoimmune CT disease
:: Rheumatoid Arthritis (most common):: SLE:: Systemic
sclerosis:: Primary billiary cirrhosis:: mixed CT disease
Lymphocytic infiltrationAcinar destruction oflacrimal &
SG
Histophatology of major glands:
-lymphocytic infiltration, initially around intralobular
ducts,eventually replacing the whole effected lobules
-20% B cells, 80% T cells (mostly T helper)
Histopatholohy of minor glands
-focal collection of lymphoid cells, initiallyaround
intralobular ducts
-# of foci reflects the severity of disease
Coagulati
ve
-
8/3/2019 ch 14 part 1
6/10
-acinar atrophy-proliferation of duct epithelium to form
epimyoepithelial islands(myoepithelial sialadenitis or benign
lymphoepithelial lesions)-unlike lymphoma, the infiltrate x cross
interlobular CT septa
-the semi-quantitative assessment of thisfocal lymphocytic
sialadenitis in labial minorSG biopsies is an imp. Investigation
inestablishing a dx, & is one of the dx criteria-however, since
the appearance is x specific,it must be interpreted in the presence
ofclinical features & serological investigations.
i. Ocular symptoms
ii. Ocular signsiii. Oral symptomsiv. SG fxv. Labial SG
histologyvi. Ro & La autoAb
(fulfill 4/6 criteria todiagnose as SS)
Investigations:
-minor SG biopsy-estimation of parotid salivary flow rates,
usually -sialography: shows sialectasia (snowstorm pattern,
cherry-tree in blossom appearance)
-salivary scintiscanning with [99Tcm] shows uptake-serological
findings: Anti-Ro & Anti-La**Although neither Anti-Ro nor
Anti-La are specific for SS, theyare diagnostically helpful since
they may be detected some time
before clinical picture develops
Etiology & pathogenesis
- autoimmune-genetic factors important in susceptibilityto
external factors that trigger SS- frequency in pts with HLA class
II MHCgenes-EBV as potential trigger-immunological mechanisms (T
cells & theircytokines) causing destruction of
glandulartissue-pathogenic significance of the range ofcirculating
auto-Ab is uncertain
Middle-aged females (F:M.9:1)Most common symptomsrelated to
xerostomia &xerophtalis
Malignant transformation-risk of B cell lymphoma developing in
affected glands 44x thanof general ppltn-risk varies from
-
8/3/2019 ch 14 part 1
7/10
of mucosa assocwith candisosis
5. rapidly progressivecaries
6. Acute bacterialsaladenitis
Oral mucosa appears dry,smooth & glazed
Dorsum of tongue appearred & atrophic with variabledegrees
of fissuring &lobulation
xerophtalmia
Salivary gland enlargement is variable
What are the other causes of SG swelling?
Sarcoidosis
Mumps
Sometimes in conditions like starvation,diabetes mellitus, HIV
pts
Variable SG enlargement-30% pts give hx ofenlargement-only 15%
present withenlargement-usually bilateral-predominantly:
parotid
gland-seldom painful
Lacrimal gland enlargementis uncommon
High incidence of cariescaused by low salivary
The antinuclear Ab are
mostly found in the
secondary Sjgren
Syndrome. What Ab
are the most helpful in
our diagnosis? It isAnti-Ro and Anti-La or
also known as anti SSA
and anti SSB. SS refers
to Sjgren Syndrome.
These can be found in
other diseases but
when present they are
good indication of
Sjgren Syndromebecause they are
found early. This
makes it as the most
Epimyoepithe
lial island
-
8/3/2019 ch 14 part 1
8/10
scretion
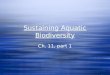
This is the serological abnormalities & autoantibodies
in
primary & secondary Sjgren Syndrome. Just look
andunderstand. You dont need to memorize them. Just to
help you in understanding this disease.
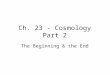
Here is example in minor SG. The minorSG biopsy is very
important to diagnoseSjgren Syndrome & of course
withassociation to other clinical symptomslike the presents of Ab,
enlargement,xerostomia, etc.
Parotid SG Submandibular SG Sublingual SG
-
8/3/2019 ch 14 part 1
9/10
serous, proteinaceous (more watery) mix of serous and mucous.
Butmainly serous
mainly mucous
Minor SGmucous, some of them are(mostly on the tongue) are
mix.
Areas where we cant findminor SG are:
Attached gingiva
Ant. part of hard palateuntil molar area
Mid palatal raphe
This is a sample from labial minorSG where we have
mostlymucinous but sometimes seroussecretion.
DEVELOPMENTAL ANOMALIES OF SG
-
8/3/2019 ch 14 part 1
10/10
The most famous is Stafnes Idiopathic Bone Cavity. At the
lingual aspect of
the mandible, we have a slight depression called submandibular
fossae.
Sometimes during development, some SG tissue entrapped within
the
submandibular fossae, either completely surrounded by bone or
partially.
Radiographically, we can see this area as a well-defined area
beneath theinferior alveolar canal.
*Assalamualaikum. Selamat study semua. Smg Allah permudahkan
kita utk memahami, menghafal dan menjawab soalan2 dgn
baik. Notes ni x termasuk buku. Kalau ada masa, boleh la tmbh2
maklumat dr buku ye. Bukan ape, selain mun x ckp rajin , lg
pun kalau masukkn semuasgt tebaaaal la notes ni.dn namenye pn
notes kan. Mestilah ringkas dn padat. Hehedn jugekalauboleh baca la
at least sekali lecture notes for labx semua mun masukkn kt cni.
Alasan spt d atsok. Selamaaat!
Slm syg