-
8/3/2019 ch 14 part 2
1/10
POLYMORPHOUS LOW GRADE ADENOCARCINOMA AGE CHANGES IN SG-minor
SG, mostly palate-good prognosis-unpredictable potential to
metastasize in 15% cases
in weight of parotid & submandibular glands relatedto
atrophy of secretory tissue & replacement byfibrofatty
tissue
Similar changes in labial minor SG
Oncocyte change in ductal epithelium
in flow rate of submandibular gland
Histopathologic:-variety of growth pattern within the same
lesion
Solid
Tubular Papillary
Cribriform-cytologically uniform-bland with infrequent
mitoses-lack of atypia-D/D adenoid cystic carcinoma (both show
perinueralinvasion)
-
8/3/2019 ch 14 part 2
2/10
-
8/3/2019 ch 14 part 2
3/10
PLEOMORPHIC ADENOMA (MIXED TUMOR)Commonest SG tumor
:: 60-65% parotid:: 45% minor SG
7% originate in minor SG esp palatalOld ages, femaleUsually
solitaryRecurrences may be multifocal
Clinicalfeatures
-Slowly growing, painless, rubbery swellingwith intact overlying
skin or mucosa-pts may be aware of lesion for several yrs
Histopathologicfeatures
-compose of cells of epithelial &myoepithelial origin-great
variety with complex intermingling ofcomponents &
mesenchyme-like areas-although benign, CT capsule is x
alwayscomplete-clearly demarcated, but apparently
isolated nodules may be seen within oreven outside the capsule,
giving theimpression of invasive growth-serial sections show that
these representoutgrowth of the main mass-These islands explain the
need for excisionwith a margin to avoid recurrence-variation in
arrangement of epithelial &stromal components btwn different
tumors& within different areas of same tumors-epithelial
components may be arranged in
duct-like structures sheets
clumps
interlacing strands
Duct
surrounded
by
Dilate
d
Kerati
n
-
8/3/2019 ch 14 part 2
4/10
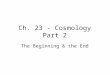
WARTHIN TUMOR(PAPILLARY CYSTADENOMA LYMPHOMATOSUM)
Mostly parotidSlow-growingMultifocalBilateral (5-10%)Old
ageMostly frm residual salivary duct epithelium entrappedwithin
lymp nodes during dvlpmnt
Clinical
features
Gross appearance:
-multiple, irregular cystic spaces of variable sizecontaining
mucoid material-lining of cyst has small projections (papillary
structures)
Histopathologicfeatures
Multiple, irregular cystic spaces containing mucoidmaterial
separated by papillary projections of tumortissue
Tumor consists of:
Epithelial component: double-layered epitheliumlining cystic
spaces in papillary arrangement
Lymphoid component within stroma, may containgerminal
centers
Epithelial cells have granular cytoplasm rich in
abnormalmitochondria, resembling oncocytes
Cyst
ic Lympho
id tissue
Double
layer of
epitheliu
-
8/3/2019 ch 14 part 2
5/10
BASAL CELL ADENOMA ONCOCYTOMA CANALICULAR ADENOMA
DUCTALPAPILLOMAS
-1-2% of all SG tumor-79% parotid, 20% upper lip-Peak incidence
in 7th decade
-rare-usually in parotid->60 yrs of age
->50 yrs of age-almost all cases in upper lip-no clinical
significance-x represent invasive growth
-rare-several subtypes
-Consist of cytologically uniform basaloidcells arranged in
variety of patterns-well-encapsulated
-thin capsule-consists of oncocyte
-consists of anastomosing strands ofbasaloid epithelial cells
arranged incanalicular structures-partly or grossly cystic due
todegeneration of loose vascularstroma-in some cases, multiple
microscopicfoci of adenomatous change seensurrounding minor SG
-papillary structureprojecting into theductal system
-
8/3/2019 ch 14 part 2
6/10
MUCOEPIDERMOID CARCINOMA
10% of all SG tumors
major SG: mostly parotid
minor SG: mostly palatal
highest incidence in 4th & 5th
decade
low grade MEC 1
low grade MEC 2
Low grade MECi. Well-differentiatedii. Mucous & epidermoid
cells
predominateiii. No cellular pleomorphismiv. Often cystic, cyst
lined by mucous-
secreting cellsv. Epidermoid cells present in strands
or clumps, show keratinizationvi. Rupture of mucin-containing
cyst
lead to inflammationvii. Advance on a broad, pushing front
low grade MEC 3
-
8/3/2019 ch 14 part 2
7/10
Clinical features:
similar to pleomorphic adenoma
grossly cystic tumors may befluctuant
more aggressive tumors maycause pain & ulceration
high grade MEC 1
High grade MECi. poorly-differentiatedii. epidermoid &
intermediate cells
predominateiii. nuclear & cellular pleomorphism,
atypiaiv. cystic spaces x prominentv. difficult to differentiate
frm SCCvi. ill defined & highly infiltrative
Histopathologic features:3 types of cells1. Squamous
(epidermoid)2. Mucous3. Intermediate
relative proportions & arrangements ofcell types are used to
distinguish btwn:
High grade MEC
Low grade MEC
Prognosis-low grade tumor rarely metastasize-however, behavior
cannot be accuratelypredicted frm histopathology
-overall 5-yr survival rate: 70%-low grade tumors 5-yr survival
rate: 95%
Local recurrence:
-
8/3/2019 ch 14 part 2
8/10
OTHERS SGCARCINOMA
ACINIC CELL CARCINOMA CARCINOMA ARISING IN PLEOMORPHIC
ADENOMA
1. ADENOCARCINOMA-relatively uncommon-1% or less of all
bodymalignancies-5% of head n neckmalignancies-most common in
majorSG esp parotid-however! Ratio ofmalignant to benign inminor SG
is higher than inmajor
*not otherwise specified(NOS)
-Uncommon-accounts for 2-3% of parotid tumors-low grade
malignancy-80-100% 5-yr survival rates for well-differentiated
tumors-65% 5-yr survival rates for poorly-differentiated tumors
-known as carcinoma ex pleomorphic adenoma-3% of all SG
tumors-almost all arises in parotid or submandibular longstanding
tumors-histological dx requires evidence of pre-existingpleomorphic
adenoma-malignant component may be an:
adenocarcinoma
undifferentiated carcinoma
other types of SG carcinoma-when the malignant part is confined
within pre-existingtumor, prognosis is excellent-poor prognosis
when there is infiltration-some mixed tumors arise as malignant de
novo
-spectrum of histopathologicalappearances-most common: sheets or
an acinargrouping of large, polyhedral cells withbasophilic,
granular cytoplasm (similar to
serous acinar cells) hence the name!
2. EPITHELIALMYOEPITHELIALCARCINOMA
3. BASAL CELLADENOCARCINOMA
-
8/3/2019 ch 14 part 2
9/10
ADENOID CYSTIC CARCINOMA-middle-aged & elderly-30% minor SG,
6% major (parotid)
Histological features:-wide spectrum of appearance
-most common: epithelium arranged as ovoid & irregularly
shaped islands, or
anastomosing cords & strands in scanty CT stroma
-numerous microscopic cyst-like spaces within epithelial islands
cribriformor Swiss cheese pattern-epithelium consists of small,
uniform, basophilic cells-rare mitoses-less common:
epithelium arranged in tubular or solid pattern-prominent
infiltration & invasion of adjacent tissues, spread around
& alongnerves-in maxilla, tumor may infiltrate along marrow
spaces with no evidence ofbone destruction-perineural invasion
Clinical features:-slow enlarging tumors (like
pleomorphicadenoma) but pain & ulceration are
morecommon-parotid tumors present with facial palsy-neurological
manifestation: infiltrate & spreadalong nerves
Prognosis:-radiotherapy used in inoperable cases, but xcure
permanently-runs a prolonged clinical course & metastases
Tumo
r cell
-
8/3/2019 ch 14 part 2
10/10
are late, usually to lungs-long term prognosis is poor-survival
rate for parotid tumors
5-yrs: 75%
10-yrs: 40%
20-yrs: