Embed Size (px)
Citation preview
71
CHAPTER 3.2
RIVASTIGMINE PHARMACOTHERAPY AND CLINICAL PHARMACOLOGY

72

73
CHAPTER 3.2.1 Discontinuation of rivastigmine in routine clinical practice
S.V. Frankfort, B.A. Appels, A. de Boer, C.R. Tulner,
J.P.C.M. van Campen, C.H.W. Koks, J.H.Beijnen
Abstract Background: Rivastigmine is used for symptomatic treatment of mild-to-moderately severe Alzheimer’s Dementia (AD). We investigated the frequency of and reasons for rivastigmine discontinuation in clinical practice and possible predictive factors for discontinuation within the first six months after starting therapy. Methods: A retrospective cohort study was performed in rivastigmine users, who started therapy in a naturalistic setting. A nurse supported a part of the studied cohort, as this was introduced during the study period. Reasons for discontinuation were investigated, including therapy discontinuation if the Maximum Achieved Dose (MAD) was below 6 mg daily. Predictors of discontinuation within the first half year were investigated by logistic regression analysis. Results: Baseline Mini-Mental-State-Examination (MMSE) of included patients (n=154) was 20.1, mean age was 78.4 years and 70% was female. Within 6 months, 61 users (39.6%) discontinued therapy, primarily (59.0%) for adverse events. Thereafter, the main reason for discontinuation was non-response according to clinimetrics. A MAD during the titration phase of 1.5-4.5 mg/day and absence of nurse support are significantly related to discontinuation within 6 months. Conclusions: Rivastigmine is primarily discontinued within the first six months for intolerable adverse events and thereafter mainly for ongoing deterioration. A MAD of 1.5-4.5 mg/day and the absence of nurse support are independently related to discontinuation of rivastigmine within the initial 6 months.
International Journal of Geriatric Psychiatry 2005;20:1167-1171

Chapter 3.2.1
74
Introduction Rivastigmine (Exelon®), an acetylcholinesterase inhibitor, has shown efficacy in the symptomatic treatment of mild to moderately severe Alzheimer’s dementia (AD)1,2. Known major occurring adverse events of rivastigmine include nausea, vomiting and diarrhoea, whereas bradycardia, dizziness, muscle cramps and weakness are of minor occurrence3. These adverse events are in certain cases reason for discontinuation of rivastigmine, whereas in others it is not continued because of ongoing decline in cognition. Geriatricians started prescribing rivastigmine in 1998 in our hospital and since April 2001 it is the policy at the geriatric department that these patients are supported by a nurse. Support consists of intensive telephone contact during the titration phase and regular telephone contact thereafter. This study aims describing reasons for discontinuation of rivastigmine in routine clinical practice and investigating predictive variables of discontinuation within the first half year after starting rivastigmine. Patients and Methods Patients This study was carried out in patients with mild-to-moderate severe AD, diagnosed according to the NINCDS-ADRDA criteria4, using rivastigmine via the geriatric outpatient department of a general hospital in the Netherlands. Only patients who had responsible relatives or friends who could monitor drug intake were included. Patients were excluded if their data were incomplete. Included patients were followed between May 1998 and September 2004. Dose titration Patients started rivastigmine at 1.5 mg twice daily. If tolerated for minimal 2 weeks doses were increased to 3.0 mg twice daily (until the end of 2001) or to once daily 3.0 mg and once daily 1.5 mg (after 2001). If tolerated for another 2 weeks, then doses were titrated to 4.5 mg twice daily (until the end of 2001) or to 3.0 mg twice daily (after 2001). Patients were further titrated by dose increments of 3.0 mg (until the end of 2001) or by 1.5 mg (after 2001), after tolerating therapy for an interval of 2 weeks at each subsequent dose level, to the individual Maximum Achieved Dose (MAD), up to a maximum of 6 mg twice daily. Rivastigmine was discontinued if daily doses of 6 mg were not achieved in case of adverse events, because lower doses are considered to be associated with less efficacy in retaining cognition, performance and behaviour1,2.

Discontinuation of rivastigmine
75
Neuropsychological assessment At baseline and at 6-months intervals effectiveness was measured in three domains: cognition, performance in daily living activities and behaviour. Decline or improvement was investigated compared to the previous 6-monthly visit. Rivastigmine had to be discontinued if one of the domains showed major deterioration or if minor decline in two domains without improvement in the third domain was shown. Discontinuation criteria are based upon score differences in a historical control cohort of AD patients. This cohort did not use cholinesterase inhibitors and was tested after an interval of 6 months with the same scales as used in our cohort. Design and Statistical analysis A retrospective analysis, describing reasons for and time window of discontinuation was carried out. If patients discontinued therapy because of adverse events, the MAD of rivastigmine was also considered and in these patients multiple reasons for discontinuation were counted. The Pearson Chi-square test for categorical data and independent sample t-tests for continuous data were used to compare patient characteristics who discontinued rivastigmine use within the first six months and who did not. Logistic regression analysis was performed to investigate possible risk factors for discontinuation within the first half year after starting therapy. Age was dichotomised to the mean of the population, ≤ 78.4 versus > 78.4, number of concomitant drugs to none versus ≥ 1, as we hypothesised taking other medication could enhance compliance, baseline MMSE score to ≤ 23 versus > 23, MAD of rivastigmine to < twice daily 3 mg versus ≥ twice daily 3 mg, level of education to low, level 1 through 4, versus high, level 5 through 7 as we used a seven-point scale, ranging from less than 6 years of elementary school (score 1) to a university degree (score 7)5, and titration schedule as 1.5 mg versus 3.0 mg dose increments, because both titration schedules were used during the study period. Gender, involvement of nurse support and place of living were examined as dichotomous variables. When multiple significant (p<0.1) covariates were identified univariately, multivariate logistic analysis was performed. Statistical calculations were performed with SPSS for Windows (version 11.0, SPSS Inc., Chicago, IL, USA). A p-value of 0.05 or less was considered statistically significant.
Chapter 3.2.1
76
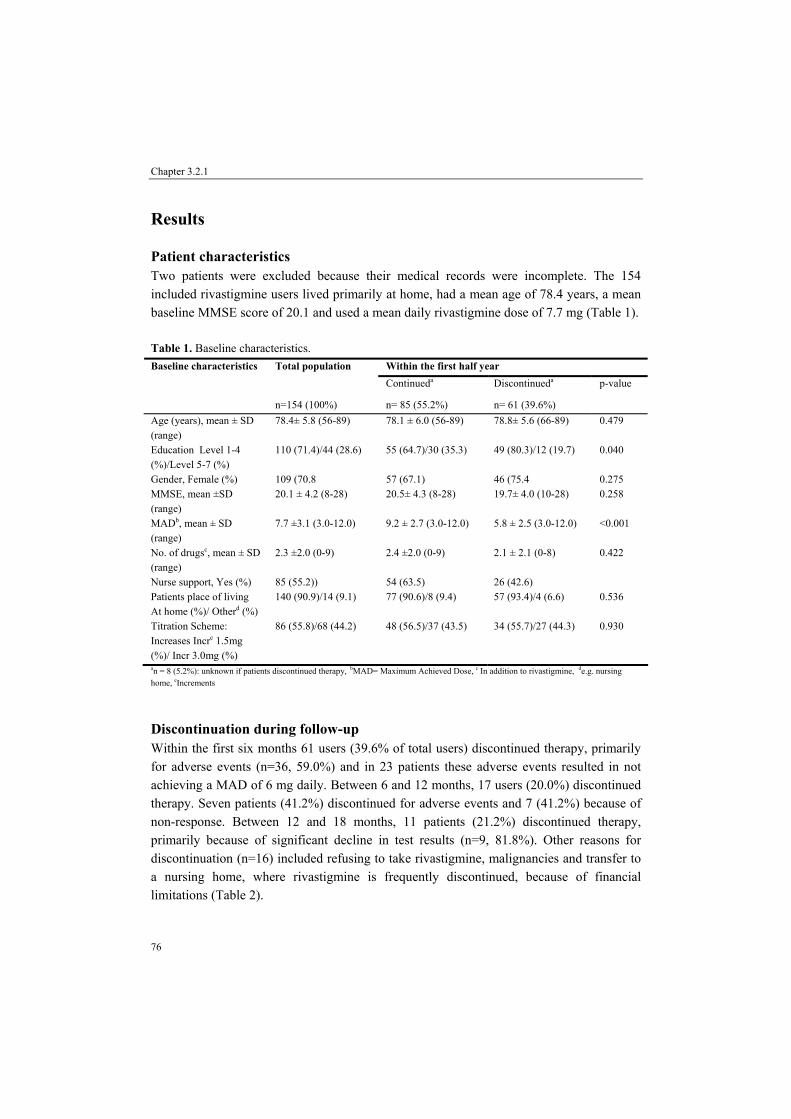
Results Patient characteristics Two patients were excluded because their medical records were incomplete. The 154 included rivastigmine users lived primarily at home, had a mean age of 78.4 years, a mean baseline MMSE score of 20.1 and used a mean daily rivastigmine dose of 7.7 mg (Table 1). Table 1. Baseline characteristics.
Within the first half year Baseline characteristics Total population Continueda Discontinueda p-value
n=154 (100%) n= 85 (55.2%) n= 61 (39.6%) Age (years), mean ± SD (range)
78.4± 5.8 (56-89) 78.1 ± 6.0 (56-89) 78.8± 5.6 (66-89) 0.479
Education Level 1-4 (%)/Level 5-7 (%)
110 (71.4)/44 (28.6) 55 (64.7)/30 (35.3) 49 (80.3)/12 (19.7) 0.040
Gender, Female (%) 109 (70.8 57 (67.1) 46 (75.4 0.275 MMSE, mean ±SD (range)
20.1 ± 4.2 (8-28) 20.5± 4.3 (8-28) 19.7± 4.0 (10-28) 0.258
MADb, mean ± SD (range)
7.7 ±3.1 (3.0-12.0) 9.2 ± 2.7 (3.0-12.0) 5.8 ± 2.5 (3.0-12.0) <0.001
No. of drugsc, mean ± SD (range)
2.3 ±2.0 (0-9) 2.4 ±2.0 (0-9) 2.1 ± 2.1 (0-8) 0.422
Nurse support, Yes (%) 85 (55.2)) 54 (63.5) 26 (42.6) Patients place of living At home (%)/ Otherd (%)
140 (90.9)/14 (9.1) 77 (90.6)/8 (9.4) 57 (93.4)/4 (6.6) 0.536
Titration Scheme: Increases Incre 1.5mg (%)/ Incr 3.0mg (%)
86 (55.8)/68 (44.2) 48 (56.5)/37 (43.5) 34 (55.7)/27 (44.3) 0.930
an = 8 (5.2%): unknown if patients discontinued therapy, bMAD= Maximum Achieved Dose, c In addition to rivastigmine, de.g. nursing home, eIncrements
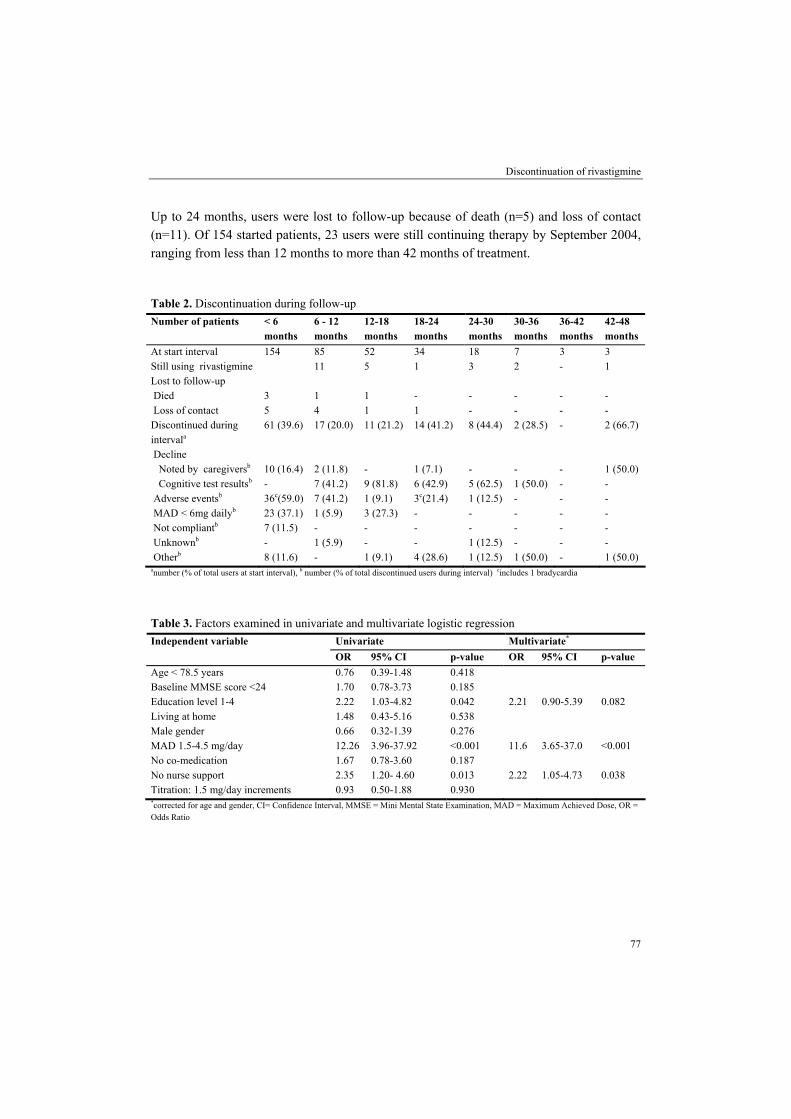
Discontinuation during follow-up Within the first six months 61 users (39.6% of total users) discontinued therapy, primarily for adverse events (n=36, 59.0%) and in 23 patients these adverse events resulted in not achieving a MAD of 6 mg daily. Between 6 and 12 months, 17 users (20.0%) discontinued therapy. Seven patients (41.2%) discontinued for adverse events and 7 (41.2%) because of non-response. Between 12 and 18 months, 11 patients (21.2%) discontinued therapy, primarily because of significant decline in test results (n=9, 81.8%). Other reasons for discontinuation (n=16) included refusing to take rivastigmine, malignancies and transfer to a nursing home, where rivastigmine is frequently discontinued, because of financial limitations (Table 2).
Discontinuation of rivastigmine
77
Up to 24 months, users were lost to follow-up because of death (n=5) and loss of contact (n=11). Of 154 started patients, 23 users were still continuing therapy by September 2004, ranging from less than 12 months to more than 42 months of treatment. Table 2. Discontinuation during follow-up Number of patients < 6
months 6 - 12 months
12-18 months
18-24 months
24-30 months
30-36 months
36-42 months
42-48 months
At start interval 154 85 52 34 18 7 3 3 Still using rivastigmine 11 5 1 3 2 - 1 Lost to follow-up Died 3 1 1 - - - - - Loss of contact 5 4 1 1 - - - - Discontinued during intervala
61 (39.6) 17 (20.0) 11 (21.2) 14 (41.2) 8 (44.4) 2 (28.5) - 2 (66.7)
Decline Noted by caregiversb 10 (16.4) 2 (11.8) - 1 (7.1) - - - 1 (50.0) Cognitive test resultsb - 7 (41.2) 9 (81.8) 6 (42.9) 5 (62.5) 1 (50.0) - - Adverse eventsb 36c(59.0) 7 (41.2) 1 (9.1) 3c(21.4) 1 (12.5) - - - MAD < 6mg dailyb 23 (37.1) 1 (5.9) 3 (27.3) - - - - - Not compliantb 7 (11.5) - - - - - - - Unknownb - 1 (5.9) - - 1 (12.5) - - - Otherb 8 (11.6) - 1 (9.1) 4 (28.6) 1 (12.5) 1 (50.0) - 1 (50.0) anumber (% of total users at start interval), b number (% of total discontinued users during interval) cincludes 1 bradycardia
Table 3. Factors examined in univariate and multivariate logistic regression
Univariate Multivariate* Independent variable OR 95% CI p-value OR 95% CI p-value
Age < 78.5 years 0.76 0.39-1.48 0.418 Baseline MMSE score <24 1.70 0.78-3.73 0.185 Education level 1-4 2.22 1.03-4.82 0.042 2.21 0.90-5.39 0.082 Living at home 1.48 0.43-5.16 0.538 Male gender 0.66 0.32-1.39 0.276 MAD 1.5-4.5 mg/day 12.26 3.96-37.92 <0.001 11.6 3.65-37.0 <0.001 No co-medication 1.67 0.78-3.60 0.187 No nurse support 2.35 1.20- 4.60 0.013 2.22 1.05-4.73 0.038 Titration: 1.5 mg/day increments 0.93 0.50-1.88 0.930 *corrected for age and gender, CI= Confidence Interval, MMSE = Mini Mental State Examination, MAD = Maximum Achieved Dose, OR = Odds Ratio

Chapter 3.2.1
78
Risk factors for discontinuation within the first half year As can be observed in table 1, the 61 patients who discontinued therapy within the first 6 months had a lower MAD (p<0.001), were less educated and were less frequently supported by a nurse (p<0.05) in comparison to the patients who continued therapy. Results of the logistic regression analysis are shown in table 3. The multivariate analysis showed that a MAD of 1.5-4.5 mg daily (OR 11.6, 95% CI 3.65-37.0 p<0.001) and no nurse support (OR 2.22, 95% CI 1.05-4.73, p=0.038) appeared to be independent predictors of discontinuation within the first half year.
Discussion Rivastigmine was frequently discontinued, because of intolerable adverse events during the first 6 months of treatment and thereafter mainly for ongoing deterioration. Discontinuation within the first 6 months was significantly related with a MAD of 1.5-4.5 mg daily and absence of nurse support. The comparison of our results to those described in literature has limitations. It is difficult to compare cholinesterase studies, because designs are substantially different6. Rivastigmine was evaluated in two large randomised placebo-controlled trials during 26 weeks which were subdivided into low (<6 mg/day) and high (6-12 mg/day) dose groups1,2. In the Newcastle (UK) study, four of 26 patients (15.4%) discontinued rivastigmine therapy because of side effects within the first 4 weeks of treatment7. As we did not investigate discontinuations in this period direct comparisons fall short. An Austrian study8, however, followed 529 patients in usual care during 24 weeks. This period is comparable to our cohort, which was followed for 26 weeks. In the Austrian study there were 67 drop-outs (12.7%) of whom 40.3% experienced side effects in that study. 39 patients were able to continue treatment although not achieving doses of 6 mg daily, which was not possible in our design and partly explains differences in number of discontinuations. As earlier described, patients are urged not to continue therapy if titration to 6 mg daily failed and explains a daily MAD <6 mg as an independent predictor of discontinuation in our clinical setting. Absence of nurse support, also an independent predictor, can be explained because adverse events and changes in titration-rate are discussed in regular telephone calls between the nurse and relatives or close friends of rivastigmine users. Strengths of our study are a relatively large population in a naturalistic setting, a total follow-up time of 42 months and accessibility to all relevant clinical data. In conclusion, initially discontinuation for intolerable adverse events is of major concern. Support by a nurse is important in this first period. After the first period major reason for discontinuation is an ongoing decline in cognition, performance or behaviour.

Discontinuation of rivastigmine
79
References 1. Corey-Bloom J, Anand R, Veach J. A randomized trial evaluating the efficacy and safety of ENA 713
(rivastigmine tartrate), a new acetylcholinesterase inhibitor, in patients with mild to moderately severe Alzheimer’s disease. International Journal of Geriatric Psychopharmacology 1998; 1:55-65.
2. Rösler M, Anand R, Cican-Sain A, et al. Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: international randomised controlled trial. BMJ 1999; 318:633-40.
3. Gauthier S. Cholinergic adverse effects of cholinesterase inhibitors in Alzheimer’s disease. Drugs Aging 2001; 18:853-62.
4. McKahnn G, Drachmann D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA work group under the auspices of department of health and human services task force on Alzheimer’s disease. Neurology 1984;34:939-44.
5. Verhage F. Intelligence and age. Van Gorcum: Assen 1964. (in Dutch). 6. Anand R, Hartman R, Sohn H, et al. Impact of study design and patient population on outcomes from
cholinesterase inhibitors trials. Am J Geriatr Psychiatry 2003;11:160-8. 7. Pakrasi S, Mukaetova EB, McKeith IG, et al. Clinical predictors of response to acetylcholinesterase
inhibitors: experience from routine clinical use in Newcastle. Int J Geriatr Psychiatry 2003;18:879-86. 8. Schmidt R, Lechner A, Petrovic K. Rivastigmine in outpatient services: experiences of 114 neurologists in
Austria. International Clinical Psychopharmacology 2002;17:81-85.

80

81
CHAPTER 3.2.2 Treatment effects of rivastigmine on cognition, performance
of daily living activities and behaviour in Alzheimer’s disease in an outpatient geriatric setting
S.V. Frankfort, B.A. Appels, A. de Boer, C.R. Tulner, J.P.C.M. van Campen,
C.H.W. Koks, J.H. Beijnen
Abstract We investigated rivastigmine effectiveness in 84 Alzheimer outpatients, with a special focus on behavioural problems. Cognition, activities in daily living (ADL) and behaviour were assessed during 30 months. Changes in test results between 6 months and baseline were compared with a historical control cohort of Alzheimer patients (n=69) by performing t-tests and calculation of Cohen’s d and standardised response mean (SRM). During 6 months rivastigmine showed effect on cognition (p<0.001, Cohen’s d = 0.33, SRM = 0.78), ADL (p<0.001, Cohen’s d = -0.43, SRM = -0.54) and memory related behaviour (p=0.006, Cohen’s d = -0.28, SRM = -0.28). Depressive behaviour worsened (p=0.001, Cohen’s d = 0.30, SRM = 0.37) and disruptive behaviour (p=0.369, Cohen’s d = -0.07, SRM = -0.09) was not effected by rivastigmine. During 30 months, a gradual decline was shown in most domains. Most RMBPC items showed stabilisation during 30 months. Improvement on disruptive behaviour items and depression items was shown after 6 months of treatment in a large proportion of patients in whom behavioural problems were present at baseline. In conclusion, a huge discontinuation rate is experienced within the first half year of treatment. In the subpopulation of patients who continued rivastigmine for 6 months, it shows modest effectiveness on cognition, functionality and memory associated behaviour compared with historical control patients. Unfortunately, disruptive behaviour is not altered by rivastigmine therapy, and depressive behaviour worsened slightly after initial treatment. During 30 months, rivastigmine showed stabilisation on numerous behaviour items as measured by the RMBPC.
International Journal of Clinical Practice 2006;60:646-654

Chapter 3.2.2
82
Introduction Rivastigmine (Exelon®), an acetylcholinesterase inhibitor, has shown efficacy in the symptomatic treatment of mild-to-moderately severe Alzheimer’s dementia (AD) in randomised placebo-controlled trials. These trials were rather liberal regarding inclusion criteria, for example co-morbidity1,2. Therefore, effectiveness in routine clinical practice would expect to be in a similar range like the trial outcomes. However, patients in trials might respond differently to drugs than patients in routine care. Complementary research in a clinical setting may reveal additional data on the effectiveness of rivastigmine in different domains. To our knowledge, a number of clinically based studies have investigated the effects of rivastigmine on cognition and activities in daily living (ADL) in routine clinical practice3,4. For example, López-Pousa et al.3 investigated cognition by MMSE and Mossello et al.4 investigated cognition by MMSE and performance in daily living activities by ADL and IADL scores. In addition, an open label extension phase of the trials investigated cognition, using the MMSE, up to 5 years of treatment5. Most trials lasted for up to 26 or 52 weeks, some were extended as open-label studies1,2,6. However, the long-term effects of cholinesterase inhibitor therapy remain largely unestablished. Although it is becoming clearer that cholinergic deficits are involved in the behavioural symptoms present in AD7 and that butyrylcholinesterase mediates behaviour8, effect of rivastigmine regarding behaviour is less described as compared with cognition. In a German open-label extension study, B 305, behaviour was measured with the CIBICplus in 34 rivastigmine users9. Meta analyses of three 6-month, double blind, placebo-controlled, regulatory trials investigated behavioural responses with the CIBICplus in rivastigmine users with mild-to-moderate severe AD10. In the clinical setting, research has predominantly been performed in nursing home residents taking rivastigmine, where behaviour was assessed using the NPI-NH. Aupperle et al.11 investigated long term effects during a 52 week open-label study in moderate-to-severe rivastigmine users. Hatoum et al.12 used the occupational disruptive scale of the NPI-NH to investigate the impact of rivastigmine on the disruptive behaviour of nursing home residents. Cummings et al.13 described the effects of rivastigmine treatment on neuropsychiatric and behavioural disturbances also in nursing home residents with moderate to severe probable AD. In the Netherlands, rivastigmine may only be prescribed if evaluation is regularly performed. Patients who are willing to start therapy are tested at baseline and at designated follow-up intervals during treatment. In our hospital, rivastigmine is prescribed via the geriatric outpatient department since 1998, and every 6 months three domains are assessed: cognition, behaviour and performance in daily living activities. In this cohort of patients, we performed retrospective analyses regarding the effectiveness of rivastigmine during 30 months.

Treatment effects of rivastigmine
83
The study aims investigating treatment effects of rivastigmine on different domains, with a special attention to behaviour, in a cohort of outpatients suffering from Alzheimer’s disease.
Patients and methods Patients This retrospective study was carried out in patients with mild-to-moderate, probable or possible AD according to the NINCDS-ADRDA criteria14 and using rivastigmine via the geriatric outpatient department of a general hospital. Only patients who had relatives or friends who could monitor drug intake and patients in whom therapy was evaluated after 6 months were included. Patients were excluded if baseline cognitive test results were incomplete. Dose titration Patients started rivastigmine at 1.5 mg twice daily, and doses were titrated up after intervals of minimal 2 weeks at each dose level, until the individual Maximum Achieved Dose (MAD) up to 6 mg twice daily. During titration, it was possible to omit a dose, to postpone dose increments, or to return to a lower dose level if adverse events required this. Assessment of domains At baseline and at 6-months intervals rivastigmine use was evaluated by assessment of three domains. Cognition was measured with MMSE15 and Cambridge Cognitive Examination (CAMCOG)16. CAMCOG consists of 60 items covering orientation, language, memory, praxis and calculation/attention, abstract reasoning and perception. Total sum scores range from 0 to 107. CAMCOG can be subdivided into a memory (maximum score 37) and a non-memory (maximum score 70) section17. Functional disability was measured with the performance subscale of the Interview for Deterioration in Daily living activities in Dementia (IDDD), a caregiver based paper-and-pencil questionnaire, which consists of 11 items with sum scores ranging from 0 to 4418. Behaviour was measured with the Revised Memory and Behavioural Problems Checklist (RMBPC). It is also a caregiver based paper-and-pencil questionnaire and consists of three subsections. First, a 7-item memory subscale (score per item 0-4, maximum score 28) that includes forgetting recent events, repeated questions, losing things, forgetting the day, forgetting past events, reduced concentration and not finishing tasks. Second, an 8-item disruptive behaviour subscale (score per item 0-4, maximum score 32) including verbal aggression, threats to hurt others, destroying property, to behave dangerous to self or others, talking loudly and rapidly, embarrassing
Chapter 3.2.2
84
behaviour, arguing and waking caregiver up. Third, a 9-item depression subscale (score per item 0-4, maximum score 36) includes comments about hopelessness, comments about being a burden, appearing sad or depressed, comments about dead, comments about being a failure, crying, comments about loneliness, appearing anxious and suicidal threats19. Lower scores on MMSE and CAMCOG and higher scores on the IDDD and subscales of the RMBPC reflect a worse functioning. Data collection All assessment results and demographic variables like gender, age and level of education20 were prospectively incorporated in a database. Place of living, number of concomitant drugs at baseline and MAD, all according to the medical records, were retrospectively obtained. Historical control cohort A research project was carried out at the memory clinic of an academic hospital in Amsterdam. In this project, 69 Alzheimer patients, who did not take rivastigmine, were tested at baseline and after 6 months with MMSE, CAMCOG, IDDD and RMBPC21. These 69 patients represent the historical control group in the present study. Statistical analysis Statistical calculations were performed with SPSS for Windows (version 11.0, SPSS Inc., Chicago, IL, USA). A p-value of 0.05 or less was considered statistically significant. Mean, standard deviation (SD) and range of baseline test results and differences between test results at 6-monthly follow-up visits and baseline were tabulated. For each of the RMBPC subitems, the percentages of patients who improved, deteriorated or remained stable after 6 months were calculated in a subpopulation of patients in whom that particular subitem was present at baseline. Deterioration was defined as an increase of equal or higher than one point and an improvement was defined as a decrease of equal or higher than one point on the RMBPC in this additional analysis. Differences in test results between the first follow-up at 6 months and baseline were compared to the historical control cohort by performing a one-sample t-test. Cohen’s d and standardised response means (SRM), were calculated to assess whether the differences are large enough to be clinically detectable. This is accomplished by dividing the raw effect size by the standard deviation of the measures in their respective populations, as shown in equation 1.
Effect Size (ES) = σ
)Y(Y-)X(X t1-t2t1-t2 (1)

Treatment effects of rivastigmine
85
To calculate a SRM, σ is the root mean square of the standard deviations of the change scores and to calculate Cohen’s d, σ is the root mean square of the baseline deviations22,23. In our calculations, X is the mean of test results in the rivastigmine group, Y is the mean of test results in the historical control cohort, t2 is after 6 months treatment and t1 is at baseline. Effect sizes greater than 0.20 are conventionally held to be clinically detectable. Effect sizes can be roughly subdivided into small (0.2), medium (0.5) and large (0.8)22. Linear regression analysis were performed to investigate relationships between effectiveness and different dosages.
Results Patient characteristics From the original population of 154 rivastigmine users, 61 patients discontinued treatment within the first 6 months because of adverse events (n=36), decline as noted by caregivers (n=10), incompliance (n=7) or for other reasons (n=8). Eight patients were lost to follow-up, because of death or losing contact within 6 months. After 6 months of treatment, patients mainly discontinued because of ongoing decline in cognition, performance or behaviour. Discontinuation of rivastigmine in this cohort of patients has been described in more detail in a separate publication24. One, six and eight patient(s) were excluded from MMSE/CAMCOG, IDDD and RMBPC analyses, respectively, because baseline data were lacking. In total, 84, 79 and 77 Alzheimer patients were included in this study for analyses on cognition, performance and behaviour, respectively. Table 1. Baseline characteristics. Baseline characteristics (n=84) n (%)* Age, mean ± SD (range) 78.2± 6.0 (56-89) Baseline MMSE, mean ±SD (range) 20.4 ±4.4 (8-28) Education < 6 years elementary school 2 (2.4) 6 years elementary school 19 (22.6) >6 years elementary school 14 (16.7) Domestic science school, junior technical school 20 (23.8) Secondary school for lower educational level 19 (22.6) Secondary school for higher educational level 10 (11.9) University degree 0 (0.0) Gender, female 58 (69.0) MADa, mean ± SD (range) 8.8 ±2.8 (1.5-12.0) Number of concomitant drugs, mean ± SD (range) 2.4 ±2.0 (0-9) Patients place of living, at home 76 (90.5) *unless otherwise noted, aMAD= Maximum Achieved Dose
Chapter 3.2.2
86
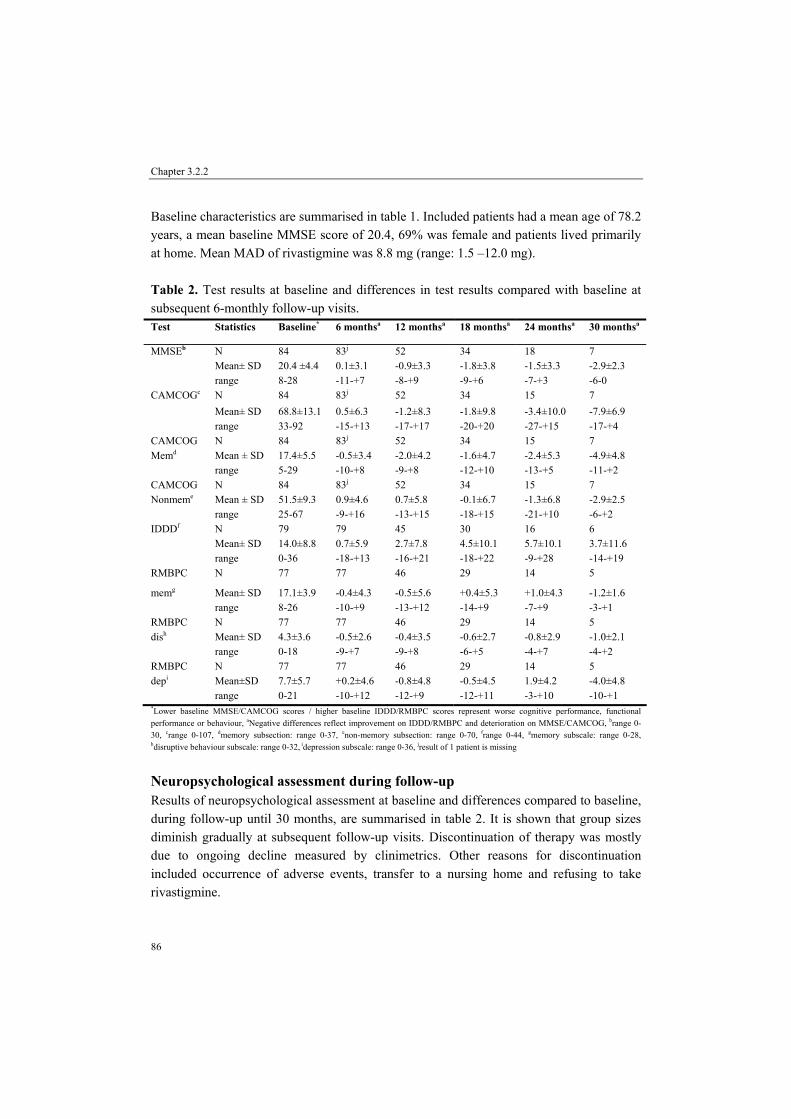
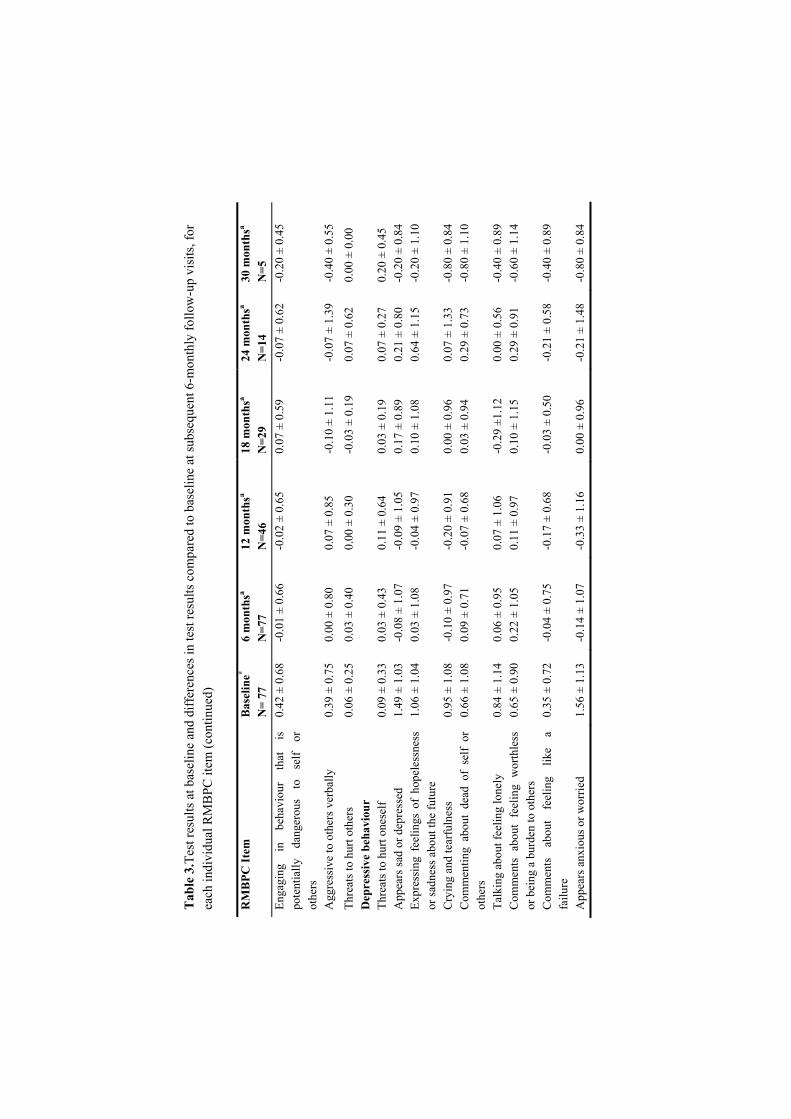
Baseline characteristics are summarised in table 1. Included patients had a mean age of 78.2 years, a mean baseline MMSE score of 20.4, 69% was female and patients lived primarily at home. Mean MAD of rivastigmine was 8.8 mg (range: 1.5 –12.0 mg). Table 2. Test results at baseline and differences in test results compared with baseline at subsequent 6-monthly follow-up visits. Test Statistics Baseline* 6 monthsa 12 monthsa 18 monthsa 24 monthsa 30 monthsa
N 84 83j 52 34 18 7 Mean± SD 20.4 ±4.4 0.1±3.1 -0.9±3.3 -1.8±3.8 -1.5±3.3 -2.9±2.3
MMSEb
range 8-28 -11-+7 -8-+9 -9-+6 -7-+3 -6-0 N 84 83j 52 34 15 7 Mean± SD 68.8±13.1 0.5±6.3 -1.2±8.3 -1.8±9.8 -3.4±10.0 -7.9±6.9
CAMCOGc
range 33-92 -15-+13 -17-+17 -20-+20 -27-+15 -17-+4 CAMCOG N 84 83j 52 34 15 7 Memd Mean ± SD 17.4±5.5 -0.5±3.4 -2.0±4.2 -1.6±4.7 -2.4±5.3 -4.9±4.8 range 5-29 -10-+8 -9-+8 -12-+10 -13-+5 -11-+2 CAMCOG N 84 83j 52 34 15 7 Nonmeme Mean ± SD 51.5±9.3 0.9±4.6 0.7±5.8 -0.1±6.7 -1.3±6.8 -2.9±2.5 range 25-67 -9-+16 -13-+15 -18-+15 -21-+10 -6-+2 IDDDf N 79 79 45 30 16 6 Mean± SD 14.0±8.8 0.7±5.9 2.7±7.8 4.5±10.1 5.7±10.1 3.7±11.6 range 0-36 -18-+13 -16-+21 -18-+22 -9-+28 -14-+19 RMBPC N 77 77 46 29 14 5
memg Mean± SD 17.1±3.9 -0.4±4.3 -0.5±5.6 +0.4±5.3 +1.0±4.3 -1.2±1.6 range 8-26 -10-+9 -13-+12 -14-+9 -7-+9 -3-+1 RMBPC N 77 77 46 29 14 5 dish Mean± SD 4.3±3.6 -0.5±2.6 -0.4±3.5 -0.6±2.7 -0.8±2.9 -1.0±2.1 range 0-18 -9-+7 -9-+8 -6-+5 -4-+7 -4-+2 RMBPC N 77 77 46 29 14 5 depi Mean±SD 7.7±5.7 +0.2±4.6 -0.8±4.8 -0.5±4.5 1.9±4.2 -4.0±4.8 range 0-21 -10-+12 -12-+9 -12-+11 -3-+10 -10-+1 *Lower baseline MMSE/CAMCOG scores / higher baseline IDDD/RMBPC scores represent worse cognitive performance, functional performance or behaviour, aNegative differences reflect improvement on IDDD/RMBPC and deterioration on MMSE/CAMCOG, brange 0-30, crange 0-107, dmemory subsection: range 0-37, enon-memory subsection: range 0-70, frange 0-44, gmemory subscale: range 0-28, hdisruptive behaviour subscale: range 0-32, idepression subscale: range 0-36, jresult of 1 patient is missing
Neuropsychological assessment during follow-up Results of neuropsychological assessment at baseline and differences compared to baseline, during follow-up until 30 months, are summarised in table 2. It is shown that group sizes diminish gradually at subsequent follow-up visits. Discontinuation of therapy was mostly due to ongoing decline measured by clinimetrics. Other reasons for discontinuation included occurrence of adverse events, transfer to a nursing home and refusing to take rivastigmine.

Treatment effects of rivastigmine
87
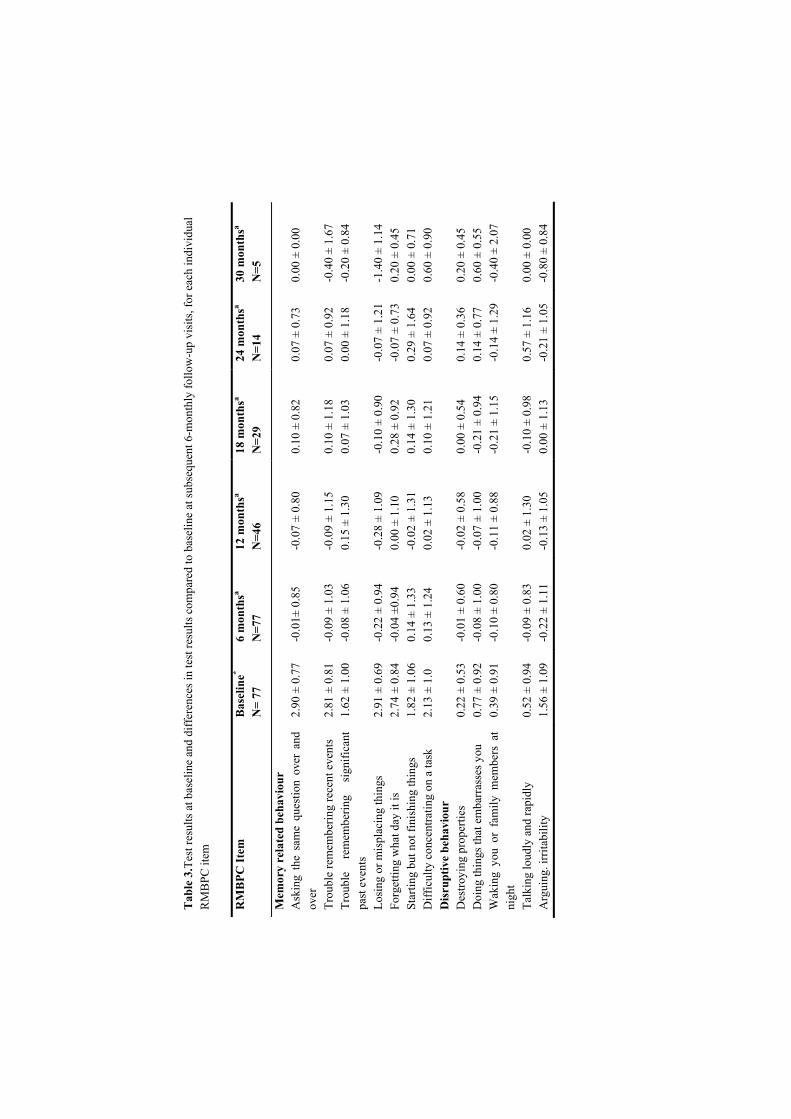
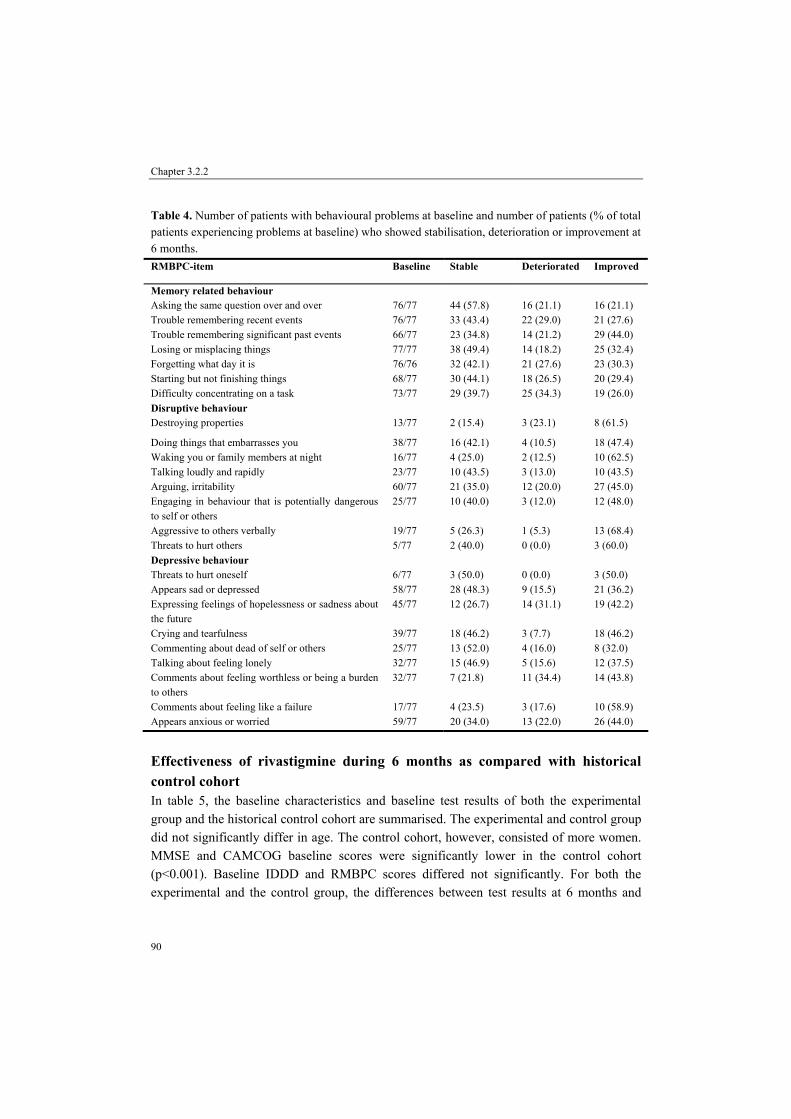
In table 2, it is shown that therapy resulted in an initial stabilisation (MMSE) or even improvement (total and non-memory section of CAMCOG) of cognition, but thereafter a slow and gradual decline during follow-up. However, the memory section of the CAMCOG showed no initial stabilisation or improvement. Performance of daily living activities (IDDD) showed a gradual decline during follow-up. The memory subsection of the RMBPC showed an initial stabilisation and thereafter a gradual decline. The disruptive subsection of the behaviour scale showed an initial improvement, which stabilises during follow-up. The depression subscale, however, showed an initial increase of depressive symptoms and thereafter an decrease of these symptoms. In table 3 are shown the test results at baseline and differences in test results compared to baseline during 30 months for each RMBPC item. Memory related behaviour disturbances are most apparent, followed by depression and disruptive behaviour. Remarkable are the items “Appears sad or depressed”, “ Appears anxious or worried” and “Arguing, irritability”. From this table, it is clear that during 30 months, numerous items remain stable. However, improvement is shown during 30 months on “losing or misplacing things”, “waking you or your family members at night”, “ arguing, irritability”, “ crying and tearfulness”, “comments about feeling like a failure” and “appears anxious or worried” A separate analysis was carried out in subgroups of patients in whom behavioural problems were present at baseline. The results of this analysis after 6 months are summarised in table 4. The percentage of patients who deteriorated is small for the disruptive behaviour items; a large proportion of patients improved actually. For the depression items also, a minor part of the patients deteriorated; exceptions here are “expressing feelings of hopelessness or sadness about the future” and “comments about feeling worthless or being a burden to others”. For the depression subsection, large number of patients remained stable. For the memory-related behaviour items, around a half of patients remained stable, whereas approximately a quarter deteriorated and a quarter improved at 6 months. Of the patients who initially did not show behavioural problems, the memory-associated behaviour items deteriorated in approximately 50% of patients, the disruptive items deteriorated in around 10% of patients with exception for “doing things that embarrasses you” (25%) and “aggressive to others verbally”(20%) and “arguing” (50%). The depression subitems deteriorated in approximately 25%, with exceptions for “comments about feeling like a failure” (10%) and “appears sad or depressed” (50%) and threats to hurt oneself (7%).
Tab
le 3
.Tes
t res
ults
at b
asel
ine
and
diff
eren
ces i
n te
st re
sults
com
pare
d to
bas
elin
e at
subs
eque
nt 6
-mon
thly
follo
w-u
p vi
sits
, for
eac
h in
divi
dual
R
MB
PC it
em
RM
BPC
Item
B
asel
ine*
N=
77
6 m
onth
sa
N=7
7 12
mon
thsa
N=4
6 18
mon
thsa
N=2
9 24
mon
thsa
N=1
4 30
mon
thsa
N=5
Mem
ory
rela
ted
beha
viou
r
A
skin
g th
e sa
me
ques
tion
over
and
ov
er
2.90
± 0
.77
-0.0
1± 0
.85
-0.0
7 ±
0.80
0.
10 ±
0.8
2 0.
07 ±
0.7
3 0.
00 ±
0.0
0
Trou
ble
rem
embe
ring
rece
nt e
vent
s 2.
81 ±
0.8
1 -0
.09
± 1.
03
-0.0
9 ±
1.15
0.
10 ±
1.1
8 0.
07 ±
0.9
2 -0
.40
± 1.
67
Trou
ble
rem
embe
ring
sign
ifica
nt
past
eve
nts
1.62
± 1
.00
-0.0
8 ±
1.06
0.
15 ±
1.3
0 0.
07 ±
1.0
3 0.
00 ±
1.1
8 -0
.20
± 0.
84
Losi
ng o
r mis
plac
ing
thin
gs
2.91
± 0
.69
-0.2
2 ±
0.94
-0
.28
± 1.
09
-0.1
0 ±
0.90
-0
.07
± 1.
21
-1.4
0 ±
1.14
Fo
rget
ting
wha
t day
it is
2.
74 ±
0.8
4 -0
.04
±0.9
4 0.
00 ±
1.1
0 0.
28 ±
0.9
2 -0
.07
± 0.
73
0.20
± 0
.45
Star
ting
but n
ot fi
nish
ing
thin
gs
1.82
± 1
.06
0.14
± 1
.33
-0.0
2 ±
1.31
0.
14 ±
1.3
0 0.
29 ±
1.6
4 0.
00 ±
0.7
1 D
iffic
ulty
con
cent
ratin
g on
a ta
sk
2.13
± 1
.0
0.13
± 1
.24
0.02
± 1
.13
0.10
± 1
.21
0.07
± 0
.92
0.60
± 0
.90
Dis
rupt
ive
beha
viou
r
D
estro
ying
pro
perti
es
0.22
± 0
.53
-0.0
1 ±
0.60
-0
.02
± 0.
58
0.00
± 0
.54
0.14
± 0
.36
0.20
± 0
.45
Doi
ng th
ings
that
em
barr
asse
s you
0.
77 ±
0.9
2 -0
.08
± 1.
00
-0.0
7 ±
1.00
-0
.21
± 0.
94
0.14
± 0
.77
0.60
± 0
.55
Wak
ing
you
or f
amily
mem
bers
at
nigh
t 0.
39 ±
0.9
1 -0
.10
± 0.
80
-0.1
1 ±
0.88
-0
.21
± 1.
15
-0.1
4 ±
1.29
-0
.40
± 2.
07
Talk
ing
loud
ly a
nd ra
pidl
y 0.
52 ±
0.9
4 -0
.09
± 0.
83
0.02
± 1
.30
-0.1
0 ±
0.98
0.
57 ±
1.1
6 0.
00 ±
0.0
0 A
rgui
ng. i
rrita
bilit
y
1.56
± 1
.09
-0.2
2 ±
1.11
-0
.13
± 1.
05
0.00
± 1
.13
-0.2
1 ±
1.05
-0
.80
± 0.
84
Tab
le 3
.Tes
t res
ults
at b
asel
ine
and
diff
eren
ces i
n te
st re
sults
com
pare
d to
bas
elin
e at
subs
eque
nt 6
-mon
thly
follo
w-u
p vi
sits
, for
ea
ch in
divi
dual
RM
BPC
item
(con
tinue
d)
RM
BPC
Item
B
asel
ine*
N=
77
6 m
onth
sa
N=7
7 12
mon
thsa
N=4
6 18
mon
thsa
N=2
9 24
mon
thsa
N=1
4 30
mon
thsa
N=5
En
gagi
ng
in
beha
viou
r th
at
is
pote
ntia
lly
dang
erou
s to
se
lf or
ot
hers
0.42
± 0
.68
-0.0
1 ±
0.66
-0
.02
± 0.
65
0.07
± 0
.59
-0.0
7 ±
0.62
-0
.20
± 0.
45
Agg
ress
ive
to o
ther
s ver
bally
0.
39 ±
0.7
5 0.
00 ±
0.8
0
0.07
± 0
.85
-0.1
0 ±
1.11
-0
.07
± 1.
39
-0.4
0 ±
0.55
Thre
ats t
o hu
rt ot
hers
0.
06 ±
0.2
5 0.
03 ±
0.4
0 0.
00 ±
0.3
0 -0
.03
± 0.
19
0.07
± 0
.62
0.00
± 0
.00
Dep
ress
ive
beha
viou
r
Th
reat
s to
hurt
ones
elf
0.09
± 0
.33
0.03
± 0
.43
0.11
± 0
.64
0.03
± 0
.19
0.07
± 0
.27
0.20
± 0
.45
App
ears
sad
or d
epre
ssed
1.
49 ±
1.0
3 -0
.08
± 1.
07
-0.0
9 ±
1.05
0.
17 ±
0.8
9 0.
21 ±
0.8
0 -0
.20
± 0.
84
Expr
essi
ng f
eelin
gs o
f ho
pele
ssne
ss
or sa
dnes
s abo
ut th
e fu
ture
1.
06 ±
1.0
4 0.
03 ±
1.0
8 -0
.04
± 0.
97
0.10
± 1
.08
0.64
± 1
.15
-0.2
0 ±
1.10
Cry
ing
and
tear
fuln
ess
0.95
± 1
.08
-0.1
0 ±
0.97
-0
.20
± 0.
91
0.00
± 0
.96
0.07
± 1
.33
-0.8
0 ±
0.84
C
omm
entin
g ab
out
dead
of
self
or
othe
rs
0.66
± 1
.08
0.09
± 0
.71
-0.0
7 ±
0.68
0.
03 ±
0.9
4 0.
29 ±
0.7
3 -0
.80
± 1.
10
Talk
ing
abou
t fee
ling
lone
ly
0.84
± 1
.14
0.06
± 0
.95
0.07
± 1
.06
-0.2
9 ±1
.12
0.00
± 0
.56
-0.4
0 ±
0.89
C
omm
ents
abo
ut f
eelin
g w
orth
less
or
bei
ng a
bur
den
to o
ther
s 0.
65 ±
0.9
0 0.
22 ±
1.0
5 0.
11 ±
0.9
7 0.
10 ±
1.1
5 0.
29 ±
0.9
1 -0
.60
± 1.
14
Com
men
ts
abou
t fe
elin
g lik
e a
failu
re
0.35
± 0
.72
-0.0
4 ±
0.75
-0
.17
± 0.
68
-0.0
3 ±
0.50
-0
.21
± 0.
58
-0.4
0 ±
0.89
App
ears
anx
ious
or w
orrie
d 1.
56 ±
1.1
3 -0
.14
± 1.
07
-0.3
3 ±
1.16
0.
00 ±
0.9
6 -0
.21
± 1.
48
-0.8
0 ±
0.84
Chapter 3.2.2
90
Table 4. Number of patients with behavioural problems at baseline and number of patients (% of total patients experiencing problems at baseline) who showed stabilisation, deterioration or improvement at 6 months. RMBPC-item Baseline Stable Deteriorated Improved
Memory related behaviour Asking the same question over and over 76/77 44 (57.8) 16 (21.1) 16 (21.1) Trouble remembering recent events 76/77 33 (43.4) 22 (29.0) 21 (27.6) Trouble remembering significant past events 66/77 23 (34.8) 14 (21.2) 29 (44.0) Losing or misplacing things 77/77 38 (49.4) 14 (18.2) 25 (32.4) Forgetting what day it is 76/76 32 (42.1) 21 (27.6) 23 (30.3) Starting but not finishing things 68/77 30 (44.1) 18 (26.5) 20 (29.4) Difficulty concentrating on a task 73/77 29 (39.7) 25 (34.3) 19 (26.0) Disruptive behaviour Destroying properties 13/77 2 (15.4) 3 (23.1) 8 (61.5)
Doing things that embarrasses you 38/77 16 (42.1) 4 (10.5) 18 (47.4) Waking you or family members at night 16/77 4 (25.0) 2 (12.5) 10 (62.5) Talking loudly and rapidly 23/77 10 (43.5) 3 (13.0) 10 (43.5) Arguing, irritability 60/77 21 (35.0) 12 (20.0) 27 (45.0) Engaging in behaviour that is potentially dangerous to self or others
25/77 10 (40.0) 3 (12.0) 12 (48.0)
Aggressive to others verbally 19/77 5 (26.3) 1 (5.3) 13 (68.4) Threats to hurt others 5/77 2 (40.0) 0 (0.0) 3 (60.0) Depressive behaviour Threats to hurt oneself 6/77 3 (50.0) 0 (0.0) 3 (50.0) Appears sad or depressed 58/77 28 (48.3) 9 (15.5) 21 (36.2) Expressing feelings of hopelessness or sadness about the future
45/77 12 (26.7) 14 (31.1) 19 (42.2)
Crying and tearfulness 39/77 18 (46.2) 3 (7.7) 18 (46.2) Commenting about dead of self or others 25/77 13 (52.0) 4 (16.0) 8 (32.0) Talking about feeling lonely 32/77 15 (46.9) 5 (15.6) 12 (37.5) Comments about feeling worthless or being a burden to others
32/77 7 (21.8) 11 (34.4) 14 (43.8)
Comments about feeling like a failure 17/77 4 (23.5) 3 (17.6) 10 (58.9) Appears anxious or worried 59/77 20 (34.0) 13 (22.0) 26 (44.0)
Effectiveness of rivastigmine during 6 months as compared with historical control cohort In table 5, the baseline characteristics and baseline test results of both the experimental group and the historical control cohort are summarised. The experimental and control group did not significantly differ in age. The control cohort, however, consisted of more women. MMSE and CAMCOG baseline scores were significantly lower in the control cohort (p<0.001). Baseline IDDD and RMBPC scores differed not significantly. For both the experimental and the control group, the differences between test results at 6 months and

Treatment effects of rivastigmine
91
baseline and effect sizes are also presented in table 5. All domains, except disruptive behaviour showed significant and clinical detectable differences between rivastigmine users and controls. Rivastigmine users showed stabilisation on MMSE and a slight improvement on the CAMCOG, whereas controls significantly deteriorated on both tests (p<0.001). Performance (IDDD) showed significantly less deterioration in rivastigmine users compared to the control group (p<0.001). Rivastigmine significantly improved memory-related behaviour (p<0.05) and non-significantly disruptive behaviour. Depression, however, significantly worsened during rivastigmine use compared with controls where this diminished (p<0.001). Table 5. Baseline characteristics and assessment results of rivastigmine users and historical controls, differences in assessment results between 6 months and baseline of rivastigmine users and historical controls and effect sizes of rivastigmine treatment after 6 months.
Baseline characteristics /Assessment scores (mean (SD))*
Differences in assessment scores between six months and baseline (mean (SD))a
Effect sizea Characteristics / Assessment scales
RIVAi
(n=84) Controls (n=69)
p-value
RIVAi (n=84)
Controls (n=69)
p-value
Cohen’s d
SRMb
Age 78.2 (6.0) 78.3 (6.2) 0.773 Gender, female 69% 81% MMSEc 20.4 (4.4) 17.5 (5.4) <0.001 0.1 (3.1) -1.6 (3.1) <0.001 0.35 0.55 CAMCOGd 68.8 (13.1) 61.0 (16.6) <0.001 0.5 (6.3) -4.5 (6.5) <0.001 0.33 0.78 IDDD-performancee
14.0 (8.8) 12.5 (8.5) 0.146 0.7 (5.9) 4.4 (7.7) <0.001 -0.43 -0.54
RMBPC memf 17.1 (3.9) 17.4 (5.8) 0.468 -0.4 (4.3) 1.0 (5.4) 0.006 -0.28 -0.28 RMBPC disg 4.3 (3.9) 4.2 (4.3) 0.786 -0.5 (2.6) -0.2 (3.9) 0.369 -0.07 -0.09 RMBPC deph 7.7 (5.7) 8.4 (6.1) 0.259 0.2 (4.6) -1.6 (5.0) 0.001 0.30 0.37 *Lower baseline MMSE/CAMCOG scores / higher baseline IDDD/RMBPC scores represent worse cognitive performance, functional performance or behaviour, aNegative differences/effect sizes reflect improvement on IDDD/RMBPC and deterioration on MMSE/CAMCOG, Standardized Response Mean, crange 0-30, drange 0-107, erange 0-44, f memory subscale: range 0-28, g disruptive behaviour subscale: range 0-32, h depression subscale: range 0-36, I Rivastigmine
If the follow-up results of the treated cohort are compared with those of the historical control cohort, it can be seen that decline as shown in 6 months in untreated controls is comparable with decline in treated patients in 18 months as measured on scales for cognition (MMSE) and activities of daily living (ADL) or 24 months as measured on scales for cognition (CAMCOG) and memory associated disturbances in behaviour.
Discussion In a cohort of Alzheimer patients, rivastigmine shows a significant but modest clinically detectable effect on cognition, performance in daily living and the memory part of the behaviour scale during 26 weeks compared with a historical control group of Alzheimer

Chapter 3.2.2
92
patients. Disruptive behaviour was not significantly altered and depressive behaviour worsened slightly. During 30 months, rivastigmine users showed stabilisation compared with baseline test results on numerous RMBPC items. Improvement was shown on a number of depression and disruptive behaviour subitems in particular. Baseline assessment results were not significantly different for the IDDD and all subsections of the RMBPC, and therefore rivastigmine effectiveness after 6 months can be easily interpreted. On the contrary, baseline assessment results differed significantly for both MMSE and CAMCOG. Although rivastigmine showed a significant and clinical detectable effect after 6 months on cognition, this should be interpreted with caution. MMSE scores can be subdivided into no cognitive impairment (24-30), mild cognitive impairment (18-23) and severe cognitive impairment (0-17)25. The control cohort may present a more advanced state of cognitive impairment and this might result in a different rate of cognitive decline compared with the experimental group of rivastigmine users. Therefore, the shown effectiveness can possibly not be attributed solely to rivastigmine use. A review by Grossberg described effects of rivastigmine on behaviour. A significant reduction in the frequency of aggressiveness as compared with placebo was shown after 6 months treatment26. In nursing home patients significant improvement was shown after 52 weeks for hallucinations, anxiety, euphoria, apathy, disinhibition, irritability, aberrant motor behaviour, nighttimes behaviour and appetite/eating change among patients with these symptoms at baseline11. In another study, in a population of nursing home patients 26 weeks of rivastigmine showed improvement of anxiety in 56% of patients showing disturbances at baseline, improvement of irritability in 66% of patients and also nighttime disturbances improved in 82% of patients13. Our cohort study showed after that 26 weeks of rivastigmine treatment, around 45% of patients with symptoms present at baseline improved for irritability and anxiety and in 62% of patients improvement of nighttime behaviour was shown. It must be pointed out also that in the studied cohort, only six patients did not receive daily doses above 6 mg. A meta-analysis showed a relation between efficacy and rivastigmine dose27. The shown effectiveness in our cohort may therefore be only representative for doses of rivastigmine above 6 mg daily. In addition, in the studied cohort, no relation was found between dose of rivastigmine and effectiveness in the three studied domains (results not shown). Our experimental cohort shows initial improvement of cognition as well as initial worsening of depressive symptoms. A possible relation could be hypothesised. Lopez et al. 28 did not find a difference in presence of depression between patients who were aware of their cognitive deficits and those who were not. Harwood et al.29 however, found a positive relation between greater insight and more depressive symptoms.

Treatment effects of rivastigmine
93
Dementia may put a burden on relatives and the health system30, and therefore, it is of primary importance if symptomatic therapy could delay deterioration in cognition, performance and behaviour. In this study, rivastigmine therapy shows a 12-18 months delay in deterioration of ADL, cognition and memory-associated behaviour compared with the historical control cohort. However, a positive bias is introduced. Responders to rivastigmine continue therapy after the first follow-up evaluation at 6 months, while others discontinue therapy, because of non-response. Therefore, only in initial responders therapy could postpone cognitive and functional deterioration with 1 - 1.5 years. In addition, because only 6-month data are available of the control cohort, a direct comparison cannot be made. However, a dropout study suggested an effect of rivastigmine on disease progression31. Moreover, a huge bias is introduced during the first period of 6 months of treatment. Rivastigmine shows more adverse events as compared to donepezil32. A large drop-out rate is the result, which is also apparent in our cohort. So only in initial survivors up to the first follow-up visit after 6 months, rivastigmine effectiveness is measured and in the sub cohort of responders, therapy is continued.
Our results show a gradual decline up to 30 months after treatment initiation. However, the long-term results of our cohort are purely descriptive in nature. Long-term effects of rivastigmine and other cholinesterase inhibitors remain largely unknown. Studies following patients beyond 12 months are scarce and descriptive in nature and placebo responses are sometimes modelled6,33. Lopez-Lousa et al.3 reported great variability in treatment response between rivastigmine users. Our results confirm this. A wide range of differences in scores between follow-up assessments and baseline scores was shown during the complete follow-up period. Rockwood and MacKnight34 proposed cholinesterase inhibitor users to be subdivided into a group of responders, a group of non-responders and a group remaining at equivocal results at retesting. In the future, more research should be performed to identify these subgroups and make it ideally possible to identify individual patients in routine clinical care as a responder or not. If it is possible to identify patients as responders or non-responders, therapy should be initiated only in patients who fulfil the characteristics for a responder. The non-responders will be spared then from the frequently occurring adverse events. Moreover, even a part of the identified responders will experience adverse events and some patients will possible discontinue therapy before the initial follow-up visit at 6 months. However, it is currently unclear which characteristics define the (long-term) rivastigmine responders, and therefore all patients should be offered therapy, as it is unethical to withdraw a possible effective therapy from patients. Strengths of our study are a relatively large population in a naturalistic setting, a total follow-up time of 30 months and full accessibility to all relevant clinical data. This study is

Chapter 3.2.2
94
an example of rivastigmine monitoring in clinical practice and could serve as a model for other memory clinics. The scales that are used are easy to apply and cover a wide range of domains; both memory and non-memory cognitive function, performance in daily living, memory, disruptive and depressive behaviour are assessed. Monitoring rivastigmine effectiveness in different domains is an advantage over only using the MMSE as instrument to monitor treatment effects. The use of CAMCOG, IDDD and RMBPC in clinical practice is not highly time-consuming, as CAMCOG screening takes about on average 30 minutes only, and in the meantime, proxies are able to fill in the IDDD and RMBPC questionnaires. It is important that the same proxy accompanies the patient every follow-up visit. An unacceptable low level of agreement was found between primary and secondary informants on the RMBPC. The RMBPC, however, is very useful for longitudinal follow-up as it showed an acceptable test-retest agreement and did not show a ceiling effect35. The CAMCOG evaluates a broad range of cognitive functions that are often affected in dementia and thus an advantage over brief screening tests16. Previous research showed this instruments’ utilities for assessing and monitoring cognitive decline in moderate and moderately severe dementia patients36. Ceiling effects are not supposed when using CAMCOG for cognitive evaluation in AD, as it showed little ceiling effect when used in the non-demented elderly37 and appeared to be sensitive to the early stages of dementia38. The IDDD, developed for community-dwelling dementia patients, has a high internal consistency and all the activities that are mentioned in this instrument are relevant and applicable to both men and women18. Our results show that the non-memory section of the CAMCOG, consisting of items regarding for example attention, praxis, abstract reasoning and perception, initially improved, whereas the memory section initially deteriorated in the rivastigmine group. As we performed a cohort study without a placebo group the results may be shaded in this descriptive open-label setting and future research should focus on investigating and confirming this further. Identification of responders is also of primary importance and should be involved in future research. In conclusion, a huge discontinuation rate is experienced within the first half year of treatment. In the subpopulation of patients who continued rivastigmine for 6 months, it shows modest, significant effectiveness on cognition, functionality and memory associated behaviour as compared with historical control patients. Unfortunately, disruptive behaviour is not significantly altered by rivastigmine therapy and depressive behaviour increased slightly after initial treatment. During 30 months, rivastigmine showed stabilisation on numerous behaviour items as measured by the RMBPC.

Treatment effects of rivastigmine
95
References 1. Corey-Bloom J, Anand R, Veach J. A randomized trial evaluating the efficacy and safety of ENA 713
(rivastigmine tartrate), a new acetylcholinesterase inhibitor, in patients with mild to moderately severe Alzheimer’s disease. Int J Geriatr Psychopharmacol 1998; 1:55-65.
2. Rösler M, Anand R, Cicin-Sain A, et al. Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: international randomized controlled trial. BMJ 1999;318:633-638.
3. Lopez-Pousa S, Turon-Estrada A, Garre-Olmo J, et al. Differential efficacy of treatment with acetylcholinesterase inhibitors with mild and moderate Alzheimer’s disease over a 6-month period. Dement Geriatr Cogn Disord 2005;19:189-195.
4. Mossello E, Tonon E, Caleri V, et al. Effectiveness and safety of cholinesterase inhibitors in elderly subjects with Alzheimer’s disease: a “real world” study. Arch Gerontol Geriatr 2004; 9:S297-S307.
5. Small GW, Kaufer D, Mendiondo MS, et al. Cognitive performance in Alzheimer’s disease patients receiving rivastigmine for up to 5 years. Int J Clin Pract 2005;59:473-77.
6. Johanssen P. Long-term cholinesterase inhibitor treatment of Alzheimer’s disease. CNS Drugs 2004; 18:757-768.
7. Wynn ZJ, Cummings JL. Cholinesterase inhibitor therapies and neuropsychiatric manifestations of Alzheimer’s disease. Dement Geriatr Cogn Disord 2004;17:100-108.
8. Lane RM, Potkin SG, Enz A. Targeting acetylcholinesterase and butyrylcholinesterase in dementia. Int J Neuropsychopharmacol 2006;9:101-124.
9. Rösler M, Retz W, Retz-Junginger P, Dennler HJ. Effects of two-year treatment with the cholinesterase inhibitor rivastigmine on behavioural symptoms in Alzheimer’s disease. Behav Neurol 1998;11:211-216.
10. Finkel SI. Effects of rivastigmine on behavioral and psychological symptoms of dementia in Alzheimer’s disease. Clin Ther 2004; 26:980-990.
11. Aupperle PM, Koumaras B, Chen M, et al. Long-term effects of rivastigmine treatment on neuropsychiatric and behavioural disturbances in nursing home residents with moderate to severe Alzheimer’s disease: results of a 52-week open-label study. Curr Med Res Opin 2004; 20:1605-1612.
12. Hatoum HT, Lin SJ, Arcona S, et al. The use of the occupational disruptiveness scale of the neuropsychiatric inventory-nursing home version to measure the impact of rivastigmine on the disruptive behaviour of nursing home residents with Alzheimer’s disease. J Am Med Dir Assoc 2005; 6:238-245.
13. Cummings JL, Koumaras B, Chen M, et al. Effects of rivastigmine treatment on the neuropsychiatric and behavioral disturbances of nursing home residents with moderate to severe probable Alzheimer’s disease: a 26-week, multicenter, open-label study. Am J Geriatr Pharmacother 2005;3:137-148.
14. McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA work group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s disease. Neurology 1984;34:939-944.
15. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state” a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189-198.
16. Roth M, Tym E, Mountjoy CQ, et al. CAMDEX A standardized instrument for the diagnosis of mental disorder in the elderly with special reference to early detection of dementia. Br J Psychiatry 1986;149:698-709.
17. Schmand B, Walstra G, Lindeboom J, Teunisse S, Jonker C. Early detection of Alzheimer’s disease using the Cambridge Cognitive Examination (CAMCOG). Psychol Med 2000;30:619-627.
18. Teunisse S, Derix MM. Measuring functional disability in community-dwelling dementia patients: development of a questionnaire (in Dutch). Tijdschr Gerontol Geriatr 1991;22:53-59.
19. Teri L, Truax P, Logsdon R, Uomoto J, Zarit S, Vitaliano PP. Assessment of behavioral problems in dementia: the revised memory and behavior problems checklist. Psychol Aging 1992;7:622-631.
20. Verhage F. Intelligence and Age (in Dutch). Assen, van Gorcum, 1964.

Chapter 3.2.2
96
21. Public Health Board. Diagnostics in Dementia (in Dutch). Amstelveen, Public Health Board, 1998. 22. Cohen J. Statistical power analysis for the behavioral sciences. New York, Academic Press, 1969. 23. Rockwood K. Size of the treatment effect on cognition of cholinesterase inhibition in Alzheimer’s disease. J
Neurol Neurosurg Psychiatry 2004;75:677-685. 24. Frankfort SV, Appels BA, de Boer A, et al. Discontinuation of rivastigmine in routine clinical practice. Int J
Geriatr Psychiatry 2005;20:1167-71. 25. Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc
1992;40:922-935. 26. Grossberg GT. Effect of rivastigmine in the treatment of behavioral disturbances associated with dementia:
review of neuropsychiatric impairment in Alzheimer’s disease. Curr Med Res Opin 2005;10:1631-1639. 27. Ritchie CW, Ames D, Clayton T, Lai R. Metaanalysis of randomized trials of the efficacy and safety of
donepezil, galantamine, and rivastigmine for the treatment of Alzheimer’s disease. Am J Geriatr Psychiatry 2004;12:358-369.
28. Lopez OL, Becker JT, Somsak D, et al. Awareness of cognitive deficits and anosognosia in probable Alzheimer’s disease. Eur Neurol 1994;34:277-282.
29. Harwood DG, Sultzer DL, Wheatly DV. Impaired insight in Alzheimer’s disease: association with cognitive deficits, psychiatric symptoms, and behavioral disturbances. Neuropsychiatry Neuropsychol Behav Neurol 2000;13:83-88.
30. Trinh NH, Hoblyn J, Mohanty S, Yaffe K. Efficacy of cholinesterase inhibitors in the treatment of neuropsychiatric symptoms and functional impairment in Alzheimer’s disease: a meta analysis. JAMA 2003;289:210-216.
31. Farlow M, Potkin S, Koumaras B, et al. Analysis of outcome in retrieved dropout patients in a rivastigmine vs placebo, 26 week, Alzheimer disease trial. Arch Neurol 2003;60:843-848.
32. Birks J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database Syst Rev 2006;25:CD005593. 33. Grossberg G, Irwin P, Satlin A, et al. Rivastigmine in Alzheimer’s disease: efficacy over two years. Am J
Geriatr Psychiatry 2004;12:420-431. 34. Rockwood K, MacKnight C. Assessing the clinical importance of statistically significant improvement in
anti-dementia drug trials. Neuroepidemiology 2001;20:51-56. 35. Teunisse S, de Haan R, Walstra GJM, et al. Behavioural problems in mild dementia: clinical relevance and
methodological evaluation of the Revised Memory and Behavioural Problems Checklist. In: Teunisse S. Clinimetrics in Dementia [Thesis]. Amsterdam: University of Amsterdam, 1997.
36. Garre-Olmo J, López-Pousa S, Vilalta-Franch J, Turon-Estrada A, Lozano-Gallego, Hernández-Ferràndiz M, et al. Neuropsychological profile of Alzheimer’s disease in women: moderate and moderately severe cognitive decline. Arch Womens Ment Health 2004;7:27-36
37. Huppert FA, Brayne C, Gill C, Paykel ES, Beardsall L. CAMCOG- A concise neuropsychological test to assist dementia diagnosis: Socio-demographic determinants in an elderly population sample. Br J Clin Psychol 1995;34:529-41.
38. Williams JG, Huppert FA, Matthews FE, Nickson J. Performance and normative values of a concise neuropsychological test (CAMCOG) in an elderly population sample. Int J Geriatr Psychiatry 2003;18:631-44

97

98
99
CHAPTER 3.2.3 Identification of responders and reactive domains to
rivastigmine in Alzheimer’s disease
S.V. Frankfort, B.A. Appels, A. de Boer, C.R.Tulner, J.P.C.M. van Campen, C.H.W. Koks, J.H. Beijnen, B.A. Schmand
Abstract Purpose Presently, it is unclear which patients suffering from Alzheimer’s Disease (AD) respond to rivastigmine and if rivastigmine acts on specific cognitive domains. The aims of this study are thus to investigate treatment effects of rivastigmine on specific cognitive domains and to find possible responsive subpopulations to rivastigmine cognitive effects. Methods Mini Mental State Examination (MMSE) and Cambridge Cognitive Examination (CAMCOG) were administered at baseline and after 6 months in 83 rivastigmine users and 96 historical controls, representing natural decline. Treatment effects on different subsections of the CAMCOG and in different subpopulations were investigated by linear regression analyses. Results Rivastigmine showed effectiveness on total CAMCOG (p<0.001), CAMCOG non-memory subsection (p<0.001) and subscales of language (p=0.002), attention/calculation (p=0.043), abstract thinking (p<0.001) and perception (p=0.031). In patients with baseline MMSE ≤19 rivastigmine showed significant and favourable effects compared to historical controls on total CAMCOG (p<0.001) and both non-memory (p<0.001) and memory subsections (p=0.002). Conclusion Rivastigmine showed primarily effectiveness on the non-memory section of the CAMCOG and patients with a baseline MMSE ≤19 appeared to show greater responses to rivastigmine compared to patients with baseline MMSE ≥20.
Pharmacoepidemiology and Drug Safety (in press)

Chapter 3.2.3
100
Introduction Rivastigmine, an acetylcholinesterase inhibitor, showed efficacy in the symptomatic treatment of mild-to-moderately severe Alzheimer’s disease (AD) in randomised placebo-controlled trials1,2. However, patients respond very differently to therapy, ranging from continuation of deterioration or maintaining baseline levels to a clear clinical effect3. Previous research showed improvement in APOE ε4 carriers treated with rivastigmine4,
more benefit of therapy in patients with a rapid rate of disease progression5,6 and an association between the occurrence of hallucinations and response to therapy, as defined by an increase of two or more points on the MMSE7. Starting therapy only in those patients in whom effect is expected would be ideal in clinical practice considered the fact that rivastigmine users often experience adverse events8.
It is presently unclear which characteristics identify rivastigmine responders. It is also uncertain if rivastigmine exerts treatment effects on certain cognitive subdomains in AD as, to our knowledge, no studies regarding this issue have been published. However, attention is one of the cognitive subdomains that indeed responded to rivastigmine therapy in a study performed in Lewy Body Disease (LBD) patients9. Therefore, attention might also specifically respond to therapy in AD patients. The aims of this study are to investigate treatment effects of rivastigmine on specific cognitive domains and to find possible responsive subpopulations to rivastigmine cognitive effects.
Methods Patients This prospective study was carried out in patients with mild-to-moderate, probable or possible AD according to the NINCDS-ADRDA criteria10. The index group consisted of patients using rivastigmine (Exelon®) via the geriatric outpatient department of a Dutch hospital. Only patients who had relatives or friends who could monitor drug intake and patients in whom therapy was evaluated after six months were included. The historical control cohort consisted of Alzheimer patients who did not take rivastigmine and were followed during a period of six months as part of a research project regarding the utility of diagnostics procedures in a memory clinic in The Netherlands11. This historical control group represents natural decline in Alzheimer’s disease. Patients were excluded if cognitive test results were incomplete. Education was scored on a seven-point scale, ranging from less than six years of elementary school (1) to a university degree (7)12.
The review board of the Slotervaart Hospital, Amsterdam, The Netherlands, approved the use of routine anonymous neuropsychological assessment data for research purposes.

Reactive domains and responders to rivastigmine
101
Assessment of domains At baseline, i.e. when starting rivastigmine in case of the index group, and after six months patients were evaluated by cognitive assessment including Mini Mental State Examination (MMSE; max score 30)13 and Cambridge Cognitive Examination (CAMCOG)14. CAMCOG consists of 60 items and total sum scores range from 0-107. CAMCOG can be subdivided into a memory (maximum score 37) and a non-memory (maximum score 70) section15. The memory subsection can be further subdivided into subscales regarding recent memory (max score: four), remote memory (max score: six), learning (max score: 17) and orientation (max score: 10). The non-memory subsection can be subdivided into subscales assessing language (max score: 30), praxis (max score: 12), attention/calculation (max score: nine), abstract thinking (max score: eight) and perception (max score: 11). One item in the CAMCOG perception subscale (asking if the respondent recognised two people in the room) was omitted and always scored as one point. Lower scores on MMSE and CAMCOG reflect more severe disease. Statistical analysis A) We performed linear regression analyses to investigate rivastigmine effectiveness on cognition compared to the historical control cohort during 6 months as measured by MMSE, CAMCOG and subsections and subscales of the CAMCOG. The dependent variable was the test result after 6 months and the independent variable was rivastigmine use. B) We investigated whether effect modification plays a role by introducing interaction terms in linear regression analyses regarding CAMCOGtotal, non-memory and memory subsections and the attention subscale. Therefore, we sequentially performed multivariate linear regression analyses including the interaction term rivastigmine by dichotomised disease severity, in addition to both terms separately. As an indicator for disease severity, the baseline MMSE score was dichotomised to the median of the whole population, resulting in MMSE ≤19 versus ≥ 20. If the interaction terms showed significance, we performed additional linear regression analyses to investigate rivastigmine effects in subgroups. We corrected analyses for age, gender and level of education, as these variables may influence cognitive performance, and for baseline test results. All statistical calculations were performed with SPSS for Windows (version 11.0, SPSS Inc. ,Chicago, IL, USA).
Chapter 3.2.3
102
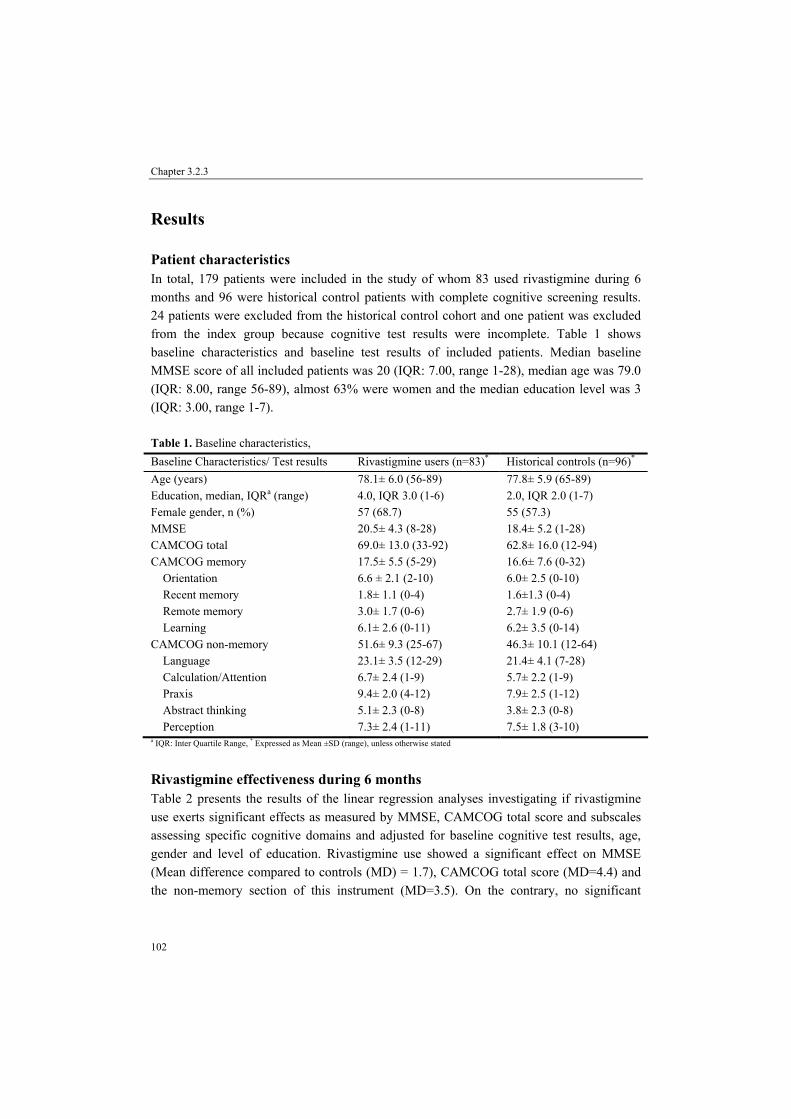
Results Patient characteristics In total, 179 patients were included in the study of whom 83 used rivastigmine during 6 months and 96 were historical control patients with complete cognitive screening results. 24 patients were excluded from the historical control cohort and one patient was excluded from the index group because cognitive test results were incomplete. Table 1 shows baseline characteristics and baseline test results of included patients. Median baseline MMSE score of all included patients was 20 (IQR: 7.00, range 1-28), median age was 79.0 (IQR: 8.00, range 56-89), almost 63% were women and the median education level was 3 (IQR: 3.00, range 1-7). Table 1. Baseline characteristics, Baseline Characteristics/ Test results Rivastigmine users (n=83)* Historical controls (n=96)*
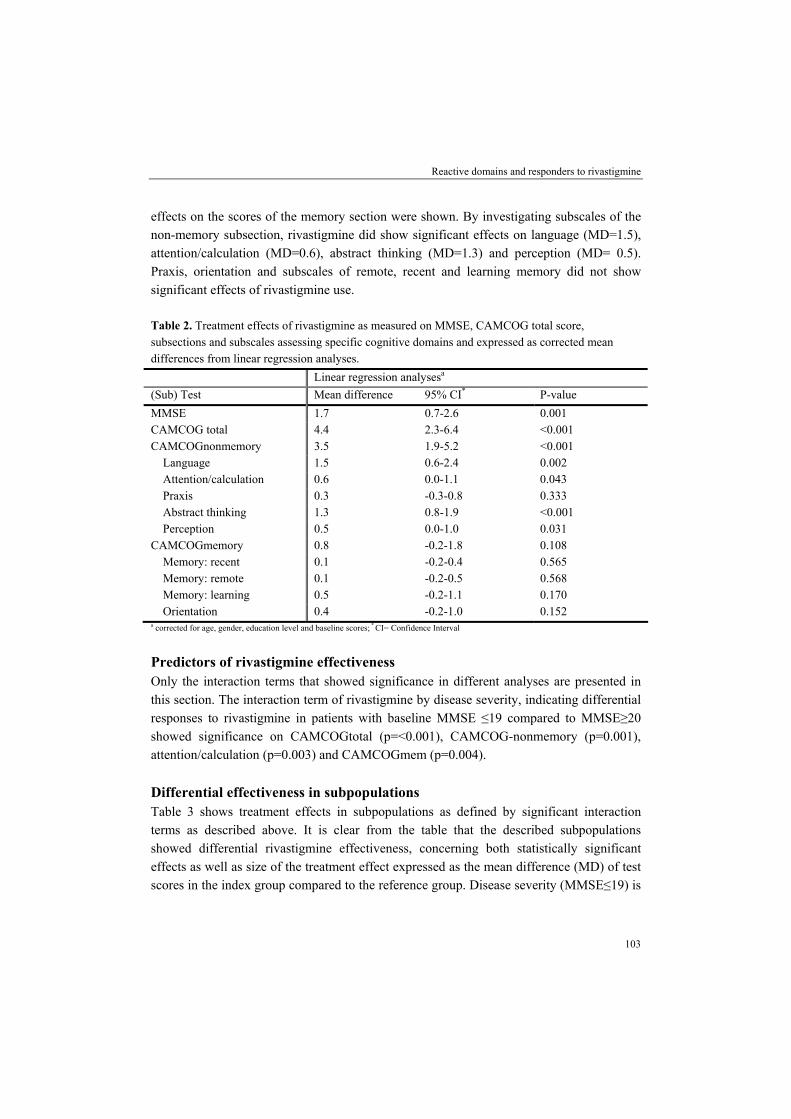
Age (years) 78.1± 6.0 (56-89) 77.8± 5.9 (65-89) Education, median, IQRa (range) 4.0, IQR 3.0 (1-6) 2.0, IQR 2.0 (1-7) Female gender, n (%) 57 (68.7) 55 (57.3) MMSE 20.5± 4.3 (8-28) 18.4± 5.2 (1-28) CAMCOG total 69.0± 13.0 (33-92) 62.8± 16.0 (12-94) CAMCOG memory 17.5± 5.5 (5-29) 16.6± 7.6 (0-32) Orientation 6.6 ± 2.1 (2-10) 6.0± 2.5 (0-10) Recent memory 1.8± 1.1 (0-4) 1.6±1.3 (0-4) Remote memory 3.0± 1.7 (0-6) 2.7± 1.9 (0-6) Learning 6.1± 2.6 (0-11) 6.2± 3.5 (0-14) CAMCOG non-memory 51.6± 9.3 (25-67) 46.3± 10.1 (12-64) Language 23.1± 3.5 (12-29) 21.4± 4.1 (7-28) Calculation/Attention 6.7± 2.4 (1-9) 5.7± 2.2 (1-9) Praxis 9.4± 2.0 (4-12) 7.9± 2.5 (1-12) Abstract thinking 5.1± 2.3 (0-8) 3.8± 2.3 (0-8) Perception 7.3± 2.4 (1-11) 7.5± 1.8 (3-10) a IQR: Inter Quartile Range, * Expressed as Mean ±SD (range), unless otherwise stated Rivastigmine effectiveness during 6 months Table 2 presents the results of the linear regression analyses investigating if rivastigmine use exerts significant effects as measured by MMSE, CAMCOG total score and subscales assessing specific cognitive domains and adjusted for baseline cognitive test results, age, gender and level of education. Rivastigmine use showed a significant effect on MMSE (Mean difference compared to controls (MD) = 1.7), CAMCOG total score (MD=4.4) and the non-memory section of this instrument (MD=3.5). On the contrary, no significant
Reactive domains and responders to rivastigmine
103
effects on the scores of the memory section were shown. By investigating subscales of the non-memory subsection, rivastigmine did show significant effects on language (MD=1.5), attention/calculation (MD=0.6), abstract thinking (MD=1.3) and perception (MD= 0.5). Praxis, orientation and subscales of remote, recent and learning memory did not show significant effects of rivastigmine use. Table 2. Treatment effects of rivastigmine as measured on MMSE, CAMCOG total score, subsections and subscales assessing specific cognitive domains and expressed as corrected mean differences from linear regression analyses. Linear regression analysesa
(Sub) Test Mean difference 95% CI* P-value
MMSE 1.7 0.7-2.6 0.001 CAMCOG total 4.4 2.3-6.4 <0.001 CAMCOGnonmemory 3.5 1.9-5.2 <0.001 Language 1.5 0.6-2.4 0.002 Attention/calculation 0.6 0.0-1.1 0.043 Praxis 0.3 -0.3-0.8 0.333 Abstract thinking 1.3 0.8-1.9 <0.001 Perception 0.5 0.0-1.0 0.031 CAMCOGmemory 0.8 -0.2-1.8 0.108 Memory: recent 0.1 -0.2-0.4 0.565 Memory: remote 0.1 -0.2-0.5 0.568 Memory: learning 0.5 -0.2-1.1 0.170 Orientation 0.4 -0.2-1.0 0.152 a corrected for age, gender, education level and baseline scores; * CI= Confidence Interval
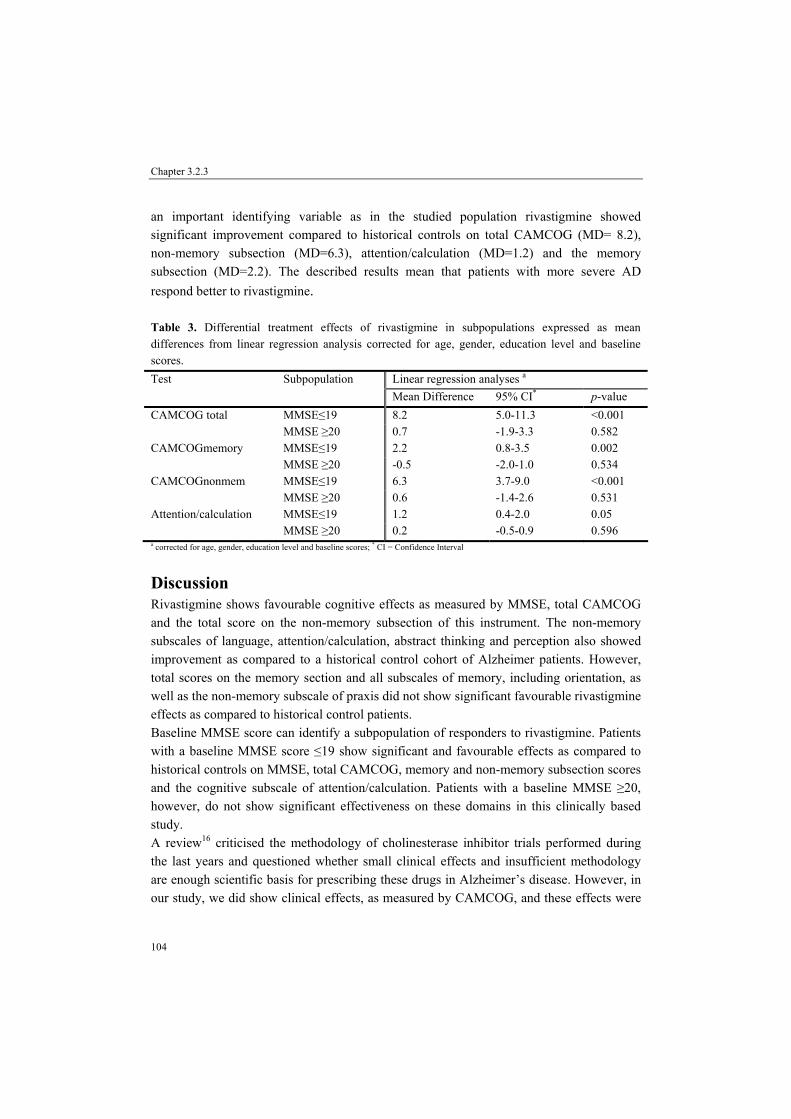
Predictors of rivastigmine effectiveness Only the interaction terms that showed significance in different analyses are presented in this section. The interaction term of rivastigmine by disease severity, indicating differential responses to rivastigmine in patients with baseline MMSE ≤19 compared to MMSE≥20 showed significance on CAMCOGtotal (p=<0.001), CAMCOG-nonmemory (p=0.001), attention/calculation (p=0.003) and CAMCOGmem (p=0.004). Differential effectiveness in subpopulations Table 3 shows treatment effects in subpopulations as defined by significant interaction terms as described above. It is clear from the table that the described subpopulations showed differential rivastigmine effectiveness, concerning both statistically significant effects as well as size of the treatment effect expressed as the mean difference (MD) of test scores in the index group compared to the reference group. Disease severity (MMSE≤19) is
Chapter 3.2.3
104
an important identifying variable as in the studied population rivastigmine showed significant improvement compared to historical controls on total CAMCOG (MD= 8.2), non-memory subsection (MD=6.3), attention/calculation (MD=1.2) and the memory subsection (MD=2.2). The described results mean that patients with more severe AD respond better to rivastigmine. Table 3. Differential treatment effects of rivastigmine in subpopulations expressed as mean differences from linear regression analysis corrected for age, gender, education level and baseline scores.
Linear regression analyses a Test Subpopulation Mean Difference 95% CI* p-value
CAMCOG total MMSE≤19 8.2 5.0-11.3 <0.001 MMSE ≥20 0.7 -1.9-3.3 0.582 CAMCOGmemory MMSE≤19 2.2 0.8-3.5 0.002 MMSE ≥20 -0.5 -2.0-1.0 0.534 CAMCOGnonmem MMSE≤19 6.3 3.7-9.0 <0.001 MMSE ≥20 0.6 -1.4-2.6 0.531 Attention/calculation MMSE≤19 1.2 0.4-2.0 0.05 MMSE ≥20 0.2 -0.5-0.9 0.596 a corrected for age, gender, education level and baseline scores; * CI = Confidence Interval
Discussion Rivastigmine shows favourable cognitive effects as measured by MMSE, total CAMCOG and the total score on the non-memory subsection of this instrument. The non-memory subscales of language, attention/calculation, abstract thinking and perception also showed improvement as compared to a historical control cohort of Alzheimer patients. However, total scores on the memory section and all subscales of memory, including orientation, as well as the non-memory subscale of praxis did not show significant favourable rivastigmine effects as compared to historical control patients. Baseline MMSE score can identify a subpopulation of responders to rivastigmine. Patients with a baseline MMSE score ≤19 show significant and favourable effects as compared to historical controls on MMSE, total CAMCOG, memory and non-memory subsection scores and the cognitive subscale of attention/calculation. Patients with a baseline MMSE ≥20, however, do not show significant effectiveness on these domains in this clinically based study. A review16 criticised the methodology of cholinesterase inhibitor trials performed during the last years and questioned whether small clinical effects and insufficient methodology are enough scientific basis for prescribing these drugs in Alzheimer’s disease. However, in our study, we did show clinical effects, as measured by CAMCOG, and these effects were

Reactive domains and responders to rivastigmine
105
more pronounced in different subpopulations. For example, in the subpopulation of more severe disease our results show a mean difference compared to control patients of 8 points on total CAMCOG scores, which is regarded a large difference in clinical practice. Our study also confirms the hypothesis of differential efficacy in cholinesterase inhibitor users3.
Our results show cognitive subdomains to respond differently to rivastigmine. Attention responds significantly and favourably and may possibly play a mediating role in effectiveness in other cognitive domains. Acetylcholine plays an important role in attentional processing and cholinergic dysfunction interferes probably indirectly with cognitive functioning via attention17. A study by Sahakian and Coull18 showed that tacrine improved attentional functions in patients with AD. In addition, rivastigmine studies performed in LBD patients, where the cholinergic deficit is probably even larger than in AD19, showed effectiveness on attention9. To our knowledge, this is the first study reporting rivastigmine differential effects in Alzheimer’s disease. However, in a trial with tacrine, a first generation cholinesterase inhibitor, patients responded significantly better compared to those receiving placebo on Alzheimer’s disease Assessment Scale-Cognition section (ADAS-Cog) items assessing recall, naming, language and word finding20,21. The differential effectiveness on cognitive domains, as our investigations showed, should be most ideally confirmed by placebo-controlled trials and/or by research using tests that are more specific. Previous research investigated rivastigmine use in more advanced Alzheimer’s disease22,23. Burns et al.23 suggested subjects with more severe disease might also benefit from rivastigmine and Kurz et al22 showed cognitive benefits to be more marked in moderate and moderately severe cohorts than the mild AD cohort. For the cholinesterase inhibitor galantamine, it was observed that patients with MMSE scores lower than 18 had a more robust response to therapy24 and similarly for another cholinesterase inhibitor, donepezil, a more robust response was noticed in patients with MMSE scores of 20 or below25. Recently, the National Institute for Health and Clinical Excellence, UK, (NICE) has issued a draft of a revised guideline that recommends donepezil, galantamine or rivastigmine to be considered only in the treatment of persons with AD of moderate severity only (MMSE 10-20)26. It is clear that disease severity may serve as a variable in identifying responsive subpopulations. A possible explanation could be a larger cholinergic deficit in more severe stages of the disease27 suggesting this subpopulation to be more responsive to cholinergic enhancement. As attention may play a key role in cognitive functioning17 and differential attentional deficits were shown in different stages of AD28, this may also attribute to a possible explanation why patients with MMSE ≤19 respond significantly better to rivastigmine therapy. Perry et al.28 investigated sustained, divided and selective attention in different severity stadia of AD. In early AD (MMSE 24-30), only selective attention showed deficits, while patients with moderately severe AD (MMSE 18-23) showed

Chapter 3.2.3
106
impairment in sustained, divided and selective attention. Finally, the rate of disease progression, as measured on scales, does not show linearity during the course of AD. A more marked change occurred in the moderate range29-31. Farlow et al.5 showed a more rapid rate of disease progression to be a predictor of rivastigmine effectiveness. This could possibly attribute to our results showing more effectiveness in more severe AD. CAMCOG evaluates a broad range of cognitive functions that are often affected in dementia.14 Although previous research showed this instruments’ utilities for assessing and monitoring cognitive decline in moderate and moderately severe patients32 and reliability of individual subscales has been reported as acceptable33, one may question the use of the CAMCOG as a monitoring instrument. Lindeboom et al.34 showed the CAMCOG to be a non-linear scale. Thus, observed score differences may possibly not represent equal differences in changes in cognition across the test’s range. In addition, it is important to keep in mind possible floor and ceiling effects of cognitive tests, which could influence the less marked changes in early and late disease. Ceiling effects, however, are not supposed when using CAMCOG for cognitive evaluation in AD, as it showed little ceiling effect when used in the non-demented elderly35 and appeared to be sensitive to the early stages of dementia36. Possible floor effects of CAMCOG screening are in our investigations of minor importance as we included few patients with low baseline CAMCOG scores. However, these results should be interpreted with caution. We did not conduct a randomised clinical trial. Our study was designed in clinical practice and included patients treated with rivastigmine and historical control patients who were untreated. Bias may have been introduced by this study design. The historical control cohort, for example, was evaluated years before the index group. As dementia care has changed over the years, this may be a confounder in our analysis. Therefore, our results should be confirmed preferably by prospective randomised controlled trials. The Investigation in the Delay to Diagnosis of AD with Exelon (InDDEx) study is currently conducted and will provide us with knowledge regarding efficacy of rivastigmine in Mild Cognitive Impairment37.
Conclusion Rivastigmine showed differential effectiveness on cognitive subdomains that is more pronounced on the non-memory subsection. In addition, disease severity can be used to identify responsive subpopulations. More severe Alzheimer’s disease, as scored by a baseline MMSE ≤19, appeared to be an important subpopulation showing more effectiveness to rivastigmine compared to patients with baseline MMSE≥20.

Reactive domains and responders to rivastigmine
107
Acknowledgements The authors would like to thank Gerard Walstra, neurologist, and Saskia Teunisse, neuropsychologist, for their permission to use the data of the historical control cohort in the described study.
References 1. Corey-Bloom J, Anand R, Veach J. A randomized trial evaluating the efficacy and safety of ENA 713
(rivastigmine tartrate), a new acetylcholinesterase inhibitor, in patients with mild to moderately severe Alzheimer’s disease. Int J Geriatr Psychopharmacol 1998;1:55-65.
2. Rösler M, Anand R, Cicin-Sain A, et al. Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: international randomised controlled trial. BMJ 1999;318:633-38.
3. Rockwood K, MacKnight C. Assessing the clinical importance of statistically significant improvement in anti-dementia drug trials. Neuroepidemiology 2001;20:51-6.
4. Farlow MR, Lane R, Kudaravalli S, He Y. Differential qualitative responses to rivastigmine in APOE ε4 carriers and non-carriers. Pharmacogenomics J 2004;4:332-5.
5. Farlow MR, Hake A, Messina J, et al. Response of patients with Alzheimer’s disease to rivastigmine treatment is predicted by the rate of disease progression. Arch Neurol 2001;58:417-22.
6. Farlow MR, Small GW, Quarg P, Krause A. Efficacy of rivastigmine in Alzheimer’s disease patients with rapid disease progression: results of a meta-analysis. Dement Geriatr Cogn Disord 2005;20:192-97.
7. Pakrasi S, Mukaetova-Ladinska EB, McKeith IG, O’Brien JT. Clinical predictors of response to acetyl cholinesterase inhibitors: experience from routine clinical use in Newcastle. Int J Geriatr Psychiatry 2003; 18:879-86.
8. Gauthier S. Cholinergic adverse events of cholinesterase inhibitors in Alzheimer’s disease. Epidemiology and management. Drugs Aging 2001;18:853-62.
9. McKeith I, Del Ser T, Spano P, et al. Efficacy of rivastigmine in dementia with Lewy Bodies: a randomized, double-blind, placebo-controlled international study. Lancet 2000;356:2031-6.
10. McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA work group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s disease. Neurology 1984;34:939-944.
11. Walstra GJ, Teunisse S, van Gool, van Crevel H. Reversible dementia in elderly patients referred to a memory clinic. J Neurol 1997;244:17-22.
12. Verhage F. Intelligence and Age. van Gorcum: Assen. (in Dutch) 1964. 13. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive
state of patients for the clinician. J Psychiatr Res 1975;12:189-198. 14. Roth M, Tym E, Mountjoy CQ, et al. CAMDEX. A standardised instrument for the diagnosis of mental
disorder in the elderly with special reference to early detection of dementia. Br J Psychiatry 1986;149:698-709.
15. Schmand B, Walstra G, Lindeboom J, et al. Early detection of Alzheimer's disease using the Cambridge Cognitive Examination (CAMCOG). Psychol Med. 2000;30:619-27.
16. Kaduszkiewicz H, Zimmermann T, Beck-Bornholdt HP, van den Bussche, H. Cholinesterase inhibitors for patients with Alzheimer’s disease: systematic review of randomised clinical trials. BMJ 2005;331:321-3.
17. Francis PT, Palmer AM, Snape M, Wilcock G. The cholinergic hypothesis of Alzheimer’s disease: a review of progress. J Neurol Neurosurg Psychiatry 1999;66:137-47.
18. Sahakian BJ, Coull JT. Nicotine and tetrahydroaminoacradine: evidence for improved attention in patients with dementia of the Alzheimer type. Drug Dev Res 1994;31:80-8.
Chapter 3.2.3
108
19. Tiraboschi P, Hansen LA, Alford M, et al. Cholinergic dysfunction in diseases with Lewy bodies. Neurology 2000;54:407-11.
20. Farlow M, Gracon SI, Hershey LA, et al. A controlled trial of tacrine in Alzheimer’s disease. JAMA 1992;268:2523-29.
21. Cummings JL. Use of cholinesterase inhibitors in clinical practice: evidence-based recommendations. Am J Geriatr Psychiatry 2003;11:131-145.
22. Kurz A, Farlow M, Quarg P, Spiegel R. Disease stage in Alzheimer’s disease and treatment effects of rivastigmine. Alzheimer Dis Assoc Disord 2004;18:123-8.
23. Burns A, Spiegel R, Quarg P. Efficacy of rivastigmine in subjects with moderately severe Alzheimer’s disease. Int J Geriatr Psychiatry 2004;19:243-9.
24. Wilcock GK, Lilienfeld S, Gaens E. Efficacy and safety of galantamine in patients with mild to moderate Alzheimer’s disease: multicentre randomised controlled trial. BMJ 2000;321:1445-9.
25. McLendon B, Murali Doraiswamy P. Defining meaningful change in Alzheimer’s disease trials: the donepezil experience. J Geriatr Psychiatry Neurol 1999;12:39-48.
26. NICE 2006/001: NICE consults on revised first draft guidance on the use of drugs to treat Alzheimer’s disease. http://www.nice.org.uk/pdf2006_001_Alz_Press_release_AD_App_ Jan06.pdf. [Accessed March 28, 2006].
27. Davis KL, Mohs RC, Marin D, et al. Cholinergic markers in elderly patients with early signs of Alzheimer’s disease. JAMA 1999;281:1401-6.
28. Perry RJ, Watson P, Hodges JR. The nature and staging of attention dysfunction in early (minimal and mild) Alzheimer’s disease: relationship to episodic and semantic memory impairment. Neuropsychologica 2000;38:252-71.
29. Morris JC, Edland S, Clarck C, et al. The consortium to establish a registry for Alzheimer’s disease (CERAD). Part IV: Rates of cognitive change in the longitudinal assessment of probable Alzheimer’s disease. Neurology 1993;43:2457-65.
30. Stern Y, Liu X, Albert M, et al. Application of a growth curve approach to modelling the progression of Alzheimer’s disease. Journal of Gerontology 1996;51A:M179-184.
31. Mendiondo MS, Wesson Ashford J, Kryscio RJ, Schmitt FA. Modelling Mini-Mental State Examination changes in Alzheimer’s disease. Statist Med 2000;19:1607-16.
32. Garre-Olmo J, López-Pousa S, Vilalta-Franch J, et al. Neuropsychological profile of Alzheimer’s disease in women: moderate and moderately severe cognitive decline. Arch Womens Ment Health 2004;7:27-36
33. Cullum S, Huppert FA, McGee M, et al. Decline across different domains of cognitive function in normal ageing: results of a longitudinal population-based study using CAMCOG. Int J Geriatr Psychiatry 2000;15:853-62.
34. Lindeboom R, Schmand B, Holman R, et al. Improved brief assessment of cognition in aging and dementia. Neurology 2004;63:543-6.
35. Huppert FA, Brayne C, Gill C, et al. CAMCOG- A concise neuropsychological test to assist dementia diagnosis: Socio-demographic determinants in an elderly population sample. Br J Clin Psychol 1995;34:529-41.
36. Williams JG, Huppert FA, Matthews FE, Nickson J. Performance and normative values of a concise neuropsychological test (CAMCOG) in an elderly population sample. Int J Geriatr Psychiatry 2003;18:631-44.
37. Farlow MR, He Y, Tekin S, et al. Impact of APOE in mild cognitive impairment. Neurology 2004;63:1898-1901.

109
110

111
CHAPTER 3.2.4 Population pharmacokinetics and pharmacodynamics of
rivastigmine and its metabolite NAP226-90 in patients with dementia
S.V. Frankfort, A.D.R. Huitema, C.R. Tulner, J.P.C.M. van Campen, J.H. Beijnen
Abstract
Objectives: To develop and evaluate a population pharmacokinetic model that describes the pharmacokinetics of rivastigmine and its metabolite NAP226-90 in elderly outpatients with dementia and to investigate the influence of demographic variables that are involved in the variability of pharmacokinetic parameters. In addition, this study also aimed to investigate the relation between pharmacokinetics and treatment efficacy. Methods: Alzheimer’s disease or Lewy Body disease outpatients using rivastigmine were included in this prospective study. Blood samples were drawn during the 6-monthly therapy evaluation visits. In a subcohort of the patients, blood samples were collected to accomplish a complete pharmacokinetic curve. Using non-linear mixed effect modelling (NONMEM), a population pharmacokinetic model was developed that described the pharmacokinetics of rivastigmine and metabolite. A pharmacokinetic-pharmacodynamic analysis was performed to investigate whether relationships exist between pharmacokinetics and therapy response. Results: From 33 patients (mean age 78.4 years), 163 plasma concentrations of both rivastigmine and NAP226-90 were available. The pharmacokinetics of both rivastigmine and metabolite were described by one-compartment models with Michaelis-Menten elimination for rivastigmine and first-order elimination for the metabolite. Volume of distribution (V1/F) was 177 L for rivastigmine and its elimination was characterised by a maximal elimination rate (Vmax/F) of 1.01 mg/h and a Michaelis Menten constant (Km) of 0.00698 mg/L. Clearance (CL/F/fm) and volume of distribution (V2/F/fm) were 126 L/h and 39.4 L, respectively, for NAP226-90, where fm represents the fraction of rivastigmine that is metabolised into NAP226-90. Interindividual variability was estimated in V1/F (70.6%), Vmax/F (14.1%), Km (65.8%), V2/F/fm (122%) and in relative bioavailability of rivastigmine (F;17.3%). Females had a 25% higher Vmax/F compared to males (p<0.01). No differences in exposure to rivastigmine or NAP226-90 were observed between responders and non-responders. Conclusion: A model was developed and evaluated that described the population pharmacokinetics of rivastigmine and NAP226-90 in geriatric outpatients with dementia. Gender was the only factor involved in the variability of pharmacokinetic parameters. No correlation could be demonstrated between the exposure to rivastigmine or NAP226-90 and effectiveness on cognition, activities in daily living or behaviour.
Submitted

Chapter 3.2.4
112
Introduction Rivastigmine (Exelon®), an acetylcholinesterase inhibitor, has shown efficacy in the symptomatic treatment of mild-to-moderate severe Alzheimer’s Disease (AD) in randomised placebo-controlled trials1,2. In Lewy Body Disease (LBD) that is clinically characterised by fluctuating cognitive impairment, attention deficits, visual hallucinations and parkinsonism, rivastigmine showed clinically improvement in behavioural symptoms3 and in memory and attention4. In LBD patients, the cholinergic deficit is probably even larger than in AD5 and this may explain why LBD patients respond more favourable to rivastigmine therapy. In addition, in the last years it is recognised that cholinergic deficits are also involved in the behavioural symptoms present in AD6 and therapy efficacy should ideally be investigated in different domains. Rivastigmine interacts with acetylcholinesterase resulting in a carbamylated complex that slowly dissociates to release active enzyme. This temporary inhibition of acetylcholinesterase (AChE), leads to an increased availability of acetylcholine in cholinergic neurons of the brain7. Increased acetylcholine availability ameliorates cognitive and behavioural disturbances8. Rivastigmine is rapidly absorbed and earlier pharmacokinetic studies revealed a bioavailability of 40% and a short elimination half-life of 2 hours. Rivastigmine is not significantly metabolised by hepatic CYP isoenzymes, but is converted by the target enzyme acetylcholinesterase into the decarbamylated metabolite NAP226-90. Thereafter, NAP226-90 may undergo N-demethylation and/or sulphate conjugation7. Although NAP226-90 itself is not pharmacodynamically active9, its concentrations correlated well with enzyme inhibition in an ex-vivo experiment in rat brain samples and plasma10. The concentration of NAP226-90 may thus better reflect the extent of enzyme inhibition than parent rivastigmine. AD patients show a highly variable response to therapy, ranging from continuation of deterioration, stabilisation of symptoms to a clear clinical beneficial effect11. It is presently unclear which characteristics identify rivastigmine responders and if therapy response is influenced by pharmacokinetic parameters. A study by Gobburu et al.12 did not find significant correlations between cognitive neuropsychological test battery scores and rivastigmine or metabolite concentrations in patients treated for 11 weeks with 1 to 6 mg bid. For donepezil, another cholinesterase inhibitor, a significant correlation was found between plasma drug concentrations and changes in the Alzheimer’s Disease Assessment Scale-Cognition subscale (ADAS-COG), Mini Mental State Examination (MMSE) and the quality of life, as reported by the patient13. In order to establish the pharmacokinetics of rivastigmine and NAP226-90 and to identify if certain patient characteristics influence the pharmacokinetic profile, a study was conducted in patients treated with rivastigmine in routine clinical practice. Furthermore, the developed

Population pharmacokinetics and pharmacodynamics of rivastigmine
113
pharmacokinetic model was used to calculate individual pharmacokinetic parameters. These pharmacokinetic parameters were linked to efficacy measures in different domains (cognition, performance of daily living activities and behaviour) in a pharmacokinetic-pharmacodynamic analysis in patients treated for a minimum of 6 months. Methods Patients This prospective study was performed at the geriatric department of the Slotervaart Hospital, Amsterdam, The Netherlands. Geriatricians prescribed rivastigmine for patients suffering from AD, diagnosed according to the NINCDS-ADRDA criteria14, or LBD as diagnosed according to the consensus criteria15. Patients started rivastigmine at 1.5 mg twice daily and doses were titrated up after intervals of minimal 2 weeks at each dose level, until the individual Maximum Achieved Dose (MAD) with a maximum of 6 mg twice daily. However, as it was shown that doses below twice daily 3 mg are associated with lower efficacy in retaining cognition, performance and behaviour1,2, doses should be equal or higher than twice daily 3 mg. In the clinical setting rivastigmine was discontinued within the first 6 months of treatment if titration to doses equal or higher than 3 mg bid failed because of intolerance. Rivastigmine effects on cognition, activities of daily living and behaviour was evaluated after 6 months of therapy, when patients were on their individual MAD, and subsequently at 6-months intervals. Patients were recruited at those 6-monthly follow-up visits at the hospital. Only patients who had relatives or friends who could monitor drug intake were included. The study protocol was approved by the Institutional Review Board of the Slotervaart Hospital, Amsterdam, The Netherlands. Written informed consent was obtained from each participant in this study. Sampling and bioanalysis Patients were admitted to the hospital for the assessment of a pharmacokinetic curve of rivastigmine and NAP226-90 in plasma during a single dose interval. During maximal 8 hours, 11 EDTA blood samples were drawn. In addition to the complete pharmacokinetic curves, blood samples at random time points were drawn at the 6-monthly follow-up visits to the clinic for the determination of the plasma concentrations of rivastigmine and NAP226-90. The time of dose and sampling were recorded. After isolation of plasma by centrifugation, the samples were stored at –20 °C until analysis. The concentrations of rivastigmine and NAP226-90 were simultaneously quantified by a validated method, using high-performance liquid chromatography coupled with tandem mass spectrometry16. Briefly, sample pre-treatment consisted of protein precipitation with

Chapter 3.2.4
114
methanol using 100 µl plasma. Chromatographic separation was performed on a 150x2.0 mm ID Gemini C18 column using a gradient system with 10 mM ammoniumhydroxide and methanol. Accuracies were within ± 14.3% for rivastigmine and NAP226-90. The inter-assay precision was less than 14.7% for both compounds. The intra-assay precision was less than 15.4% for rivastigmine and less than 14.0% for NAP226-90 at the lower limit of quantification level. The intra-assay precision of quality control samples at other concentration levels was less than 14.9% for both compounds. The validated concentration ranges were 0.00025 to 0.050 mg/L for rivastigmine and 0.00050 to 0.025 mg/L for NAP226-90. Pharmacokinetic analysis The nonlinear mixed effect modelling program (NONMEM) Version V (double precision, level 1.1, GloboMax LLC, Hanover MD, USA)17 was used to perform the analysis. The first-order estimation procedure (FO) was used throughout in combination with logarithmic transformation of the data. The adequacy of the tested models was evaluated using statistical and graphical methods. The minimal value of the objective function (OFV, equal to minus twice the log likelihood) provided by NONMEM was used as a goodness of fit characteristic to discriminate between hierarchical models using the log likelihood ratio test17. Standard errors for all parameters were calculated with the COVARIANCE option in NONMEM, individual Bayesian pharmacokinetic parameters were obtained using the POSTHOC option17. The program PDx-POP (version 1.1, release 4, Globomax LLC, Hanover MD, USA) was used as a tool for expediting population pharmacokinetic analysis with NONMEM and for graphical model diagnostics. Basic pharmacokinetic model For rivastigmine absorption, both first-order absorption models with and without absorption lag-time were tested. Also a chain of transition compartments was tested to describe the absorption process, as earlier investigated for the antiretroviral drug efavirenz18. To describe the distribution kinetics of rivastigmine and NAP 226-90, single and multiple compartment models with linear and non-linear elimination were investigated. Interindividual variability in the pharmacokinetic parameters and in the relative bioavailability were estimated from an exponential model19. For instance, variability in clearance was determined from the equation Cl/Fi= θ1*exp(ηi) in which CL/Fi represents the clearance of the ith individual, θ1 is the typical value of apparent clearance, ηi is the interindividual random effect with a mean of 0 and variance ω2. Residual variability was modelled with a combined additive and proportional error model.20 Larger residual variability was likely to be associated with samples collected closer to the time of intake for instance because of irregular absorption. A residual error model

Population pharmacokinetics and pharmacodynamics of rivastigmine
115
accounting for this increased variability was used and is represented by Ci=Ĉi+ θip x εi in which Ci and Ĉi are, respectively, the measured and model predicted drug concentration of the ith individual, εi is the residual random error with mean 0 and variance σ2 and θip is an increment proportion (ip) whose value is to be estimated but fixed to 1 for time points exceeding 2h after intake. Covariate pharmacokinetic model To identify possible relationships between the pharmacokinetics of rivastigmine or NAP 226-90 and patient characteristics, the following co-variates were collected: age (years), gender and body weight (in kg). A covariate was included in an intermediate model when the inclusion of this covariate was statistically significant. A covariate was considered statistically significant when the inclusion was associated with a decrease in minimal value of the OFV of 3.84 points associated with a p-value of <0.05 (log-likelihood ratio test, chi-square distribution, degrees of freedom (df)=1). Finally, a backward elimination procedure was carried out. A parameter was only retained in the model when the influence of this parameter was statistically significant (log likelihood ratio test: p≤0.01, corresponding to an increase in OFV of 6.63 points). Model evaluation The model was evaluated using the jackknife method that investigates the influence of a individual patient on the population model21. A number of new datasets were made by deleting subsequently data of one patient from the primary dataset. Pharmacokinetic parameters were estimated according to the final pharmacokinetic model in each of the new datasets. The median and range were tabulated for all pharmacokinetic parameters and compared with the parameters as obtained during model building with the original full dataset. Pharmacokinetic-Pharmacodynamic analysis Individual pharmacokinetic parameters Individual values for the area under the plasma concentration versus time curve during 12 hours (AUC12) for both rivastigmine and NAP226-90 were calculated as a measure of exposure. Bayesian analysis was used to estimate maximal plasma concentrations (Cmax) and AUC12 of rivastigmine and NAP226-90.

Chapter 3.2.4
116
Efficacy Measurements At baseline and at 6-months intervals rivastigmine use was evaluated by assessment of three domains. Cognition was measured with MMSE22 and Cambridge Cognitive Examination (CAMCOG)23. CAMCOG consists of 60 items covering orientation, language, memory, praxis and calculation/attention, abstract reasoning and perception. Total sum scores range from 0-107. CAMCOG can be subdivided into a memory (maximum score 37) and a non-memory (maximum score 70) section24. Functional disability was measured with the performance subscale of the Interview for Deterioration in Daily living activities in Dementia (IDDD), a caregiver based paper-and-pencil questionnaire, which consists of 11 items with sum scores ranging from 0 to 4425. Behaviour was measured with the Revised Memory and Behavioural Problems Checklist (RMBPC). It is also a caregiver based paper-and-pencil questionnaire and consists of three subsections. First, a 7-item memory subscale (score per item 0-4, maximum score 28,) that includes forgetting recent events, repeated questions, losing things, forgetting the day, forgetting past events, reduced concentration and not finishing tasks. Second, an 8-item disruptive behaviour subscale (score per item 0-4, maximum score 32) including verbal aggression, threats to hurt others, destroying property, to behave dangerous to self or others, talking loudly and rapidly, embarrassing behaviour, arguing and waking caregiver up. Third, a 9-item depression subscale (score per item 0-4, maximum score 36) includes comments about hopelessness, comments about being a burden, appearing sad or depressed, comments about dead, comments about being a failure, crying, comments about loneliness, appearing anxious and suicidal threats26. Lower scores on MMSE and CAMCOG and higher scores on the IDDD and subscales of the RMBPC reflect a worse functioning. Statistics Alzheimer’s disease patients were included in the pharmacokinetic-pharmacodynamic analysis. Patients were divided into responders and non-responders as measured on the different domains: memory related cognition, non-memory related cognition, performance in daily living activities, memory related behaviour, disruptive behaviour and depressive behaviour. For all these test results a median increase or decrease between current test results and the test results at the previous 6-monthly visit was calculated for the total population. Patients were regarded responders if their differences in test results measured on the CAMCOG were equal or larger compared to the median of the population. Patients were also regarded as responders if their differences in test results as measured on the IDDD and subscales of the RMBPC were equal or lower than the median of the population. Mann-Whitney-U testing or Chi-square testing was performed to investigate whether patient characteristics between responders and non-responders were significantly different. As a measure of exposure to rivastigmine and NAP226-90 the maximal plasma

Population pharmacokinetics and pharmacodynamics of rivastigmine
117
concentration (Cmax) and area under the plasma concentration versus time curve (AUC12) were compared between responders and non-responders by Mann-Whitney-U testing. Statistical calculations were performed with SPSS for Windows, version 11.0 (SPSS Inc., Chicago, IL, USA)
Results Patients A total of 33 patients were included with a mean age of 78.4 years, a mean MMSE score of 21.5, the median education level was 4 (on a seven-point scale, ranging from less than 6 years of elementary school (score 1) to a university degree (score 7))27 and they used a mean daily rivastigmine dose of 9.6 mg in different bid dosing regimens (table 1). From these 33 patients, 13 pharmacokinetic curves and 43 plasma concentrations at single time points were available, resulting in a database of 163 rivastigmine and 163 NAP226-90 concentrations. Plasma concentrations of rivastigmine and NAP226-90 are shown in figures 1A and 1B. The concentrations varied between 0.000833 and 0.148 mg/L for rivastigmine and between 0.000544 and 0.0115 mg/L for NAP226-90. Table 1. Baseline characteristics of rivastigmine users. Baseline characteristic Rivastigmine users (n=33) Age (years), mean ± SD (range) 78.4 ± 4.8 (71-94) Gender Male / Female (%) 12/ 21 (36 / 64) Education median, IQR (range) 4, IQR: 2 (2-6) MMSE, mean ± SD (range) 21.5 ± 3.9 (14-29) Weight (kg), mean ± SD (range) 72.4 ± 13.1 (51-110) Clinical Diagnosis Alzheimer’s Disease / Lewy Body Dementia (%)
30 / 3 (91 / 9)
Maximum Achieved Dose, n (%) 3 mg bid 5 (15) 3 mg qd and 4.5 mg qd 6 (18) 4.5 mg bid 5 (15) 4.5 mg qd and 6 mg qd 5 (15) 6 mg bid 12 (37) IQR = interquartile range, MMSE = Mini Mental State Examination
Population pharmacokinetics Both rivastigmine and NAP226-90 data were best described by one-compartment models. The absorption process of rivastigmine was best described by first-order absorption.
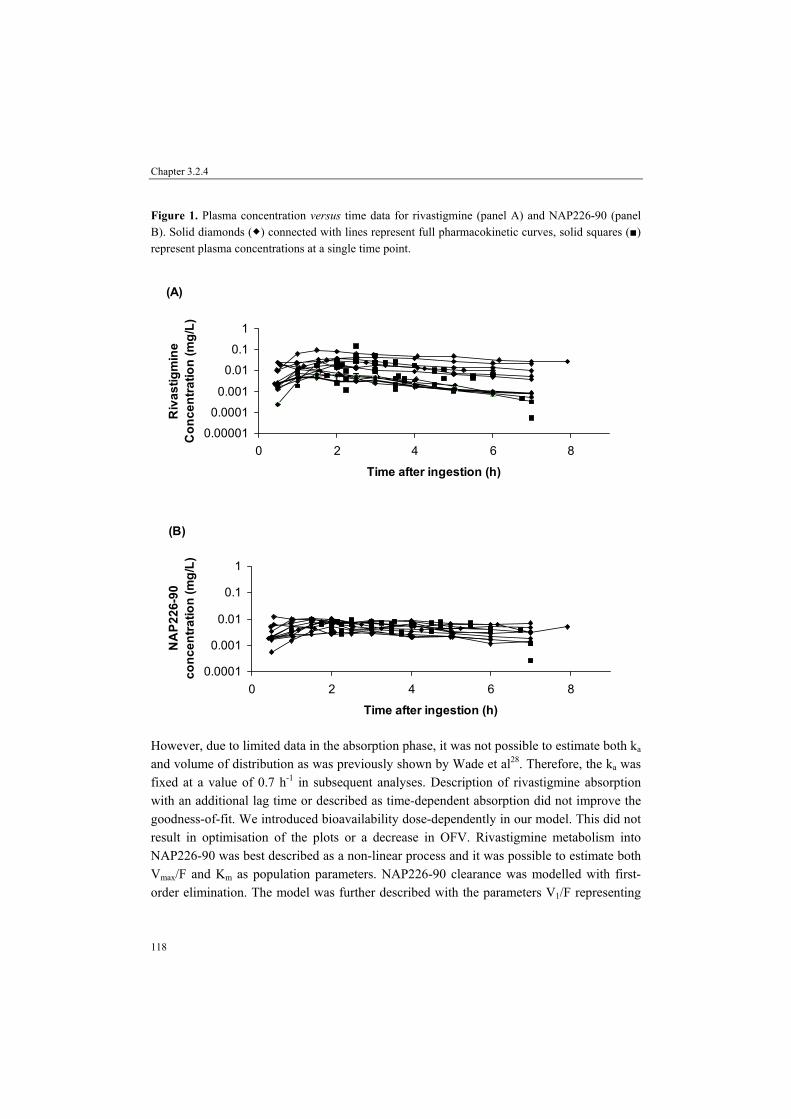
Chapter 3.2.4
118
Figure 1. Plasma concentration versus time data for rivastigmine (panel A) and NAP226-90 (panel B). Solid diamonds ( ) connected with lines represent full pharmacokinetic curves, solid squares (■) represent plasma concentrations at a single time point.
(A)
0.00001
0.0001
0.001
0.01
0.1
1
0 2 4 6 8
Time after ingestion (h)
Riv
astig
min
e C
once
ntra
tion
(mg/
L)
(B)
0.0001
0.001
0.01
0.1
1
0 2 4 6 8
Time after ingestion (h)
NA
P226
-90
conc
entra
tion
(mg/
L)
However, due to limited data in the absorption phase, it was not possible to estimate both ka and volume of distribution as was previously shown by Wade et al28. Therefore, the ka was fixed at a value of 0.7 h-1 in subsequent analyses. Description of rivastigmine absorption with an additional lag time or described as time-dependent absorption did not improve the goodness-of-fit. We introduced bioavailability dose-dependently in our model. This did not result in optimisation of the plots or a decrease in OFV. Rivastigmine metabolism into NAP226-90 was best described as a non-linear process and it was possible to estimate both Vmax/F and Km as population parameters. NAP226-90 clearance was modelled with first-order elimination. The model was further described with the parameters V1/F representing

Population pharmacokinetics and pharmacodynamics of rivastigmine
119
he apparent volume of distribution of rivastigmine and V2/F/fm representing the apparent volume of distribution of NAP226-90 divided by the fraction of rivastigmine metabolised to NAP226-90 (fm). The apparent maximum elimination rate (Vmax/F) of rivastigmine, the oral clearance (CL/F/fm) of NAP226-90 and volumes of distribution of both rivastigmine and NAP226-90 were allometrically scaled for bodyweight as follows29: Vmax/Fi=θ1*(weight/70)0.7, CL/F/fm,i=θ2*(weight/70)0.7, V1/Fi=θ3*(weight/70)1, V2/F/fm,i=θ4*(weight/70)1
In which Vmax/Fi, CL/F/fm,i, V1/Fi and V2/F/fm,i represent Vmax/F, Cl/F/fm, V1/F and V2/F/fm of the ith individual, θ1 is the typical value of Vmax/F, θ2 is the typical value of CL/F/fm, θ3 the typical value of V1/F and θ4 is the typical value of V2/F/fm. With this code, the estimated values of Vmax/F, CL/F/fm. V1/F and V2/F/fm represent the value for patients weighing 70 kg. The introduction of an increment proportion (θip) in the error model resulted in an increase in goodness-of-fit (OFV decrease of 39.8 points). Interindividual variability could be estimated in V1/F, V2/F/fm, Km, Vmax/F and F, although all these estimations showed high relative standard errors. Both an additive and proportional error component could be estimated20. The results of the basic pharmacokinetic model are summarised in table 2. The different covariates were introduced separately in the basic model for Vmax/F, Km and CL2/F/fm. Only gender showed a significant relation with Vmax/F by decreasing the OFV with 7.5 points (p<0.01). Females showed a higher maximal elimination rate of rivastigmine compared to males (θGENDER =1.25 (95% confidence interval: 1.04 – 1.46)). The results of the final pharmacokinetic model are summarised in table 2. Figure 2 shows the logarithm of model predicted concentrations (PRED; panel A and C) and the individual model predicted concentrations (IPRED; panel B and D) from the final model versus the observed concentrations of rivastigmine (DV; panel A and B) and NAP226-90 (DV; panel C and D). The following equation describes the final model for Vmax/F: Vmax/F = 1.0 * 1.25GENDER * (weight/70)0.7 where GENDER is 0 for males and 1 for females.
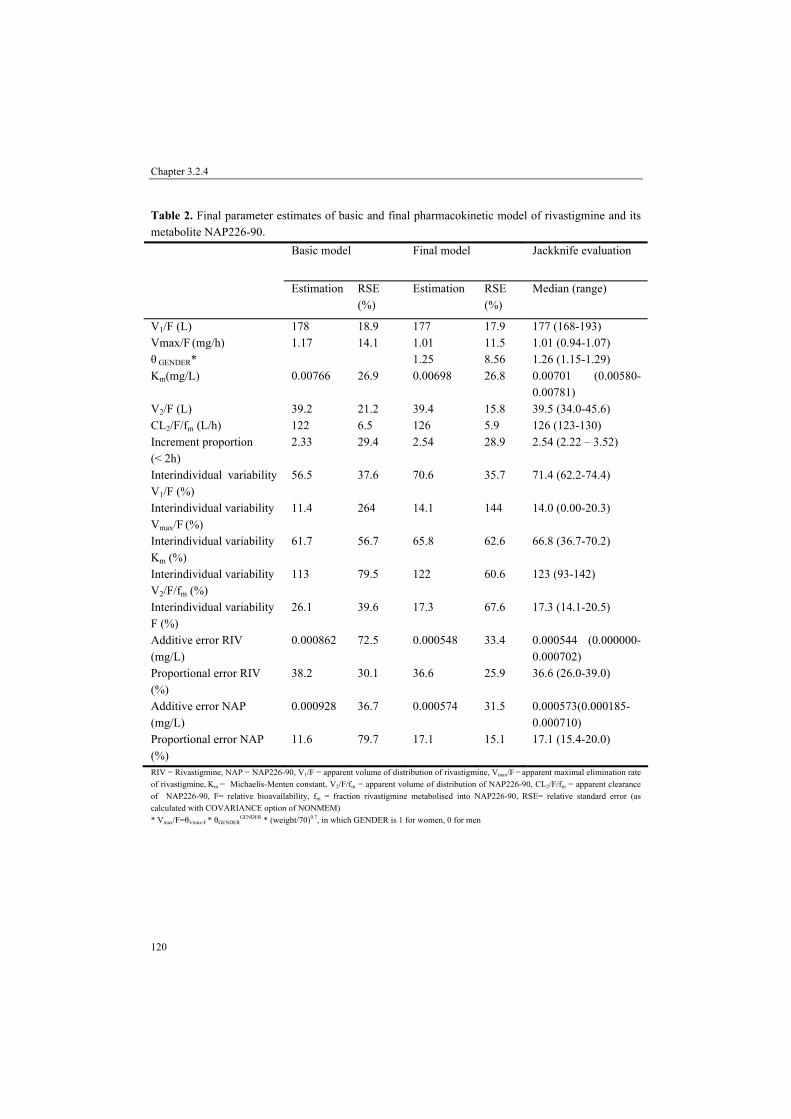
Chapter 3.2.4
120
Table 2. Final parameter estimates of basic and final pharmacokinetic model of rivastigmine and its metabolite NAP226-90.
Basic model Final model
Jackknife evaluation
Estimation RSE (%)
Estimation RSE (%)
Median (range)
V1/F (L) 178 18.9 177 17.9 177 (168-193) Vmax/F (mg/h) 1.17 14.1 1.01 11.5 1.01 (0.94-1.07) θ GENDER* 1.25 8.56 1.26 (1.15-1.29) Km(mg/L) 0.00766 26.9 0.00698 26.8 0.00701 (0.00580-
0.00781) V2/F (L) 39.2 21.2 39.4 15.8 39.5 (34.0-45.6) CL2/F/fm (L/h) 122 6.5 126 5.9 126 (123-130) Increment proportion (< 2h)
2.33 29.4 2.54 28.9 2.54 (2.22 – 3.52)
Interindividual variability V1/F (%)
56.5 37.6 70.6 35.7 71.4 (62.2-74.4)
Interindividual variability Vmax/F (%)
11.4 264 14.1 144 14.0 (0.00-20.3)
Interindividual variability Km (%)
61.7 56.7 65.8 62.6 66.8 (36.7-70.2)
Interindividual variability V2/F/fm (%)
113 79.5 122 60.6 123 (93-142)
Interindividual variability F (%)
26.1 39.6 17.3 67.6 17.3 (14.1-20.5)
Additive error RIV (mg/L)
0.000862 72.5 0.000548 33.4 0.000544 (0.000000-0.000702)
Proportional error RIV (%)
38.2 30.1 36.6 25.9 36.6 (26.0-39.0)
Additive error NAP (mg/L)
0.000928 36.7 0.000574 31.5 0.000573(0.000185-0.000710)
Proportional error NAP (%)
11.6 79.7 17.1 15.1 17.1 (15.4-20.0)
RIV = Rivastigmine, NAP = NAP226-90, V1/F = apparent volume of distribution of rivastigmine, Vmax/F = apparent maximal elimination rate of rivastigmine, Km = Michaelis-Menten constant, V2/F/fm = apparent volume of distribution of NAP226-90, CL2/F/fm = apparent clearance of NAP226-90, F= relative bioavailability, fm = fraction rivastigmine metabolised into NAP226-90, RSE= relative standard error (as calculated with COVARIANCE option of NONMEM) * Vmax/F=θVmax/F * θGENDER
GENDER * (weight/70)0.7, in which GENDER is 1 for women, 0 for men
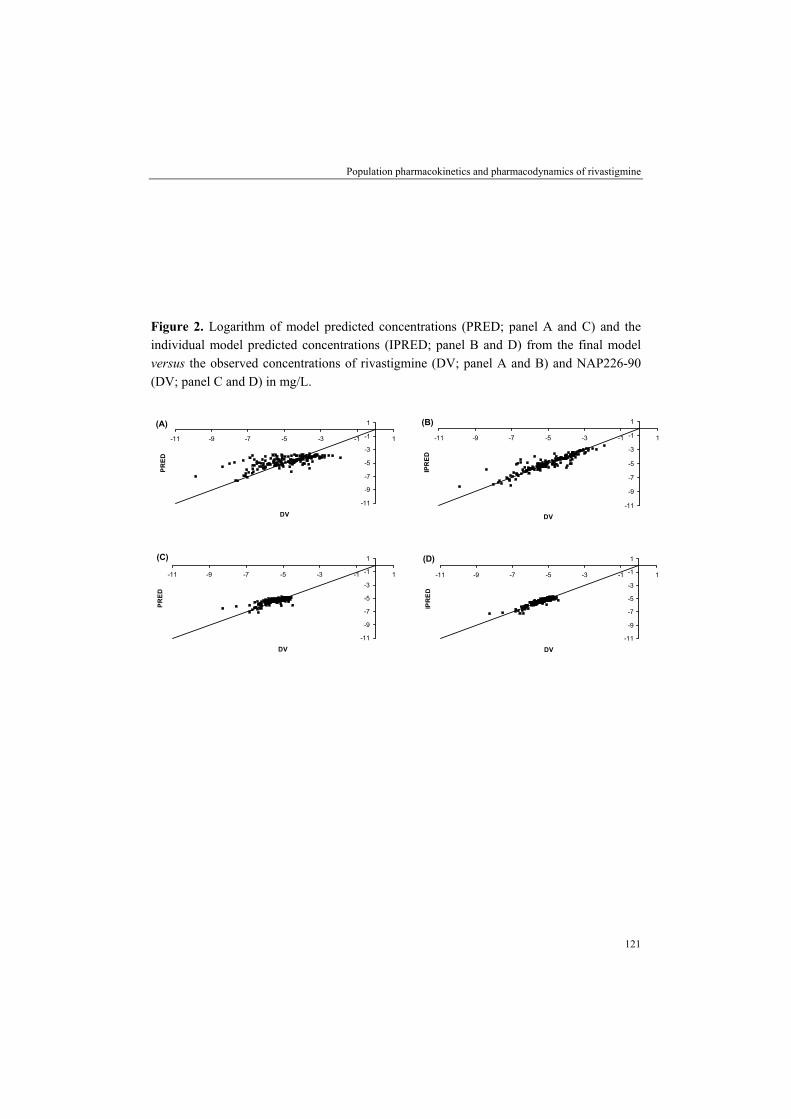
Population pharmacokinetics and pharmacodynamics of rivastigmine
121
Figure 2. Logarithm of model predicted concentrations (PRED; panel A and C) and the individual model predicted concentrations (IPRED; panel B and D) from the final model versus the observed concentrations of rivastigmine (DV; panel A and B) and NAP226-90 (DV; panel C and D) in mg/L.
(A)
-11
-9
-7
-5
-3
-1
1
-11 -9 -7 -5 -3 -1 1
DV
PR
ED
(B)
-11
-9
-7
-5
-3
-1
1
-11 -9 -7 -5 -3 -1 1
DV
IPR
ED
(C)
-11
-9
-7
-5
-3
-1
1
-11 -9 -7 -5 -3 -1 1
DV
PR
ED
(D)
-11
-9
-7
-5
-3
-1
1
-11 -9 -7 -5 -3 -1 1
DV
IPR
ED

Chapter 3.2.4
122
Pharmacokinetic-Pharmacodynamic correlations From the 33 included patients in the study, 6-monthly test results of 30 AD patients could be used in the pharmacokinetic-pharmacodynamic analysis. The results of these analyses for the different tests are summarised in table 3. No significant differences were shown between responders and non-responders on the different tests for the pharmacokinetic parameters. Table 3. Results of the pharmacokinetic-pharmacodynamic analysis. CAMCOGmem CAMCOGnonmem R (n=17) NR (n=13) p-value* R (n=13) NR (n=17) p-value* Age (years) 78.5 79.8 0.786 77.4 79.8 0.391 Gender, % male 29.4 30.8 1.000 38.5 23.5 0.443 Education 4 4 0.881 4 4 0.864 Baseline 18 19 0.283 54 56 0.600 Riva Cmax (mg/L) 0.00926 0.0112 0.917 0.00866 0.0140 0.346 Riva AUC12 (mg*h/L) 0.0439 0.0556 0.917 0.0395 0.0698 0.439 NAP Cmax (mg/L) 0.00618 0.00502 0.917 0.00519 0.00618 0.722 NAP AUC12 (mg*h/L) 0.0396 0.0352 0.346 0.0352 0.0396 0.884 IDDD RMBPCmem R (n=13) NR (n=13) p-value* R (N=18) NR (=10) p-value* Age (years) 79.8 76.9 0.427 79.0 79.9 0.962 Gender, % male 30.8 23.1 1.000 27.8 40.0 0.677 Education 3 4 0.527 4 4 0.571 Baseline 14 11 0.511 17 15.5 0.323 Riva Cmax (mg/L) 0.0103 0.00926 0.817 0.00953 0.0168 0.270 Riva AUC12 (mg*h/L) 0.0400 0.0439 0.701 0.0397 0.0808 0.164 NAP Cmax (mg/L) 0.00660 0.00490 0.397 0.00566 0.00618 0.145 NAP AUC12 (mg*h/L) 0.0396 0.0265 0.369 0.0317 0.0436 0.057 RMBPCdis RMBPCdep R (n=13) NR (n=16) p-value* R (n=22) NR (n=6) p-value* Age (years) 78.5 79.7 0.759 79.1 77.3 0.314 Gender, % male 15.4 43.8 0.130 31.8 33.3 1.000 Education 4 4 0.892 4 4.5 0.372 Baseline 5 1 0.009 4.5 3 0.612 Riva Cmax (mg/L) 0.00866 0.0105 0.599 0.0100 0.00665 0.145 Riva AUC12 (mg*h/L) 0.0395 0.0570 0.430 0.0497 0.0256 0.117 NAP Cmax (mg/L) 0.00638 0.00535 0.456 0.00628 0.00484 0.145 NAP AUC12 (mg*h/L) 0.0352 0.0351 0.693 0.0374 0.0239 0.057 R=responder , NR=nonresponder, CAMCOGmem= memory subsection of camcog cognitive screening, CAMCOGnonmem= non-memory subsection of camcog cognitive screening, IDDD= performance in daily living activities in dementia, RMBPCdis= disruptive subscale of the RMBPC, RMBPCmem= memory subscale of the RMBPC, RMBPCdep= depressive subscale of RMBPC, Riva Cmax= rivastigmine maximal plasma concentration, Riva AUC12= Area under the plasma concentration time curve (0-12 h) of rivastigmine, NAP Cmax= NAP226-90 maximal plasma concentration, NAP AUC12= Area under the plasma concentration time curve (0-12h) of NAP226-90, *based upon Mann-Whitney-U testing or Chi-square statistics when appropriate

Population pharmacokinetics and pharmacodynamics of rivastigmine
123
Discussion Observed plasma concentrations of rivastigmine and its metabolite NAP226-90 in our relatively unselected outpatient population were in the same range as earlier described in rivastigmine controlled clinical trials in Alzheimer patients12,30. Pronounced non-linear elimination of rivastigmine was found in our study, which in agreement with Hossain et al.30 but not with the study of Gobburu et al.12. Final parameter estimates for V1/F and Vmax/F were comparable to those estimated by Hossain et al.30 in 11 AD patients (mean age 69.5 years). The typical values of Km and volumes of distribution of rivastigmine and NAP226-90 were lower compared to those earlier described studies12,30. We showed a non-linear elimination of rivastigmine in the treated outpatients with a value for Km of 0.00698 mg/L. The concentrations that we measured in our study are in a wide range around this value and indicate that there is variability in rivastigmine elimination between individuals. Concentrations of rivastigmine increase thus non-lineary with higher doses. Our results indicate that increasing doses may lead to disproportional increases in exposure of rivastigmine. Higher doses of rivastigmine are often not tolerated by patients because of gastrointestinal adverse events31. It is known that daily doses above twice daily 3 mg are required for optimal efficacy1,2, but it is questionable if it should be intended to increase rivastigmine dose up to twice daily 6 mg in all patients, because that may result in disproportionally higher rivastigmine concentrations and an increased risk of adverse events. Interindividual variability for both rivastigmine and NAP226-90 pharmacokinetics were large in our population. For example the interindividual variability of V/F for rivastigmine was 70.6%. Goburru et al.12 did not show any correlation between pharmacokinetic parameters with age, gender or body weight. The maximal elimination rate of rivastigmine was, however, significantly increased in females in our study, which results in a lower exposure to rivastigmine in females. The basal acetylcholinesterase activity is significantly larger in females compared to men12. Because rivastigmine is metabolised by acetylcholinesterase into NAP226-90 this possibly explains why females showed an increased maximal rate of rivastigmine elimination. In clinical practice often only the MMSE is used to evaluate effect of rivastigmine therapy. We measured the effects of rivastigmine in clinical practice extensively in the domains cognition (CAMCOG), activities of daily living (IDDD) and behaviour (RMBPC). No relation between both rivastigmine and NAP226-90 exposure and effect parameters in the different domains was found in this population of outpatients treated with rivastigmine for minimal 6 months. An earlier study in rats indicated that the concentration NAP226-90 was probably a better predictor of cholinesterase inhibition than rivastigmine itself10. Our results in the pharmacokinetic-pharmacodynamic analysis, however, do not reveal differences in the relation between exposure to rivastigmine or NAP226-90 and effectiveness.

Chapter 3.2.4
124
Rivastigmine inhibits both acetylcholinesterase and butyrylcholinesterase. Plasma butyrylcholinesterase activity has not been related to cognitive screening results while cerebrospinal fluid butyrylcholinesterase activity was related32. Therefore, it can be questioned whether inhibition of plasma cholinesterase and the concentration of NAP226-90 are useful as surrogate markers for brain cholinesterase inhibition and therapy effectiveness. Rivastigmine treatment effects on cognition, activities of daily living and behaviour show large variability between individual patients treated in a outpatient setting33. This variability in treatment effects was also found in patients included in the currently described pharmacokinetic-pharmacodynamic analysis. It is largely unknown which patients respond to cholinesterase-inhibitor treatment. Unfortunately, we did not found a relation between rivastigmine pharmacokinetics and treatment effects. This may be explained because the period of enzyme inhibition is substantially longer compared to the appearance of rivastigmine in plasma7. Therefore, differences in enzyme inhibition between individuals may be better predictors of therapy effects compared to pharmacokinetic variables. However, plasma cholinesterase activity may not be useful at all as a surrogate marker as described above. Clinical or neurophysiologic parameters may better predict therapy efficacy than differences in pharmacokinetics between individuals. We have shown that patients with more severe AD, as defined by a MMSE score ≤ 19, responded better to rivastigmine therapy compared to AD patients with a baseline MMSE score ≥ 20 in a study performed in patients treated via our geriatric outpatient department34. Adler et al.35 have shown that treatment responders had a greater decrease in theta power as measured with a electro encephalogram (EEG). In conclusion, we developed a population pharmacokinetic model that simultaneously described rivastigmine and its metabolite NAP226-90 plasma pharmacokinetics. This study is the first to describe a pharmacokinetic model in geriatric outpatients suffering from Alzheimer’s disease or Lewy body dementia and treated for minimal 6 months. We found no relation between plasma pharmacokinetics of both rivastigmine and NAP226-90 and therapy effectiveness of rivastigmine as measured on cognition, activities of daily living and behaviour, which indicates that other factors may be more important in the observed variability in treatment response.
Acknowledgements Edith Vermaat is kindly acknowledged for her help in including patients when they attended the geriatric outpatient department for 6-monthly cognitive screening visits.
Population pharmacokinetics and pharmacodynamics of rivastigmine
125
References 1. Corey-Bloom J, Anand R, Veach J. A randomized trial evaluating the efficacy and safety of ENA 713
(rivastigmine tartrate), a new acetylcholinesterase inhibitor, in patients with mild to moderately severe Alzheimer’s disease. Int J Geriatr Psychopharmacol 1998; 1:55-65.
2. Rösler M, Anand R, Cicin-Sain A, et al. Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: international randomized controlled trial. BMJ 1999;318:633-638.
3. McKeith IG, Del Ser T, Spano P, et al. Efficacy of rivastigmine in dementia with Lewy Bodies: a randomised, double-blind, placebo-controlled international study. Lancet 2000;356:2031-36.
4. Wesnes KA, McKeith IG, Ferrar R, et al. Effects of rivastigmine on cognitive function in dementia with Lewy Bodies: a randomised placebo-controlled international study using the cognitive drug research computerised assessment system. Dement Geriatr Cogn Disord 2002;13:183-192.
5. Tiraboschi P, Hansen LA, Alford M, Sabbagh MN, Schoos S, Masliah E, et al. Cholinergic dysfunction in diseases with Lewy bodies. Neurology 2000;54:407-11.
6. Wynn ZJ, Cummings JL. Cholinesterase inhibitor therapies and neuropsychiatric manifestations of Alzheimer’s disease. Dement Geriatr Cogn Disord 2004;17:100-108.
7. Jann MW, Shirley KL, Small GW. Clinical pharmacokinetics and pharmacodynamics of cholinesterase inhibitors. Clin Pharmacokinet 2002;41:719-739.
8. Davis KL, Mohs RC, Marin D, et al. Cholinergic markers in elderly patients with early signs of Alzheimer’s disease. JAMA 1999;281:1401-6.
9. Nordberg A, Svensson AL. Cholinesterase inhibitors in the treatment of Alzheimer´s disease: a comparison of tolerability and pharmacology. Drug Saf 1998;19:465-80.
10. Enz A, Chappuis A, Dattler A. A simple, rapid and sensitive method for simultaneous determination of rivastigmine and its major metabolite NAP 226-90 in rat brain and plasma by reversed-phase liquid chromatography to electrospray ionization mass spectrometry. Biomed Chromatogr 2004;18:160-166.
11. Rockwood K, MacKnight C. Assessing the clinical importance of statistically significant improvement in anti-dementia drug trials. Neuroepidemiology 2001;20:51-56.
12. Gobburu JVS, Tammara V, Lesko L, et al. Pharmacokinetic-pharmacodynamic modeling of rivastigmine, a cholinesterase inhibitor, in patients with Alzheimer´s disease. J Clin Pharm 2001;41:1082-1090.
13. Rogers SL, Friedhoff LT. The efficacy and safety of donepezil in patients with Alzheimer´s Disease: results of a US multicentre, randomized, double blind, placebo controlled trial. Dementia 1996;7:293-303.
14. McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA work group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s disease. Neurology 1984;34:939-944.
15. McKeith IG, Tatemichi TK, Erkinjutti T, et al. Consensus guidelines for the clinical and pathological diagnosis of dementia with Lewy Bodies (DLB): report of the consortium on DLB international workshop. Neurology 1996;47:1113-1124.
16. Frankfort SV, Ouwehand M, van Maanen MJ, et al. A simple and sensitive assay for the quantitative analysis of rivastigmine and its metabolite NAP 226-90 in human EDTA plasma using coupled liquid chromatography and tandem mass spectrometry. Rapid Comm Mass Spectr 2006; 20:3330-3336.
17. Beal SL, Sheiner LB. NONMEM User´s guides. NONMEM Project Group, University of California at San Francisco, 1998.
18. Kappelhoff BS, Huitema ADR, Yalvac Z, et al. Population pharmacokinetics of efavirenz in an unselected cohort of HIV-1-infected individuals. Clin Pharmacokinet 2005;44:849-861.
19. Karlsson MO, Sheiner LB. The importance of modelling interoccassion variability in population pharmacokinetic analyses. J Pharmacokinet Biopharm 1993;21:735-750.
20. Beal SL. Ways to fit a PK model with some data below the quantification limit. J Pharmacokinet Pharmacodyn 2001;28:481-504.
Chapter 3.2.4
126
21. Armitage P, Berry G, Matthews JNS. Statistical methods in medical research. Blackwell Publishing: Berlin Germany, 2002.
22. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state” a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189-198.
23. Roth M, Tym E, Mountjoy CQ, et al. CAMDEX A standardized instrument for the diagnosis of mental disorder in the elderly with special reference to early detection of dementia. Br J Psychiatry 1986;149:698-709.
24. Schmand B, Walstra G, Lindeboom J, Teunisse S, Jonker C. Early detection of Alzheimer’s disease using the Cambridge Cognitive Examination (CAMCOG). Psychol Med 2000;30:619-627.
25. Teunisse S, Derix MM. Measuring functional disability in community-dwelling dementia patients: development of a questionnaire (in Dutch). Tijdschr Gerontol Geriatr 1991;22:53-59.
26. Teri L, Truax P, Logsdon R, Uomoto J, Zarit S, Vitaliano PP. Assessment of behavioral problems in dementia: the revised memory and behavior problems checklist. Psychol Aging 1992;7:622-631.
27. Verhage F. Intelligence and Age (in Dutch). Assen, van Gorcum, 1964. 28. Wade JR, Kelman AW, Howie CA, Whiting B. Effect of misspecification of the “absorption process” on
subsequent parameter estimates in population analysis. J Pharmacokinet Biopharm 1993;21:209-222. 29. Hu TM, Hayton WL. Allometric scaling of xenobiotic clearance: uncertainty versus universality. AAPS
PharmSci2001;3:E29. 30. Hossain M, Jhee SS, Shiovitz T, et al. Estimation of the absolute bioavailability of rivastigmine in patients
with mild-to-moderate dementia of the Alzheimer´s type. Clin Pharmacokinet 2002;41:225-234. 31. Gauthier S. Cholinergic adverse effects of cholinesterase inhibitors in Alzheimer’s disease. Drugs Aging
200;118:853-862. 32. Giacobini E, Spiegel R, Enz A, et al. Inhibition of acetyl- and butyrylcholinesterase in the cerebrospinal fluid
of patients with Alzheimer’s disease by rivastigmine: correlation with cognitive benefit. J Neural Transm 2002;109:1053-1065.
33. Frankfort SV, Appels BA, de Boer A, et al. Treatment effects of rivastigmine on cognition, performance of daily living activities and behaviour in Alzheimer’s disease in an outpatient geriatric setting. Int J Clin Pract 2006;60:646-654.
34. Frankfort SV, Appels BA, de Boer A, et al. Identification of responders and reactive domains to rivastigmine in Alzheimer’s disease. Pharmacoepidemiol Drug Saf 2006; in press.
35. Adler G, Brassen S, Chwalek K, et al. Prediction of treatment respons to rivastigmine in Alzheimer’s dementia. J Neurol Neurosurg Psychiatry 2004;75:292-294.