Embed Size (px)
Citation preview

Cirrhosis and Liver TransplantPaul “Skip” H. Hayashi, MD, MPH
Medical Director, Liver TransplantationUniversity of North Carolina, Chapel Hill, NC
Aug 15, 2015

Outline
• Cirrhosis• Cirrhosis assessment• Cirrhosis care:
• Varices: bleed prophylaxis• Ascites care• Cirrhosis “health care maintenance”
• Transplantation• When to refer• Special circumstances
• PPH, HPS• HCC

Do you have cirrhosis?
• Clinical diagnosis• Platelets, albumin, bilirubin, INR• Imaging—usually CT or MRI
• Liver biopsy• Serum Marker Scores• Non-invasive ‘imaging’

Liver biopsy
• Percutaneous or transjugular• Same day procedure• 30% chance of pain• Mild/moderate bleed risk: 1/500• Severe bleed: 1:5000• Death: 1:10,000
Bedossa P, et al. Clin Liv Dis 2015; Rockey D, et al. AASLD Guideline 2009

Serum Marker Scores
Bedossa P, et al. Clin Liv Dis 2015
Performances: ROC’s in the 0.80 range for determining advanced fibrosis/cirrhosis

Non-invasive ‘imaging’ techniques
Fibroscan performance: ROC’s 0.87-0.98 for determining advanced fibrosis/cirrhosis

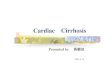
Transient Elastography
• Ultrasound transducer probe• On same axis as narrow vibration source
• Pulse vibration creates elastic shear• Probe reads vibration return or echo
• Stiffness of tissue increases velocity of return.

http://medgadget.com/archives/2007/01/fibroscan.html
http://www.hepcentro.com.br/investigacao_de_doenca_hepatica.htm
Castera L. Hepato-Gastro. 2007
x 6-10 x 1-2
Liver biopsy
Transient Elastography

When to use these tests
• When the underlying diagnosis is clear and cirrhosis, yes/no is all that is needed.
• Staging for hepatitis C therapy• Monitoring patients on methotrexate• Older or frail patient population• Step-wise approach with liver biopsy as a back-up• Deciding on whether cirrhosis care testing is needed.

Cirrhosis: Clinical Severity
• MELD• MELD-Na• Childs-Pugh• Nutritional / functional status

MELD
• INR, total bilirubin, creatinine• Predicts 3 month mortality risk• Developed to predict survival after TIPS• ROC curve ~ 80%
Transplant referral?

MELD-Na: the importance of hyponatremia
• Deranged hemodynamics• Increased plasma renin/angiotensin• SIADH
• Decreased free water clearance• Hyponatremia
“In patients with liver disease, serum Na levels below 130 mEq/L must be regarded as serious and, if below 125, ominous.”
• Dame Sheila Sherlock, 1956

MELD-Na: the importance of hyponatremia
• Predictive of mortality beyond just MELD especially at MELD scores <20-22
• MELD-Na = MELD score + 1.59 (135 – serum Na).
Biggins, S et al. Gastro 2006; Wong VW, et al. Liver Transpl 2007

MELD-Na
Kim, RW, et al. NEJM 2008
MELDMELD-Na

Childs Pugh??
MELD & MELD-Na• INR• Bilirubin• Cr & Na
Childs Pugh• INR• Bilirubin• Ascites / portal hypertension• Hepatic encephalopathy• Albumin—nutritional status.
CTP 1 year 2 yearA (5-6) 100% 85%B (7-9) 80% 60%C (10-15) 45% 35%
Transplant referral?

“HepCalc” Version 2.52Gary Poleynard, MD, FGAF

Jalan R, et al. for the CANIONIC Study Investigators of the EASL-CLIF ConsortiumJ of Hepatology, Nov 2014

Jalan R, et al. for the CANIONIC Study Investigators of the EASL-CLIF ConsortiumJ of Hepatology, Nov 2014

Jalan R, et al. for the CANIONIC Study Investigators of the EASL-CLIF ConsortiumJ of Hepatology, Nov 2014
28-day mortality prediction 90-day mortality prediction

Jalan R, et al. for the CANIONIC Study Investigators of the EASL-CLIF ConsortiumJ of Hepatology, Nov 2014
% improvement using CLIF-C compared to: MELD MELD-Na CP
CLIF-C performed much better than MELD, MELD-Na and CP

Jalan R, et al. for the CANIONIC Study Investigators of the EASL-CLIF ConsortiumJ of Hepatology, Nov 2014

WHO / ECOG Performance Status
Grade Explanation of activity0 Fully active, able to carry on all pre-disease performance without restriction1 Restricted in physically strenuous activity but ambulatory and able to carry out work of a
light or sedentary nature, e.g., light house work, office work2 Ambulatory and capable of all self-care but unable to carry out any work activities. Up and
about >50% of waking hours3 Capable of only limited self-care.
Up and about < 50% of waking hours4 Completely disabled. Cannot carry on any selfcare. Totally confined to bed or chair5 Dead

Surveillance and Primary Variceal Bleed Prophylaxis
No decompensationCP = 5
Decompensation CP = 6
Decompensation (Child B/C)
No varices q 3 yrs q 1 yr q 1 yr
Small (Gr I)
q 2 yrs q 1 yr Beta block
Large (Gr II-III)
Beta block Beta block Beta block
Garcia-Tsao, G, Sanyal, AJ, Grace ND, Carey W. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology, September 2007.

Non-selective Beta Blockade• Agents (dose low and slow)
• Propranolol• Nadolol• Carvedilol
• Target • 25% fall in heart rate or• Highest tolerated dosing to get heart rate in the 60’s
• Stop the beta blocker• Refractory ascites• Spontaneous bacterial peritonitis• Hepatorenal syndrome.
Garcia-Tsao, G, Sanyal, AJ, Grace ND, Carey W. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology, September 2007.
Mandorfer M, et al. Gastroenterology 2014
Serste T, et al. Hepatology 2010.

Ascites Management
• Furosemide• 20-40 mg/d• Max: 160 mg/d
• Spironolactone• 100 mg/d• Max: 400 mg/d
• Large volume paracentesis• Over 3-5 liters give 8 g/L 25% albumin (25g/3 liters taken)• Give it for first 3-5 liters in the setting of renal insufficiency or hyponatremia
Runyon, BA. AALD Guidelines 2012

Ascites Management
• Dietary advice• Low Na diet: <2 g/d• Fluid restriction: 1.8-2.0 L/d free water
• How much fluid to withdraw a LVP: more art than science
• Spontaneous peritoneal peritonitis• Diagnostic tap recommend for any hospitalized cirrhotic with ascites• 1st choice: cefotaxime; 2nd : fluoroquinolone• Albumin must be given (1.5 g/kg day 1; 1.0 g/kg day 3)
Runyon, BA. AALD Guidelines 2012

Cirrhosis Health Care Maintenance
1. EGD: Varices surveillance2. Imaging: HCC surveillance3. Vaccination: hepatitis A/B4. Bone density: osteoporosis
risk5. Transplant: referral?


Abs. 588 (Poster) AASLD Liver Meeting 2014, Boston, MA Delay in Appropriate Antimicrobial Therapy Increases Mortality in Cirrhotics with Spontaneous Bacterial Peritonitis and Septic ShockKarvellas C.J., et al. University of Alberta, King Saul Bin Abdulaziz University, and University of Manitoba
• Retrospective look at cirrhosis with septic shock and SBP from 1996-2011.
• Looked factors that effect survival in multivariate analysis.• 3 center study.

Abs. 588 (Poster) AASLD Liver Meeting 2014, Boston, MA Delay in Appropriate Antimicrobial Therapy Increases Mortality in Cirrhotics with Spontaneous Bacterial Peritonitis and Septic ShockKarvellas C.J., et al. University of Alberta, King Saul Bin Abdulaziz University, and University of Manitoba
Characteristics Survivors (n=23) Non-survivors (n=103) p-value
MELD (mean) 24 34 <0.01
APACHE II (mean) 22 32 <0.01
(+) blood culture 22% 50% 0.02
Appropriate initial antibiotics
100% 75% 0.01
Delay in antibioticsfrom SIRS (Median, hrs)
1.8 9.5 <0.01
Lactate (mean) 4.9 8.9 <0.01
APACHE II: OR 1.45 (1.04-2.02)
Lactate:OR 2.34 (1.04-5.29)
Delay in antibiotics:

Abs. 588 (Poster) AASLD Liver Meeting 2014, Boston, MA Delay in Appropriate Antimicrobial Therapy Increases Mortality in Cirrhotics with Spontaneous Bacterial Peritonitis and Septic ShockKarvellas C.J., et al. University of Alberta, King Saul Bin Abdulaziz University, and University of Manitoba

When to refer for transplantation
• MELD >/= 10-12• Child-Turcotte-Pugh >/= 7
• Child’s B
• Index decompensatory event• Encephalopathy• Variceal bleed• Ascites
• Other

Exceptional cases: Referrals when MELD may be low
• Hepatocellular carcinoma• Two lung associated disorders
• Hepatopulmonary syndrome• Portopulmonary hypertension

Hepatocellular Carcinoma• Milan criteria or “5-3-3” rule or TMN </=T2
• One tumor < 5 cm or…• Up to 3 tumors, but…• All < 3 cm.
Stage ScoreT1(one lesion < 2cm)
No upgrade
T2(over T1 but less than “5,3,3” Milan criteria)
22*
*Score increased every 90 days to reflect 10% increase in drop-out.

Hepatopulmonary Syndrome
• Hypoxia due to intra-pulmonary shunting
• Screening• Pulse oximetry—
• Diagnosis• Doppler echocardiogram with
bubble study• RA ABG• Rule out other causes for hypoxia
Rodriguez-Roisin R, Krowka MJ. NEJM 2008

Hepatopulmonary syndromeAllocation of exception points for hepatopulmonary syndrome.
American Association for the Study of Liver Diseases
PaO2 < 60 mm Hg---22 MELD points
10% mortality upgrade every 90 Days

Portopulmonary Syndrome
Diagnostic Criteria:MPAP > 35 mm HgPVR > 240 dynes/sec/cm(-5)Transpulmonary gradient > 12 mm Hg
Qualification for MELD of 22:FDA approved therapy results in the following:
MPAP < 35 mm Hg and PVR < 400 dynes/sec/cm-5Satisfactory right ventricular function exists (center-specific testing).

Liver-Lung Disorders: Bottom line
• If cirrhotic patient complains of shortness of breath, consider…• Pulse oximetry• Echocardiogram with Doppler and bubble study.

A few last notes “from the trenches”…
• No NSAIDs in cirrhotics• How to give lactulose• We don’t biopsy for HCC lesions much anymore.

Thanks for listening…