Embed Size (px)
Citation preview

ANTIPHOSPHOLIPID SYNDROME (D ERKAN, SECTION EDITOR)
Clinical Relevance of β2-Glycoprotein-I Plasma Levelsin Antiphospholipid Syndrome (APS)
Alessandra Banzato & Vittorio Pengo
Published online: 6 May 2014# Springer Science+Business Media New York 2014
Abstract Antiphospholipid syndrome (APS) is characterizedby the presence of antiphospholipid (aPL) antibodies associat-ed with thrombosis or pregnancy morbidity. The antibodiesmainly involved in this disorder are directed againstβ2-glycoprotein I (β2-GPI). β2-GPI plasma level is usuallynot reported in studies on APS, because it is not regarded asrelevant to the diagnosis and prognosis of APS. Neverthelessits measurement may be important for understanding the path-ophysiology of the syndrome. This review summarizes avail-able data from the literature on plasma concentrations ofβ2-GPI in patients with different antibody profiles.
Keywords Beta-2-glycoprotein I . Antiphospholipidsyndrome . Plasma levels . APS . Antiphospholipidantibodies . Thrombosis
Introduction
Beta-2 glycoprotein I (β2-GPI), an apolipoprotein with anapproximate molecular weight of 50 kD, is the main factorimplicated in the pathophysiology of antiphospholipid syn-drome (APS). Discovered more than 50 years ago [1–3] itconsists of five short consensus repeats, also called sushidomains [4]. The crystal structure of this protein was firstreported in 1999 by two independent groups [5, 6]; it has aJ-shaped conformation, with a vertical ascending part calleddomain I and a positive area in the bottom part of the moleculecalled domain V. Domains I, II, III, and IVare each composed
of approximately 60 amino acids whereas domain V differsfrom the other four domains and consists of 82 amino acidsincluding a C-terminal, hydrophilic, positively charged patchenabling β2-GPI to bind to anionic surfaces, for example asactivated blood cells [6].
The physiological function of β2-GPI is not clear. It isbelieved to be involved in regulation of FXI and in plasmin-ogen activation [7, 8]. It contributes to triglyceride clearance[9] and regulates uptake and proteolytic degradation of oxi-dized low-density lipoprotein by scavenger cells [10]. Itsprocoagulant activity is attributed to reduction of protein C-related activity, thus inhibiting the phospholipid-dependentcoagulation pathway [11]. In APS patients, another antibodyis believed to be involved in protein C activity: anti-cardiolipin antibodies (aCLs) [12, 13].
Recently our group demonstrated an important interactionbetween β2-GPI and thrombin [14]. β2-GPI has unique anti-coagulant properties and selectively inhibits the procoagulantfunctions of thrombin without altering its anticoagulant activ-ity. These findings shed light on a novel physiological antico-agulant function of this protein.
For many years, attention has been focused on anti-β2-GPIantibodies rather than on the β2-GPI itself. However, there isgrowing interest in understanding the physiological effect ofβ2-GPI and determining its plasma levels.
Historical Perspective
In 1993, Vlachoyiannopoulos et al. [15] studied the corre-lation between anti-phosphatidylethanolamine (PE) anti-bodies, aCLs, and β2-GPI plasma levels in patients withAPS and systemic lupus erythematosus (SLE). They foundthat APS patients had higher β2-GPI levels than SLE pa-tients and its concentration was associated with aCL andanti-phosphatidylethanolamine (aPE) activity.
This article is part of the Topical Collection on Antiphospholipid Syndrome
A. Banzato (*) :V. PengoDepartment of Cardiac Thoracic and Vascular Sciences, Universityof Padova, Via Giustiniani, 2, 35128 Padova, Italye-mail: [email protected]
Curr Rheumatol Rep (2014) 16:424DOI 10.1007/s11926-014-0424-9

In 1995, McNally et al. [16] measured plasma levels of β2-GPI antigen and β2-GPI binding antibodies in patients withSLE and primary APS (PAPS). They found both were in-creased in patients with PAPS and a history of thromboem-bolic complications or recurrent fetal loss. In their work, theymeasured β2-GPI antigen (β2-GPI:Ag), β2-GPI aPL cofactoractivity (β2-GPI:Cof), and antibodies to β2-GPI (alpha β2-GPI) in SLE patients with aPL antibodies (SLE-aPL+) and inpatients with primary APS (PAPS). β2-GPI:Ag levels weresignificantly increased in SLE-aPL + patients and PAPS pa-tients compared with SLE-aPL − patients and normal healthycontrols. The β2-GPI:Cof/Ag ratio was significantly reducedin SLE-aPL + patients compared with SLE-aPL − patients,indicating functional modification of β2-GPI in SLE-aPL +patients. These results suggested involvement of β2-GPI inthe pathogenic mechanism of thrombosis associated withaPLs.
The same group [17] investigated levels of β2-GPI inAPS patients. Although the total β2-GPI levels of the SLE-aPL + patients were significantly increased compared withSLE-aPL − patients and normal controls, no significantdifferences between free β2-GPI levels were observed be-tween these groups. These results suggested that levels ofcomplexed β2-GPI were increased in patients with aPL,perhaps as a result of immune complex formation, or al-tered binding to other plasma constituents.
In 1998, Balasubramanian et al. [18] measured plasma β2-GPI levels, by use of a novel competitive ELISA assay, todetermine the concentration of free β2-GPI and the fraction ofantibody-bound β2-GPI. In this way, quantification of totalantigen in individuals with autoimmune antibodies could beeasily achieved. When plasma samples from normal individ-uals (free from blocking antibodies) were assessed with bothcompetitive and standard ELISA the results did not differ.However, in plasma samples from APS patients, β2-GPIlevels were significantly lower, indicating that a substantialfraction of the plasma β2-GPI was bound by antibody.
Mehdi et al. [19], in 1999, reported a correlation between agenetic variation in the apolipoprotein H gene (APOH, gene)and plasma concentrations of β2-GPI (apoH, protein). APOHis polymorphic, with three common alleles (APOH*1,APOH*2, and APOH*3). The APOH*2 allele is the mostfrequent in all populations. The authors sought to determinethe effect of APOH polymorphism on apoH levels innormoglycemic non-Hispanic Whites. Levels of apoH proteinwere positively related to the polymorphism in older women(a 3.4 % phenotypic variance). However, analysis of varianceshowed that APOH polymorphism and apoH protein levelswere positively correlated in both men and women. As inother metabolic pathways, genetic polymorphism might becorrelated with β2-GPI (apoH, protein) levels.
In 2000, Yasuda et al. [20] studied β2-GPI deficiency inhealthy Japanese individuals. Low plasma concentrations of
β2-GPI were not associated with apparent abnormalities inlipoprotein metabolism.
Lower levels of β2-GPI might, in fact, be determined byreduced gene expression as related to a functional polymor-phism at the transcriptional initiation site [21]. Large inter-individual variability in β2-GPI plasma levels, mostly underthe control of genetic factors, is widely accepted but its mo-lecular basis remains largely unknown. When analyzed byDHPLC, the 5’ flanking region of the β2-GPI gene had apoint mutation at the transcriptional initiation site (-1C→A)with a carrier frequency of 12.1 %. The mutation was associ-ated with significantly lower β2-GPI plasma levels(P<0.0001) and low occurrence of aPL in lupus patients(4.8 % antibody-positive group vs. 16.6 % in the antibody-negative group; P=0.019).
In 2004, Song et al. [22] evaluated the correlation betweenthrombotic events in patients with liver cirrhosis and theprevalence of β2-GPI antibodies. Plasma β2-GPI levels wereaffected by the presence of cirrhosis and correlated well withChild classification. Anti-β2-GPI antibodies were not corre-lated either with β2-GPI levels or with thrombosis occurrencein these patients.
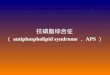
Fig. 1 a Patients with a high-risk aPL pattern (triple-positivity) have ahigh plasma β2GPI concentration (0.386±0.19 mgmL−1) compared withother, less risky, profiles (double or single-positivity patients, 0.218±0.09 mg mL−1 and 0.229±0.09 mg mL−1, respectively). b Patients withcatastrophic APS (CAPS) have higher β2GPI levels during the quiescentperiod (0.431±0.094 mg mL−1) than on the day of catastrophic clinicalmanifestations (0.361±0.088 mg mL−1, P=0.3)
424, Page 2 of 5 Curr Rheumatol Rep (2014) 16:424

Table1
Articlesreportingβ2-G
PIlevels
Articlesanalyzed
Results
Author
Year
Journal
Beta2
levels
Groupsevaluated
Rem
arks
VlachoyiannopoulosPG
etal.[15]
1993
Autoimmunity
APS
patientshadhigh
β2-G
PIlevels
SLEandAPS
APS
patientshadhigher
β2-G
PIlevelsthan
SLEpatients
McN
ally
etal.[16]
1995
BrJRheum
atol
Highβ2-G
PIlevelsin
APS
SLEor
PAPS
Resultssuggestthatβ
2-G
PIiscrucialin
thrombosisassociated
with
APS
McN
ally
etal.[17]
1995
Blood
CoagulF
ibrinolysis
Highβ2-G
PIlevelsin
APS
SLE+APS
orSLE
β2-G
PIcomplexed
iselevated
inpatientswith
APS
BalasubramanianKetal.[18]
1998
Throm
bRes
Highβ2-G
PIlevelsin
APS
APS
β2-G
PIplasmafractio
nisboundto
antibodies
inAPS
patients
MehediH
etal.[19]
1999
Hum
Genet
Low
β2-G
PIlevel
Polym
orphism
ornot
Geneticvariations
ofβ2-G
PIdeterm
ine
differentβ
2-G
PIplasmalevels
YasudaSetal.[20]
2000
Atherosclerosis
Low
β2-G
PIlevel
β2-G
PIdeficiency
Abnormallip
oprotein
metabolism
caused
β2-G
PIlevelsvariation
MehediH
etal.[21]
2003
Eur
JBiochem
Low
β2-G
PIlevel
Polym
orphism
Geneticvariations
ofβ2-G
PIdeterm
inedifferent
β2-G
PIplasmalevels
Song
KSetal.[22]
2004
Clin
ApplT
hrom
bHem
ost
Low
β2-G
PIlevel
Liver
cirrhosis
Noβ2-G
PIvariations
with
positiv
ea-β2-G
PIantib
odies
Lin
Fetal.[23]
2006
Lupus
Low
β2-G
PIlevel
Throm
botic
disordersand
inflam
mation
Largestreductionin
β2-G
PIlevelsoccurred
inpatientswith
thehighestC
RPvalues
deLaatB
etal.[24]
2009
Blood
Highβ2-G
PIlevel
Elderly
men
with
myocardial
infarctio
nReduced
β2-G
PIlevelsareassociated
with
alower
risk
ofmyocardialinfarction
Gries
A[25]
2009
Clin
Chim
Acta
Low
erβ2-G
PIlevel
Liver
cirrhosispopulatio
nβ2-G
PIplasmalevelsarereducedin
liver
disorders
Banzato
etal.
2014
CurrRheum
atol
Rep
Highβ2-G
PIplasmalevelin
triple-positive
APS
Triple,double,singleaPLor
CAPS
β2-G
PIishigh
intriplepositiv
itypatientsand
decreasesin
catastrophiccondition
Curr Rheumatol Rep (2014) 16:424 Page 3 of 5, 424

To further investigate the involvement of β2-GPI in throm-bosis and inflammation, in 2006, Lin et al. [23] measuredcirculating levels of β2-GPI in healthy controls, normal preg-nancies, patients with non-hemorrhagic stroke, patients withacute coronary syndrome, and patients with elevated C-reactive protein (CRP). β2-GPI levels were positively corre-lated with age (r=0.274, P<0.001) and dropped significantlyafter the eighth week of pregnancy (P=0.002). Reduced levelsof β2-GPI protein over time were reported for patients withstroke and myocardial infarction. As for inflammation, β2-GPI levels were negatively related to CRP (r=−0.284,P<0.001) and positively related to albumin and transferrin(r=0.372 and 0.453, respectively, with P<0.001 for both).
In 2009, de Laat et al. [24] showed that β2-GPI plasmalevels were related to the risk of myocardial infarction in oldermen. When men with a first myocardial infarction were com-pared with controls there was no important correlation be-tween β2-GPI plasma levels and the incidence of myocardialinfarction in the overall population. However, they found adose-dependent protective effect of increasing β2-GPI plasmalevels in men 60 years and older (OR 0.41, 95 % CI 0.22–0,74). This protective effect persisted despite high levels ofvWF.
Gries, in 2009 [25], studied β2-GPI plasma levels in livercirrhosis. They found thatβ2-GPI plasma levels are reduced inchronic liver disease.
Personal Experience
Our group set up a “sandwich” ELISA using a rabbit poly-clonal anti-human β2-GPI coated on a plate and a mousemonoclonal anti-human β2-GPI to detect the plasma concen-tration of bound β2-GPI. The system was developed by usinga phosphatase-labeled goat anti-mouse antibody. Increasingconcentrations of human purified β2-GPI were used to gener-ate a calibration reference curve. Plasma of 23 patients withAPS and triple positivity (LAC+, IgG aCL+, IgG aβ2-GPI+),eight with double positivity (IgG aCL+, IgG aβ2-GPI+, LACnegative), five with single positivity (IgG aβ2-GPI+, LAC andaCL negative) and 20 controls were evaluated. Moreover,plasma of four catastrophic APS patients (CAPS) were eval-uated on the day of CAPS clinical manifestations and afterrecovery. Median values between groups were compared byuse of the Mann–Whitney test (Fig. 1).
β2GPI concentrations were significantly higher in plasmafrom patients with triple positivity (LAC+, IgG aCL+, IgGaβ2GPI+) than in that from control subjects (0.386±0.19 mg mL−1 vs 0.175±0.06 mg mL−1, P=0.009). For dou-ble positivity (IgG aCL+, IgG aβ2GPI+) and single positivity(IgG aβ2GPI+) patients β2GPI levels were similar to those ofcontrols (0.218±0.09 mg mL−1 and 0.229±0.09 mg mL−1,respectively). Plasma from patients with CAPS contained
higher concentrations of β2GPI during the quiescent period(0.431±0.094 mg mL−1) than on the day of catastrophicclinical manifestations (0.361±0.088 mg mL−1, P=0.3). Ourresults revealed that the aPL profile was an important deter-minant of β2-GPI level.
Clinical Significance of Measuring β2-GPI Levels
On the basis of the results presented in Table 1, it is reasonableto affirm that β2-GPI plasma levels are increased in patientswith APS. The presence of free β2-GPI and β2-GPI–a β2-GPIcomplexes or altered binding to other plasma constituentscould explain the larger amount of circulating protein [17,18, 26]. Moreover, this might account for the higher β2-GPIlevels in APS patients than in SLE patients. Looking at ourown results, it is apparent that levels are increased in patientswith aβ2-GPI antibodies and especially in those with a hightiter of antibodies and those with triple positivity. On the otherhand, the increased amount of β2-GPI may be related tooverproduction by the liver because of its rapid turnover.This second hypothesis is not easy to demonstrate, becausethe protein should be tagged and re-injected in patients withAPS. Interestingly enough, the level of β2-GPI decreases inpatients with CAPS, meaning that its rapid consumption istaking place without immediate compensation by the liver. Tounderstand if this consumption is because of formation ofthrombi in the microcirculation remain to be proved. We donot see, at this time, a need for systematic measurement of theprotein in clinical practice; this is, at the moment, a matter forresearch only.
Conclusions and Future Research Directions
It could be useful and relevant to understand whether β2-GPIis directly involved in micro thrombi formation in CAPS.Immunochemical studies of biopsies of patients with CAPSmight provide insight into this.
Compliance with Ethics Guidelines
Conflict of Interest Alessandra Banzato and Vittorio Pengo declarethat they have no conflict of interest.
Human and Animal Rights and Informed Consent This article doesnot contain any studies with animal subjects performed by any of theauthors.
References
1. Schultze HE. Glycoproteins of human plasma. Bull Schweiz AkadMed Wiss. 1961;17:77–91.
424, Page 4 of 5 Curr Rheumatol Rep (2014) 16:424

2. Schultze HE,Mahling A. On the problem of the chemical structure ofplasma proteins. Bibl Haematol. 1961;12:197–224.
3. Aoyama Y, Chan YL, Wool IG. The primary structure of rat beta 2-glycoprotein I. Nucleic Acids Res. 1989;17:6401.
4. Lozier J, Takahashi N, Putnam FW. Complete amino acid sequenceof human plasma beta 2-glycoprotein I. Proc Natl Acad Sci U S A.1984;81:3640–4.
5. Bouma B, de Groot PG, van den Elsen JM, et al. Adhesion mecha-nism of human beta(2)-glycoprotein I to phospholipids based on itscrystal structure. EMBO J. 1999;18:5166–74.
6. Schwarzenbacher R, Zeth K, Diederichs K, et al. Crystal structure ofhuman beta2-glycoprotein I: implications for phospholipid bindingand the antiphospholipid syndrome. EMBO J. 1999;18:6228–39.
7. Shi T, Iverson GM,Qi JC, et al. Beta 2-Glycoprotein I binds factor XIand inhibits its activation by thrombin and factor XIIa: loss ofinhibition by clipped beta 2-glycoprotein I. Proc Natl Acad Sci U SA. 2004;101:3939–44.
8. Yasuda S, Atsumi T, Ieko M, Koike T. Beta2-glycoprotein I, anti-beta2-glycoprotein I, and fibrinolysis. Thromb Res. 2004;114:461–5.
9. Wurm H, Beubler E, Polz E, Holasek A, Kostner G. Studies on thepossible function of beta 2-glycoprotein-I: influence in the triglycer-ide metabolism in the rat. Metabolism. 1982;31:484–6.
10. Hasunuma Y, Matsuura E, Makita Z, Katahira T, Nishi S, Koike T.Involvement of beta 2-glycoprotein I and anticardiolipin antibodies inoxidatively modified low-density lipoprotein uptake by macro-phages. Clin Exp Immunol. 1997;107:569–73.
11. Mori T, Takeya H, Nishioka J, Gabazza EC, Suzuki K. beta 2-Glycoprotein I modulates the anticoagulant activity of activated proteinC on the phospholipid surface. Thromb Haemost. 1996;75:49–55.
12. Ieko M, Ichikawa K, Triplett DA, et al. Beta2-glycoprotein I isnecessary to inhibit protein C activity by monoclonal anticardiolipinantibodies. Arthritis Rheum. 1999;42:167–74.
13. Agar C, de Groot PG, Morgelin M, et al. beta(2)-glycoprotein I: anovel component of innate immunity. Blood. 2011;117:6939–47.
14. Pozzi N, Acquasaliente L, Frasson R, et al. beta2 -Glycoprotein Ibinds to thrombin and selectively inhibits the enzyme procoagulantfunctions. JThromb Haemost. 2013;11:1093–102.
15. Vlachoyiannopoulos PG, Beigbeder G, Dueymes M, et al.Antibodies to phosphatidylethanolamine in antiphospholipid syn-drome and systemic lupus erythematosus: their correlation withanticardiolipin antibodies and beta 2 glycoprotein-I plasma levels.Autoimmunity. 1993;16:245–9.
16. McNally T, Mackie IJ, Machin SJ, Isenberg DA. Increased levels ofbeta 2 glycoprotein-I antigen and beta 2 glycoprotein-I bindingantibodies are associated with a history of thromboembolic compli-cations in patients with SLE and primary antiphospholipid syndrome.Br J Rheumatol. 1995;34:1031–6.
17. McNally T, Mackie IJ, Machin SJ, Isenberg DA. Elevated levels ofbeta 2 glycoprotein-I (beta 2 GPI) in antiphospholipid antibodysyndrome are due to increased amounts of beta 2 GPI in associationwith other plasma constituents. Blood Coagul Fibrinolysis. 1995;6:411–6.
18. Balasubramanian K, Killion JJ, Schroit AJ. Estimation of plasmabeta-2-glycoprotein levels by competitive ELISA. Thromb Res.1998;92:91–7.
19. Mehdi H, Aston CE, Sanghera DK, Hamman RF, Kamboh MI.Genetic variation in the apolipoprotein H (beta2-glycoprotein I) geneaffects plasma apolipoprotein H concentrations. Hum Genet.1999;105:63–71.
20. Yasuda S, Tsutsumi A, Chiba H, et al. beta(2)-glycoprotein I defi-ciency: prevalence, genetic background and effects on plasma lipo-protein metabolism and hemostasis. Atherosclerosis. 2000;152:337–46.
21. Mehdi H, Manzi S, Desai P, et al. A functional polymorphism atthe transcriptional initiation site in beta2-glycoprotein I (apoli-poprotein H) associated with reduced gene expression and lowerplasma levels of beta2-glycoprotein I. Eur J Biochem. 2003;270:230–8.
22. Song KS, Kim HK. Prevalence of beta2-glycoprotein I antibody inpatients with liver cirrhosis: relationship with beta2-glycoprotein Iplasma levels and thrombosis. Clin Appl Thromb Hemost. 2004;10:183–6.
23. Lin F, Murphy R, White B, et al. Circulating levels of beta2-glycoprotein I in thrombotic disorders and in inflammation. Lupus.2006;15:87–93.
24. de Laat B, de Groot PG, Derksen RH, et al. Association betweenbeta2-glycoprotein I plasma levels and the risk of myocardial infarc-tion in older men. Blood. 2009;114:3656–61.
25. Gries A, Putz-Bankuti C, Stauber RE, Haditsch B, Stojakovic T.Beta2-glycoprotein-I plasma levels in liver cirrhosis. Clin ChimActa. 2009;403:257–8.
26. Banzato A, Frasson R, Acquasaliente L, et al. Circulating β2 glyco-protein I-IgG anti-β2 glycoprotein I immunocomplexes in patientswith definite antiphospholipid syndrome. Lupus. 2012;21(7):784–6.
Curr Rheumatol Rep (2014) 16:424 Page 5 of 5, 424