Embed Size (px)
Citation preview

Clinical StudyNewborn Screening for Sickle Cell Disease Technical andLegal Aspects of a German Pilot Study with 38220 Participants
Claudia Froumlmmel12 Annemarie Brose1 Jeannette Klein3
Oliver Blankenstein3 and Stephan Lobitz4
1 Labor Berlin-Charite Vivantes GmbH Sylter Straszlige 2 13353 Berlin Germany2 INSTAND eV Gesellschaft zur Forderung der Qualitatssicherung in Medizinischen Laboratorien eVUbierstraszlige 20 40223 Dusseldorf Germany
3Newborn Screening Laboratory Charite-Universitatsmedizin Berlin Augustenburger Platz 1 13353 Berlin Germany4Department of Pediatric OncologyHematologyBMT Charite-Universitatsmedizin BerlinAugustenburger Platz 1 13353 Berlin Germany
Correspondence should be addressed to Stephan Lobitz stephanlobitzcharitede
Received 20 January 2014 Revised 15 April 2014 Accepted 1 July 2014 Published 23 July 2014
Academic Editor Martin Bornhaeuser
Copyright copy 2014 Claudia Frommel et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Sickle cell disease (SCD) does not occur in the indigenous German population but with the increasing number of immigrantsfrom countries at high risk for hemoglobinopathies the question emerges whether or not a newborn screening program (NBS) forSCD disease should be initiated in Germany anyhow We have recently shown that in Berlin a city with a very large immigrantpopulation the incidence of SCD is considerable but our findings are insufficient to make a decision for the country as a wholeIn this paper we will show that a large body of epidemiological data can be generated in a relatively short period of time with avery high degree of precision and at relatively little expensemdasha result that might motivate other working groups to start such apilot project locally We examined previously collected dried blood cards that were up to six months old using high performanceliquid chromatography (HPLC) as first method and capillary electrophoresis (CE) as secondmethod A single part-time laboratorytechnician processed 38220 samples in a period of 162 working daysThe total costs per sample including all incidentals (as well aslabor costs) were EUR 144
1 Introduction
11 Sickle Cell Disease SCD is one of the most commonmonogenetic diseases worldwide Although it is most preva-lent in Africa in parts of the easternMediterranean and Asiaas a result of migration the prevalence is also continuouslyincreasing in central and northern Europe SCD comprises agroup of autosomal recessive 120573-hemoglobinopathies whosecommon feature is the occurrence of the pathognomonichemoglobin variant hemoglobin S (HbS) Its genetic correlateis the mutation HBBc20AgtT which is found in all patientsand which can occur homozygously or as compound het-erozygous state in combinationwith a number of othermuta-tions (eg HbC or 120573-thalassemia) In comparison with adulthemoglobin A (HbA) there is an amino acid substitution
in the HbS molecule with valine instead of glutamic acidin position 6 of the 120573-globin polypeptide chain If the HbScontent in an erythrocyte exceeds a critical concentration thisleads under certain conditions to polymerization of deoxy-genated HbS molecules the central pathophysiological eventof SCD Through a complex process this results in acute andchronic hemolysis as well as recurrent vasoocclusive eventscausing pain ischemia-reperfusion injury and finally chronicorgan damage [1]
12 Newborn Screening for Sickle Cell Disease Numerousstudies provide clear evidence that life-threatening early com-plications of SCD (eg sepsis splenic sequestration crisisetc) can be largely avoided if the diagnosis is made early thatis if possible in the first three to six months of life Simple
Hindawi Publishing CorporationBioMed Research InternationalVolume 2014 Article ID 695828 10 pageshttpdxdoiorg1011552014695828
2 BioMed Research International
but very effective prophylactic measures (eg vaccinationpenicillin prophylaxis etc) can then be initiated sufficientlyearly This can considerably reduce morbidity and mortality[2ndash10] In numerous countries SCD is therefore an establishedcomponent of national NBS programs In many other coun-tries in which there are no national NBS programs there areat least some regional projects and pilot studies [11ndash30]
The physicochemical properties of HbS differ from thoseof the normal HbAThis phenomenon is utilized for diagno-sis All physiological hemoglobins as well as all hemoglobinvariants show characteristic but not unambiguous migrationpatterns in all established separation methods As in eachmethod there are hemoglobins with the same or comparablemigration characteristics it is not possible to establish conclu-sively which hemoglobin is present in the concrete case Thismeans that the results of at least two different methods haveto be combined in order to be able to identify the hemoglobinpresent with sufficient certainty [31ndash34]This rule also appliesto NBS for SCD to avoid false-positive results The methodsmost commonly used in NBS for SCD for separation of thehemoglobins in dried blood specimens are HPLC isoelectricfocusing (IEF) and CE [32 35ndash37]
13TheGermanNewborn Screening Program InGermany allnewborns are entitled by law to take part in a national (so-called extended) NBS program [38] However participationis voluntary The extended NBS comprises 14 congenitalendocrine and metabolic disorders It does not include SCDIn addition all newborns are screened for hearing defectsThelist of disorders screened for in the German NBS programis laid down by the Federal Joint Committee (ldquoGemeinsamerBundesausschussrdquo G-BA)TheG-BA issues the guidelines forthe statutory health insurance funds (GKV) covering morethan 70 million insured persons in Germany It specifieswhich services in medical care are reimbursed by the GKV Ifa new disease is to be included in the extended NBS programit must meet the Wilson-Jungner criteria as modified byAndermann et al [39 40] to fit the special conditions of theGerman health system In particular there must be sufficientepidemiological data and it must have been demonstratedthat early detection of the disease in question is associatedwith a medical andor economic benefit
14 Sickle Cell Disease in Germany In Germany there arepractically no epidemiological data on the incidence andprevalence of SCD SCD has therefore not been perceived as asignificant problem in the German healthcare system to dateIn Berlin a city presumed to have a high incidence we per-formed a pilot project hitherto unique in Germany in whichall newborns born between 1 September 2011 and 30 Novem-ber 2012 who had given blood samples in the context ofthe extended NBS program were retrospectively additionallytested for SCD [41] The age of the specimens presented amethodological challenge However two earlier publicationshave shown that storage for at least six weeks at roomtemperature or 13 months at minus20∘C was possible [42 43]In addition to generation of epidemiological data a furthergoal of the project was therefore to investigate whether
the dried blood specimens can be stored for longer thansix weeks at room temperature and how they need to beprocessed after longer storage times in order to obtain reliablemeasurements These are important parameters for planningsimilar epidemiological pilot studies
In this paper we report on the technical aspects of ourstudy and we discuss in more detail the special legal situationin Germany
2 Methods
21 Ethics and Consent The ethics committee of the Chariteuniversity hospital approved the study on 28 September 2011(reference number EA208811) The parents of all newbornsinvestigated gave their written informed consent to reanalysisof blood in advance of sampling
22 Study Design and Population The present study is aretrospective cross-sectional investigation of an unselectedcohort of newborns All children born in Berlin between1 September 2011 and 30 November 2012 were consideredeligible for this project provided they took part in theextended NBS program Berlin is the capital of Germany andafter London the secondmost populated city in the EuropeanUnion On December 31 2010 Berlin had a populationof 3460725 of which 864065 (2497) had a migrationbackground Of those at least one half immigrated fromcountries with a high prevalence of hemoglobinopathies [44]
Altogether 39249 babies were born in the study periodOf these 95 parents or guardians did not give their consent toparticipation in the extended NBS A further 422 babies werenot included in the study because the parents or guardians didnot consent to storage of their childrenrsquos specimens beyondthe time necessary for the regular screening In 126 casesno consent was given to use of the specimens in a scientificproject and in 386 cases there was too little material availableto test additionally for SCD after the regular screening so thatin the end 38220 samples could be tested
23 Target Conditions The primary target conditions of thisstudy included SCD-SS SCD-SC SCD-SDPunjab SCD-SESCD-SLepore SCD-SOArab SCD-S120573-thalassemia SCD-S120575120573-thalassemia and SCD-SHPFH (hereditary persistenceof fetal hemoglobin) Secondary target conditions were HbSheterozygosity severe thalassemia and all hemoglobin vari-ants other than HbS in hetero- or homozygous form
24 Blood Sampling and Logistics The screening specimenswere normally collected from the newborns in the maternityclinic or at home between the 36th and 72nd hours oflife and sent to the Berlin NBS laboratory the same dayin the form of dried blood spot cards (Ahlstrom 226 IDBiological SystemsGreenville SCUSA)TheBerlinNBS lab-oratory (Laboratory 1) is one of 11 NBS laboratories inGermany (httpwwwscreening-dgnsdescreening-3php)which analyze specimens in the context of the extended NBSprogram and is the only NBS laboratory in Berlin
In newborns with a gestational age of less than 32 weeksthe initial screening was followed by a second screening at
BioMed Research International 3
Appropriate material and written consent Exclude sample
HPLC second variant present HPLC HbS present Screening negativeNo further action
CE HbS and second variant present
CE HbS present Repeat HPLC and CE HbS present
Determine HbSHbA ratio
Presumptive diagnosissickle cell disease
Presumptive diagnosissickle cell trait
RecallMolecular genetic analysis
Must not be reportedaccording to law
Confirmation ofpresumptive diagnosis
Definitive diagnosis sickle cell disease
Definitive diagnosis no sickle cell disease
No
No
No
No
No
NoYes
Yes
Yes
YesYes
Yes
Yes
gt2 lt2
Figure 1 Decision tree for handling samples of the babies born in the study period (119899 = 39249) Samples were excluded if there was noconsent for screening (119899 = 95) no consent to store the sample (119899 = 422) and no consent to use the sample in a scientific project (119899 = 126)too little material (119899 = 386) or a low AUC on the HPLC machine (119899 = 4236) Please note if any hemoglobin variant other than HbS wasdetected by means of HPLC this result was also confirmed by CE
a corrected age of 32 gestational weeks Further reasons forrepeat screening were performance of blood transfusions orcorticosteroid or dopamine therapy before collection of thespecimens for the first screening [45] In patients screenedmore than once the test for SCD was performed with the lastspecimen obtained
After completion of the regular screening in the contextof the extended NBS program the specimens were storedat room temperature in the NBS laboratory They were for-warded after 42 to 171 days for examination in the context ofour project
25 Measuring Methods All specimens were first examinedby HPLC Specimens with HPLC profiles consistent withSCD sickle cell trait 120573-thalassemia or variant hemoglobinsother than HbS were subsequently analyzed by CE as aconfirmatory method [41] (Figure 1)
26 High Performance Liquid Chromatography (HPLC) TheHPLC was performed on a VARIANT nbs Newborn Screen-ing System (Bio-Rad Laboratories Munich Germany) using
the VARIANT nbs Sickle Cell Program Unless expresslystated otherwise we followed the manufacturerrsquos recom-mendations The columns and all reagents such as buffersprimers and retention timemarkerswere purchased from themanufacturer
A disk with a diameter of 1810158401015840 (32mm) was punched outof the dried blood card and placed in a well of a 96-well plate240120583L distilled water was added per punched-out disk andthe sample incubated for 21 hours (overnight) at 4ndash6∘C Theeluate was then centrifuged for 10minutes at 1200 g to removethe solid elements (disk blood clots cellulose remains etc)remaining in the sampleThe pellet was left in the sample andthe supernatant measured with evaporation protection
The VARIANT nbs Newborn Screening System has adual-wavelength detector which measures the absorbanceof the sample components at 415 nm Background noise isreduced by additionally measuring each sample at 690 nmThe absorbance data are then transferred from the detectorto a connected PC and converted with the software GDM30 (Bio-Rad Laboratories Munich Germany) to a real timechromatogram in which the measured voltages (119910-axis) are
4 BioMed Research International
plotted against the time (119909-axis) The software analyzes thechromatograms fully automatically using the principle ofvalley-to-valley integration
In addition all chromatograms were visually inspectedWater blanks served as negative controls and were
included in every run As controls of the preanalytical processand the automated integration and quantitation of the peakswe used eluates from dried blood spot cards from HbS andHbC carriers and retention time markers provided by themanufacturer Interrun coefficients of variation (CV) weredetermined
27 Capillary Electrophoresis (CE) For the CE a disk 38mmin diameter was punched out of the dried blood spot card andplaced in a well of an 8-well strip tube After adding 50 120583Ldistilled water the sample was incubated in the CAPILLARYShumidity chamber at 4ndash6∘C for not less than two hoursand not more than 72 hours Then 06mL of hemolysingsolution was added Measurement of the hemolysate wasthen performed on a CAPILLARYS 2 CE system In eachrun controls with hemoglobins A F S and C provided bythe manufacturer were measured Data acquisition manage-ment and analysis were conducted with the PHORESIS 651software All material for the CE was purchased from SebiaFulda Germany
28 Handling of Results If both HPLC and CE analysesof a babyrsquos blood were indicative of SCD the family wascontacted and referred to our department of pediatric hema-tology where the presumed diagnosis was confirmed from afresh blood sample by molecular genetic analysis Telephonenumbers and addresses were extracted from the routine NBSdatabase Carrier states were not reported as required by ourlocal ethics committee
3 Results
A maximum of four 96-well plates was measured per dayand 455 plates were measured in 180 runs Six column lotswere used during the entire study Altogether 38220 sampleswere screened by HPLC 34084 of which were subject toevaluation 4236 samples had to be excluded because thecorresponding chromatograms showed a low total AUCAs expected the percentage of samples with a low AUCwas positively correlated with sample age (Figure 2) Oldersamples showed more degradation of hemoglobin resultingin more background noise and less analyzable materialOlder samples also contained more filter paper lint whichinterfered with the analysis by causing technical problemssuch as pressure increases or detector errors In one casewe observed a retention time shift With 74 of our oldest84 samples (881) we obtained chromatograms with anAUC gt 900000120583Vs although they had been taken fromdried blood spot cards 171 days previously The samples thusfulfilled theminimum criteria for testing which we defined asldquoadequate qualityrdquo Nevertheless the proportion of unusableresults increased significantly when the dried blood cardswere more than three months old (Figure 2)
50
60
70
80
90
100
40 60 80 100 120 140 160 180
Eval
uabl
e sam
ples
()
Age of samples (days)
Figure 2 Each dot represents themean of an average of 353 samples(range 24ndash1090) of the same age Of the samples that were analyzedwithin threemonths after being taken normallymore than 90wereevaluable
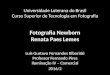
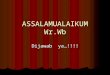
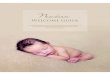
31 Screening-Positive Newborns Of 34084 samplesincluded 14 samples showed an HPLC pattern consistentwith the diagnosis of SCD 10 of which were interpreted asFS that is only hemoglobins F and S were assumed to bepresent An FS pattern indicates homozygosity for HbS aswell as compound heterozygosity for HbS and 120573-thalassemiaor 120575120573-thalassemia or HPFH respectively In four newbornswe detected an FSC pattern that is only hemoglobins F Sand C were present in these babies This is only explainableby compound heterozygosity for HbS and HbC clinicallyresulting in SCD-SC (Figure 3)
CE was used to corroborate HPLC results In all 14cases CE patterns were consistent with the correspondingHPLC results Consequently these newborns were consid-ered ldquoscreening positiverdquo and appointed to our pediatrichematology outpatient clinic to finally confirm diagnoses(Table 1) We did not observe false-positive findings
32 Screening-Negative Newborns The remaining 34070newborns showed hemoglobin patterns without any evi-dence of any phenotype of SCD and were thus classified asldquoscreening negativerdquo Among these we identified a total of 236newborns who were heterozygous for a hemoglobin variantThis was HbS in 165 cases HbE in 27 HbC in 23 and HbDin 11 In ten further cases there was a variant other than HbSE C or D In the cases interpreted as heterozygosity for HbSthe HbS HbA ratio was lt20
Until to date it has not come to our attention that inany of these screening-negative babies the diagnosis of SCDhas been made afterwards However these children are nowbetween 14 and 28 months of age and follow-up is notsystematically organized So it is possible that screening false-negative subjects for example children suffering frommildersubtypes of SCD like SCD-S120573+ thalassemia are missed
33 Precision of HPLC Retention time markers (RTM) wereprovided by the manufacturer RTM are lyophilized controlscontaining hemoglobins F A E and S and hemoglobins F A
BioMed Research International 5
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
011
020
029
070
079
144
(a)
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
012
021 031
050
070
080
116
(b)
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
011
020
028
049
070
076
115
141
(c)
04
03
02
01
00
01
00 05 10 15 20
Time (min)
011
020
029
050
071
077
117
167
(d)
Figure 3 Representative HPL chromatograms with the presumed hemoglobin patterns FA (a) FAS (b) FS (c) and FSC (d)
D and C respectively to monitor the precise separation ofthe aforementioned hemoglobins by the HPLC instrument[46] RTM help to detect instabilities in pump pressure orgradient composition which is an indispensable requirementfor correct analytical performance because raw data areprocessed electronically and the correct interpretation andintegration of peaks appearing in particular time windowsrequire the full functionality of the hardware
If the RTM indicated a functional disorder of the HPLCmachine we repeated the runs that were probably affectedTable 2 shows our results of several measurements (119899 =130) of the retention time markers in comparison to themanufacturerrsquos specifications Our data show a high precision
of retention times (CVle 15)Themaximumdeviation frommean retention time was plusmn0042min for HbS
Table 3 shows the mean and the range of retention timesof the various hemoglobins detected in the dried blood spotsamples of our study population The retrospective analysisof these retention times provides information about thestability of the HPLC system over the whole study periodwith this challenging material The CV was le 1 for all mainhemoglobins (A S E D and C)
As many factors during the whole analytical proceduremay affect test results dried blood samples from five new-borns found to be heterozygous for either HbS or HbCrespectively were established as additional quality controls
6 BioMed Research International
Table 1 Detailed information on screening-positive babies
Patient number (ethnical origin) Screening patterns HPLCCE Molecular genetic result 1 (West African) FSaFS SCD-SS 2 (West African) F5SaBFS SCD-SS 3 (Middle East) FSa5BFS SCD-S1205730 thalassemia 4 (West African) FaCSFSC SCD-SC 5 (Middle East) F4SAFS SCD-SS 6 (West African) FSCaFSC SCD-SC 7 (Middle East) FSa5FS SCD-SS 8 (West African) FSaBFS SCD-SS 9 (West African) FS4aFS SCD-SS 10 (West African) FS5aBFS SCD-SS 11 (West African) FCSaFSC SCD-SC 12 (West African) FSa2BFS SCD-SS 13 (West African) FSa2BFS SCD-SS 14 (West African) FCS1FSC SCD-SC
Table 2 High interrun precision of HPLC retention times of retention time markers
Hemoglobin Retention times of RTMmean (range) [min] CV []
Manufacturerrsquosspecifications mean
(range) [min]F 0494 (0471ndash0510) 15 0530 (0470ndash0590)A 0792 (0770ndash0804) 09 0800 (0730ndash0870)EA2 0954 (0919ndash0970) 10 0970 (0930ndash1010)D 1042 (1005ndash1072) 11 1060 (1010ndash1110)S 1158 (1116ndash1183) 12 1190 (1130ndash1250)C 1663 (1634ndash1684) 06 1680 (1610ndash1750)
Table 3 High precision of HPLC retention times of hemoglobins derived from dried blood spot samples
Presumptive hemoglobin Retention times mean (range) [min] CV [] 119899
A 0800 (0785ndash0816) 08 100E 0952 (0936ndash0968) 08 26D 1044 (1028ndash1060) 10 11S 1154 (1190ndash1130) 09 100C 1660 (1647ndash1670) 04 23
These samples were randomly integrated into several runsincluding all steps from pre- to postanalytics to include allinfluencing factors Table 4 shows the results of repeated ana-lyzes of these quality control samples known to be heterozy-gous for HbS (A) or HbC (B) on different working days
34 Precision of CE As quality controls of CE liquid controlsamples containing hemoglobins F A S and C were used ineach run on different working days (Table 5)
35 Costs All in all we examined samples from 38220 new-borns 37970 only by HPLC 250 additionally by CE becausethe samples showed an abnormal hemoglobin pattern in theHPLC For the examination of the entire cohort we incurredcosts of EUR 55000 A large part of this sum (just under50) was labor costs However the sum also contains the
costs for instrument hire for consumables and so forthThistranslates into a per-sample cost of EUR 144 (US$197)
4 Discussion
There are practically no epidemiological data to date on theprevalence and incidence of SCD in Germany [41 47 48]Cautious estimates made so far suggest a figure of about 3000to 4000 patients in the whole country These patients arewithout exception of immigrant origin [47]
Over a period of more than one year we tested withoutpreselection on the basis of ethnic origin 87 of all childrenborn in Berlin (34084 of 39249) for the presence of SCDand identified 14 with the disease [41] The incidence of SCD(41110000) amongst the children examined was thus higherthan the incidence of any other endocrine or metabolic
BioMed Research International 7
Table 4 (a) Interrun precision of HPLC determined on two dried blood spot samples from newborns heterozygous for HbS (b) Interrunprecision of HPLC determined on a dried blood spot sample from a newborn heterozygous for HbC
(a)
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] 119899
Control 1 373 29 89 53 36 63 11Control 2 401 48 19 27 10 50 8
(b)
HbF mean [] CV [] HbA mean [] CV [] HbC mean [] CV [] 119899
Control 3 396 57 17 22 13 28 11Precision was reduced if certain hemoglobin fractions were present in an order close to the detection limit of 1 of the total AUC
Table 5 Interrun precision of CE determined on liquid control samples provided by the manufacturer
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] HbC mean [] CV [] 119899Control FASC 188 48 355 20 145 43 54 77 5
disorder tested for in the context of the German extendedNBS program SCD should therefore be included in the NBSat least in Berlin In order to decidewhether there is a need fora national NBS program for SCD we now require data fromother regions particularly from presumed low-prevalenceareas
The results presented in this paper show that such epi-demiological data can be generated with investment ofrelatively little time and money as the samples do not needto be examined fresh on a day-to-day basis Instead largenumbers of samples can be analyzed retrospectively It is clearthat the costs per sample (144 EUR) in the context of ourpilot study will not be comparable with the expenses in thecontext of a national screening program While the costs forconsumables and so forth would probably be a little loweron account of the substantially higher patient numbers therewould be considerable additional expenses for administrativepurposes such as quality assurance Further additional costswould arise for staff training and for the entire infrastructurewhich has to be made available around the actual testing
In this study dried blood spot cards up to six monthsold provided satisfactory results However very old samplespresent a particular challenge because cellulose particleswhich come off the dried blood cards together with the bloodcan interfere considerably with the measurement They aredeposited in the fine capillaries of themeasuring instrumentsclogging them or creating additional unspecific measuringsignals The continuously increasing degradation of thehemoglobin also leads to additional measuring signals par-ticularly to increased background noise as well as reducingthe amount of analyzable material In the worst case onemight evenmiss a significant disease due tomisinterpretationof a peak resembling HbA for example a 120573-thalassemiamajor pattern could be confused with a physiological FApattern or homozygosity forHbS could be confusedwith SCTSample preparation is therefore of decisive importance
Factors which can influence the sample quality are asfollows
(1) The concentration of the hemoglobin in thehemolysate This depends on the volume of theblood sample thus on the saturation of the filter cardand on the degree of degradation of the hemoglobinThe latter is essentially dependent on the age and thestorage conditions of the sample Further importantparameters are the elution volume and elution time
(2) Instrument performance is influenced significantly bythe condition of the dried blood spot card This isin turn also dependent on the sample age and thestorage conditions In the case of older cards celluloseparticles are removed from the card together with theblood and can then interfere with the measurement
Prolonging the elution time increases the hemoglobinconcentration in the hemolysate and also the likelihood ofcellulose particles becoming detached from the filter cardThe elution conditions described in the methods section takeinto account both phenomena and represent the necessarycompromise
The implementation of pilot studies of this kind requiresthe availability of a high throughput method In our expe-rience HPLC and CE are equally suitable The CE electro-pherograms appeared to us to be easier to interpret than theHPLC chromatograms because there were fewer unspecificsignals in the former Whichever method is chosen it iscrucial that the analytical laboratory has special expertisewith regard to the IT-supported interpretation of the rawmeasurements
Disease screening programs are characterized by the factthat certain people are examined for the presence of a certaindisease simply because they belong to a certain populationThe subjects are examined or tested regardless of whetherthere is any concrete reason to suspect the presence of
8 BioMed Research International
the target disease The large majority of the subjects screenedare completely healthy This raises particular ethical legaltechnical and economic issues
The German Genetic Testing Act (GenDG) came intoforce on January 2 2010 and is a constant topic of debate onaccount of its very strict regulations [49] It controls genetictesting in humans and the use of genetic samples and dataThe GenDG specifies interalia that analyses of the productsof nucleic acids (gene product analyses) are also consideredgenetic analyses and therefore deemed legally equal to exam-ination of the number and structure of the chromosomes andof themolecular structure of DNA and RNAThismeans thathemoglobinopathy testing using protein separation methodssuch as HPLC or CE comes under the GenDG
Theultimate goal of theGenDG is to prevent the potentialdangers and discrimination associated with the examina-tion of human genetic traits One of the most importantprinciples is the right of the individual to informationalself-determination This right which enjoys internationallyunique protection in Germany includes the right to knowand more important in this context the right not to knowIts most important implication is that we are not allowed inGermany to report sickle cell trait
The GenDG distinguishes between genetic tests per-formed in amedical context and tests performed in a researchcontext and only applies to tests ordered in amedical contextA distinction is also made between diagnostic tests andpredictive tests In addition the GenDG regulates geneticscreening which would include NBS for SCD German lawrequires the establishment of an independent interdisci-plinary Genetic Testing Commission (GEKO) which hasbeen set up at the Robert Koch Institute and amongst otherthings lays down the requirements for the performance ofgenetic screening tests [49]These requirements are based onthe specific criteria for genetic screening developed byAnder-mann et al on the basis of theWHO screening criteria ofWil-son and Jungner [39 50]The GEKO has expressly stated thatresults of studies performed in other countries with differenthealthcare systems and different population structures can-not necessarily be extrapolated toGermany [51] For examplesome screening criteria are based on local conditions whichdo not obtain in Germany or at least not in all parts of thecountry Sickle cell patients cannot in particular be offeredstate-of-the-art care everywhere in Germany Nonmalignanthematology has been almost entirely neglected in the trainingof all groups of healthcare professionals in the past and thehemoglobinopathies as a whole are still not seen as a problemin Germany However a national strategy for preventionand treatment of SCD is currently under development TheSociety for Pediatric Oncology and Hematology (GPOH)has commissioned the establishment of a patient registerreference centers and a treatment guidelineThis is importantbecause if it is to make any sense a newborn screeningprogram requires not only the identification of sick babies butalso a functioning infrastructure which ensures that affectedchildren also receive appropriate care after the diagnosisThis includes both medical and psychosocial care as wellas sufficient counseling resources for the patients and theirparents
5 Conclusions
Our pilot project shows that itmakes sense at least regionallyto think about the introduction of some kind ofNBS programfor SCD in Germany whatever specific form this takesThe pilot projects necessary for this must be embarked onnow In addition to the presumed high-prevalence regionssuch as Berlin Hamburg the Ruhr region or Frankfurtepidemiological data should also be collected from pre-sumed low-prevalence regions (eg rural Bavaria and Baden-Wurttemberg)
Our data show that the organization and realization ofsuch pilot projects is relatively unproblematic and inexpen-sive as samples can be collected over several months and thenanalyzed together However we recommend that the samplesshould not be older than three months at the time of analysisIt is of fundamental importance that the Genetic Testing Actdoes not apply to such pilot projects as they involve genetictesting in the context of research
Conflict of Interests
Stephan Lobitz Claudia Frommel and Oliver Blankensteinreceived a research grant from Novartis Oncology GmbH(Nuremberg Germany) to perform this study In additionBio-Rad Laboratories GmbH (Munich Germany) indirectlyfunded this project through a preferential price for HPLCconsumables Beyond that the authors declare no competinginterest
Acknowledgments
This work is part of Stephan Lobitzrsquos dissertation in theUniversity College London ldquoMaster of Science in Haemoglo-binopathyrdquo program Stephan Lobitz is deeply indebted toDr Ratna Chatterjee Dr Rekha Bajoria the ThalassaemiaInternational Federation (TIF) and ldquoKINDerLEBEN-Vereinzur Forderung der Klinik fur krebskranke Kinder eV BerlinrdquoThe authors thank Novartis Oncology GmbH and Bio-RadLaboratories GmbH who generously funded this projectMany thanks are due to all parents and patients who took partin this study
References
[1] D C Rees T N Williams and M T Gladwin ldquoSickle-celldiseaserdquoThe Lancet vol 376 no 9757 pp 2018ndash2031 2010
[2] D Powars G Overturf J Weiss S Lee and L Chan ldquoPneumo-coccal septicemia in children with sickle cell anemia Changingtrend of survivalrdquo Journal of the American Medical Associationvol 245 no 18 pp 1839ndash1842 1981
[3] A M Emond R Collis D Darvill D R Higgs G H Maudeand G R Serjeant ldquoAcute splenic sequestration in homozygoussickle cell disease natural history and managementrdquo The Jour-nal of Pediatrics vol 107 no 2 pp 201ndash206 1985
[4] M H Gaston J I Verter G Woods et al ldquoProphylaxis withoral penicillin in children with sickle cell anemia a randomizedtrialrdquoThe New England Journal of Medicine vol 314 no 25 pp1593ndash1599 1986
BioMed Research International 9
[5] G R Serjeant and B E Serjeant ldquoManagement of sickle celldisease lessons from the Jamaican cohort studyrdquo Blood Reviewsvol 7 no 3 pp 137ndash145 1993
[6] A Lee P Thomas L Cupidore B Serjeant and G SerjeantldquoImproved survival in homozygous sickle cell disease lessonsfrom a cohort studyrdquo British Medical Journal vol 311 no 7020pp 1600ndash1602 1995
[7] T V Adamkiewicz S Sarnaik G R Buchanan et al ldquoInvasivepneumococcal infections in children with sickle cell diseasein the era of penicillin prophylaxis antibiotic resistance and23-valent pneumococcal polysaccharide vaccinationrdquo Journal ofPediatrics vol 143 no 4 pp 438ndash444 2003
[8] N B Halasa S M Shankar T R Talbot et al ldquoIncidence ofinvasive pneumococcal disease among individuals with sicklecell disease before and after the introduction of the pneumo-coccal conjugate vaccinerdquo Clinical Infectious Diseases vol 44no 11 pp 1428ndash1433 2007
[9] T V Adamkiewicz B J Silk J Howgate et al ldquoEffectiveness ofthe 7-valent pneumococcal conjugate vaccine in children withsickle cell disease in the first decade of liferdquo Pediatrics vol 121no 3 pp 562ndash569 2008
[10] S D Grosse H K Atrash I Odame D Amendah F B Pieland T N Williams ldquoThe Jamaican historical experience of theimpact of educational interventions on sickle cell disease childmortalityrdquoTheAmerican Journal of PreventiveMedicine vol 42no 6 pp e101ndashe103 2012
[11] H Heijboer X W van den Tweel M Peters M Knuist JPrins and H S Heymans ldquoOne year of neonatal screening forsickle cell disease in the emma kinderziekenhuisacademischmedisch centrum Amsterdamrdquo Nederlands Tijdschrift voorGeneeskunde vol 145 no 37 pp 1795ndash1799 2001
[12] B Gulbis F Cotton A Ferster et al ldquoNeonatal haemoglobin-opathy screening in Belgiumrdquo Journal of Clinical Pathology vol62 no 1 pp 49ndash52 2009
[13] A Streetly R Latinovic and J Henthorn ldquoPositive screeningand carrier results for the England-wide universal newbornsickle cell screening programme by ethnicity and area for 2005-07rdquo Journal of Clinical Pathology vol 63 no 7 pp 626ndash6292010
[14] E Ballardini A TaroccoMMarsella et al ldquoUniversal neonatalscreening for sickle cell disease and other haemoglobinopathiesin Ferrara Italyrdquo Blood Transfusion vol 11 no 2 pp 245ndash2492013
[15] J Bardakdjian-Michau M Bahuau D Hurtrel et al ldquoNeonatalscreening for sickle cell disease in Francerdquo Journal of ClinicalPathology vol 62 no 1 pp 31ndash33 2009
[16] E Cela De Julian E Dulın Iniguez M Guerrero Soler etal ldquoEvaluation of systematic neonatal screening for sickle celldiseases in Madrid three years after its introductionrdquo Anales dePediatria vol 66 no 4 pp 382ndash386 2007
[17] M J Bouva K Mohrmann H B J M Brinkman et alldquoImplementing neonatal screening for haemoglobinopathies inthe Netherlandsrdquo Journal of Medical Screening vol 17 no 2 pp58ndash65 2010
[18] P C GiordanoM J Bouva and C L Harteveld ldquoA confidentialinquiry estimating the number of patients affected with sicklecell disease and thalassemia major confirms the need for aprevention strategy in theNetherlandsrdquoHemoglobin vol 28 no4 pp 287ndash296 2004
[19] S Berthet F Monpoux A-M Soummer E Berard J Sarlesand C Badens ldquoNeonatal screening for sickle cell disease in
Nice University Hospital review of 8 last yearsrdquo Archives dePediatrie vol 17 no 12 pp 1652ndash1656 2010
[20] R Ducrocq M Benkerrou L Brahimi et al ldquoNeonatal screen-ing for sickle cell anemia evaluation of a five-year experience inan area of northern ParisrdquoArchives de Pediatrie vol 8 no 5 pp474ndash480 2001
[21] M Manu Pereira and J Vives Corrons ldquoNeonatal haemo-globinopathy screening in Spainrdquo Journal of Clinical Pathologyvol 62 no 1 pp 22ndash25 2009
[22] C Saint-Martin M Romana A Bibrac et al ldquoUniversalnewborn screening for haemoglobinopathies in Guadeloupe(French West Indies) a 27-year experiencerdquo Journal of MedicalScreening vol 20 no 4 pp 177ndash182 2013
[23] C L Lobo S K Ballas A C Domingos P G Moura E M doNascimento and G P Cardoso ldquoNewborn screening programfor hemoglobinopathies in Rio de Janeiro Brazilrdquo PediatricBlood and Cancer vol 61 no 1 pp 34ndash39 2014
[24] P T McGann M G Ferris U Ramamurthy et al ldquoA prospec-tive newborn screening and treatment program for sickle cellanemia in Luanda Angolardquo The American Journal of Hematol-ogy vol 88 no 12 pp 984ndash989 2013
[25] J Patel and G R Serjeant ldquoNewborn screening for sickle celldisease in India the need for defining optimal clinical carerdquoIndian Journal of Pediatrics vol 81 no 3 pp 229ndash230 2014
[26] S Hajer T Neila H F Sondess et al ldquoA lower-cost protocolfor sickle cell disease neonatal screening in Tunisiardquo Annals ofSaudi Medicine vol 32 no 1 pp 49ndash52 2012
[27] V S Hertzberg C F Hinton B L Therrell and S K ShapiraldquoBirth prevalence rates of newborn screening disorders inrelation to screening practices in the United Statesrdquo Journal ofPediatrics vol 159 no 4 pp 555ndash560 2011
[28] M C Rahimy A Gangbo G Ahouignan and E AlihonouldquoNewborn screening for sickle cell disease in the Republic ofBeninrdquo Journal of Clinical Pathology vol 62 no 1 pp 46ndash482009
[29] E Kafando E Nacoulma Y Ouattara et al ldquoNeonatal haemo-globinopathy screening in Burkina Fasordquo Journal of ClinicalPathology vol 62 no 1 pp 39ndash41 2009
[30] L Tshilolo L M Aissi D Lukusa et al ldquoNeonatal screening forsickle cell anaemia in the Democratic Republic of the Congoexperience from a pioneer project on 31 204 newbornsrdquo Journalof Clinical Pathology vol 62 no 1 pp 35ndash38 2009
[31] B J Bain ldquoHaemoglobinopathy diagnosis algorithms lessonsand pitfallsrdquo Blood Reviews vol 25 no 5 pp 205ndash213 2011
[32] K Ryan B J Bain D Worthington et al ldquoSignificant haemo-globinopathies guidelines for screening and diagnosisrdquo BritishJournal of Haematology vol 149 no 1 pp 35ndash49 2010
[33] J Riou C Godart D Hurtrel et al ldquoCation-exchange HPLCevaluated for presumptive identification of hemoglobin vari-antsrdquo Clinical Chemistry vol 43 no 1 pp 34ndash39 1997
[34] G RenomCMereau PMaboudou and J-M Perini ldquoPotentialof the Sebia Capillarys neonat fast automated system forneonatal screening of sickle cell diseaserdquoClinical Chemistry andLaboratory Medicine vol 47 no 11 pp 1423ndash1432 2009
[35] M Campbell J S Henthorn and S C Davies ldquoEvaluation ofcation-exchange HPLC compared with isoelectric focusing forneonatal hemoglobinopathy screeningrdquoClinical Chemistry vol45 no 7 pp 969ndash975 1999
[36] E Mantikou C L Harteveld and P C Giordano ldquoNewbornscreening for hemoglobinopathies using capillary electrophore-sis technology testing the Capillarys Neonat Fast Hb devicerdquoClinical Biochemistry vol 43 no 16-17 pp 1345ndash1350 2010
10 BioMed Research International
[37] F Kutlar ldquoDiagnostic approach to hemoglobinopathiesrdquoHemoglobin vol 31 no 2 pp 243ndash250 2007
[38] G Bundesausschuss Anlage 2 Erweitertes Neugeborenen-screening 2010 httpwwwg-badedownloads83-691-233RL Kinder Anlage-2 2010-12-16pdf
[39] A Andermann I Blancquaert S Beauchamp and I CostealdquoGuiding policy decisions for genetic screening developing asystematic and transparent approachrdquo Public Health Genomicsvol 14 no 1 pp 9ndash16 2010
[40] A Andermann I Blancquaert S Beauchamp and V DeryldquoRevisiting Wilson and Jungner in the genomic age a review ofscreening criteria over the past 40 yearsrdquo Bulletin of the WorldHealth Organization vol 86 no 4 pp 317ndash319 2008
[41] S Lobitz C Frommel A Brose J Klein and O BlankensteinldquoIncidence of sickle cell disease in an unselected cohort ofneonates born in Berlin Germanyrdquo European Journal of HumanGenetics 2014
[42] P D Roa E A Turner and M D P Aguinaga ldquoHemoglobinvariant detection from dried blood specimens by high perfor-mance liquid chromatographyrdquo Annals of Clinical and Labora-tory Science vol 23 no 6 pp 433ndash438 1993
[43] CMurray S KHall andPGriffiths ldquoAn evaluation of the Sebiacapillarys Neonat Haemoglobin FASTŮ system for routinenewborn screening for sickle cell diseaserdquo International Journalof Laboratory Hematology vol 33 no 5 pp 533ndash539 2011
[44] A F S B Brandenburg ldquoStatistisches Jahrbuch 2011rdquo 2011httpswwwstatistik-berlin-brandenburgdeprodukteJahrbuchjb2011JB 2011 BEpdf
[45] E Harms and B Olgemoller ldquoNeonatal screening for metabolicand endocrine disordersrdquo Deutsches Arzteblatt Internationalvol 108 no 1-2 pp 11ndash22 2011
[46] A Joutovsky J Hadzi-Nesic andM A Nardi ldquoHPLC retentiontime as a diagnostic tool for hemoglobin variants and hemo-globinopathies a study of 60 000 samples in a clinical diagnosticlaboratoryrdquo Clinical Chemistry vol 50 no 10 pp 1736ndash17472004
[47] E Kohne and E Kleihauer ldquoHemoglobinopathies in Ger-manymdasha longitudinal study over four decadesrdquo DeutschesArzteblatt vol 107 no 5 pp 65ndash71 2010
[48] R Dickerhoff O Genzel-Boroviczeny and E Kohne ldquoHaemo-globinopathies and newborn haemoglobinopathy screening inGermanyrdquo Journal of Clinical Pathology vol 62 no 1 article 342009
[49] Enactment of the German Federal Parliament (Bundestag)ldquoHuman Genetic Examination Act (Genetic Diagnosis Act-GenDG)rdquo 2009 httpswwweshgorgfileadminwwweshgorgdocumentsEuropeLegalWSGermany GenDG Law GermanEnglishpdf
[50] J M Wilson and Y G Jungner Principles and Practice of MassScreening for Disease WHO Public Health Papers 1968
[51] Gendiagnostik-Kommission ldquoRichtlinien der Gendiagnostik-Komission (GEKO) fur die Anforderung an die Durchfuhrunggenetischer Reihenuntersuchungen gemaszlig sect23 Abs 2 Nr 6GenDGrdquo Bundesgesundheitsblatt vol 56 pp 321ndash324 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
but very effective prophylactic measures (eg vaccinationpenicillin prophylaxis etc) can then be initiated sufficientlyearly This can considerably reduce morbidity and mortality[2ndash10] In numerous countries SCD is therefore an establishedcomponent of national NBS programs In many other coun-tries in which there are no national NBS programs there areat least some regional projects and pilot studies [11ndash30]
The physicochemical properties of HbS differ from thoseof the normal HbAThis phenomenon is utilized for diagno-sis All physiological hemoglobins as well as all hemoglobinvariants show characteristic but not unambiguous migrationpatterns in all established separation methods As in eachmethod there are hemoglobins with the same or comparablemigration characteristics it is not possible to establish conclu-sively which hemoglobin is present in the concrete case Thismeans that the results of at least two different methods haveto be combined in order to be able to identify the hemoglobinpresent with sufficient certainty [31ndash34]This rule also appliesto NBS for SCD to avoid false-positive results The methodsmost commonly used in NBS for SCD for separation of thehemoglobins in dried blood specimens are HPLC isoelectricfocusing (IEF) and CE [32 35ndash37]
13TheGermanNewborn Screening Program InGermany allnewborns are entitled by law to take part in a national (so-called extended) NBS program [38] However participationis voluntary The extended NBS comprises 14 congenitalendocrine and metabolic disorders It does not include SCDIn addition all newborns are screened for hearing defectsThelist of disorders screened for in the German NBS programis laid down by the Federal Joint Committee (ldquoGemeinsamerBundesausschussrdquo G-BA)TheG-BA issues the guidelines forthe statutory health insurance funds (GKV) covering morethan 70 million insured persons in Germany It specifieswhich services in medical care are reimbursed by the GKV Ifa new disease is to be included in the extended NBS programit must meet the Wilson-Jungner criteria as modified byAndermann et al [39 40] to fit the special conditions of theGerman health system In particular there must be sufficientepidemiological data and it must have been demonstratedthat early detection of the disease in question is associatedwith a medical andor economic benefit
14 Sickle Cell Disease in Germany In Germany there arepractically no epidemiological data on the incidence andprevalence of SCD SCD has therefore not been perceived as asignificant problem in the German healthcare system to dateIn Berlin a city presumed to have a high incidence we per-formed a pilot project hitherto unique in Germany in whichall newborns born between 1 September 2011 and 30 Novem-ber 2012 who had given blood samples in the context ofthe extended NBS program were retrospectively additionallytested for SCD [41] The age of the specimens presented amethodological challenge However two earlier publicationshave shown that storage for at least six weeks at roomtemperature or 13 months at minus20∘C was possible [42 43]In addition to generation of epidemiological data a furthergoal of the project was therefore to investigate whether
the dried blood specimens can be stored for longer thansix weeks at room temperature and how they need to beprocessed after longer storage times in order to obtain reliablemeasurements These are important parameters for planningsimilar epidemiological pilot studies
In this paper we report on the technical aspects of ourstudy and we discuss in more detail the special legal situationin Germany
2 Methods
21 Ethics and Consent The ethics committee of the Chariteuniversity hospital approved the study on 28 September 2011(reference number EA208811) The parents of all newbornsinvestigated gave their written informed consent to reanalysisof blood in advance of sampling
22 Study Design and Population The present study is aretrospective cross-sectional investigation of an unselectedcohort of newborns All children born in Berlin between1 September 2011 and 30 November 2012 were consideredeligible for this project provided they took part in theextended NBS program Berlin is the capital of Germany andafter London the secondmost populated city in the EuropeanUnion On December 31 2010 Berlin had a populationof 3460725 of which 864065 (2497) had a migrationbackground Of those at least one half immigrated fromcountries with a high prevalence of hemoglobinopathies [44]
Altogether 39249 babies were born in the study periodOf these 95 parents or guardians did not give their consent toparticipation in the extended NBS A further 422 babies werenot included in the study because the parents or guardians didnot consent to storage of their childrenrsquos specimens beyondthe time necessary for the regular screening In 126 casesno consent was given to use of the specimens in a scientificproject and in 386 cases there was too little material availableto test additionally for SCD after the regular screening so thatin the end 38220 samples could be tested
23 Target Conditions The primary target conditions of thisstudy included SCD-SS SCD-SC SCD-SDPunjab SCD-SESCD-SLepore SCD-SOArab SCD-S120573-thalassemia SCD-S120575120573-thalassemia and SCD-SHPFH (hereditary persistenceof fetal hemoglobin) Secondary target conditions were HbSheterozygosity severe thalassemia and all hemoglobin vari-ants other than HbS in hetero- or homozygous form
24 Blood Sampling and Logistics The screening specimenswere normally collected from the newborns in the maternityclinic or at home between the 36th and 72nd hours oflife and sent to the Berlin NBS laboratory the same dayin the form of dried blood spot cards (Ahlstrom 226 IDBiological SystemsGreenville SCUSA)TheBerlinNBS lab-oratory (Laboratory 1) is one of 11 NBS laboratories inGermany (httpwwwscreening-dgnsdescreening-3php)which analyze specimens in the context of the extended NBSprogram and is the only NBS laboratory in Berlin
In newborns with a gestational age of less than 32 weeksthe initial screening was followed by a second screening at
BioMed Research International 3
Appropriate material and written consent Exclude sample
HPLC second variant present HPLC HbS present Screening negativeNo further action
CE HbS and second variant present
CE HbS present Repeat HPLC and CE HbS present
Determine HbSHbA ratio
Presumptive diagnosissickle cell disease
Presumptive diagnosissickle cell trait
RecallMolecular genetic analysis
Must not be reportedaccording to law
Confirmation ofpresumptive diagnosis
Definitive diagnosis sickle cell disease
Definitive diagnosis no sickle cell disease
No
No
No
No
No
NoYes
Yes
Yes
YesYes
Yes
Yes
gt2 lt2
Figure 1 Decision tree for handling samples of the babies born in the study period (119899 = 39249) Samples were excluded if there was noconsent for screening (119899 = 95) no consent to store the sample (119899 = 422) and no consent to use the sample in a scientific project (119899 = 126)too little material (119899 = 386) or a low AUC on the HPLC machine (119899 = 4236) Please note if any hemoglobin variant other than HbS wasdetected by means of HPLC this result was also confirmed by CE
a corrected age of 32 gestational weeks Further reasons forrepeat screening were performance of blood transfusions orcorticosteroid or dopamine therapy before collection of thespecimens for the first screening [45] In patients screenedmore than once the test for SCD was performed with the lastspecimen obtained
After completion of the regular screening in the contextof the extended NBS program the specimens were storedat room temperature in the NBS laboratory They were for-warded after 42 to 171 days for examination in the context ofour project
25 Measuring Methods All specimens were first examinedby HPLC Specimens with HPLC profiles consistent withSCD sickle cell trait 120573-thalassemia or variant hemoglobinsother than HbS were subsequently analyzed by CE as aconfirmatory method [41] (Figure 1)
26 High Performance Liquid Chromatography (HPLC) TheHPLC was performed on a VARIANT nbs Newborn Screen-ing System (Bio-Rad Laboratories Munich Germany) using
the VARIANT nbs Sickle Cell Program Unless expresslystated otherwise we followed the manufacturerrsquos recom-mendations The columns and all reagents such as buffersprimers and retention timemarkerswere purchased from themanufacturer
A disk with a diameter of 1810158401015840 (32mm) was punched outof the dried blood card and placed in a well of a 96-well plate240120583L distilled water was added per punched-out disk andthe sample incubated for 21 hours (overnight) at 4ndash6∘C Theeluate was then centrifuged for 10minutes at 1200 g to removethe solid elements (disk blood clots cellulose remains etc)remaining in the sampleThe pellet was left in the sample andthe supernatant measured with evaporation protection
The VARIANT nbs Newborn Screening System has adual-wavelength detector which measures the absorbanceof the sample components at 415 nm Background noise isreduced by additionally measuring each sample at 690 nmThe absorbance data are then transferred from the detectorto a connected PC and converted with the software GDM30 (Bio-Rad Laboratories Munich Germany) to a real timechromatogram in which the measured voltages (119910-axis) are
4 BioMed Research International
plotted against the time (119909-axis) The software analyzes thechromatograms fully automatically using the principle ofvalley-to-valley integration
In addition all chromatograms were visually inspectedWater blanks served as negative controls and were
included in every run As controls of the preanalytical processand the automated integration and quantitation of the peakswe used eluates from dried blood spot cards from HbS andHbC carriers and retention time markers provided by themanufacturer Interrun coefficients of variation (CV) weredetermined
27 Capillary Electrophoresis (CE) For the CE a disk 38mmin diameter was punched out of the dried blood spot card andplaced in a well of an 8-well strip tube After adding 50 120583Ldistilled water the sample was incubated in the CAPILLARYShumidity chamber at 4ndash6∘C for not less than two hoursand not more than 72 hours Then 06mL of hemolysingsolution was added Measurement of the hemolysate wasthen performed on a CAPILLARYS 2 CE system In eachrun controls with hemoglobins A F S and C provided bythe manufacturer were measured Data acquisition manage-ment and analysis were conducted with the PHORESIS 651software All material for the CE was purchased from SebiaFulda Germany
28 Handling of Results If both HPLC and CE analysesof a babyrsquos blood were indicative of SCD the family wascontacted and referred to our department of pediatric hema-tology where the presumed diagnosis was confirmed from afresh blood sample by molecular genetic analysis Telephonenumbers and addresses were extracted from the routine NBSdatabase Carrier states were not reported as required by ourlocal ethics committee
3 Results
A maximum of four 96-well plates was measured per dayand 455 plates were measured in 180 runs Six column lotswere used during the entire study Altogether 38220 sampleswere screened by HPLC 34084 of which were subject toevaluation 4236 samples had to be excluded because thecorresponding chromatograms showed a low total AUCAs expected the percentage of samples with a low AUCwas positively correlated with sample age (Figure 2) Oldersamples showed more degradation of hemoglobin resultingin more background noise and less analyzable materialOlder samples also contained more filter paper lint whichinterfered with the analysis by causing technical problemssuch as pressure increases or detector errors In one casewe observed a retention time shift With 74 of our oldest84 samples (881) we obtained chromatograms with anAUC gt 900000120583Vs although they had been taken fromdried blood spot cards 171 days previously The samples thusfulfilled theminimum criteria for testing which we defined asldquoadequate qualityrdquo Nevertheless the proportion of unusableresults increased significantly when the dried blood cardswere more than three months old (Figure 2)
50
60
70
80
90
100
40 60 80 100 120 140 160 180
Eval
uabl
e sam
ples
()
Age of samples (days)
Figure 2 Each dot represents themean of an average of 353 samples(range 24ndash1090) of the same age Of the samples that were analyzedwithin threemonths after being taken normallymore than 90wereevaluable
31 Screening-Positive Newborns Of 34084 samplesincluded 14 samples showed an HPLC pattern consistentwith the diagnosis of SCD 10 of which were interpreted asFS that is only hemoglobins F and S were assumed to bepresent An FS pattern indicates homozygosity for HbS aswell as compound heterozygosity for HbS and 120573-thalassemiaor 120575120573-thalassemia or HPFH respectively In four newbornswe detected an FSC pattern that is only hemoglobins F Sand C were present in these babies This is only explainableby compound heterozygosity for HbS and HbC clinicallyresulting in SCD-SC (Figure 3)
CE was used to corroborate HPLC results In all 14cases CE patterns were consistent with the correspondingHPLC results Consequently these newborns were consid-ered ldquoscreening positiverdquo and appointed to our pediatrichematology outpatient clinic to finally confirm diagnoses(Table 1) We did not observe false-positive findings
32 Screening-Negative Newborns The remaining 34070newborns showed hemoglobin patterns without any evi-dence of any phenotype of SCD and were thus classified asldquoscreening negativerdquo Among these we identified a total of 236newborns who were heterozygous for a hemoglobin variantThis was HbS in 165 cases HbE in 27 HbC in 23 and HbDin 11 In ten further cases there was a variant other than HbSE C or D In the cases interpreted as heterozygosity for HbSthe HbS HbA ratio was lt20
Until to date it has not come to our attention that inany of these screening-negative babies the diagnosis of SCDhas been made afterwards However these children are nowbetween 14 and 28 months of age and follow-up is notsystematically organized So it is possible that screening false-negative subjects for example children suffering frommildersubtypes of SCD like SCD-S120573+ thalassemia are missed
33 Precision of HPLC Retention time markers (RTM) wereprovided by the manufacturer RTM are lyophilized controlscontaining hemoglobins F A E and S and hemoglobins F A
BioMed Research International 5
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
011
020
029
070
079
144
(a)
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
012
021 031
050
070
080
116
(b)
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
011
020
028
049
070
076
115
141
(c)
04
03
02
01
00
01
00 05 10 15 20
Time (min)
011
020
029
050
071
077
117
167
(d)
Figure 3 Representative HPL chromatograms with the presumed hemoglobin patterns FA (a) FAS (b) FS (c) and FSC (d)
D and C respectively to monitor the precise separation ofthe aforementioned hemoglobins by the HPLC instrument[46] RTM help to detect instabilities in pump pressure orgradient composition which is an indispensable requirementfor correct analytical performance because raw data areprocessed electronically and the correct interpretation andintegration of peaks appearing in particular time windowsrequire the full functionality of the hardware
If the RTM indicated a functional disorder of the HPLCmachine we repeated the runs that were probably affectedTable 2 shows our results of several measurements (119899 =130) of the retention time markers in comparison to themanufacturerrsquos specifications Our data show a high precision
of retention times (CVle 15)Themaximumdeviation frommean retention time was plusmn0042min for HbS
Table 3 shows the mean and the range of retention timesof the various hemoglobins detected in the dried blood spotsamples of our study population The retrospective analysisof these retention times provides information about thestability of the HPLC system over the whole study periodwith this challenging material The CV was le 1 for all mainhemoglobins (A S E D and C)
As many factors during the whole analytical proceduremay affect test results dried blood samples from five new-borns found to be heterozygous for either HbS or HbCrespectively were established as additional quality controls
6 BioMed Research International
Table 1 Detailed information on screening-positive babies
Patient number (ethnical origin) Screening patterns HPLCCE Molecular genetic result 1 (West African) FSaFS SCD-SS 2 (West African) F5SaBFS SCD-SS 3 (Middle East) FSa5BFS SCD-S1205730 thalassemia 4 (West African) FaCSFSC SCD-SC 5 (Middle East) F4SAFS SCD-SS 6 (West African) FSCaFSC SCD-SC 7 (Middle East) FSa5FS SCD-SS 8 (West African) FSaBFS SCD-SS 9 (West African) FS4aFS SCD-SS 10 (West African) FS5aBFS SCD-SS 11 (West African) FCSaFSC SCD-SC 12 (West African) FSa2BFS SCD-SS 13 (West African) FSa2BFS SCD-SS 14 (West African) FCS1FSC SCD-SC
Table 2 High interrun precision of HPLC retention times of retention time markers
Hemoglobin Retention times of RTMmean (range) [min] CV []
Manufacturerrsquosspecifications mean
(range) [min]F 0494 (0471ndash0510) 15 0530 (0470ndash0590)A 0792 (0770ndash0804) 09 0800 (0730ndash0870)EA2 0954 (0919ndash0970) 10 0970 (0930ndash1010)D 1042 (1005ndash1072) 11 1060 (1010ndash1110)S 1158 (1116ndash1183) 12 1190 (1130ndash1250)C 1663 (1634ndash1684) 06 1680 (1610ndash1750)
Table 3 High precision of HPLC retention times of hemoglobins derived from dried blood spot samples
Presumptive hemoglobin Retention times mean (range) [min] CV [] 119899
A 0800 (0785ndash0816) 08 100E 0952 (0936ndash0968) 08 26D 1044 (1028ndash1060) 10 11S 1154 (1190ndash1130) 09 100C 1660 (1647ndash1670) 04 23
These samples were randomly integrated into several runsincluding all steps from pre- to postanalytics to include allinfluencing factors Table 4 shows the results of repeated ana-lyzes of these quality control samples known to be heterozy-gous for HbS (A) or HbC (B) on different working days
34 Precision of CE As quality controls of CE liquid controlsamples containing hemoglobins F A S and C were used ineach run on different working days (Table 5)
35 Costs All in all we examined samples from 38220 new-borns 37970 only by HPLC 250 additionally by CE becausethe samples showed an abnormal hemoglobin pattern in theHPLC For the examination of the entire cohort we incurredcosts of EUR 55000 A large part of this sum (just under50) was labor costs However the sum also contains the
costs for instrument hire for consumables and so forthThistranslates into a per-sample cost of EUR 144 (US$197)
4 Discussion
There are practically no epidemiological data to date on theprevalence and incidence of SCD in Germany [41 47 48]Cautious estimates made so far suggest a figure of about 3000to 4000 patients in the whole country These patients arewithout exception of immigrant origin [47]
Over a period of more than one year we tested withoutpreselection on the basis of ethnic origin 87 of all childrenborn in Berlin (34084 of 39249) for the presence of SCDand identified 14 with the disease [41] The incidence of SCD(41110000) amongst the children examined was thus higherthan the incidence of any other endocrine or metabolic
BioMed Research International 7
Table 4 (a) Interrun precision of HPLC determined on two dried blood spot samples from newborns heterozygous for HbS (b) Interrunprecision of HPLC determined on a dried blood spot sample from a newborn heterozygous for HbC
(a)
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] 119899
Control 1 373 29 89 53 36 63 11Control 2 401 48 19 27 10 50 8
(b)
HbF mean [] CV [] HbA mean [] CV [] HbC mean [] CV [] 119899
Control 3 396 57 17 22 13 28 11Precision was reduced if certain hemoglobin fractions were present in an order close to the detection limit of 1 of the total AUC
Table 5 Interrun precision of CE determined on liquid control samples provided by the manufacturer
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] HbC mean [] CV [] 119899Control FASC 188 48 355 20 145 43 54 77 5
disorder tested for in the context of the German extendedNBS program SCD should therefore be included in the NBSat least in Berlin In order to decidewhether there is a need fora national NBS program for SCD we now require data fromother regions particularly from presumed low-prevalenceareas
The results presented in this paper show that such epi-demiological data can be generated with investment ofrelatively little time and money as the samples do not needto be examined fresh on a day-to-day basis Instead largenumbers of samples can be analyzed retrospectively It is clearthat the costs per sample (144 EUR) in the context of ourpilot study will not be comparable with the expenses in thecontext of a national screening program While the costs forconsumables and so forth would probably be a little loweron account of the substantially higher patient numbers therewould be considerable additional expenses for administrativepurposes such as quality assurance Further additional costswould arise for staff training and for the entire infrastructurewhich has to be made available around the actual testing
In this study dried blood spot cards up to six monthsold provided satisfactory results However very old samplespresent a particular challenge because cellulose particleswhich come off the dried blood cards together with the bloodcan interfere considerably with the measurement They aredeposited in the fine capillaries of themeasuring instrumentsclogging them or creating additional unspecific measuringsignals The continuously increasing degradation of thehemoglobin also leads to additional measuring signals par-ticularly to increased background noise as well as reducingthe amount of analyzable material In the worst case onemight evenmiss a significant disease due tomisinterpretationof a peak resembling HbA for example a 120573-thalassemiamajor pattern could be confused with a physiological FApattern or homozygosity forHbS could be confusedwith SCTSample preparation is therefore of decisive importance
Factors which can influence the sample quality are asfollows
(1) The concentration of the hemoglobin in thehemolysate This depends on the volume of theblood sample thus on the saturation of the filter cardand on the degree of degradation of the hemoglobinThe latter is essentially dependent on the age and thestorage conditions of the sample Further importantparameters are the elution volume and elution time
(2) Instrument performance is influenced significantly bythe condition of the dried blood spot card This isin turn also dependent on the sample age and thestorage conditions In the case of older cards celluloseparticles are removed from the card together with theblood and can then interfere with the measurement
Prolonging the elution time increases the hemoglobinconcentration in the hemolysate and also the likelihood ofcellulose particles becoming detached from the filter cardThe elution conditions described in the methods section takeinto account both phenomena and represent the necessarycompromise
The implementation of pilot studies of this kind requiresthe availability of a high throughput method In our expe-rience HPLC and CE are equally suitable The CE electro-pherograms appeared to us to be easier to interpret than theHPLC chromatograms because there were fewer unspecificsignals in the former Whichever method is chosen it iscrucial that the analytical laboratory has special expertisewith regard to the IT-supported interpretation of the rawmeasurements
Disease screening programs are characterized by the factthat certain people are examined for the presence of a certaindisease simply because they belong to a certain populationThe subjects are examined or tested regardless of whetherthere is any concrete reason to suspect the presence of
8 BioMed Research International
the target disease The large majority of the subjects screenedare completely healthy This raises particular ethical legaltechnical and economic issues
The German Genetic Testing Act (GenDG) came intoforce on January 2 2010 and is a constant topic of debate onaccount of its very strict regulations [49] It controls genetictesting in humans and the use of genetic samples and dataThe GenDG specifies interalia that analyses of the productsof nucleic acids (gene product analyses) are also consideredgenetic analyses and therefore deemed legally equal to exam-ination of the number and structure of the chromosomes andof themolecular structure of DNA and RNAThismeans thathemoglobinopathy testing using protein separation methodssuch as HPLC or CE comes under the GenDG
Theultimate goal of theGenDG is to prevent the potentialdangers and discrimination associated with the examina-tion of human genetic traits One of the most importantprinciples is the right of the individual to informationalself-determination This right which enjoys internationallyunique protection in Germany includes the right to knowand more important in this context the right not to knowIts most important implication is that we are not allowed inGermany to report sickle cell trait
The GenDG distinguishes between genetic tests per-formed in amedical context and tests performed in a researchcontext and only applies to tests ordered in amedical contextA distinction is also made between diagnostic tests andpredictive tests In addition the GenDG regulates geneticscreening which would include NBS for SCD German lawrequires the establishment of an independent interdisci-plinary Genetic Testing Commission (GEKO) which hasbeen set up at the Robert Koch Institute and amongst otherthings lays down the requirements for the performance ofgenetic screening tests [49]These requirements are based onthe specific criteria for genetic screening developed byAnder-mann et al on the basis of theWHO screening criteria ofWil-son and Jungner [39 50]The GEKO has expressly stated thatresults of studies performed in other countries with differenthealthcare systems and different population structures can-not necessarily be extrapolated toGermany [51] For examplesome screening criteria are based on local conditions whichdo not obtain in Germany or at least not in all parts of thecountry Sickle cell patients cannot in particular be offeredstate-of-the-art care everywhere in Germany Nonmalignanthematology has been almost entirely neglected in the trainingof all groups of healthcare professionals in the past and thehemoglobinopathies as a whole are still not seen as a problemin Germany However a national strategy for preventionand treatment of SCD is currently under development TheSociety for Pediatric Oncology and Hematology (GPOH)has commissioned the establishment of a patient registerreference centers and a treatment guidelineThis is importantbecause if it is to make any sense a newborn screeningprogram requires not only the identification of sick babies butalso a functioning infrastructure which ensures that affectedchildren also receive appropriate care after the diagnosisThis includes both medical and psychosocial care as wellas sufficient counseling resources for the patients and theirparents
5 Conclusions
Our pilot project shows that itmakes sense at least regionallyto think about the introduction of some kind ofNBS programfor SCD in Germany whatever specific form this takesThe pilot projects necessary for this must be embarked onnow In addition to the presumed high-prevalence regionssuch as Berlin Hamburg the Ruhr region or Frankfurtepidemiological data should also be collected from pre-sumed low-prevalence regions (eg rural Bavaria and Baden-Wurttemberg)
Our data show that the organization and realization ofsuch pilot projects is relatively unproblematic and inexpen-sive as samples can be collected over several months and thenanalyzed together However we recommend that the samplesshould not be older than three months at the time of analysisIt is of fundamental importance that the Genetic Testing Actdoes not apply to such pilot projects as they involve genetictesting in the context of research
Conflict of Interests
Stephan Lobitz Claudia Frommel and Oliver Blankensteinreceived a research grant from Novartis Oncology GmbH(Nuremberg Germany) to perform this study In additionBio-Rad Laboratories GmbH (Munich Germany) indirectlyfunded this project through a preferential price for HPLCconsumables Beyond that the authors declare no competinginterest
Acknowledgments
This work is part of Stephan Lobitzrsquos dissertation in theUniversity College London ldquoMaster of Science in Haemoglo-binopathyrdquo program Stephan Lobitz is deeply indebted toDr Ratna Chatterjee Dr Rekha Bajoria the ThalassaemiaInternational Federation (TIF) and ldquoKINDerLEBEN-Vereinzur Forderung der Klinik fur krebskranke Kinder eV BerlinrdquoThe authors thank Novartis Oncology GmbH and Bio-RadLaboratories GmbH who generously funded this projectMany thanks are due to all parents and patients who took partin this study
References
[1] D C Rees T N Williams and M T Gladwin ldquoSickle-celldiseaserdquoThe Lancet vol 376 no 9757 pp 2018ndash2031 2010
[2] D Powars G Overturf J Weiss S Lee and L Chan ldquoPneumo-coccal septicemia in children with sickle cell anemia Changingtrend of survivalrdquo Journal of the American Medical Associationvol 245 no 18 pp 1839ndash1842 1981
[3] A M Emond R Collis D Darvill D R Higgs G H Maudeand G R Serjeant ldquoAcute splenic sequestration in homozygoussickle cell disease natural history and managementrdquo The Jour-nal of Pediatrics vol 107 no 2 pp 201ndash206 1985
[4] M H Gaston J I Verter G Woods et al ldquoProphylaxis withoral penicillin in children with sickle cell anemia a randomizedtrialrdquoThe New England Journal of Medicine vol 314 no 25 pp1593ndash1599 1986
BioMed Research International 9
[5] G R Serjeant and B E Serjeant ldquoManagement of sickle celldisease lessons from the Jamaican cohort studyrdquo Blood Reviewsvol 7 no 3 pp 137ndash145 1993
[6] A Lee P Thomas L Cupidore B Serjeant and G SerjeantldquoImproved survival in homozygous sickle cell disease lessonsfrom a cohort studyrdquo British Medical Journal vol 311 no 7020pp 1600ndash1602 1995
[7] T V Adamkiewicz S Sarnaik G R Buchanan et al ldquoInvasivepneumococcal infections in children with sickle cell diseasein the era of penicillin prophylaxis antibiotic resistance and23-valent pneumococcal polysaccharide vaccinationrdquo Journal ofPediatrics vol 143 no 4 pp 438ndash444 2003
[8] N B Halasa S M Shankar T R Talbot et al ldquoIncidence ofinvasive pneumococcal disease among individuals with sicklecell disease before and after the introduction of the pneumo-coccal conjugate vaccinerdquo Clinical Infectious Diseases vol 44no 11 pp 1428ndash1433 2007
[9] T V Adamkiewicz B J Silk J Howgate et al ldquoEffectiveness ofthe 7-valent pneumococcal conjugate vaccine in children withsickle cell disease in the first decade of liferdquo Pediatrics vol 121no 3 pp 562ndash569 2008
[10] S D Grosse H K Atrash I Odame D Amendah F B Pieland T N Williams ldquoThe Jamaican historical experience of theimpact of educational interventions on sickle cell disease childmortalityrdquoTheAmerican Journal of PreventiveMedicine vol 42no 6 pp e101ndashe103 2012
[11] H Heijboer X W van den Tweel M Peters M Knuist JPrins and H S Heymans ldquoOne year of neonatal screening forsickle cell disease in the emma kinderziekenhuisacademischmedisch centrum Amsterdamrdquo Nederlands Tijdschrift voorGeneeskunde vol 145 no 37 pp 1795ndash1799 2001
[12] B Gulbis F Cotton A Ferster et al ldquoNeonatal haemoglobin-opathy screening in Belgiumrdquo Journal of Clinical Pathology vol62 no 1 pp 49ndash52 2009
[13] A Streetly R Latinovic and J Henthorn ldquoPositive screeningand carrier results for the England-wide universal newbornsickle cell screening programme by ethnicity and area for 2005-07rdquo Journal of Clinical Pathology vol 63 no 7 pp 626ndash6292010
[14] E Ballardini A TaroccoMMarsella et al ldquoUniversal neonatalscreening for sickle cell disease and other haemoglobinopathiesin Ferrara Italyrdquo Blood Transfusion vol 11 no 2 pp 245ndash2492013
[15] J Bardakdjian-Michau M Bahuau D Hurtrel et al ldquoNeonatalscreening for sickle cell disease in Francerdquo Journal of ClinicalPathology vol 62 no 1 pp 31ndash33 2009
[16] E Cela De Julian E Dulın Iniguez M Guerrero Soler etal ldquoEvaluation of systematic neonatal screening for sickle celldiseases in Madrid three years after its introductionrdquo Anales dePediatria vol 66 no 4 pp 382ndash386 2007
[17] M J Bouva K Mohrmann H B J M Brinkman et alldquoImplementing neonatal screening for haemoglobinopathies inthe Netherlandsrdquo Journal of Medical Screening vol 17 no 2 pp58ndash65 2010
[18] P C GiordanoM J Bouva and C L Harteveld ldquoA confidentialinquiry estimating the number of patients affected with sicklecell disease and thalassemia major confirms the need for aprevention strategy in theNetherlandsrdquoHemoglobin vol 28 no4 pp 287ndash296 2004
[19] S Berthet F Monpoux A-M Soummer E Berard J Sarlesand C Badens ldquoNeonatal screening for sickle cell disease in
Nice University Hospital review of 8 last yearsrdquo Archives dePediatrie vol 17 no 12 pp 1652ndash1656 2010
[20] R Ducrocq M Benkerrou L Brahimi et al ldquoNeonatal screen-ing for sickle cell anemia evaluation of a five-year experience inan area of northern ParisrdquoArchives de Pediatrie vol 8 no 5 pp474ndash480 2001
[21] M Manu Pereira and J Vives Corrons ldquoNeonatal haemo-globinopathy screening in Spainrdquo Journal of Clinical Pathologyvol 62 no 1 pp 22ndash25 2009
[22] C Saint-Martin M Romana A Bibrac et al ldquoUniversalnewborn screening for haemoglobinopathies in Guadeloupe(French West Indies) a 27-year experiencerdquo Journal of MedicalScreening vol 20 no 4 pp 177ndash182 2013
[23] C L Lobo S K Ballas A C Domingos P G Moura E M doNascimento and G P Cardoso ldquoNewborn screening programfor hemoglobinopathies in Rio de Janeiro Brazilrdquo PediatricBlood and Cancer vol 61 no 1 pp 34ndash39 2014
[24] P T McGann M G Ferris U Ramamurthy et al ldquoA prospec-tive newborn screening and treatment program for sickle cellanemia in Luanda Angolardquo The American Journal of Hematol-ogy vol 88 no 12 pp 984ndash989 2013
[25] J Patel and G R Serjeant ldquoNewborn screening for sickle celldisease in India the need for defining optimal clinical carerdquoIndian Journal of Pediatrics vol 81 no 3 pp 229ndash230 2014
[26] S Hajer T Neila H F Sondess et al ldquoA lower-cost protocolfor sickle cell disease neonatal screening in Tunisiardquo Annals ofSaudi Medicine vol 32 no 1 pp 49ndash52 2012
[27] V S Hertzberg C F Hinton B L Therrell and S K ShapiraldquoBirth prevalence rates of newborn screening disorders inrelation to screening practices in the United Statesrdquo Journal ofPediatrics vol 159 no 4 pp 555ndash560 2011
[28] M C Rahimy A Gangbo G Ahouignan and E AlihonouldquoNewborn screening for sickle cell disease in the Republic ofBeninrdquo Journal of Clinical Pathology vol 62 no 1 pp 46ndash482009
[29] E Kafando E Nacoulma Y Ouattara et al ldquoNeonatal haemo-globinopathy screening in Burkina Fasordquo Journal of ClinicalPathology vol 62 no 1 pp 39ndash41 2009
[30] L Tshilolo L M Aissi D Lukusa et al ldquoNeonatal screening forsickle cell anaemia in the Democratic Republic of the Congoexperience from a pioneer project on 31 204 newbornsrdquo Journalof Clinical Pathology vol 62 no 1 pp 35ndash38 2009
[31] B J Bain ldquoHaemoglobinopathy diagnosis algorithms lessonsand pitfallsrdquo Blood Reviews vol 25 no 5 pp 205ndash213 2011
[32] K Ryan B J Bain D Worthington et al ldquoSignificant haemo-globinopathies guidelines for screening and diagnosisrdquo BritishJournal of Haematology vol 149 no 1 pp 35ndash49 2010
[33] J Riou C Godart D Hurtrel et al ldquoCation-exchange HPLCevaluated for presumptive identification of hemoglobin vari-antsrdquo Clinical Chemistry vol 43 no 1 pp 34ndash39 1997
[34] G RenomCMereau PMaboudou and J-M Perini ldquoPotentialof the Sebia Capillarys neonat fast automated system forneonatal screening of sickle cell diseaserdquoClinical Chemistry andLaboratory Medicine vol 47 no 11 pp 1423ndash1432 2009
[35] M Campbell J S Henthorn and S C Davies ldquoEvaluation ofcation-exchange HPLC compared with isoelectric focusing forneonatal hemoglobinopathy screeningrdquoClinical Chemistry vol45 no 7 pp 969ndash975 1999
[36] E Mantikou C L Harteveld and P C Giordano ldquoNewbornscreening for hemoglobinopathies using capillary electrophore-sis technology testing the Capillarys Neonat Fast Hb devicerdquoClinical Biochemistry vol 43 no 16-17 pp 1345ndash1350 2010
10 BioMed Research International
[37] F Kutlar ldquoDiagnostic approach to hemoglobinopathiesrdquoHemoglobin vol 31 no 2 pp 243ndash250 2007
[38] G Bundesausschuss Anlage 2 Erweitertes Neugeborenen-screening 2010 httpwwwg-badedownloads83-691-233RL Kinder Anlage-2 2010-12-16pdf
[39] A Andermann I Blancquaert S Beauchamp and I CostealdquoGuiding policy decisions for genetic screening developing asystematic and transparent approachrdquo Public Health Genomicsvol 14 no 1 pp 9ndash16 2010
[40] A Andermann I Blancquaert S Beauchamp and V DeryldquoRevisiting Wilson and Jungner in the genomic age a review ofscreening criteria over the past 40 yearsrdquo Bulletin of the WorldHealth Organization vol 86 no 4 pp 317ndash319 2008
[41] S Lobitz C Frommel A Brose J Klein and O BlankensteinldquoIncidence of sickle cell disease in an unselected cohort ofneonates born in Berlin Germanyrdquo European Journal of HumanGenetics 2014
[42] P D Roa E A Turner and M D P Aguinaga ldquoHemoglobinvariant detection from dried blood specimens by high perfor-mance liquid chromatographyrdquo Annals of Clinical and Labora-tory Science vol 23 no 6 pp 433ndash438 1993
[43] CMurray S KHall andPGriffiths ldquoAn evaluation of the Sebiacapillarys Neonat Haemoglobin FASTŮ system for routinenewborn screening for sickle cell diseaserdquo International Journalof Laboratory Hematology vol 33 no 5 pp 533ndash539 2011
[44] A F S B Brandenburg ldquoStatistisches Jahrbuch 2011rdquo 2011httpswwwstatistik-berlin-brandenburgdeprodukteJahrbuchjb2011JB 2011 BEpdf
[45] E Harms and B Olgemoller ldquoNeonatal screening for metabolicand endocrine disordersrdquo Deutsches Arzteblatt Internationalvol 108 no 1-2 pp 11ndash22 2011
[46] A Joutovsky J Hadzi-Nesic andM A Nardi ldquoHPLC retentiontime as a diagnostic tool for hemoglobin variants and hemo-globinopathies a study of 60 000 samples in a clinical diagnosticlaboratoryrdquo Clinical Chemistry vol 50 no 10 pp 1736ndash17472004
[47] E Kohne and E Kleihauer ldquoHemoglobinopathies in Ger-manymdasha longitudinal study over four decadesrdquo DeutschesArzteblatt vol 107 no 5 pp 65ndash71 2010
[48] R Dickerhoff O Genzel-Boroviczeny and E Kohne ldquoHaemo-globinopathies and newborn haemoglobinopathy screening inGermanyrdquo Journal of Clinical Pathology vol 62 no 1 article 342009
[49] Enactment of the German Federal Parliament (Bundestag)ldquoHuman Genetic Examination Act (Genetic Diagnosis Act-GenDG)rdquo 2009 httpswwweshgorgfileadminwwweshgorgdocumentsEuropeLegalWSGermany GenDG Law GermanEnglishpdf
[50] J M Wilson and Y G Jungner Principles and Practice of MassScreening for Disease WHO Public Health Papers 1968
[51] Gendiagnostik-Kommission ldquoRichtlinien der Gendiagnostik-Komission (GEKO) fur die Anforderung an die Durchfuhrunggenetischer Reihenuntersuchungen gemaszlig sect23 Abs 2 Nr 6GenDGrdquo Bundesgesundheitsblatt vol 56 pp 321ndash324 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
Appropriate material and written consent Exclude sample
HPLC second variant present HPLC HbS present Screening negativeNo further action
CE HbS and second variant present
CE HbS present Repeat HPLC and CE HbS present
Determine HbSHbA ratio
Presumptive diagnosissickle cell disease
Presumptive diagnosissickle cell trait
RecallMolecular genetic analysis
Must not be reportedaccording to law
Confirmation ofpresumptive diagnosis
Definitive diagnosis sickle cell disease
Definitive diagnosis no sickle cell disease
No
No
No
No
No
NoYes
Yes
Yes
YesYes
Yes
Yes
gt2 lt2
Figure 1 Decision tree for handling samples of the babies born in the study period (119899 = 39249) Samples were excluded if there was noconsent for screening (119899 = 95) no consent to store the sample (119899 = 422) and no consent to use the sample in a scientific project (119899 = 126)too little material (119899 = 386) or a low AUC on the HPLC machine (119899 = 4236) Please note if any hemoglobin variant other than HbS wasdetected by means of HPLC this result was also confirmed by CE
a corrected age of 32 gestational weeks Further reasons forrepeat screening were performance of blood transfusions orcorticosteroid or dopamine therapy before collection of thespecimens for the first screening [45] In patients screenedmore than once the test for SCD was performed with the lastspecimen obtained
After completion of the regular screening in the contextof the extended NBS program the specimens were storedat room temperature in the NBS laboratory They were for-warded after 42 to 171 days for examination in the context ofour project
25 Measuring Methods All specimens were first examinedby HPLC Specimens with HPLC profiles consistent withSCD sickle cell trait 120573-thalassemia or variant hemoglobinsother than HbS were subsequently analyzed by CE as aconfirmatory method [41] (Figure 1)
26 High Performance Liquid Chromatography (HPLC) TheHPLC was performed on a VARIANT nbs Newborn Screen-ing System (Bio-Rad Laboratories Munich Germany) using
the VARIANT nbs Sickle Cell Program Unless expresslystated otherwise we followed the manufacturerrsquos recom-mendations The columns and all reagents such as buffersprimers and retention timemarkerswere purchased from themanufacturer
A disk with a diameter of 1810158401015840 (32mm) was punched outof the dried blood card and placed in a well of a 96-well plate240120583L distilled water was added per punched-out disk andthe sample incubated for 21 hours (overnight) at 4ndash6∘C Theeluate was then centrifuged for 10minutes at 1200 g to removethe solid elements (disk blood clots cellulose remains etc)remaining in the sampleThe pellet was left in the sample andthe supernatant measured with evaporation protection
The VARIANT nbs Newborn Screening System has adual-wavelength detector which measures the absorbanceof the sample components at 415 nm Background noise isreduced by additionally measuring each sample at 690 nmThe absorbance data are then transferred from the detectorto a connected PC and converted with the software GDM30 (Bio-Rad Laboratories Munich Germany) to a real timechromatogram in which the measured voltages (119910-axis) are
4 BioMed Research International
plotted against the time (119909-axis) The software analyzes thechromatograms fully automatically using the principle ofvalley-to-valley integration
In addition all chromatograms were visually inspectedWater blanks served as negative controls and were
included in every run As controls of the preanalytical processand the automated integration and quantitation of the peakswe used eluates from dried blood spot cards from HbS andHbC carriers and retention time markers provided by themanufacturer Interrun coefficients of variation (CV) weredetermined
27 Capillary Electrophoresis (CE) For the CE a disk 38mmin diameter was punched out of the dried blood spot card andplaced in a well of an 8-well strip tube After adding 50 120583Ldistilled water the sample was incubated in the CAPILLARYShumidity chamber at 4ndash6∘C for not less than two hoursand not more than 72 hours Then 06mL of hemolysingsolution was added Measurement of the hemolysate wasthen performed on a CAPILLARYS 2 CE system In eachrun controls with hemoglobins A F S and C provided bythe manufacturer were measured Data acquisition manage-ment and analysis were conducted with the PHORESIS 651software All material for the CE was purchased from SebiaFulda Germany
28 Handling of Results If both HPLC and CE analysesof a babyrsquos blood were indicative of SCD the family wascontacted and referred to our department of pediatric hema-tology where the presumed diagnosis was confirmed from afresh blood sample by molecular genetic analysis Telephonenumbers and addresses were extracted from the routine NBSdatabase Carrier states were not reported as required by ourlocal ethics committee
3 Results
A maximum of four 96-well plates was measured per dayand 455 plates were measured in 180 runs Six column lotswere used during the entire study Altogether 38220 sampleswere screened by HPLC 34084 of which were subject toevaluation 4236 samples had to be excluded because thecorresponding chromatograms showed a low total AUCAs expected the percentage of samples with a low AUCwas positively correlated with sample age (Figure 2) Oldersamples showed more degradation of hemoglobin resultingin more background noise and less analyzable materialOlder samples also contained more filter paper lint whichinterfered with the analysis by causing technical problemssuch as pressure increases or detector errors In one casewe observed a retention time shift With 74 of our oldest84 samples (881) we obtained chromatograms with anAUC gt 900000120583Vs although they had been taken fromdried blood spot cards 171 days previously The samples thusfulfilled theminimum criteria for testing which we defined asldquoadequate qualityrdquo Nevertheless the proportion of unusableresults increased significantly when the dried blood cardswere more than three months old (Figure 2)
50
60
70
80
90
100
40 60 80 100 120 140 160 180
Eval
uabl
e sam
ples
()
Age of samples (days)
Figure 2 Each dot represents themean of an average of 353 samples(range 24ndash1090) of the same age Of the samples that were analyzedwithin threemonths after being taken normallymore than 90wereevaluable
31 Screening-Positive Newborns Of 34084 samplesincluded 14 samples showed an HPLC pattern consistentwith the diagnosis of SCD 10 of which were interpreted asFS that is only hemoglobins F and S were assumed to bepresent An FS pattern indicates homozygosity for HbS aswell as compound heterozygosity for HbS and 120573-thalassemiaor 120575120573-thalassemia or HPFH respectively In four newbornswe detected an FSC pattern that is only hemoglobins F Sand C were present in these babies This is only explainableby compound heterozygosity for HbS and HbC clinicallyresulting in SCD-SC (Figure 3)
CE was used to corroborate HPLC results In all 14cases CE patterns were consistent with the correspondingHPLC results Consequently these newborns were consid-ered ldquoscreening positiverdquo and appointed to our pediatrichematology outpatient clinic to finally confirm diagnoses(Table 1) We did not observe false-positive findings
32 Screening-Negative Newborns The remaining 34070newborns showed hemoglobin patterns without any evi-dence of any phenotype of SCD and were thus classified asldquoscreening negativerdquo Among these we identified a total of 236newborns who were heterozygous for a hemoglobin variantThis was HbS in 165 cases HbE in 27 HbC in 23 and HbDin 11 In ten further cases there was a variant other than HbSE C or D In the cases interpreted as heterozygosity for HbSthe HbS HbA ratio was lt20
Until to date it has not come to our attention that inany of these screening-negative babies the diagnosis of SCDhas been made afterwards However these children are nowbetween 14 and 28 months of age and follow-up is notsystematically organized So it is possible that screening false-negative subjects for example children suffering frommildersubtypes of SCD like SCD-S120573+ thalassemia are missed
33 Precision of HPLC Retention time markers (RTM) wereprovided by the manufacturer RTM are lyophilized controlscontaining hemoglobins F A E and S and hemoglobins F A
BioMed Research International 5
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
011
020
029
070
079
144
(a)
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
012
021 031
050
070
080
116
(b)
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
011
020
028
049
070
076
115
141
(c)
04
03
02
01
00
01
00 05 10 15 20
Time (min)
011
020
029
050
071
077
117
167
(d)
Figure 3 Representative HPL chromatograms with the presumed hemoglobin patterns FA (a) FAS (b) FS (c) and FSC (d)
D and C respectively to monitor the precise separation ofthe aforementioned hemoglobins by the HPLC instrument[46] RTM help to detect instabilities in pump pressure orgradient composition which is an indispensable requirementfor correct analytical performance because raw data areprocessed electronically and the correct interpretation andintegration of peaks appearing in particular time windowsrequire the full functionality of the hardware
If the RTM indicated a functional disorder of the HPLCmachine we repeated the runs that were probably affectedTable 2 shows our results of several measurements (119899 =130) of the retention time markers in comparison to themanufacturerrsquos specifications Our data show a high precision
of retention times (CVle 15)Themaximumdeviation frommean retention time was plusmn0042min for HbS
Table 3 shows the mean and the range of retention timesof the various hemoglobins detected in the dried blood spotsamples of our study population The retrospective analysisof these retention times provides information about thestability of the HPLC system over the whole study periodwith this challenging material The CV was le 1 for all mainhemoglobins (A S E D and C)
As many factors during the whole analytical proceduremay affect test results dried blood samples from five new-borns found to be heterozygous for either HbS or HbCrespectively were established as additional quality controls
6 BioMed Research International
Table 1 Detailed information on screening-positive babies
Patient number (ethnical origin) Screening patterns HPLCCE Molecular genetic result 1 (West African) FSaFS SCD-SS 2 (West African) F5SaBFS SCD-SS 3 (Middle East) FSa5BFS SCD-S1205730 thalassemia 4 (West African) FaCSFSC SCD-SC 5 (Middle East) F4SAFS SCD-SS 6 (West African) FSCaFSC SCD-SC 7 (Middle East) FSa5FS SCD-SS 8 (West African) FSaBFS SCD-SS 9 (West African) FS4aFS SCD-SS 10 (West African) FS5aBFS SCD-SS 11 (West African) FCSaFSC SCD-SC 12 (West African) FSa2BFS SCD-SS 13 (West African) FSa2BFS SCD-SS 14 (West African) FCS1FSC SCD-SC
Table 2 High interrun precision of HPLC retention times of retention time markers
Hemoglobin Retention times of RTMmean (range) [min] CV []
Manufacturerrsquosspecifications mean
(range) [min]F 0494 (0471ndash0510) 15 0530 (0470ndash0590)A 0792 (0770ndash0804) 09 0800 (0730ndash0870)EA2 0954 (0919ndash0970) 10 0970 (0930ndash1010)D 1042 (1005ndash1072) 11 1060 (1010ndash1110)S 1158 (1116ndash1183) 12 1190 (1130ndash1250)C 1663 (1634ndash1684) 06 1680 (1610ndash1750)
Table 3 High precision of HPLC retention times of hemoglobins derived from dried blood spot samples
Presumptive hemoglobin Retention times mean (range) [min] CV [] 119899
A 0800 (0785ndash0816) 08 100E 0952 (0936ndash0968) 08 26D 1044 (1028ndash1060) 10 11S 1154 (1190ndash1130) 09 100C 1660 (1647ndash1670) 04 23
These samples were randomly integrated into several runsincluding all steps from pre- to postanalytics to include allinfluencing factors Table 4 shows the results of repeated ana-lyzes of these quality control samples known to be heterozy-gous for HbS (A) or HbC (B) on different working days
34 Precision of CE As quality controls of CE liquid controlsamples containing hemoglobins F A S and C were used ineach run on different working days (Table 5)
35 Costs All in all we examined samples from 38220 new-borns 37970 only by HPLC 250 additionally by CE becausethe samples showed an abnormal hemoglobin pattern in theHPLC For the examination of the entire cohort we incurredcosts of EUR 55000 A large part of this sum (just under50) was labor costs However the sum also contains the
costs for instrument hire for consumables and so forthThistranslates into a per-sample cost of EUR 144 (US$197)
4 Discussion
There are practically no epidemiological data to date on theprevalence and incidence of SCD in Germany [41 47 48]Cautious estimates made so far suggest a figure of about 3000to 4000 patients in the whole country These patients arewithout exception of immigrant origin [47]
Over a period of more than one year we tested withoutpreselection on the basis of ethnic origin 87 of all childrenborn in Berlin (34084 of 39249) for the presence of SCDand identified 14 with the disease [41] The incidence of SCD(41110000) amongst the children examined was thus higherthan the incidence of any other endocrine or metabolic
BioMed Research International 7
Table 4 (a) Interrun precision of HPLC determined on two dried blood spot samples from newborns heterozygous for HbS (b) Interrunprecision of HPLC determined on a dried blood spot sample from a newborn heterozygous for HbC
(a)
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] 119899
Control 1 373 29 89 53 36 63 11Control 2 401 48 19 27 10 50 8
(b)
HbF mean [] CV [] HbA mean [] CV [] HbC mean [] CV [] 119899
Control 3 396 57 17 22 13 28 11Precision was reduced if certain hemoglobin fractions were present in an order close to the detection limit of 1 of the total AUC
Table 5 Interrun precision of CE determined on liquid control samples provided by the manufacturer
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] HbC mean [] CV [] 119899Control FASC 188 48 355 20 145 43 54 77 5
disorder tested for in the context of the German extendedNBS program SCD should therefore be included in the NBSat least in Berlin In order to decidewhether there is a need fora national NBS program for SCD we now require data fromother regions particularly from presumed low-prevalenceareas
The results presented in this paper show that such epi-demiological data can be generated with investment ofrelatively little time and money as the samples do not needto be examined fresh on a day-to-day basis Instead largenumbers of samples can be analyzed retrospectively It is clearthat the costs per sample (144 EUR) in the context of ourpilot study will not be comparable with the expenses in thecontext of a national screening program While the costs forconsumables and so forth would probably be a little loweron account of the substantially higher patient numbers therewould be considerable additional expenses for administrativepurposes such as quality assurance Further additional costswould arise for staff training and for the entire infrastructurewhich has to be made available around the actual testing
In this study dried blood spot cards up to six monthsold provided satisfactory results However very old samplespresent a particular challenge because cellulose particleswhich come off the dried blood cards together with the bloodcan interfere considerably with the measurement They aredeposited in the fine capillaries of themeasuring instrumentsclogging them or creating additional unspecific measuringsignals The continuously increasing degradation of thehemoglobin also leads to additional measuring signals par-ticularly to increased background noise as well as reducingthe amount of analyzable material In the worst case onemight evenmiss a significant disease due tomisinterpretationof a peak resembling HbA for example a 120573-thalassemiamajor pattern could be confused with a physiological FApattern or homozygosity forHbS could be confusedwith SCTSample preparation is therefore of decisive importance
Factors which can influence the sample quality are asfollows
(1) The concentration of the hemoglobin in thehemolysate This depends on the volume of theblood sample thus on the saturation of the filter cardand on the degree of degradation of the hemoglobinThe latter is essentially dependent on the age and thestorage conditions of the sample Further importantparameters are the elution volume and elution time
(2) Instrument performance is influenced significantly bythe condition of the dried blood spot card This isin turn also dependent on the sample age and thestorage conditions In the case of older cards celluloseparticles are removed from the card together with theblood and can then interfere with the measurement
Prolonging the elution time increases the hemoglobinconcentration in the hemolysate and also the likelihood ofcellulose particles becoming detached from the filter cardThe elution conditions described in the methods section takeinto account both phenomena and represent the necessarycompromise
The implementation of pilot studies of this kind requiresthe availability of a high throughput method In our expe-rience HPLC and CE are equally suitable The CE electro-pherograms appeared to us to be easier to interpret than theHPLC chromatograms because there were fewer unspecificsignals in the former Whichever method is chosen it iscrucial that the analytical laboratory has special expertisewith regard to the IT-supported interpretation of the rawmeasurements
Disease screening programs are characterized by the factthat certain people are examined for the presence of a certaindisease simply because they belong to a certain populationThe subjects are examined or tested regardless of whetherthere is any concrete reason to suspect the presence of
8 BioMed Research International
the target disease The large majority of the subjects screenedare completely healthy This raises particular ethical legaltechnical and economic issues
The German Genetic Testing Act (GenDG) came intoforce on January 2 2010 and is a constant topic of debate onaccount of its very strict regulations [49] It controls genetictesting in humans and the use of genetic samples and dataThe GenDG specifies interalia that analyses of the productsof nucleic acids (gene product analyses) are also consideredgenetic analyses and therefore deemed legally equal to exam-ination of the number and structure of the chromosomes andof themolecular structure of DNA and RNAThismeans thathemoglobinopathy testing using protein separation methodssuch as HPLC or CE comes under the GenDG
Theultimate goal of theGenDG is to prevent the potentialdangers and discrimination associated with the examina-tion of human genetic traits One of the most importantprinciples is the right of the individual to informationalself-determination This right which enjoys internationallyunique protection in Germany includes the right to knowand more important in this context the right not to knowIts most important implication is that we are not allowed inGermany to report sickle cell trait
The GenDG distinguishes between genetic tests per-formed in amedical context and tests performed in a researchcontext and only applies to tests ordered in amedical contextA distinction is also made between diagnostic tests andpredictive tests In addition the GenDG regulates geneticscreening which would include NBS for SCD German lawrequires the establishment of an independent interdisci-plinary Genetic Testing Commission (GEKO) which hasbeen set up at the Robert Koch Institute and amongst otherthings lays down the requirements for the performance ofgenetic screening tests [49]These requirements are based onthe specific criteria for genetic screening developed byAnder-mann et al on the basis of theWHO screening criteria ofWil-son and Jungner [39 50]The GEKO has expressly stated thatresults of studies performed in other countries with differenthealthcare systems and different population structures can-not necessarily be extrapolated toGermany [51] For examplesome screening criteria are based on local conditions whichdo not obtain in Germany or at least not in all parts of thecountry Sickle cell patients cannot in particular be offeredstate-of-the-art care everywhere in Germany Nonmalignanthematology has been almost entirely neglected in the trainingof all groups of healthcare professionals in the past and thehemoglobinopathies as a whole are still not seen as a problemin Germany However a national strategy for preventionand treatment of SCD is currently under development TheSociety for Pediatric Oncology and Hematology (GPOH)has commissioned the establishment of a patient registerreference centers and a treatment guidelineThis is importantbecause if it is to make any sense a newborn screeningprogram requires not only the identification of sick babies butalso a functioning infrastructure which ensures that affectedchildren also receive appropriate care after the diagnosisThis includes both medical and psychosocial care as wellas sufficient counseling resources for the patients and theirparents
5 Conclusions
Our pilot project shows that itmakes sense at least regionallyto think about the introduction of some kind ofNBS programfor SCD in Germany whatever specific form this takesThe pilot projects necessary for this must be embarked onnow In addition to the presumed high-prevalence regionssuch as Berlin Hamburg the Ruhr region or Frankfurtepidemiological data should also be collected from pre-sumed low-prevalence regions (eg rural Bavaria and Baden-Wurttemberg)
Our data show that the organization and realization ofsuch pilot projects is relatively unproblematic and inexpen-sive as samples can be collected over several months and thenanalyzed together However we recommend that the samplesshould not be older than three months at the time of analysisIt is of fundamental importance that the Genetic Testing Actdoes not apply to such pilot projects as they involve genetictesting in the context of research
Conflict of Interests
Stephan Lobitz Claudia Frommel and Oliver Blankensteinreceived a research grant from Novartis Oncology GmbH(Nuremberg Germany) to perform this study In additionBio-Rad Laboratories GmbH (Munich Germany) indirectlyfunded this project through a preferential price for HPLCconsumables Beyond that the authors declare no competinginterest
Acknowledgments
This work is part of Stephan Lobitzrsquos dissertation in theUniversity College London ldquoMaster of Science in Haemoglo-binopathyrdquo program Stephan Lobitz is deeply indebted toDr Ratna Chatterjee Dr Rekha Bajoria the ThalassaemiaInternational Federation (TIF) and ldquoKINDerLEBEN-Vereinzur Forderung der Klinik fur krebskranke Kinder eV BerlinrdquoThe authors thank Novartis Oncology GmbH and Bio-RadLaboratories GmbH who generously funded this projectMany thanks are due to all parents and patients who took partin this study
References
[1] D C Rees T N Williams and M T Gladwin ldquoSickle-celldiseaserdquoThe Lancet vol 376 no 9757 pp 2018ndash2031 2010
[2] D Powars G Overturf J Weiss S Lee and L Chan ldquoPneumo-coccal septicemia in children with sickle cell anemia Changingtrend of survivalrdquo Journal of the American Medical Associationvol 245 no 18 pp 1839ndash1842 1981
[3] A M Emond R Collis D Darvill D R Higgs G H Maudeand G R Serjeant ldquoAcute splenic sequestration in homozygoussickle cell disease natural history and managementrdquo The Jour-nal of Pediatrics vol 107 no 2 pp 201ndash206 1985
[4] M H Gaston J I Verter G Woods et al ldquoProphylaxis withoral penicillin in children with sickle cell anemia a randomizedtrialrdquoThe New England Journal of Medicine vol 314 no 25 pp1593ndash1599 1986
BioMed Research International 9
[5] G R Serjeant and B E Serjeant ldquoManagement of sickle celldisease lessons from the Jamaican cohort studyrdquo Blood Reviewsvol 7 no 3 pp 137ndash145 1993
[6] A Lee P Thomas L Cupidore B Serjeant and G SerjeantldquoImproved survival in homozygous sickle cell disease lessonsfrom a cohort studyrdquo British Medical Journal vol 311 no 7020pp 1600ndash1602 1995
[7] T V Adamkiewicz S Sarnaik G R Buchanan et al ldquoInvasivepneumococcal infections in children with sickle cell diseasein the era of penicillin prophylaxis antibiotic resistance and23-valent pneumococcal polysaccharide vaccinationrdquo Journal ofPediatrics vol 143 no 4 pp 438ndash444 2003
[8] N B Halasa S M Shankar T R Talbot et al ldquoIncidence ofinvasive pneumococcal disease among individuals with sicklecell disease before and after the introduction of the pneumo-coccal conjugate vaccinerdquo Clinical Infectious Diseases vol 44no 11 pp 1428ndash1433 2007
[9] T V Adamkiewicz B J Silk J Howgate et al ldquoEffectiveness ofthe 7-valent pneumococcal conjugate vaccine in children withsickle cell disease in the first decade of liferdquo Pediatrics vol 121no 3 pp 562ndash569 2008
[10] S D Grosse H K Atrash I Odame D Amendah F B Pieland T N Williams ldquoThe Jamaican historical experience of theimpact of educational interventions on sickle cell disease childmortalityrdquoTheAmerican Journal of PreventiveMedicine vol 42no 6 pp e101ndashe103 2012
[11] H Heijboer X W van den Tweel M Peters M Knuist JPrins and H S Heymans ldquoOne year of neonatal screening forsickle cell disease in the emma kinderziekenhuisacademischmedisch centrum Amsterdamrdquo Nederlands Tijdschrift voorGeneeskunde vol 145 no 37 pp 1795ndash1799 2001
[12] B Gulbis F Cotton A Ferster et al ldquoNeonatal haemoglobin-opathy screening in Belgiumrdquo Journal of Clinical Pathology vol62 no 1 pp 49ndash52 2009
[13] A Streetly R Latinovic and J Henthorn ldquoPositive screeningand carrier results for the England-wide universal newbornsickle cell screening programme by ethnicity and area for 2005-07rdquo Journal of Clinical Pathology vol 63 no 7 pp 626ndash6292010
[14] E Ballardini A TaroccoMMarsella et al ldquoUniversal neonatalscreening for sickle cell disease and other haemoglobinopathiesin Ferrara Italyrdquo Blood Transfusion vol 11 no 2 pp 245ndash2492013
[15] J Bardakdjian-Michau M Bahuau D Hurtrel et al ldquoNeonatalscreening for sickle cell disease in Francerdquo Journal of ClinicalPathology vol 62 no 1 pp 31ndash33 2009
[16] E Cela De Julian E Dulın Iniguez M Guerrero Soler etal ldquoEvaluation of systematic neonatal screening for sickle celldiseases in Madrid three years after its introductionrdquo Anales dePediatria vol 66 no 4 pp 382ndash386 2007
[17] M J Bouva K Mohrmann H B J M Brinkman et alldquoImplementing neonatal screening for haemoglobinopathies inthe Netherlandsrdquo Journal of Medical Screening vol 17 no 2 pp58ndash65 2010
[18] P C GiordanoM J Bouva and C L Harteveld ldquoA confidentialinquiry estimating the number of patients affected with sicklecell disease and thalassemia major confirms the need for aprevention strategy in theNetherlandsrdquoHemoglobin vol 28 no4 pp 287ndash296 2004
[19] S Berthet F Monpoux A-M Soummer E Berard J Sarlesand C Badens ldquoNeonatal screening for sickle cell disease in
Nice University Hospital review of 8 last yearsrdquo Archives dePediatrie vol 17 no 12 pp 1652ndash1656 2010
[20] R Ducrocq M Benkerrou L Brahimi et al ldquoNeonatal screen-ing for sickle cell anemia evaluation of a five-year experience inan area of northern ParisrdquoArchives de Pediatrie vol 8 no 5 pp474ndash480 2001
[21] M Manu Pereira and J Vives Corrons ldquoNeonatal haemo-globinopathy screening in Spainrdquo Journal of Clinical Pathologyvol 62 no 1 pp 22ndash25 2009
[22] C Saint-Martin M Romana A Bibrac et al ldquoUniversalnewborn screening for haemoglobinopathies in Guadeloupe(French West Indies) a 27-year experiencerdquo Journal of MedicalScreening vol 20 no 4 pp 177ndash182 2013
[23] C L Lobo S K Ballas A C Domingos P G Moura E M doNascimento and G P Cardoso ldquoNewborn screening programfor hemoglobinopathies in Rio de Janeiro Brazilrdquo PediatricBlood and Cancer vol 61 no 1 pp 34ndash39 2014
[24] P T McGann M G Ferris U Ramamurthy et al ldquoA prospec-tive newborn screening and treatment program for sickle cellanemia in Luanda Angolardquo The American Journal of Hematol-ogy vol 88 no 12 pp 984ndash989 2013
[25] J Patel and G R Serjeant ldquoNewborn screening for sickle celldisease in India the need for defining optimal clinical carerdquoIndian Journal of Pediatrics vol 81 no 3 pp 229ndash230 2014
[26] S Hajer T Neila H F Sondess et al ldquoA lower-cost protocolfor sickle cell disease neonatal screening in Tunisiardquo Annals ofSaudi Medicine vol 32 no 1 pp 49ndash52 2012
[27] V S Hertzberg C F Hinton B L Therrell and S K ShapiraldquoBirth prevalence rates of newborn screening disorders inrelation to screening practices in the United Statesrdquo Journal ofPediatrics vol 159 no 4 pp 555ndash560 2011
[28] M C Rahimy A Gangbo G Ahouignan and E AlihonouldquoNewborn screening for sickle cell disease in the Republic ofBeninrdquo Journal of Clinical Pathology vol 62 no 1 pp 46ndash482009
[29] E Kafando E Nacoulma Y Ouattara et al ldquoNeonatal haemo-globinopathy screening in Burkina Fasordquo Journal of ClinicalPathology vol 62 no 1 pp 39ndash41 2009
[30] L Tshilolo L M Aissi D Lukusa et al ldquoNeonatal screening forsickle cell anaemia in the Democratic Republic of the Congoexperience from a pioneer project on 31 204 newbornsrdquo Journalof Clinical Pathology vol 62 no 1 pp 35ndash38 2009
[31] B J Bain ldquoHaemoglobinopathy diagnosis algorithms lessonsand pitfallsrdquo Blood Reviews vol 25 no 5 pp 205ndash213 2011
[32] K Ryan B J Bain D Worthington et al ldquoSignificant haemo-globinopathies guidelines for screening and diagnosisrdquo BritishJournal of Haematology vol 149 no 1 pp 35ndash49 2010
[33] J Riou C Godart D Hurtrel et al ldquoCation-exchange HPLCevaluated for presumptive identification of hemoglobin vari-antsrdquo Clinical Chemistry vol 43 no 1 pp 34ndash39 1997
[34] G RenomCMereau PMaboudou and J-M Perini ldquoPotentialof the Sebia Capillarys neonat fast automated system forneonatal screening of sickle cell diseaserdquoClinical Chemistry andLaboratory Medicine vol 47 no 11 pp 1423ndash1432 2009
[35] M Campbell J S Henthorn and S C Davies ldquoEvaluation ofcation-exchange HPLC compared with isoelectric focusing forneonatal hemoglobinopathy screeningrdquoClinical Chemistry vol45 no 7 pp 969ndash975 1999
[36] E Mantikou C L Harteveld and P C Giordano ldquoNewbornscreening for hemoglobinopathies using capillary electrophore-sis technology testing the Capillarys Neonat Fast Hb devicerdquoClinical Biochemistry vol 43 no 16-17 pp 1345ndash1350 2010
10 BioMed Research International
[37] F Kutlar ldquoDiagnostic approach to hemoglobinopathiesrdquoHemoglobin vol 31 no 2 pp 243ndash250 2007
[38] G Bundesausschuss Anlage 2 Erweitertes Neugeborenen-screening 2010 httpwwwg-badedownloads83-691-233RL Kinder Anlage-2 2010-12-16pdf
[39] A Andermann I Blancquaert S Beauchamp and I CostealdquoGuiding policy decisions for genetic screening developing asystematic and transparent approachrdquo Public Health Genomicsvol 14 no 1 pp 9ndash16 2010
[40] A Andermann I Blancquaert S Beauchamp and V DeryldquoRevisiting Wilson and Jungner in the genomic age a review ofscreening criteria over the past 40 yearsrdquo Bulletin of the WorldHealth Organization vol 86 no 4 pp 317ndash319 2008
[41] S Lobitz C Frommel A Brose J Klein and O BlankensteinldquoIncidence of sickle cell disease in an unselected cohort ofneonates born in Berlin Germanyrdquo European Journal of HumanGenetics 2014
[42] P D Roa E A Turner and M D P Aguinaga ldquoHemoglobinvariant detection from dried blood specimens by high perfor-mance liquid chromatographyrdquo Annals of Clinical and Labora-tory Science vol 23 no 6 pp 433ndash438 1993
[43] CMurray S KHall andPGriffiths ldquoAn evaluation of the Sebiacapillarys Neonat Haemoglobin FASTŮ system for routinenewborn screening for sickle cell diseaserdquo International Journalof Laboratory Hematology vol 33 no 5 pp 533ndash539 2011
[44] A F S B Brandenburg ldquoStatistisches Jahrbuch 2011rdquo 2011httpswwwstatistik-berlin-brandenburgdeprodukteJahrbuchjb2011JB 2011 BEpdf
[45] E Harms and B Olgemoller ldquoNeonatal screening for metabolicand endocrine disordersrdquo Deutsches Arzteblatt Internationalvol 108 no 1-2 pp 11ndash22 2011
[46] A Joutovsky J Hadzi-Nesic andM A Nardi ldquoHPLC retentiontime as a diagnostic tool for hemoglobin variants and hemo-globinopathies a study of 60 000 samples in a clinical diagnosticlaboratoryrdquo Clinical Chemistry vol 50 no 10 pp 1736ndash17472004
[47] E Kohne and E Kleihauer ldquoHemoglobinopathies in Ger-manymdasha longitudinal study over four decadesrdquo DeutschesArzteblatt vol 107 no 5 pp 65ndash71 2010
[48] R Dickerhoff O Genzel-Boroviczeny and E Kohne ldquoHaemo-globinopathies and newborn haemoglobinopathy screening inGermanyrdquo Journal of Clinical Pathology vol 62 no 1 article 342009
[49] Enactment of the German Federal Parliament (Bundestag)ldquoHuman Genetic Examination Act (Genetic Diagnosis Act-GenDG)rdquo 2009 httpswwweshgorgfileadminwwweshgorgdocumentsEuropeLegalWSGermany GenDG Law GermanEnglishpdf
[50] J M Wilson and Y G Jungner Principles and Practice of MassScreening for Disease WHO Public Health Papers 1968
[51] Gendiagnostik-Kommission ldquoRichtlinien der Gendiagnostik-Komission (GEKO) fur die Anforderung an die Durchfuhrunggenetischer Reihenuntersuchungen gemaszlig sect23 Abs 2 Nr 6GenDGrdquo Bundesgesundheitsblatt vol 56 pp 321ndash324 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 BioMed Research International
plotted against the time (119909-axis) The software analyzes thechromatograms fully automatically using the principle ofvalley-to-valley integration
In addition all chromatograms were visually inspectedWater blanks served as negative controls and were
included in every run As controls of the preanalytical processand the automated integration and quantitation of the peakswe used eluates from dried blood spot cards from HbS andHbC carriers and retention time markers provided by themanufacturer Interrun coefficients of variation (CV) weredetermined
27 Capillary Electrophoresis (CE) For the CE a disk 38mmin diameter was punched out of the dried blood spot card andplaced in a well of an 8-well strip tube After adding 50 120583Ldistilled water the sample was incubated in the CAPILLARYShumidity chamber at 4ndash6∘C for not less than two hoursand not more than 72 hours Then 06mL of hemolysingsolution was added Measurement of the hemolysate wasthen performed on a CAPILLARYS 2 CE system In eachrun controls with hemoglobins A F S and C provided bythe manufacturer were measured Data acquisition manage-ment and analysis were conducted with the PHORESIS 651software All material for the CE was purchased from SebiaFulda Germany
28 Handling of Results If both HPLC and CE analysesof a babyrsquos blood were indicative of SCD the family wascontacted and referred to our department of pediatric hema-tology where the presumed diagnosis was confirmed from afresh blood sample by molecular genetic analysis Telephonenumbers and addresses were extracted from the routine NBSdatabase Carrier states were not reported as required by ourlocal ethics committee
3 Results
A maximum of four 96-well plates was measured per dayand 455 plates were measured in 180 runs Six column lotswere used during the entire study Altogether 38220 sampleswere screened by HPLC 34084 of which were subject toevaluation 4236 samples had to be excluded because thecorresponding chromatograms showed a low total AUCAs expected the percentage of samples with a low AUCwas positively correlated with sample age (Figure 2) Oldersamples showed more degradation of hemoglobin resultingin more background noise and less analyzable materialOlder samples also contained more filter paper lint whichinterfered with the analysis by causing technical problemssuch as pressure increases or detector errors In one casewe observed a retention time shift With 74 of our oldest84 samples (881) we obtained chromatograms with anAUC gt 900000120583Vs although they had been taken fromdried blood spot cards 171 days previously The samples thusfulfilled theminimum criteria for testing which we defined asldquoadequate qualityrdquo Nevertheless the proportion of unusableresults increased significantly when the dried blood cardswere more than three months old (Figure 2)
50
60
70
80
90
100
40 60 80 100 120 140 160 180
Eval
uabl
e sam
ples
()
Age of samples (days)
Figure 2 Each dot represents themean of an average of 353 samples(range 24ndash1090) of the same age Of the samples that were analyzedwithin threemonths after being taken normallymore than 90wereevaluable
31 Screening-Positive Newborns Of 34084 samplesincluded 14 samples showed an HPLC pattern consistentwith the diagnosis of SCD 10 of which were interpreted asFS that is only hemoglobins F and S were assumed to bepresent An FS pattern indicates homozygosity for HbS aswell as compound heterozygosity for HbS and 120573-thalassemiaor 120575120573-thalassemia or HPFH respectively In four newbornswe detected an FSC pattern that is only hemoglobins F Sand C were present in these babies This is only explainableby compound heterozygosity for HbS and HbC clinicallyresulting in SCD-SC (Figure 3)
CE was used to corroborate HPLC results In all 14cases CE patterns were consistent with the correspondingHPLC results Consequently these newborns were consid-ered ldquoscreening positiverdquo and appointed to our pediatrichematology outpatient clinic to finally confirm diagnoses(Table 1) We did not observe false-positive findings
32 Screening-Negative Newborns The remaining 34070newborns showed hemoglobin patterns without any evi-dence of any phenotype of SCD and were thus classified asldquoscreening negativerdquo Among these we identified a total of 236newborns who were heterozygous for a hemoglobin variantThis was HbS in 165 cases HbE in 27 HbC in 23 and HbDin 11 In ten further cases there was a variant other than HbSE C or D In the cases interpreted as heterozygosity for HbSthe HbS HbA ratio was lt20
Until to date it has not come to our attention that inany of these screening-negative babies the diagnosis of SCDhas been made afterwards However these children are nowbetween 14 and 28 months of age and follow-up is notsystematically organized So it is possible that screening false-negative subjects for example children suffering frommildersubtypes of SCD like SCD-S120573+ thalassemia are missed
33 Precision of HPLC Retention time markers (RTM) wereprovided by the manufacturer RTM are lyophilized controlscontaining hemoglobins F A E and S and hemoglobins F A
BioMed Research International 5
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
011
020
029
070
079
144
(a)
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
012
021 031
050
070
080
116
(b)
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
011
020
028
049
070
076
115
141
(c)
04
03
02
01
00
01
00 05 10 15 20
Time (min)
011
020
029
050
071
077
117
167
(d)
Figure 3 Representative HPL chromatograms with the presumed hemoglobin patterns FA (a) FAS (b) FS (c) and FSC (d)
D and C respectively to monitor the precise separation ofthe aforementioned hemoglobins by the HPLC instrument[46] RTM help to detect instabilities in pump pressure orgradient composition which is an indispensable requirementfor correct analytical performance because raw data areprocessed electronically and the correct interpretation andintegration of peaks appearing in particular time windowsrequire the full functionality of the hardware
If the RTM indicated a functional disorder of the HPLCmachine we repeated the runs that were probably affectedTable 2 shows our results of several measurements (119899 =130) of the retention time markers in comparison to themanufacturerrsquos specifications Our data show a high precision
of retention times (CVle 15)Themaximumdeviation frommean retention time was plusmn0042min for HbS
Table 3 shows the mean and the range of retention timesof the various hemoglobins detected in the dried blood spotsamples of our study population The retrospective analysisof these retention times provides information about thestability of the HPLC system over the whole study periodwith this challenging material The CV was le 1 for all mainhemoglobins (A S E D and C)
As many factors during the whole analytical proceduremay affect test results dried blood samples from five new-borns found to be heterozygous for either HbS or HbCrespectively were established as additional quality controls
6 BioMed Research International
Table 1 Detailed information on screening-positive babies
Patient number (ethnical origin) Screening patterns HPLCCE Molecular genetic result 1 (West African) FSaFS SCD-SS 2 (West African) F5SaBFS SCD-SS 3 (Middle East) FSa5BFS SCD-S1205730 thalassemia 4 (West African) FaCSFSC SCD-SC 5 (Middle East) F4SAFS SCD-SS 6 (West African) FSCaFSC SCD-SC 7 (Middle East) FSa5FS SCD-SS 8 (West African) FSaBFS SCD-SS 9 (West African) FS4aFS SCD-SS 10 (West African) FS5aBFS SCD-SS 11 (West African) FCSaFSC SCD-SC 12 (West African) FSa2BFS SCD-SS 13 (West African) FSa2BFS SCD-SS 14 (West African) FCS1FSC SCD-SC
Table 2 High interrun precision of HPLC retention times of retention time markers
Hemoglobin Retention times of RTMmean (range) [min] CV []
Manufacturerrsquosspecifications mean
(range) [min]F 0494 (0471ndash0510) 15 0530 (0470ndash0590)A 0792 (0770ndash0804) 09 0800 (0730ndash0870)EA2 0954 (0919ndash0970) 10 0970 (0930ndash1010)D 1042 (1005ndash1072) 11 1060 (1010ndash1110)S 1158 (1116ndash1183) 12 1190 (1130ndash1250)C 1663 (1634ndash1684) 06 1680 (1610ndash1750)
Table 3 High precision of HPLC retention times of hemoglobins derived from dried blood spot samples
Presumptive hemoglobin Retention times mean (range) [min] CV [] 119899
A 0800 (0785ndash0816) 08 100E 0952 (0936ndash0968) 08 26D 1044 (1028ndash1060) 10 11S 1154 (1190ndash1130) 09 100C 1660 (1647ndash1670) 04 23
These samples were randomly integrated into several runsincluding all steps from pre- to postanalytics to include allinfluencing factors Table 4 shows the results of repeated ana-lyzes of these quality control samples known to be heterozy-gous for HbS (A) or HbC (B) on different working days
34 Precision of CE As quality controls of CE liquid controlsamples containing hemoglobins F A S and C were used ineach run on different working days (Table 5)
35 Costs All in all we examined samples from 38220 new-borns 37970 only by HPLC 250 additionally by CE becausethe samples showed an abnormal hemoglobin pattern in theHPLC For the examination of the entire cohort we incurredcosts of EUR 55000 A large part of this sum (just under50) was labor costs However the sum also contains the
costs for instrument hire for consumables and so forthThistranslates into a per-sample cost of EUR 144 (US$197)
4 Discussion
There are practically no epidemiological data to date on theprevalence and incidence of SCD in Germany [41 47 48]Cautious estimates made so far suggest a figure of about 3000to 4000 patients in the whole country These patients arewithout exception of immigrant origin [47]
Over a period of more than one year we tested withoutpreselection on the basis of ethnic origin 87 of all childrenborn in Berlin (34084 of 39249) for the presence of SCDand identified 14 with the disease [41] The incidence of SCD(41110000) amongst the children examined was thus higherthan the incidence of any other endocrine or metabolic
BioMed Research International 7
Table 4 (a) Interrun precision of HPLC determined on two dried blood spot samples from newborns heterozygous for HbS (b) Interrunprecision of HPLC determined on a dried blood spot sample from a newborn heterozygous for HbC
(a)
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] 119899
Control 1 373 29 89 53 36 63 11Control 2 401 48 19 27 10 50 8
(b)
HbF mean [] CV [] HbA mean [] CV [] HbC mean [] CV [] 119899
Control 3 396 57 17 22 13 28 11Precision was reduced if certain hemoglobin fractions were present in an order close to the detection limit of 1 of the total AUC
Table 5 Interrun precision of CE determined on liquid control samples provided by the manufacturer
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] HbC mean [] CV [] 119899Control FASC 188 48 355 20 145 43 54 77 5
disorder tested for in the context of the German extendedNBS program SCD should therefore be included in the NBSat least in Berlin In order to decidewhether there is a need fora national NBS program for SCD we now require data fromother regions particularly from presumed low-prevalenceareas
The results presented in this paper show that such epi-demiological data can be generated with investment ofrelatively little time and money as the samples do not needto be examined fresh on a day-to-day basis Instead largenumbers of samples can be analyzed retrospectively It is clearthat the costs per sample (144 EUR) in the context of ourpilot study will not be comparable with the expenses in thecontext of a national screening program While the costs forconsumables and so forth would probably be a little loweron account of the substantially higher patient numbers therewould be considerable additional expenses for administrativepurposes such as quality assurance Further additional costswould arise for staff training and for the entire infrastructurewhich has to be made available around the actual testing
In this study dried blood spot cards up to six monthsold provided satisfactory results However very old samplespresent a particular challenge because cellulose particleswhich come off the dried blood cards together with the bloodcan interfere considerably with the measurement They aredeposited in the fine capillaries of themeasuring instrumentsclogging them or creating additional unspecific measuringsignals The continuously increasing degradation of thehemoglobin also leads to additional measuring signals par-ticularly to increased background noise as well as reducingthe amount of analyzable material In the worst case onemight evenmiss a significant disease due tomisinterpretationof a peak resembling HbA for example a 120573-thalassemiamajor pattern could be confused with a physiological FApattern or homozygosity forHbS could be confusedwith SCTSample preparation is therefore of decisive importance
Factors which can influence the sample quality are asfollows
(1) The concentration of the hemoglobin in thehemolysate This depends on the volume of theblood sample thus on the saturation of the filter cardand on the degree of degradation of the hemoglobinThe latter is essentially dependent on the age and thestorage conditions of the sample Further importantparameters are the elution volume and elution time
(2) Instrument performance is influenced significantly bythe condition of the dried blood spot card This isin turn also dependent on the sample age and thestorage conditions In the case of older cards celluloseparticles are removed from the card together with theblood and can then interfere with the measurement
Prolonging the elution time increases the hemoglobinconcentration in the hemolysate and also the likelihood ofcellulose particles becoming detached from the filter cardThe elution conditions described in the methods section takeinto account both phenomena and represent the necessarycompromise
The implementation of pilot studies of this kind requiresthe availability of a high throughput method In our expe-rience HPLC and CE are equally suitable The CE electro-pherograms appeared to us to be easier to interpret than theHPLC chromatograms because there were fewer unspecificsignals in the former Whichever method is chosen it iscrucial that the analytical laboratory has special expertisewith regard to the IT-supported interpretation of the rawmeasurements
Disease screening programs are characterized by the factthat certain people are examined for the presence of a certaindisease simply because they belong to a certain populationThe subjects are examined or tested regardless of whetherthere is any concrete reason to suspect the presence of
8 BioMed Research International
the target disease The large majority of the subjects screenedare completely healthy This raises particular ethical legaltechnical and economic issues
The German Genetic Testing Act (GenDG) came intoforce on January 2 2010 and is a constant topic of debate onaccount of its very strict regulations [49] It controls genetictesting in humans and the use of genetic samples and dataThe GenDG specifies interalia that analyses of the productsof nucleic acids (gene product analyses) are also consideredgenetic analyses and therefore deemed legally equal to exam-ination of the number and structure of the chromosomes andof themolecular structure of DNA and RNAThismeans thathemoglobinopathy testing using protein separation methodssuch as HPLC or CE comes under the GenDG
Theultimate goal of theGenDG is to prevent the potentialdangers and discrimination associated with the examina-tion of human genetic traits One of the most importantprinciples is the right of the individual to informationalself-determination This right which enjoys internationallyunique protection in Germany includes the right to knowand more important in this context the right not to knowIts most important implication is that we are not allowed inGermany to report sickle cell trait
The GenDG distinguishes between genetic tests per-formed in amedical context and tests performed in a researchcontext and only applies to tests ordered in amedical contextA distinction is also made between diagnostic tests andpredictive tests In addition the GenDG regulates geneticscreening which would include NBS for SCD German lawrequires the establishment of an independent interdisci-plinary Genetic Testing Commission (GEKO) which hasbeen set up at the Robert Koch Institute and amongst otherthings lays down the requirements for the performance ofgenetic screening tests [49]These requirements are based onthe specific criteria for genetic screening developed byAnder-mann et al on the basis of theWHO screening criteria ofWil-son and Jungner [39 50]The GEKO has expressly stated thatresults of studies performed in other countries with differenthealthcare systems and different population structures can-not necessarily be extrapolated toGermany [51] For examplesome screening criteria are based on local conditions whichdo not obtain in Germany or at least not in all parts of thecountry Sickle cell patients cannot in particular be offeredstate-of-the-art care everywhere in Germany Nonmalignanthematology has been almost entirely neglected in the trainingof all groups of healthcare professionals in the past and thehemoglobinopathies as a whole are still not seen as a problemin Germany However a national strategy for preventionand treatment of SCD is currently under development TheSociety for Pediatric Oncology and Hematology (GPOH)has commissioned the establishment of a patient registerreference centers and a treatment guidelineThis is importantbecause if it is to make any sense a newborn screeningprogram requires not only the identification of sick babies butalso a functioning infrastructure which ensures that affectedchildren also receive appropriate care after the diagnosisThis includes both medical and psychosocial care as wellas sufficient counseling resources for the patients and theirparents
5 Conclusions
Our pilot project shows that itmakes sense at least regionallyto think about the introduction of some kind ofNBS programfor SCD in Germany whatever specific form this takesThe pilot projects necessary for this must be embarked onnow In addition to the presumed high-prevalence regionssuch as Berlin Hamburg the Ruhr region or Frankfurtepidemiological data should also be collected from pre-sumed low-prevalence regions (eg rural Bavaria and Baden-Wurttemberg)
Our data show that the organization and realization ofsuch pilot projects is relatively unproblematic and inexpen-sive as samples can be collected over several months and thenanalyzed together However we recommend that the samplesshould not be older than three months at the time of analysisIt is of fundamental importance that the Genetic Testing Actdoes not apply to such pilot projects as they involve genetictesting in the context of research
Conflict of Interests
Stephan Lobitz Claudia Frommel and Oliver Blankensteinreceived a research grant from Novartis Oncology GmbH(Nuremberg Germany) to perform this study In additionBio-Rad Laboratories GmbH (Munich Germany) indirectlyfunded this project through a preferential price for HPLCconsumables Beyond that the authors declare no competinginterest
Acknowledgments
This work is part of Stephan Lobitzrsquos dissertation in theUniversity College London ldquoMaster of Science in Haemoglo-binopathyrdquo program Stephan Lobitz is deeply indebted toDr Ratna Chatterjee Dr Rekha Bajoria the ThalassaemiaInternational Federation (TIF) and ldquoKINDerLEBEN-Vereinzur Forderung der Klinik fur krebskranke Kinder eV BerlinrdquoThe authors thank Novartis Oncology GmbH and Bio-RadLaboratories GmbH who generously funded this projectMany thanks are due to all parents and patients who took partin this study
References
[1] D C Rees T N Williams and M T Gladwin ldquoSickle-celldiseaserdquoThe Lancet vol 376 no 9757 pp 2018ndash2031 2010
[2] D Powars G Overturf J Weiss S Lee and L Chan ldquoPneumo-coccal septicemia in children with sickle cell anemia Changingtrend of survivalrdquo Journal of the American Medical Associationvol 245 no 18 pp 1839ndash1842 1981
[3] A M Emond R Collis D Darvill D R Higgs G H Maudeand G R Serjeant ldquoAcute splenic sequestration in homozygoussickle cell disease natural history and managementrdquo The Jour-nal of Pediatrics vol 107 no 2 pp 201ndash206 1985
[4] M H Gaston J I Verter G Woods et al ldquoProphylaxis withoral penicillin in children with sickle cell anemia a randomizedtrialrdquoThe New England Journal of Medicine vol 314 no 25 pp1593ndash1599 1986
BioMed Research International 9
[5] G R Serjeant and B E Serjeant ldquoManagement of sickle celldisease lessons from the Jamaican cohort studyrdquo Blood Reviewsvol 7 no 3 pp 137ndash145 1993
[6] A Lee P Thomas L Cupidore B Serjeant and G SerjeantldquoImproved survival in homozygous sickle cell disease lessonsfrom a cohort studyrdquo British Medical Journal vol 311 no 7020pp 1600ndash1602 1995
[7] T V Adamkiewicz S Sarnaik G R Buchanan et al ldquoInvasivepneumococcal infections in children with sickle cell diseasein the era of penicillin prophylaxis antibiotic resistance and23-valent pneumococcal polysaccharide vaccinationrdquo Journal ofPediatrics vol 143 no 4 pp 438ndash444 2003
[8] N B Halasa S M Shankar T R Talbot et al ldquoIncidence ofinvasive pneumococcal disease among individuals with sicklecell disease before and after the introduction of the pneumo-coccal conjugate vaccinerdquo Clinical Infectious Diseases vol 44no 11 pp 1428ndash1433 2007
[9] T V Adamkiewicz B J Silk J Howgate et al ldquoEffectiveness ofthe 7-valent pneumococcal conjugate vaccine in children withsickle cell disease in the first decade of liferdquo Pediatrics vol 121no 3 pp 562ndash569 2008
[10] S D Grosse H K Atrash I Odame D Amendah F B Pieland T N Williams ldquoThe Jamaican historical experience of theimpact of educational interventions on sickle cell disease childmortalityrdquoTheAmerican Journal of PreventiveMedicine vol 42no 6 pp e101ndashe103 2012
[11] H Heijboer X W van den Tweel M Peters M Knuist JPrins and H S Heymans ldquoOne year of neonatal screening forsickle cell disease in the emma kinderziekenhuisacademischmedisch centrum Amsterdamrdquo Nederlands Tijdschrift voorGeneeskunde vol 145 no 37 pp 1795ndash1799 2001
[12] B Gulbis F Cotton A Ferster et al ldquoNeonatal haemoglobin-opathy screening in Belgiumrdquo Journal of Clinical Pathology vol62 no 1 pp 49ndash52 2009
[13] A Streetly R Latinovic and J Henthorn ldquoPositive screeningand carrier results for the England-wide universal newbornsickle cell screening programme by ethnicity and area for 2005-07rdquo Journal of Clinical Pathology vol 63 no 7 pp 626ndash6292010
[14] E Ballardini A TaroccoMMarsella et al ldquoUniversal neonatalscreening for sickle cell disease and other haemoglobinopathiesin Ferrara Italyrdquo Blood Transfusion vol 11 no 2 pp 245ndash2492013
[15] J Bardakdjian-Michau M Bahuau D Hurtrel et al ldquoNeonatalscreening for sickle cell disease in Francerdquo Journal of ClinicalPathology vol 62 no 1 pp 31ndash33 2009
[16] E Cela De Julian E Dulın Iniguez M Guerrero Soler etal ldquoEvaluation of systematic neonatal screening for sickle celldiseases in Madrid three years after its introductionrdquo Anales dePediatria vol 66 no 4 pp 382ndash386 2007
[17] M J Bouva K Mohrmann H B J M Brinkman et alldquoImplementing neonatal screening for haemoglobinopathies inthe Netherlandsrdquo Journal of Medical Screening vol 17 no 2 pp58ndash65 2010
[18] P C GiordanoM J Bouva and C L Harteveld ldquoA confidentialinquiry estimating the number of patients affected with sicklecell disease and thalassemia major confirms the need for aprevention strategy in theNetherlandsrdquoHemoglobin vol 28 no4 pp 287ndash296 2004
[19] S Berthet F Monpoux A-M Soummer E Berard J Sarlesand C Badens ldquoNeonatal screening for sickle cell disease in
Nice University Hospital review of 8 last yearsrdquo Archives dePediatrie vol 17 no 12 pp 1652ndash1656 2010
[20] R Ducrocq M Benkerrou L Brahimi et al ldquoNeonatal screen-ing for sickle cell anemia evaluation of a five-year experience inan area of northern ParisrdquoArchives de Pediatrie vol 8 no 5 pp474ndash480 2001
[21] M Manu Pereira and J Vives Corrons ldquoNeonatal haemo-globinopathy screening in Spainrdquo Journal of Clinical Pathologyvol 62 no 1 pp 22ndash25 2009
[22] C Saint-Martin M Romana A Bibrac et al ldquoUniversalnewborn screening for haemoglobinopathies in Guadeloupe(French West Indies) a 27-year experiencerdquo Journal of MedicalScreening vol 20 no 4 pp 177ndash182 2013
[23] C L Lobo S K Ballas A C Domingos P G Moura E M doNascimento and G P Cardoso ldquoNewborn screening programfor hemoglobinopathies in Rio de Janeiro Brazilrdquo PediatricBlood and Cancer vol 61 no 1 pp 34ndash39 2014
[24] P T McGann M G Ferris U Ramamurthy et al ldquoA prospec-tive newborn screening and treatment program for sickle cellanemia in Luanda Angolardquo The American Journal of Hematol-ogy vol 88 no 12 pp 984ndash989 2013
[25] J Patel and G R Serjeant ldquoNewborn screening for sickle celldisease in India the need for defining optimal clinical carerdquoIndian Journal of Pediatrics vol 81 no 3 pp 229ndash230 2014
[26] S Hajer T Neila H F Sondess et al ldquoA lower-cost protocolfor sickle cell disease neonatal screening in Tunisiardquo Annals ofSaudi Medicine vol 32 no 1 pp 49ndash52 2012
[27] V S Hertzberg C F Hinton B L Therrell and S K ShapiraldquoBirth prevalence rates of newborn screening disorders inrelation to screening practices in the United Statesrdquo Journal ofPediatrics vol 159 no 4 pp 555ndash560 2011
[28] M C Rahimy A Gangbo G Ahouignan and E AlihonouldquoNewborn screening for sickle cell disease in the Republic ofBeninrdquo Journal of Clinical Pathology vol 62 no 1 pp 46ndash482009
[29] E Kafando E Nacoulma Y Ouattara et al ldquoNeonatal haemo-globinopathy screening in Burkina Fasordquo Journal of ClinicalPathology vol 62 no 1 pp 39ndash41 2009
[30] L Tshilolo L M Aissi D Lukusa et al ldquoNeonatal screening forsickle cell anaemia in the Democratic Republic of the Congoexperience from a pioneer project on 31 204 newbornsrdquo Journalof Clinical Pathology vol 62 no 1 pp 35ndash38 2009
[31] B J Bain ldquoHaemoglobinopathy diagnosis algorithms lessonsand pitfallsrdquo Blood Reviews vol 25 no 5 pp 205ndash213 2011
[32] K Ryan B J Bain D Worthington et al ldquoSignificant haemo-globinopathies guidelines for screening and diagnosisrdquo BritishJournal of Haematology vol 149 no 1 pp 35ndash49 2010
[33] J Riou C Godart D Hurtrel et al ldquoCation-exchange HPLCevaluated for presumptive identification of hemoglobin vari-antsrdquo Clinical Chemistry vol 43 no 1 pp 34ndash39 1997
[34] G RenomCMereau PMaboudou and J-M Perini ldquoPotentialof the Sebia Capillarys neonat fast automated system forneonatal screening of sickle cell diseaserdquoClinical Chemistry andLaboratory Medicine vol 47 no 11 pp 1423ndash1432 2009
[35] M Campbell J S Henthorn and S C Davies ldquoEvaluation ofcation-exchange HPLC compared with isoelectric focusing forneonatal hemoglobinopathy screeningrdquoClinical Chemistry vol45 no 7 pp 969ndash975 1999
[36] E Mantikou C L Harteveld and P C Giordano ldquoNewbornscreening for hemoglobinopathies using capillary electrophore-sis technology testing the Capillarys Neonat Fast Hb devicerdquoClinical Biochemistry vol 43 no 16-17 pp 1345ndash1350 2010
10 BioMed Research International
[37] F Kutlar ldquoDiagnostic approach to hemoglobinopathiesrdquoHemoglobin vol 31 no 2 pp 243ndash250 2007
[38] G Bundesausschuss Anlage 2 Erweitertes Neugeborenen-screening 2010 httpwwwg-badedownloads83-691-233RL Kinder Anlage-2 2010-12-16pdf
[39] A Andermann I Blancquaert S Beauchamp and I CostealdquoGuiding policy decisions for genetic screening developing asystematic and transparent approachrdquo Public Health Genomicsvol 14 no 1 pp 9ndash16 2010
[40] A Andermann I Blancquaert S Beauchamp and V DeryldquoRevisiting Wilson and Jungner in the genomic age a review ofscreening criteria over the past 40 yearsrdquo Bulletin of the WorldHealth Organization vol 86 no 4 pp 317ndash319 2008
[41] S Lobitz C Frommel A Brose J Klein and O BlankensteinldquoIncidence of sickle cell disease in an unselected cohort ofneonates born in Berlin Germanyrdquo European Journal of HumanGenetics 2014
[42] P D Roa E A Turner and M D P Aguinaga ldquoHemoglobinvariant detection from dried blood specimens by high perfor-mance liquid chromatographyrdquo Annals of Clinical and Labora-tory Science vol 23 no 6 pp 433ndash438 1993
[43] CMurray S KHall andPGriffiths ldquoAn evaluation of the Sebiacapillarys Neonat Haemoglobin FASTŮ system for routinenewborn screening for sickle cell diseaserdquo International Journalof Laboratory Hematology vol 33 no 5 pp 533ndash539 2011
[44] A F S B Brandenburg ldquoStatistisches Jahrbuch 2011rdquo 2011httpswwwstatistik-berlin-brandenburgdeprodukteJahrbuchjb2011JB 2011 BEpdf
[45] E Harms and B Olgemoller ldquoNeonatal screening for metabolicand endocrine disordersrdquo Deutsches Arzteblatt Internationalvol 108 no 1-2 pp 11ndash22 2011
[46] A Joutovsky J Hadzi-Nesic andM A Nardi ldquoHPLC retentiontime as a diagnostic tool for hemoglobin variants and hemo-globinopathies a study of 60 000 samples in a clinical diagnosticlaboratoryrdquo Clinical Chemistry vol 50 no 10 pp 1736ndash17472004
[47] E Kohne and E Kleihauer ldquoHemoglobinopathies in Ger-manymdasha longitudinal study over four decadesrdquo DeutschesArzteblatt vol 107 no 5 pp 65ndash71 2010
[48] R Dickerhoff O Genzel-Boroviczeny and E Kohne ldquoHaemo-globinopathies and newborn haemoglobinopathy screening inGermanyrdquo Journal of Clinical Pathology vol 62 no 1 article 342009
[49] Enactment of the German Federal Parliament (Bundestag)ldquoHuman Genetic Examination Act (Genetic Diagnosis Act-GenDG)rdquo 2009 httpswwweshgorgfileadminwwweshgorgdocumentsEuropeLegalWSGermany GenDG Law GermanEnglishpdf
[50] J M Wilson and Y G Jungner Principles and Practice of MassScreening for Disease WHO Public Health Papers 1968
[51] Gendiagnostik-Kommission ldquoRichtlinien der Gendiagnostik-Komission (GEKO) fur die Anforderung an die Durchfuhrunggenetischer Reihenuntersuchungen gemaszlig sect23 Abs 2 Nr 6GenDGrdquo Bundesgesundheitsblatt vol 56 pp 321ndash324 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
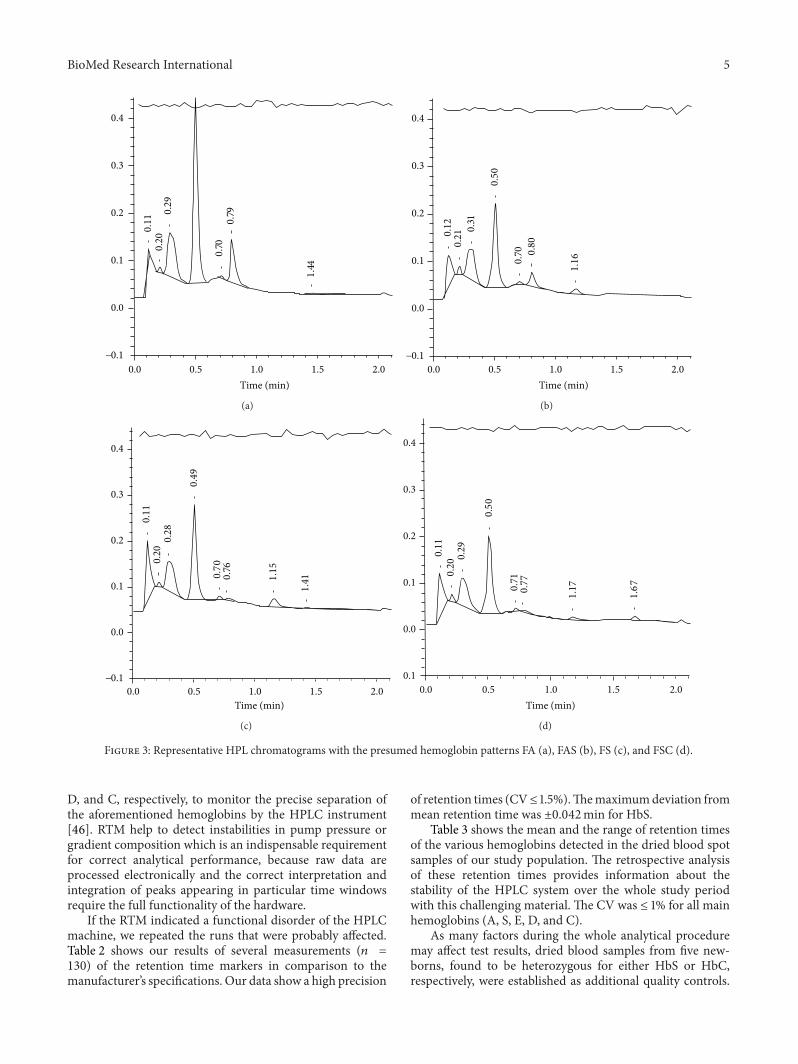
BioMed Research International 5
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
011
020
029
070
079
144
(a)
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
012
021 031
050
070
080
116
(b)
04
03
02
01
00
minus01
00 05 10 15 20
Time (min)
011
020
028
049
070
076
115
141
(c)
04
03
02
01
00
01
00 05 10 15 20
Time (min)
011
020
029
050
071
077
117
167
(d)
Figure 3 Representative HPL chromatograms with the presumed hemoglobin patterns FA (a) FAS (b) FS (c) and FSC (d)
D and C respectively to monitor the precise separation ofthe aforementioned hemoglobins by the HPLC instrument[46] RTM help to detect instabilities in pump pressure orgradient composition which is an indispensable requirementfor correct analytical performance because raw data areprocessed electronically and the correct interpretation andintegration of peaks appearing in particular time windowsrequire the full functionality of the hardware
If the RTM indicated a functional disorder of the HPLCmachine we repeated the runs that were probably affectedTable 2 shows our results of several measurements (119899 =130) of the retention time markers in comparison to themanufacturerrsquos specifications Our data show a high precision
of retention times (CVle 15)Themaximumdeviation frommean retention time was plusmn0042min for HbS
Table 3 shows the mean and the range of retention timesof the various hemoglobins detected in the dried blood spotsamples of our study population The retrospective analysisof these retention times provides information about thestability of the HPLC system over the whole study periodwith this challenging material The CV was le 1 for all mainhemoglobins (A S E D and C)
As many factors during the whole analytical proceduremay affect test results dried blood samples from five new-borns found to be heterozygous for either HbS or HbCrespectively were established as additional quality controls
6 BioMed Research International
Table 1 Detailed information on screening-positive babies
Patient number (ethnical origin) Screening patterns HPLCCE Molecular genetic result 1 (West African) FSaFS SCD-SS 2 (West African) F5SaBFS SCD-SS 3 (Middle East) FSa5BFS SCD-S1205730 thalassemia 4 (West African) FaCSFSC SCD-SC 5 (Middle East) F4SAFS SCD-SS 6 (West African) FSCaFSC SCD-SC 7 (Middle East) FSa5FS SCD-SS 8 (West African) FSaBFS SCD-SS 9 (West African) FS4aFS SCD-SS 10 (West African) FS5aBFS SCD-SS 11 (West African) FCSaFSC SCD-SC 12 (West African) FSa2BFS SCD-SS 13 (West African) FSa2BFS SCD-SS 14 (West African) FCS1FSC SCD-SC
Table 2 High interrun precision of HPLC retention times of retention time markers
Hemoglobin Retention times of RTMmean (range) [min] CV []
Manufacturerrsquosspecifications mean
(range) [min]F 0494 (0471ndash0510) 15 0530 (0470ndash0590)A 0792 (0770ndash0804) 09 0800 (0730ndash0870)EA2 0954 (0919ndash0970) 10 0970 (0930ndash1010)D 1042 (1005ndash1072) 11 1060 (1010ndash1110)S 1158 (1116ndash1183) 12 1190 (1130ndash1250)C 1663 (1634ndash1684) 06 1680 (1610ndash1750)
Table 3 High precision of HPLC retention times of hemoglobins derived from dried blood spot samples
Presumptive hemoglobin Retention times mean (range) [min] CV [] 119899
A 0800 (0785ndash0816) 08 100E 0952 (0936ndash0968) 08 26D 1044 (1028ndash1060) 10 11S 1154 (1190ndash1130) 09 100C 1660 (1647ndash1670) 04 23
These samples were randomly integrated into several runsincluding all steps from pre- to postanalytics to include allinfluencing factors Table 4 shows the results of repeated ana-lyzes of these quality control samples known to be heterozy-gous for HbS (A) or HbC (B) on different working days
34 Precision of CE As quality controls of CE liquid controlsamples containing hemoglobins F A S and C were used ineach run on different working days (Table 5)
35 Costs All in all we examined samples from 38220 new-borns 37970 only by HPLC 250 additionally by CE becausethe samples showed an abnormal hemoglobin pattern in theHPLC For the examination of the entire cohort we incurredcosts of EUR 55000 A large part of this sum (just under50) was labor costs However the sum also contains the
costs for instrument hire for consumables and so forthThistranslates into a per-sample cost of EUR 144 (US$197)
4 Discussion
There are practically no epidemiological data to date on theprevalence and incidence of SCD in Germany [41 47 48]Cautious estimates made so far suggest a figure of about 3000to 4000 patients in the whole country These patients arewithout exception of immigrant origin [47]
Over a period of more than one year we tested withoutpreselection on the basis of ethnic origin 87 of all childrenborn in Berlin (34084 of 39249) for the presence of SCDand identified 14 with the disease [41] The incidence of SCD(41110000) amongst the children examined was thus higherthan the incidence of any other endocrine or metabolic
BioMed Research International 7
Table 4 (a) Interrun precision of HPLC determined on two dried blood spot samples from newborns heterozygous for HbS (b) Interrunprecision of HPLC determined on a dried blood spot sample from a newborn heterozygous for HbC
(a)
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] 119899
Control 1 373 29 89 53 36 63 11Control 2 401 48 19 27 10 50 8
(b)
HbF mean [] CV [] HbA mean [] CV [] HbC mean [] CV [] 119899
Control 3 396 57 17 22 13 28 11Precision was reduced if certain hemoglobin fractions were present in an order close to the detection limit of 1 of the total AUC
Table 5 Interrun precision of CE determined on liquid control samples provided by the manufacturer
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] HbC mean [] CV [] 119899Control FASC 188 48 355 20 145 43 54 77 5
disorder tested for in the context of the German extendedNBS program SCD should therefore be included in the NBSat least in Berlin In order to decidewhether there is a need fora national NBS program for SCD we now require data fromother regions particularly from presumed low-prevalenceareas
The results presented in this paper show that such epi-demiological data can be generated with investment ofrelatively little time and money as the samples do not needto be examined fresh on a day-to-day basis Instead largenumbers of samples can be analyzed retrospectively It is clearthat the costs per sample (144 EUR) in the context of ourpilot study will not be comparable with the expenses in thecontext of a national screening program While the costs forconsumables and so forth would probably be a little loweron account of the substantially higher patient numbers therewould be considerable additional expenses for administrativepurposes such as quality assurance Further additional costswould arise for staff training and for the entire infrastructurewhich has to be made available around the actual testing
In this study dried blood spot cards up to six monthsold provided satisfactory results However very old samplespresent a particular challenge because cellulose particleswhich come off the dried blood cards together with the bloodcan interfere considerably with the measurement They aredeposited in the fine capillaries of themeasuring instrumentsclogging them or creating additional unspecific measuringsignals The continuously increasing degradation of thehemoglobin also leads to additional measuring signals par-ticularly to increased background noise as well as reducingthe amount of analyzable material In the worst case onemight evenmiss a significant disease due tomisinterpretationof a peak resembling HbA for example a 120573-thalassemiamajor pattern could be confused with a physiological FApattern or homozygosity forHbS could be confusedwith SCTSample preparation is therefore of decisive importance
Factors which can influence the sample quality are asfollows
(1) The concentration of the hemoglobin in thehemolysate This depends on the volume of theblood sample thus on the saturation of the filter cardand on the degree of degradation of the hemoglobinThe latter is essentially dependent on the age and thestorage conditions of the sample Further importantparameters are the elution volume and elution time
(2) Instrument performance is influenced significantly bythe condition of the dried blood spot card This isin turn also dependent on the sample age and thestorage conditions In the case of older cards celluloseparticles are removed from the card together with theblood and can then interfere with the measurement
Prolonging the elution time increases the hemoglobinconcentration in the hemolysate and also the likelihood ofcellulose particles becoming detached from the filter cardThe elution conditions described in the methods section takeinto account both phenomena and represent the necessarycompromise
The implementation of pilot studies of this kind requiresthe availability of a high throughput method In our expe-rience HPLC and CE are equally suitable The CE electro-pherograms appeared to us to be easier to interpret than theHPLC chromatograms because there were fewer unspecificsignals in the former Whichever method is chosen it iscrucial that the analytical laboratory has special expertisewith regard to the IT-supported interpretation of the rawmeasurements
Disease screening programs are characterized by the factthat certain people are examined for the presence of a certaindisease simply because they belong to a certain populationThe subjects are examined or tested regardless of whetherthere is any concrete reason to suspect the presence of
8 BioMed Research International
the target disease The large majority of the subjects screenedare completely healthy This raises particular ethical legaltechnical and economic issues
The German Genetic Testing Act (GenDG) came intoforce on January 2 2010 and is a constant topic of debate onaccount of its very strict regulations [49] It controls genetictesting in humans and the use of genetic samples and dataThe GenDG specifies interalia that analyses of the productsof nucleic acids (gene product analyses) are also consideredgenetic analyses and therefore deemed legally equal to exam-ination of the number and structure of the chromosomes andof themolecular structure of DNA and RNAThismeans thathemoglobinopathy testing using protein separation methodssuch as HPLC or CE comes under the GenDG
Theultimate goal of theGenDG is to prevent the potentialdangers and discrimination associated with the examina-tion of human genetic traits One of the most importantprinciples is the right of the individual to informationalself-determination This right which enjoys internationallyunique protection in Germany includes the right to knowand more important in this context the right not to knowIts most important implication is that we are not allowed inGermany to report sickle cell trait
The GenDG distinguishes between genetic tests per-formed in amedical context and tests performed in a researchcontext and only applies to tests ordered in amedical contextA distinction is also made between diagnostic tests andpredictive tests In addition the GenDG regulates geneticscreening which would include NBS for SCD German lawrequires the establishment of an independent interdisci-plinary Genetic Testing Commission (GEKO) which hasbeen set up at the Robert Koch Institute and amongst otherthings lays down the requirements for the performance ofgenetic screening tests [49]These requirements are based onthe specific criteria for genetic screening developed byAnder-mann et al on the basis of theWHO screening criteria ofWil-son and Jungner [39 50]The GEKO has expressly stated thatresults of studies performed in other countries with differenthealthcare systems and different population structures can-not necessarily be extrapolated toGermany [51] For examplesome screening criteria are based on local conditions whichdo not obtain in Germany or at least not in all parts of thecountry Sickle cell patients cannot in particular be offeredstate-of-the-art care everywhere in Germany Nonmalignanthematology has been almost entirely neglected in the trainingof all groups of healthcare professionals in the past and thehemoglobinopathies as a whole are still not seen as a problemin Germany However a national strategy for preventionand treatment of SCD is currently under development TheSociety for Pediatric Oncology and Hematology (GPOH)has commissioned the establishment of a patient registerreference centers and a treatment guidelineThis is importantbecause if it is to make any sense a newborn screeningprogram requires not only the identification of sick babies butalso a functioning infrastructure which ensures that affectedchildren also receive appropriate care after the diagnosisThis includes both medical and psychosocial care as wellas sufficient counseling resources for the patients and theirparents
5 Conclusions
Our pilot project shows that itmakes sense at least regionallyto think about the introduction of some kind ofNBS programfor SCD in Germany whatever specific form this takesThe pilot projects necessary for this must be embarked onnow In addition to the presumed high-prevalence regionssuch as Berlin Hamburg the Ruhr region or Frankfurtepidemiological data should also be collected from pre-sumed low-prevalence regions (eg rural Bavaria and Baden-Wurttemberg)
Our data show that the organization and realization ofsuch pilot projects is relatively unproblematic and inexpen-sive as samples can be collected over several months and thenanalyzed together However we recommend that the samplesshould not be older than three months at the time of analysisIt is of fundamental importance that the Genetic Testing Actdoes not apply to such pilot projects as they involve genetictesting in the context of research
Conflict of Interests
Stephan Lobitz Claudia Frommel and Oliver Blankensteinreceived a research grant from Novartis Oncology GmbH(Nuremberg Germany) to perform this study In additionBio-Rad Laboratories GmbH (Munich Germany) indirectlyfunded this project through a preferential price for HPLCconsumables Beyond that the authors declare no competinginterest
Acknowledgments
This work is part of Stephan Lobitzrsquos dissertation in theUniversity College London ldquoMaster of Science in Haemoglo-binopathyrdquo program Stephan Lobitz is deeply indebted toDr Ratna Chatterjee Dr Rekha Bajoria the ThalassaemiaInternational Federation (TIF) and ldquoKINDerLEBEN-Vereinzur Forderung der Klinik fur krebskranke Kinder eV BerlinrdquoThe authors thank Novartis Oncology GmbH and Bio-RadLaboratories GmbH who generously funded this projectMany thanks are due to all parents and patients who took partin this study
References
[1] D C Rees T N Williams and M T Gladwin ldquoSickle-celldiseaserdquoThe Lancet vol 376 no 9757 pp 2018ndash2031 2010
[2] D Powars G Overturf J Weiss S Lee and L Chan ldquoPneumo-coccal septicemia in children with sickle cell anemia Changingtrend of survivalrdquo Journal of the American Medical Associationvol 245 no 18 pp 1839ndash1842 1981
[3] A M Emond R Collis D Darvill D R Higgs G H Maudeand G R Serjeant ldquoAcute splenic sequestration in homozygoussickle cell disease natural history and managementrdquo The Jour-nal of Pediatrics vol 107 no 2 pp 201ndash206 1985
[4] M H Gaston J I Verter G Woods et al ldquoProphylaxis withoral penicillin in children with sickle cell anemia a randomizedtrialrdquoThe New England Journal of Medicine vol 314 no 25 pp1593ndash1599 1986
BioMed Research International 9
[5] G R Serjeant and B E Serjeant ldquoManagement of sickle celldisease lessons from the Jamaican cohort studyrdquo Blood Reviewsvol 7 no 3 pp 137ndash145 1993
[6] A Lee P Thomas L Cupidore B Serjeant and G SerjeantldquoImproved survival in homozygous sickle cell disease lessonsfrom a cohort studyrdquo British Medical Journal vol 311 no 7020pp 1600ndash1602 1995
[7] T V Adamkiewicz S Sarnaik G R Buchanan et al ldquoInvasivepneumococcal infections in children with sickle cell diseasein the era of penicillin prophylaxis antibiotic resistance and23-valent pneumococcal polysaccharide vaccinationrdquo Journal ofPediatrics vol 143 no 4 pp 438ndash444 2003
[8] N B Halasa S M Shankar T R Talbot et al ldquoIncidence ofinvasive pneumococcal disease among individuals with sicklecell disease before and after the introduction of the pneumo-coccal conjugate vaccinerdquo Clinical Infectious Diseases vol 44no 11 pp 1428ndash1433 2007
[9] T V Adamkiewicz B J Silk J Howgate et al ldquoEffectiveness ofthe 7-valent pneumococcal conjugate vaccine in children withsickle cell disease in the first decade of liferdquo Pediatrics vol 121no 3 pp 562ndash569 2008
[10] S D Grosse H K Atrash I Odame D Amendah F B Pieland T N Williams ldquoThe Jamaican historical experience of theimpact of educational interventions on sickle cell disease childmortalityrdquoTheAmerican Journal of PreventiveMedicine vol 42no 6 pp e101ndashe103 2012
[11] H Heijboer X W van den Tweel M Peters M Knuist JPrins and H S Heymans ldquoOne year of neonatal screening forsickle cell disease in the emma kinderziekenhuisacademischmedisch centrum Amsterdamrdquo Nederlands Tijdschrift voorGeneeskunde vol 145 no 37 pp 1795ndash1799 2001
[12] B Gulbis F Cotton A Ferster et al ldquoNeonatal haemoglobin-opathy screening in Belgiumrdquo Journal of Clinical Pathology vol62 no 1 pp 49ndash52 2009
[13] A Streetly R Latinovic and J Henthorn ldquoPositive screeningand carrier results for the England-wide universal newbornsickle cell screening programme by ethnicity and area for 2005-07rdquo Journal of Clinical Pathology vol 63 no 7 pp 626ndash6292010
[14] E Ballardini A TaroccoMMarsella et al ldquoUniversal neonatalscreening for sickle cell disease and other haemoglobinopathiesin Ferrara Italyrdquo Blood Transfusion vol 11 no 2 pp 245ndash2492013
[15] J Bardakdjian-Michau M Bahuau D Hurtrel et al ldquoNeonatalscreening for sickle cell disease in Francerdquo Journal of ClinicalPathology vol 62 no 1 pp 31ndash33 2009
[16] E Cela De Julian E Dulın Iniguez M Guerrero Soler etal ldquoEvaluation of systematic neonatal screening for sickle celldiseases in Madrid three years after its introductionrdquo Anales dePediatria vol 66 no 4 pp 382ndash386 2007
[17] M J Bouva K Mohrmann H B J M Brinkman et alldquoImplementing neonatal screening for haemoglobinopathies inthe Netherlandsrdquo Journal of Medical Screening vol 17 no 2 pp58ndash65 2010
[18] P C GiordanoM J Bouva and C L Harteveld ldquoA confidentialinquiry estimating the number of patients affected with sicklecell disease and thalassemia major confirms the need for aprevention strategy in theNetherlandsrdquoHemoglobin vol 28 no4 pp 287ndash296 2004
[19] S Berthet F Monpoux A-M Soummer E Berard J Sarlesand C Badens ldquoNeonatal screening for sickle cell disease in
Nice University Hospital review of 8 last yearsrdquo Archives dePediatrie vol 17 no 12 pp 1652ndash1656 2010
[20] R Ducrocq M Benkerrou L Brahimi et al ldquoNeonatal screen-ing for sickle cell anemia evaluation of a five-year experience inan area of northern ParisrdquoArchives de Pediatrie vol 8 no 5 pp474ndash480 2001
[21] M Manu Pereira and J Vives Corrons ldquoNeonatal haemo-globinopathy screening in Spainrdquo Journal of Clinical Pathologyvol 62 no 1 pp 22ndash25 2009
[22] C Saint-Martin M Romana A Bibrac et al ldquoUniversalnewborn screening for haemoglobinopathies in Guadeloupe(French West Indies) a 27-year experiencerdquo Journal of MedicalScreening vol 20 no 4 pp 177ndash182 2013
[23] C L Lobo S K Ballas A C Domingos P G Moura E M doNascimento and G P Cardoso ldquoNewborn screening programfor hemoglobinopathies in Rio de Janeiro Brazilrdquo PediatricBlood and Cancer vol 61 no 1 pp 34ndash39 2014
[24] P T McGann M G Ferris U Ramamurthy et al ldquoA prospec-tive newborn screening and treatment program for sickle cellanemia in Luanda Angolardquo The American Journal of Hematol-ogy vol 88 no 12 pp 984ndash989 2013
[25] J Patel and G R Serjeant ldquoNewborn screening for sickle celldisease in India the need for defining optimal clinical carerdquoIndian Journal of Pediatrics vol 81 no 3 pp 229ndash230 2014
[26] S Hajer T Neila H F Sondess et al ldquoA lower-cost protocolfor sickle cell disease neonatal screening in Tunisiardquo Annals ofSaudi Medicine vol 32 no 1 pp 49ndash52 2012
[27] V S Hertzberg C F Hinton B L Therrell and S K ShapiraldquoBirth prevalence rates of newborn screening disorders inrelation to screening practices in the United Statesrdquo Journal ofPediatrics vol 159 no 4 pp 555ndash560 2011
[28] M C Rahimy A Gangbo G Ahouignan and E AlihonouldquoNewborn screening for sickle cell disease in the Republic ofBeninrdquo Journal of Clinical Pathology vol 62 no 1 pp 46ndash482009
[29] E Kafando E Nacoulma Y Ouattara et al ldquoNeonatal haemo-globinopathy screening in Burkina Fasordquo Journal of ClinicalPathology vol 62 no 1 pp 39ndash41 2009
[30] L Tshilolo L M Aissi D Lukusa et al ldquoNeonatal screening forsickle cell anaemia in the Democratic Republic of the Congoexperience from a pioneer project on 31 204 newbornsrdquo Journalof Clinical Pathology vol 62 no 1 pp 35ndash38 2009
[31] B J Bain ldquoHaemoglobinopathy diagnosis algorithms lessonsand pitfallsrdquo Blood Reviews vol 25 no 5 pp 205ndash213 2011
[32] K Ryan B J Bain D Worthington et al ldquoSignificant haemo-globinopathies guidelines for screening and diagnosisrdquo BritishJournal of Haematology vol 149 no 1 pp 35ndash49 2010
[33] J Riou C Godart D Hurtrel et al ldquoCation-exchange HPLCevaluated for presumptive identification of hemoglobin vari-antsrdquo Clinical Chemistry vol 43 no 1 pp 34ndash39 1997
[34] G RenomCMereau PMaboudou and J-M Perini ldquoPotentialof the Sebia Capillarys neonat fast automated system forneonatal screening of sickle cell diseaserdquoClinical Chemistry andLaboratory Medicine vol 47 no 11 pp 1423ndash1432 2009
[35] M Campbell J S Henthorn and S C Davies ldquoEvaluation ofcation-exchange HPLC compared with isoelectric focusing forneonatal hemoglobinopathy screeningrdquoClinical Chemistry vol45 no 7 pp 969ndash975 1999
[36] E Mantikou C L Harteveld and P C Giordano ldquoNewbornscreening for hemoglobinopathies using capillary electrophore-sis technology testing the Capillarys Neonat Fast Hb devicerdquoClinical Biochemistry vol 43 no 16-17 pp 1345ndash1350 2010
10 BioMed Research International
[37] F Kutlar ldquoDiagnostic approach to hemoglobinopathiesrdquoHemoglobin vol 31 no 2 pp 243ndash250 2007
[38] G Bundesausschuss Anlage 2 Erweitertes Neugeborenen-screening 2010 httpwwwg-badedownloads83-691-233RL Kinder Anlage-2 2010-12-16pdf
[39] A Andermann I Blancquaert S Beauchamp and I CostealdquoGuiding policy decisions for genetic screening developing asystematic and transparent approachrdquo Public Health Genomicsvol 14 no 1 pp 9ndash16 2010
[40] A Andermann I Blancquaert S Beauchamp and V DeryldquoRevisiting Wilson and Jungner in the genomic age a review ofscreening criteria over the past 40 yearsrdquo Bulletin of the WorldHealth Organization vol 86 no 4 pp 317ndash319 2008
[41] S Lobitz C Frommel A Brose J Klein and O BlankensteinldquoIncidence of sickle cell disease in an unselected cohort ofneonates born in Berlin Germanyrdquo European Journal of HumanGenetics 2014
[42] P D Roa E A Turner and M D P Aguinaga ldquoHemoglobinvariant detection from dried blood specimens by high perfor-mance liquid chromatographyrdquo Annals of Clinical and Labora-tory Science vol 23 no 6 pp 433ndash438 1993
[43] CMurray S KHall andPGriffiths ldquoAn evaluation of the Sebiacapillarys Neonat Haemoglobin FASTŮ system for routinenewborn screening for sickle cell diseaserdquo International Journalof Laboratory Hematology vol 33 no 5 pp 533ndash539 2011
[44] A F S B Brandenburg ldquoStatistisches Jahrbuch 2011rdquo 2011httpswwwstatistik-berlin-brandenburgdeprodukteJahrbuchjb2011JB 2011 BEpdf
[45] E Harms and B Olgemoller ldquoNeonatal screening for metabolicand endocrine disordersrdquo Deutsches Arzteblatt Internationalvol 108 no 1-2 pp 11ndash22 2011
[46] A Joutovsky J Hadzi-Nesic andM A Nardi ldquoHPLC retentiontime as a diagnostic tool for hemoglobin variants and hemo-globinopathies a study of 60 000 samples in a clinical diagnosticlaboratoryrdquo Clinical Chemistry vol 50 no 10 pp 1736ndash17472004
[47] E Kohne and E Kleihauer ldquoHemoglobinopathies in Ger-manymdasha longitudinal study over four decadesrdquo DeutschesArzteblatt vol 107 no 5 pp 65ndash71 2010
[48] R Dickerhoff O Genzel-Boroviczeny and E Kohne ldquoHaemo-globinopathies and newborn haemoglobinopathy screening inGermanyrdquo Journal of Clinical Pathology vol 62 no 1 article 342009
[49] Enactment of the German Federal Parliament (Bundestag)ldquoHuman Genetic Examination Act (Genetic Diagnosis Act-GenDG)rdquo 2009 httpswwweshgorgfileadminwwweshgorgdocumentsEuropeLegalWSGermany GenDG Law GermanEnglishpdf
[50] J M Wilson and Y G Jungner Principles and Practice of MassScreening for Disease WHO Public Health Papers 1968
[51] Gendiagnostik-Kommission ldquoRichtlinien der Gendiagnostik-Komission (GEKO) fur die Anforderung an die Durchfuhrunggenetischer Reihenuntersuchungen gemaszlig sect23 Abs 2 Nr 6GenDGrdquo Bundesgesundheitsblatt vol 56 pp 321ndash324 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 BioMed Research International
Table 1 Detailed information on screening-positive babies
Patient number (ethnical origin) Screening patterns HPLCCE Molecular genetic result 1 (West African) FSaFS SCD-SS 2 (West African) F5SaBFS SCD-SS 3 (Middle East) FSa5BFS SCD-S1205730 thalassemia 4 (West African) FaCSFSC SCD-SC 5 (Middle East) F4SAFS SCD-SS 6 (West African) FSCaFSC SCD-SC 7 (Middle East) FSa5FS SCD-SS 8 (West African) FSaBFS SCD-SS 9 (West African) FS4aFS SCD-SS 10 (West African) FS5aBFS SCD-SS 11 (West African) FCSaFSC SCD-SC 12 (West African) FSa2BFS SCD-SS 13 (West African) FSa2BFS SCD-SS 14 (West African) FCS1FSC SCD-SC
Table 2 High interrun precision of HPLC retention times of retention time markers
Hemoglobin Retention times of RTMmean (range) [min] CV []
Manufacturerrsquosspecifications mean
(range) [min]F 0494 (0471ndash0510) 15 0530 (0470ndash0590)A 0792 (0770ndash0804) 09 0800 (0730ndash0870)EA2 0954 (0919ndash0970) 10 0970 (0930ndash1010)D 1042 (1005ndash1072) 11 1060 (1010ndash1110)S 1158 (1116ndash1183) 12 1190 (1130ndash1250)C 1663 (1634ndash1684) 06 1680 (1610ndash1750)
Table 3 High precision of HPLC retention times of hemoglobins derived from dried blood spot samples
Presumptive hemoglobin Retention times mean (range) [min] CV [] 119899
A 0800 (0785ndash0816) 08 100E 0952 (0936ndash0968) 08 26D 1044 (1028ndash1060) 10 11S 1154 (1190ndash1130) 09 100C 1660 (1647ndash1670) 04 23
These samples were randomly integrated into several runsincluding all steps from pre- to postanalytics to include allinfluencing factors Table 4 shows the results of repeated ana-lyzes of these quality control samples known to be heterozy-gous for HbS (A) or HbC (B) on different working days
34 Precision of CE As quality controls of CE liquid controlsamples containing hemoglobins F A S and C were used ineach run on different working days (Table 5)
35 Costs All in all we examined samples from 38220 new-borns 37970 only by HPLC 250 additionally by CE becausethe samples showed an abnormal hemoglobin pattern in theHPLC For the examination of the entire cohort we incurredcosts of EUR 55000 A large part of this sum (just under50) was labor costs However the sum also contains the
costs for instrument hire for consumables and so forthThistranslates into a per-sample cost of EUR 144 (US$197)
4 Discussion
There are practically no epidemiological data to date on theprevalence and incidence of SCD in Germany [41 47 48]Cautious estimates made so far suggest a figure of about 3000to 4000 patients in the whole country These patients arewithout exception of immigrant origin [47]
Over a period of more than one year we tested withoutpreselection on the basis of ethnic origin 87 of all childrenborn in Berlin (34084 of 39249) for the presence of SCDand identified 14 with the disease [41] The incidence of SCD(41110000) amongst the children examined was thus higherthan the incidence of any other endocrine or metabolic
BioMed Research International 7
Table 4 (a) Interrun precision of HPLC determined on two dried blood spot samples from newborns heterozygous for HbS (b) Interrunprecision of HPLC determined on a dried blood spot sample from a newborn heterozygous for HbC
(a)
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] 119899
Control 1 373 29 89 53 36 63 11Control 2 401 48 19 27 10 50 8
(b)
HbF mean [] CV [] HbA mean [] CV [] HbC mean [] CV [] 119899
Control 3 396 57 17 22 13 28 11Precision was reduced if certain hemoglobin fractions were present in an order close to the detection limit of 1 of the total AUC
Table 5 Interrun precision of CE determined on liquid control samples provided by the manufacturer
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] HbC mean [] CV [] 119899Control FASC 188 48 355 20 145 43 54 77 5
disorder tested for in the context of the German extendedNBS program SCD should therefore be included in the NBSat least in Berlin In order to decidewhether there is a need fora national NBS program for SCD we now require data fromother regions particularly from presumed low-prevalenceareas
The results presented in this paper show that such epi-demiological data can be generated with investment ofrelatively little time and money as the samples do not needto be examined fresh on a day-to-day basis Instead largenumbers of samples can be analyzed retrospectively It is clearthat the costs per sample (144 EUR) in the context of ourpilot study will not be comparable with the expenses in thecontext of a national screening program While the costs forconsumables and so forth would probably be a little loweron account of the substantially higher patient numbers therewould be considerable additional expenses for administrativepurposes such as quality assurance Further additional costswould arise for staff training and for the entire infrastructurewhich has to be made available around the actual testing
In this study dried blood spot cards up to six monthsold provided satisfactory results However very old samplespresent a particular challenge because cellulose particleswhich come off the dried blood cards together with the bloodcan interfere considerably with the measurement They aredeposited in the fine capillaries of themeasuring instrumentsclogging them or creating additional unspecific measuringsignals The continuously increasing degradation of thehemoglobin also leads to additional measuring signals par-ticularly to increased background noise as well as reducingthe amount of analyzable material In the worst case onemight evenmiss a significant disease due tomisinterpretationof a peak resembling HbA for example a 120573-thalassemiamajor pattern could be confused with a physiological FApattern or homozygosity forHbS could be confusedwith SCTSample preparation is therefore of decisive importance
Factors which can influence the sample quality are asfollows
(1) The concentration of the hemoglobin in thehemolysate This depends on the volume of theblood sample thus on the saturation of the filter cardand on the degree of degradation of the hemoglobinThe latter is essentially dependent on the age and thestorage conditions of the sample Further importantparameters are the elution volume and elution time
(2) Instrument performance is influenced significantly bythe condition of the dried blood spot card This isin turn also dependent on the sample age and thestorage conditions In the case of older cards celluloseparticles are removed from the card together with theblood and can then interfere with the measurement
Prolonging the elution time increases the hemoglobinconcentration in the hemolysate and also the likelihood ofcellulose particles becoming detached from the filter cardThe elution conditions described in the methods section takeinto account both phenomena and represent the necessarycompromise
The implementation of pilot studies of this kind requiresthe availability of a high throughput method In our expe-rience HPLC and CE are equally suitable The CE electro-pherograms appeared to us to be easier to interpret than theHPLC chromatograms because there were fewer unspecificsignals in the former Whichever method is chosen it iscrucial that the analytical laboratory has special expertisewith regard to the IT-supported interpretation of the rawmeasurements
Disease screening programs are characterized by the factthat certain people are examined for the presence of a certaindisease simply because they belong to a certain populationThe subjects are examined or tested regardless of whetherthere is any concrete reason to suspect the presence of
8 BioMed Research International
the target disease The large majority of the subjects screenedare completely healthy This raises particular ethical legaltechnical and economic issues
The German Genetic Testing Act (GenDG) came intoforce on January 2 2010 and is a constant topic of debate onaccount of its very strict regulations [49] It controls genetictesting in humans and the use of genetic samples and dataThe GenDG specifies interalia that analyses of the productsof nucleic acids (gene product analyses) are also consideredgenetic analyses and therefore deemed legally equal to exam-ination of the number and structure of the chromosomes andof themolecular structure of DNA and RNAThismeans thathemoglobinopathy testing using protein separation methodssuch as HPLC or CE comes under the GenDG
Theultimate goal of theGenDG is to prevent the potentialdangers and discrimination associated with the examina-tion of human genetic traits One of the most importantprinciples is the right of the individual to informationalself-determination This right which enjoys internationallyunique protection in Germany includes the right to knowand more important in this context the right not to knowIts most important implication is that we are not allowed inGermany to report sickle cell trait
The GenDG distinguishes between genetic tests per-formed in amedical context and tests performed in a researchcontext and only applies to tests ordered in amedical contextA distinction is also made between diagnostic tests andpredictive tests In addition the GenDG regulates geneticscreening which would include NBS for SCD German lawrequires the establishment of an independent interdisci-plinary Genetic Testing Commission (GEKO) which hasbeen set up at the Robert Koch Institute and amongst otherthings lays down the requirements for the performance ofgenetic screening tests [49]These requirements are based onthe specific criteria for genetic screening developed byAnder-mann et al on the basis of theWHO screening criteria ofWil-son and Jungner [39 50]The GEKO has expressly stated thatresults of studies performed in other countries with differenthealthcare systems and different population structures can-not necessarily be extrapolated toGermany [51] For examplesome screening criteria are based on local conditions whichdo not obtain in Germany or at least not in all parts of thecountry Sickle cell patients cannot in particular be offeredstate-of-the-art care everywhere in Germany Nonmalignanthematology has been almost entirely neglected in the trainingof all groups of healthcare professionals in the past and thehemoglobinopathies as a whole are still not seen as a problemin Germany However a national strategy for preventionand treatment of SCD is currently under development TheSociety for Pediatric Oncology and Hematology (GPOH)has commissioned the establishment of a patient registerreference centers and a treatment guidelineThis is importantbecause if it is to make any sense a newborn screeningprogram requires not only the identification of sick babies butalso a functioning infrastructure which ensures that affectedchildren also receive appropriate care after the diagnosisThis includes both medical and psychosocial care as wellas sufficient counseling resources for the patients and theirparents
5 Conclusions
Our pilot project shows that itmakes sense at least regionallyto think about the introduction of some kind ofNBS programfor SCD in Germany whatever specific form this takesThe pilot projects necessary for this must be embarked onnow In addition to the presumed high-prevalence regionssuch as Berlin Hamburg the Ruhr region or Frankfurtepidemiological data should also be collected from pre-sumed low-prevalence regions (eg rural Bavaria and Baden-Wurttemberg)
Our data show that the organization and realization ofsuch pilot projects is relatively unproblematic and inexpen-sive as samples can be collected over several months and thenanalyzed together However we recommend that the samplesshould not be older than three months at the time of analysisIt is of fundamental importance that the Genetic Testing Actdoes not apply to such pilot projects as they involve genetictesting in the context of research
Conflict of Interests
Stephan Lobitz Claudia Frommel and Oliver Blankensteinreceived a research grant from Novartis Oncology GmbH(Nuremberg Germany) to perform this study In additionBio-Rad Laboratories GmbH (Munich Germany) indirectlyfunded this project through a preferential price for HPLCconsumables Beyond that the authors declare no competinginterest
Acknowledgments
This work is part of Stephan Lobitzrsquos dissertation in theUniversity College London ldquoMaster of Science in Haemoglo-binopathyrdquo program Stephan Lobitz is deeply indebted toDr Ratna Chatterjee Dr Rekha Bajoria the ThalassaemiaInternational Federation (TIF) and ldquoKINDerLEBEN-Vereinzur Forderung der Klinik fur krebskranke Kinder eV BerlinrdquoThe authors thank Novartis Oncology GmbH and Bio-RadLaboratories GmbH who generously funded this projectMany thanks are due to all parents and patients who took partin this study
References
[1] D C Rees T N Williams and M T Gladwin ldquoSickle-celldiseaserdquoThe Lancet vol 376 no 9757 pp 2018ndash2031 2010
[2] D Powars G Overturf J Weiss S Lee and L Chan ldquoPneumo-coccal septicemia in children with sickle cell anemia Changingtrend of survivalrdquo Journal of the American Medical Associationvol 245 no 18 pp 1839ndash1842 1981
[3] A M Emond R Collis D Darvill D R Higgs G H Maudeand G R Serjeant ldquoAcute splenic sequestration in homozygoussickle cell disease natural history and managementrdquo The Jour-nal of Pediatrics vol 107 no 2 pp 201ndash206 1985
[4] M H Gaston J I Verter G Woods et al ldquoProphylaxis withoral penicillin in children with sickle cell anemia a randomizedtrialrdquoThe New England Journal of Medicine vol 314 no 25 pp1593ndash1599 1986
BioMed Research International 9
[5] G R Serjeant and B E Serjeant ldquoManagement of sickle celldisease lessons from the Jamaican cohort studyrdquo Blood Reviewsvol 7 no 3 pp 137ndash145 1993
[6] A Lee P Thomas L Cupidore B Serjeant and G SerjeantldquoImproved survival in homozygous sickle cell disease lessonsfrom a cohort studyrdquo British Medical Journal vol 311 no 7020pp 1600ndash1602 1995
[7] T V Adamkiewicz S Sarnaik G R Buchanan et al ldquoInvasivepneumococcal infections in children with sickle cell diseasein the era of penicillin prophylaxis antibiotic resistance and23-valent pneumococcal polysaccharide vaccinationrdquo Journal ofPediatrics vol 143 no 4 pp 438ndash444 2003
[8] N B Halasa S M Shankar T R Talbot et al ldquoIncidence ofinvasive pneumococcal disease among individuals with sicklecell disease before and after the introduction of the pneumo-coccal conjugate vaccinerdquo Clinical Infectious Diseases vol 44no 11 pp 1428ndash1433 2007
[9] T V Adamkiewicz B J Silk J Howgate et al ldquoEffectiveness ofthe 7-valent pneumococcal conjugate vaccine in children withsickle cell disease in the first decade of liferdquo Pediatrics vol 121no 3 pp 562ndash569 2008
[10] S D Grosse H K Atrash I Odame D Amendah F B Pieland T N Williams ldquoThe Jamaican historical experience of theimpact of educational interventions on sickle cell disease childmortalityrdquoTheAmerican Journal of PreventiveMedicine vol 42no 6 pp e101ndashe103 2012
[11] H Heijboer X W van den Tweel M Peters M Knuist JPrins and H S Heymans ldquoOne year of neonatal screening forsickle cell disease in the emma kinderziekenhuisacademischmedisch centrum Amsterdamrdquo Nederlands Tijdschrift voorGeneeskunde vol 145 no 37 pp 1795ndash1799 2001
[12] B Gulbis F Cotton A Ferster et al ldquoNeonatal haemoglobin-opathy screening in Belgiumrdquo Journal of Clinical Pathology vol62 no 1 pp 49ndash52 2009
[13] A Streetly R Latinovic and J Henthorn ldquoPositive screeningand carrier results for the England-wide universal newbornsickle cell screening programme by ethnicity and area for 2005-07rdquo Journal of Clinical Pathology vol 63 no 7 pp 626ndash6292010
[14] E Ballardini A TaroccoMMarsella et al ldquoUniversal neonatalscreening for sickle cell disease and other haemoglobinopathiesin Ferrara Italyrdquo Blood Transfusion vol 11 no 2 pp 245ndash2492013
[15] J Bardakdjian-Michau M Bahuau D Hurtrel et al ldquoNeonatalscreening for sickle cell disease in Francerdquo Journal of ClinicalPathology vol 62 no 1 pp 31ndash33 2009
[16] E Cela De Julian E Dulın Iniguez M Guerrero Soler etal ldquoEvaluation of systematic neonatal screening for sickle celldiseases in Madrid three years after its introductionrdquo Anales dePediatria vol 66 no 4 pp 382ndash386 2007
[17] M J Bouva K Mohrmann H B J M Brinkman et alldquoImplementing neonatal screening for haemoglobinopathies inthe Netherlandsrdquo Journal of Medical Screening vol 17 no 2 pp58ndash65 2010
[18] P C GiordanoM J Bouva and C L Harteveld ldquoA confidentialinquiry estimating the number of patients affected with sicklecell disease and thalassemia major confirms the need for aprevention strategy in theNetherlandsrdquoHemoglobin vol 28 no4 pp 287ndash296 2004
[19] S Berthet F Monpoux A-M Soummer E Berard J Sarlesand C Badens ldquoNeonatal screening for sickle cell disease in
Nice University Hospital review of 8 last yearsrdquo Archives dePediatrie vol 17 no 12 pp 1652ndash1656 2010
[20] R Ducrocq M Benkerrou L Brahimi et al ldquoNeonatal screen-ing for sickle cell anemia evaluation of a five-year experience inan area of northern ParisrdquoArchives de Pediatrie vol 8 no 5 pp474ndash480 2001
[21] M Manu Pereira and J Vives Corrons ldquoNeonatal haemo-globinopathy screening in Spainrdquo Journal of Clinical Pathologyvol 62 no 1 pp 22ndash25 2009
[22] C Saint-Martin M Romana A Bibrac et al ldquoUniversalnewborn screening for haemoglobinopathies in Guadeloupe(French West Indies) a 27-year experiencerdquo Journal of MedicalScreening vol 20 no 4 pp 177ndash182 2013
[23] C L Lobo S K Ballas A C Domingos P G Moura E M doNascimento and G P Cardoso ldquoNewborn screening programfor hemoglobinopathies in Rio de Janeiro Brazilrdquo PediatricBlood and Cancer vol 61 no 1 pp 34ndash39 2014
[24] P T McGann M G Ferris U Ramamurthy et al ldquoA prospec-tive newborn screening and treatment program for sickle cellanemia in Luanda Angolardquo The American Journal of Hematol-ogy vol 88 no 12 pp 984ndash989 2013
[25] J Patel and G R Serjeant ldquoNewborn screening for sickle celldisease in India the need for defining optimal clinical carerdquoIndian Journal of Pediatrics vol 81 no 3 pp 229ndash230 2014
[26] S Hajer T Neila H F Sondess et al ldquoA lower-cost protocolfor sickle cell disease neonatal screening in Tunisiardquo Annals ofSaudi Medicine vol 32 no 1 pp 49ndash52 2012
[27] V S Hertzberg C F Hinton B L Therrell and S K ShapiraldquoBirth prevalence rates of newborn screening disorders inrelation to screening practices in the United Statesrdquo Journal ofPediatrics vol 159 no 4 pp 555ndash560 2011
[28] M C Rahimy A Gangbo G Ahouignan and E AlihonouldquoNewborn screening for sickle cell disease in the Republic ofBeninrdquo Journal of Clinical Pathology vol 62 no 1 pp 46ndash482009
[29] E Kafando E Nacoulma Y Ouattara et al ldquoNeonatal haemo-globinopathy screening in Burkina Fasordquo Journal of ClinicalPathology vol 62 no 1 pp 39ndash41 2009
[30] L Tshilolo L M Aissi D Lukusa et al ldquoNeonatal screening forsickle cell anaemia in the Democratic Republic of the Congoexperience from a pioneer project on 31 204 newbornsrdquo Journalof Clinical Pathology vol 62 no 1 pp 35ndash38 2009
[31] B J Bain ldquoHaemoglobinopathy diagnosis algorithms lessonsand pitfallsrdquo Blood Reviews vol 25 no 5 pp 205ndash213 2011
[32] K Ryan B J Bain D Worthington et al ldquoSignificant haemo-globinopathies guidelines for screening and diagnosisrdquo BritishJournal of Haematology vol 149 no 1 pp 35ndash49 2010
[33] J Riou C Godart D Hurtrel et al ldquoCation-exchange HPLCevaluated for presumptive identification of hemoglobin vari-antsrdquo Clinical Chemistry vol 43 no 1 pp 34ndash39 1997
[34] G RenomCMereau PMaboudou and J-M Perini ldquoPotentialof the Sebia Capillarys neonat fast automated system forneonatal screening of sickle cell diseaserdquoClinical Chemistry andLaboratory Medicine vol 47 no 11 pp 1423ndash1432 2009
[35] M Campbell J S Henthorn and S C Davies ldquoEvaluation ofcation-exchange HPLC compared with isoelectric focusing forneonatal hemoglobinopathy screeningrdquoClinical Chemistry vol45 no 7 pp 969ndash975 1999
[36] E Mantikou C L Harteveld and P C Giordano ldquoNewbornscreening for hemoglobinopathies using capillary electrophore-sis technology testing the Capillarys Neonat Fast Hb devicerdquoClinical Biochemistry vol 43 no 16-17 pp 1345ndash1350 2010
10 BioMed Research International
[37] F Kutlar ldquoDiagnostic approach to hemoglobinopathiesrdquoHemoglobin vol 31 no 2 pp 243ndash250 2007
[38] G Bundesausschuss Anlage 2 Erweitertes Neugeborenen-screening 2010 httpwwwg-badedownloads83-691-233RL Kinder Anlage-2 2010-12-16pdf
[39] A Andermann I Blancquaert S Beauchamp and I CostealdquoGuiding policy decisions for genetic screening developing asystematic and transparent approachrdquo Public Health Genomicsvol 14 no 1 pp 9ndash16 2010
[40] A Andermann I Blancquaert S Beauchamp and V DeryldquoRevisiting Wilson and Jungner in the genomic age a review ofscreening criteria over the past 40 yearsrdquo Bulletin of the WorldHealth Organization vol 86 no 4 pp 317ndash319 2008
[41] S Lobitz C Frommel A Brose J Klein and O BlankensteinldquoIncidence of sickle cell disease in an unselected cohort ofneonates born in Berlin Germanyrdquo European Journal of HumanGenetics 2014
[42] P D Roa E A Turner and M D P Aguinaga ldquoHemoglobinvariant detection from dried blood specimens by high perfor-mance liquid chromatographyrdquo Annals of Clinical and Labora-tory Science vol 23 no 6 pp 433ndash438 1993
[43] CMurray S KHall andPGriffiths ldquoAn evaluation of the Sebiacapillarys Neonat Haemoglobin FASTŮ system for routinenewborn screening for sickle cell diseaserdquo International Journalof Laboratory Hematology vol 33 no 5 pp 533ndash539 2011
[44] A F S B Brandenburg ldquoStatistisches Jahrbuch 2011rdquo 2011httpswwwstatistik-berlin-brandenburgdeprodukteJahrbuchjb2011JB 2011 BEpdf
[45] E Harms and B Olgemoller ldquoNeonatal screening for metabolicand endocrine disordersrdquo Deutsches Arzteblatt Internationalvol 108 no 1-2 pp 11ndash22 2011
[46] A Joutovsky J Hadzi-Nesic andM A Nardi ldquoHPLC retentiontime as a diagnostic tool for hemoglobin variants and hemo-globinopathies a study of 60 000 samples in a clinical diagnosticlaboratoryrdquo Clinical Chemistry vol 50 no 10 pp 1736ndash17472004
[47] E Kohne and E Kleihauer ldquoHemoglobinopathies in Ger-manymdasha longitudinal study over four decadesrdquo DeutschesArzteblatt vol 107 no 5 pp 65ndash71 2010
[48] R Dickerhoff O Genzel-Boroviczeny and E Kohne ldquoHaemo-globinopathies and newborn haemoglobinopathy screening inGermanyrdquo Journal of Clinical Pathology vol 62 no 1 article 342009
[49] Enactment of the German Federal Parliament (Bundestag)ldquoHuman Genetic Examination Act (Genetic Diagnosis Act-GenDG)rdquo 2009 httpswwweshgorgfileadminwwweshgorgdocumentsEuropeLegalWSGermany GenDG Law GermanEnglishpdf
[50] J M Wilson and Y G Jungner Principles and Practice of MassScreening for Disease WHO Public Health Papers 1968
[51] Gendiagnostik-Kommission ldquoRichtlinien der Gendiagnostik-Komission (GEKO) fur die Anforderung an die Durchfuhrunggenetischer Reihenuntersuchungen gemaszlig sect23 Abs 2 Nr 6GenDGrdquo Bundesgesundheitsblatt vol 56 pp 321ndash324 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
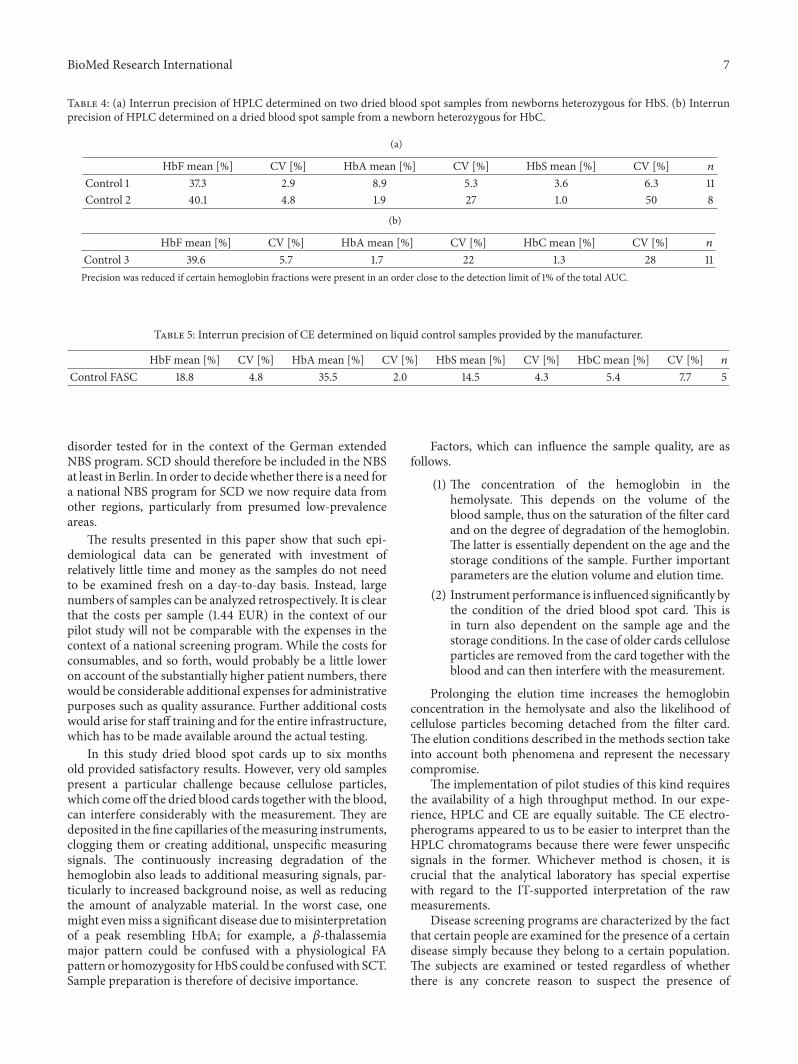
BioMed Research International 7
Table 4 (a) Interrun precision of HPLC determined on two dried blood spot samples from newborns heterozygous for HbS (b) Interrunprecision of HPLC determined on a dried blood spot sample from a newborn heterozygous for HbC
(a)
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] 119899
Control 1 373 29 89 53 36 63 11Control 2 401 48 19 27 10 50 8
(b)
HbF mean [] CV [] HbA mean [] CV [] HbC mean [] CV [] 119899
Control 3 396 57 17 22 13 28 11Precision was reduced if certain hemoglobin fractions were present in an order close to the detection limit of 1 of the total AUC
Table 5 Interrun precision of CE determined on liquid control samples provided by the manufacturer
HbF mean [] CV [] HbA mean [] CV [] HbS mean [] CV [] HbC mean [] CV [] 119899Control FASC 188 48 355 20 145 43 54 77 5
disorder tested for in the context of the German extendedNBS program SCD should therefore be included in the NBSat least in Berlin In order to decidewhether there is a need fora national NBS program for SCD we now require data fromother regions particularly from presumed low-prevalenceareas
The results presented in this paper show that such epi-demiological data can be generated with investment ofrelatively little time and money as the samples do not needto be examined fresh on a day-to-day basis Instead largenumbers of samples can be analyzed retrospectively It is clearthat the costs per sample (144 EUR) in the context of ourpilot study will not be comparable with the expenses in thecontext of a national screening program While the costs forconsumables and so forth would probably be a little loweron account of the substantially higher patient numbers therewould be considerable additional expenses for administrativepurposes such as quality assurance Further additional costswould arise for staff training and for the entire infrastructurewhich has to be made available around the actual testing
In this study dried blood spot cards up to six monthsold provided satisfactory results However very old samplespresent a particular challenge because cellulose particleswhich come off the dried blood cards together with the bloodcan interfere considerably with the measurement They aredeposited in the fine capillaries of themeasuring instrumentsclogging them or creating additional unspecific measuringsignals The continuously increasing degradation of thehemoglobin also leads to additional measuring signals par-ticularly to increased background noise as well as reducingthe amount of analyzable material In the worst case onemight evenmiss a significant disease due tomisinterpretationof a peak resembling HbA for example a 120573-thalassemiamajor pattern could be confused with a physiological FApattern or homozygosity forHbS could be confusedwith SCTSample preparation is therefore of decisive importance
Factors which can influence the sample quality are asfollows
(1) The concentration of the hemoglobin in thehemolysate This depends on the volume of theblood sample thus on the saturation of the filter cardand on the degree of degradation of the hemoglobinThe latter is essentially dependent on the age and thestorage conditions of the sample Further importantparameters are the elution volume and elution time
(2) Instrument performance is influenced significantly bythe condition of the dried blood spot card This isin turn also dependent on the sample age and thestorage conditions In the case of older cards celluloseparticles are removed from the card together with theblood and can then interfere with the measurement
Prolonging the elution time increases the hemoglobinconcentration in the hemolysate and also the likelihood ofcellulose particles becoming detached from the filter cardThe elution conditions described in the methods section takeinto account both phenomena and represent the necessarycompromise
The implementation of pilot studies of this kind requiresthe availability of a high throughput method In our expe-rience HPLC and CE are equally suitable The CE electro-pherograms appeared to us to be easier to interpret than theHPLC chromatograms because there were fewer unspecificsignals in the former Whichever method is chosen it iscrucial that the analytical laboratory has special expertisewith regard to the IT-supported interpretation of the rawmeasurements
Disease screening programs are characterized by the factthat certain people are examined for the presence of a certaindisease simply because they belong to a certain populationThe subjects are examined or tested regardless of whetherthere is any concrete reason to suspect the presence of
8 BioMed Research International
the target disease The large majority of the subjects screenedare completely healthy This raises particular ethical legaltechnical and economic issues
The German Genetic Testing Act (GenDG) came intoforce on January 2 2010 and is a constant topic of debate onaccount of its very strict regulations [49] It controls genetictesting in humans and the use of genetic samples and dataThe GenDG specifies interalia that analyses of the productsof nucleic acids (gene product analyses) are also consideredgenetic analyses and therefore deemed legally equal to exam-ination of the number and structure of the chromosomes andof themolecular structure of DNA and RNAThismeans thathemoglobinopathy testing using protein separation methodssuch as HPLC or CE comes under the GenDG
Theultimate goal of theGenDG is to prevent the potentialdangers and discrimination associated with the examina-tion of human genetic traits One of the most importantprinciples is the right of the individual to informationalself-determination This right which enjoys internationallyunique protection in Germany includes the right to knowand more important in this context the right not to knowIts most important implication is that we are not allowed inGermany to report sickle cell trait
The GenDG distinguishes between genetic tests per-formed in amedical context and tests performed in a researchcontext and only applies to tests ordered in amedical contextA distinction is also made between diagnostic tests andpredictive tests In addition the GenDG regulates geneticscreening which would include NBS for SCD German lawrequires the establishment of an independent interdisci-plinary Genetic Testing Commission (GEKO) which hasbeen set up at the Robert Koch Institute and amongst otherthings lays down the requirements for the performance ofgenetic screening tests [49]These requirements are based onthe specific criteria for genetic screening developed byAnder-mann et al on the basis of theWHO screening criteria ofWil-son and Jungner [39 50]The GEKO has expressly stated thatresults of studies performed in other countries with differenthealthcare systems and different population structures can-not necessarily be extrapolated toGermany [51] For examplesome screening criteria are based on local conditions whichdo not obtain in Germany or at least not in all parts of thecountry Sickle cell patients cannot in particular be offeredstate-of-the-art care everywhere in Germany Nonmalignanthematology has been almost entirely neglected in the trainingof all groups of healthcare professionals in the past and thehemoglobinopathies as a whole are still not seen as a problemin Germany However a national strategy for preventionand treatment of SCD is currently under development TheSociety for Pediatric Oncology and Hematology (GPOH)has commissioned the establishment of a patient registerreference centers and a treatment guidelineThis is importantbecause if it is to make any sense a newborn screeningprogram requires not only the identification of sick babies butalso a functioning infrastructure which ensures that affectedchildren also receive appropriate care after the diagnosisThis includes both medical and psychosocial care as wellas sufficient counseling resources for the patients and theirparents
5 Conclusions
Our pilot project shows that itmakes sense at least regionallyto think about the introduction of some kind ofNBS programfor SCD in Germany whatever specific form this takesThe pilot projects necessary for this must be embarked onnow In addition to the presumed high-prevalence regionssuch as Berlin Hamburg the Ruhr region or Frankfurtepidemiological data should also be collected from pre-sumed low-prevalence regions (eg rural Bavaria and Baden-Wurttemberg)
Our data show that the organization and realization ofsuch pilot projects is relatively unproblematic and inexpen-sive as samples can be collected over several months and thenanalyzed together However we recommend that the samplesshould not be older than three months at the time of analysisIt is of fundamental importance that the Genetic Testing Actdoes not apply to such pilot projects as they involve genetictesting in the context of research
Conflict of Interests
Stephan Lobitz Claudia Frommel and Oliver Blankensteinreceived a research grant from Novartis Oncology GmbH(Nuremberg Germany) to perform this study In additionBio-Rad Laboratories GmbH (Munich Germany) indirectlyfunded this project through a preferential price for HPLCconsumables Beyond that the authors declare no competinginterest
Acknowledgments
This work is part of Stephan Lobitzrsquos dissertation in theUniversity College London ldquoMaster of Science in Haemoglo-binopathyrdquo program Stephan Lobitz is deeply indebted toDr Ratna Chatterjee Dr Rekha Bajoria the ThalassaemiaInternational Federation (TIF) and ldquoKINDerLEBEN-Vereinzur Forderung der Klinik fur krebskranke Kinder eV BerlinrdquoThe authors thank Novartis Oncology GmbH and Bio-RadLaboratories GmbH who generously funded this projectMany thanks are due to all parents and patients who took partin this study
References
[1] D C Rees T N Williams and M T Gladwin ldquoSickle-celldiseaserdquoThe Lancet vol 376 no 9757 pp 2018ndash2031 2010
[2] D Powars G Overturf J Weiss S Lee and L Chan ldquoPneumo-coccal septicemia in children with sickle cell anemia Changingtrend of survivalrdquo Journal of the American Medical Associationvol 245 no 18 pp 1839ndash1842 1981
[3] A M Emond R Collis D Darvill D R Higgs G H Maudeand G R Serjeant ldquoAcute splenic sequestration in homozygoussickle cell disease natural history and managementrdquo The Jour-nal of Pediatrics vol 107 no 2 pp 201ndash206 1985
[4] M H Gaston J I Verter G Woods et al ldquoProphylaxis withoral penicillin in children with sickle cell anemia a randomizedtrialrdquoThe New England Journal of Medicine vol 314 no 25 pp1593ndash1599 1986
BioMed Research International 9
[5] G R Serjeant and B E Serjeant ldquoManagement of sickle celldisease lessons from the Jamaican cohort studyrdquo Blood Reviewsvol 7 no 3 pp 137ndash145 1993
[6] A Lee P Thomas L Cupidore B Serjeant and G SerjeantldquoImproved survival in homozygous sickle cell disease lessonsfrom a cohort studyrdquo British Medical Journal vol 311 no 7020pp 1600ndash1602 1995
[7] T V Adamkiewicz S Sarnaik G R Buchanan et al ldquoInvasivepneumococcal infections in children with sickle cell diseasein the era of penicillin prophylaxis antibiotic resistance and23-valent pneumococcal polysaccharide vaccinationrdquo Journal ofPediatrics vol 143 no 4 pp 438ndash444 2003
[8] N B Halasa S M Shankar T R Talbot et al ldquoIncidence ofinvasive pneumococcal disease among individuals with sicklecell disease before and after the introduction of the pneumo-coccal conjugate vaccinerdquo Clinical Infectious Diseases vol 44no 11 pp 1428ndash1433 2007
[9] T V Adamkiewicz B J Silk J Howgate et al ldquoEffectiveness ofthe 7-valent pneumococcal conjugate vaccine in children withsickle cell disease in the first decade of liferdquo Pediatrics vol 121no 3 pp 562ndash569 2008
[10] S D Grosse H K Atrash I Odame D Amendah F B Pieland T N Williams ldquoThe Jamaican historical experience of theimpact of educational interventions on sickle cell disease childmortalityrdquoTheAmerican Journal of PreventiveMedicine vol 42no 6 pp e101ndashe103 2012
[11] H Heijboer X W van den Tweel M Peters M Knuist JPrins and H S Heymans ldquoOne year of neonatal screening forsickle cell disease in the emma kinderziekenhuisacademischmedisch centrum Amsterdamrdquo Nederlands Tijdschrift voorGeneeskunde vol 145 no 37 pp 1795ndash1799 2001
[12] B Gulbis F Cotton A Ferster et al ldquoNeonatal haemoglobin-opathy screening in Belgiumrdquo Journal of Clinical Pathology vol62 no 1 pp 49ndash52 2009
[13] A Streetly R Latinovic and J Henthorn ldquoPositive screeningand carrier results for the England-wide universal newbornsickle cell screening programme by ethnicity and area for 2005-07rdquo Journal of Clinical Pathology vol 63 no 7 pp 626ndash6292010
[14] E Ballardini A TaroccoMMarsella et al ldquoUniversal neonatalscreening for sickle cell disease and other haemoglobinopathiesin Ferrara Italyrdquo Blood Transfusion vol 11 no 2 pp 245ndash2492013
[15] J Bardakdjian-Michau M Bahuau D Hurtrel et al ldquoNeonatalscreening for sickle cell disease in Francerdquo Journal of ClinicalPathology vol 62 no 1 pp 31ndash33 2009
[16] E Cela De Julian E Dulın Iniguez M Guerrero Soler etal ldquoEvaluation of systematic neonatal screening for sickle celldiseases in Madrid three years after its introductionrdquo Anales dePediatria vol 66 no 4 pp 382ndash386 2007
[17] M J Bouva K Mohrmann H B J M Brinkman et alldquoImplementing neonatal screening for haemoglobinopathies inthe Netherlandsrdquo Journal of Medical Screening vol 17 no 2 pp58ndash65 2010
[18] P C GiordanoM J Bouva and C L Harteveld ldquoA confidentialinquiry estimating the number of patients affected with sicklecell disease and thalassemia major confirms the need for aprevention strategy in theNetherlandsrdquoHemoglobin vol 28 no4 pp 287ndash296 2004
[19] S Berthet F Monpoux A-M Soummer E Berard J Sarlesand C Badens ldquoNeonatal screening for sickle cell disease in
Nice University Hospital review of 8 last yearsrdquo Archives dePediatrie vol 17 no 12 pp 1652ndash1656 2010
[20] R Ducrocq M Benkerrou L Brahimi et al ldquoNeonatal screen-ing for sickle cell anemia evaluation of a five-year experience inan area of northern ParisrdquoArchives de Pediatrie vol 8 no 5 pp474ndash480 2001
[21] M Manu Pereira and J Vives Corrons ldquoNeonatal haemo-globinopathy screening in Spainrdquo Journal of Clinical Pathologyvol 62 no 1 pp 22ndash25 2009
[22] C Saint-Martin M Romana A Bibrac et al ldquoUniversalnewborn screening for haemoglobinopathies in Guadeloupe(French West Indies) a 27-year experiencerdquo Journal of MedicalScreening vol 20 no 4 pp 177ndash182 2013
[23] C L Lobo S K Ballas A C Domingos P G Moura E M doNascimento and G P Cardoso ldquoNewborn screening programfor hemoglobinopathies in Rio de Janeiro Brazilrdquo PediatricBlood and Cancer vol 61 no 1 pp 34ndash39 2014
[24] P T McGann M G Ferris U Ramamurthy et al ldquoA prospec-tive newborn screening and treatment program for sickle cellanemia in Luanda Angolardquo The American Journal of Hematol-ogy vol 88 no 12 pp 984ndash989 2013
[25] J Patel and G R Serjeant ldquoNewborn screening for sickle celldisease in India the need for defining optimal clinical carerdquoIndian Journal of Pediatrics vol 81 no 3 pp 229ndash230 2014
[26] S Hajer T Neila H F Sondess et al ldquoA lower-cost protocolfor sickle cell disease neonatal screening in Tunisiardquo Annals ofSaudi Medicine vol 32 no 1 pp 49ndash52 2012
[27] V S Hertzberg C F Hinton B L Therrell and S K ShapiraldquoBirth prevalence rates of newborn screening disorders inrelation to screening practices in the United Statesrdquo Journal ofPediatrics vol 159 no 4 pp 555ndash560 2011
[28] M C Rahimy A Gangbo G Ahouignan and E AlihonouldquoNewborn screening for sickle cell disease in the Republic ofBeninrdquo Journal of Clinical Pathology vol 62 no 1 pp 46ndash482009
[29] E Kafando E Nacoulma Y Ouattara et al ldquoNeonatal haemo-globinopathy screening in Burkina Fasordquo Journal of ClinicalPathology vol 62 no 1 pp 39ndash41 2009
[30] L Tshilolo L M Aissi D Lukusa et al ldquoNeonatal screening forsickle cell anaemia in the Democratic Republic of the Congoexperience from a pioneer project on 31 204 newbornsrdquo Journalof Clinical Pathology vol 62 no 1 pp 35ndash38 2009
[31] B J Bain ldquoHaemoglobinopathy diagnosis algorithms lessonsand pitfallsrdquo Blood Reviews vol 25 no 5 pp 205ndash213 2011
[32] K Ryan B J Bain D Worthington et al ldquoSignificant haemo-globinopathies guidelines for screening and diagnosisrdquo BritishJournal of Haematology vol 149 no 1 pp 35ndash49 2010
[33] J Riou C Godart D Hurtrel et al ldquoCation-exchange HPLCevaluated for presumptive identification of hemoglobin vari-antsrdquo Clinical Chemistry vol 43 no 1 pp 34ndash39 1997
[34] G RenomCMereau PMaboudou and J-M Perini ldquoPotentialof the Sebia Capillarys neonat fast automated system forneonatal screening of sickle cell diseaserdquoClinical Chemistry andLaboratory Medicine vol 47 no 11 pp 1423ndash1432 2009
[35] M Campbell J S Henthorn and S C Davies ldquoEvaluation ofcation-exchange HPLC compared with isoelectric focusing forneonatal hemoglobinopathy screeningrdquoClinical Chemistry vol45 no 7 pp 969ndash975 1999
[36] E Mantikou C L Harteveld and P C Giordano ldquoNewbornscreening for hemoglobinopathies using capillary electrophore-sis technology testing the Capillarys Neonat Fast Hb devicerdquoClinical Biochemistry vol 43 no 16-17 pp 1345ndash1350 2010
10 BioMed Research International
[37] F Kutlar ldquoDiagnostic approach to hemoglobinopathiesrdquoHemoglobin vol 31 no 2 pp 243ndash250 2007
[38] G Bundesausschuss Anlage 2 Erweitertes Neugeborenen-screening 2010 httpwwwg-badedownloads83-691-233RL Kinder Anlage-2 2010-12-16pdf
[39] A Andermann I Blancquaert S Beauchamp and I CostealdquoGuiding policy decisions for genetic screening developing asystematic and transparent approachrdquo Public Health Genomicsvol 14 no 1 pp 9ndash16 2010
[40] A Andermann I Blancquaert S Beauchamp and V DeryldquoRevisiting Wilson and Jungner in the genomic age a review ofscreening criteria over the past 40 yearsrdquo Bulletin of the WorldHealth Organization vol 86 no 4 pp 317ndash319 2008
[41] S Lobitz C Frommel A Brose J Klein and O BlankensteinldquoIncidence of sickle cell disease in an unselected cohort ofneonates born in Berlin Germanyrdquo European Journal of HumanGenetics 2014
[42] P D Roa E A Turner and M D P Aguinaga ldquoHemoglobinvariant detection from dried blood specimens by high perfor-mance liquid chromatographyrdquo Annals of Clinical and Labora-tory Science vol 23 no 6 pp 433ndash438 1993
[43] CMurray S KHall andPGriffiths ldquoAn evaluation of the Sebiacapillarys Neonat Haemoglobin FASTŮ system for routinenewborn screening for sickle cell diseaserdquo International Journalof Laboratory Hematology vol 33 no 5 pp 533ndash539 2011
[44] A F S B Brandenburg ldquoStatistisches Jahrbuch 2011rdquo 2011httpswwwstatistik-berlin-brandenburgdeprodukteJahrbuchjb2011JB 2011 BEpdf
[45] E Harms and B Olgemoller ldquoNeonatal screening for metabolicand endocrine disordersrdquo Deutsches Arzteblatt Internationalvol 108 no 1-2 pp 11ndash22 2011
[46] A Joutovsky J Hadzi-Nesic andM A Nardi ldquoHPLC retentiontime as a diagnostic tool for hemoglobin variants and hemo-globinopathies a study of 60 000 samples in a clinical diagnosticlaboratoryrdquo Clinical Chemistry vol 50 no 10 pp 1736ndash17472004
[47] E Kohne and E Kleihauer ldquoHemoglobinopathies in Ger-manymdasha longitudinal study over four decadesrdquo DeutschesArzteblatt vol 107 no 5 pp 65ndash71 2010
[48] R Dickerhoff O Genzel-Boroviczeny and E Kohne ldquoHaemo-globinopathies and newborn haemoglobinopathy screening inGermanyrdquo Journal of Clinical Pathology vol 62 no 1 article 342009
[49] Enactment of the German Federal Parliament (Bundestag)ldquoHuman Genetic Examination Act (Genetic Diagnosis Act-GenDG)rdquo 2009 httpswwweshgorgfileadminwwweshgorgdocumentsEuropeLegalWSGermany GenDG Law GermanEnglishpdf
[50] J M Wilson and Y G Jungner Principles and Practice of MassScreening for Disease WHO Public Health Papers 1968
[51] Gendiagnostik-Kommission ldquoRichtlinien der Gendiagnostik-Komission (GEKO) fur die Anforderung an die Durchfuhrunggenetischer Reihenuntersuchungen gemaszlig sect23 Abs 2 Nr 6GenDGrdquo Bundesgesundheitsblatt vol 56 pp 321ndash324 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 BioMed Research International
the target disease The large majority of the subjects screenedare completely healthy This raises particular ethical legaltechnical and economic issues
The German Genetic Testing Act (GenDG) came intoforce on January 2 2010 and is a constant topic of debate onaccount of its very strict regulations [49] It controls genetictesting in humans and the use of genetic samples and dataThe GenDG specifies interalia that analyses of the productsof nucleic acids (gene product analyses) are also consideredgenetic analyses and therefore deemed legally equal to exam-ination of the number and structure of the chromosomes andof themolecular structure of DNA and RNAThismeans thathemoglobinopathy testing using protein separation methodssuch as HPLC or CE comes under the GenDG
Theultimate goal of theGenDG is to prevent the potentialdangers and discrimination associated with the examina-tion of human genetic traits One of the most importantprinciples is the right of the individual to informationalself-determination This right which enjoys internationallyunique protection in Germany includes the right to knowand more important in this context the right not to knowIts most important implication is that we are not allowed inGermany to report sickle cell trait
The GenDG distinguishes between genetic tests per-formed in amedical context and tests performed in a researchcontext and only applies to tests ordered in amedical contextA distinction is also made between diagnostic tests andpredictive tests In addition the GenDG regulates geneticscreening which would include NBS for SCD German lawrequires the establishment of an independent interdisci-plinary Genetic Testing Commission (GEKO) which hasbeen set up at the Robert Koch Institute and amongst otherthings lays down the requirements for the performance ofgenetic screening tests [49]These requirements are based onthe specific criteria for genetic screening developed byAnder-mann et al on the basis of theWHO screening criteria ofWil-son and Jungner [39 50]The GEKO has expressly stated thatresults of studies performed in other countries with differenthealthcare systems and different population structures can-not necessarily be extrapolated toGermany [51] For examplesome screening criteria are based on local conditions whichdo not obtain in Germany or at least not in all parts of thecountry Sickle cell patients cannot in particular be offeredstate-of-the-art care everywhere in Germany Nonmalignanthematology has been almost entirely neglected in the trainingof all groups of healthcare professionals in the past and thehemoglobinopathies as a whole are still not seen as a problemin Germany However a national strategy for preventionand treatment of SCD is currently under development TheSociety for Pediatric Oncology and Hematology (GPOH)has commissioned the establishment of a patient registerreference centers and a treatment guidelineThis is importantbecause if it is to make any sense a newborn screeningprogram requires not only the identification of sick babies butalso a functioning infrastructure which ensures that affectedchildren also receive appropriate care after the diagnosisThis includes both medical and psychosocial care as wellas sufficient counseling resources for the patients and theirparents
5 Conclusions
Our pilot project shows that itmakes sense at least regionallyto think about the introduction of some kind ofNBS programfor SCD in Germany whatever specific form this takesThe pilot projects necessary for this must be embarked onnow In addition to the presumed high-prevalence regionssuch as Berlin Hamburg the Ruhr region or Frankfurtepidemiological data should also be collected from pre-sumed low-prevalence regions (eg rural Bavaria and Baden-Wurttemberg)
Our data show that the organization and realization ofsuch pilot projects is relatively unproblematic and inexpen-sive as samples can be collected over several months and thenanalyzed together However we recommend that the samplesshould not be older than three months at the time of analysisIt is of fundamental importance that the Genetic Testing Actdoes not apply to such pilot projects as they involve genetictesting in the context of research
Conflict of Interests
Stephan Lobitz Claudia Frommel and Oliver Blankensteinreceived a research grant from Novartis Oncology GmbH(Nuremberg Germany) to perform this study In additionBio-Rad Laboratories GmbH (Munich Germany) indirectlyfunded this project through a preferential price for HPLCconsumables Beyond that the authors declare no competinginterest
Acknowledgments
This work is part of Stephan Lobitzrsquos dissertation in theUniversity College London ldquoMaster of Science in Haemoglo-binopathyrdquo program Stephan Lobitz is deeply indebted toDr Ratna Chatterjee Dr Rekha Bajoria the ThalassaemiaInternational Federation (TIF) and ldquoKINDerLEBEN-Vereinzur Forderung der Klinik fur krebskranke Kinder eV BerlinrdquoThe authors thank Novartis Oncology GmbH and Bio-RadLaboratories GmbH who generously funded this projectMany thanks are due to all parents and patients who took partin this study
References
[1] D C Rees T N Williams and M T Gladwin ldquoSickle-celldiseaserdquoThe Lancet vol 376 no 9757 pp 2018ndash2031 2010
[2] D Powars G Overturf J Weiss S Lee and L Chan ldquoPneumo-coccal septicemia in children with sickle cell anemia Changingtrend of survivalrdquo Journal of the American Medical Associationvol 245 no 18 pp 1839ndash1842 1981
[3] A M Emond R Collis D Darvill D R Higgs G H Maudeand G R Serjeant ldquoAcute splenic sequestration in homozygoussickle cell disease natural history and managementrdquo The Jour-nal of Pediatrics vol 107 no 2 pp 201ndash206 1985
[4] M H Gaston J I Verter G Woods et al ldquoProphylaxis withoral penicillin in children with sickle cell anemia a randomizedtrialrdquoThe New England Journal of Medicine vol 314 no 25 pp1593ndash1599 1986
BioMed Research International 9
[5] G R Serjeant and B E Serjeant ldquoManagement of sickle celldisease lessons from the Jamaican cohort studyrdquo Blood Reviewsvol 7 no 3 pp 137ndash145 1993
[6] A Lee P Thomas L Cupidore B Serjeant and G SerjeantldquoImproved survival in homozygous sickle cell disease lessonsfrom a cohort studyrdquo British Medical Journal vol 311 no 7020pp 1600ndash1602 1995
[7] T V Adamkiewicz S Sarnaik G R Buchanan et al ldquoInvasivepneumococcal infections in children with sickle cell diseasein the era of penicillin prophylaxis antibiotic resistance and23-valent pneumococcal polysaccharide vaccinationrdquo Journal ofPediatrics vol 143 no 4 pp 438ndash444 2003
[8] N B Halasa S M Shankar T R Talbot et al ldquoIncidence ofinvasive pneumococcal disease among individuals with sicklecell disease before and after the introduction of the pneumo-coccal conjugate vaccinerdquo Clinical Infectious Diseases vol 44no 11 pp 1428ndash1433 2007
[9] T V Adamkiewicz B J Silk J Howgate et al ldquoEffectiveness ofthe 7-valent pneumococcal conjugate vaccine in children withsickle cell disease in the first decade of liferdquo Pediatrics vol 121no 3 pp 562ndash569 2008
[10] S D Grosse H K Atrash I Odame D Amendah F B Pieland T N Williams ldquoThe Jamaican historical experience of theimpact of educational interventions on sickle cell disease childmortalityrdquoTheAmerican Journal of PreventiveMedicine vol 42no 6 pp e101ndashe103 2012
[11] H Heijboer X W van den Tweel M Peters M Knuist JPrins and H S Heymans ldquoOne year of neonatal screening forsickle cell disease in the emma kinderziekenhuisacademischmedisch centrum Amsterdamrdquo Nederlands Tijdschrift voorGeneeskunde vol 145 no 37 pp 1795ndash1799 2001
[12] B Gulbis F Cotton A Ferster et al ldquoNeonatal haemoglobin-opathy screening in Belgiumrdquo Journal of Clinical Pathology vol62 no 1 pp 49ndash52 2009
[13] A Streetly R Latinovic and J Henthorn ldquoPositive screeningand carrier results for the England-wide universal newbornsickle cell screening programme by ethnicity and area for 2005-07rdquo Journal of Clinical Pathology vol 63 no 7 pp 626ndash6292010
[14] E Ballardini A TaroccoMMarsella et al ldquoUniversal neonatalscreening for sickle cell disease and other haemoglobinopathiesin Ferrara Italyrdquo Blood Transfusion vol 11 no 2 pp 245ndash2492013
[15] J Bardakdjian-Michau M Bahuau D Hurtrel et al ldquoNeonatalscreening for sickle cell disease in Francerdquo Journal of ClinicalPathology vol 62 no 1 pp 31ndash33 2009
[16] E Cela De Julian E Dulın Iniguez M Guerrero Soler etal ldquoEvaluation of systematic neonatal screening for sickle celldiseases in Madrid three years after its introductionrdquo Anales dePediatria vol 66 no 4 pp 382ndash386 2007
[17] M J Bouva K Mohrmann H B J M Brinkman et alldquoImplementing neonatal screening for haemoglobinopathies inthe Netherlandsrdquo Journal of Medical Screening vol 17 no 2 pp58ndash65 2010
[18] P C GiordanoM J Bouva and C L Harteveld ldquoA confidentialinquiry estimating the number of patients affected with sicklecell disease and thalassemia major confirms the need for aprevention strategy in theNetherlandsrdquoHemoglobin vol 28 no4 pp 287ndash296 2004
[19] S Berthet F Monpoux A-M Soummer E Berard J Sarlesand C Badens ldquoNeonatal screening for sickle cell disease in
Nice University Hospital review of 8 last yearsrdquo Archives dePediatrie vol 17 no 12 pp 1652ndash1656 2010
[20] R Ducrocq M Benkerrou L Brahimi et al ldquoNeonatal screen-ing for sickle cell anemia evaluation of a five-year experience inan area of northern ParisrdquoArchives de Pediatrie vol 8 no 5 pp474ndash480 2001
[21] M Manu Pereira and J Vives Corrons ldquoNeonatal haemo-globinopathy screening in Spainrdquo Journal of Clinical Pathologyvol 62 no 1 pp 22ndash25 2009
[22] C Saint-Martin M Romana A Bibrac et al ldquoUniversalnewborn screening for haemoglobinopathies in Guadeloupe(French West Indies) a 27-year experiencerdquo Journal of MedicalScreening vol 20 no 4 pp 177ndash182 2013
[23] C L Lobo S K Ballas A C Domingos P G Moura E M doNascimento and G P Cardoso ldquoNewborn screening programfor hemoglobinopathies in Rio de Janeiro Brazilrdquo PediatricBlood and Cancer vol 61 no 1 pp 34ndash39 2014
[24] P T McGann M G Ferris U Ramamurthy et al ldquoA prospec-tive newborn screening and treatment program for sickle cellanemia in Luanda Angolardquo The American Journal of Hematol-ogy vol 88 no 12 pp 984ndash989 2013
[25] J Patel and G R Serjeant ldquoNewborn screening for sickle celldisease in India the need for defining optimal clinical carerdquoIndian Journal of Pediatrics vol 81 no 3 pp 229ndash230 2014
[26] S Hajer T Neila H F Sondess et al ldquoA lower-cost protocolfor sickle cell disease neonatal screening in Tunisiardquo Annals ofSaudi Medicine vol 32 no 1 pp 49ndash52 2012
[27] V S Hertzberg C F Hinton B L Therrell and S K ShapiraldquoBirth prevalence rates of newborn screening disorders inrelation to screening practices in the United Statesrdquo Journal ofPediatrics vol 159 no 4 pp 555ndash560 2011
[28] M C Rahimy A Gangbo G Ahouignan and E AlihonouldquoNewborn screening for sickle cell disease in the Republic ofBeninrdquo Journal of Clinical Pathology vol 62 no 1 pp 46ndash482009
[29] E Kafando E Nacoulma Y Ouattara et al ldquoNeonatal haemo-globinopathy screening in Burkina Fasordquo Journal of ClinicalPathology vol 62 no 1 pp 39ndash41 2009
[30] L Tshilolo L M Aissi D Lukusa et al ldquoNeonatal screening forsickle cell anaemia in the Democratic Republic of the Congoexperience from a pioneer project on 31 204 newbornsrdquo Journalof Clinical Pathology vol 62 no 1 pp 35ndash38 2009
[31] B J Bain ldquoHaemoglobinopathy diagnosis algorithms lessonsand pitfallsrdquo Blood Reviews vol 25 no 5 pp 205ndash213 2011
[32] K Ryan B J Bain D Worthington et al ldquoSignificant haemo-globinopathies guidelines for screening and diagnosisrdquo BritishJournal of Haematology vol 149 no 1 pp 35ndash49 2010
[33] J Riou C Godart D Hurtrel et al ldquoCation-exchange HPLCevaluated for presumptive identification of hemoglobin vari-antsrdquo Clinical Chemistry vol 43 no 1 pp 34ndash39 1997
[34] G RenomCMereau PMaboudou and J-M Perini ldquoPotentialof the Sebia Capillarys neonat fast automated system forneonatal screening of sickle cell diseaserdquoClinical Chemistry andLaboratory Medicine vol 47 no 11 pp 1423ndash1432 2009
[35] M Campbell J S Henthorn and S C Davies ldquoEvaluation ofcation-exchange HPLC compared with isoelectric focusing forneonatal hemoglobinopathy screeningrdquoClinical Chemistry vol45 no 7 pp 969ndash975 1999
[36] E Mantikou C L Harteveld and P C Giordano ldquoNewbornscreening for hemoglobinopathies using capillary electrophore-sis technology testing the Capillarys Neonat Fast Hb devicerdquoClinical Biochemistry vol 43 no 16-17 pp 1345ndash1350 2010
10 BioMed Research International
[37] F Kutlar ldquoDiagnostic approach to hemoglobinopathiesrdquoHemoglobin vol 31 no 2 pp 243ndash250 2007
[38] G Bundesausschuss Anlage 2 Erweitertes Neugeborenen-screening 2010 httpwwwg-badedownloads83-691-233RL Kinder Anlage-2 2010-12-16pdf
[39] A Andermann I Blancquaert S Beauchamp and I CostealdquoGuiding policy decisions for genetic screening developing asystematic and transparent approachrdquo Public Health Genomicsvol 14 no 1 pp 9ndash16 2010
[40] A Andermann I Blancquaert S Beauchamp and V DeryldquoRevisiting Wilson and Jungner in the genomic age a review ofscreening criteria over the past 40 yearsrdquo Bulletin of the WorldHealth Organization vol 86 no 4 pp 317ndash319 2008
[41] S Lobitz C Frommel A Brose J Klein and O BlankensteinldquoIncidence of sickle cell disease in an unselected cohort ofneonates born in Berlin Germanyrdquo European Journal of HumanGenetics 2014
[42] P D Roa E A Turner and M D P Aguinaga ldquoHemoglobinvariant detection from dried blood specimens by high perfor-mance liquid chromatographyrdquo Annals of Clinical and Labora-tory Science vol 23 no 6 pp 433ndash438 1993
[43] CMurray S KHall andPGriffiths ldquoAn evaluation of the Sebiacapillarys Neonat Haemoglobin FASTŮ system for routinenewborn screening for sickle cell diseaserdquo International Journalof Laboratory Hematology vol 33 no 5 pp 533ndash539 2011
[44] A F S B Brandenburg ldquoStatistisches Jahrbuch 2011rdquo 2011httpswwwstatistik-berlin-brandenburgdeprodukteJahrbuchjb2011JB 2011 BEpdf
[45] E Harms and B Olgemoller ldquoNeonatal screening for metabolicand endocrine disordersrdquo Deutsches Arzteblatt Internationalvol 108 no 1-2 pp 11ndash22 2011
[46] A Joutovsky J Hadzi-Nesic andM A Nardi ldquoHPLC retentiontime as a diagnostic tool for hemoglobin variants and hemo-globinopathies a study of 60 000 samples in a clinical diagnosticlaboratoryrdquo Clinical Chemistry vol 50 no 10 pp 1736ndash17472004
[47] E Kohne and E Kleihauer ldquoHemoglobinopathies in Ger-manymdasha longitudinal study over four decadesrdquo DeutschesArzteblatt vol 107 no 5 pp 65ndash71 2010
[48] R Dickerhoff O Genzel-Boroviczeny and E Kohne ldquoHaemo-globinopathies and newborn haemoglobinopathy screening inGermanyrdquo Journal of Clinical Pathology vol 62 no 1 article 342009
[49] Enactment of the German Federal Parliament (Bundestag)ldquoHuman Genetic Examination Act (Genetic Diagnosis Act-GenDG)rdquo 2009 httpswwweshgorgfileadminwwweshgorgdocumentsEuropeLegalWSGermany GenDG Law GermanEnglishpdf
[50] J M Wilson and Y G Jungner Principles and Practice of MassScreening for Disease WHO Public Health Papers 1968
[51] Gendiagnostik-Kommission ldquoRichtlinien der Gendiagnostik-Komission (GEKO) fur die Anforderung an die Durchfuhrunggenetischer Reihenuntersuchungen gemaszlig sect23 Abs 2 Nr 6GenDGrdquo Bundesgesundheitsblatt vol 56 pp 321ndash324 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 9
[5] G R Serjeant and B E Serjeant ldquoManagement of sickle celldisease lessons from the Jamaican cohort studyrdquo Blood Reviewsvol 7 no 3 pp 137ndash145 1993
[6] A Lee P Thomas L Cupidore B Serjeant and G SerjeantldquoImproved survival in homozygous sickle cell disease lessonsfrom a cohort studyrdquo British Medical Journal vol 311 no 7020pp 1600ndash1602 1995
[7] T V Adamkiewicz S Sarnaik G R Buchanan et al ldquoInvasivepneumococcal infections in children with sickle cell diseasein the era of penicillin prophylaxis antibiotic resistance and23-valent pneumococcal polysaccharide vaccinationrdquo Journal ofPediatrics vol 143 no 4 pp 438ndash444 2003
[8] N B Halasa S M Shankar T R Talbot et al ldquoIncidence ofinvasive pneumococcal disease among individuals with sicklecell disease before and after the introduction of the pneumo-coccal conjugate vaccinerdquo Clinical Infectious Diseases vol 44no 11 pp 1428ndash1433 2007
[9] T V Adamkiewicz B J Silk J Howgate et al ldquoEffectiveness ofthe 7-valent pneumococcal conjugate vaccine in children withsickle cell disease in the first decade of liferdquo Pediatrics vol 121no 3 pp 562ndash569 2008
[10] S D Grosse H K Atrash I Odame D Amendah F B Pieland T N Williams ldquoThe Jamaican historical experience of theimpact of educational interventions on sickle cell disease childmortalityrdquoTheAmerican Journal of PreventiveMedicine vol 42no 6 pp e101ndashe103 2012
[11] H Heijboer X W van den Tweel M Peters M Knuist JPrins and H S Heymans ldquoOne year of neonatal screening forsickle cell disease in the emma kinderziekenhuisacademischmedisch centrum Amsterdamrdquo Nederlands Tijdschrift voorGeneeskunde vol 145 no 37 pp 1795ndash1799 2001
[12] B Gulbis F Cotton A Ferster et al ldquoNeonatal haemoglobin-opathy screening in Belgiumrdquo Journal of Clinical Pathology vol62 no 1 pp 49ndash52 2009
[13] A Streetly R Latinovic and J Henthorn ldquoPositive screeningand carrier results for the England-wide universal newbornsickle cell screening programme by ethnicity and area for 2005-07rdquo Journal of Clinical Pathology vol 63 no 7 pp 626ndash6292010
[14] E Ballardini A TaroccoMMarsella et al ldquoUniversal neonatalscreening for sickle cell disease and other haemoglobinopathiesin Ferrara Italyrdquo Blood Transfusion vol 11 no 2 pp 245ndash2492013
[15] J Bardakdjian-Michau M Bahuau D Hurtrel et al ldquoNeonatalscreening for sickle cell disease in Francerdquo Journal of ClinicalPathology vol 62 no 1 pp 31ndash33 2009
[16] E Cela De Julian E Dulın Iniguez M Guerrero Soler etal ldquoEvaluation of systematic neonatal screening for sickle celldiseases in Madrid three years after its introductionrdquo Anales dePediatria vol 66 no 4 pp 382ndash386 2007
[17] M J Bouva K Mohrmann H B J M Brinkman et alldquoImplementing neonatal screening for haemoglobinopathies inthe Netherlandsrdquo Journal of Medical Screening vol 17 no 2 pp58ndash65 2010
[18] P C GiordanoM J Bouva and C L Harteveld ldquoA confidentialinquiry estimating the number of patients affected with sicklecell disease and thalassemia major confirms the need for aprevention strategy in theNetherlandsrdquoHemoglobin vol 28 no4 pp 287ndash296 2004
[19] S Berthet F Monpoux A-M Soummer E Berard J Sarlesand C Badens ldquoNeonatal screening for sickle cell disease in
Nice University Hospital review of 8 last yearsrdquo Archives dePediatrie vol 17 no 12 pp 1652ndash1656 2010
[20] R Ducrocq M Benkerrou L Brahimi et al ldquoNeonatal screen-ing for sickle cell anemia evaluation of a five-year experience inan area of northern ParisrdquoArchives de Pediatrie vol 8 no 5 pp474ndash480 2001
[21] M Manu Pereira and J Vives Corrons ldquoNeonatal haemo-globinopathy screening in Spainrdquo Journal of Clinical Pathologyvol 62 no 1 pp 22ndash25 2009
[22] C Saint-Martin M Romana A Bibrac et al ldquoUniversalnewborn screening for haemoglobinopathies in Guadeloupe(French West Indies) a 27-year experiencerdquo Journal of MedicalScreening vol 20 no 4 pp 177ndash182 2013
[23] C L Lobo S K Ballas A C Domingos P G Moura E M doNascimento and G P Cardoso ldquoNewborn screening programfor hemoglobinopathies in Rio de Janeiro Brazilrdquo PediatricBlood and Cancer vol 61 no 1 pp 34ndash39 2014
[24] P T McGann M G Ferris U Ramamurthy et al ldquoA prospec-tive newborn screening and treatment program for sickle cellanemia in Luanda Angolardquo The American Journal of Hematol-ogy vol 88 no 12 pp 984ndash989 2013
[25] J Patel and G R Serjeant ldquoNewborn screening for sickle celldisease in India the need for defining optimal clinical carerdquoIndian Journal of Pediatrics vol 81 no 3 pp 229ndash230 2014
[26] S Hajer T Neila H F Sondess et al ldquoA lower-cost protocolfor sickle cell disease neonatal screening in Tunisiardquo Annals ofSaudi Medicine vol 32 no 1 pp 49ndash52 2012
[27] V S Hertzberg C F Hinton B L Therrell and S K ShapiraldquoBirth prevalence rates of newborn screening disorders inrelation to screening practices in the United Statesrdquo Journal ofPediatrics vol 159 no 4 pp 555ndash560 2011
[28] M C Rahimy A Gangbo G Ahouignan and E AlihonouldquoNewborn screening for sickle cell disease in the Republic ofBeninrdquo Journal of Clinical Pathology vol 62 no 1 pp 46ndash482009
[29] E Kafando E Nacoulma Y Ouattara et al ldquoNeonatal haemo-globinopathy screening in Burkina Fasordquo Journal of ClinicalPathology vol 62 no 1 pp 39ndash41 2009
[30] L Tshilolo L M Aissi D Lukusa et al ldquoNeonatal screening forsickle cell anaemia in the Democratic Republic of the Congoexperience from a pioneer project on 31 204 newbornsrdquo Journalof Clinical Pathology vol 62 no 1 pp 35ndash38 2009
[31] B J Bain ldquoHaemoglobinopathy diagnosis algorithms lessonsand pitfallsrdquo Blood Reviews vol 25 no 5 pp 205ndash213 2011
[32] K Ryan B J Bain D Worthington et al ldquoSignificant haemo-globinopathies guidelines for screening and diagnosisrdquo BritishJournal of Haematology vol 149 no 1 pp 35ndash49 2010
[33] J Riou C Godart D Hurtrel et al ldquoCation-exchange HPLCevaluated for presumptive identification of hemoglobin vari-antsrdquo Clinical Chemistry vol 43 no 1 pp 34ndash39 1997
[34] G RenomCMereau PMaboudou and J-M Perini ldquoPotentialof the Sebia Capillarys neonat fast automated system forneonatal screening of sickle cell diseaserdquoClinical Chemistry andLaboratory Medicine vol 47 no 11 pp 1423ndash1432 2009
[35] M Campbell J S Henthorn and S C Davies ldquoEvaluation ofcation-exchange HPLC compared with isoelectric focusing forneonatal hemoglobinopathy screeningrdquoClinical Chemistry vol45 no 7 pp 969ndash975 1999
[36] E Mantikou C L Harteveld and P C Giordano ldquoNewbornscreening for hemoglobinopathies using capillary electrophore-sis technology testing the Capillarys Neonat Fast Hb devicerdquoClinical Biochemistry vol 43 no 16-17 pp 1345ndash1350 2010
10 BioMed Research International
[37] F Kutlar ldquoDiagnostic approach to hemoglobinopathiesrdquoHemoglobin vol 31 no 2 pp 243ndash250 2007
[38] G Bundesausschuss Anlage 2 Erweitertes Neugeborenen-screening 2010 httpwwwg-badedownloads83-691-233RL Kinder Anlage-2 2010-12-16pdf
[39] A Andermann I Blancquaert S Beauchamp and I CostealdquoGuiding policy decisions for genetic screening developing asystematic and transparent approachrdquo Public Health Genomicsvol 14 no 1 pp 9ndash16 2010
[40] A Andermann I Blancquaert S Beauchamp and V DeryldquoRevisiting Wilson and Jungner in the genomic age a review ofscreening criteria over the past 40 yearsrdquo Bulletin of the WorldHealth Organization vol 86 no 4 pp 317ndash319 2008
[41] S Lobitz C Frommel A Brose J Klein and O BlankensteinldquoIncidence of sickle cell disease in an unselected cohort ofneonates born in Berlin Germanyrdquo European Journal of HumanGenetics 2014
[42] P D Roa E A Turner and M D P Aguinaga ldquoHemoglobinvariant detection from dried blood specimens by high perfor-mance liquid chromatographyrdquo Annals of Clinical and Labora-tory Science vol 23 no 6 pp 433ndash438 1993
[43] CMurray S KHall andPGriffiths ldquoAn evaluation of the Sebiacapillarys Neonat Haemoglobin FASTŮ system for routinenewborn screening for sickle cell diseaserdquo International Journalof Laboratory Hematology vol 33 no 5 pp 533ndash539 2011
[44] A F S B Brandenburg ldquoStatistisches Jahrbuch 2011rdquo 2011httpswwwstatistik-berlin-brandenburgdeprodukteJahrbuchjb2011JB 2011 BEpdf
[45] E Harms and B Olgemoller ldquoNeonatal screening for metabolicand endocrine disordersrdquo Deutsches Arzteblatt Internationalvol 108 no 1-2 pp 11ndash22 2011
[46] A Joutovsky J Hadzi-Nesic andM A Nardi ldquoHPLC retentiontime as a diagnostic tool for hemoglobin variants and hemo-globinopathies a study of 60 000 samples in a clinical diagnosticlaboratoryrdquo Clinical Chemistry vol 50 no 10 pp 1736ndash17472004
[47] E Kohne and E Kleihauer ldquoHemoglobinopathies in Ger-manymdasha longitudinal study over four decadesrdquo DeutschesArzteblatt vol 107 no 5 pp 65ndash71 2010
[48] R Dickerhoff O Genzel-Boroviczeny and E Kohne ldquoHaemo-globinopathies and newborn haemoglobinopathy screening inGermanyrdquo Journal of Clinical Pathology vol 62 no 1 article 342009
[49] Enactment of the German Federal Parliament (Bundestag)ldquoHuman Genetic Examination Act (Genetic Diagnosis Act-GenDG)rdquo 2009 httpswwweshgorgfileadminwwweshgorgdocumentsEuropeLegalWSGermany GenDG Law GermanEnglishpdf
[50] J M Wilson and Y G Jungner Principles and Practice of MassScreening for Disease WHO Public Health Papers 1968
[51] Gendiagnostik-Kommission ldquoRichtlinien der Gendiagnostik-Komission (GEKO) fur die Anforderung an die Durchfuhrunggenetischer Reihenuntersuchungen gemaszlig sect23 Abs 2 Nr 6GenDGrdquo Bundesgesundheitsblatt vol 56 pp 321ndash324 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

10 BioMed Research International
[37] F Kutlar ldquoDiagnostic approach to hemoglobinopathiesrdquoHemoglobin vol 31 no 2 pp 243ndash250 2007
[38] G Bundesausschuss Anlage 2 Erweitertes Neugeborenen-screening 2010 httpwwwg-badedownloads83-691-233RL Kinder Anlage-2 2010-12-16pdf
[39] A Andermann I Blancquaert S Beauchamp and I CostealdquoGuiding policy decisions for genetic screening developing asystematic and transparent approachrdquo Public Health Genomicsvol 14 no 1 pp 9ndash16 2010
[40] A Andermann I Blancquaert S Beauchamp and V DeryldquoRevisiting Wilson and Jungner in the genomic age a review ofscreening criteria over the past 40 yearsrdquo Bulletin of the WorldHealth Organization vol 86 no 4 pp 317ndash319 2008
[41] S Lobitz C Frommel A Brose J Klein and O BlankensteinldquoIncidence of sickle cell disease in an unselected cohort ofneonates born in Berlin Germanyrdquo European Journal of HumanGenetics 2014
[42] P D Roa E A Turner and M D P Aguinaga ldquoHemoglobinvariant detection from dried blood specimens by high perfor-mance liquid chromatographyrdquo Annals of Clinical and Labora-tory Science vol 23 no 6 pp 433ndash438 1993
[43] CMurray S KHall andPGriffiths ldquoAn evaluation of the Sebiacapillarys Neonat Haemoglobin FASTŮ system for routinenewborn screening for sickle cell diseaserdquo International Journalof Laboratory Hematology vol 33 no 5 pp 533ndash539 2011
[44] A F S B Brandenburg ldquoStatistisches Jahrbuch 2011rdquo 2011httpswwwstatistik-berlin-brandenburgdeprodukteJahrbuchjb2011JB 2011 BEpdf
[45] E Harms and B Olgemoller ldquoNeonatal screening for metabolicand endocrine disordersrdquo Deutsches Arzteblatt Internationalvol 108 no 1-2 pp 11ndash22 2011
[46] A Joutovsky J Hadzi-Nesic andM A Nardi ldquoHPLC retentiontime as a diagnostic tool for hemoglobin variants and hemo-globinopathies a study of 60 000 samples in a clinical diagnosticlaboratoryrdquo Clinical Chemistry vol 50 no 10 pp 1736ndash17472004
[47] E Kohne and E Kleihauer ldquoHemoglobinopathies in Ger-manymdasha longitudinal study over four decadesrdquo DeutschesArzteblatt vol 107 no 5 pp 65ndash71 2010
[48] R Dickerhoff O Genzel-Boroviczeny and E Kohne ldquoHaemo-globinopathies and newborn haemoglobinopathy screening inGermanyrdquo Journal of Clinical Pathology vol 62 no 1 article 342009
[49] Enactment of the German Federal Parliament (Bundestag)ldquoHuman Genetic Examination Act (Genetic Diagnosis Act-GenDG)rdquo 2009 httpswwweshgorgfileadminwwweshgorgdocumentsEuropeLegalWSGermany GenDG Law GermanEnglishpdf
[50] J M Wilson and Y G Jungner Principles and Practice of MassScreening for Disease WHO Public Health Papers 1968
[51] Gendiagnostik-Kommission ldquoRichtlinien der Gendiagnostik-Komission (GEKO) fur die Anforderung an die Durchfuhrunggenetischer Reihenuntersuchungen gemaszlig sect23 Abs 2 Nr 6GenDGrdquo Bundesgesundheitsblatt vol 56 pp 321ndash324 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom


![Prenatal Screening for Co-Inheritance of Sickle Cell ... · Sickle cell anemia and β-thalassemia are genetic disorders caused by different genetic mutations [11]. Therefore, patients](https://img.pdfslide.tips/doc/110x75/5f5a186f300c56026200ab34/prenatal-screening-for-co-inheritance-of-sickle-cell-sickle-cell-anemia-and.jpg)