Embed Size (px)
Citation preview

Santiago Ponce Aix
Hospital Universitario Doce de Octubre,
Madrid, Spain
CNMP AvanzadoEstrategias Terapéuticas
▪ Regímenes estándar
- antes y después de 1990s
- dobletes actuales
▪ Regímenes alternativos
- regímenes sin platino
- Cis vs Carbo
- tripletes
▪ Duración de la QT
▪ Terapia de Mantenimiento
▪ Edad avanzada / Mal PS
▪ Papel de la Inmunoterapia
▪ Segunda línea y posteriores
▪ “Oncogene driven” CNMP
CNMP Avanzado

▪ Regímenes estándar
- antes y después de 1990s
- dobletes actuales
▪ Regímenes alternativos
- regímenes sin platino
- Cis vs Carbo
- tripletes
▪ Duración de la QT
▪ Terapia de Mantenimiento
▪ Edad avanzada / Mal PS
▪ Papel de la Inmunoterapia
▪ Segunda línea y posteriores
▪ “Oncogene driven” CNMP
CNMP Avanzado
▪ Regimenes: EP, CDDP-Vds, MVP, MIC,...
▪ Incremento de supervivencia
- Mediana: 2 meses
- 1-año: 10%
- Disminución Hazard Rate: 26%
▪ Beneficio sintomático: 66%–78% pacientes
▪ Mejoría calidad de vida
▪ Costo-efectiva
QT basada en cisplatinoAntes de 1990
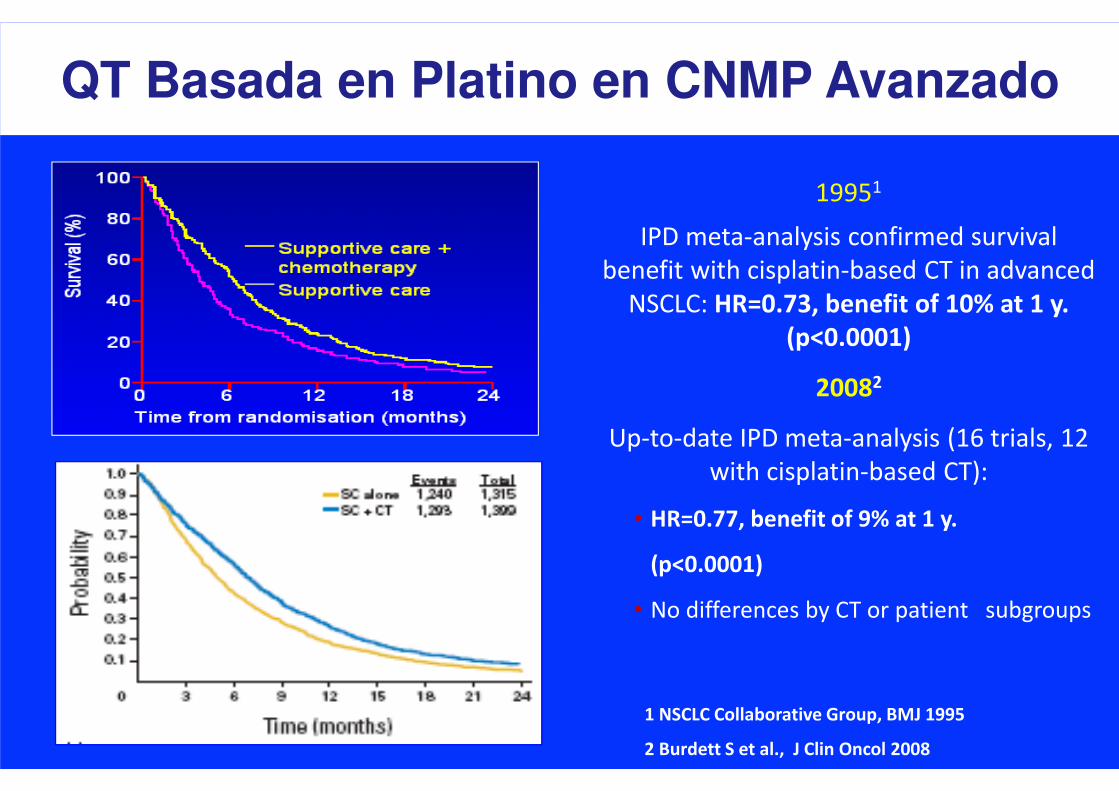
QT Basada en Platino en CNMP Avanzado
1 NSCLC Collaborative Group, BMJ 1995
2 Burdett S et al., J Clin Oncol 2008
IPD meta-analysis confirmed survival
benefit with cisplatin-based CT in advanced
NSCLC: HR=0.73, benefit of 10% at 1 y.
(p<0.0001)
20082
Up-to-date IPD meta-analysis (16 trials, 12
with cisplatin-based CT):
• HR=0.77, benefit of 9% at 1 y.
(p<0.0001)
• No differences by CT or patient subgroups
19951

“Nuevos” Citotóxicos (>1990)
▪ Docetaxel
▪ Paclitaxel
▪ Vinorelbina
▪ Gemcitabina
▪ Pemetrexed
▪ Irinotecan
▪ Agente único
- RR: 20-25%
▪ Dobletes con platino
-RR: 30-50%
-Superv.: 8-12 m

ECOG 1594 Trial - Supervivencia
Schiller J et al., NEJM 2002
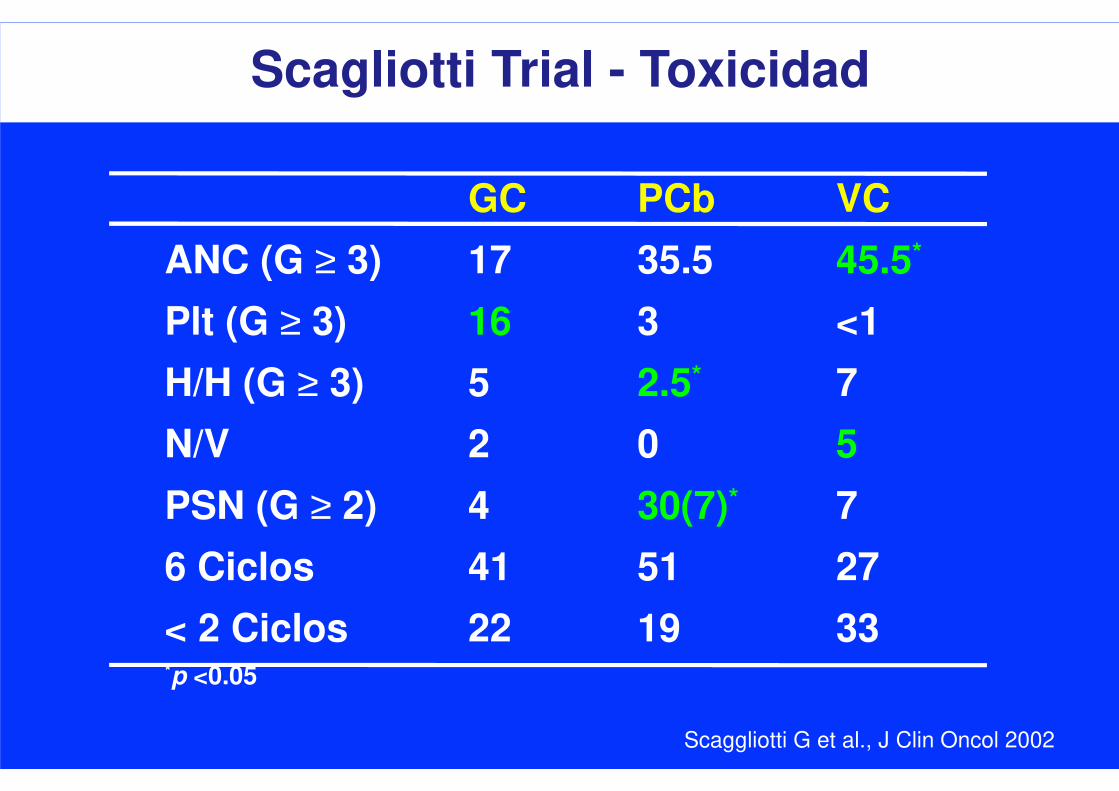
Scagliotti Trial - Toxicidad
GC PCb VC
ANC (G ≥ 3) 17 35.5 45.5*
Plt (G ≥ 3) 16 3 <1
H/H (G ≥ 3) 5 2.5* 7
N/V 2 0 5
PSN (G ≥ 2) 4 30(7)* 7
6 Ciclos 41 51 27
< 2 Ciclos 22 19 33*p <0.05
Scaggliotti G et al., J Clin Oncol 2002

▪ Dada la ausencia de diferencias clínicamente relevantes
en cuanto a eficacia, DEPENDE DE:
- Perfil de toxicidad
- Características del paciente (co-morbilidad, PS)
- Características del tumor ???
- Conveniencia (paciente, entorno sanitario)
- Costes (paciente, hospital, patentes)
- Experiencia
Regimen de elección
▪ Dada la ausencia de diferencias clínicamente relevantes
en cuanto a eficacia, DEPENDE DE:
- Perfil de toxicidad
- Características del paciente (co-morbilidad, PS)
- Características del tumor ???
- Conveniencia (paciente, entorno sanitario)
- Costes (paciente, hospital, patentes)
- Experiencia
Regimen de elección

Cis/Pem vs Cis/Gem en CNMP (1ª línea)
Scaggliotti G et al., J Clin Oncol 2008
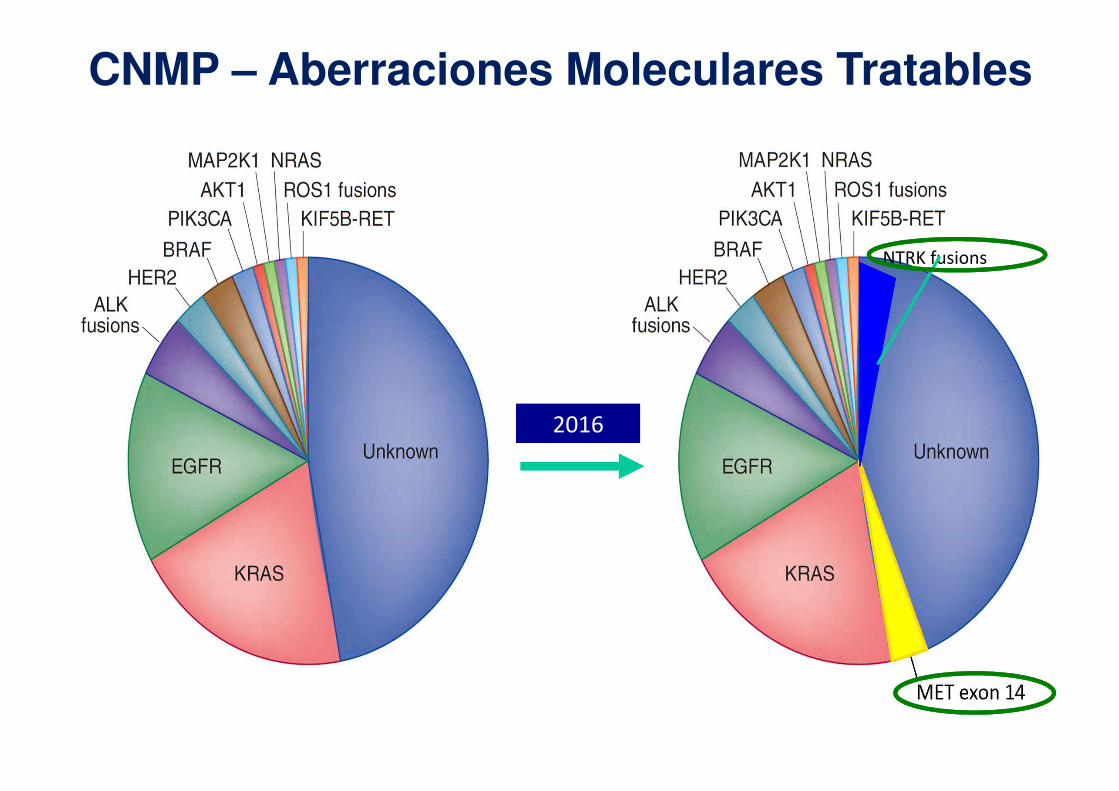
CNMP – Aberraciones Moleculares Tratables
NTRK fusions
2016
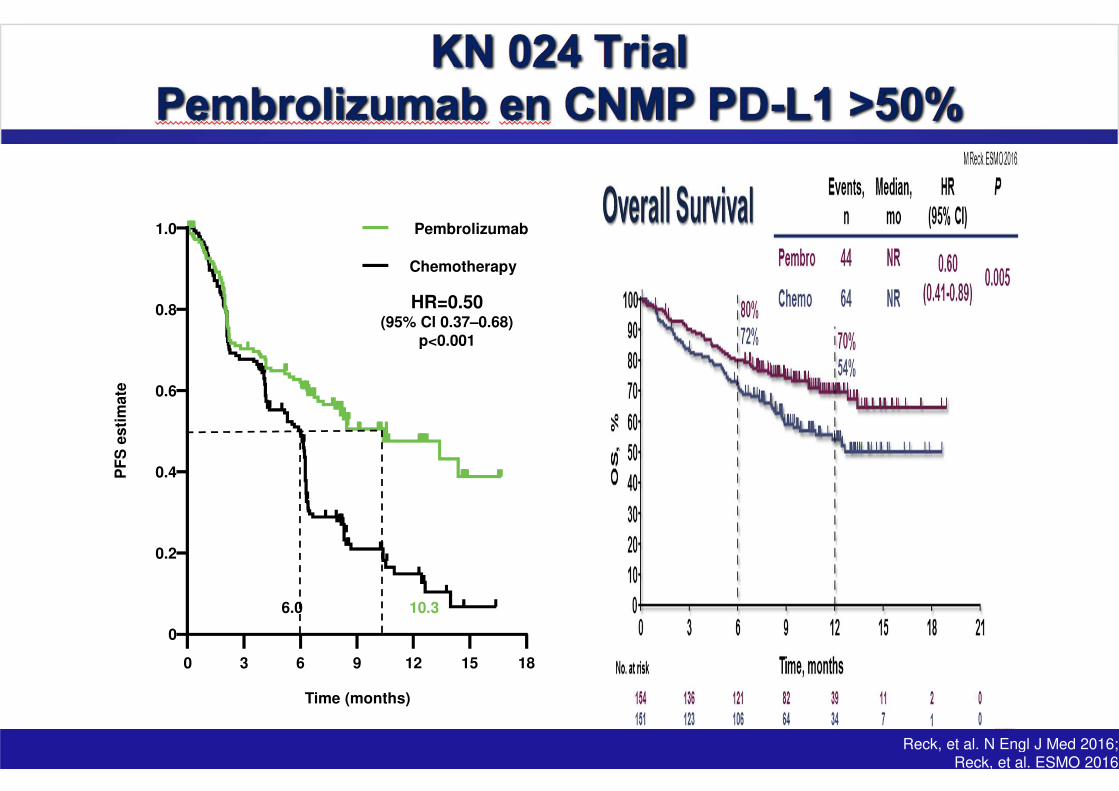
1.0
0.8
0.6
0.4
0.2
0
0
Time (months)
PF
S e
sti
mate
63 9 181512
Pembrolizumab
Chemotherapy
HR=0.50 (95% Cl 0.37–0.68)
p<0.001
CheckMate-026 PFS3
6.0 10.3
1. Reck, et al. N Engl J Med 2016; 2. Reck, et al. ESMO 2016; 3. Socinski, et al. ESMO 2016
Reck, et al. N Engl J Med 2016; Reck, et al. ESMO 2016
▪ Regímenes estándar
- antes y después de 1990s
- dobletes actuales
▪ Regímenes alternativos
- regímenes sin platino
- Cis vs Carbo
- tripletes
▪ Duración de la QT
▪ Terapia de Mantenimiento
▪ Edad avanzada / Mal PS
▪ Papel de la Inmunoterapia
▪ Segunda línea y posteriores
▪ “Oncogene driven” CNMP
CNMP Avanzado
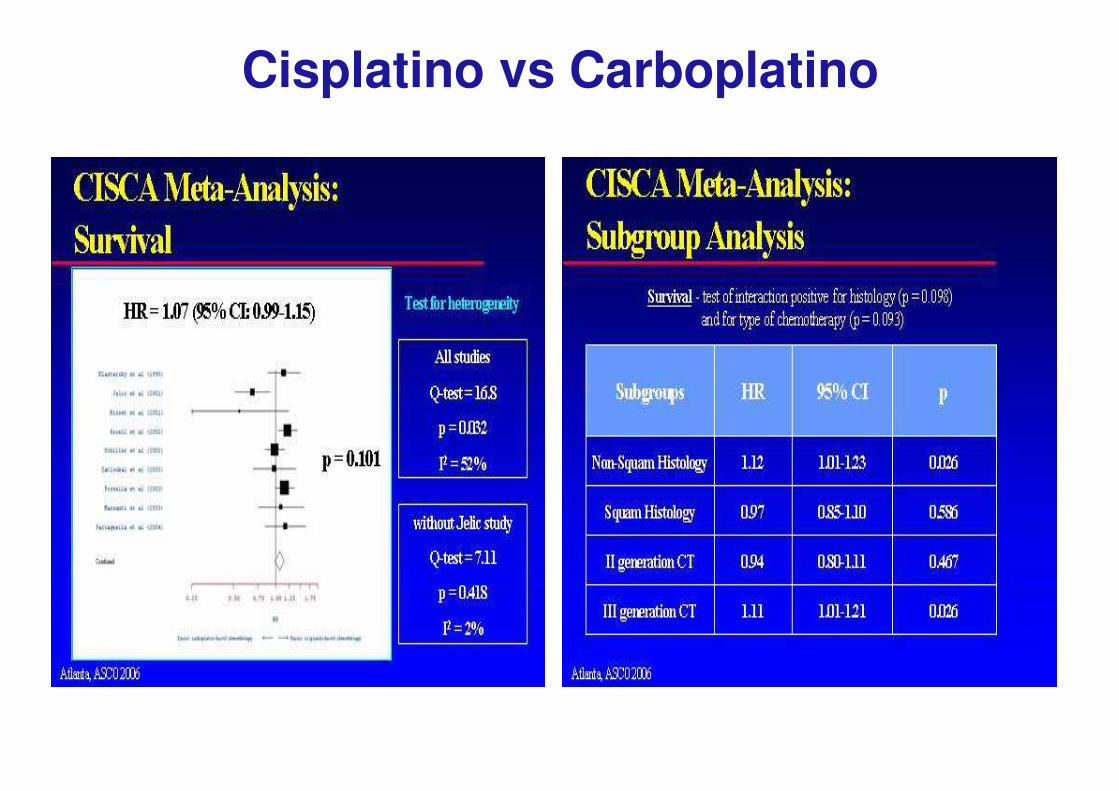
Cisplatino vs Carboplatino
Ardizzoni A et al., JNCI 2007

Comparison of 1-Yr Survival Between
Platinum Arms and Non-platinum Arms of All Identified Assessable
Trials (N = 6,504)
Platin Non-Platin
1 Yr survival
34% 29%
Odds Ratio
1.21
(CI: 1.09-1.35)
P = 0.0003
D'Addario G. et al. J Clin Oncol 2005
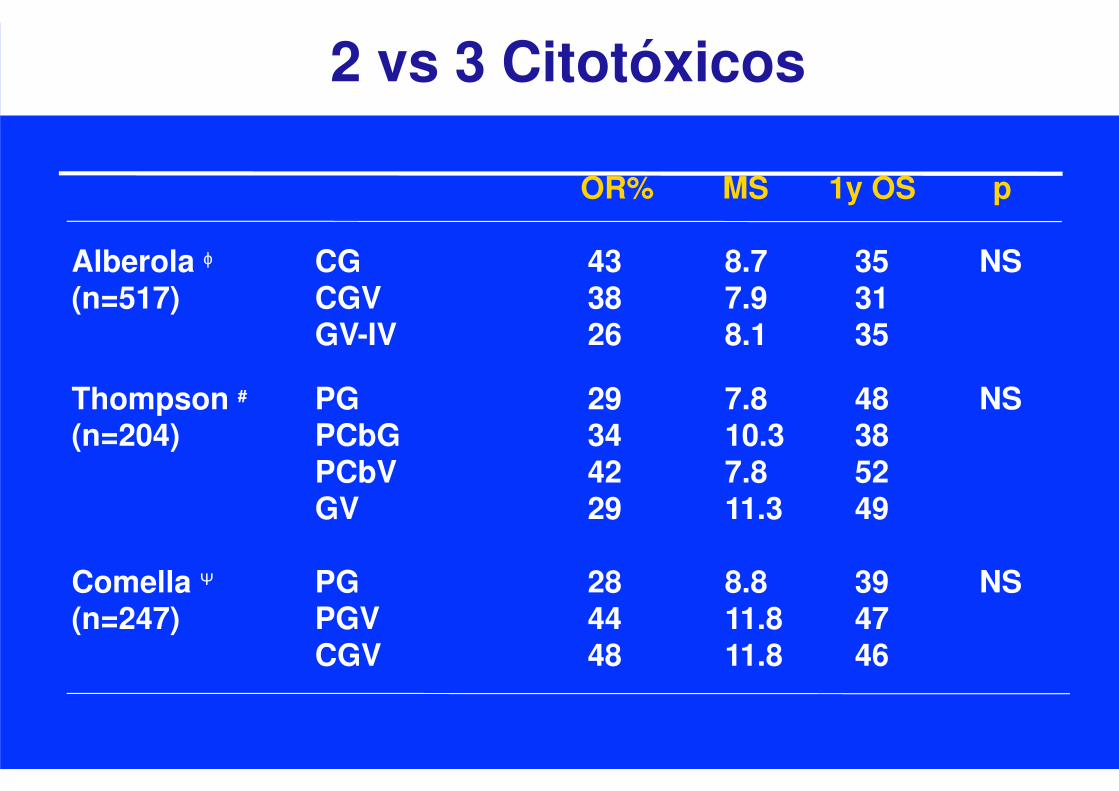
2 vs 3 Citotóxicos
OR% MS 1y OS p
Alberola ϕ CG 43 8.7 35 NS(n=517) CGV 38 7.9 31
GV-IV 26 8.1 35
Thompson # PG 29 7.8 48 NS(n=204) PCbG 34 10.3 38
PCbV 42 7.8 52GV 29 11.3 49
Comella Ψ PG 28 8.8 39 NS(n=247) PGV 44 11.8 47
CGV 48 11.8 46

Dobletes + Targeted Agent
• Inhibidores de MPI (BMS 275291)
• Inhibidores de FT (Lonafamib)
• Agonistas de retinoides (Bexaroteno)
• Inhibidores de TKI de EGFR (Gefitinib, Erlotinib)
• Inhibidores de PKC-α (ISIS 3521)
• ....
• Bevacizumab
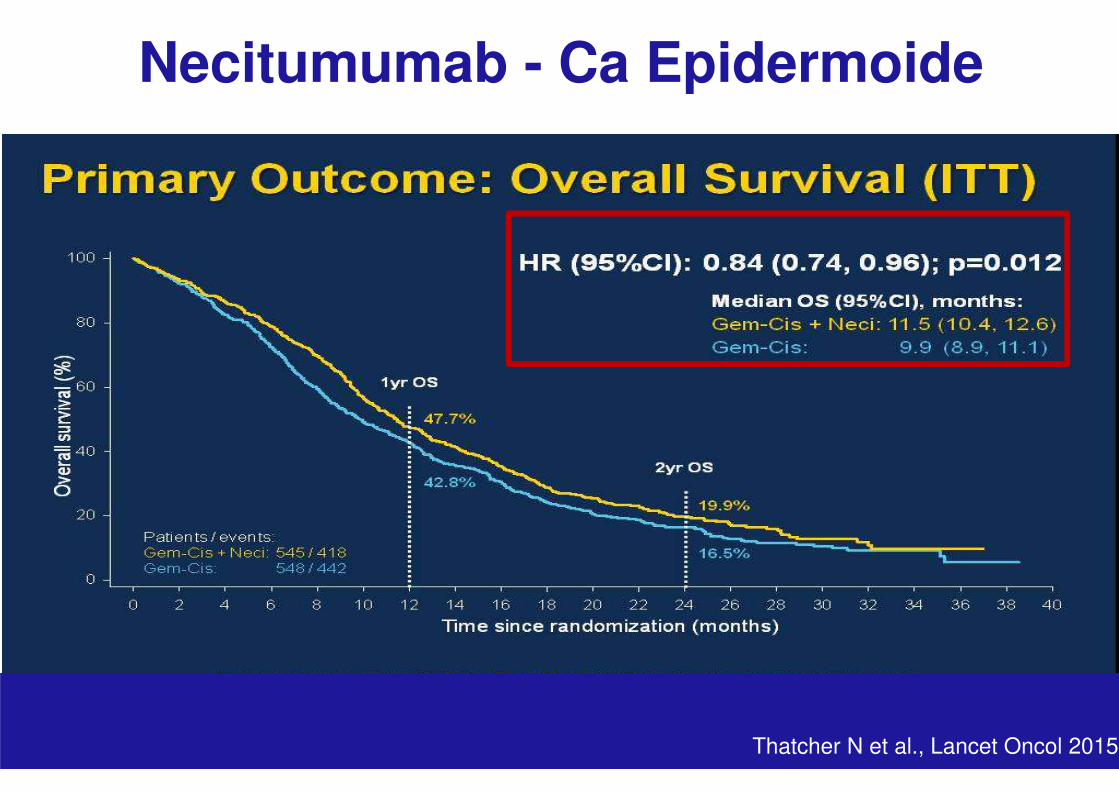
• Necitumumab

Paclitaxel-Carboplatino + BevacizumabSupervivencia
Sandler et al. N Eng J Med 2006
Slide 9
Necitumumab - Ca Epidermoide
Thatcher N et al., Lancet Oncol 2015
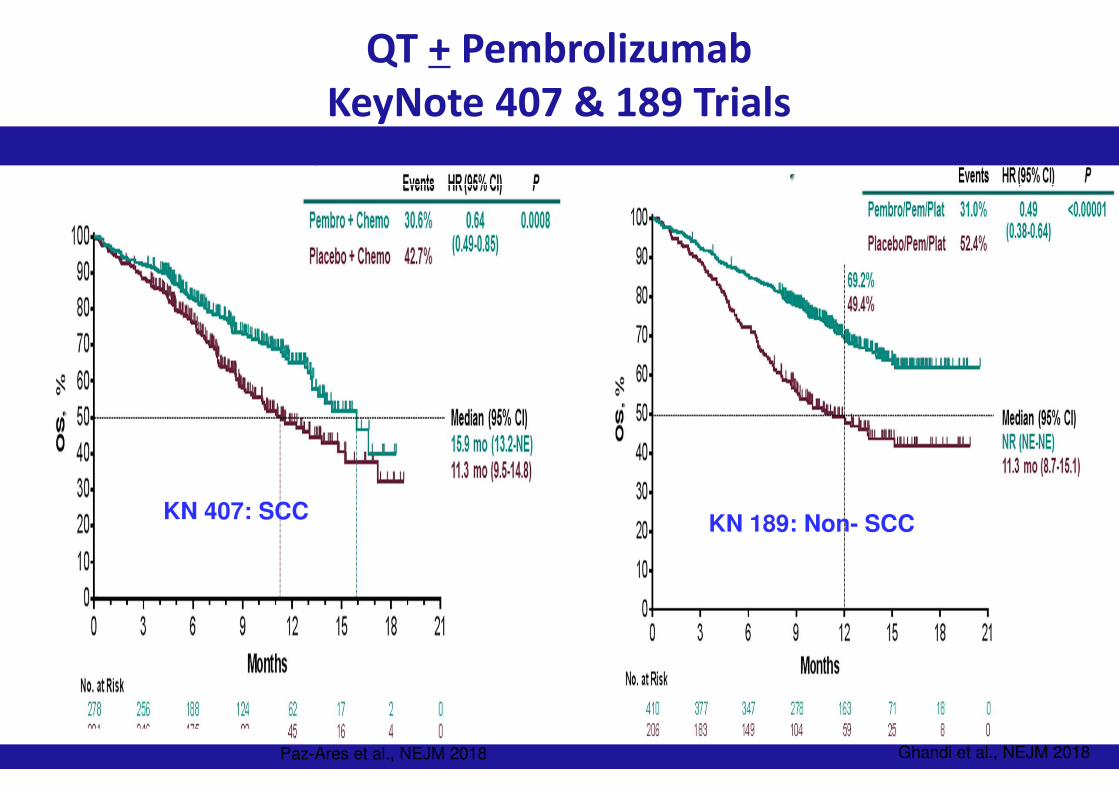
QT + Pembrolizumab
KeyNote 407 & 189 Trials
KN 407: SCCKN 189: Non- SCC
Ghandi et al., NEJM 2018Paz-Ares et al., NEJM 2018 Ghandi et al., NEJM 2018
▪ Regímenes estándar
- antes y después de 1990s
- dobletes actuales
▪ Regímenes alternativos
- regímenes sin platino
- Cis vs Carbo
- tripletes
▪ Duración de la QT
▪ Terapia de Mantenimiento
▪ Edad avanzada / Mal PS
▪ Papel de la Inmunoterapia
▪ Segunda línea y posteriores
▪ “Oncogene driven” CNMP
CNMP Avanzado

Duración Optima de la QT UK Trial: MIC* x 3 v MIC x 6
Smith et al., JCO 19: 1336-1343, 2001
PFS Alivio Sintomático
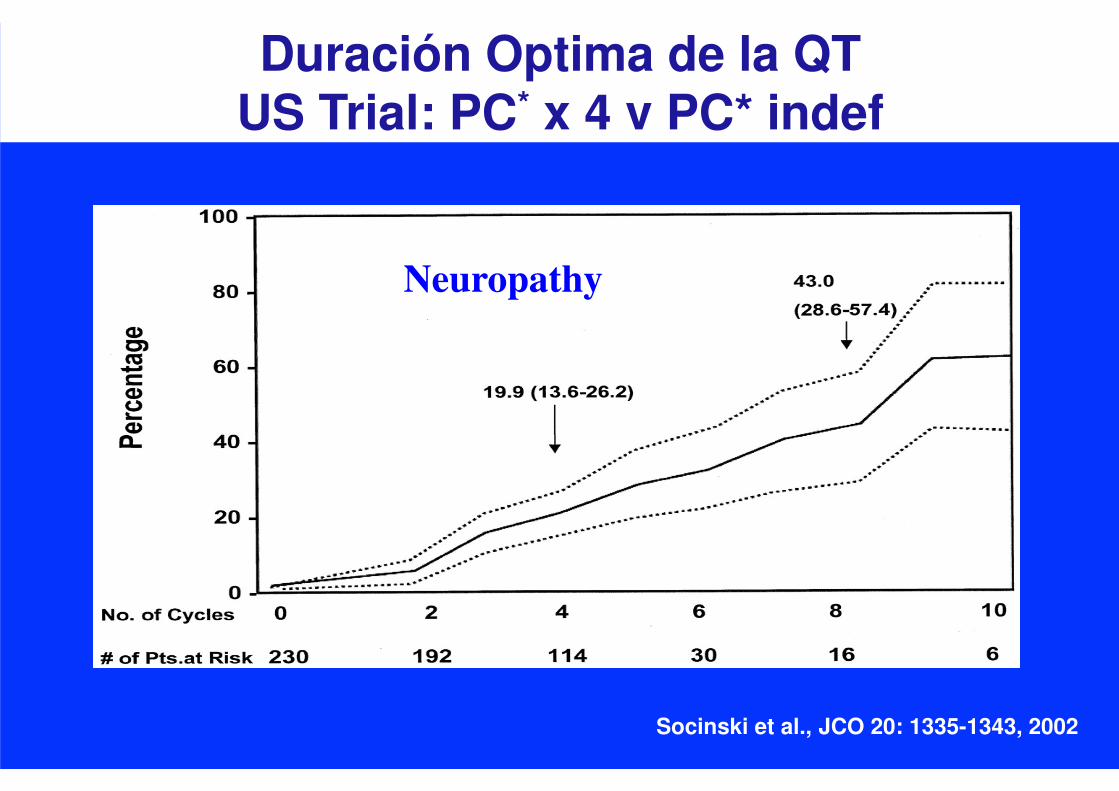
Duración Optima de la QT US Trial: PC* x 4 v PC* indef
Socinski et al., JCO 20: 1335-1343, 2002
Neuropathy

▪ Regímenes estándar
- antes y después de 1990s
- dobletes actuales
▪ Regímenes alternativos
- regímenes sin platino
- Cis vs Carbo
- tripletes
▪ Duración de la QT
▪ Terapia de Mantenimiento
▪ Edad avanzada / Mal PS
▪ Papel de la Inmunoterapia
▪ Segunda línea y posteriores
▪ “Oncogene driven” CNMP
CNMP Avanzado
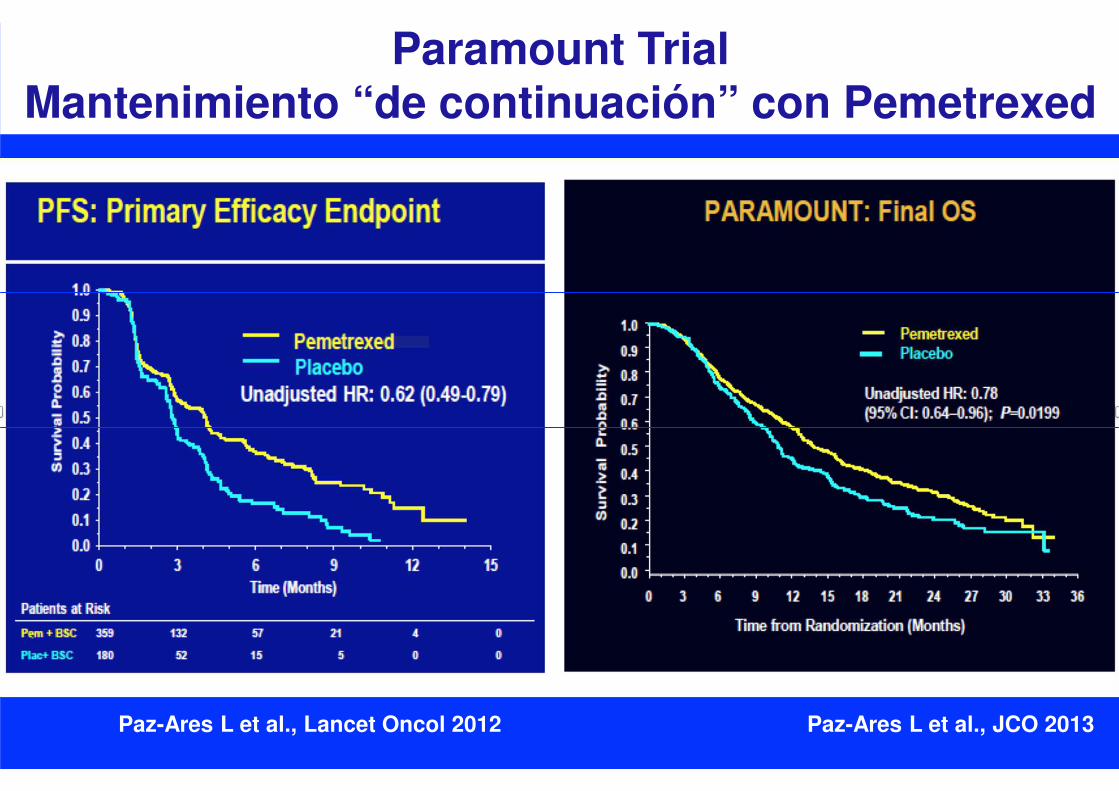
Paramount TrialMantenimiento “de continuación” con Pemetrexed
Paz-Ares L et al., Lancet Oncol 2012 Paz-Ares L et al., JCO 2013
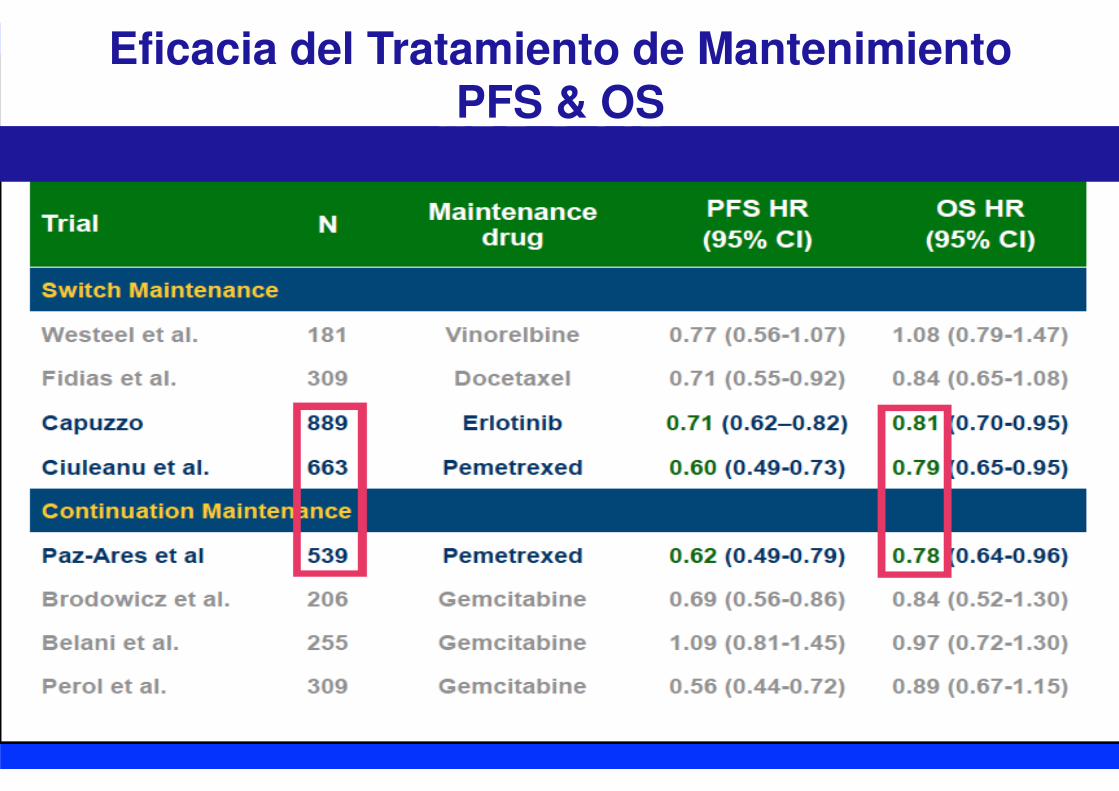
Eficacia del Tratamiento de MantenimientoPFS & OS
▪ Regímenes estándar
- antes y después de 1990s
- dobletes actuales
▪ Regímenes alternativos
- regímenes sin platino
- Cis vs Carbo
- tripletes
▪ Duración de la QT
▪ Terapia de Mantenimiento
▪ Edad avanzada / Mal PS
▪ Papel de la Inmunoterapia
▪ Segunda línea y posteriores
▪ “Oncogene driven” CNMP
CNMP Avanzado
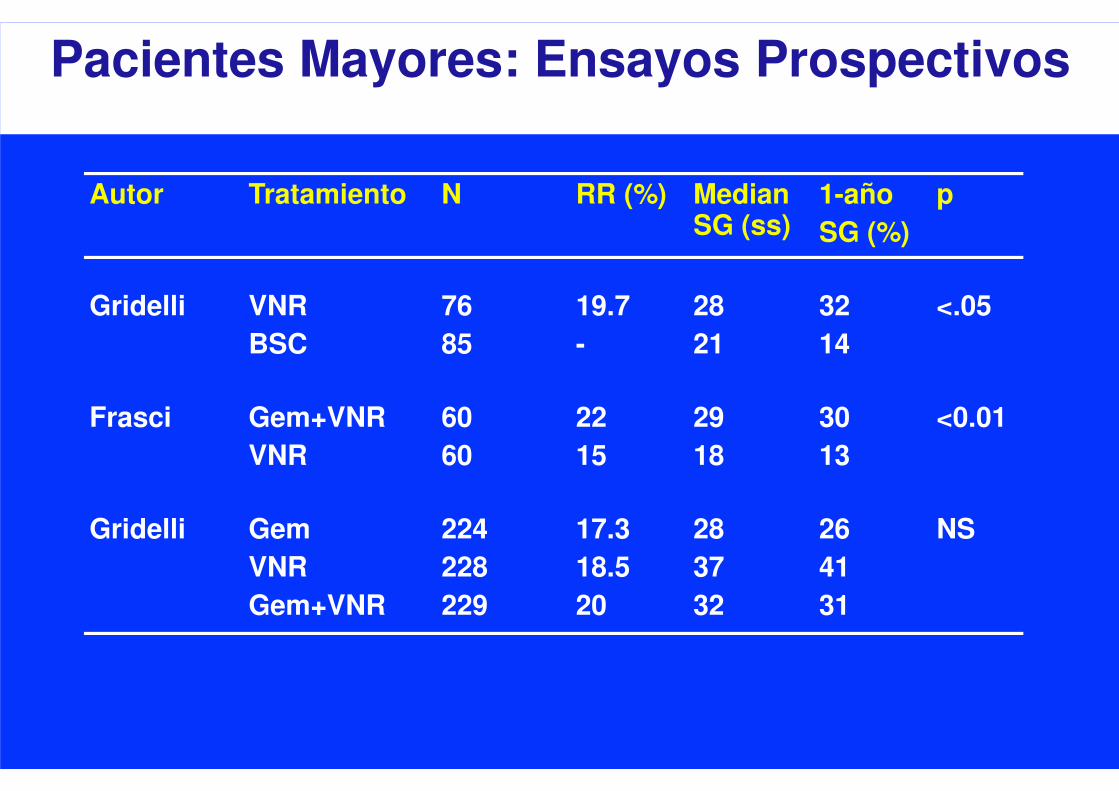
Autor Tratamiento N RR (%) Median SG (ss)
1-año
SG (%)
p
Gridelli VNR
BSC
76
85
19.7
-
28
21
32
14
<.05
Frasci Gem+VNR
VNR
60
60
22
15
29
18
30
13
<0.01
Gridelli Gem
VNR
Gem+VNR
224
228
229
17.3
18.5
20
28
37
32
26
41
31
NS
Pacientes Mayores: Ensayos Prospectivos

Doublet
Single agent
Months 0 6 12 18 24 30 36 42
Single 226 112 45 24 11 4 1
Doublet 225 150 78 46 30 14 7
Doublet
Single
s
u
r
v
i
v
a
l
p
r
o
b
a
b
i
l
i
t
y
MST = 10.3 months (95% CI 8.3-13.3
1-year survival 45.1% (95% CI 38.2-51.8)
MST = 6.2 months (95% CI 5.3-7.4)
1-year survival 26.9% (95% CI 21-33.1)
p= 0.00004
Quoix E et al., LANCET 2011
IFCT 0501 Trial Carboplatino/Taxol semanal v Monoterapia

▪ El tratamiento óptimo no ha sido definido
▪ PS: factor pronóstico reconocido
▪ ECOG 1594 trial (pacientes PS 2)
- Regimenes con cisplatino son demasiado
tóxicos
- Cb/Taxol es acceptable
▪ CALGB trial (Taxol vs Cb/taxol)
- Mediana SG: 2.4 vs 4.7 meses (p<0.05)
- Mayor toxicidad que PS 0-1, pero aceptable
▪ Other regimens: Cb/Gem, Cb/Pem, Tax/Gem
Estado Funcional Alterado
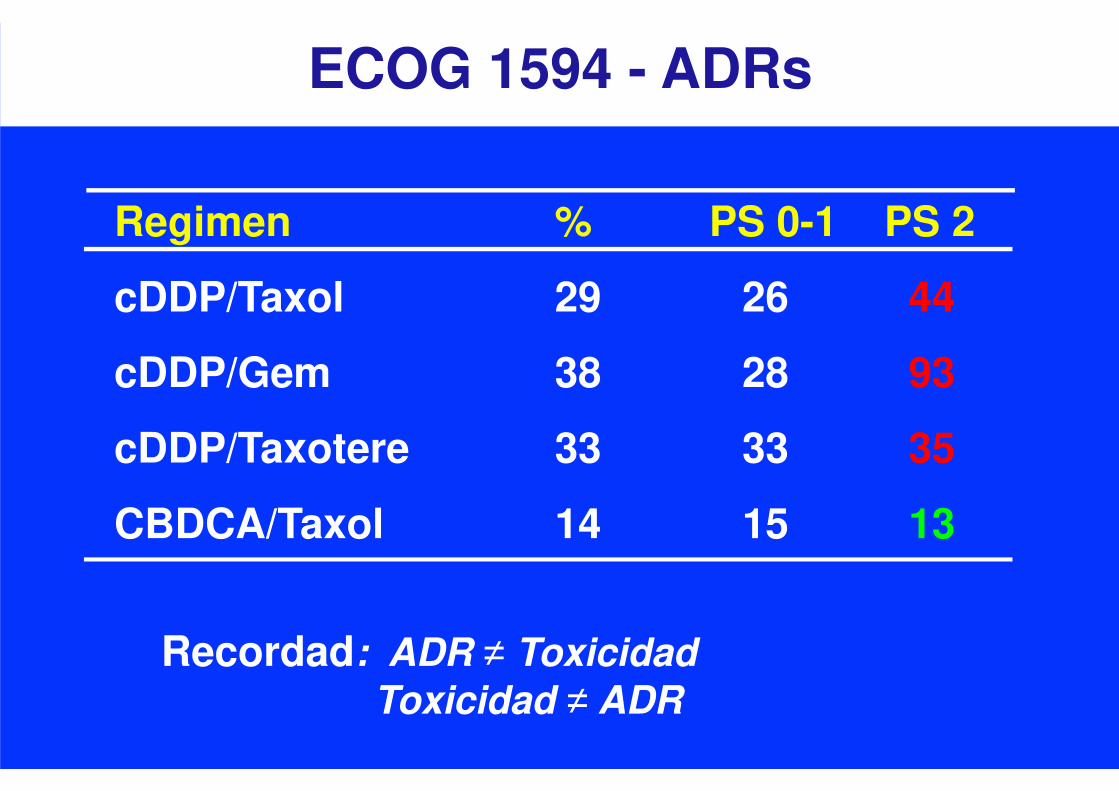
ECOG 1594 - ADRs
Regimen % PS 0-1 PS 2
cDDP/Taxol 29 26 44
cDDP/Gem 38 28 93
cDDP/Taxotere 33 33 35
CBDCA/Taxol 14 15 13
Recordad: ADR ≠ Toxicidad
Toxicidad ≠ ADR

▪ Regímenes estándar
- antes y después de 1990s
- dobletes actuales
▪ Regímenes alternativos
- regímenes sin platino
- Cis vs Carbo
- tripletes
▪ Duración de la QT
▪ Terapia de Mantenimiento
▪ Edad avanzada / Mal PS
▪ Papel de la Inmunoterapia
▪ Segunda línea y posteriores
▪ “Oncogene driven” CNMP
CNMP Avanzado

Brahmer et al. WLCC 2017, Lopez et al.., ASCO 2018
30% of 1ºL patients
KEYNOTE-024 & 042 Trial: Pembro v QTFirst Line treatment in PD-L1 > 50% NSCLC

Ghandi et al., NEJM 2018
Non SCC KeyNote 189 Trial SCC KeyNote 407 Trial
Paz-Ares et al., NEJM 2018
QT + Pembrolizumab en CNMP
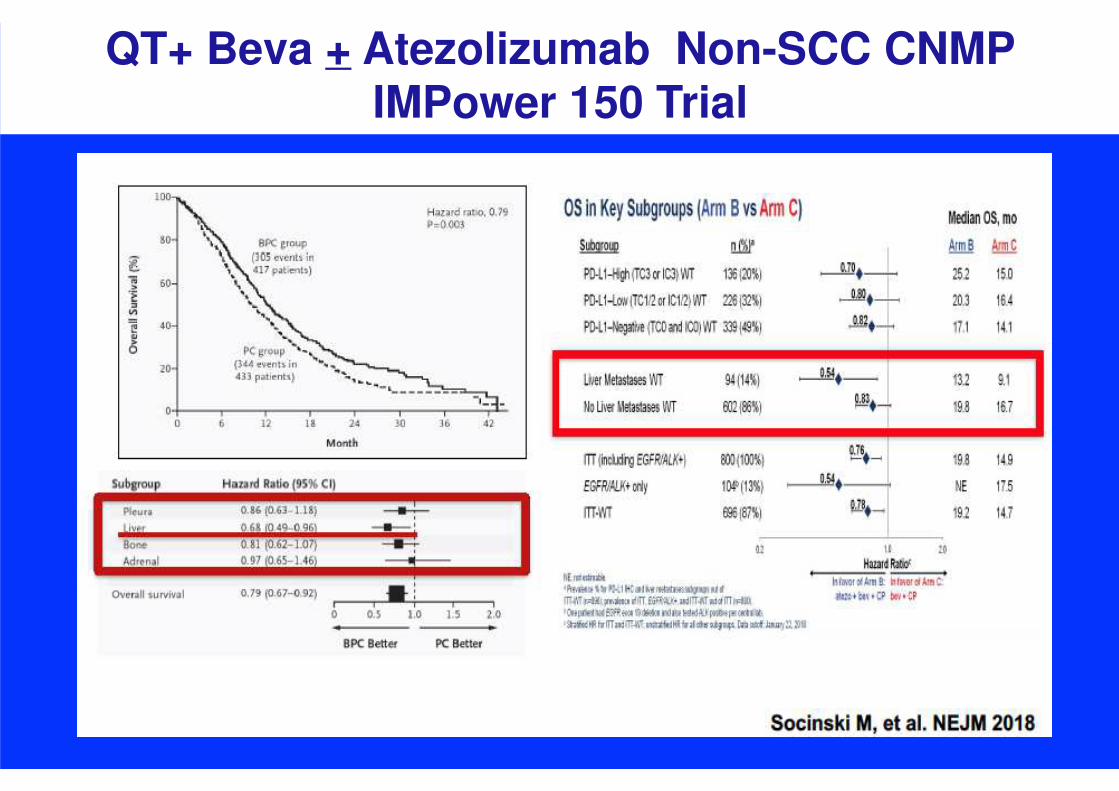
QT+ Beva + Atezolizumab Non-SCC CNMPIMPower 150 Trial
Socinski et al, NEJM, 2018
Socinski et al, NEJM, 2018
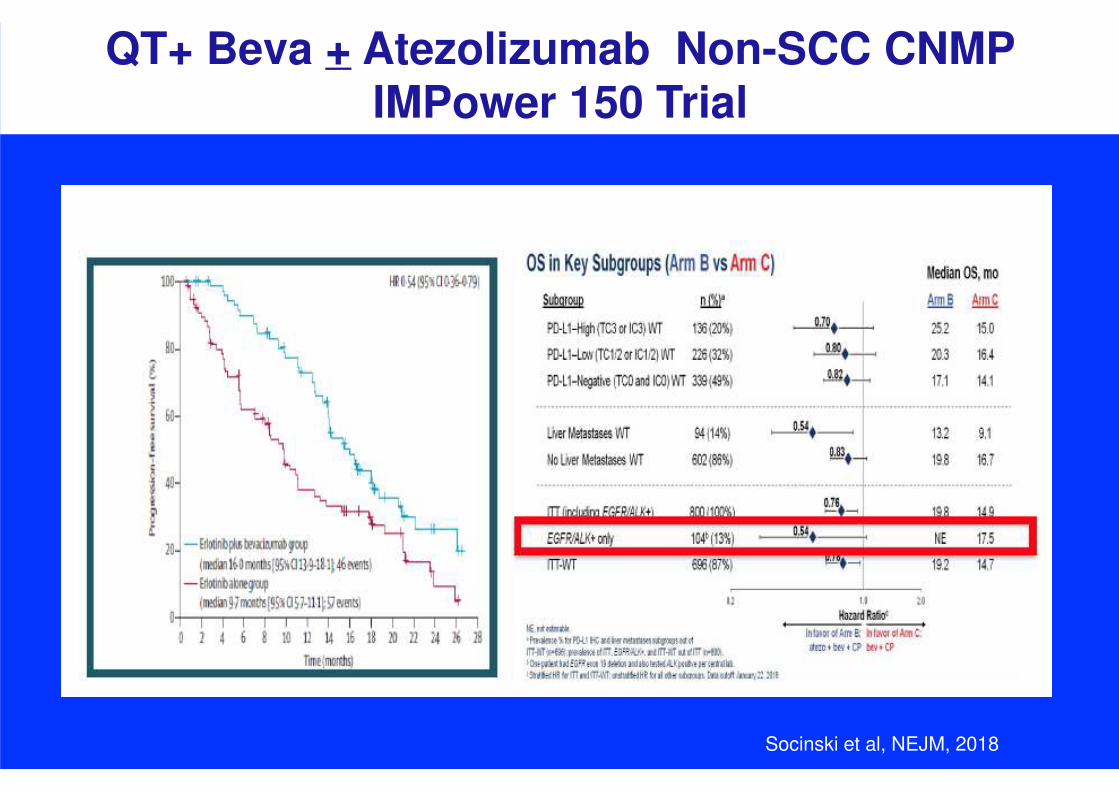
QT+ Beva + Atezolizumab Non-SCC CNMPIMPower 150 Trial
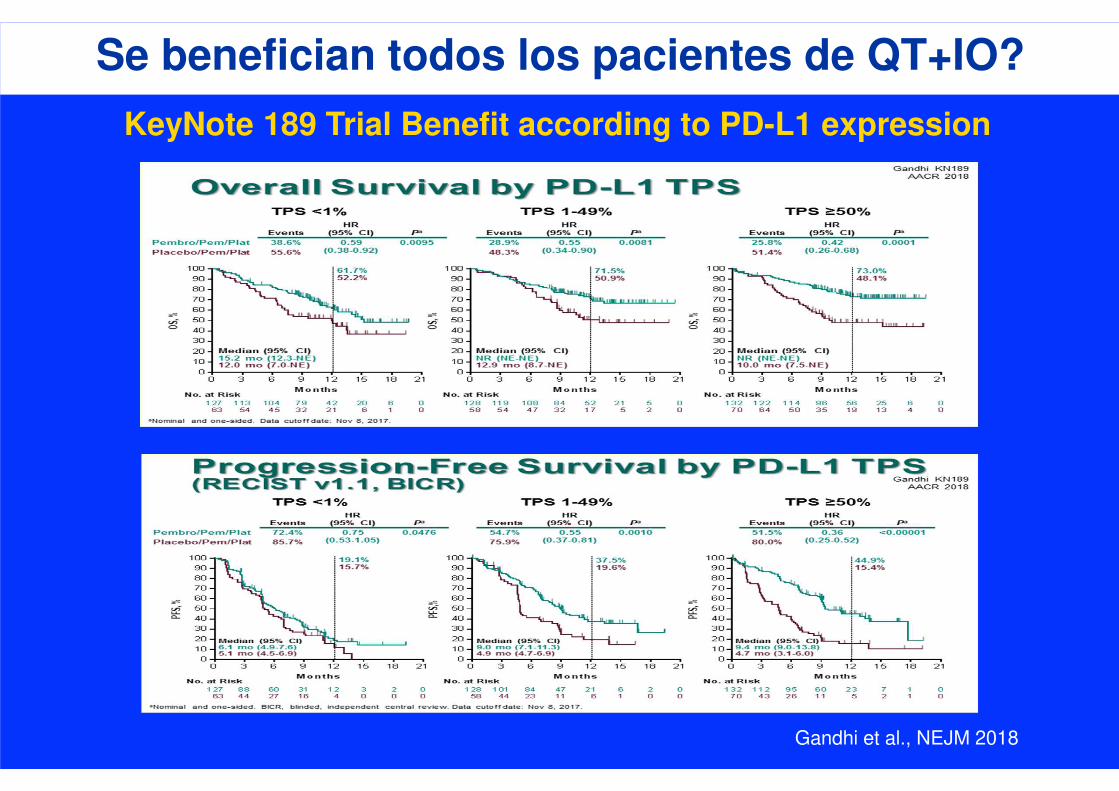
Gandhi et al., NEJM 2018
KeyNote 189 Trial Benefit according to PD-L1 expression
Se benefician todos los pacientes de QT+IO?
Nivolumab + Chemotherapy
Chemotherapy
43 36 21 14 9 5 2 0
No. at risk
48 30 16 4 1 1 1 0Chemo
Nivo + chemo(n =
43)Chemo(n = 48)
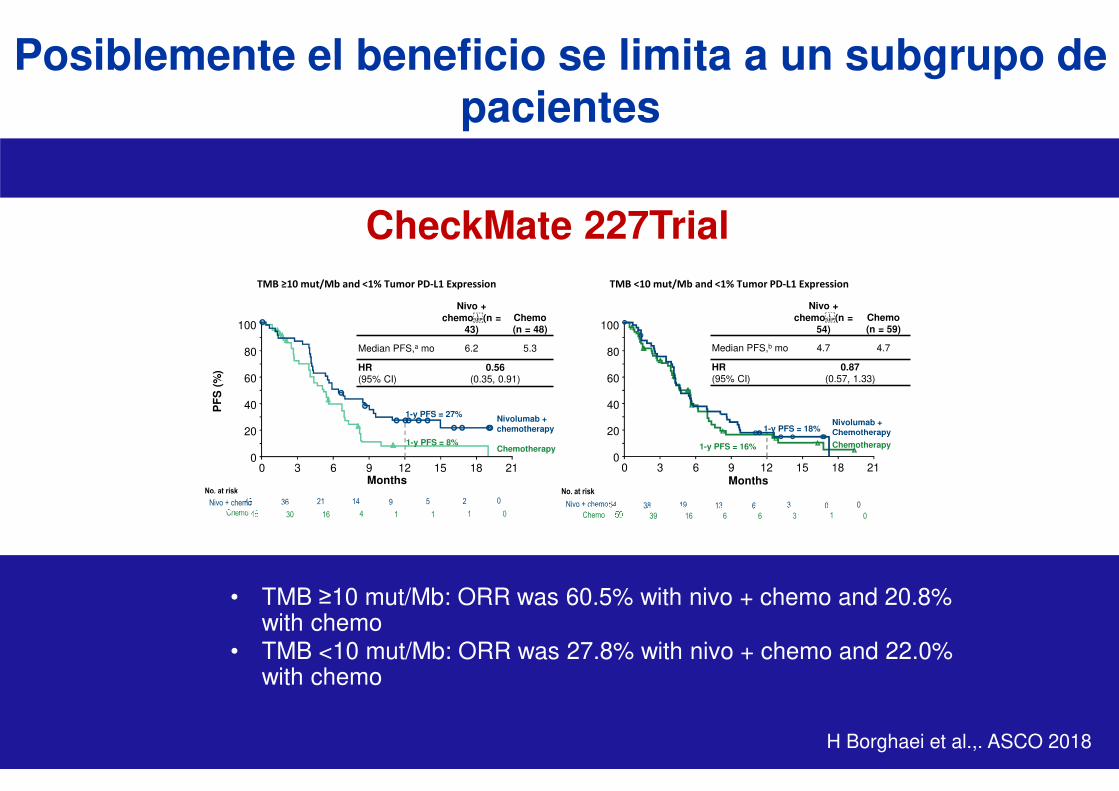
Median PFS,a mo 6.2 5.3
HR(95% CI)
0.56(0.35, 0.91)
Nivolumab + chemotherapy
Months
Chemotherapy
TMB ≥10 mut/Mb and <1% Tumor PD-L1 Expression
1-y PFS = 27%
1-y PFS = 8%
Months
TMB <10 mut/Mb and <1% Tumor PD-L1 Expression
Nivo + chemo(n =
54)Chemo(n = 59)
Median PFS,b mo 4.7 4.7
HR(95% CI)
0.87 (0.57, 1.33)
0
20
40
60
80
100
0 6 12 183 9 15 210
20
40
60
80
100
0 6 12 183 9 15 21
1-y PFS = 18%
1-y PFS = 16%
54 38 19 13 6 3 0 0
59 39 16 6 6 3 1 0
Nivo + chemo
No. at risk
Chemo
PF
S (
%)
Nivo + chemo
Posiblemente el beneficio se limita a un subgrupo de pacientes
CheckMate 227Trial
H Borghaei et al.,. ASCO 2018
• TMB ≥10 mut/Mb: ORR was 60.5% with nivo + chemo and 20.8% with chemo
• TMB <10 mut/Mb: ORR was 27.8% with nivo + chemo and 22.0% with chemo
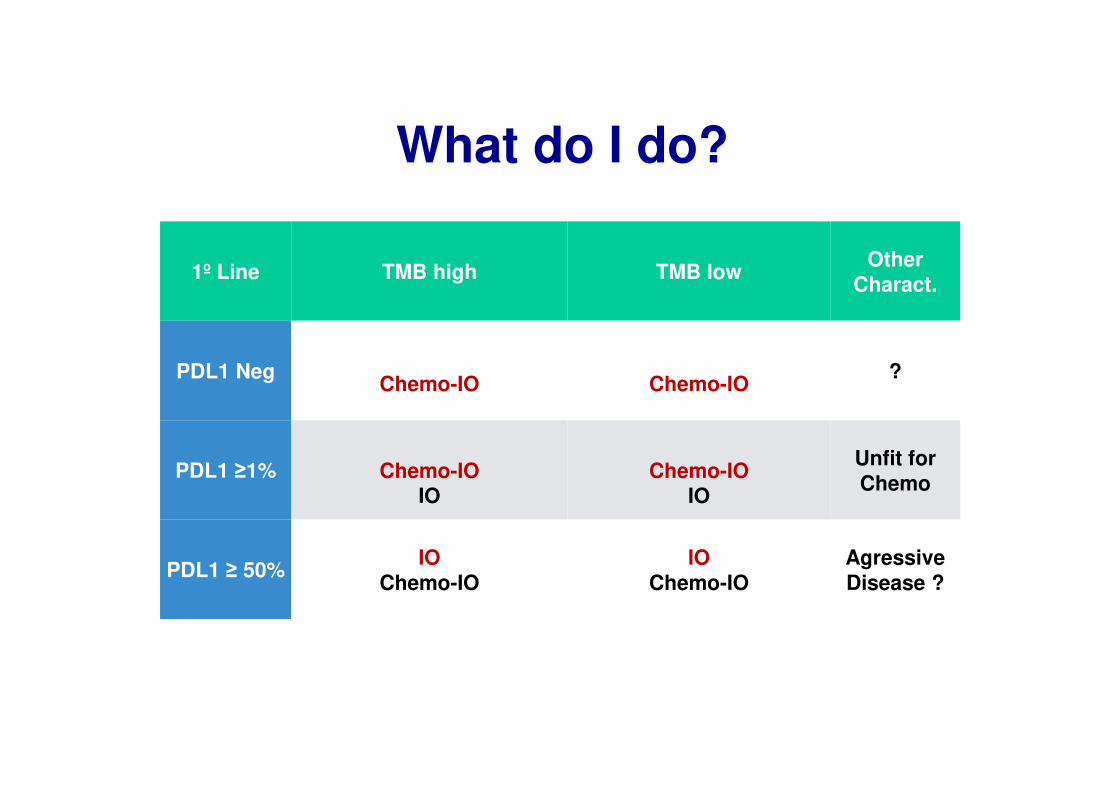
1º Line TMB high TMB lowOther
Charact.
PDL1 NegChemo-IO Chemo-IO
?
PDL1 ≥1% Chemo-IO IO
Chemo-IOIO
Unfit for Chemo
PDL1 ≥ 50%IO
Chemo-IO IO
Chemo-IOAgressiveDisease ?
What do I do?
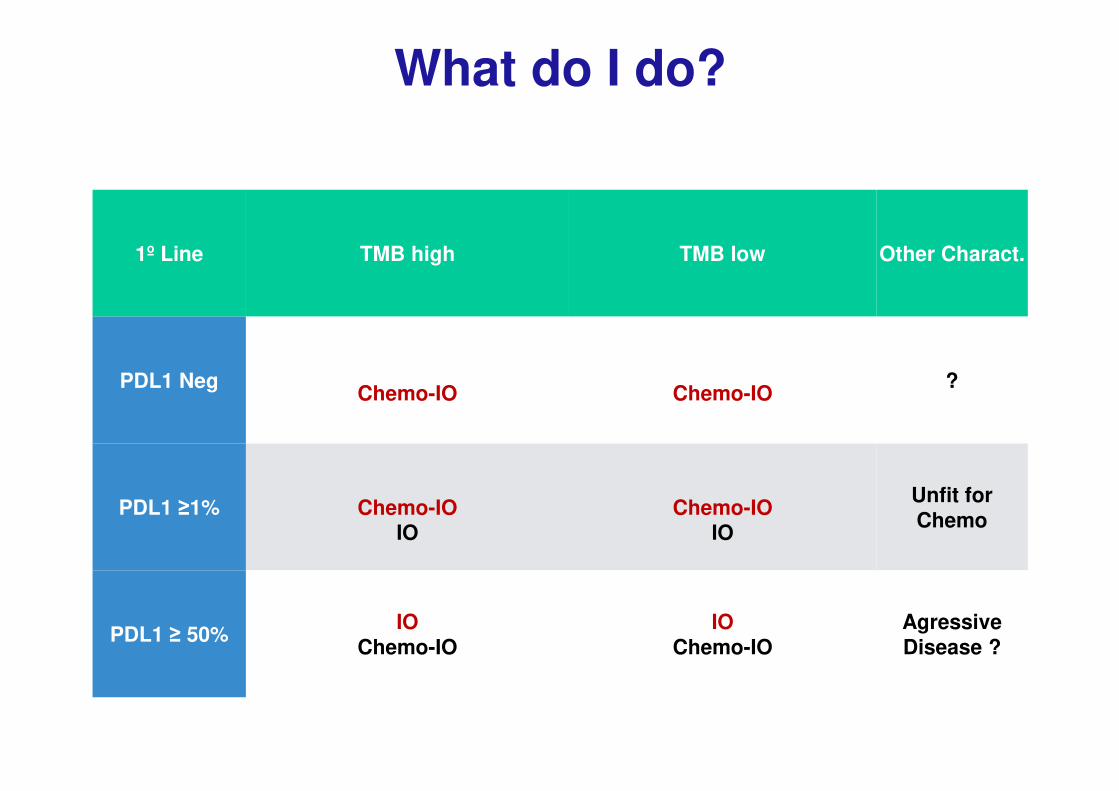
What do I do?
1º Line TMB high TMB low Other Charact.
PDL1 NegChemo-IO Chemo-IO
?
PDL1 ≥1% Chemo-IO IO
Chemo-IOIO
Unfit for Chemo
PDL1 ≥ 50%IO
Chemo-IO IO
Chemo-IOAgressiveDisease ?

1º Line TMB high TMB low Other Charact.
PDL1 NegChemo
Chemo-IO
Chemo
Chemo-IO?
PDL1 ≥1% IO Chemo-IO
IOChemo-IO
Unfit for Chemo
PDL1 ≥ 50%IO
Chemo-IO
IO
Chemo-IO
AgressiveDisease ?
What will I do?
▪ Regímenes estándar
- antes y después de 1990s
- dobletes actuales
▪ Regímenes alternativos
- regímenes sin platino
- Cis vs Carbo
- tripletes
▪ Duración de la QT
▪ Terapia de Mantenimiento
▪ Edad avanzada / Mal PS
▪ Papel de la Inmunoterapia
▪ Segunda línea y posteriores
▪ “Oncogene driven” CNMP
CNMP Avanzado

Segunda Línea: Docetaxel vs BSC

Pemetrexed
< Neutropenia
< Hospitalizac.
< Uso GCSF
< Alopecia
Segunda Línea Pemetrexed vs Docetaxel
Overall Survival<br />ITT Population
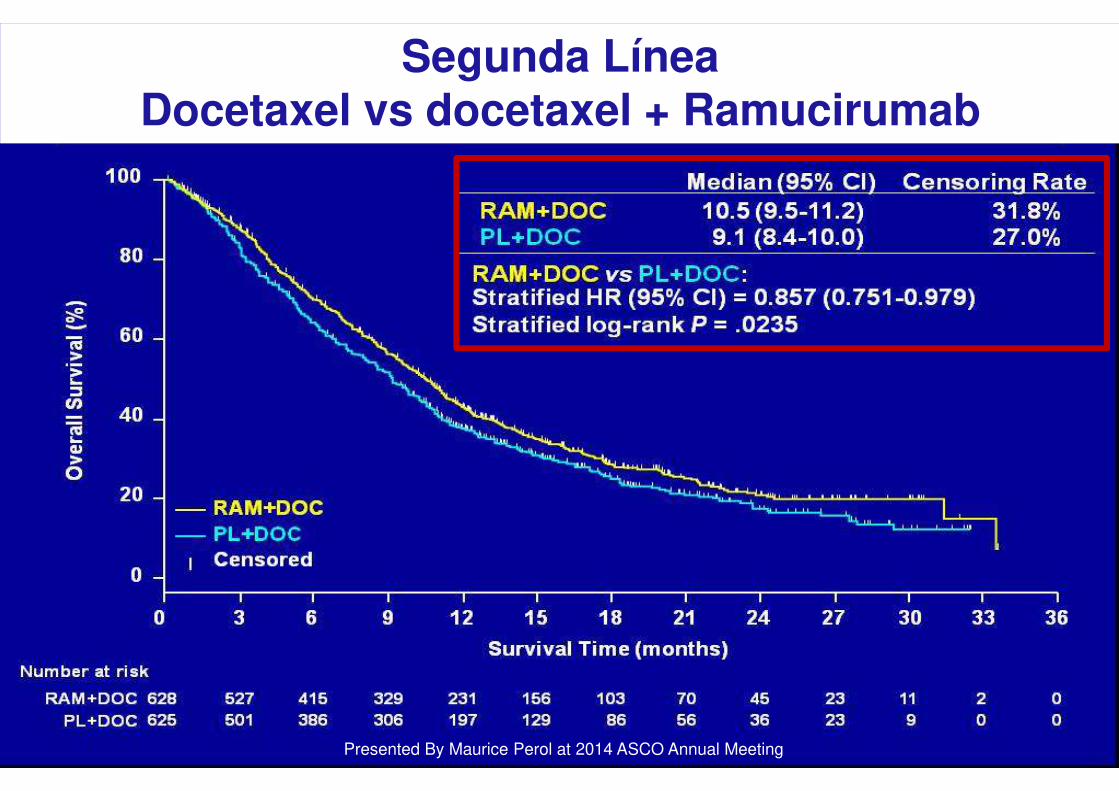
Presented By Maurice Perol at 2014 ASCO Annual Meeting
Segunda LíneaDocetaxel vs docetaxel + Ramucirumab

Tto de 2ª/3ª Línea- Erlotinib
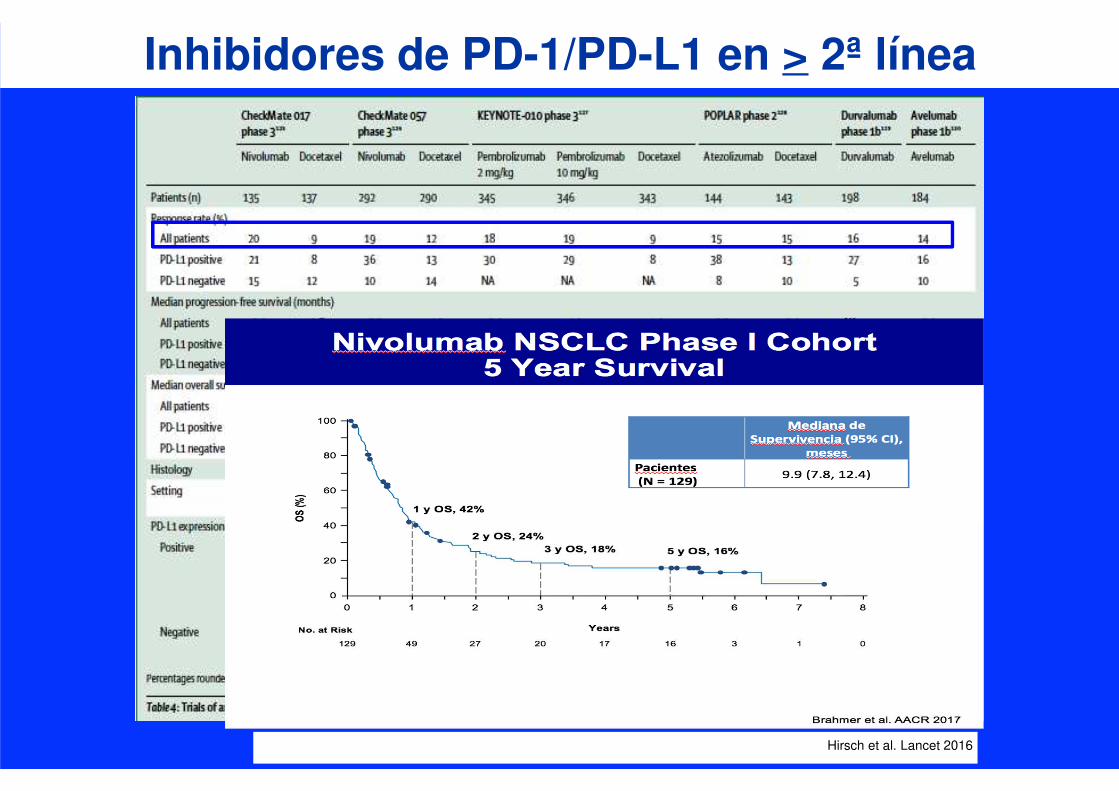
Inhibidores de PD-1/PD-L1 en > 2ª línea
Hirsch et al. Lancet 2016

Estudios de Fase III con IOen pacientes previamente tratados
*850 in primary population
NR = not reached 1. Borghaei, et al. ASCO 2016 2. Herbst, et al. Lancet 2015; 3. Barlesi, et al. ESMO 2016
CheckMate 0171
Nivolumab
vs docetaxel
CheckMate 0571
Nivolumab
vs docetaxel
KEYNOTE-0102
Pembrolizumab (2mg/kg or
10mg/kg) vs docetaxel
OAK3
Atezolizumab
vs docetaxel
Phase of study III III II/III III
PD-L1 selected No No Yes (TPS* ≥1%) No
Study size, n 272 (135 vs 137) 582 (292 vs 290) 1,033 (344 vs 346 vs 343)1,225
(425 vs 425)*
Histology Squamous Non-squamous All-comers All-comers
Line of therapy, %
2L
3L
>3L
Other/unknown
100
0
0
0
88
11
<1
0
69
20
9
<1
75
25
0
0
Subsequent CIT
(immunotherapy arm vs
chemo arm), %
<1 vs 2 1 vs 2 0.6 vs 1.7 vs 13.1 4.5 vs 17.2
Crossover from chemo arm to
study immunotherapy, %4 6 Not permitted Not permitted
Median OS, months
HR vs docetaxel (p value)
9.2 vs 6.0
0.62 (p=0.0004)
12.2 vs 9.5
0.75 (p<0.001)
10.4 vs 12.7 vs 8.5
2mg/kg: 0.71 (p=0.0008)
10mg/kg: 0.61 (p<0.0001)
13.8 vs 9.6
0.73 (p=0.0003)

Atezolizumab en 2L CNMPOAK Trial: Supervivencia (ITT Population)
51
*Stratified HR.Atezo, atezolizumab; CI, confidence interval; HR, hazard ratio; ITT, intent-to-treat; mos, months; NSCLC, non-small cell lung cancer; OS, overall survival.
Barlesi F et al. Oral presentation at ESMO 2016. LBA044.
100
80
60
40
20
00 3 6
Time (months)
21189 12 24 2715
HR=0.73* (95% CI: 0.62–0.87), P=0.0003
Atezolizumab
Docetaxel
Median 9.6 mos(95% CI: 8.6–11.2)
Median 13.8 mos(95% CI: 11.8–15.7)
OS
(%
)
Atezolizumab:12-month OS=55% 18-month OS=40%
Docetaxel:12-month OS=41% 18-month OS=27%
NSCLC

Supervivencia según la expresión de PD-L1CheckMate 057 - Nivolumab
52
La expresión de PD-L1 en tumor es predictiva
Nivo
Doc
100
90
80
70
60
50
40
30
10
0
20
Time (months)
24211815129630 27
Median OS(mo)
Nivo 10.4
Doc 10.1
Median OS (mo)
Nivo 17.2
Doc 9.0
≥1% PD-L1 expression level
HR (95% CI)=0.59 (0.43, 0.82)
<1% PD-L1 expression level
OS
(%
)
HR (95% CI)=0.90 (0.66, 1.24)OS
(%
)
24211815129630 27
100
90
80
70
60
50
40
30
10
0
20
Nivo
Doc
aPD-L1 expression was measured in pretreatment tumor biopsies (DAKO automated IHC assay).2
CI=confidence interval; Doc=docetaxel; IHC=immunohistochemistry; Nivo=nivolumab;
1. Paz-Ares L, et al. Presented at ASCO 2015, Abstract LBA109. 2. Rizvi NA, et al. Lancet Oncol 2015;16:257–265.
PD-L1 expression level
Median OS (mo)HR
Nivolumab Docetaxel
≥5%
<5%
18.2
9.7
8.1
10.1
HR (95% CI) = 0.43 (0.30, 0.63)
HR (95% CI) = 1.01 (0.77, 1.34)
≥10%
<10%
19.4
9.9
8.0
10.3
HR (95% CI) = 0.40 (0.26, 0.59)
HR (95% CI) = 1.00 (0.76, 1.31)
0
60
70
80
90
100
% T
um
ou
r C
ell S
tain
ing
10
20
30
40
50
Cases
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39
22C3 28-8
SP142 SP263
Tumour Cells1
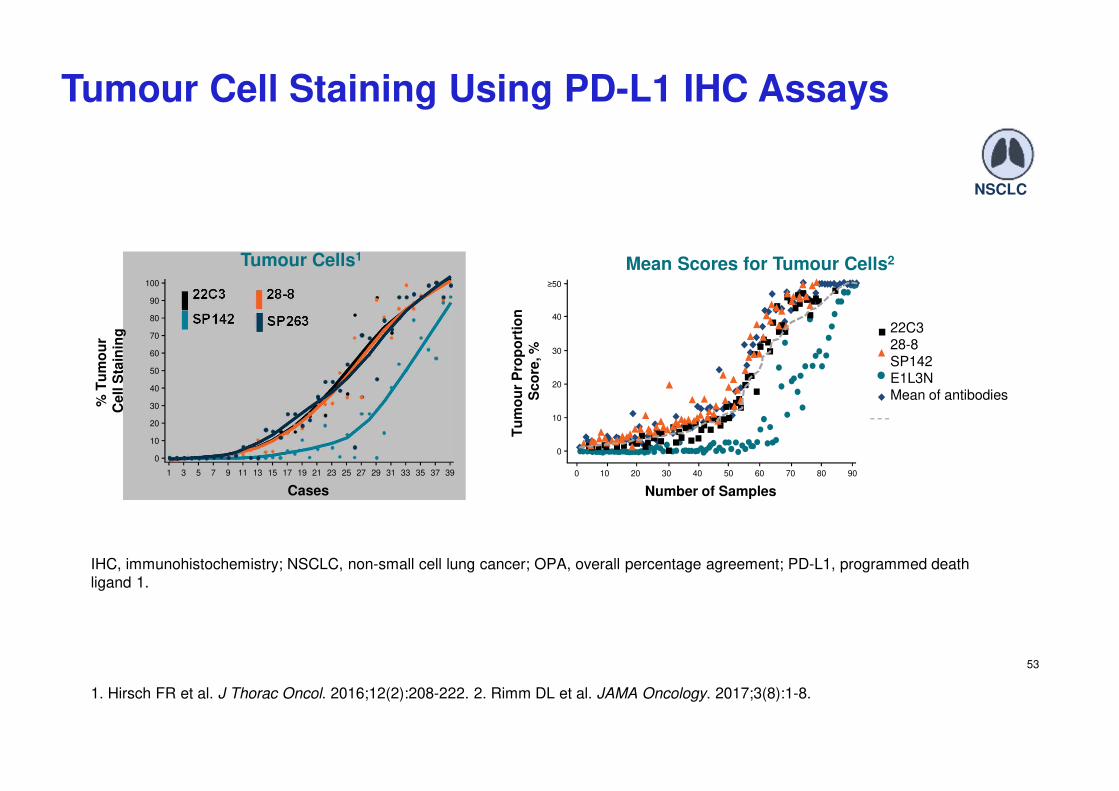
Tumour Cell Staining Using PD-L1 IHC Assays
IHC, immunohistochemistry; NSCLC, non-small cell lung cancer; OPA, overall percentage agreement; PD-L1, programmed death ligand 1.
1. Hirsch FR et al. J Thorac Oncol. 2016;12(2):208-222. 2. Rimm DL et al. JAMA Oncology. 2017;3(8):1-8.
53
0
30
40
≥50
Tu
mo
ur
Pro
po
rtio
n
Sc
ore
, %
10
20
Number of Samples
0 10 20 30 40 50 70 80 90
Mean Scores for Tumour Cells2
60
22C328-8
SP142E1L3NMean of antibodies
NSCLC
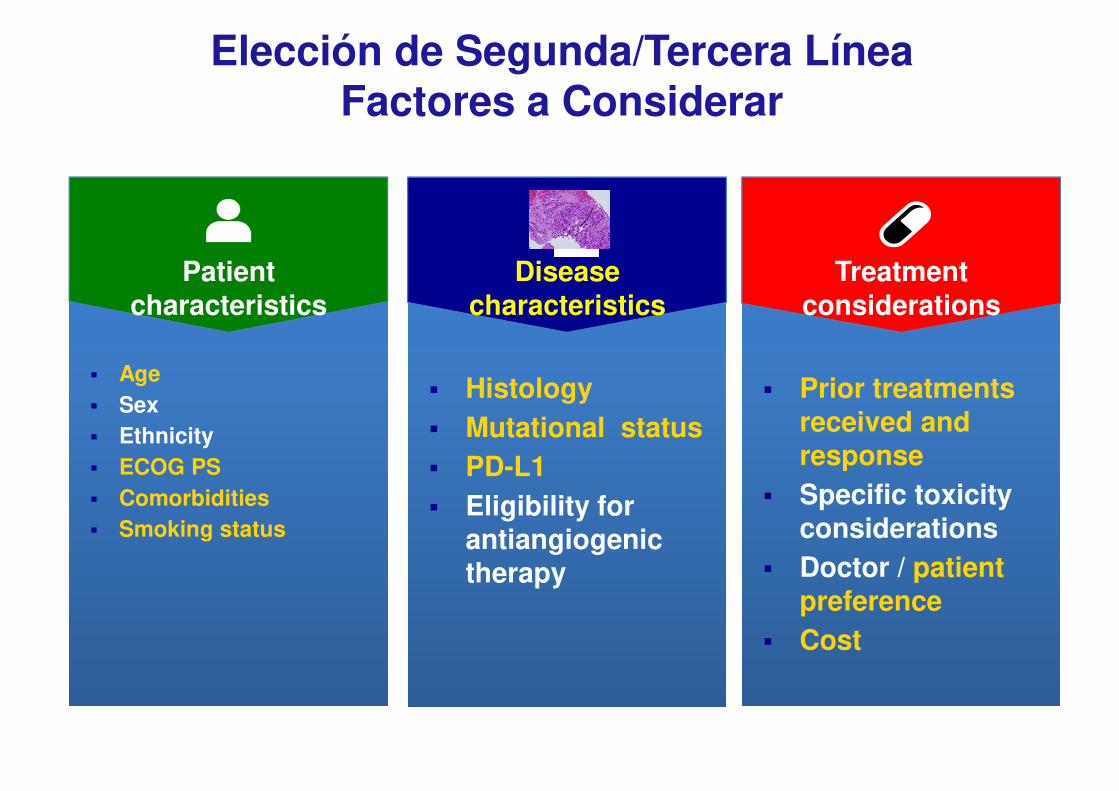
Elección de Segunda/Tercera LíneaFactores a Considerar
▪ Age
▪ Sex
▪ Ethnicity
▪ ECOG PS
▪ Comorbidities
▪ Smoking status
▪ Histology
▪ Mutational status
▪ PD-L1
▪ Eligibility for antiangiogenic therapy
▪ Prior treatments received and response
▪ Specific toxicity considerations
▪ Doctor / patient preference
▪ Cost
Patient characteristics
Disease characteristics
Treatment considerations
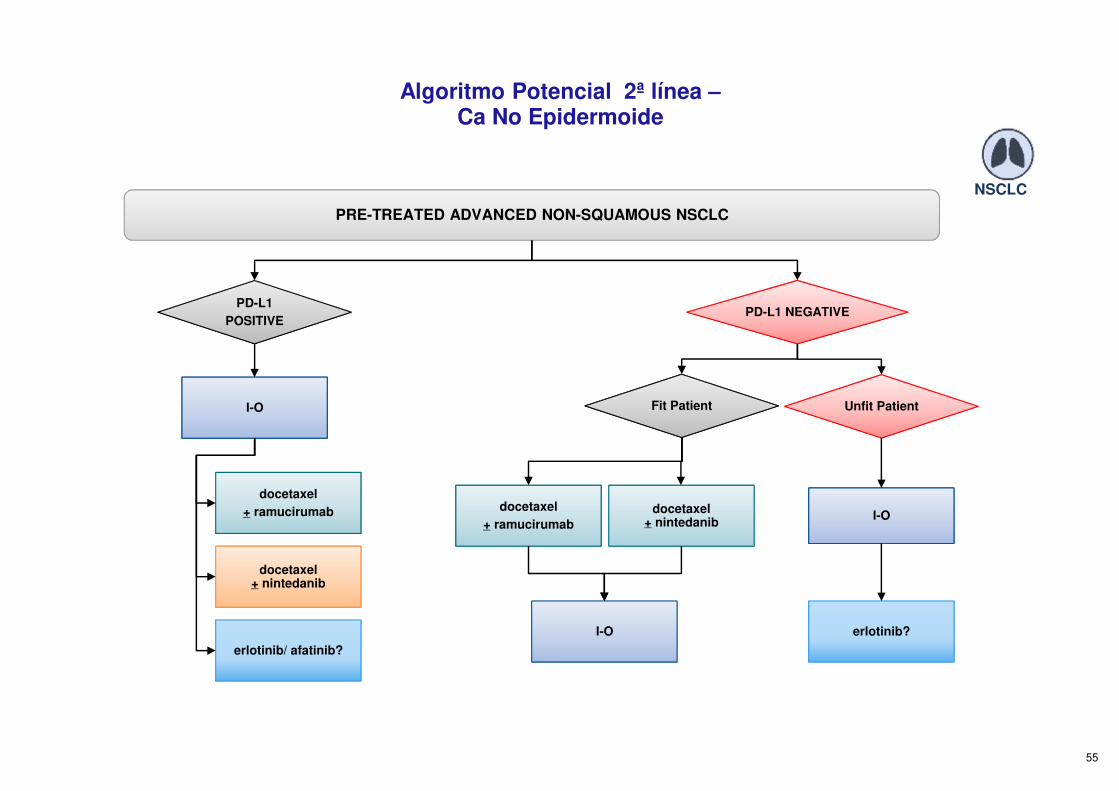
Algoritmo Potencial 2ª línea –Ca No Epidermoide
55
PRE-TREATED ADVANCED NON-SQUAMOUS NSCLC
PD-L1
POSITIVE
I-O
docetaxel
+ ramucirumab
docetaxel+ nintedanib
erlotinib/ afatinib?
PD-L1 NEGATIVE
Fit Patient
docetaxel
+ ramucirumab
docetaxel+ nintedanib
I-O
Unfit Patient
I-O
erlotinib?
NSCLC
56
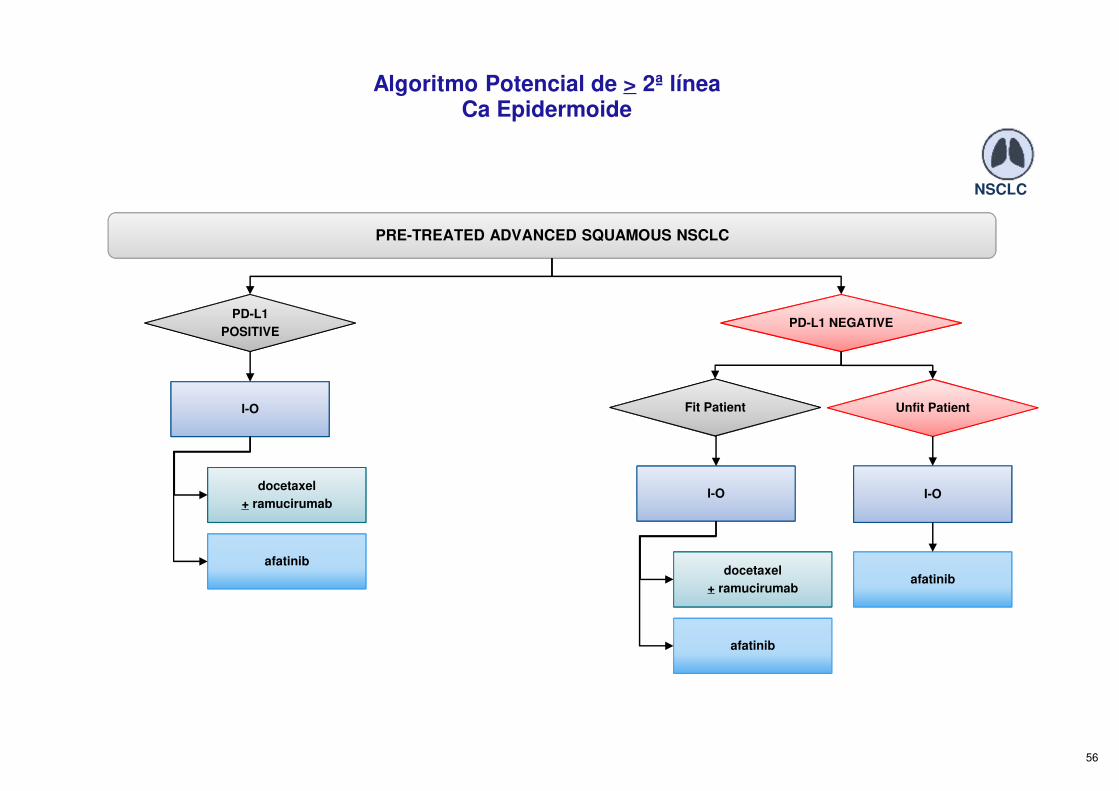
afatinib
PRE-TREATED ADVANCED SQUAMOUS NSCLC
PD-L1
POSITIVE
I-O
docetaxel
+ ramucirumab
PD-L1 NEGATIVE
Fit Patient Unfit Patient
I-O
afatinib
afatinib
I-O
docetaxel
+ ramucirumab
NSCLC
Algoritmo Potencial de > 2ª línea Ca Epidermoide
▪ Regímenes estándar
- antes y después de 1990s
- dobletes actuales
▪ Regímenes alternativos
- regímenes sin platino
- Cis vs Carbo
- tripletes
▪ Duración de la QT
▪ Terapia de Mantenimiento
▪ Edad avanzada / Mal PS
▪ Papel de la Inmunoterapia
▪ Segunda línea y posteriores
▪ “Oncogene driven” CNMP
CNMP Avanzado

NTRK fusions
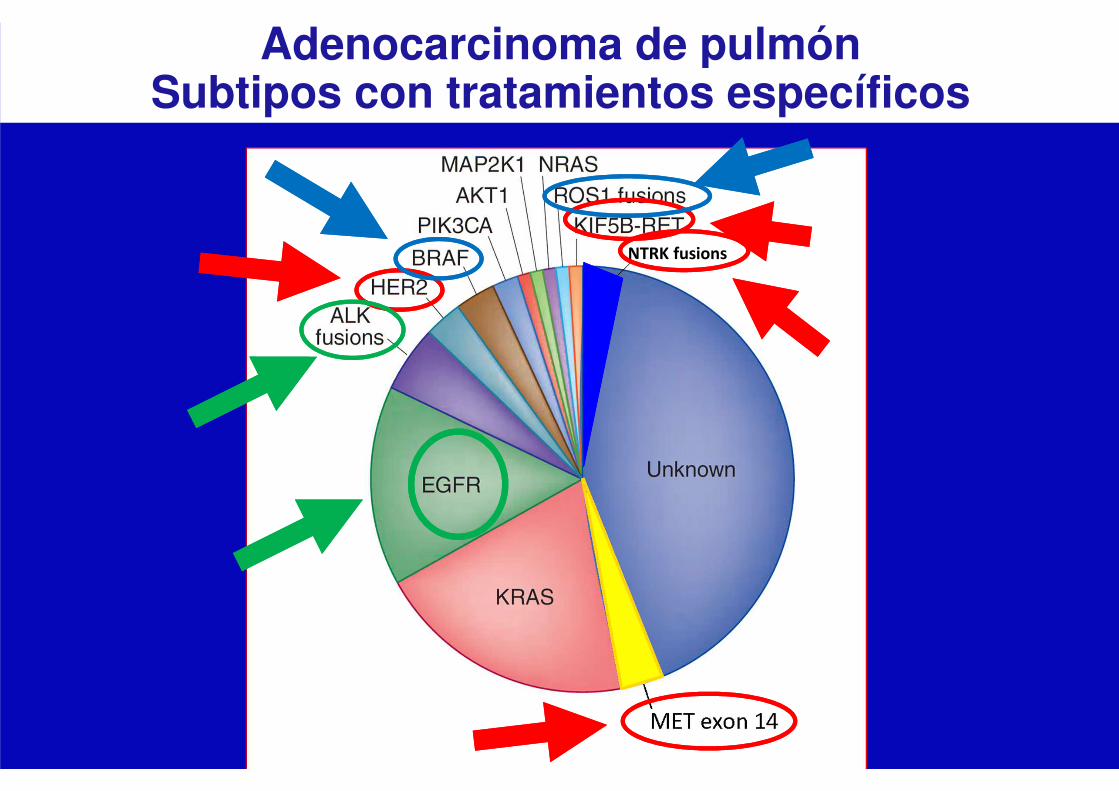
Adenocarcinoma de pulmón Subtipos con tratamientos específicos

Tratamiento del CNMP con Adición Oncogénica
Rosell R et al. Lancet Oncol. 2012;13:239–46; Shaw AT et al. N Engl J Med. 2013;368:2385–94
Erlotinib vs chemotherapy inEGFR mutant advanced NSCLC
Crizotinib vs chemotherapy inALK positive NSCLC
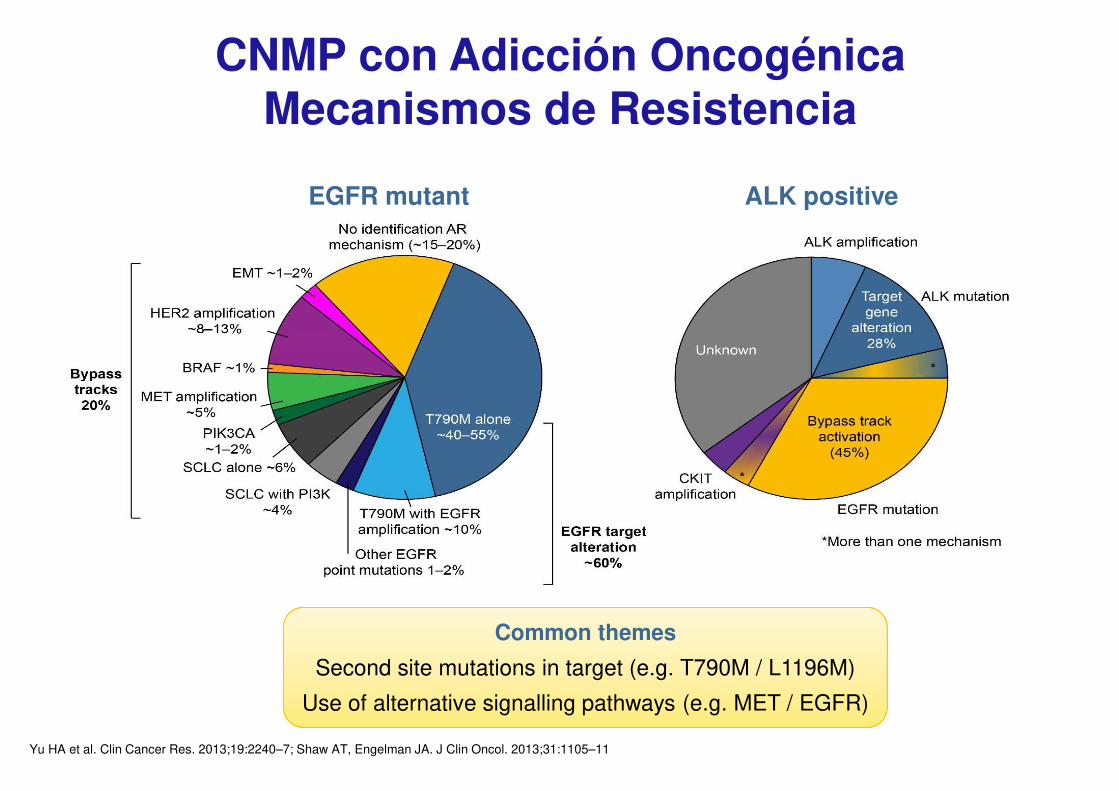
CNMP con Adicción OncogénicaMecanismos de Resistencia
Yu HA et al. Clin Cancer Res. 2013;19:2240–7; Shaw AT, Engelman JA. J Clin Oncol. 2013;31:1105–11
EGFR mutant ALK positive
Common themes
Second site mutations in target (e.g. T790M / L1196M)
Use of alternative signalling pathways (e.g. MET / EGFR)
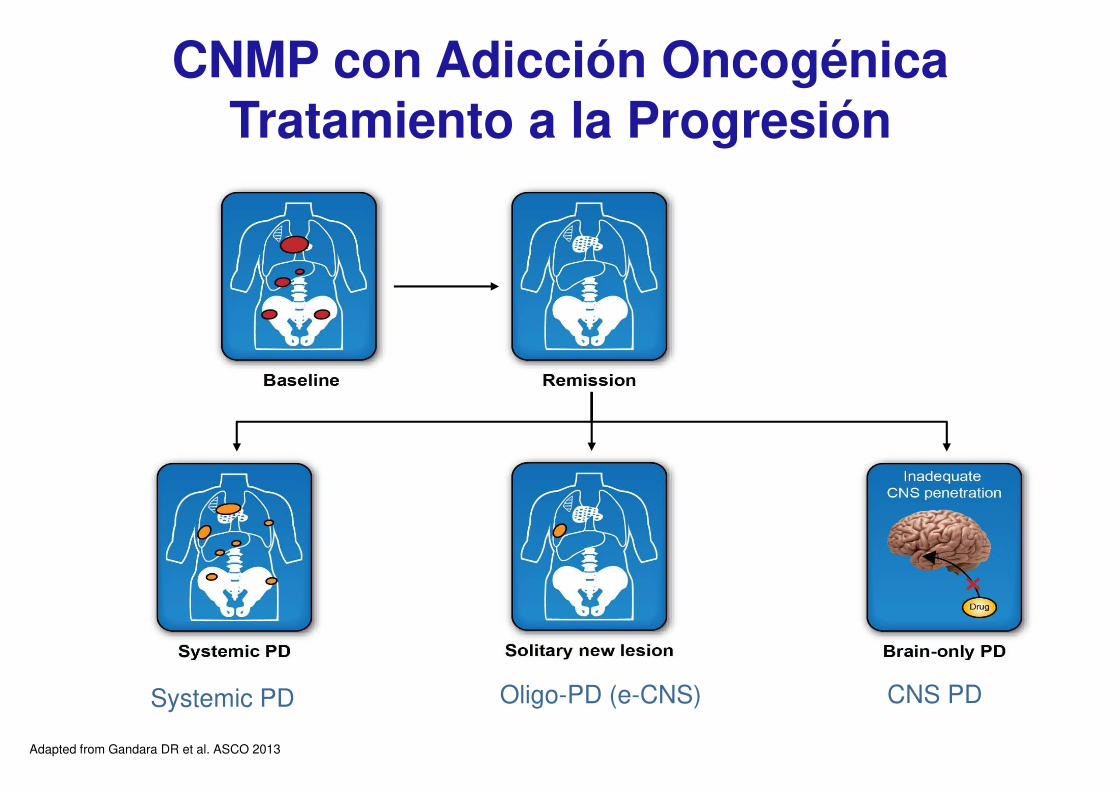
Systemic PD Oligo-PD (e-CNS) CNS PD
Therapy
Adapted from Gandara DR et al. ASCO 2013
CNMP con Adicción OncogénicaTratamiento a la Progresión

CNMP EGFR M+: Resistencia Adquirida
Michalczyk A et al. Bioorg Med Chem. 2008
T790M - Exon 20 Inhibidor específico de T790MOsimertinib
Mok T et al. NEJM 2017
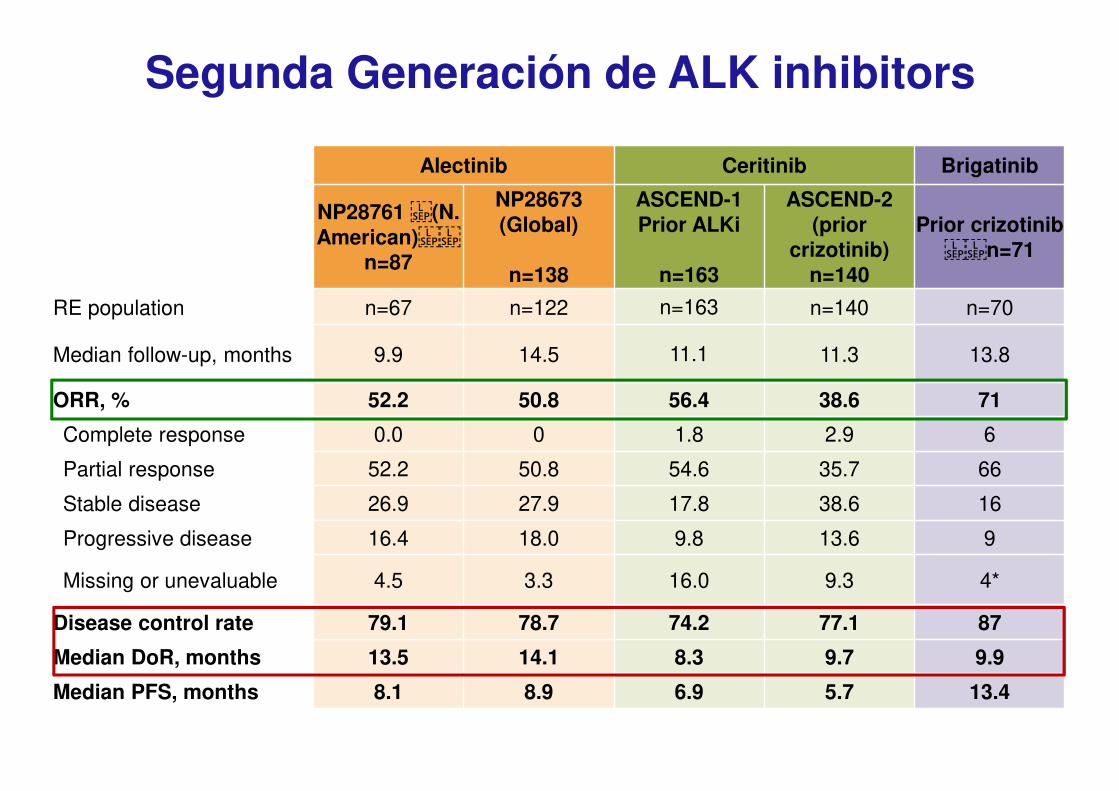
Shaw, et al. WCLC 2015; Barlesi, et al. ECC 2015; Felip, et al. ESMO 2014Mok, et al. ASCO 2015; Gettinger, et al. WCLC 2015; Camidge, et al. ECC 2015
Alectinib Ceritinib Brigatinib
NP28761 (N. American)
n=87
NP28673(Global)
n=138
ASCEND-1Prior ALKi
n=163
ASCEND-2(prior
crizotinib)n=140
Prior crizotinib n=71
RE population n=67 n=122 n=163 n=140 n=70
Median follow-up, months 9.9 14.5 11.1 11.3 13.8
ORR, % 52.2 50.8 56.4 38.6 71
Complete response 0.0 0 1.8 2.9 6
Partial response 52.2 50.8 54.6 35.7 66
Stable disease 26.9 27.9 17.8 38.6 16
Progressive disease 16.4 18.0 9.8 13.6 9
Missing or unevaluable 4.5 3.3 16.0 9.3 4*
Disease control rate 79.1 78.7 74.2 77.1 87
Median DoR, months 13.5 14.1 8.3 9.7 9.9
Median PFS, months 8.1 8.9 6.9 5.7 13.4
Segunda Generación de ALK inhibitors
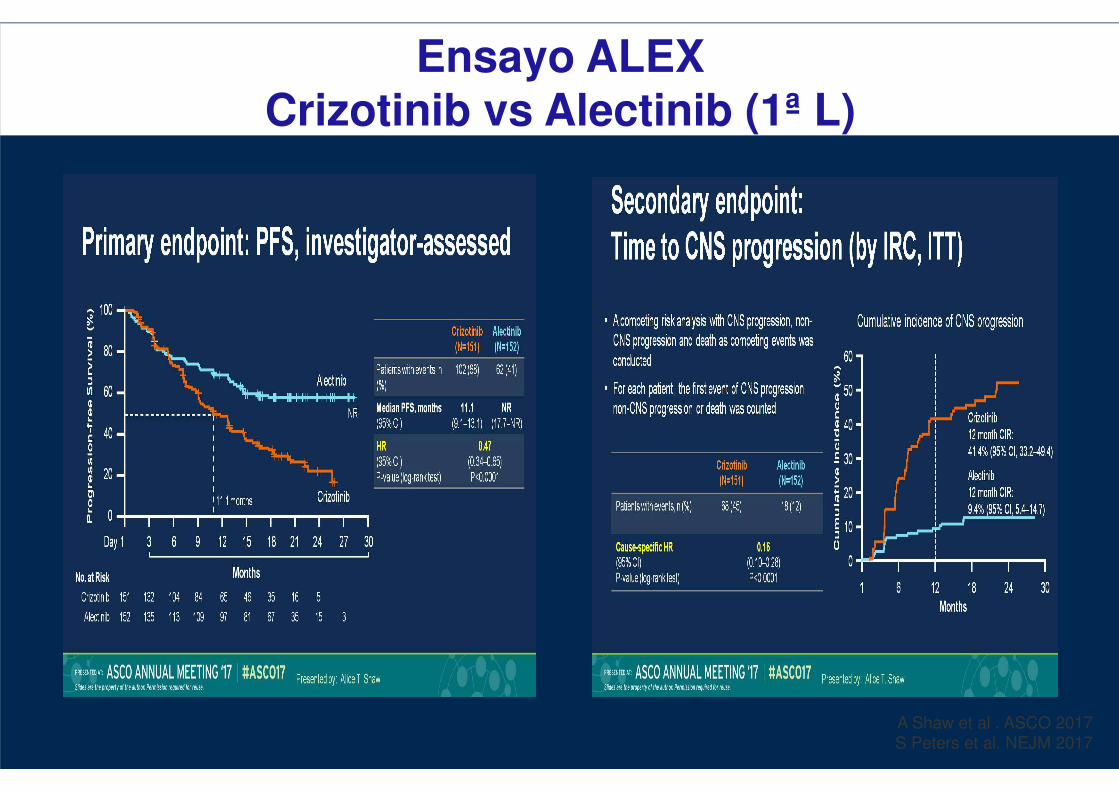
Ensayo ALEXCrizotinib vs Alectinib (1ª L)
A Shaw et al . ASCO 2017
S Peters et al. NEJM 2017

Ensayo FlauraITK de 1ª generación v ITK de T790M
Progression-Free Survival Overall Survival
Soria et al. NEJM 2018
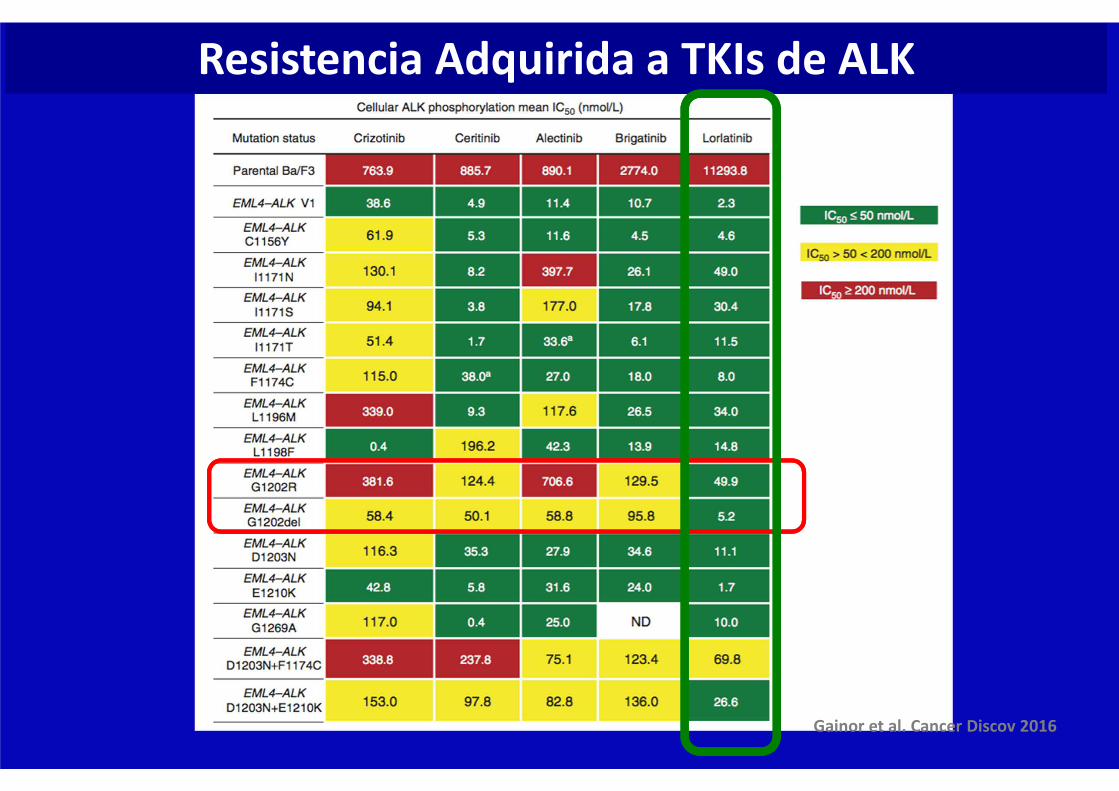
Gainor et al. Cancer Discov 2016
Resistencia Adquirida a TKIs de ALK
NTRK fusions
Adenocarcinoma de pulmón Subtipos con tratamientos específicos

NTRK fusions
Adenocarcinoma de pulmón Subtipos con tratamientos específicos
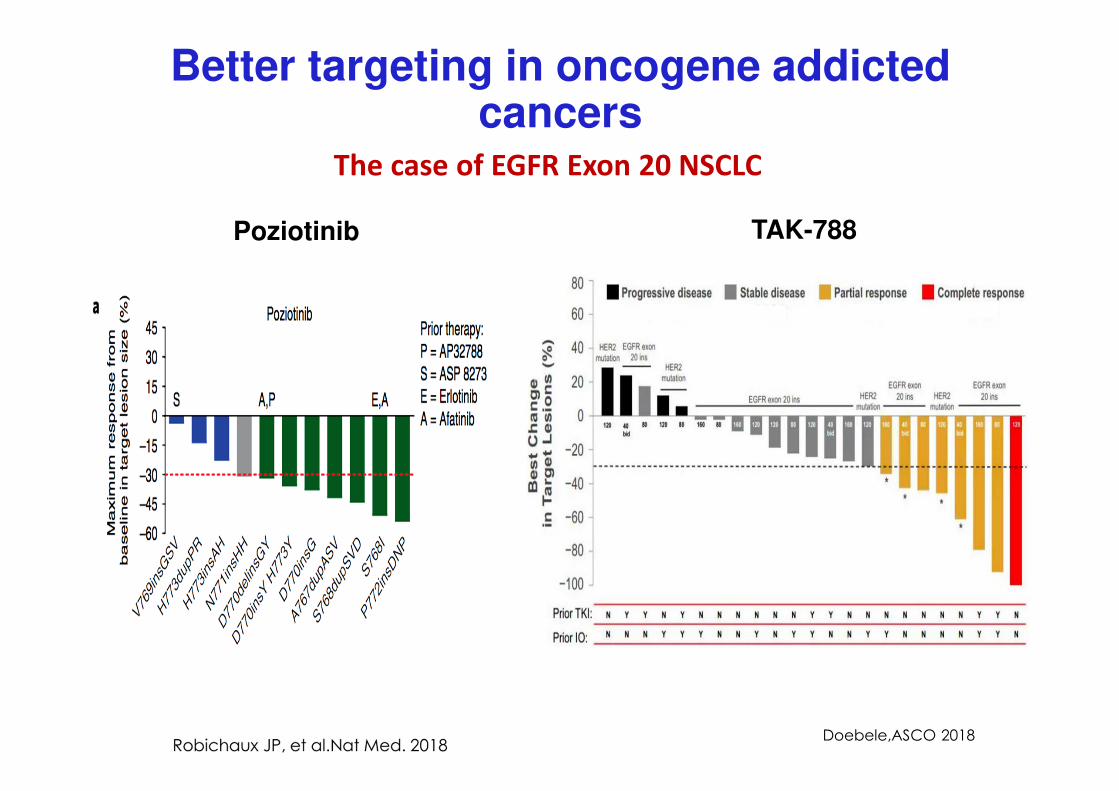
Poziotinib TAK-788
Doebele,ASCO 2018
Better targeting in oncogene addicted cancers
The case of EGFR Exon 20 NSCLC

NTRK fusions
Adenocarcinoma de pulmón Subtipos con tratamientos específicos
Miguel Angel 1500
Visión de la
Oncología
Tradicional
Un CANCER que crece
Visión de la Inmuno-
Oncologia
Un CUERPO
Que deja crecer el cáncer
Una visión diferente del cáncer…
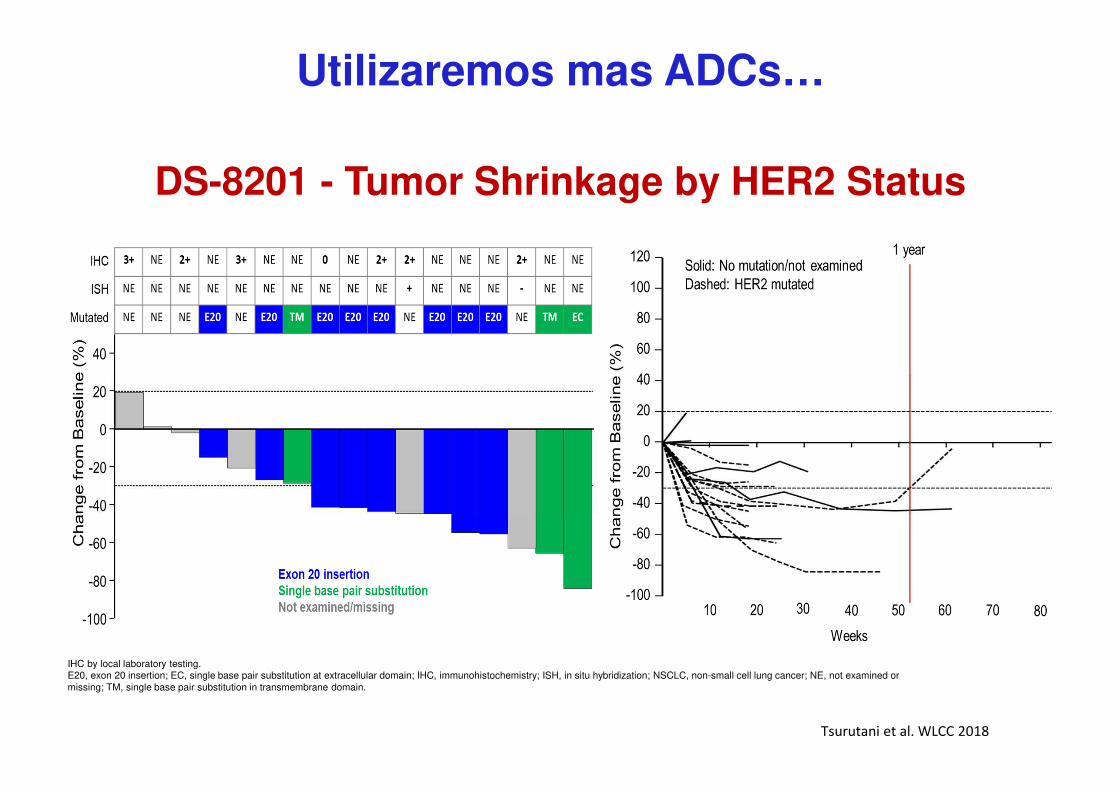
Utilizaremos mas ADCs…
Tsurutani et al. WLCC 2018
DS-8201 - Tumor Shrinkage by HER2 Status
IHC by local laboratory testing.E20, exon 20 insertion; EC, single base pair substitution at extracellular domain; IHC, immunohistochemistry; ISH, in situ hybridization; NSCLC, non-small cell lung cancer; NE, not examined or
missing; TM, single base pair substitution in transmembrane domain.
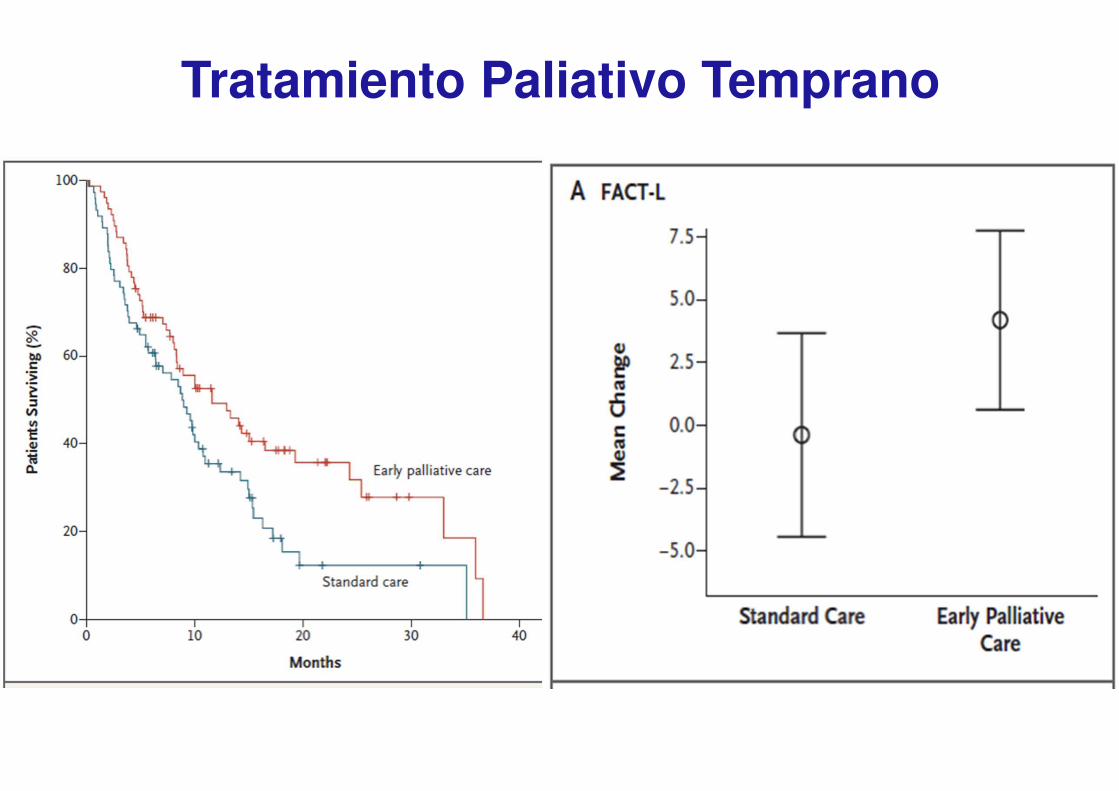
Tratamiento Paliativo Temprano
Temel et al., NEJM 2010