Embed Size (px)
Citation preview
¿Cómo va a modificar la Inmuno-
oncología, el panorama terapéutico
del cáncer?
José Antonio López Martín
HU 12 Octubre. Madrid
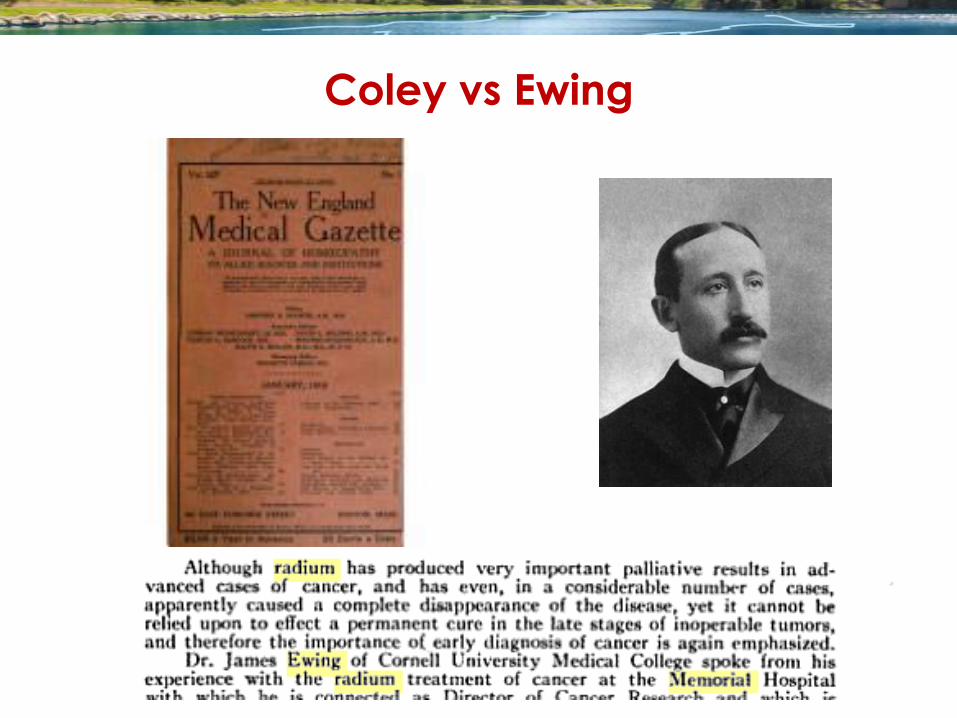
1890: Bessie Dashiel y el Dr Coley
?
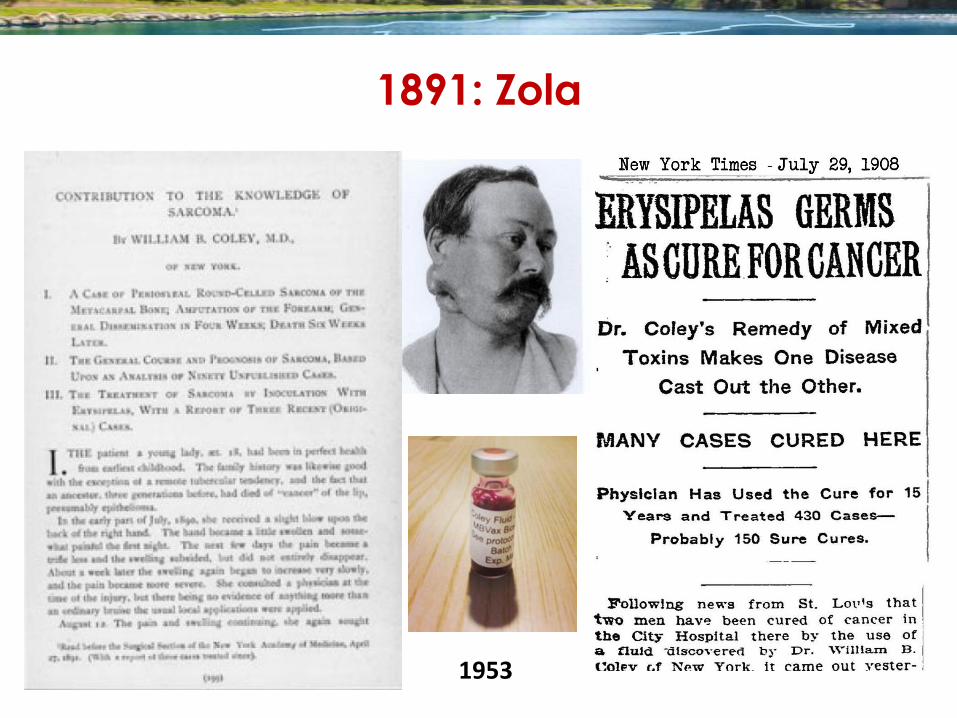
1891: Zola
1953
1953
Coley vs Ewing
? = Rockefeller Jr
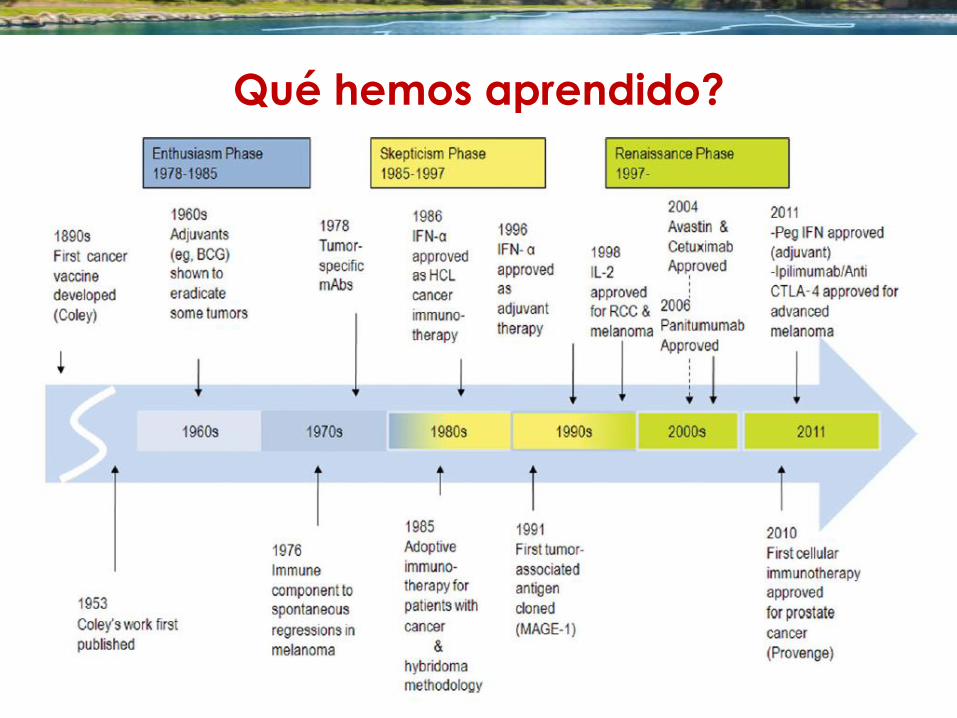
Qué hemos aprendido?
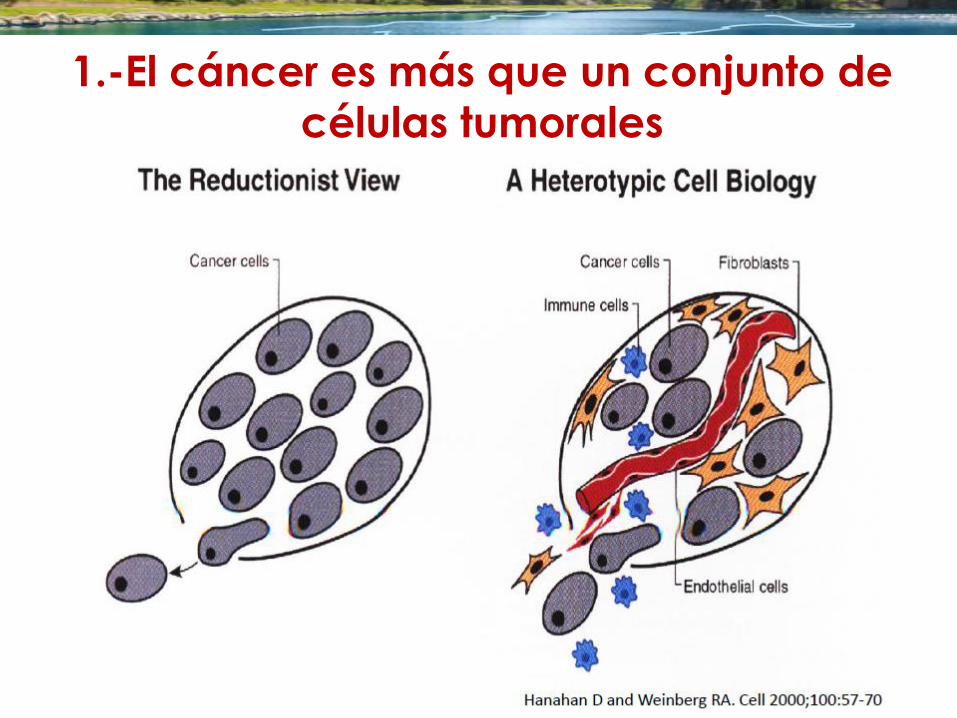
1.-El cáncer es más que un conjunto de
células tumorales
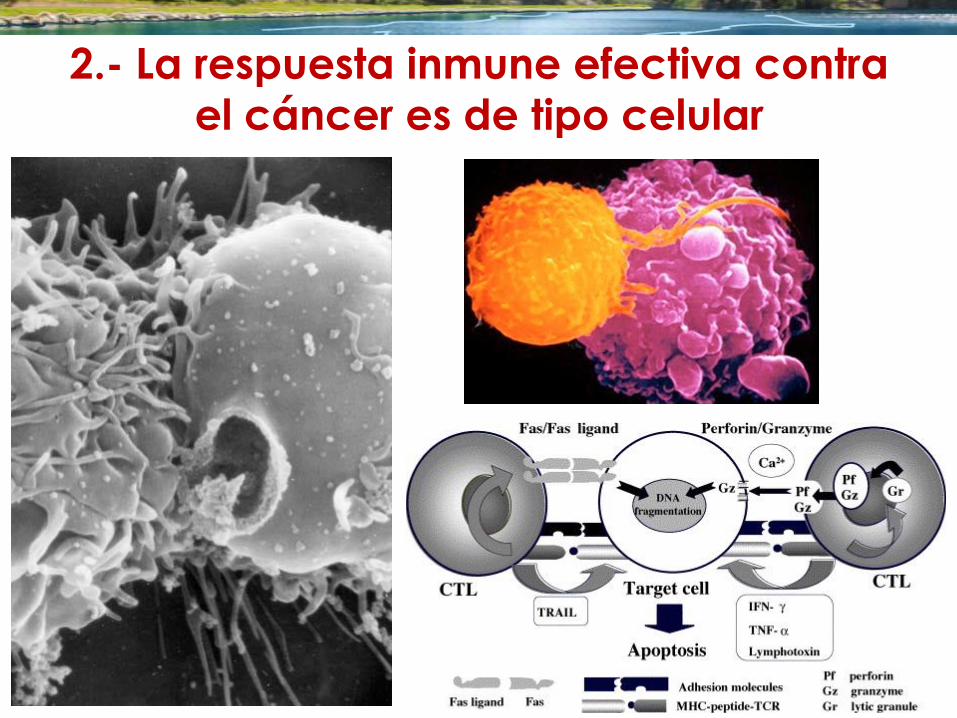
2.- La respuesta inmune efectiva contra
el cáncer es de tipo celular
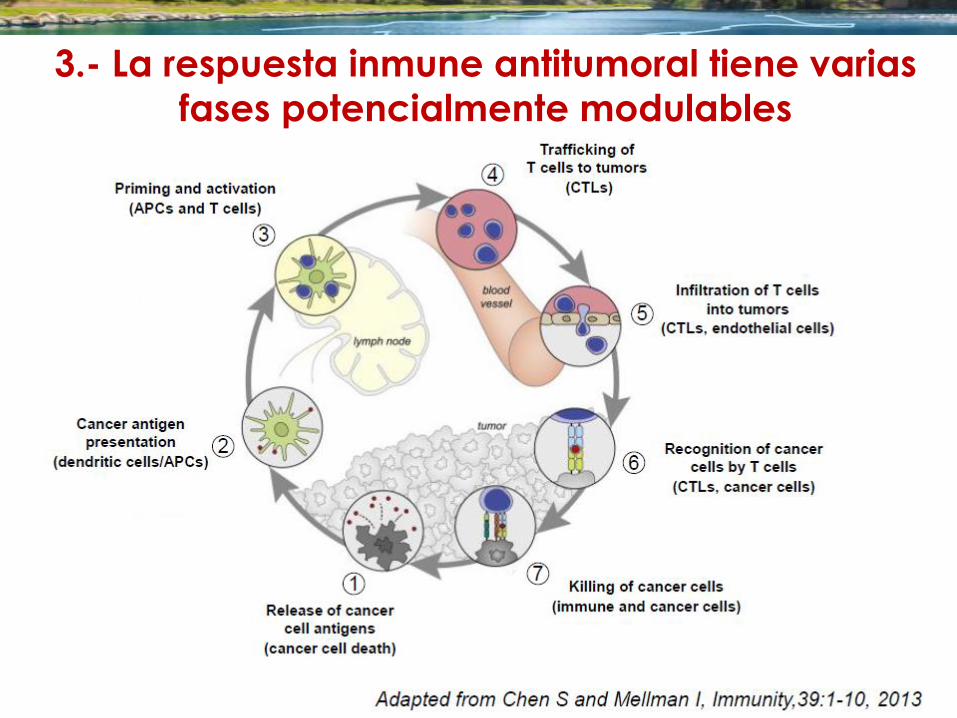
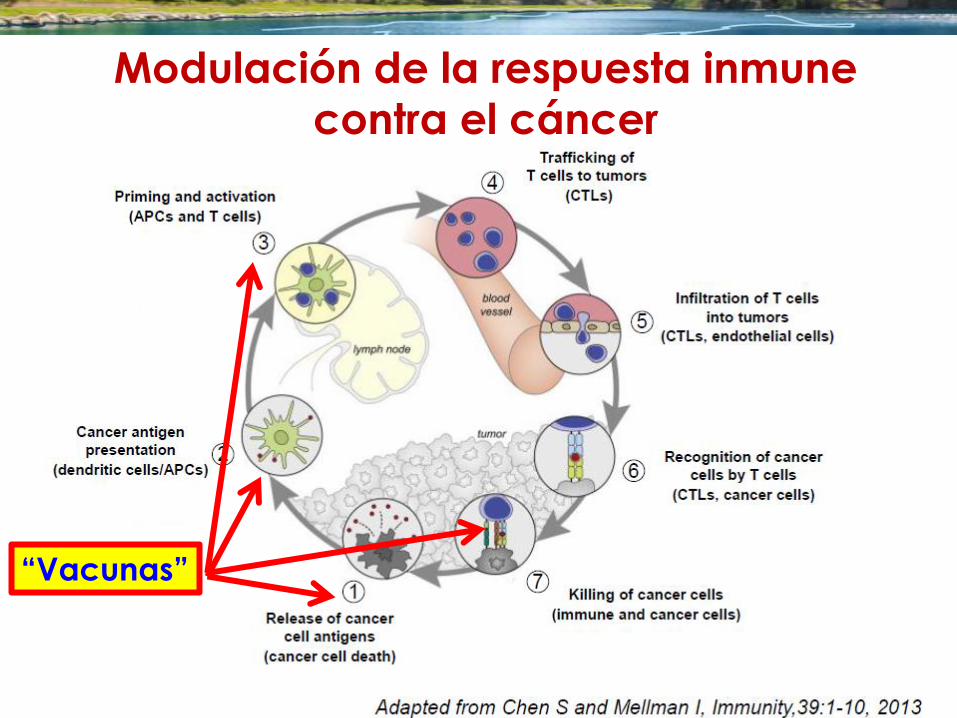
3.- La respuesta inmune antitumoral tiene varias
fases potencialmente modulables
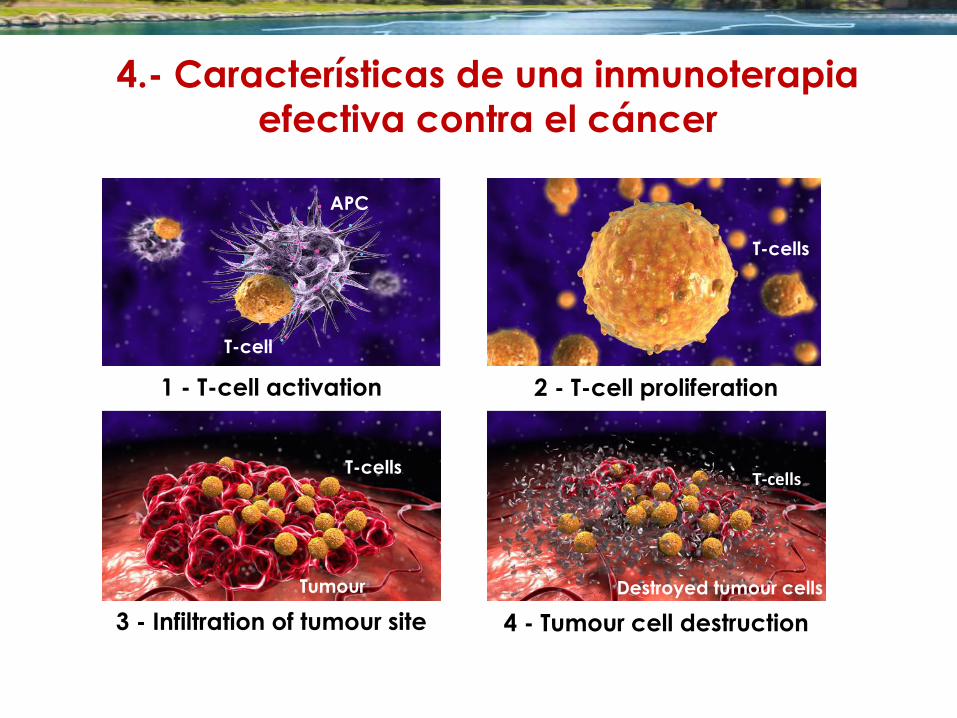
1 - T-cell activation 2 - T-cell proliferation
3 - Infiltration of tumour site 4 - Tumour cell destruction
T-cell
APC
T-cells
Destroyed tumour cells
T-cells
T-cells
Tumour
4.- Características de una inmunoterapia
efectiva contra el cáncer

5.- El tumor puede generar supresión de la
respuesta inmune
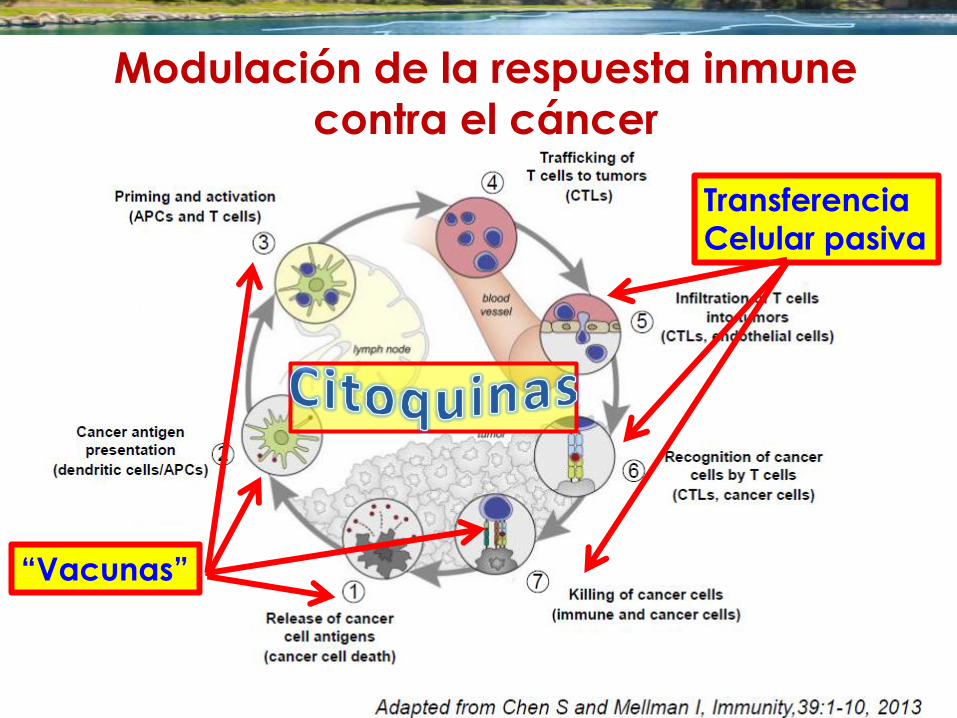
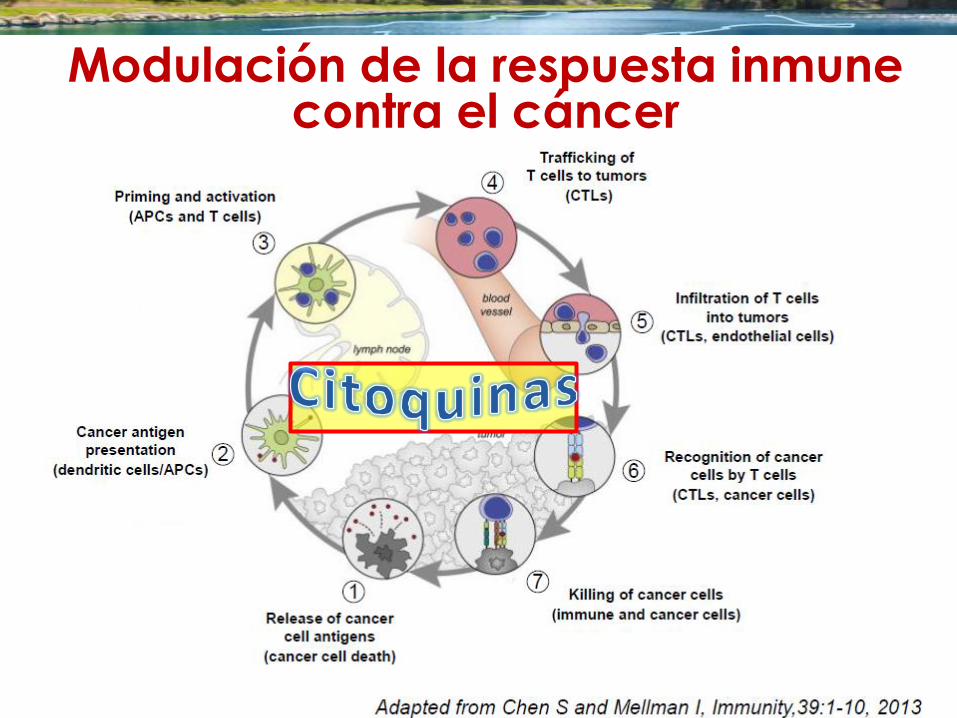
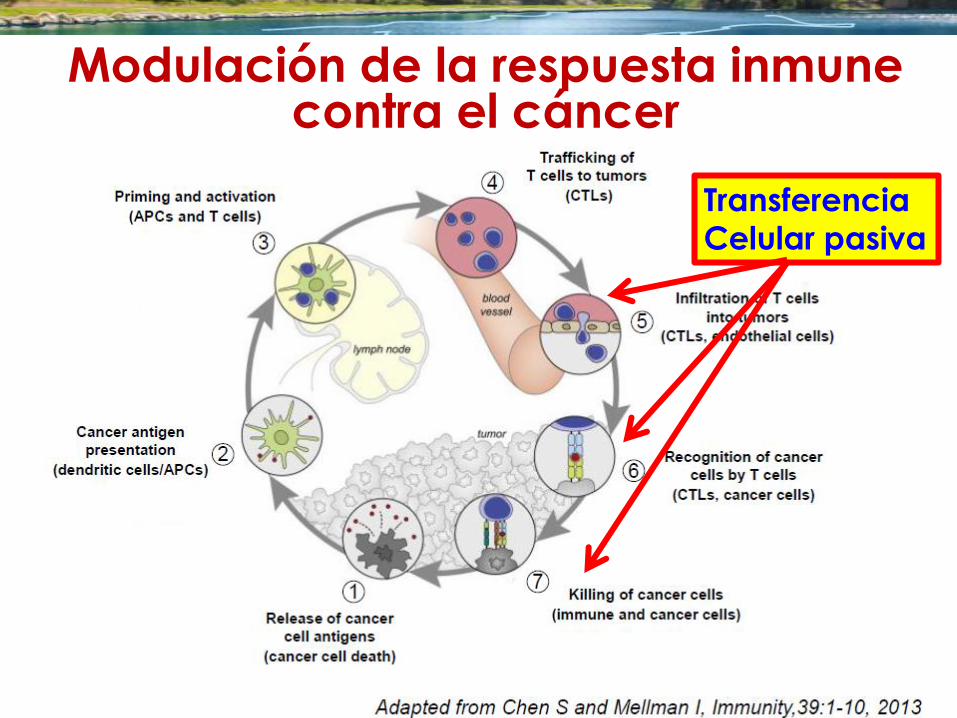
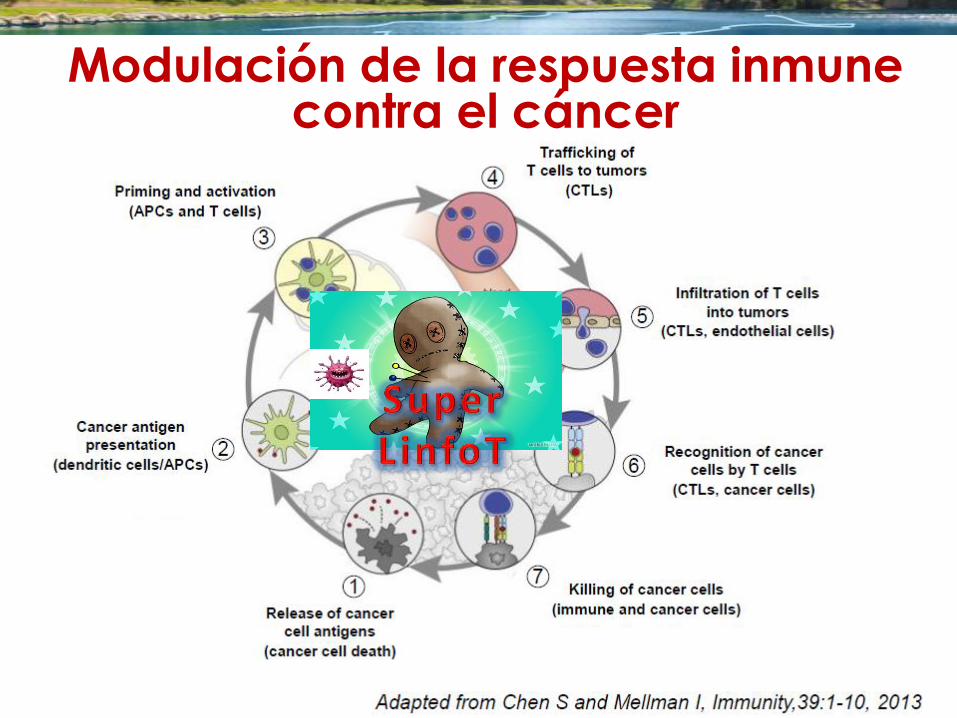
Modulación de la respuesta inmune
contra el cáncer
“Vacunas”
Transferencia
Celular pasiva
Modulación de la respuesta inmune
contra el cáncer
“Vacunas”
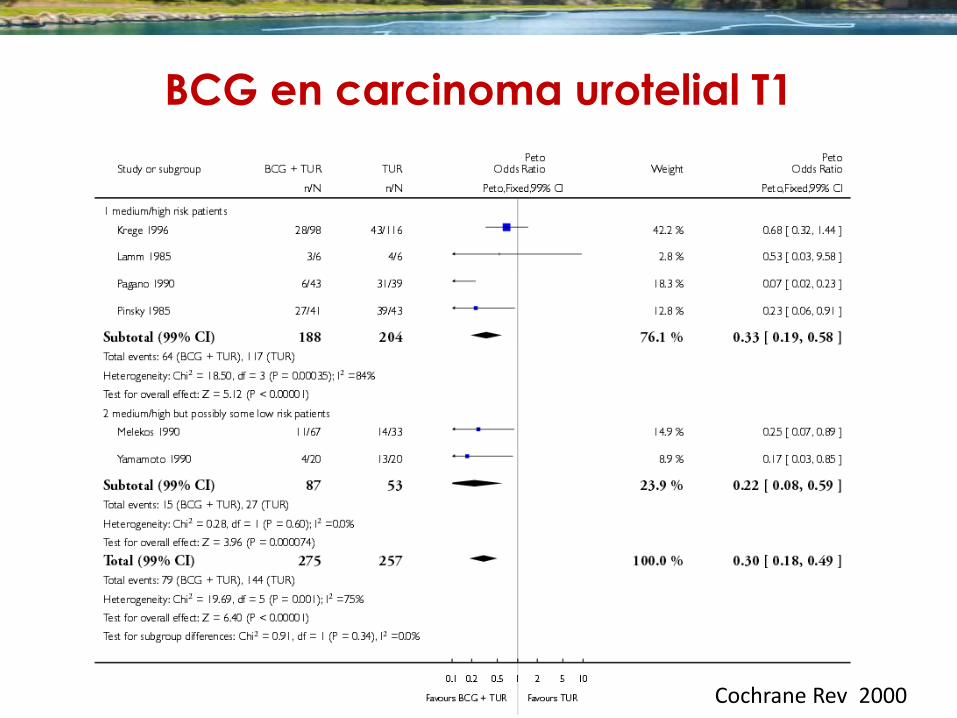
BCG en carcinoma urotelial T1
Cochrane Rev 2000
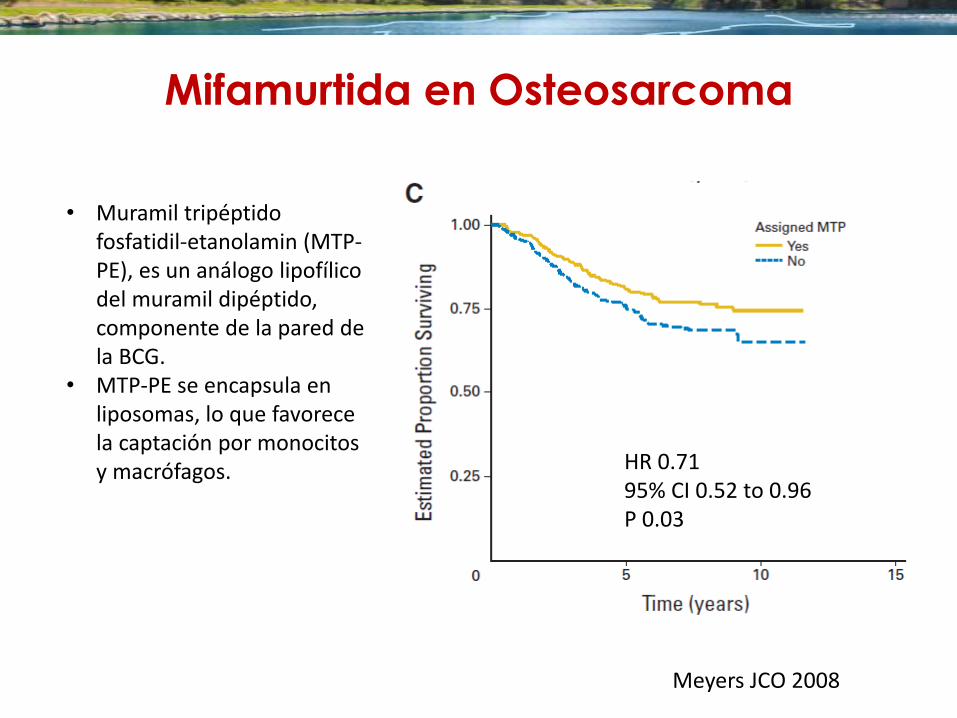
Mifamurtida en Osteosarcoma
• Muramil tripéptido fosfatidil-etanolamin (MTP-PE), es un análogo lipofílico del muramil dipéptido, componente de la pared de la BCG.
• MTP-PE se encapsula en liposomas, lo que favorece la captación por monocitos y macrófagos.
Meyers JCO 2008
HR 0.71 95% CI 0.52 to 0.96 P 0.03
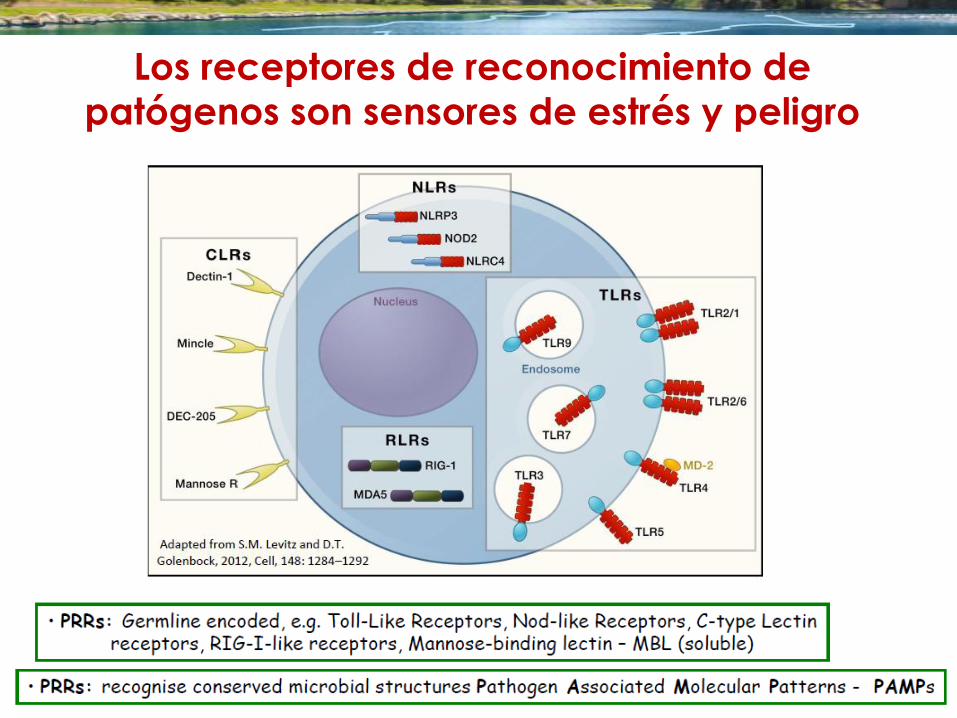
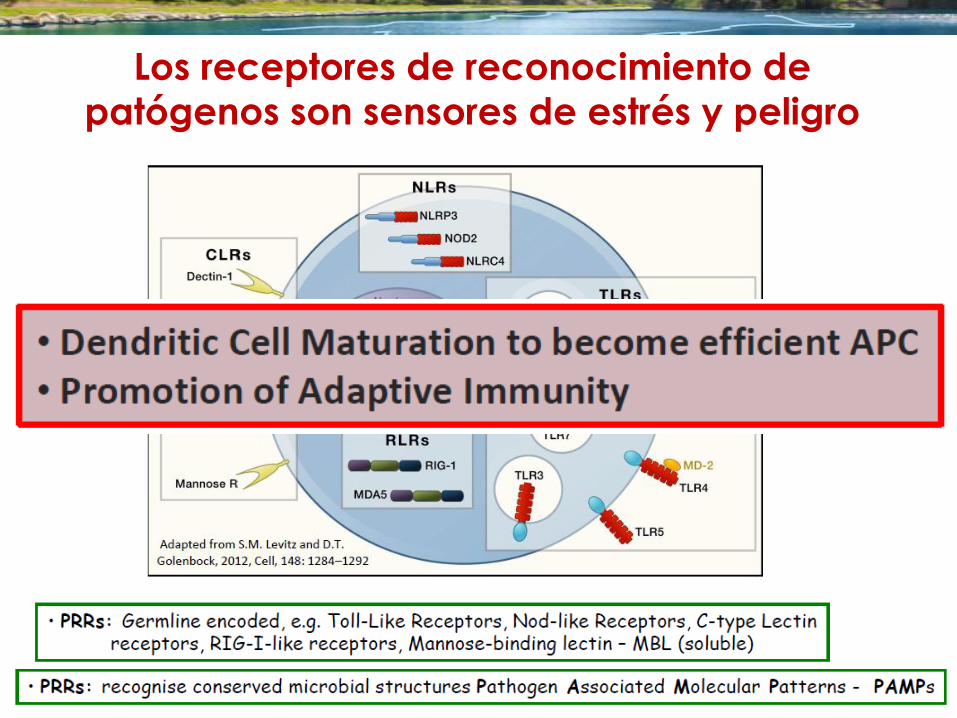
Los receptores de reconocimiento de
patógenos son sensores de estrés y peligro
Los receptores de reconocimiento de
patógenos son sensores de estrés y peligro
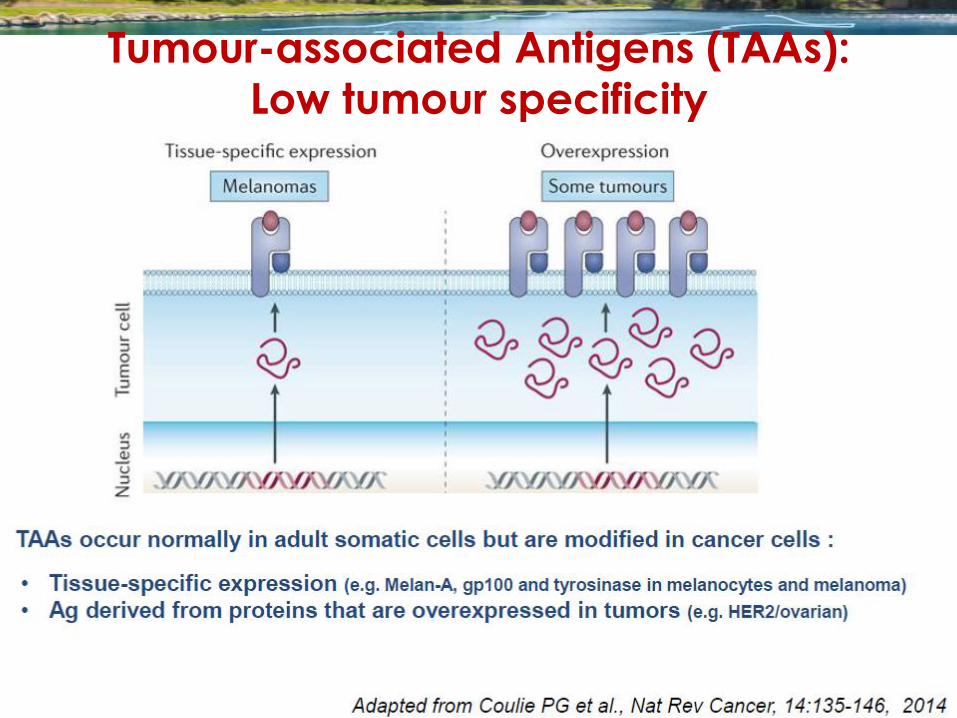
Tumour-associated Antigens (TAAs):
Low tumour specificity
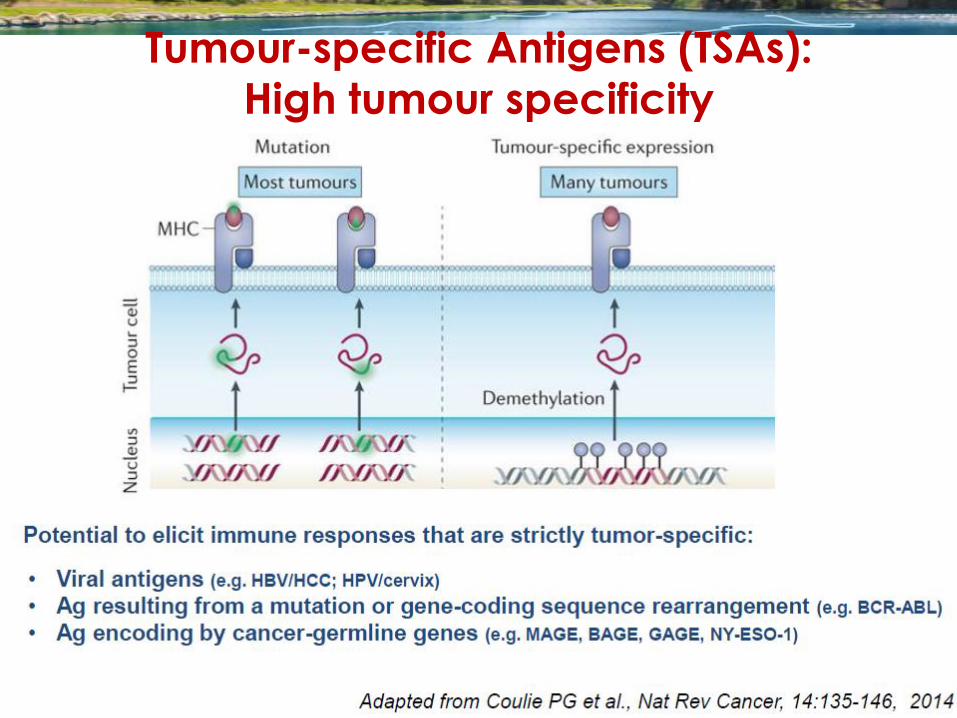
Tumour-specific Antigens (TSAs):
High tumour specificity
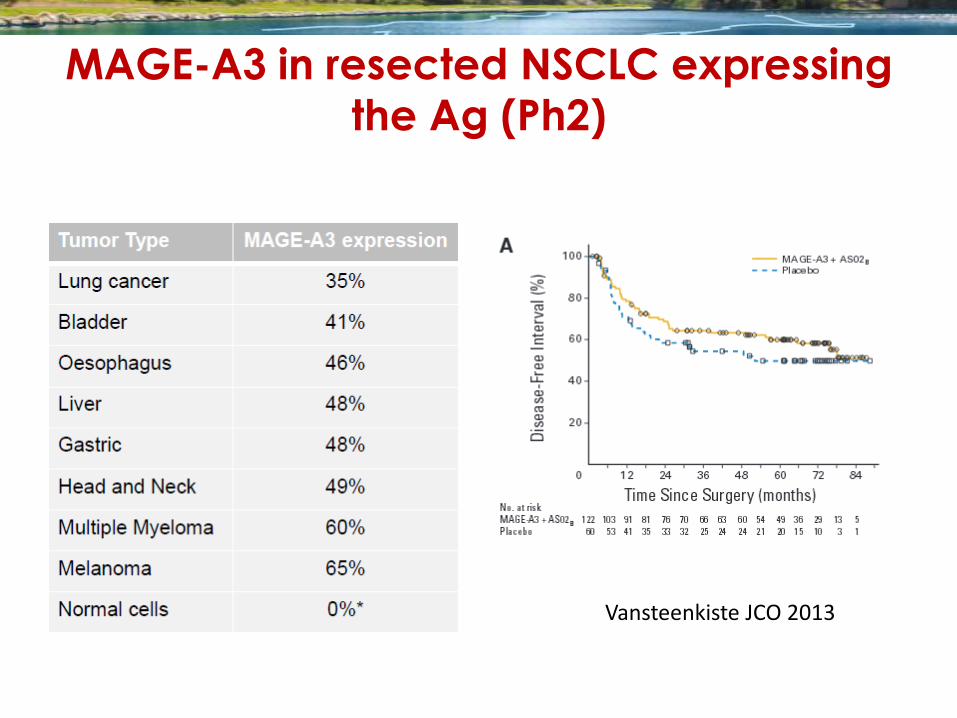
MAGE-A3 in resected NSCLC expressing
the Ag (Ph2)
Vansteenkiste JCO 2013
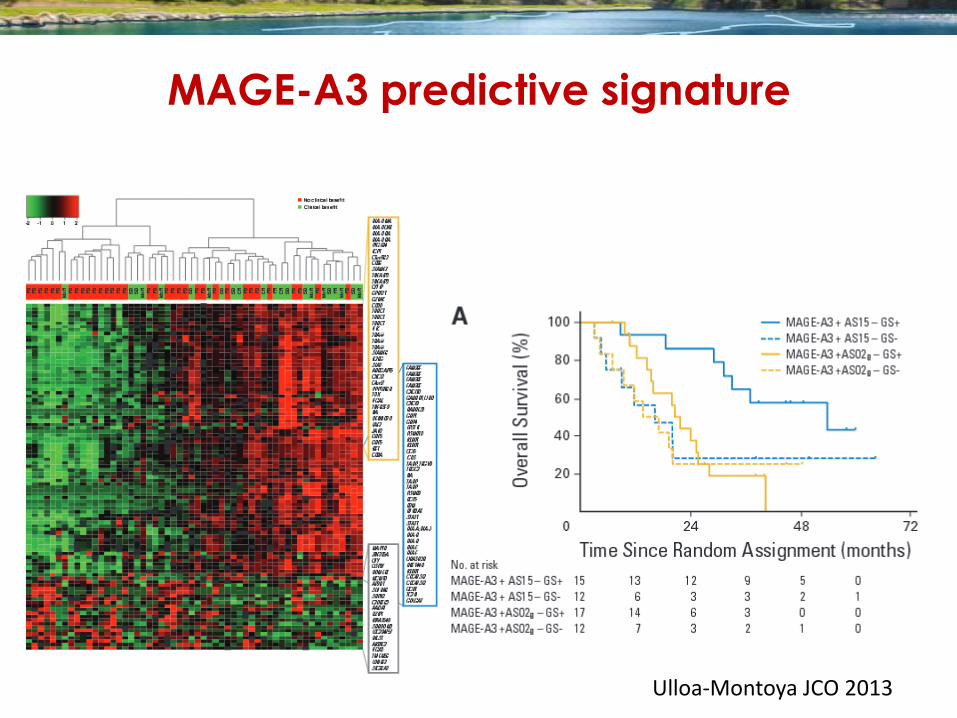
MAGE-A3 predictive signature
Ulloa-Montoya JCO 2013
Vacunas antitumorales: comentarios
• Inducen reacción inmune contra la vacuna.. ¿contra el tumor?
• El sistema inmune reconoce sobre todo “neo-antigenos” secundarios a mutaciones o Dichos antígenos deben ser personalizados
o Las vacunas idealmente deben implicar tumor autólogo
• La mayoría de los tumores inmunogénicos son “autovacunas”. El problema es la supresión de la respuesta inmune
• La vacuna puede generar una respuesta inmune efectiva, pero el estroma supresor la extingue
• Conclusión: Las vacunas solas no tendrán un papel relevante si no se les asocia otros fármacos que controlen los mecanismos reguladores de la respuesta inmune
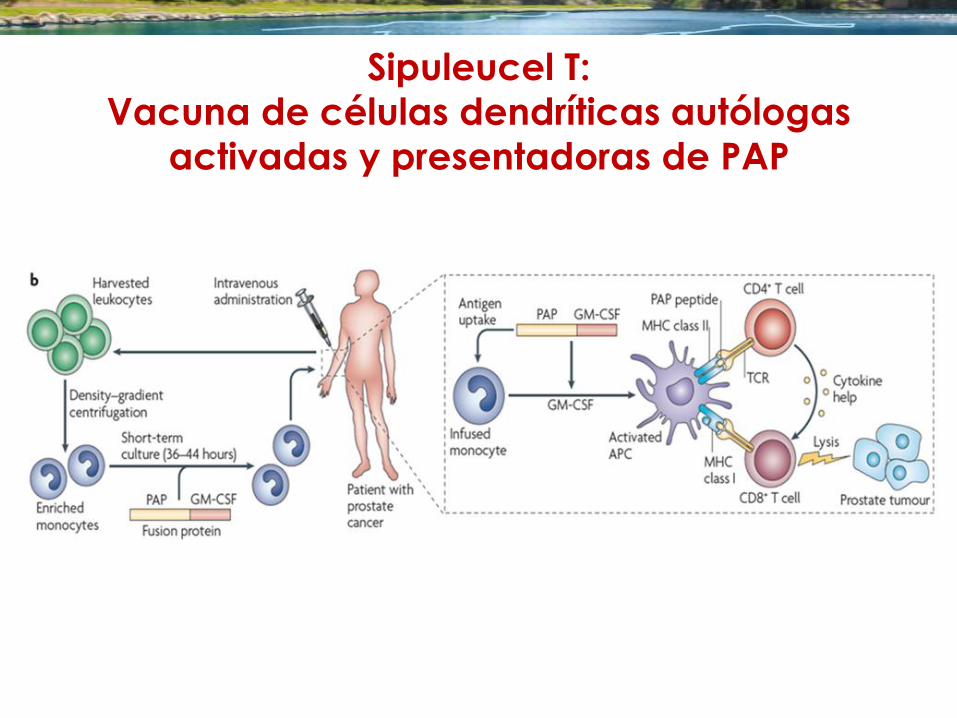
Sipuleucel T:
Vacuna de células dendríticas autólogas
activadas y presentadoras de PAP
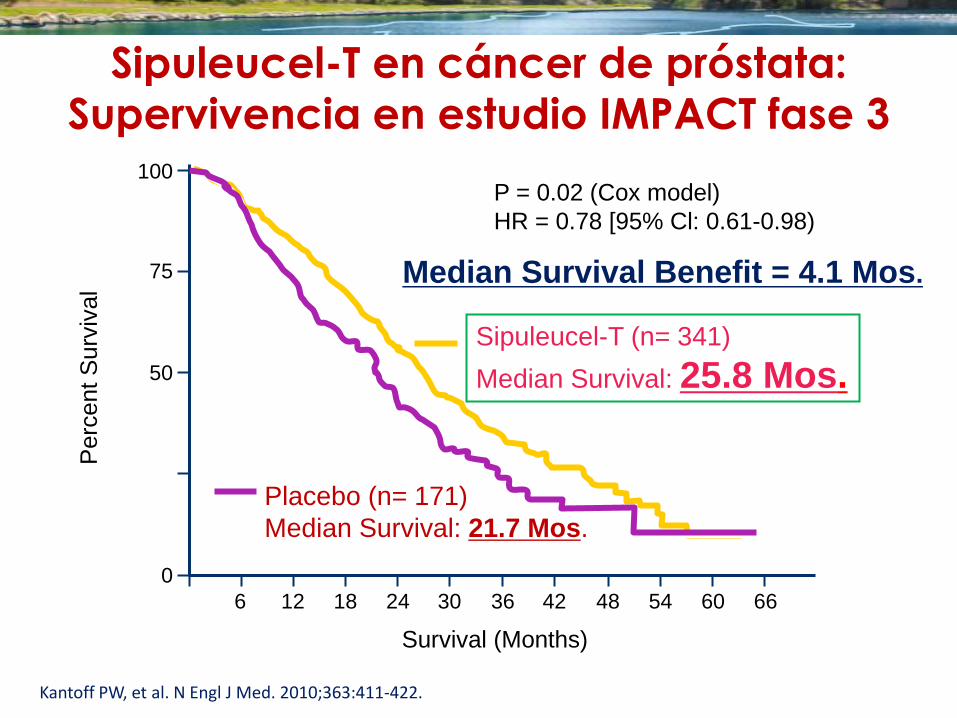
Sipuleucel-T en cáncer de próstata:
Supervivencia en estudio IMPACT fase 3
Kantoff PW, et al. N Engl J Med. 2010;363:411-422.
0
25
50
75
100
0 6 12 18 24 30 36 42 48 54 60 66
Survival (Months)
Perc
ent
Surv
ival
Placebo (n= 171)
Median Survival: 21.7 Mos.
Sipuleucel-T (n= 341)
Median Survival: 25.8 Mos.
P = 0.02 (Cox model)
HR = 0.78 [95% Cl: 0.61-0.98)
Median Survival Benefit = 4.1 Mos.
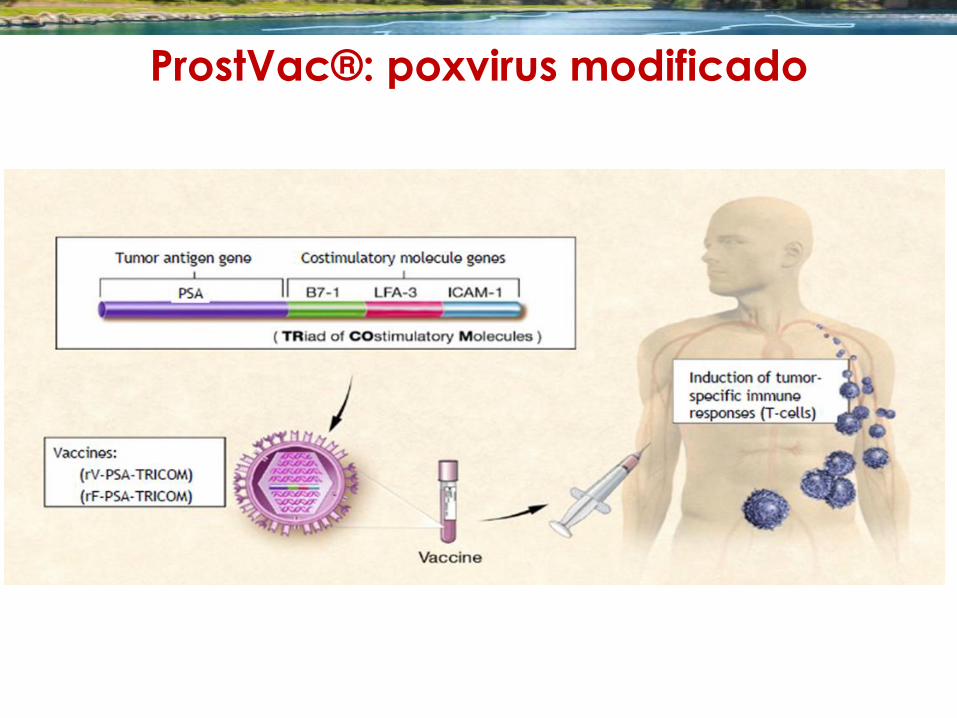
ProstVac®: poxvirus modificado
0
40
60
80
100
0 12 24 60
Time (Months)
ove
rall
Surv
ival
(%
)
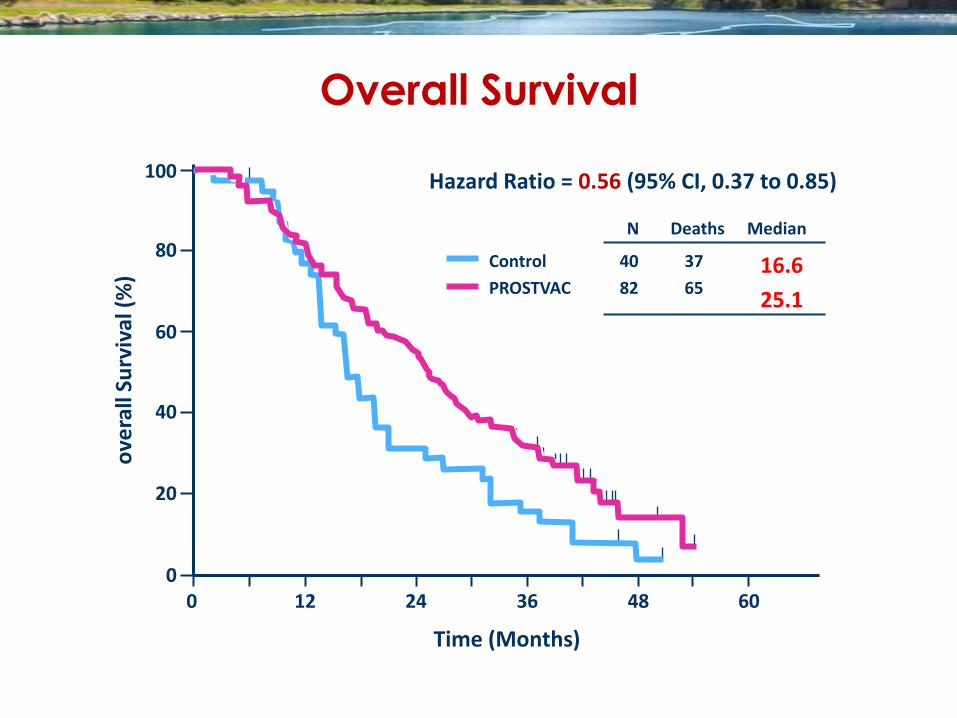
Hazard Ratio = 0.56 (95% CI, 0.37 to 0.85)
20
Control
PROSTVAC
40
82
37
65 16.6
25.1
N Deaths Median
36 48
Overall Survival
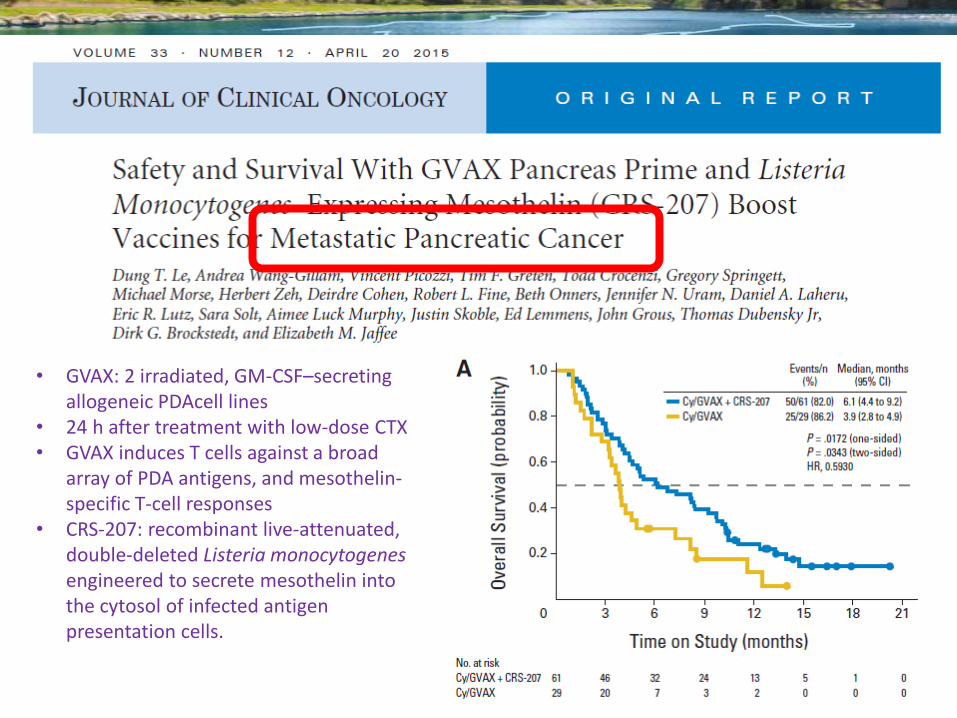
• GVAX: 2 irradiated, GM-CSF–secreting allogeneic PDAcell lines
• 24 h after treatment with low-dose CTX • GVAX induces T cells against a broad
array of PDA antigens, and mesothelin-specific T-cell responses
• CRS-207: recombinant live-attenuated, double-deleted Listeria monocytogenes engineered to secrete mesothelin into the cytosol of infected antigen presentation cells.
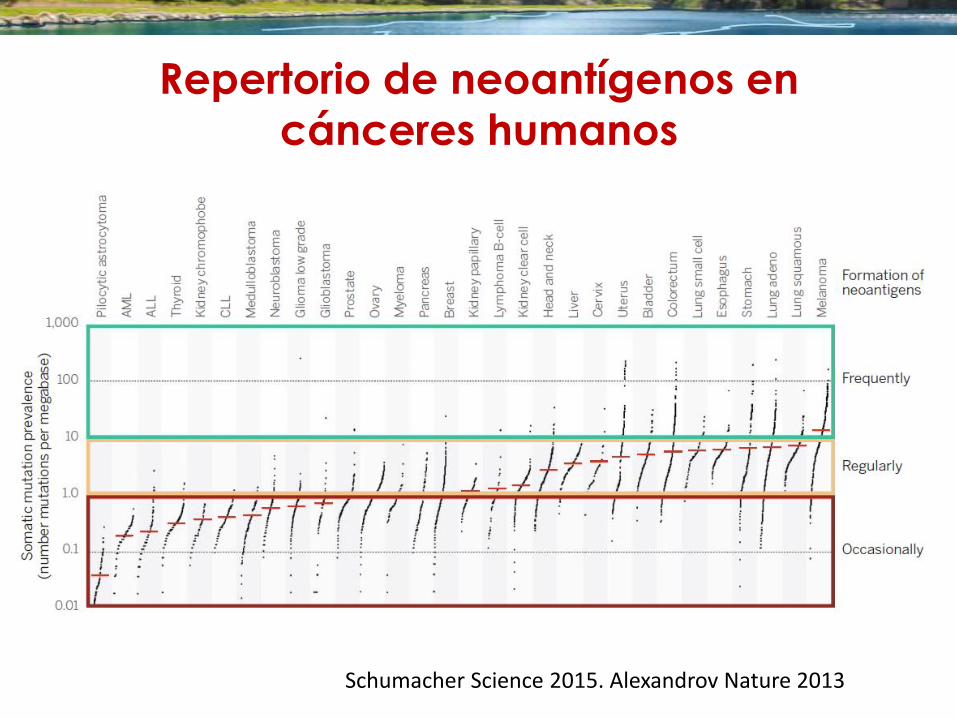
Repertorio de neoantígenos en
cánceres humanos
Schumacher Science 2015. Alexandrov Nature 2013
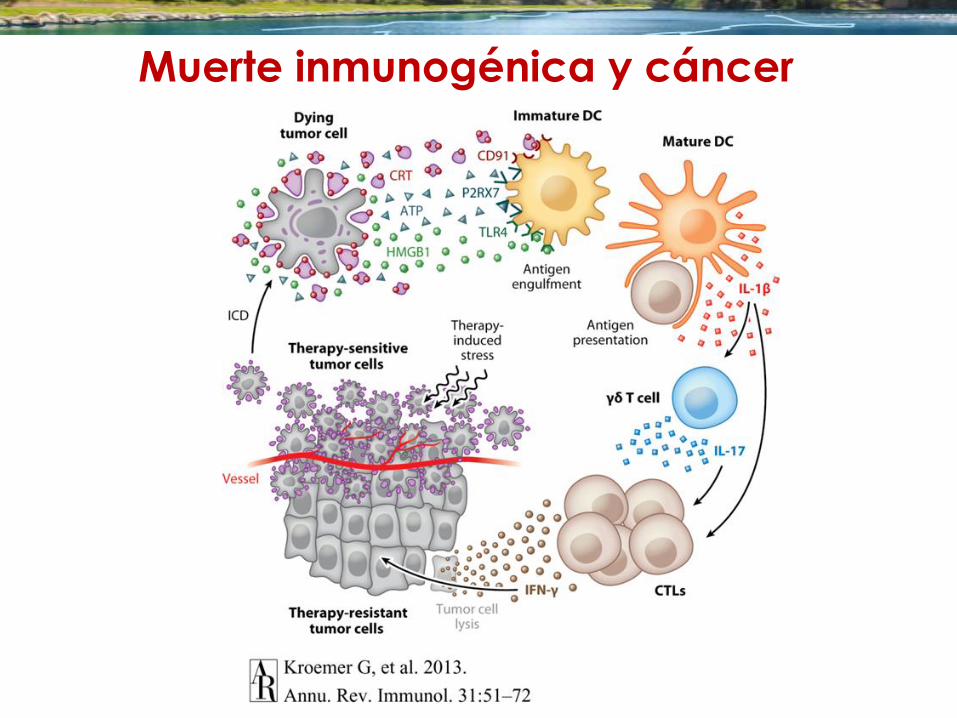
Muerte inmunogénica y cáncer
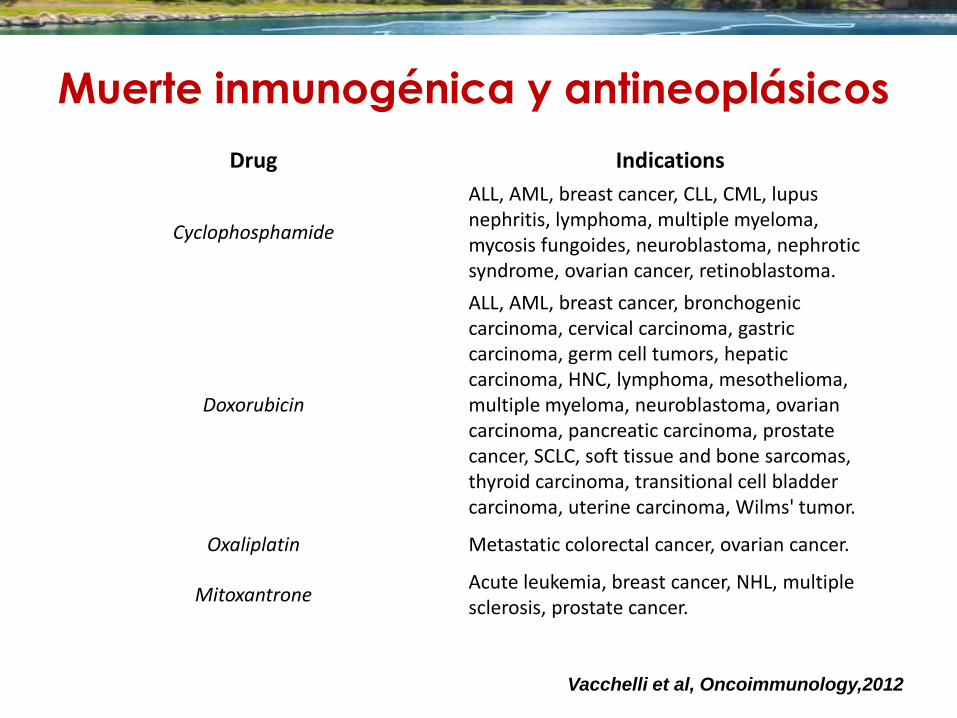
Drug Indications
Cyclophosphamide
ALL, AML, breast cancer, CLL, CML, lupus nephritis, lymphoma, multiple myeloma, mycosis fungoides, neuroblastoma, nephrotic syndrome, ovarian cancer, retinoblastoma.
Doxorubicin
ALL, AML, breast cancer, bronchogenic carcinoma, cervical carcinoma, gastric carcinoma, germ cell tumors, hepatic carcinoma, HNC, lymphoma, mesothelioma, multiple myeloma, neuroblastoma, ovarian carcinoma, pancreatic carcinoma, prostate cancer, SCLC, soft tissue and bone sarcomas, thyroid carcinoma, transitional cell bladder carcinoma, uterine carcinoma, Wilms' tumor.
Oxaliplatin Metastatic colorectal cancer, ovarian cancer.
Mitoxantrone Acute leukemia, breast cancer, NHL, multiple sclerosis, prostate cancer.
Vacchelli et al, Oncoimmunology,2012
Muerte inmunogénica y antineoplásicos

ABSCOPAL, from the latin
“ab scopus”, away from the target.
MOLE, RH BR. J. RADIOL 1953 :26 (305):234-241
Muerte inmunogénica y radioterapia
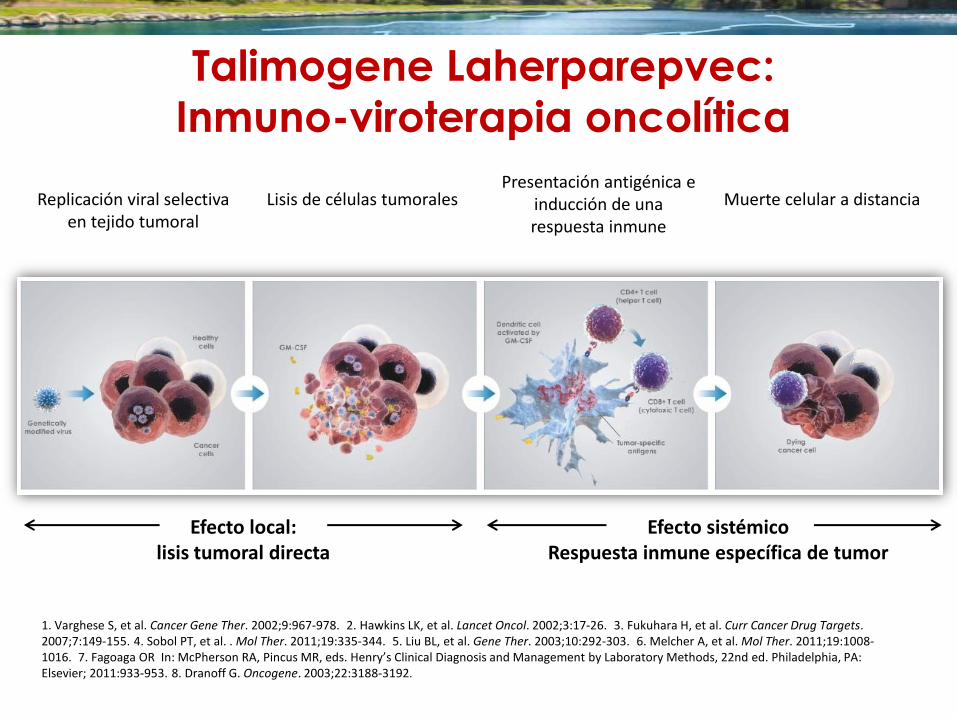
Talimogene Laherparepvec:
Inmuno-viroterapia oncolítica
Efecto local: lisis tumoral directa
Efecto sistémico Respuesta inmune específica de tumor
Replicación viral selectiva en tejido tumoral
Lisis de células tumorales Presentación antigénica e
inducción de una respuesta inmune
Muerte celular a distancia
1. Varghese S, et al. Cancer Gene Ther. 2002;9:967-978. 2. Hawkins LK, et al. Lancet Oncol. 2002;3:17-26. 3. Fukuhara H, et al. Curr Cancer Drug Targets. 2007;7:149-155. 4. Sobol PT, et al. . Mol Ther. 2011;19:335-344. 5. Liu BL, et al. Gene Ther. 2003;10:292-303. 6. Melcher A, et al. Mol Ther. 2011;19:1008-1016. 7. Fagoaga OR In: McPherson RA, Pincus MR, eds. Henry’s Clinical Diagnosis and Management by Laboratory Methods, 22nd ed. Philadelphia, PA: Elsevier; 2011:933-953. 8. Dranoff G. Oncogene. 2003;22:3188-3192.
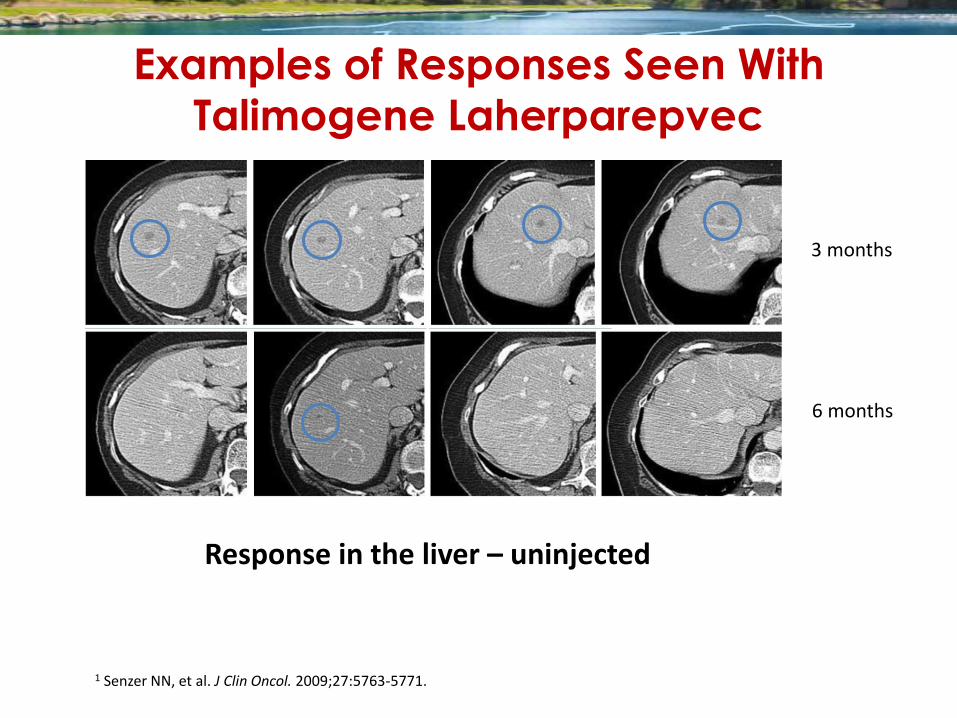
3 months
6 months
Response in the liver – uninjected
Examples of Responses Seen With
Talimogene Laherparepvec
1 Senzer NN, et al. J Clin Oncol. 2009;27:5763-5771.
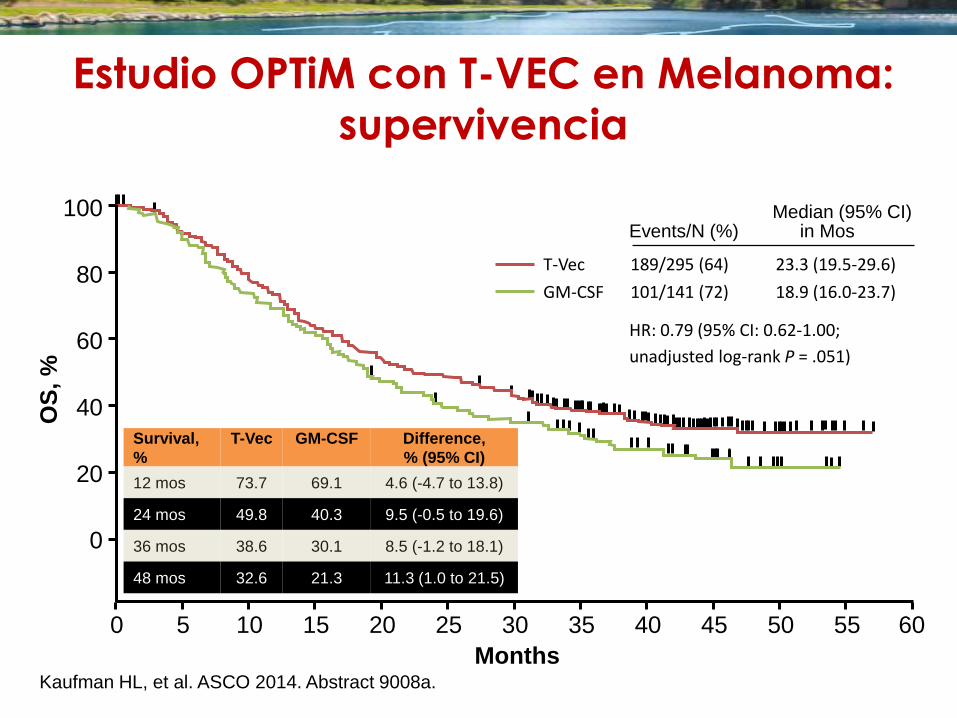
Estudio OPTiM con T-VEC en Melanoma:
supervivencia
Survival,
%
T-Vec GM-CSF Difference,
% (95% CI)
12 mos 73.7 69.1 4.6 (-4.7 to 13.8)
24 mos 49.8 40.3 9.5 (-0.5 to 19.6)
36 mos 38.6 30.1 8.5 (-1.2 to 18.1)
48 mos 32.6 21.3 11.3 (1.0 to 21.5)
Events/N (%) Median (95% CI)
in Mos
T-Vec 189/295 (64) 23.3 (19.5-29.6)
GM-CSF 101/141 (72) 18.9 (16.0-23.7)
HR: 0.79 (95% CI: 0.62-1.00;
unadjusted log-rank P = .051)
Kaufman HL, et al. ASCO 2014. Abstract 9008a.
100
80
60
40
20
0
OS
, %
60 0 10 15 20 5 25 30 35 40 45 50 55
Months
Modulación de la respuesta inmune contra el cáncer
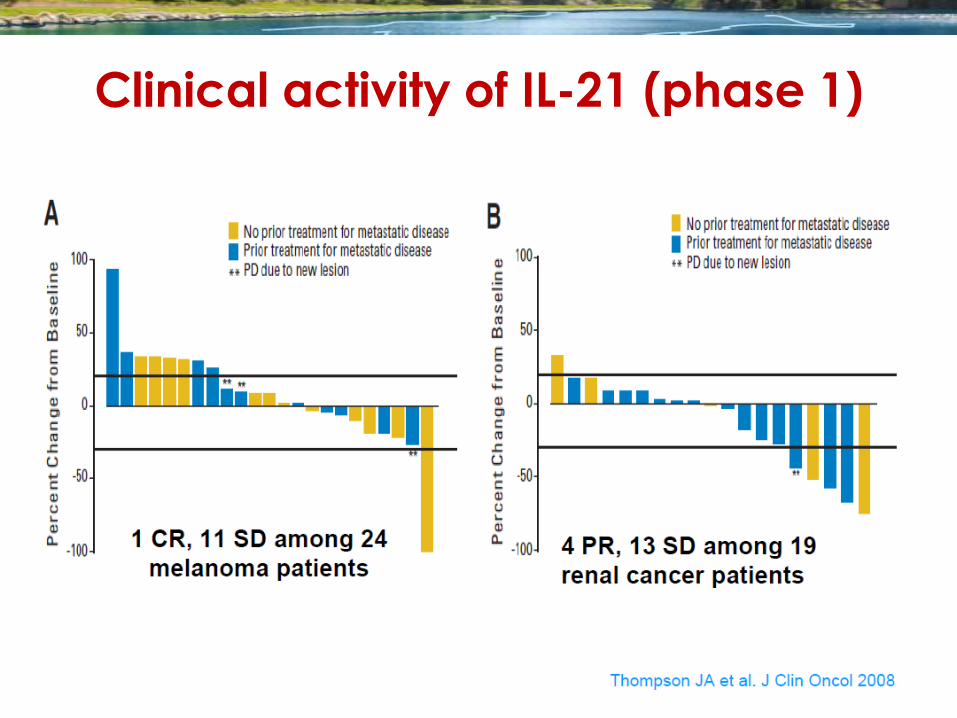
Clinical activity of IL-21 (phase 1)
Modulación de la respuesta inmune contra el cáncer
Transferencia
Celular pasiva
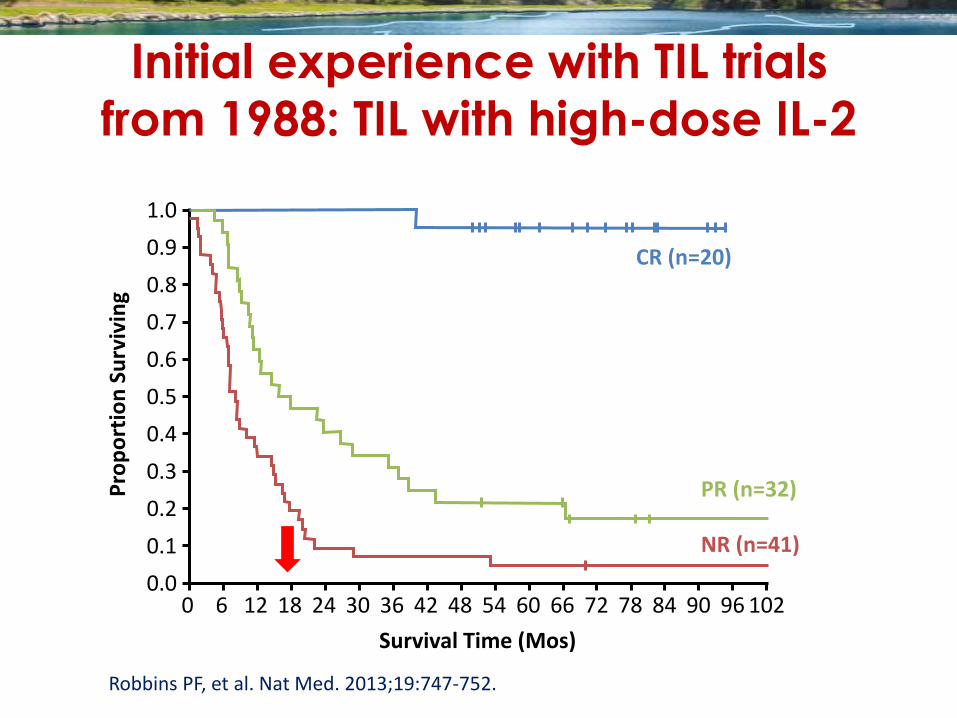
Robbins PF, et al. Nat Med. 2013;19:747-752.
Pro
po
rtio
n S
urv
ivin
g
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Survival Time (Mos)
102 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96
PR (n=32)
NR (n=41)
CR (n=20)
Initial experience with TIL trials
from 1988: TIL with high-dose IL-2
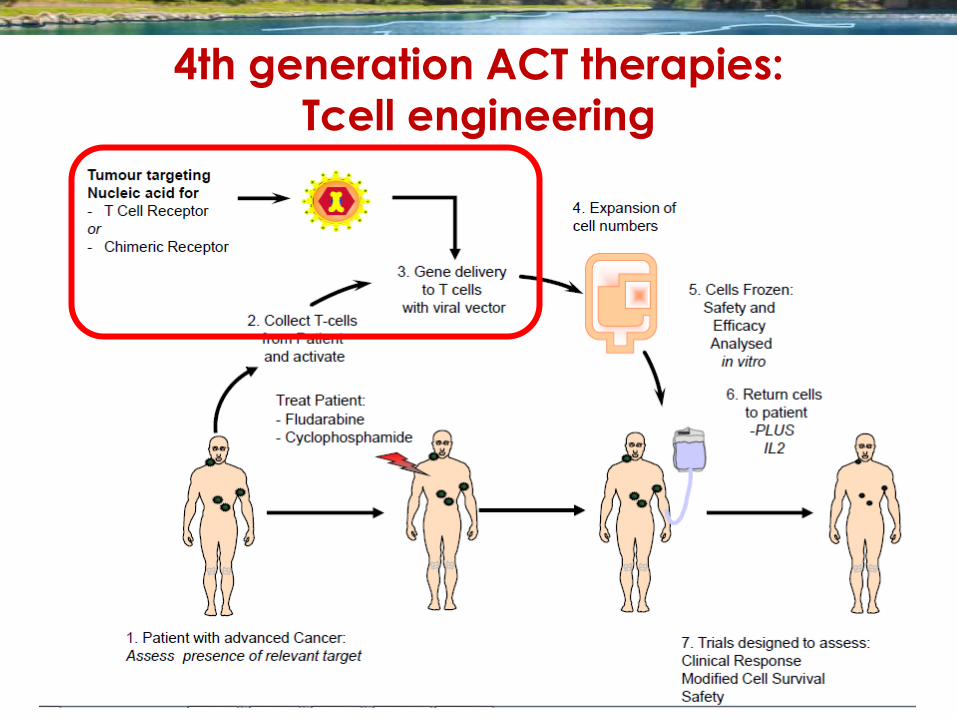
4th generation ACT therapies:
Tcell engineering
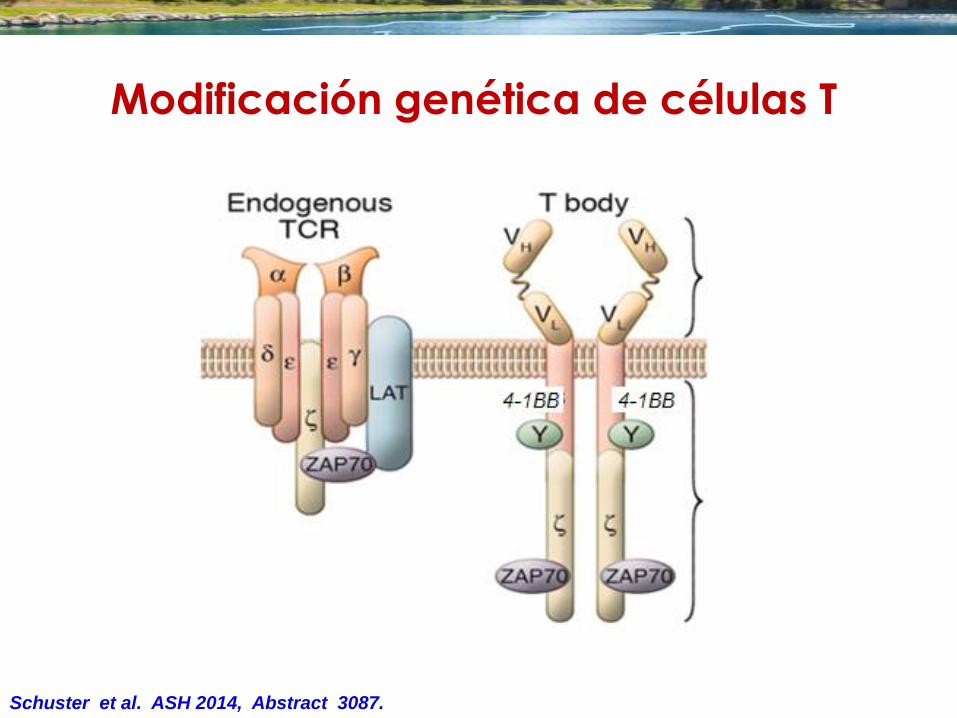
Schuster et al. ASH 2014, Abstract 3087.
scFv = anti-CD19
4-1BB +TCR ζ
signaling domains
Modificación genética de células T
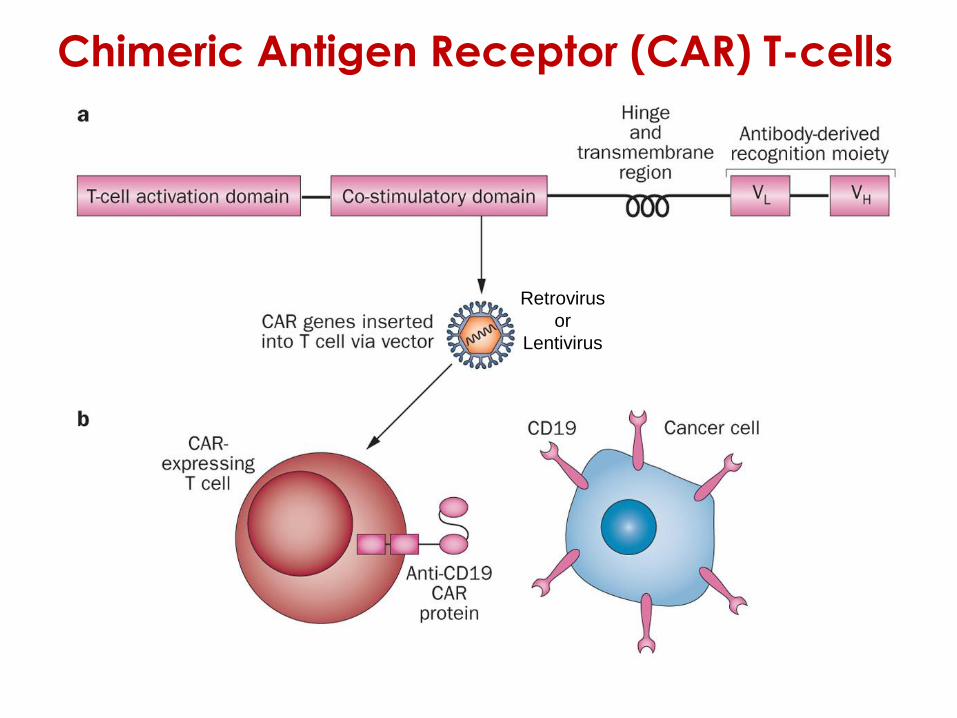
Retrovirus
or
Lentivirus
Chimeric Antigen Receptor (CAR) T-cells
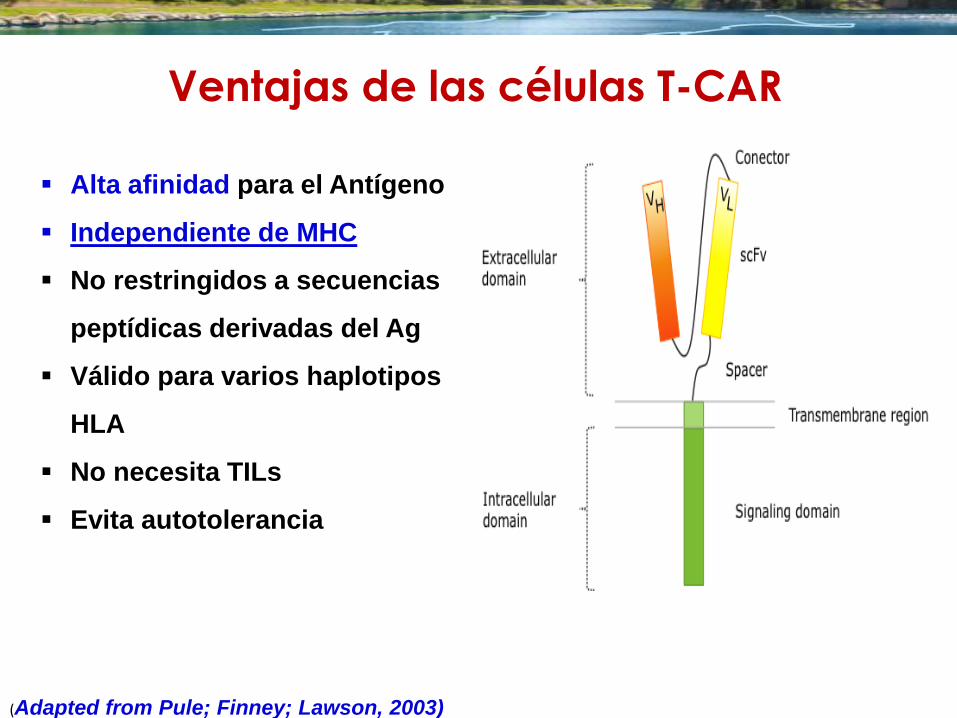
(Adapted from Pule; Finney; Lawson, 2003)
Alta afinidad para el Antígeno
Independiente de MHC
No restringidos a secuencias
peptídicas derivadas del Ag
Válido para varios haplotipos
HLA
No necesita TILs
Evita autotolerancia
Ventajas de las células T-CAR

Resultados con células T-CAR CD19
Institution Disease Number of
patients
Responses Ref.
COH FL 2 none Jensen et al. BBMT 2010
Baylor Indolent
lymphomas
6 2 SD Savoldo et al. JCI 2011
NCI FL, CLL 8 1 CR, 2 SD, 5 PR Kochenderfer et al., Blood 2010, 2011
MSKCC CLL, 1 ALL 9 3 SD, 1 PR Brentjens et al., Blood 2011
MSKCC ALL 16 88% CR Brentjens et al., Sci TM 2013
Davila et al., Sci TM 2014
UPenn CLL 3 2 CR, 1 PR Porter et al., NEJM 2011,
Kalos et al., Sci TM 2011
UPenn ALL 2 2 CR (MRD-) Grupp et al., NEJM 2013
NCI CLL,
lymphoma
10 1 CR, 2 PR Kochenderfer et al., Blood 2013
Baylor ALL, CLL 8 2 of 6 PR, 2 = CR Cruz et al., Blood 2013
64 + ASH 2013: Many more coming up soon
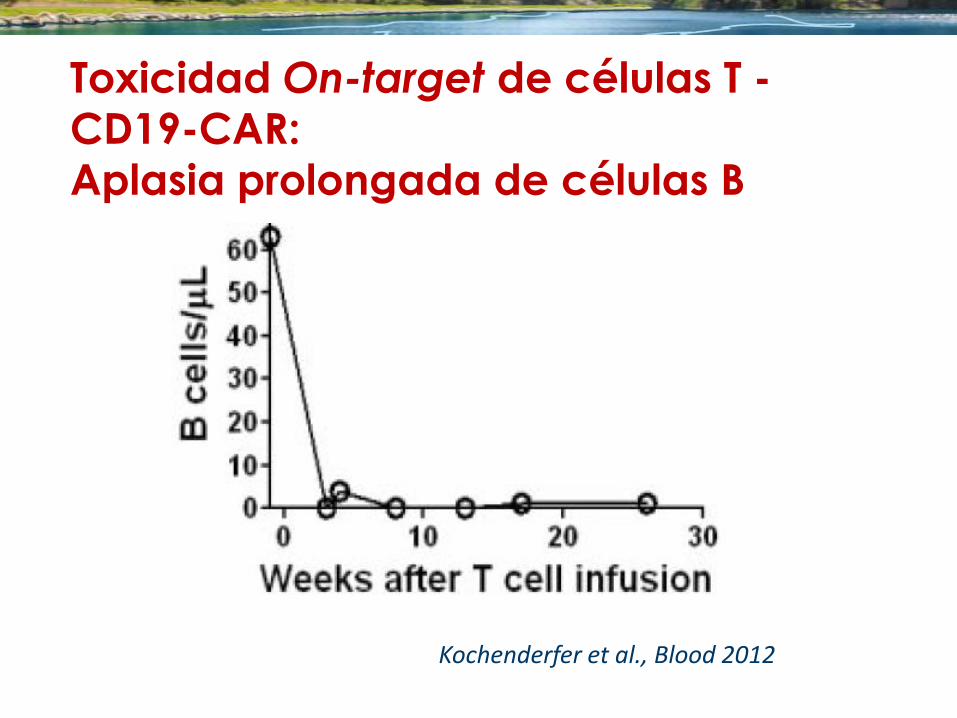
Toxicidad On-target de células T -
CD19-CAR:
Aplasia prolongada de células B
Kochenderfer et al., Blood 2012
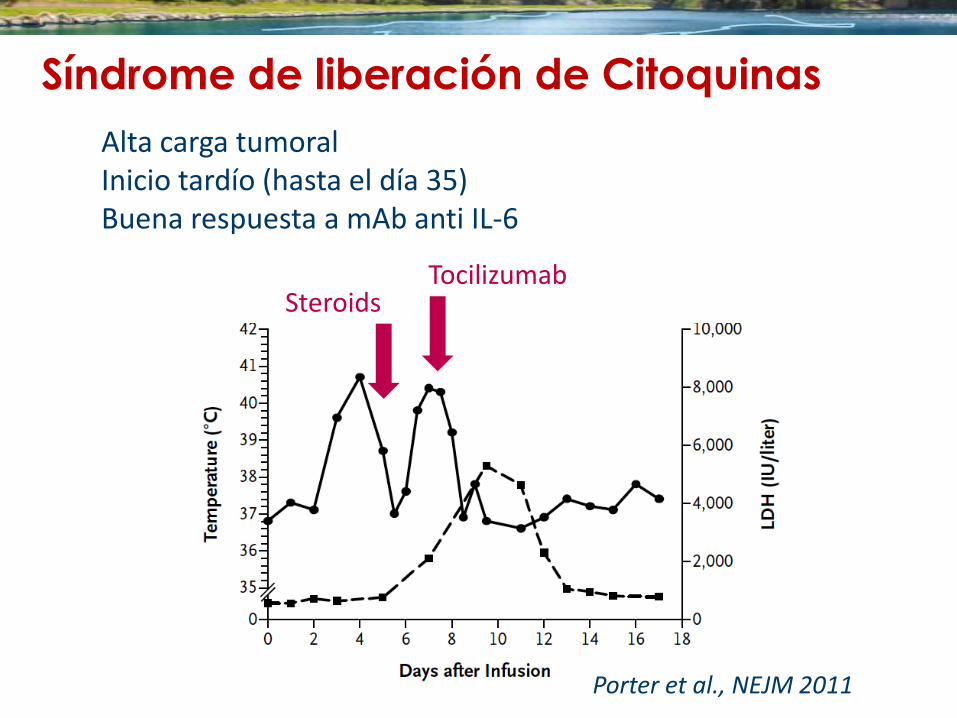
Síndrome de liberación de Citoquinas
Alta carga tumoral Inicio tardío (hasta el día 35) Buena respuesta a mAb anti IL-6
Porter et al., NEJM 2011
Steroids Tocilizumab
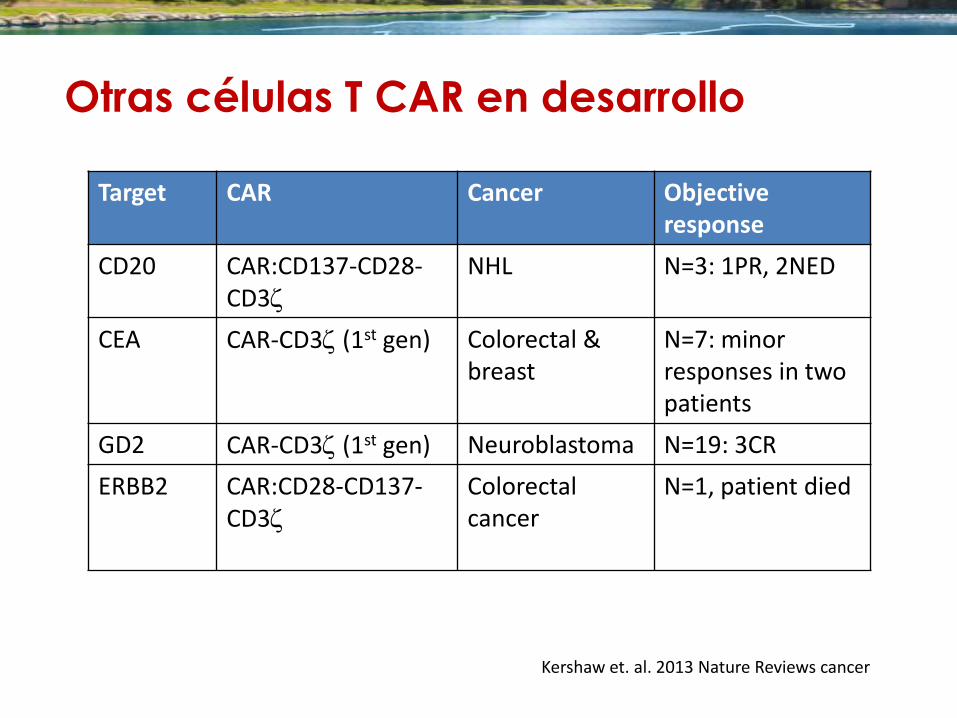
Otras células T CAR en desarrollo
Target CAR Cancer Objective response
CD20 CAR:CD137-CD28-CD3z
NHL N=3: 1PR, 2NED
CEA CAR-CD3z (1st gen)
Colorectal & breast
N=7: minor responses in two patients
GD2 CAR-CD3z (1st gen) Neuroblastoma N=19: 3CR
ERBB2 CAR:CD28-CD137-CD3z
Colorectal cancer
N=1, patient died
Kershaw et. al. 2013 Nature Reviews cancer
Modulación de la respuesta inmune contra el cáncer
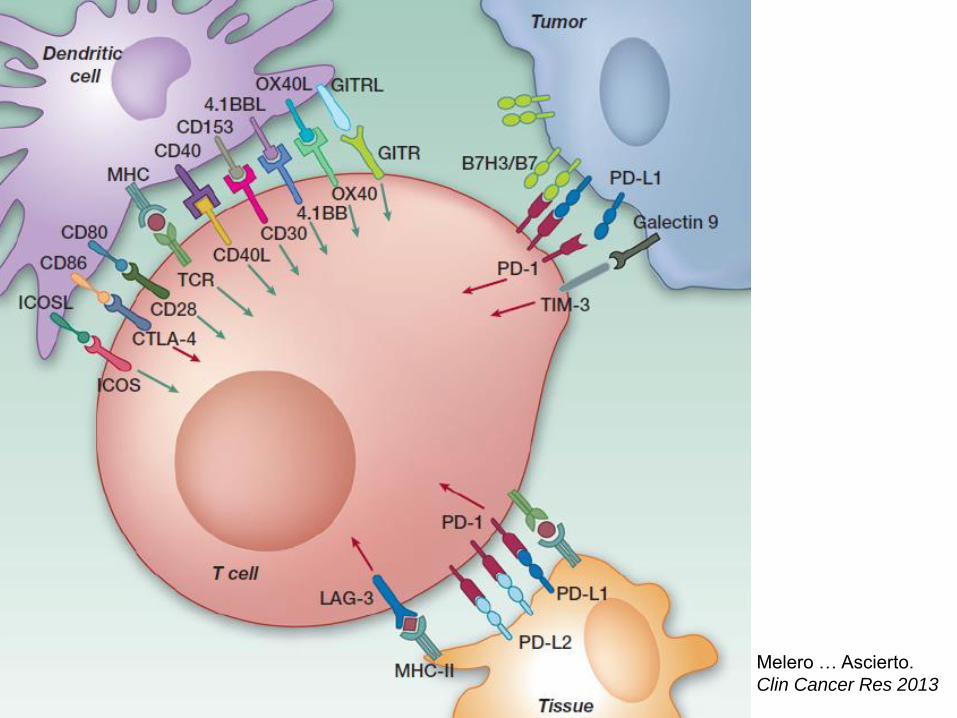
Melero … Ascierto.
Clin Cancer Res 2013
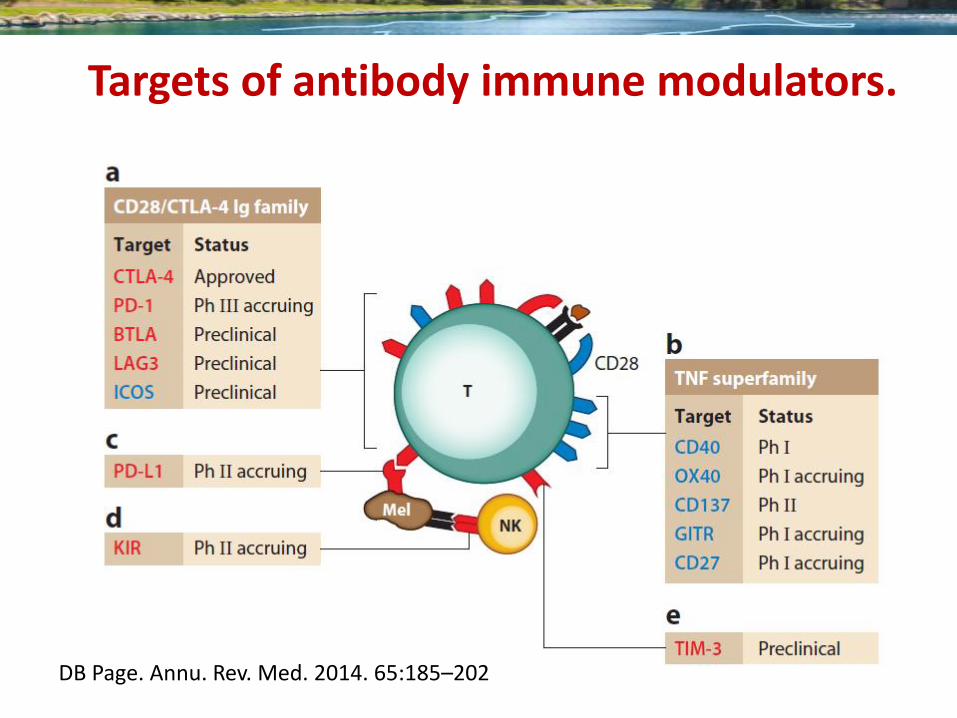
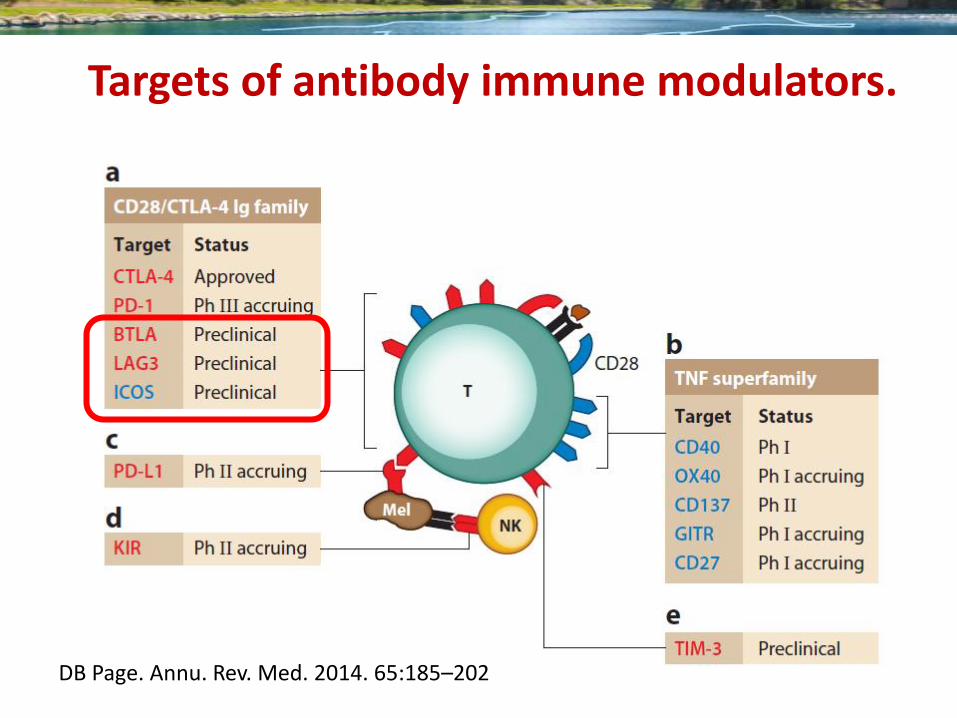
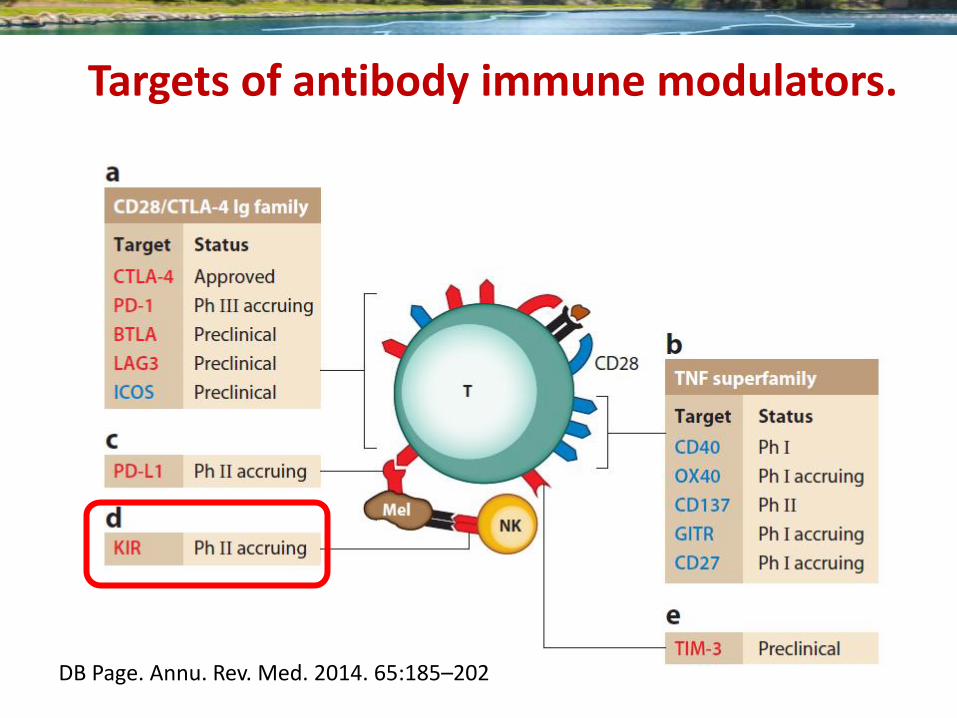
Targets of antibody immune modulators.
DB Page. Annu. Rev. Med. 2014. 65:185–202
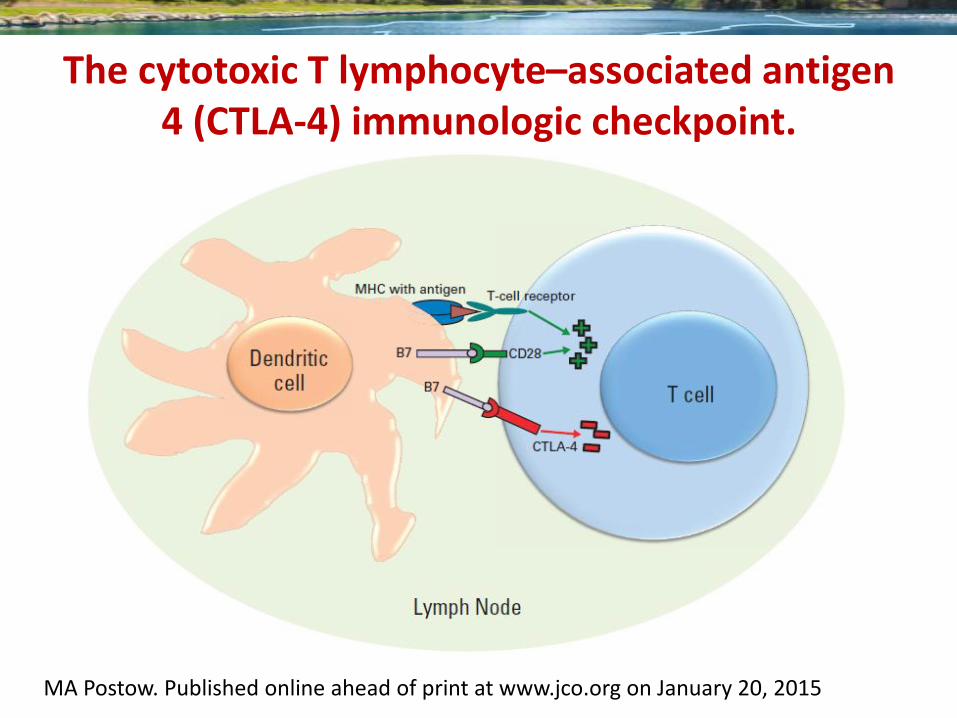
The cytotoxic T lymphocyte–associated antigen 4 (CTLA-4) immunologic checkpoint.
MA Postow. Published online ahead of print at www.jco.org on January 20, 2015
54
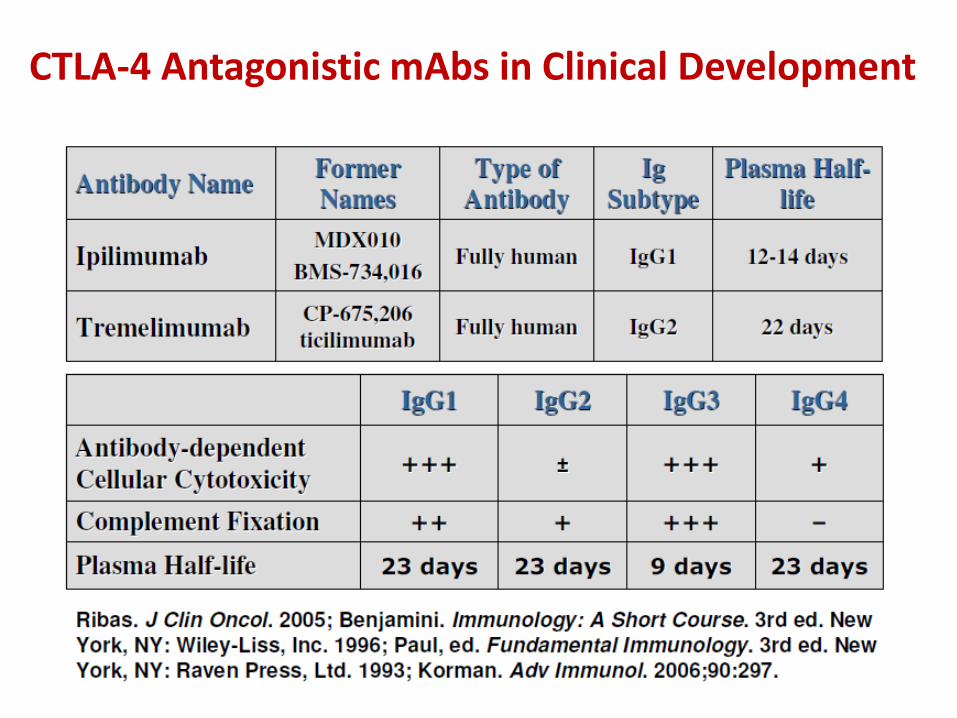
CTLA-4 Antagonistic mAbs in Clinical Development
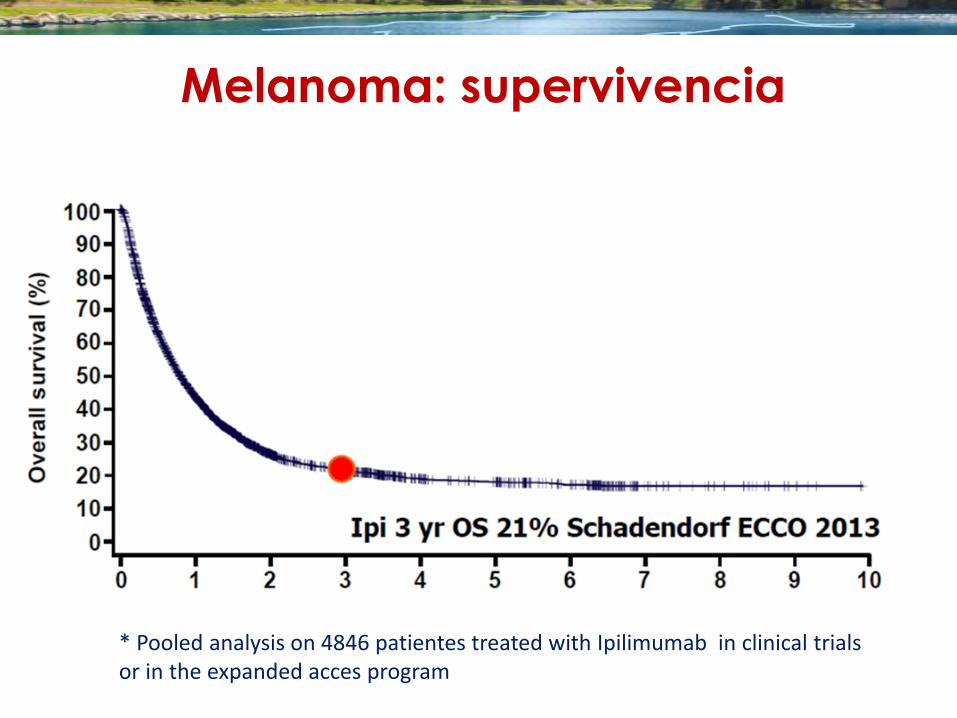
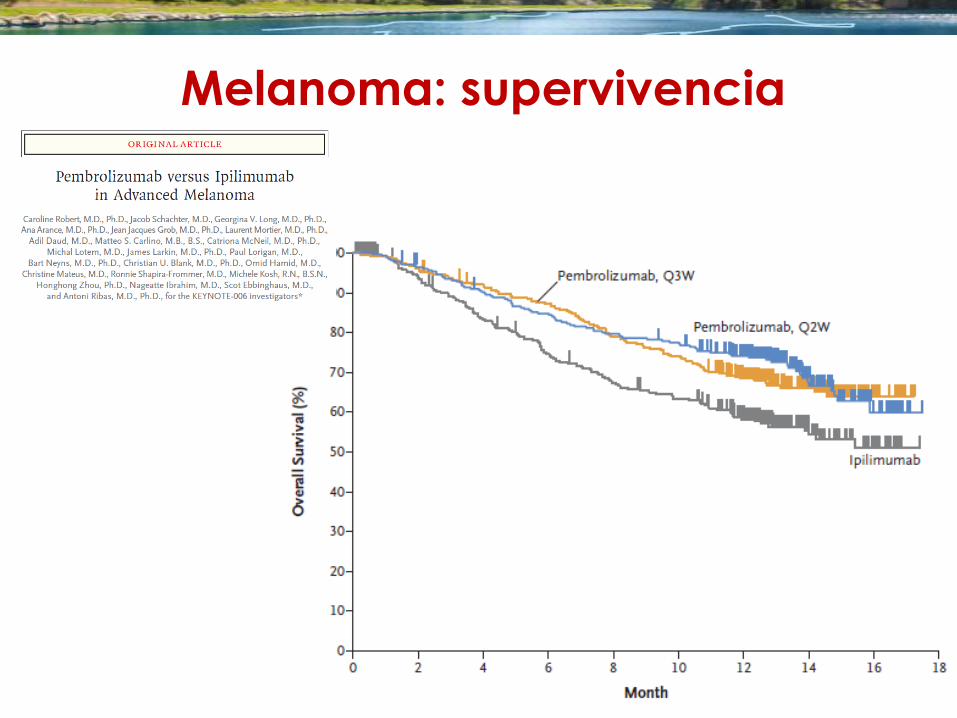
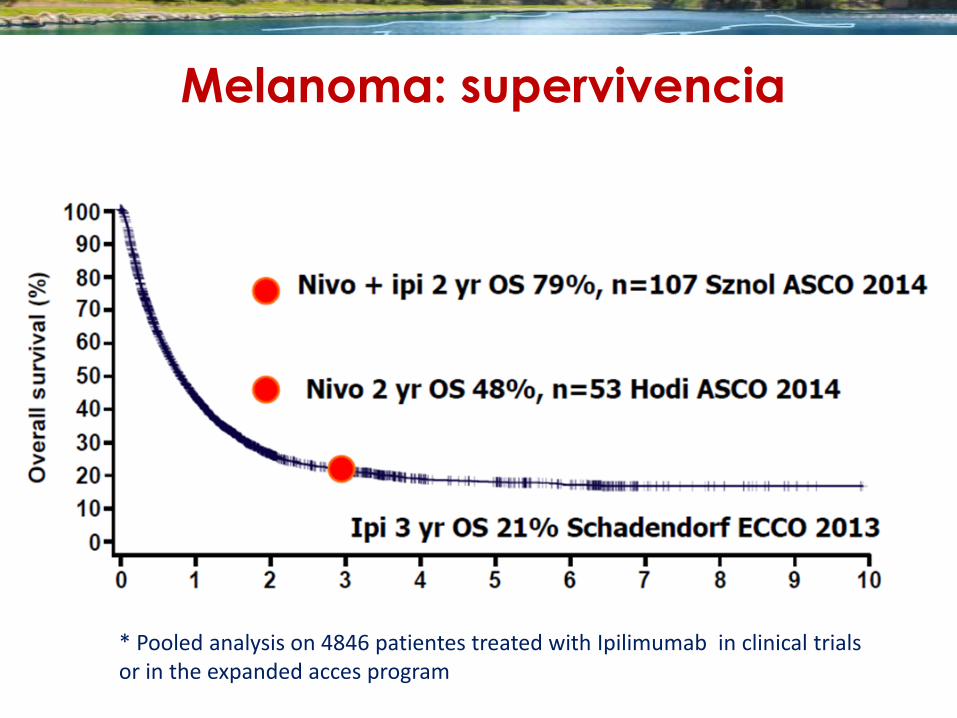
Melanoma: supervivencia
(*)
* Pooled analysis on 4846 patientes treated with Ipilimumab in clinical trials or in the expanded acces program
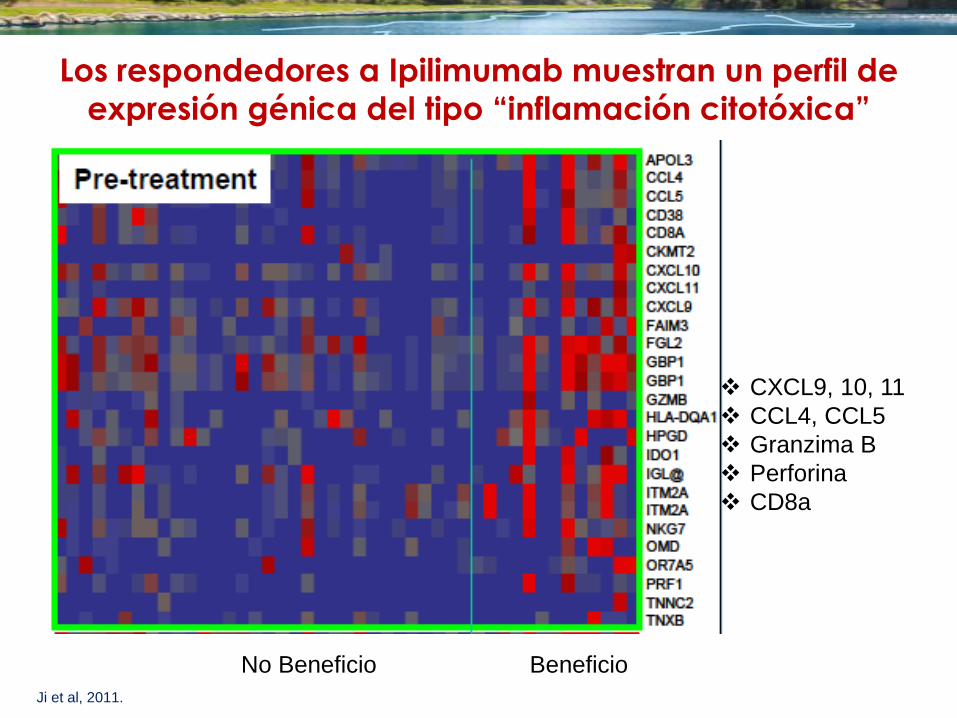
Los respondedores a Ipilimumab muestran un perfil de
expresión génica del tipo “inflamación citotóxica”
Ji et al, 2011.
CXCL9, 10, 11
CCL4, CCL5
Granzima B
Perforina
CD8a
No Beneficio Beneficio
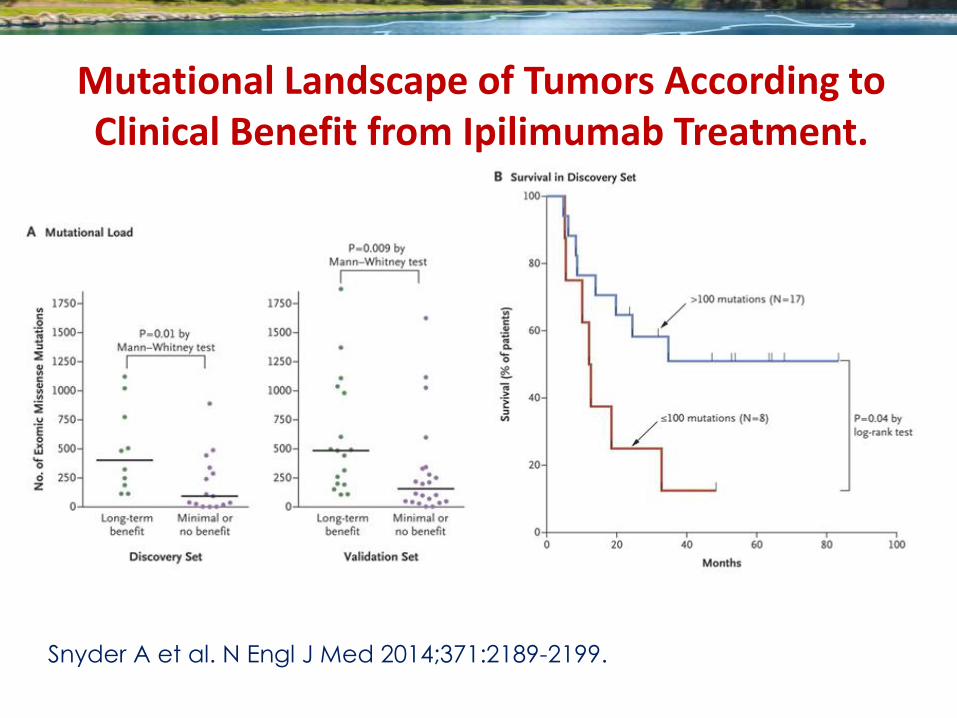
Snyder A et al. N Engl J Med 2014;371:2189-2199.
Mutational Landscape of Tumors According to Clinical Benefit from Ipilimumab Treatment.
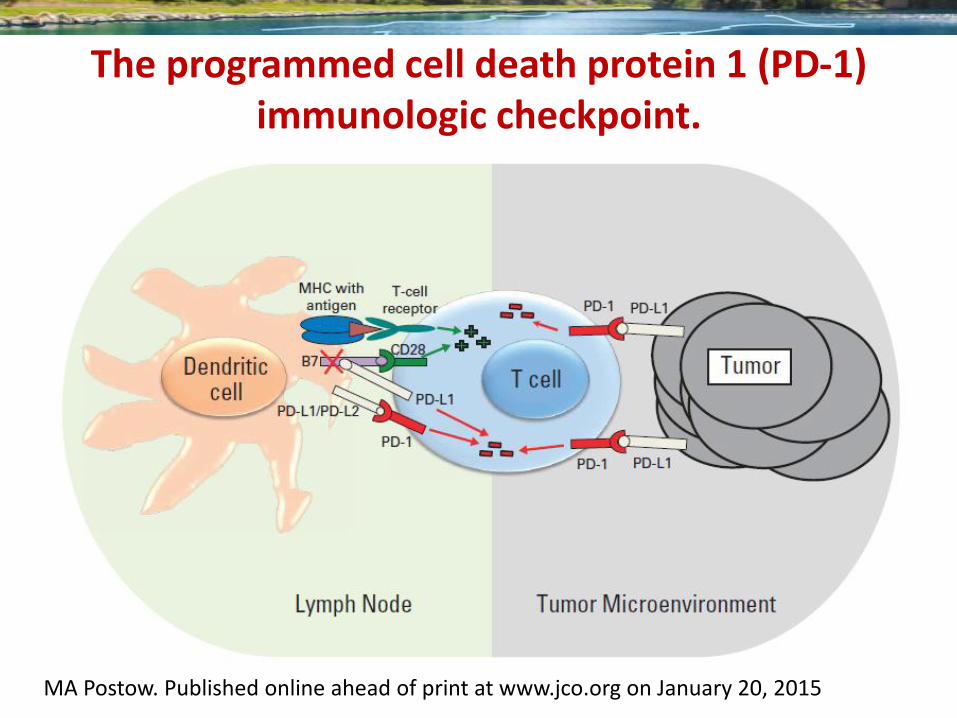
The programmed cell death protein 1 (PD-1) immunologic checkpoint.
MA Postow. Published online ahead of print at www.jco.org on January 20, 2015
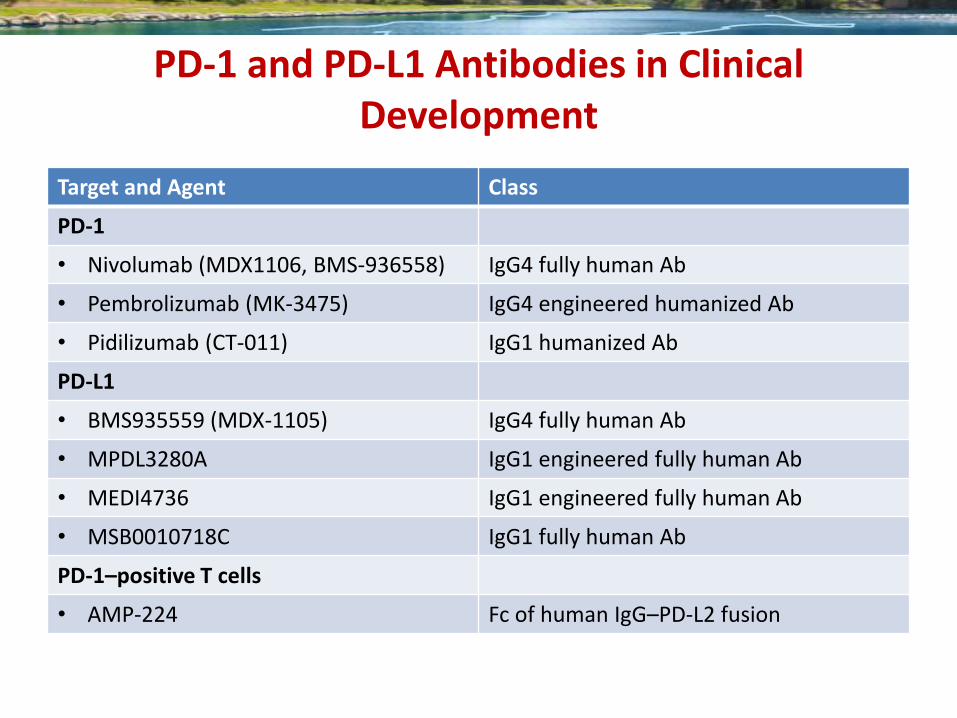
PD-1 and PD-L1 Antibodies in Clinical Development
Target and Agent Class
PD-1
• Nivolumab (MDX1106, BMS-936558) IgG4 fully human Ab
• Pembrolizumab (MK-3475) IgG4 engineered humanized Ab
• Pidilizumab (CT-011) IgG1 humanized Ab
PD-L1
• BMS935559 (MDX-1105) IgG4 fully human Ab
• MPDL3280A IgG1 engineered fully human Ab
• MEDI4736 IgG1 engineered fully human Ab
• MSB0010718C IgG1 fully human Ab
PD-1–positive T cells
• AMP-224 Fc of human IgG–PD-L2 fusion
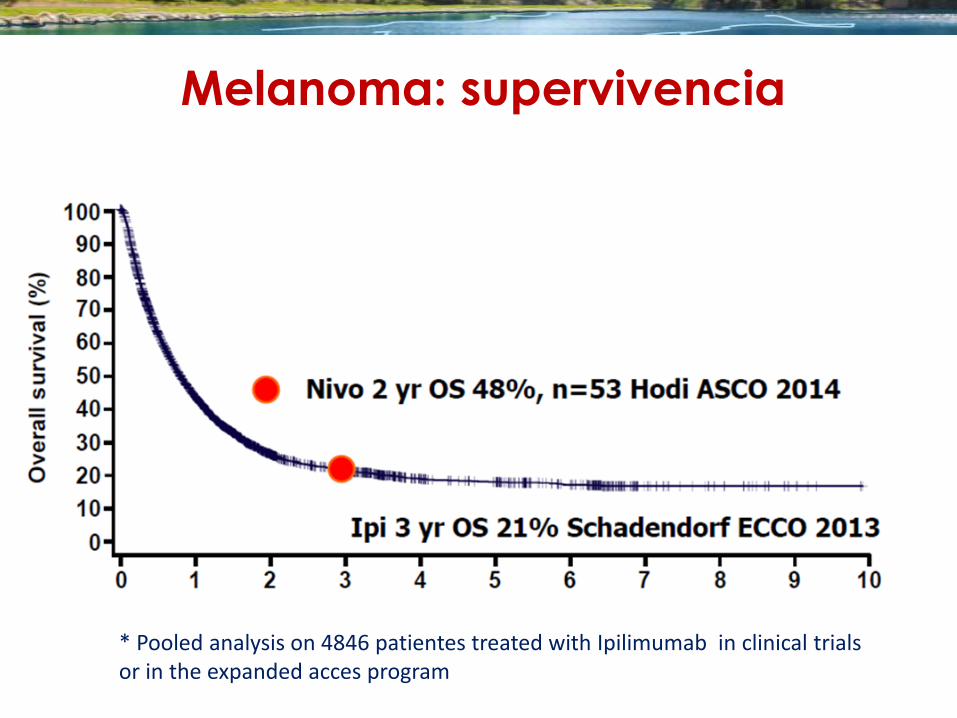
Melanoma: supervivencia
(*)
* Pooled analysis on 4846 patientes treated with Ipilimumab in clinical trials or in the expanded acces program
Melanoma: supervivencia
(*)
04 de Marzo 2015 FDA approved nivolumab for the treatment of
patients with metastatic squamous non-small
cell lung cancer with progression on or after
platinum-based chemotherapy.
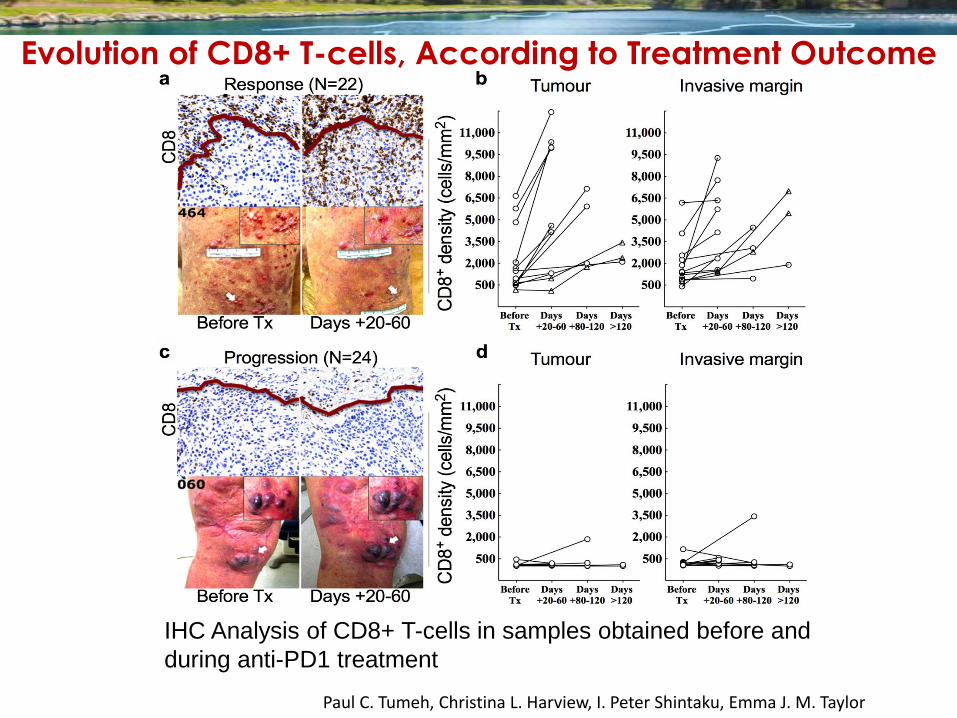
Evolution of CD8+ T-cells, According to Treatment Outcome
IHC Analysis of CD8+ T-cells in samples obtained before and
during anti-PD1 treatment
Paul C. Tumeh, Christina L. Harview, I. Peter Shintaku, Emma J. M. Taylor
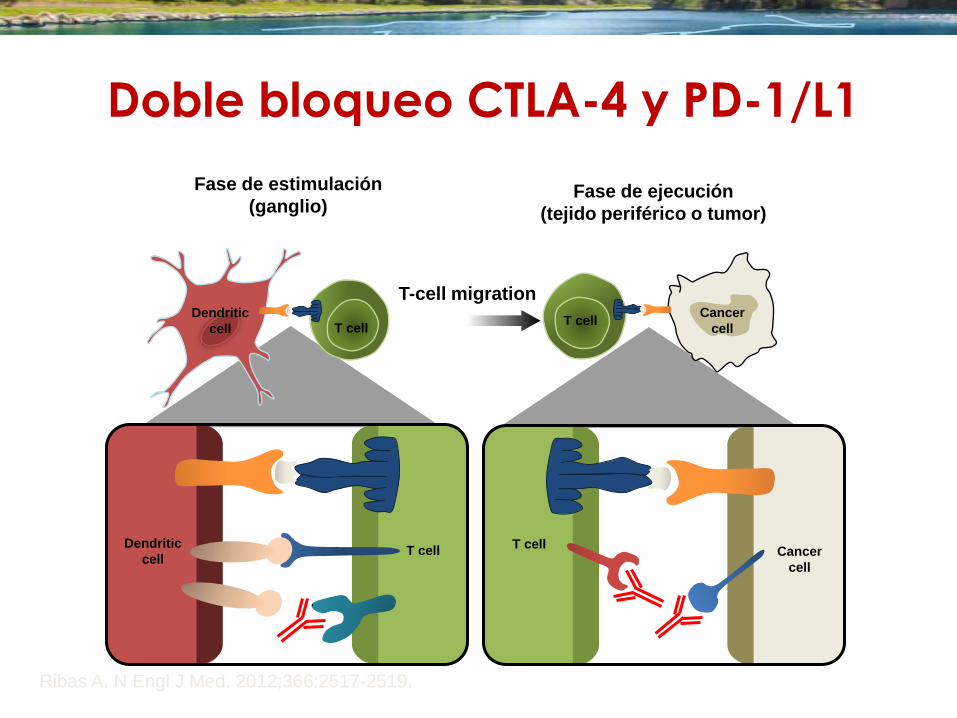
Doble bloqueo CTLA-4 y PD-1/L1
Ribas A. N Engl J Med. 2012;366:2517-2519.
Fase de estimulación
(ganglio) Fase de ejecución
(tejido periférico o tumor)
T-cell migration
Dendritic
cell T cell
MHC TCR
B7
CD28
CTLA-4
T cell Cancer
cell
MHC TCR
PD-1
PD-L1
T cell Cancer
cell
Dendritic
cell T cell
Melanoma: supervivencia
(*)
* Pooled analysis on 4846 patientes treated with Ipilimumab in clinical trials or in the expanded acces program
DB Page. Annu. Rev. Med. 2014. 65:185–202
Targets of antibody immune modulators.
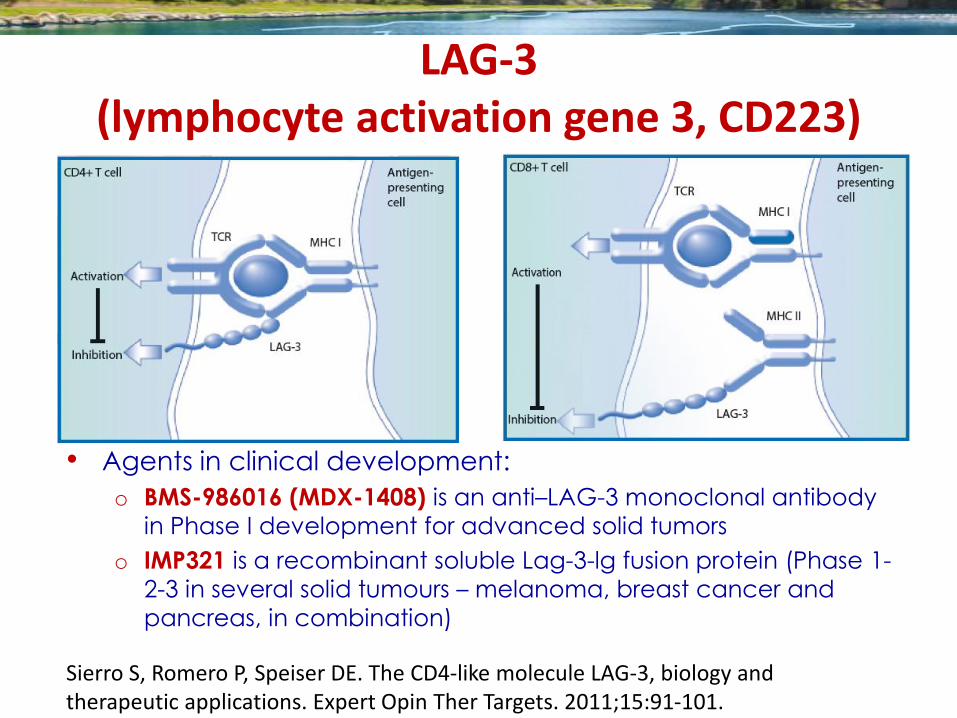
LAG-3 (lymphocyte activation gene 3, CD223)
Sierro S, Romero P, Speiser DE. The CD4-like molecule LAG-3, biology and therapeutic applications. Expert Opin Ther Targets. 2011;15:91-101.
• Agents in clinical development:
o BMS-986016 (MDX-1408) is an anti–LAG-3 monoclonal antibody
in Phase I development for advanced solid tumors
o IMP321 is a recombinant soluble Lag-3-lg fusion protein (Phase 1-
2-3 in several solid tumours – melanoma, breast cancer and
pancreas, in combination)
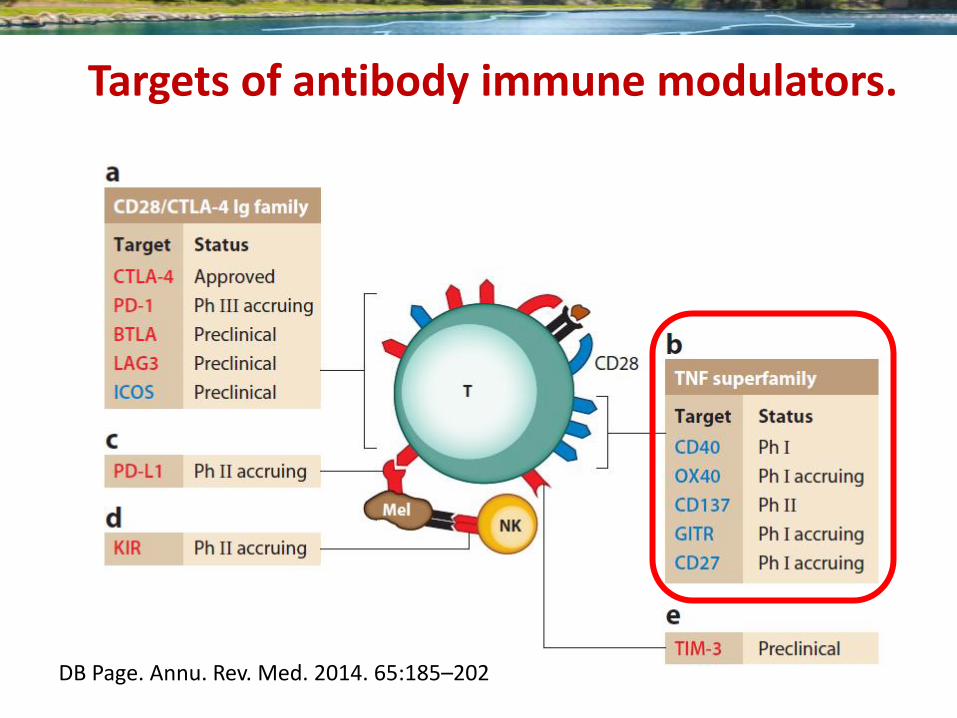
DB Page. Annu. Rev. Med. 2014. 65:185–202
Targets of antibody immune modulators.
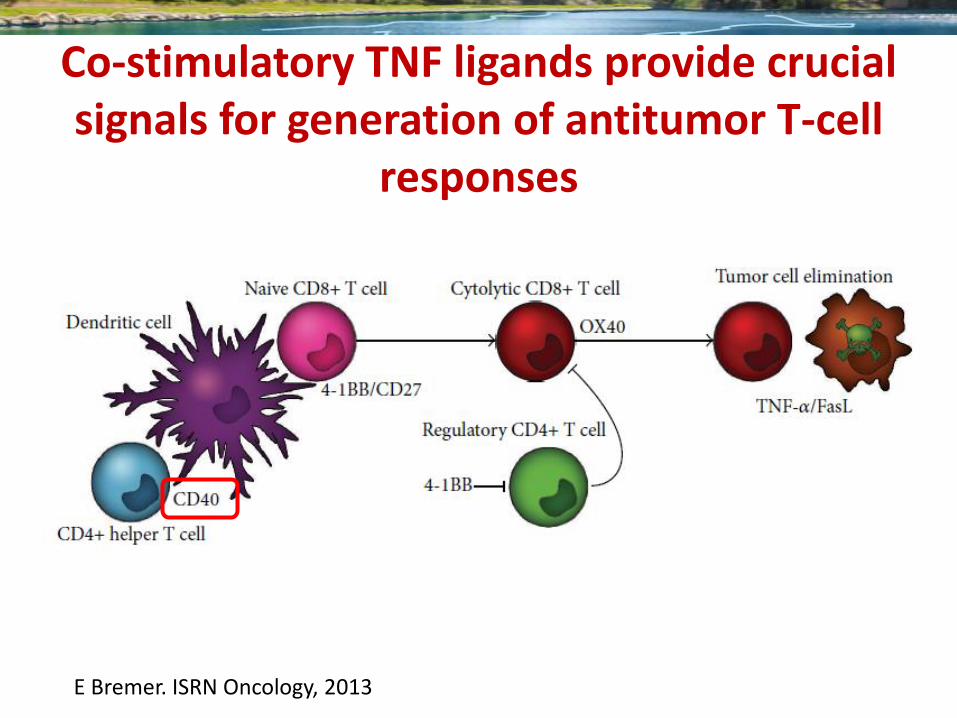
Co-stimulatory TNF ligands provide crucial signals for generation of antitumor T-cell
responses
E Bremer. ISRN Oncology, 2013
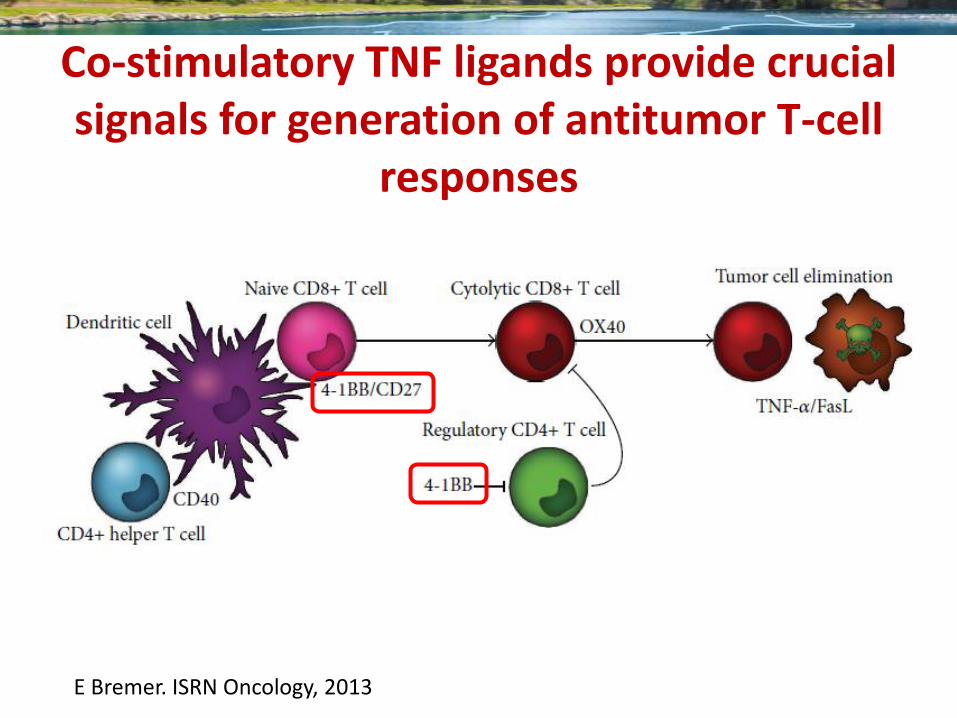
Co-stimulatory TNF ligands provide crucial signals for generation of antitumor T-cell
responses
E Bremer. ISRN Oncology, 2013
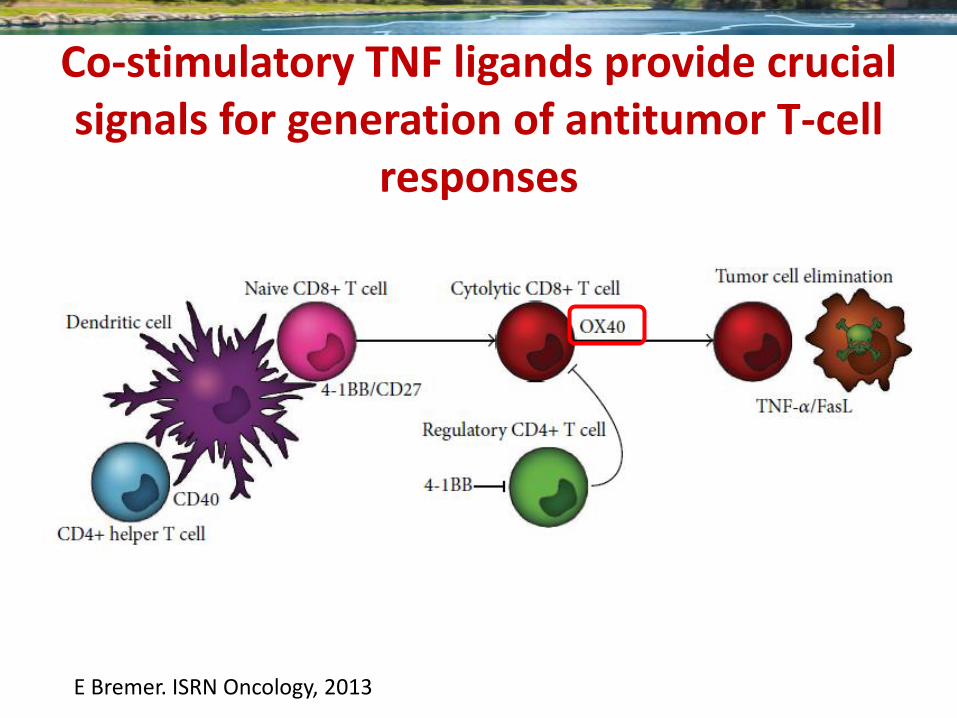
Co-stimulatory TNF ligands provide crucial signals for generation of antitumor T-cell
responses
E Bremer. ISRN Oncology, 2013
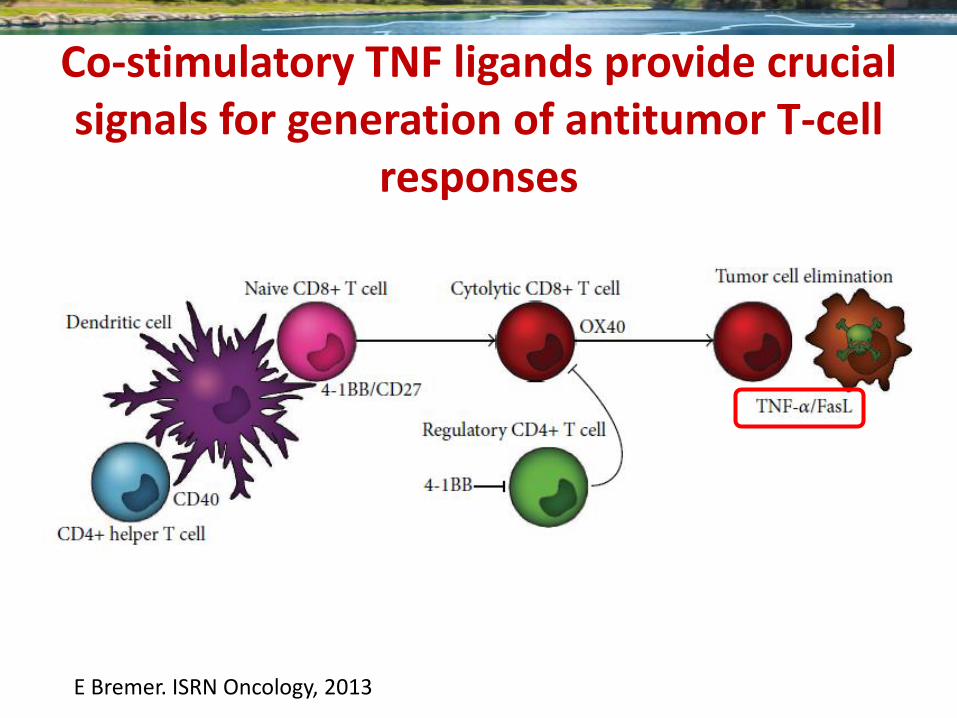
Co-stimulatory TNF ligands provide crucial signals for generation of antitumor T-cell
responses
E Bremer. ISRN Oncology, 2013
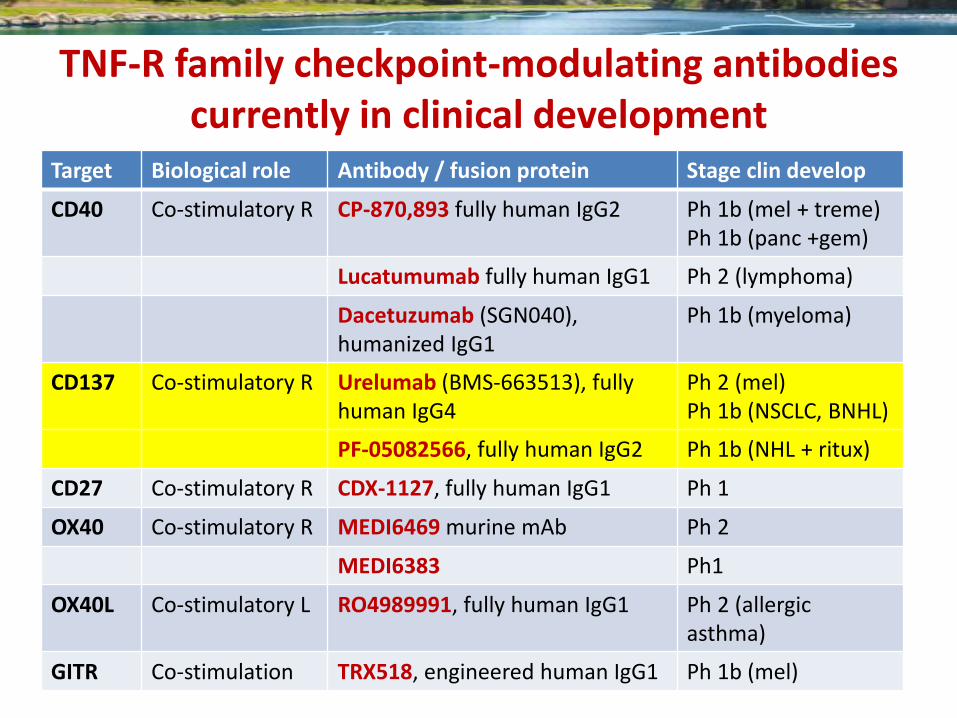
TNF-R family checkpoint-modulating antibodies currently in clinical development
Target Biological role Antibody / fusion protein Stage clin develop
CD40 Co-stimulatory R CP-870,893 fully human IgG2 Ph 1b (mel + treme) Ph 1b (panc +gem)
Lucatumumab fully human IgG1 Ph 2 (lymphoma)
Dacetuzumab (SGN040), humanized IgG1
Ph 1b (myeloma)
CD137 Co-stimulatory R Urelumab (BMS-663513), fully human IgG4
Ph 2 (mel) Ph 1b (NSCLC, BNHL)
PF-05082566, fully human IgG2 Ph 1b (NHL + ritux)
CD27 Co-stimulatory R CDX-1127, fully human IgG1 Ph 1
OX40 Co-stimulatory R MEDI6469 murine mAb Ph 2
MEDI6383 Ph1
OX40L Co-stimulatory L RO4989991, fully human IgG1 Ph 2 (allergic asthma)
GITR Co-stimulation TRX518, engineered human IgG1 Ph 1b (mel)
DB Page. Annu. Rev. Med. 2014. 65:185–202
Targets of antibody immune modulators.
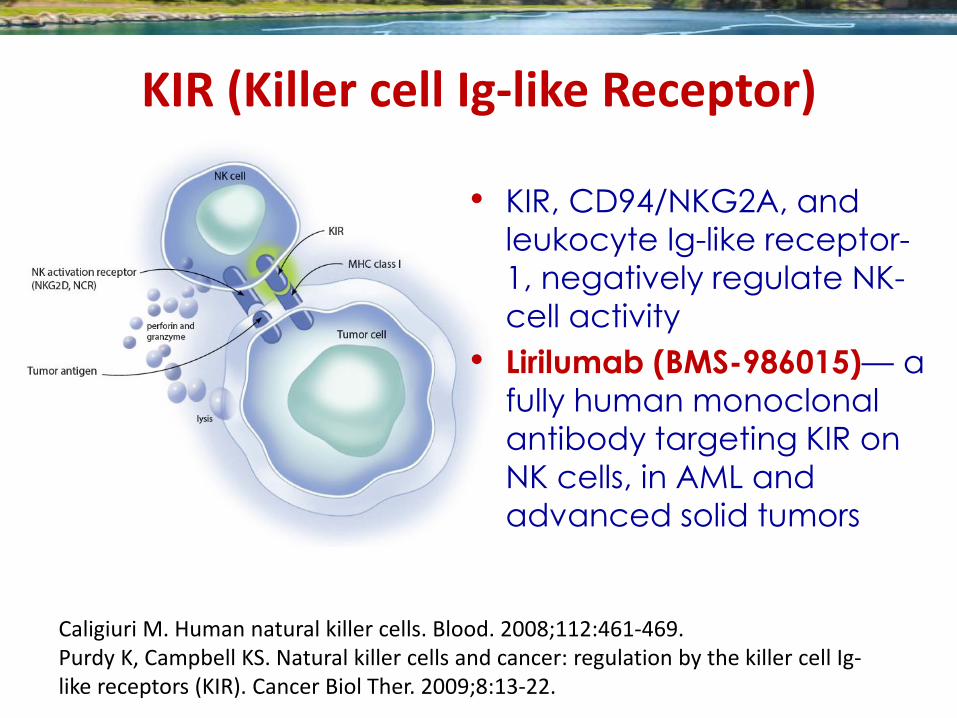
KIR (Killer cell Ig-like Receptor)
Caligiuri M. Human natural killer cells. Blood. 2008;112:461-469. Purdy K, Campbell KS. Natural killer cells and cancer: regulation by the killer cell Ig-like receptors (KIR). Cancer Biol Ther. 2009;8:13-22.
• KIR, CD94/NKG2A, and
leukocyte Ig-like receptor-
1, negatively regulate NK-
cell activity
• Lirilumab (BMS-986015)— a
fully human monoclonal
antibody targeting KIR on
NK cells, in AML and
advanced solid tumors
78
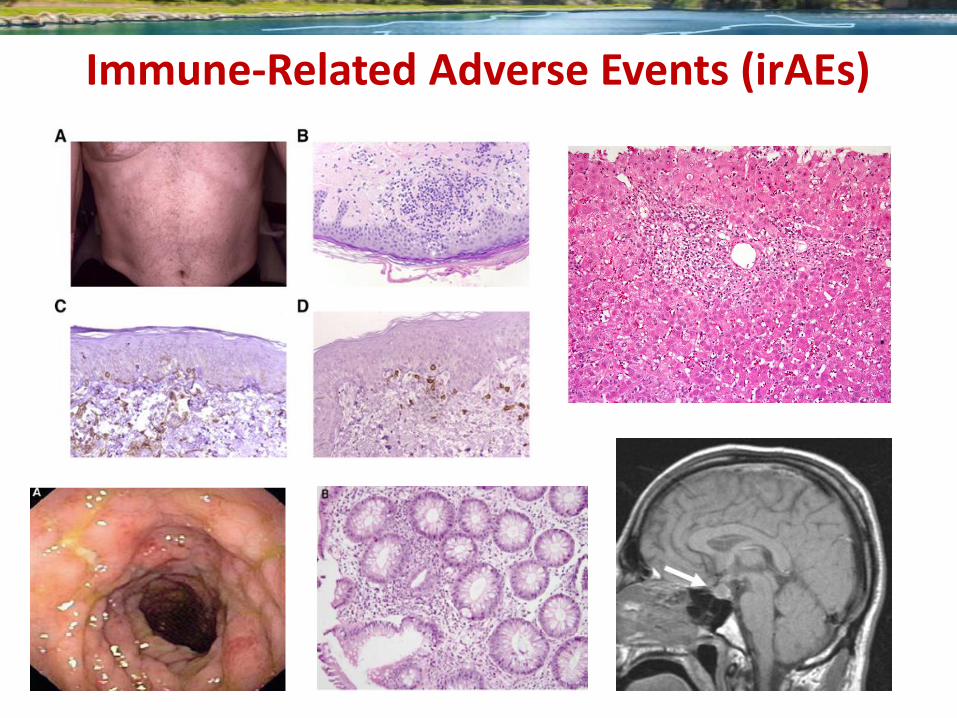
Immune-Related Adverse Events (irAEs)
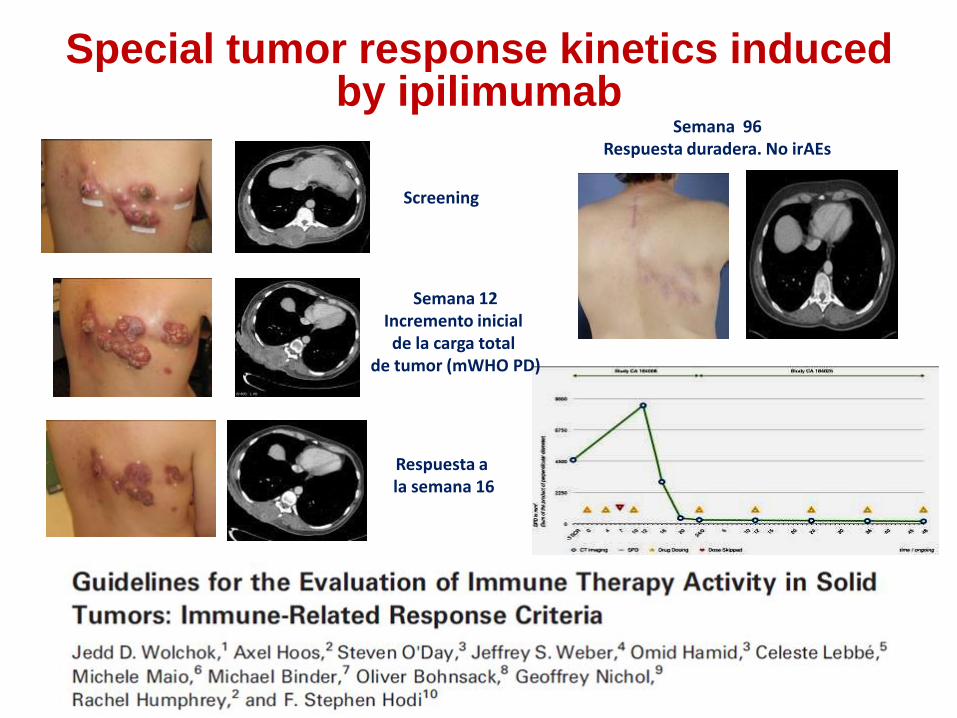
Screening
Respuesta a la semana 16
Semana 96 Respuesta duradera. No irAEs
Cortesía de f K. Harmankaya, Viena
Harmankaya K, et al. Presented at EADO 2009, Vienna, Austria
Special tumor response kinetics induced by ipilimumab
Semana 12 Incremento inicial de la carga total
de tumor (mWHO PD)
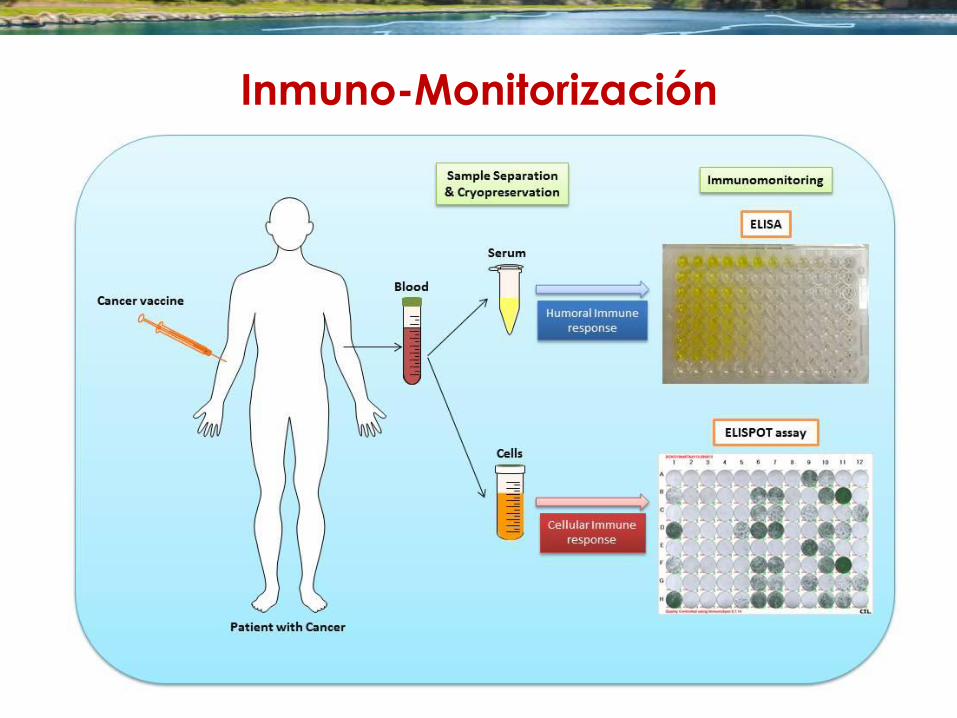
Inmuno-Monitorización
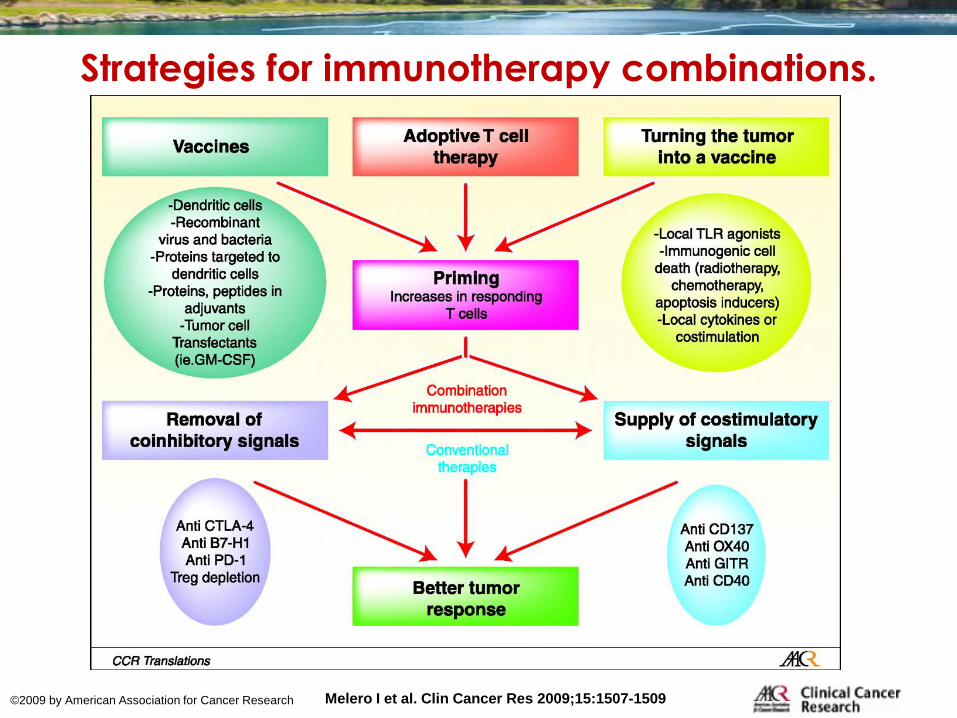
Strategies for immunotherapy combinations.
Melero I et al. Clin Cancer Res 2009;15:1507-1509 ©2009 by American Association for Cancer Research
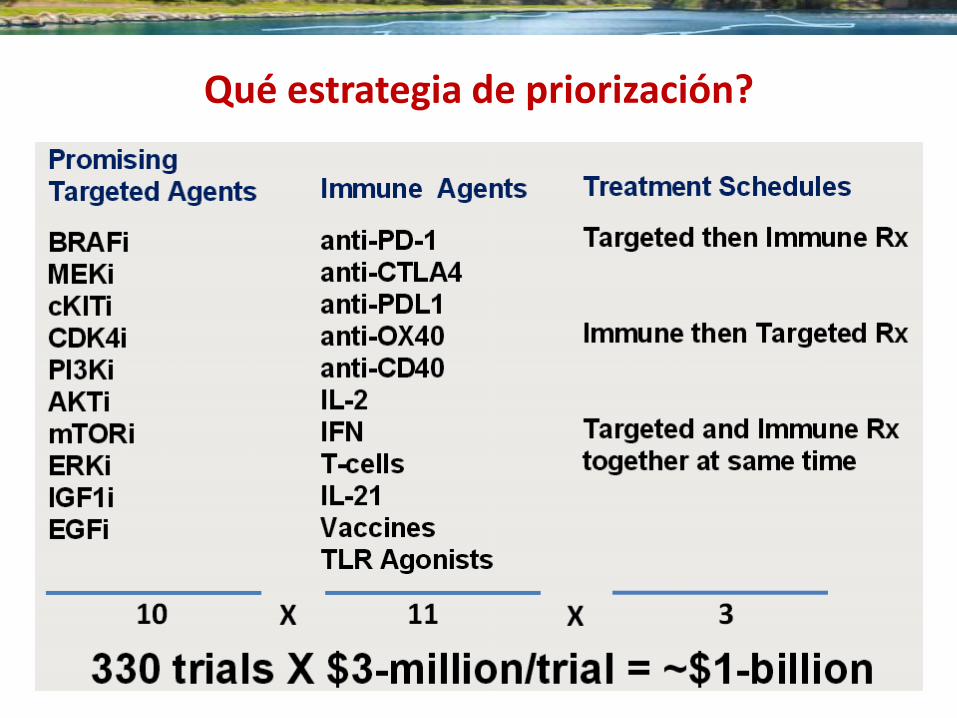
Qué estrategia de priorización?
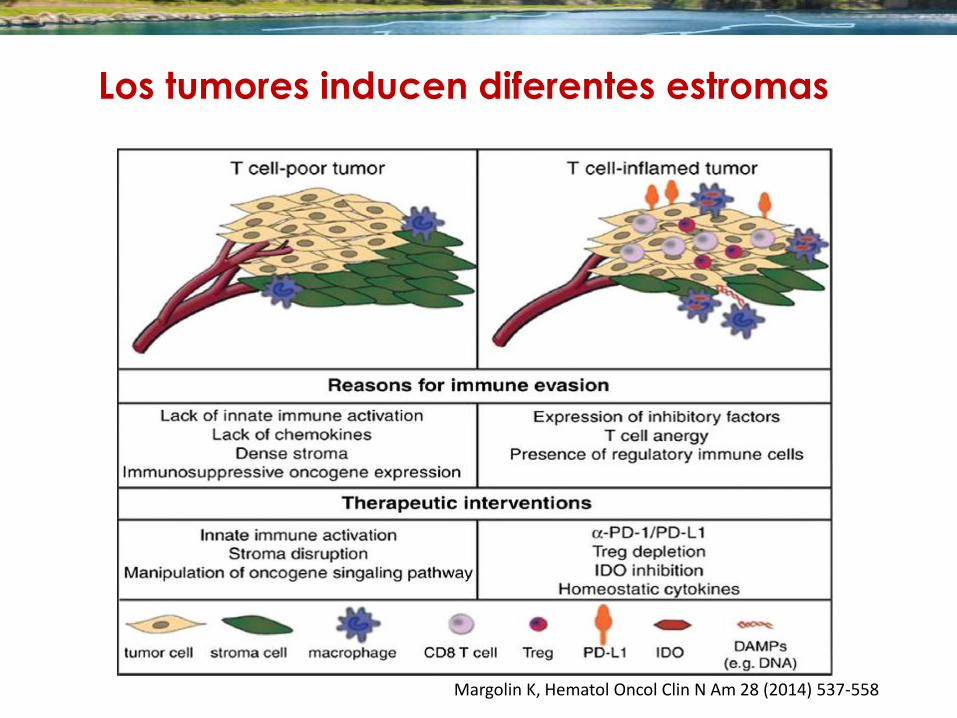
Margolin K, Hematol Oncol Clin N Am 28 (2014) 537-558
Los tumores inducen diferentes estromas
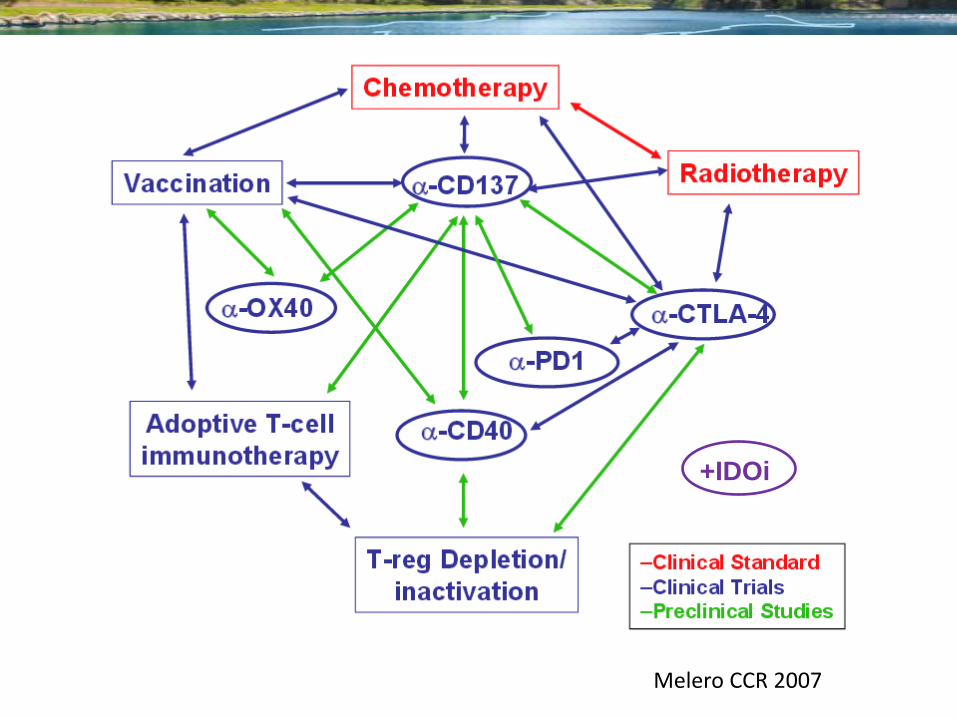
Otras combinaciones en preclínica
Melero CCR 2007
+IDOi
¿Cómo va a modificar la Inmuno-
oncología, el panorama terapéutico
del cáncer? • Incremento de arsenal terapéutico
• Incremento de estrategias de combinación/secuenciación
• Necesidad de investigación traslacional o Personalización
o Monitorización
o Priorización de EECC
• Nuevos eventos adversos - entrenamiento
• Nuevo enfoque de la enfermedad tumoral
• Transversalidad de conceptos
• Más multidisdiplinariedad
¿Cómo va a modificar la Inmuno-
oncología, el panorama terapéutico
del cáncer? • Incremento de arsenal terapéutico
• Incremento de estrategias de combinación/secuenciación o IT + IT
o No IT + IT
• Personalización
• Monitorización
• Manejo de nuevos eventos adversos
• Nuevo enfoque de la enfermedad tumoral
• Transversalidad de conceptos
• Multidisdiplinariedad

Agradecimientos
Grupo Español de Terapias
Inmuno-Biológicas del Cáncer
Spanish Group for
Cancer Immuno-Biotherapy
Maite Carpio y familia