Embed Size (px)
Citation preview

ISSN 1607�6729, Doklady Biochemistry and Biophysics, 2014, Vol. 454, pp. 29–33. © Pleiades Publishing, Ltd., 2014.Original Russian Text © T.A. Bogush, A.S. Shaturova, E.A. Dudko, E.A. Bogush, B.E. Polotsky, S.A. Tyulandin, M.I. Davydov, 2014, published in Doklady Akademii Nauk, 2014,Vol. 454, No. 6, pp. 620–624.
29
Non�small cell lung carcinoma (NSCLC) is one ofthe most severe cancers with adverse outcome; theresults of its treatment cannot be regarded as satisfac�tory. Therefore, the search for pathogeneticallygrounded and patient�centered approaches to thetreatment of NSCLC is undoubtedly one of the toppriorities. In our opinion, discovery of a new class ofreceptors, estrogen receptors β (ERβ), created thepreconditions for the development of a new treatmentstrategy for NSCLC, namely anti�estrogen therapy.
ERβ were opened in 1996 and now attract closeattention of oncologists. Unlike “classical” receptors(now called ERα), ERβ have been detected not onlyin the breast cancer tissue, but also in solid tumors ofvarious localizations.
They are not only prognostic markers of the diseasecourse, but also the targets of anti�estrogen action [1].The interaction of anti�estrogens with ERβ are purelyantagonistic, whereas the effect on ERα is alsoaccompanied by agonist manifestations [2].
As for NSCLC, only 60–80% of tumors are ERβ�positive according to different authors [3–5]. Somestudies indicate the prevalence of ERβ in the cyto�plasm [6]. The nuclear ERβ expression has beendetected in 31–84% of cases [7, 8]; the cytoplasmicstaining, in 10–100% of the tumor tissue samples[9, 10].
The ERβ expression in the NSCLC tissue predictsa more favorable course of disease compared with thegroup of patients in which the tumor ERβ are absent,regardless of gender [11, 12]. The absence of ERβ
expression is an independent factor that worsens theprognosis of NSCLC [13].
Analysis of the published data shows that only thefrequency of ERβ detection in the group of patientsexamined was reported in the vast majority of papers(often contradictory), whereas the information on thelevel and intensity of receptor expression in a tumor ofspecific patients is virtually absent. The reason for thisis the lack of a unified quantitative procedure forassessing ERβ in solid tissues, the need for which isdiscussed continually at international forums [14].Nevertheless, the undisputed fact is that a new targetfor anti�estrogens was discovered in human solidtumors of different localization, i.e., ERβ, which arethe pathogenetic characteristics of tumors and theprognostic marker of disease aggressiveness. There is aneed for their accurate quantitative evaluation anddetailed study. It should be noted that there are nopublished data about the ERβ expression in tumormetastases.
In the present study, a comparative quantitativeestimation of the level, intensity, and frequency of theERβ expression in NSCLC tissues and also in lungmetastases of tumor of another primary localizationwas carried out. In addition to the undoubted funda�mental importance of this kind of knowledge, themain question that we tried to answer is how manypatients with NSCLC and possible lung metastases oftumors of another primary localization are potentialcandidates for anti�estrogen treatment.
In this study, we used the quantitative immunoflu�orescent method developed and patented by us [15].Briefly, a suspension of tumor cells was obtained fromthe surgical biopsy material of NSCLC and lungmetastases and fixed with 4% formaldehyde solution.
Comparative Assessment of the Estrogen Receptor β Expressionin the Tissues of Non�Small Cell Lung Carcinoma
and Lung Metastases of Tumors of Other Primary Localizations
T. A. Bogush, A. S. Shaturova, E. A. Dudko, E. A. Bogush, B. E. Polotsky, S. A. Tyulandin, and Academician M. I. Davydov
Received October 28, 2013
DOI: 10.1134/S1607672914010232
Blokhin Russian Cancer Research Center, Russian Academy of Medical Sciences, Moscow, 115478 Russia
BIOCHEMISTRY, BIOPHYSICSAND MOLECULAR BIOLOGY

30
DOKLADY BIOCHEMISTRY AND BIOPHYSICS Vol. 454 2014
BOGUSH et al.
Before the immunofluorescent staining, the cellswere sedimented from the suspension by centrifuga�tion at 3000 rpm for 10 min, the supernatant wasremoved, and 1 mL of 1% Tween 20 (Sigma, UnitedStates) was added to the pellet and incubated at roomtemperature for 20 min. Then, in order to wash off thedetergent, 10 mL of phosphate buffer solution (pH 7.4)was added to the test tube and centrifuged at 3000 rpmfor 10 min. The supernatant was removed, and phos�phate buffer (pH 7.4) was added to the pellet in a vol�ume sufficient to obtain the necessary concentrationof cells (3 × 105 to 4 × 105 cells/mL), which were thancounted in a hemocytometer.
Incubation of cells with antibodies was carried outat 4°C in the dark in plastic test tubes for the flowcytofluorimetry in 100 μL of the cell suspension. Theduration of incubation with primary monoclonal anti�bodies (Abcam, clone 14C8) at a 1 : 400 dilution (thefinal concentration of 2.5 μg/mL) and correspondingisotypical antibodies in a 1 : 400 dilution at an equiva�lent final concentration (Abcam, clone MG2a�53)was 15–20 h; with secondary antibodies conjugatedwith fluorescent dye FITC in a final dilution of 1 : 500(Sigma, F2772), 1.5 h. After incubation, free antibod�ies were washed off with 20 volumes of phosphatebuffer solution (pH 7.4) by centrifugation at 3000 rpmfor 10 min. The supernatant was removed, and the pel�let was resuspended in 200 μL of phosphate buffersolution (pH 7.4).
The measurement of fluorescence was carried outusing a FACSCanto II (Beckon Dickinson) flowcytofluorimeter with the FACSDiva 6.0 software. ACoherent Sapphire solid�state laser with light emittedat a wavelength of 488 nm was used for fluorescenceexcitation. The fluorescence signals were recordedusing the FTIC�H parameter with a voltage of 500 V.The threshold value was 10 000, the “number of eventsper second” index was average, and the number ofanalyzed events was 5000. The fluorescence intensitywas calculated using the WinMDI 2.9 software; thenumber of specifically fluorescent cells was calculated
using the Kolmogorov–Smirnov test included in theFlowJo 7.6 software. To monitor the activity of anti�bodies (positive control), we used a culture of MCF�7human breast adenocarcinoma cells. In total, we stud�ied the ERβ expression in 83 tumor samples obtainedduring surgery (40 primary tumors and 43 metastases).
The statistical processing of quantitative dataobtained by comparing the parameters of ERβ expres�sion in different groups of patients was carried outusing the STATISTICA 6.0 software package (Stat�Soft, United States). To evaluate the differencesbetween the comparison groups by the parameters ofspecific fluorescence, we used the Student’s t test,because the values of the number of stained cells andfluorescence intensity had a normal distribution(assessed using the Shapiro–Wilk test) and the samevariance (assessed using the Levene test).
The following indicators of the ERβ expressionwere determined in this study. The expression level isthe number of cells with specific fluorescence exceed�ing this parameter for isotypical control after the incu�bation with monoclonal antibodies to ERβ. Theexpression intensity is the exceeding of the averagespecific fluorescence intensity of cells compared toisotypical fluorescence staining. The expression fre�quency is the number of patients in the comparisongroups with different ERβ expression rates.
The results of comparative assessment of the levelof ERβ expression in NSCLC tissue and lungmetastases of tumors of other primary localization areshown in Table 1. It is important to emphasize that, foraccurate quantification of this indicator, i.e., forrevealing all the cells expressing ERβ, we used theconcentrations of monoclonal antibodies at which aplateau of the specific fluorescent staining of cells isreached.
According to the results, the average level of ERβexpression in NSCLC tissue was 42.0%, and inmetastases of tumors of other primary localizationswas lower, 34.6%. The differences are small but statis�tically significant (p = 0.03).
At the same time, the data presented in Table 1show that the differences between the intensity of ERβexpression in NSCLC cells and this indicator in lungmetastases of tumors of another localization were notrevealed (p = 0.06).
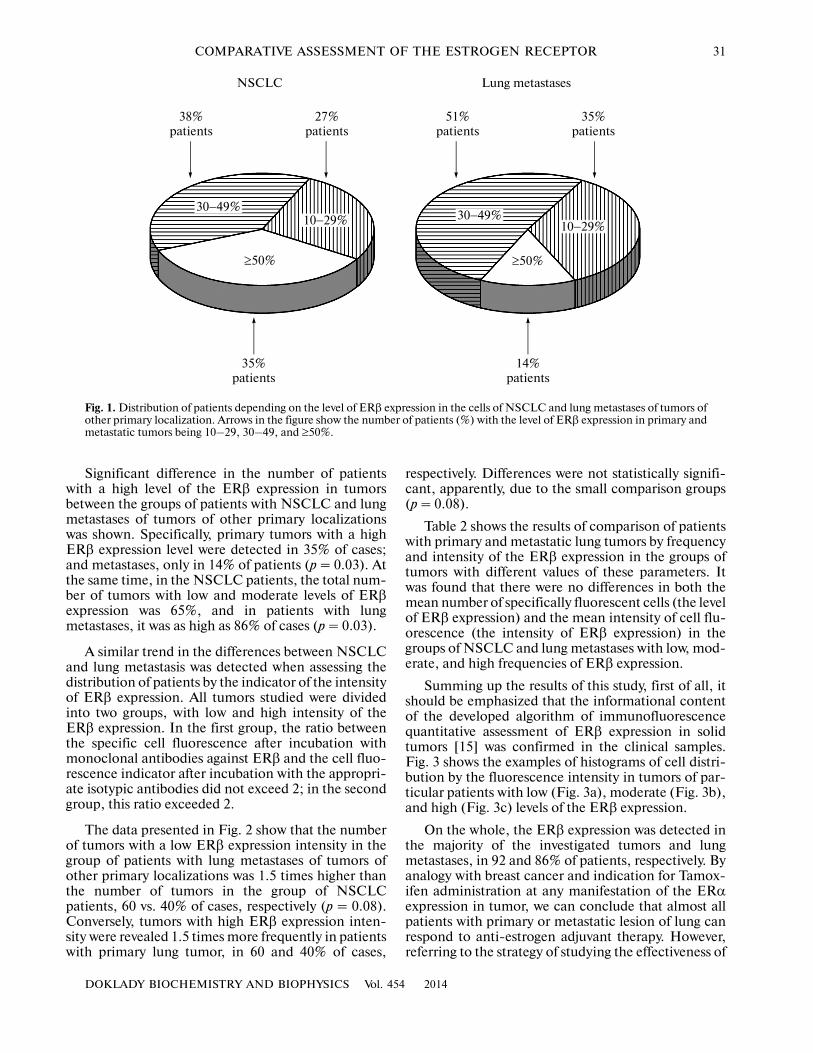
Figure 1 shows the distribution of patients withNSCLC and lung metastases of tumors of other pri�mary localizations depending on the level of ERβexpression in the tumor tissue. All tumors were dividedinto the following three groups: with low expressionlevel, ERβ were detected in less than 30% of cells(from 10 to 29%); with moderate level, ERβ weredetected in 30–49% of cells; and with high level ofexpression, ERβ were detected in no less than 50% ofcells.
Table 1. Frequency and intensity of the ERβ expression inthe tissue of NSCLC and lung metastases of tumors of otherprimary localizations
Compari�son groups
Samplesize
Level of ERβexpression (%)*
Intensity of ERβexpression (arbi�
trary units)**
NSCLC 37 42.0 ± 15.3 2.1 ± 0.8
Metastases 37 34.6 ± 12.1 2.5 ± 1.2
Significance of differ�ences between groups
p = 0.03 p = 0.06
* The number of specifically fluorescent cells (%) ± standard deviation;** The mean specific intensity of cell fluorescence (arbitrary units) ±standard deviation.
DOKLADY BIOCHEMISTRY AND BIOPHYSICS Vol. 454 2014
COMPARATIVE ASSESSMENT OF THE ESTROGEN RECEPTOR 31
Significant difference in the number of patientswith a high level of the ERβ expression in tumorsbetween the groups of patients with NSCLC and lungmetastases of tumors of other primary localizationswas shown. Specifically, primary tumors with a highERβ expression level were detected in 35% of cases;and metastases, only in 14% of patients (p = 0.03). Atthe same time, in the NSCLC patients, the total num�ber of tumors with low and moderate levels of ERβexpression was 65%, and in patients with lungmetastases, it was as high as 86% of cases (p = 0.03).
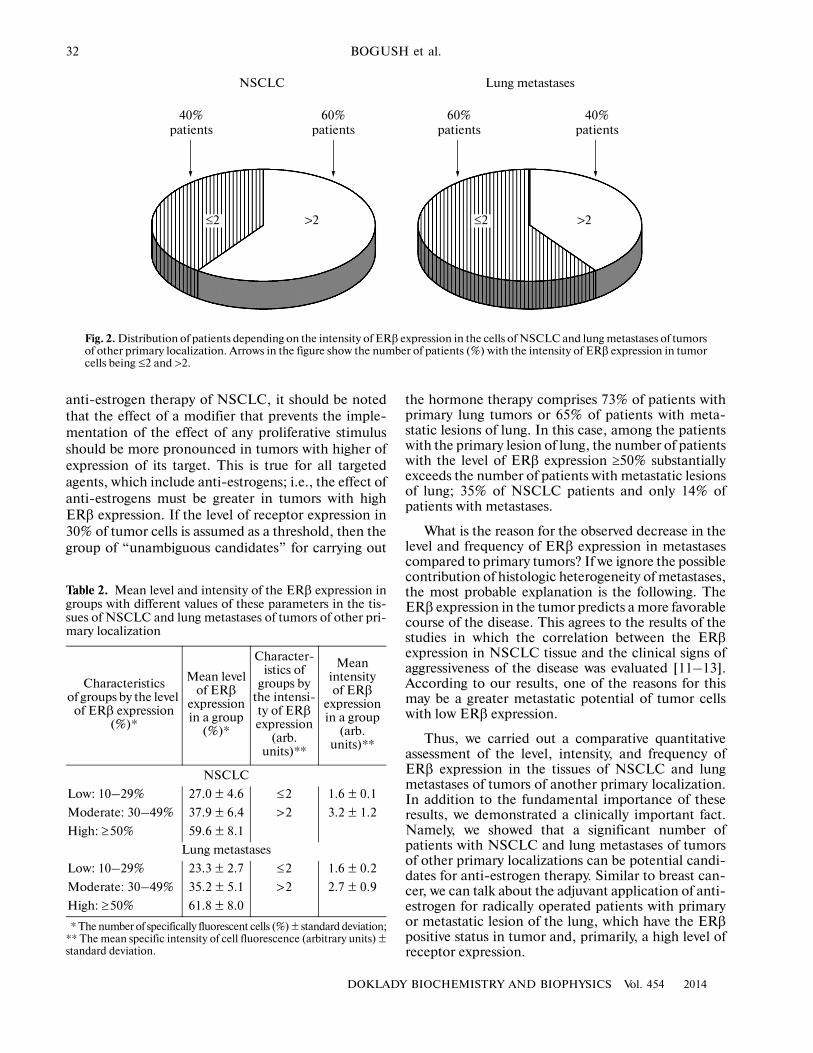
A similar trend in the differences between NSCLCand lung metastasis was detected when assessing thedistribution of patients by the indicator of the intensityof ERβ expression. All tumors studied were dividedinto two groups, with low and high intensity of theERβ expression. In the first group, the ratio betweenthe specific cell fluorescence after incubation withmonoclonal antibodies against ERβ and the cell fluo�rescence indicator after incubation with the appropri�ate isotypic antibodies did not exceed 2; in the secondgroup, this ratio exceeded 2.
The data presented in Fig. 2 show that the numberof tumors with a low ERβ expression intensity in thegroup of patients with lung metastases of tumors ofother primary localizations was 1.5 times higher thanthe number of tumors in the group of NSCLCpatients, 60 vs. 40% of cases, respectively (p = 0.08).Conversely, tumors with high ERβ expression inten�sity were revealed 1.5 times more frequently in patientswith primary lung tumor, in 60 and 40% of cases,
respectively. Differences were not statistically signifi�cant, apparently, due to the small comparison groups(p = 0.08).
Table 2 shows the results of comparison of patientswith primary and metastatic lung tumors by frequencyand intensity of the ERβ expression in the groups oftumors with different values of these parameters. Itwas found that there were no differences in both themean number of specifically fluorescent cells (the levelof ERβ expression) and the mean intensity of cell flu�orescence (the intensity of ERβ expression) in thegroups of NSCLC and lung metastases with low, mod�erate, and high frequencies of ERβ expression.
Summing up the results of this study, first of all, itshould be emphasized that the informational contentof the developed algorithm of immunofluorescencequantitative assessment of ERβ expression in solidtumors [15] was confirmed in the clinical samples.Fig. 3 shows the examples of histograms of cell distri�bution by the fluorescence intensity in tumors of par�ticular patients with low (Fig. 3a), moderate (Fig. 3b),and high (Fig. 3c) levels of the ERβ expression.
On the whole, the ERβ expression was detected inthe majority of the investigated tumors and lungmetastases, in 92 and 86% of patients, respectively. Byanalogy with breast cancer and indication for Tamox�ifen administration at any manifestation of the ERαexpression in tumor, we can conclude that almost allpatients with primary or metastatic lesion of lung canrespond to anti�estrogen adjuvant therapy. However,referring to the strategy of studying the effectiveness of
38%patients
27%patients
35%patients
NSCLC
10−29%30−49%
≥50%
30−49%10−29%
≥50%
51%patients
35%patients
Lung metastases
14%patients
Fig. 1. Distribution of patients depending on the level of ERβ expression in the cells of NSCLC and lung metastases of tumors ofother primary localization. Arrows in the figure show the number of patients (%) with the level of ERβ expression in primary andmetastatic tumors being 10–29, 30–49, and ≥50%.
32
DOKLADY BIOCHEMISTRY AND BIOPHYSICS Vol. 454 2014
BOGUSH et al.
anti�estrogen therapy of NSCLC, it should be notedthat the effect of a modifier that prevents the imple�mentation of the effect of any proliferative stimulusshould be more pronounced in tumors with higher ofexpression of its target. This is true for all targetedagents, which include anti�estrogens; i.e., the effect ofanti�estrogens must be greater in tumors with highERβ expression. If the level of receptor expression in30% of tumor cells is assumed as a threshold, then thegroup of “unambiguous candidates” for carrying out
the hormone therapy comprises 73% of patients withprimary lung tumors or 65% of patients with meta�static lesions of lung. In this case, among the patientswith the primary lesion of lung, the number of patientswith the level of ERβ expression ≥50% substantiallyexceeds the number of patients with metastatic lesionsof lung; 35% of NSCLC patients and only 14% ofpatients with metastases.
What is the reason for the observed decrease in thelevel and frequency of ERβ expression in metastasescompared to primary tumors? If we ignore the possiblecontribution of histologic heterogeneity of metastases,the most probable explanation is the following. TheERβ expression in the tumor predicts a more favorablecourse of the disease. This agrees to the results of thestudies in which the correlation between the ERβexpression in NSCLC tissue and the clinical signs ofaggressiveness of the disease was evaluated [11–13].According to our results, one of the reasons for thismay be a greater metastatic potential of tumor cellswith low ERβ expression.
Thus, we carried out a comparative quantitativeassessment of the level, intensity, and frequency ofERβ expression in the tissues of NSCLC and lungmetastases of tumors of another primary localization.In addition to the fundamental importance of theseresults, we demonstrated a clinically important fact.Namely, we showed that a significant number ofpatients with NSCLC and lung metastases of tumorsof other primary localizations can be potential candi�dates for anti�estrogen therapy. Similar to breast can�cer, we can talk about the adjuvant application of anti�estrogen for radically operated patients with primaryor metastatic lesion of the lung, which have the ERβpositive status in tumor and, primarily, a high level ofreceptor expression.
Fig. 2. Distribution of patients depending on the intensity of ERβ expression in the cells of NSCLC and lung metastases of tumorsof other primary localization. Arrows in the figure show the number of patients (%) with the intensity of ERβ expression in tumorcells being ≤2 and >2.
Table 2. Mean level and intensity of the ERβ expression ingroups with different values of these parameters in the tis�sues of NSCLC and lung metastases of tumors of other pri�mary localization
Characteristicsof groups by the level
of ERβ expression (%)*
Mean level of ERβ
expression in a group
(%)*
Character�istics of
groups by the intensi�ty of ERβ expression
(arb. units)**
Meanintensityof ERβ
expression in a group
(arb. units)**
NSCLC
Low: 10–29% 27.0 ± 4.6 ≤2 1.6 ± 0.1
Moderate: 30–49% 37.9 ± 6.4 >2 3.2 ± 1.2
High: ≥50% 59.6 ± 8.1
Lung metastases
Low: 10–29% 23.3 ± 2.7 ≤2 1.6 ± 0.2
Moderate: 30–49% 35.2 ± 5.1 >2 2.7 ± 0.9
High: ≥50% 61.8 ± 8.0
* The number of specifically fluorescent cells (%) ± standard deviation;** The mean specific intensity of cell fluorescence (arbitrary units) ±standard deviation.
40%patients
60%patients
NSCLC
60%patients
40%patients
Lung metastases
≤2≤2 >2 >2

DOKLADY BIOCHEMISTRY AND BIOPHYSICS Vol. 454 2014
COMPARATIVE ASSESSMENT OF THE ESTROGEN RECEPTOR 33
ACKNOWLEDGMENTS
This study was supported by the Russian Founda�tion for Basic Research (project nos. 13�04�01004�aand 12�04�00028�a) and grants of the President of theRussian Federation (project nos. SP_376.2012.4 andSP_359.2012.4).
REFERENCES1. Bogush, T.A., Dudko, E.A., Beme, A.A., et al.,
Biokhimiya, 2010, vol. 75, no. 12, pp. 1633–1641.2. Barkhem, T., Carlsson, B., Nilsson, Y., et al., Mol.
Pharmacol., 1998, vol. 1, no. 54, pp. 105–112.3. Raso, M.G., Behrens, C., Herynk, M.H., et al., Clin.
Cancer. Res., 2009, vol. 17, no. 15, pp. 5359–5368.4. Davydov, M.I., Polotskii, B.E., Zhuraev, E.E., et al.,
Vestn. RONTs im. N.N. Blokhina RAMN, 2011, vol. 22,no. 3, pp. 47–54.
5. Shaturova, A.S., Bogush, T.A., Dudko, E.A., et al.,Antibiot. Khimioter., 2012, vol. 57, no. 5�6, pp. 11–17.
6. Zhang, G., Liu, X., Farkas, A.M., et al., Mol. Endo�crinol., 2009, vol. 2, no. 23, pp. 146–156.
7. Schwartz, A.G., Prysak, G.M., Murphy, V., et al., Clin.Cancer Res., 2005, vol. 20, no. 11, pp. 7280–7287.
8. Ishibashi, H., Suzuki, T., Suzuki, S., et al., Cancer Res.,2005, vol. 14, no. 65, pp. 6450–6458.
9. Skov, B.G., Fischer, B.M., and Pappot, H., Lung Can�cer, 2008, vol. 1, no. 59, pp. 88–94.
10. Marquez�Garban, D.C., Chen, H.W., Fishbein, M.C.,et al., Steroids, 2007, vol. 2, no. 72, pp. 135–143.
11. Wu, C.T., Chang, Y.L., Shih, J.Y., and Lee, Y.C.,J. Thorac. Cardiovasc. Surg., 2005, vol. 4, no. 130,pp. 979–986.
12. Kawai, H., Ishii, A., Washiya, K., et al., AnticancerRes., 2005, vol. 6, no. 25, pp. 4693–4698.
13. Kawai, H., Ishii, A., Washiya, K., et al., Clin. CancerRes., 2005, vol. 14, no. 11, pp. 5084–5089.
14. Goldhirsch, A., Ingle, J.N., Gelber, R.D., et al., Ann.Oncol., 2009, vol. 8, no. 20, pp. 1319–1329.
15. Bogush, T.A., Shaturova, E.A., Dudko, et al., Vestn.Mosk. Univ., Ser. 2 Khim., 2011, vol. 52, no. 4, pp. 305–312.
Translated by G. Levit
32
0100
(a)
101 102 103 104
20%
100
(b)
101 102 103 104
41%
100
(c)
101 102 103 104
63%
Fig. 3. Examples of histograms of the NSCLC cells distribution depending on the fluorescence intensity, which characterize (a)low, (b) moderate, and (c) high levels of the ERβ expression. The fluorescence intensity (arbitrary units) is plotted along the ab�scissa; the number of cells, along the ordinate. Shaded histograms represent the distribution of cells after incubation with isotyp�ical antibodies; unfilled histograms, after incubation with specific antibodies to ERβ.
 KANEDA, …[AJS] works not over $\mathrm{F}_{p},$ $\mathbb{Q}(\zeta)$ or $\mathbb{Z}$, but over various localizations of the completions of](https://img.pdfslide.tips/doc/110x75/5ed6f67a538823436c4d4a90/title-a-survey-of-ajslusztig-program-kaneda-ajs-works-not-over-mathrmfp.jpg)