Embed Size (px)
Citation preview

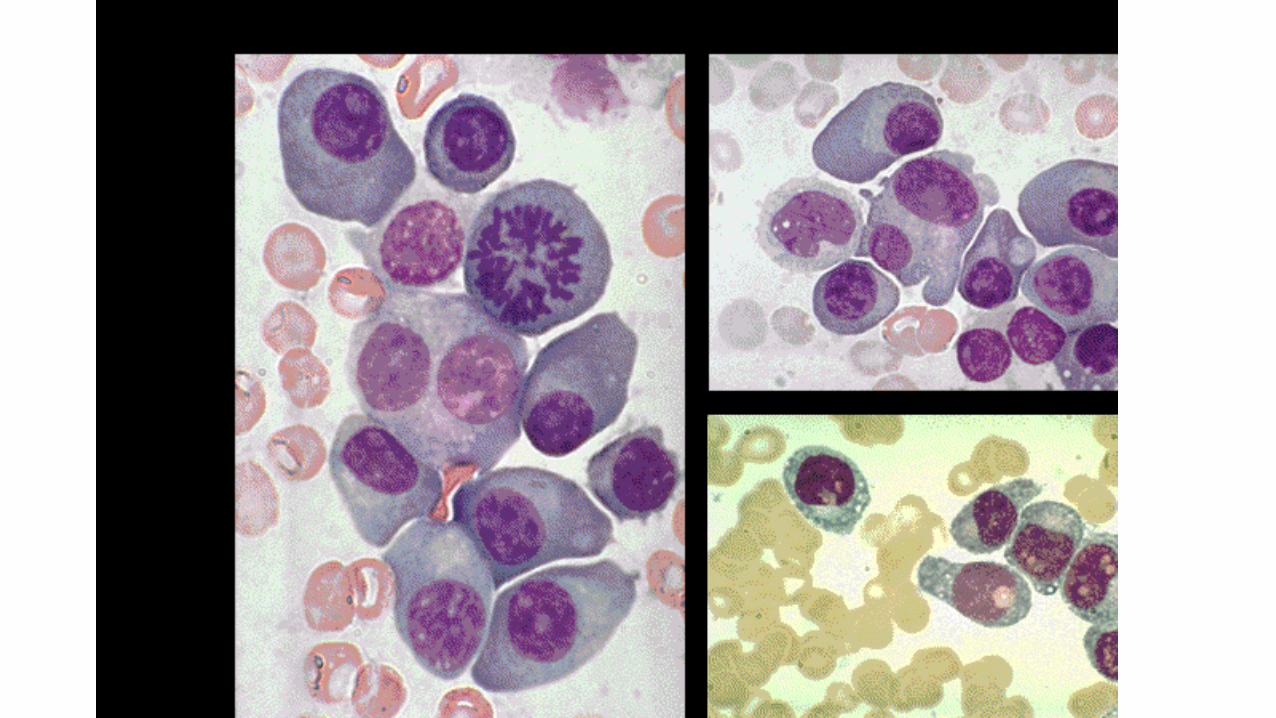
De afwijkende witte bloedcel: Van leukemieën, lymfomen en myeloma.
IWC Domus Medica, 06.04.2016, Molenheide.


De hematopoïese.
• Complex proces met regulatie vraag-aanbod.
• Enorme productie: 150x106 Rbc
150x106 Tr
50x106 Granulocyten
Per MINUUT !!
• Vlot x 3 tot x 8 bij bloeding of infectie.
• Stamcellen kunnen uitrijpen tot rijpe bloedcellen én zichzelf in stand houden door verdubbeling.
• Rol van groeifactoren: G-CSF, EPO en TPO.

Hematopoïese: Het beenmerg.

Hematopoïese: stamcel model.
• Pluripotente stamcel
• Progenitor cel
• Rol van cytokines: IL-1, IL-6, IFN-g, G-CSF, EPO, …
• Rol van micro-milieu

Overzicht hematologische tumoren.
• Leukemie:
• Acuut
• Chronisch
• Myeloïd
• Lymfoïd
• Multipel Myeloma
• Ziekte van Hodgkin
• Non-Hodgkin lymfomen

De leukemieën.
• Virchow 1846 leukos
• Definitie = neoplastische woekering in één of meerdere van de bloedvormende cellijnen.
• = Beenmerg-aandoening => bloed en evtl andere weefsels.
• 4 types: ALL – AML – CLL – CML
• Verschil in: spontane evolutie – uitrijping leukemische cellen –klinische expressie – behandeling.
• Chronische vormen + 50%.



Ontstaan van hematologische kanker.

ALL en AML.• Incidentie: 4 à 5/100.000/jaar.• Man > Vrouw.• AL bij volw: 85% AML – Bij Kk. >> ALL.• Op kinderleeftijd is ALL frequentste mal. tumor.• Klachten: moeheid ! - infecties – bloedingen.Minder freq: botpijnen – metabole stoornissen –
extramedullaire lokalisaties.• Kliniek: bleekzucht, koorts en petechieën. Bij ALL: adenopathieën, hepato/splenomegalie. Tandvleeslokalisaties (M4/5), intracerebrale
bloedingen, cerebrospinale aantasting (ALL, M3).

Oorzakelijke factoren AL.
• Eigenlijke oorzaak onbekend.
• Toegenomen risico bij:
• Congenitale afwijkingen: trisomie 21, immuundeficiënties, eeneiïge tweeling.
• Infecties: HTLV?
• Carcinogenen: benzeen, farmaca, ioniserende stralen.

Classificatie AML.
• M1: myeloblastair, niet uitrijpend• M2: myeloblastair, wel uitrijpend 50-60%• M3: promyelocytair
5-15%• M4: myelomonocytair
20-30%• M5: monocytair
5-10%• M6: erythroleukemie
<5%• M7: acute megakaryoblasten <5%


Major cytogenetic subgroups of acute myeloid leukemia (AML) (excluding acute promyelocytic leukemia) and associated gene mutations.
Konstanze Döhner, and Hartmut Döhner Haematologica 2008;93:976-982
©2008 by Ferrata Storti Foundation

Kaplan–Meier survival estimates, according to genotype, in younger adult patients with cytogenetically normal AML. Data are shown for relapse-free survival (Panel A) and overall survival (Panel B).
Konstanze Döhner, and Hartmut Döhner Haematologica 2008;93:976-982
©2008 by Ferrata Storti Foundation

Classificatie ALL.
• Common-ALL 70%
• T-ALL 10-20%
• B-ALL 1-2%
• Null-ALL 10-15%



Diagnose van AL.
• Blastaire populatie in beenmerg: > 30% FAB (of 20% volgens WHO).
• Bloed: leukemische populatie kan, maar niet steeds –leukopenie zonder blasten + 10% - hyperleukocytose > 100.000 bij 10-15%.
• Meestal anemie, granulopenie en thrombopenie.
• Soms stollings- en metabole afwijkingen.


Prognose van AL.
• Afhankelijk van veel factoren:
• Leeftijd (M: < of > 60 jr – L: < of > 14 jr)
• Chromosomale afwijkingen
• Tumormassa
• Morfologie (ALL>AML)
• PS
• Geslacht
• Na MDS
• Secundaire leukemie
• …


Behandeling van AL.
• Zonder behandeling < 3 maand.
• Combinatiechemotherapie:
• ALL: vincristine, corticoïden, antracyclines, cyclofosfamide en asparaginase. Belang van intrathecale therapie!
• AML: cytarabine, etoposide en antracyclines.
• Inductiechemotherapie – consolidatietherapie –stamceltransplantatie.
• Belangrijk deel = supportief!

• ALGEMENE HEMATOLOGIE
• Hemoglobine 13.4 g/dl 13.1 - 17.2
• Hematocriet 0.40 ratio 0.39 - 0.50
• Rode bloedcellen 4.54 10.E12/l 4.5 - 6.5
• MCV 88.6 fl 81 - 101
• MCH 29.5 pg 27 - 35
• MCHC 33.2 g/dl 32 - 36
• Bloedplaatjes 167 10.E9/l 140 - 440
• Witte bloedcellen + 60.2 10.E9/l 4.5 - 11.0
• Myelocyten + 13 % 0 - 0
• Metamyelocyten + 2 % 0 - 0
• Staven + 7 % 0 - 5
• Neutrofielen 63 % 40 - 75
• Eosinofielen 1 % 0 - 6
• Basofielen + 7 % 0 - 1
• Lymfocyten - 4 % 15 - 40
• Monocyten - 3 % 4 - 12
• Commentaar RBC Anisocytose +
• Reticulocyten 17.3 / 1000 RBC 5 - 23
• ALGEMENE STOLLING
• Quicktijd 83 % 60 - 100
• INR (internationale ratio) 1.19 ratio
• Cefalinetijd (aPTT) 31 sec. 22 - 38
• Fibrinogeen 320 mg/dl 160 - 415


CML: een aandoening gekenmerkt door eenunieke moleculaire afwijking.
• Typisch klinisch verloop: rustige chronische fase –acceleratiefase – blastencrisis (terminale fase).
• Philadelphia (Ph) chromosoom = Unieke chromosomale abnormaliteit.
• Bcr-Abl tyrosine kinase: – De moleculaire abnormaliteit verantwoordelijk voor de
transformatie van een hematopoïetische progenitor in een maligne cloon.

Incidentie van CML.
Type leukemie Incidentie per 100,000*Overall 6–10
CML 1–2CLL 2–3
AML 2–3ALL 1–2
*1990, Western hemisphere. CLL = chronic lymphoid leukaemia; AML = acute myeloid leukaemia; ALL = acute lymphoid leukaemia.Black RJ et al. Eur J Cancer. 1997;33:1075-1107.


Klinisch verloop CML.
Chronic phase
Median duration 5–6 years
Accelerated phase
Median duration6–9 months
Blast crisis
Median survival3–6 months
Advanced phases

De cytogenetische abnormaliteit in CML:het Ph Chromosoom.
1 2 3 4 5
6 7 8 10 119 12
13 14 15 16 17 18
19 20 21 22 x Y

CML: Een beetje geschiedenis.
• 1845: eerste beschrijving van CML.
• 1960: Philadelphia chromosoom.
• 1984: Breakpunten chromosoom
22q11.
• 1992: Inhibitie van tyrosine kinase
activiteit door 2-phenylaminopyri-
midine.
• 2000: Start IRIS.

Philadelphia chromosoom t(9;22)
p210BCR-ABL
p190BCR-ABL
p230BCR-ABL

Ph Chromosoom en bcr-abl Gen.
bcr-abl
ablFUSION PROTEIN
WITH TYROSINEKINASE
ACTIVITY
22
bcr
Ph (or 22q-)
99 q+
1
p210Bcr-Abl
p185Bcr-Abl
2-11
2-11
Chromosome 9
c-bcr
Chromosome 22
c-abl
2-11
Exons
Introns
CML Breakpoints
ALL Breakpoints
t(9;22) translocation bcr-abl gene structure

• ‘Cancer is hundreds or thousands of unique molecular diseases”
• George D. Lundberg, The Scientist

CML: Therapie.
• 1865: Arsenicum.
• 1903: Miltbestraling.
• 1953: Busulfan.
• 1964: Hydroxyurea.
• 1975: Stamcel transplantatie.
• 1983: Interferon.
• 1999: Imatinib.
• 2005: Dasatinib, Nilotinib.

Allogene SCT is geassocieerd met belangrijkemorbiditeit en mortaliteit in CML.
National Marrow Donor Program (NMDP) overview slide presentation. Available at http://www.marrow.org/NMDP/SLIDESET/sld031.htm#slide. Accessed 17 June 2002.
Survival by Disease Stage, June 2001, based on transplants 1987 – Feb 2001.
P=.0001


Werkingsmechanisme van Glivec.
Goldman JM, Melo JV. N Engl J Med. 2001;344:1084-1086.




Nilotinib Dasatinib
Afgeleid van imatinib Ontwikkeld als inhibitor van
Scr
20-50 x in vitro ~ 300 x in vitro



CRP 24.9 mg/l < 5.0 Hemoglobine 8.2 g/dl 13.1 - 17.2 Hematocriet 0.27 ratio 0.39 - 0.50 Rode bloedcellen 3.15 10.E12/l 4.5 - 6.5 MCV 84.6 fl 81 - 101 MCH 26.1 pg 27 - 35 MCHC 30.9 g/dl 32 - 36 Bloedplaatjes 887 10.E9/l 150 - 450 Witte bloedcellen 331.1 10.E9/l 4.5 - 11.0 Blasten 4 % 0 - 0 Promyelocyten 8 % 0 - 0 Myelocyten 5 % 0 - 0 Metamyelocyten 7 % 0 - 0 Staven 8 % 0 - 5 Neutrofielen 53 % 40 - 75 Eosinofielen 6 % 0 - 6 Basofielen 9 % 0 - 1 Lymfocyten 0 % 15 - 40 Monocyten 0 % 4 - 12 Atypische lymfocyten 0 % 0 - 0 Plasmocyten 0

CRP 6.5 mg/l < 5.0 Hemoglobine 11.6 g/dl 12.6 - 17.4 Hematocriet 0.35 ratio 0.37 - 0.51 Rode bloedcellen 3.84 10.E12/l 4.5 - 6.5 MCV 90.7 fl 81 - 103 MCH 30.2 pg 27 - 34 MCHC 33.3 g/dl 31 - 36 Bloedplaatjes 176 10.E9/l 150 - 450 MPV 7.0 fL 7.4 - 11.4 Witte bloedcellen 276.1 10.E9/l 4.5 - 11.0 Neutrofielen 0 % 40 - 75 Eosinofielen 0 % 0 - 6 Basofielen 0 % 0 - 1 Lymfocyten 98 % 15 - 40 Extra resultaat: Iets grotere lymfocyten met licht geblokt aspect

Chronische lymfatische leukemie (CLL).
• = laaggradig NHL.
• Incidentie: 3/100.000/jaar.
• Frequentiemaximum + 60 jaar.
• Diagnose: leukocytose (lymfocytose), adenopathieën en splenomegalie.
• Prognose: overleving RAI stadium 0 = 10-15 jaar.
• Behandeling: ‘wait-and-see’ – po of IV chemotherapie – SCT.





Ziekte van Hodgkin (HD).
• Incidentie: 2/100.000/jaar (m:2/v:1)• Meestal 3° levensdecade; 2° piek 50-60 jaar.• Reed-Sternbergcellen.• EBV?• 4 Hoofdtypes: Lymfocytenrijk Nodulair
Diffuus
Nodulaire scleroseGemengde cellulariteit Lymfocytendepletie


Ziekte van Hodgkin.
• Kliniek: - adenopathieën
- feci, jeuk, vermagering
- pijn na alcohol (?)
• Stadia: - I, II, III, IV
- A, B
- E, S


Ziekte van Hodgkin: Prognose.
• Stadium
• Leeftijd
• Histologisch type
• Aanwezigheid van B-symptomen
• Ziektevrije 5-jaars overleving: 70-95% voor stadia I-II; 50-60% voor stadia III-IV.

Ziekte van Hodgkin: Therapie.
• Radiotherapie (st. I en II).
• Combinatiechemotherapie (ABVD, BEACOPP, Stanford V, …).
• Combinatie radio/chemotherapie.
• Stamceltransplantatie - Autoloog (A)
- Allogeen (a)

Non-Hodgkin lymfomen (NHL).
• = kwaadaardige proliferaties uitgaande van lymfoïde cellijnen.
• 6-10/100.000/jaar.
• Incidentie AIDS
Milieufactoren?
• Kliniek: - pijnloze adenopathie
- splenomegalie
- extranodulaire lokalisaties (huid, GI, …)


NHL.
• Stadia: cfr. HD.
• Klassificatie: van laag- tot hooggradig.
• Cfr. CLL als prototype laaggradig NHL!
• Prognose: ~ type
~ stadium
~ tumormassa
~ leeftijd







NHL: Therapie.
• Wait-and-see
• Radiotherapie
• Polychemotherapie
• Autologe stamceltransplantatie (ASCT)
• Allogene stamceltransplantatie (aSCT)
• ‘Mini’, ‘Lite’ of niet-myeloablatieve transplant
• Monoclonale antilichamen
• Immunotherapie

Monoclonale AL: Werkingsmechanisme.

Event-free en overall survival in oudere patiënten met DLBC behandeld met CHOP vs. MabThera + CHOP.
Coiffier B, et al. N Engl J Med 2002;346:235–43
1.0
0.8
0.6
0.4
0.2
0
1.0
0.8
0.6
0.4
0.2
0
Pro
bab
ility
of
eve
nt-
fre
e s
urv
ival
Ove
rall
pro
bab
ility
o
f su
rviv
al
0 0.5 1.0 1.5 2.0 2.5 3.0 0 0.5 1.0 1.5 2.0 2.5 3.0
Years after randomisation Years after randomisation
CHOP + MabThera
CHOP
CHOP + MabThera
CHOP
p<0.001 p<0.007
202 177 137 108 63 19197 144 101 72 42 17
CHOP plusMabTheraCHOP
No. at risk
202 187 167 118 64 21197 171 136 96 58 16
CHOP plusMabTheraCHOP
No. at risk

MabThera plus CHOP voor DLBCL in British Columbia: progressie-vrije overleving.
1.0
0.8
0.6
0.4
0.2
0
Years
0 1 2 3 4
Post-MabThera
Pre-MabThera
p=0.0009
Sehn LH, et al. Blood 2003;102:29a (Abstract 88)

Overleving indolent NHL IV in MD Anderson 1977-1997.
Years
p=0.001
1992–97
1988–92
1982–88
1977–82
Aliv
e (
%)
100
75
50
25
01 5 10 15 20
Years
Total
Deaths
Median survival
1977–82 96 68 7 years
1982–88 131 69 11 years
1988–92 136 49 NR
1992–97 142 24 NR
Courtesy of P McLaughlin

De toekomst?

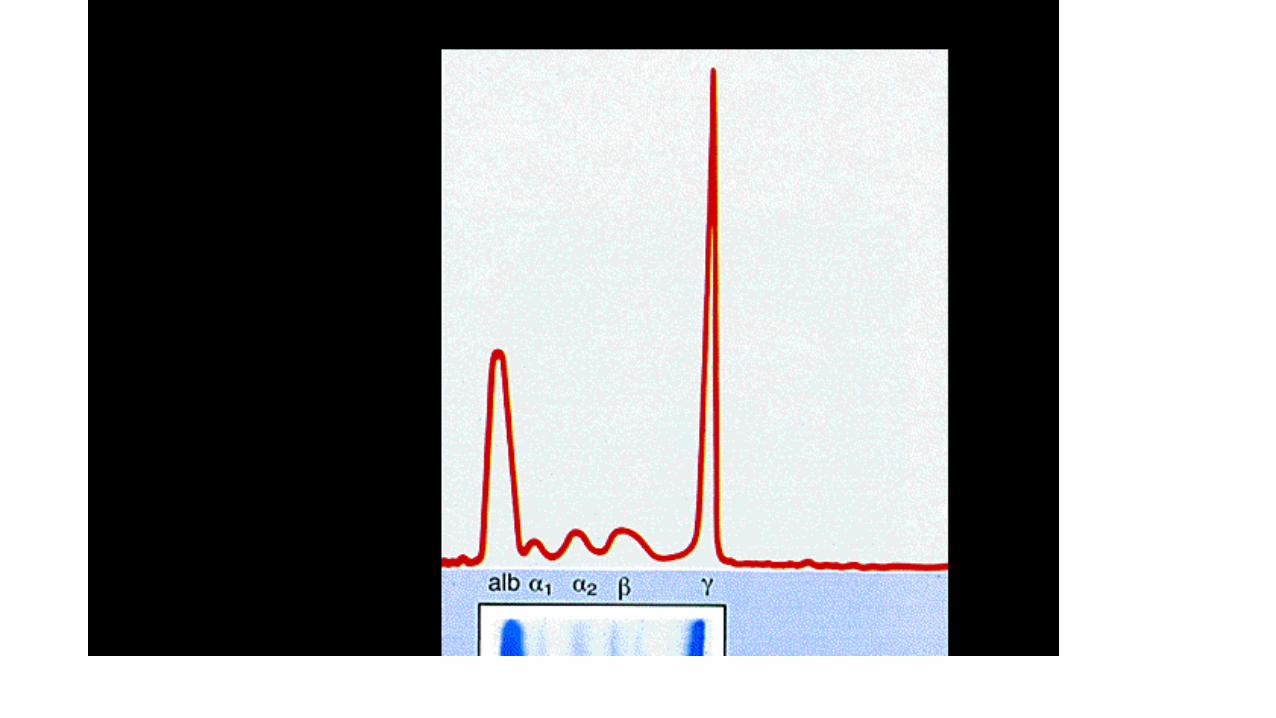
Totaal eiwit 82.7 g/L 64 - 83 Albumine % 35.1 % 54.6 - 65.7 Alfa 1 globulines % 4.9 % 3.0 - 5.7 Alfa 2 globulines % 7.6 % 7.1 - 12.1 Bèta globulines % 6.5 % 9.2 - 13.8 Gamma globulines % 45.9 % 9.4 - 18.2 fractie 1 39.9 % Albumine 29.0 g/L 39 - 54 Alfa 1 globulines 4.1 g/L 2.0 - 4.0 Alfa 2 globulines 6.3 g/L 5.0 - 9.0 Bèta globulines 5.4 g/L 7.0 - 11.0 Gamma globulines 38.0 g/L 7.0 - 15.0 fractie 1 33.0 g/L Besluit EP Extra fractie in de gamma-zone: zie immunofixatie. Immunofixatie Monoclonaal IgA kappa. Vrije Kappa ketens 26.5 mg/l < 19 Vrije Lambda ketens <4.7 mg/l < 26 Vrije Kappa/Lambda Kan niet berekend worden 0.26 - 1.65 IgA 38.71 g/L 0.70 - 4.00 IgG 2.17 g/L 7.00 - 16.00 IgM 0.12 g/L 0.40 - 2.30 Beta-2 microglobuline 2.46 mg/l 0.70 - 1.80

Risk of progression of MGUS to myeloma or related disorder using a risk-stratification model
that incorporates the FLC ratio and the size and type of the serum monoclonal protein.
S. Vincent Rajkumar et al. Blood 2005;106:812-817
©2005 by American Society of Hematology

HypercalcaemiaOncological Emergencies
Multipel Myeloma
Multipel Myeloma.
–Wat is multipel myeloma (MM)?–Historiek–Epidemiologie–Kliniek; symptomatologie–Stagering en prognostische factoren–‘Klassieke’ (chemo)therapie–Ondersteunende therapie–Nieuwe behandelingen

Multipel Myeloma: Wat?
Maligniteit van plasmacellen.
Myelum = merg Multipel = meerdere
Meestal: wervels, ribben, bekken en schedel.
Soms: solitair plasmocytoma.
Zelden: weke delen plasmocytoma.

Sarah Newburry (1844)Kyle. Br J Haematol, 2001
Multipel myeloma: Historiek (I).
1845: Thomas Alexander McBean door Dr. William Macintyre.
1848: Dr. Henry Bence Jones publiceert resultaten urine.
1873: Term ‘Multipel myeloma’ gebruikt door Rustizky.
1889: Otto Kahler publiceert klinische beschrijving van multipel myeloma.

Otto Kahler

Multipel myeloma: Historiek (II).
1890: Ramon y Cajal geeft microscopische beschrijving van plasmacellen.
1900: Wright ontdekt dat MM-cellen plasmacellen zijn.
1903: Weber beschrijft de lytische MM-letsels op RX.
1953: Introductie van immunoelektroforese.
1962: Eerste succesvolle behandeling met alkeran.

Multipel myeloma: Historiek (III).
1976-92: Verschillende chemotherapie-schemata => geen verschil. (1984: VAD)
1996: Autologe stamcel transplantatie beter dan conventionele chemo? (Attal)
1997: HHV-8 speelt mogelijks rol in ontstaan.
1999: Thalidomide werkzaam in herval/refractaire ziekte.

Multipel myeloma: Epidemiologie.
Westerse wereld: 3-4/100.000/jaar.
+ 1% van alle kankers.
Zwarte Amerikanen: 9-10/100.000/jaar.
China: < 1/100.000/jaar.
Man/Vrouw: 3/2.
Toenemende incidentie met de leeftijd.

Multipel myeloma: Epidemiologie (2).
• Palumbo, EHA ’07: • Torino: pop. 902.000
• 1974: 5.9/100.000
• 2002: 8.9/100.000
• 31%: 25-64 years
• 36%: 65-75 years
• 33%: 75-101 years


5-yrs-OS during 1971-00 in England & Wales.
0
20
40
60
80
100
1971-
1975
1976-
1980
1981-
1985
1986-
1990
1991-
1995
1996-
1999
2000-
2001
Period of diagnosis
%
Men
Women

Natuurlijk verloop van MM.
MGUS of smoldering myeloma
Asymptomatisch Symptomatisch
ACTIEF MYELOMA
M P
rote
in (
g/L
)
20
50
100
1. RELAPS
2. RELAPS
REFRACTAIRE RELAPS
1° lijns therapie
Plateau remissie
2° lijnstherapie
3° lijnstherapie

Multipel myeloma: Oorzaken.
• Radiatie? Niet bewezen in Hiroshima en Nagasaki bij overlevers van de bom.
• Socio-economische status? Vanaf ‘70 niet.
• Nicotine? Cohort-studie bij > 250.000 US veteranen gedurende 26 jaar: geen invloed.
• Beroep? Landbouwers ++ Metaalbewerkers + Expositie aan benzeen - Schilders + Petroleumraffinaderij - Hout-, leder- en textielindustrie + Kappers ++

MM: Oorzaken (2).
• Substantial environmental etiologic component? Complex interactions between genes and environment?
• Independent risk factors and modifiers of each other?
• New bioaccumulations of toxins in resident coastal dolphins signal dangers of human myeloma. Brian Durie, et al; ASH ’06.
• Alaska, Florida, Japan, Sweden and coastal UK.
• Highly significant correlation between fish contamination/consumption and excess risk of human myeloma.
• Water repellants, flame-retardants, …

MM: oorzaken (3).

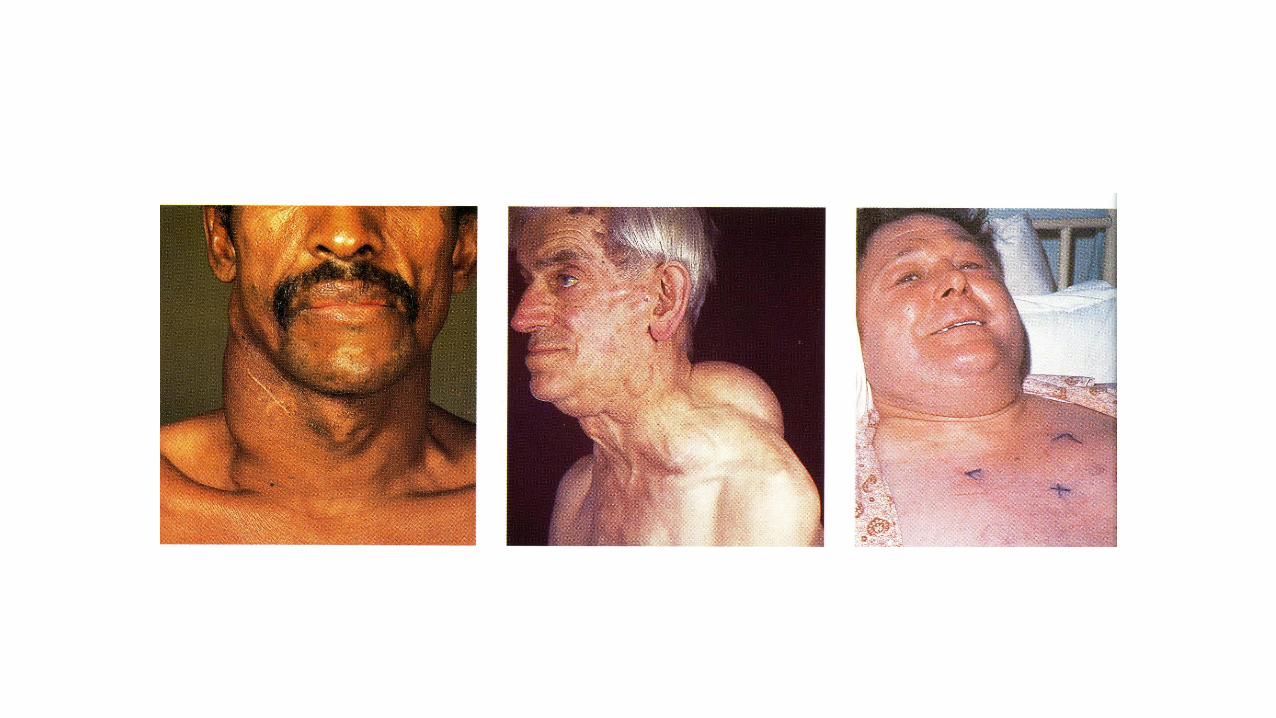
Multipel myeloma: Kliniek.
+ 70% pijn in wisselende mate.
Vermoeidheid en algemene malaise.
Toename infecties (Pneumococ, Herpes, ..).
Hypercalcemie (~ 30%): nausea en dorst.
Hyperviscositeit (< 10%): neusbloeding, hoofdpijn, duizeligheid, …
Neurologische problemen (tintelingen, verlamming, …).
Spontane breuk.

Multipel myeloma: Diagnose.
Bloedonderzoek met immunoelektroferese, immunofixatie, biochemie, CRP, immuunglobulinebepaling, FLCA (!), …
Urine onderzoek naar Bence Jones eiwitten.
RX Skelet.
Beenmergonderzoek.
NMR wervelzuil (?).

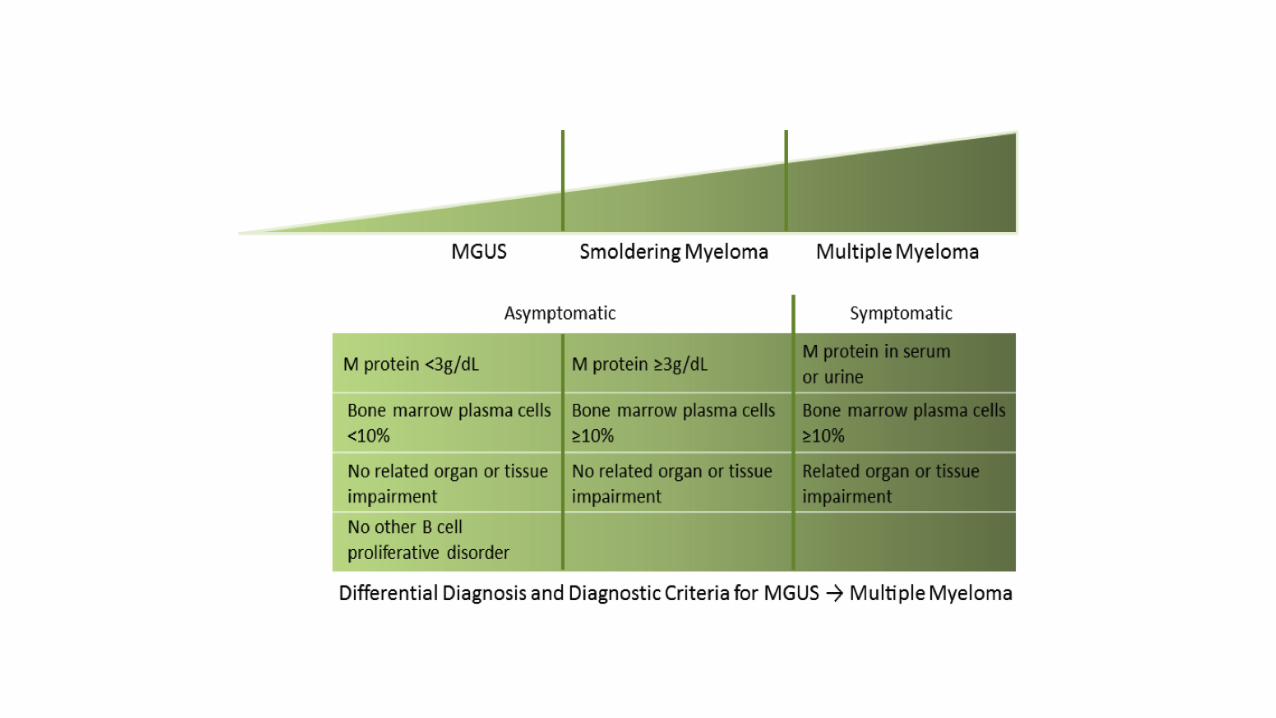
Multipel Myeloma:Minimale criteria voor diagnose.
Minstens 10% plasmacellen in het beenmerg of 1 plasmocytoma plus 1 van de volgende:
M-proteïne in serum (> 3 g/dl)
M-proteïne in urine
Lytische botletsels
Afwezigheid van weefselziekten, chronische infecties, carcinoma of lymfoma.





Multipel myeloma: Stagering.
1975: Salmon en Durie.
Nieuwe parameters sinds: b2M, labeling index, chromosomal aberrations (chrom. 13 en 11q), FISH defined gain of 1q21 (CKS1B)
Merlini 1980, MRC 1980, Cavo 1989, Greipp 1998, Bladé 1989, San Miguel 1989, San Miguel 1995, IMWG 2005

Classificatie volgens Salmon en Durie(1).
Stadium I: Alle volgende kenmerken:
Hemoglobine > 10g/dl
Calcemie: normaal.
RX: maximaal 1 plasmocytoom.
Lage M-component: IgG < 5 g/dl,
Ig A < 3 g/dl, urine lichte ketens < 4 g/d.
Stadium II: past niet bij I of III.

Classificatie volgens Salmon en Durie (2).
Stadium III: Een of meer van volgende:
Hemoglobine < 8.5 g/dl.
Calcemie verhoogd.
Meerdere botletsels.
Hoge M-component: IgG > 7 g/dl,
IgA > 5 g/dl, urine lichte keten > 12 g/d.
Subclassificatie:
A: normale nierfunctie.
B: abnormale nierfunctie.



Normal MGUS Myeloma
Progression to MyelomaGene Expression Analysis.
Davies FE, et al. Blood. 2003;102:4504-4511.

Overall survival of MM patients from the start of therapy based on 70 highly overexpressed or underexpressed genes distinguished 3 groups of patients: good,
intermediate or poor prognosis
Gene Expression Profiling Predicts Outcome
0.0
0.2
0.4
0.6
0.8
1.0
P < .0001
0 10 3020 40 50 60
R2 = 0.46
Group 1, 7 / 125 median NR*
Group 2, 36 / 159 median NR
Group 3, 33 / 67, Median 36.1
Pro
po
rtio
n S
urv
ivin
g
a) b)
Deaths/ N
Months From Start of Therapy
*NR= not reached



Multipel myeloma: Bifosfonaten.
Bifosfonaten: binden op oppervlak van beschadigde botten => vermindering botdestructie.
In combinatie met chemotherapie, minder botletsels => minder pijn.
Nut van pamidronate (Aredia) en zoledronate (Zometa).
Cave ONJ!



ONJ

Bifosfonaat necrose onderkaak



a Cox model adjusted for chemotherapy, and minimization factors.
Riskreduction
Hazard ratio (ZOL versus CLO)
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8 2
P value
.01180.842
16%
In favor of ZOL In favor of CLO
OS
.017912%0.883
PFS
ZOL significantly reduced the relative risk of death by 16% vs CLO
(HR = 0.842; 95% CI = 0.736, 0.963; P = .0118)
Morgan GJ, et al, Lancet. 2010;376:1989-1999.
MRC Myeloma IX: Verbetering van OS en PFS met ZOL vs CLOa

Supportieve maatregelen: Skeletale complicaties.
Pathologische fracturen, ruggemerg-compressie, pijn en/of hypercalcemie.
Vooral gevolg van toegenomen osteoclasten-activiteit, op zijn beurt gevolg van om. IL-1, IL-6, en TNF.

Supportieve maatregelen: Skeletale complicaties.
Bifosfonaten (cfr. supra).
Patiënten moeten zo actief mogelijk zijn, maar onnodige traumata vermijden.
Pijnstilling zo nodig.
Behandeling fracturen; kyfoplastie.
Eventuele radiotherapie.

Huidige behandeling van MM botziekte.
• Bisfosfonaten• Pamidronaat
• Zoledronaat
• Heelkunde• Vertebroplastie
• Ballon kyfoplastie
• Radiotherapie
• Systemische therapie van myeloma
Roodman GD. Hematology Am Soc Hematol Educ Program. 2008:313-319.

Supportieve maatregelen: Hypercalcemie.
Verminderde eetlust, misselijkheid, overgeven, polydipsie, polyurie, obstipatie, zwakte, gedragswijzigingen en verwardheid, hartkloppingen.
Behandeling met vocht IV, diuretica (Lasix), corticoïden en bifosfonaten.

Supportieve maatregelen: Anemie.
1/3 tot 60% patiënten wellicht nut van erythropoïetine.
Niet alleen minder transfusienood, maar ook betere levenskwaliteit.
Antitumoraal effect in vitro !
40.000 E SC/week.

Supportieve maatregelen: Nierfalen.
Tgv. ‘myeloma nier’ (aanwezigheid van neerslag met monoclonale lichte ketens, albumine, fibrinogeen) en/of hypercalcemie.
Extra effect van dehydratatie, infectie, NSAIDs en contrast bij RX-onderzoek (!), aminoglycosides (AB) en hyperuricemie.
Amyloïd depositie in 10-15%.

Supportieve maatregelen: Nierfalen.
Urinedebiet van minstens 3 liter/24 uur.
Opvangen hypercalcemie (cfr. supra).
Allopurinol (ZyloricR) zo hyperuricemie.
Corrigeren electrolieten.
Chemotherapie met VAD.
Plasmaferese soms.
Nierdialyse bij irreversibel nierfalen.

Supportieve maatregelen: Infecties.
Snelle en adequate therapie van bacteriële infecties is essentieel.
Vaccinaties tegen pneumococcen en influenza.
Peni profylaxie bij recurrente pneumococceninfecties.
Intraveneuze immunoglobulines bij recurrente infecties.

Supportieve maatregelen: Neurologische problemen.
Ruggemergcompressie vermoeden bij ernstige rugpijn en zwakte of tintelingen thv. de onderste ledematen.
Soms urineblaas- of darmdysfunctie.
NMR !
Dringende radiotherapie en dexamethasone.
Soms chirurgische decompressie vereist.

Supportieve maatregelen: Hyperviscositeit.
Mond- of neusbloeding, verminderd zicht, neurologische symptomen, hartfalen.
Meestal bij hoge IgA-titers, zelden bij IgG.
Plasmaferese afhankelijk van symptomen en oogfundusafwijkingen; NIET van plasmaviscositeit.

Supportieve maatregelen: Emotionele ondersteuning.
Emotionele ondersteuning zeer belangrijk.
Wijzen op positieve effecten van de therapie.
Substantieel aantal patiënten overleeft langer dan 10 jaar.

HypercalcaemiaOncological Emergencies
Multipel Myeloma
CRABSlimCRAB



Multipel Myeloma: Nieuwe therapieën.
Gericht tegen tumorcellen.
Gericht tegen factoren in micromilieu die groei en overleving van tumor bevorderen.

Factoren in micromilieu.
Anti-angeiogenese:
Thalidomide.
IMiDs (immunomodulatory drugs).
Proteasome inhibitoren (proteasomes regelen cel cyclus progressie): PS-341.
Inhibitie van TNFa: Thalidomide, PS-341,
...
VEGF receptor inhibitoren.

Hideshima T & Anderson KC. Nat Rev Cancer 2002;2:927-937.
Interactie van MM Cellen en het BM Micromilieu.

Thalidomide: historiek.
• 1956: introductie als slaapmedicatie.
• 1958: gepositioneerd bij ZS-braken.
• 1961: 10.000 kinderen met malformaties.
• 1962: wereldwijd van markt gehaald.
• 1999: Barlogie (MIRT) - N=84 met refractair/relaps MM: 1/3 respons.
• 1999-03: bevestigd door MD Anderson, Mayo Clinic, ...

Bijwerkingen thalidomide.
Slaperigheid (cfr. SoftenonR).
Obstipatie (cave: + pijnstillers).
Polyneuropathie (tintelingen).
Huidrash.
Zeldzamer: syncopes, ...
CAVE teratogeniciteit!!

Lenalidomide (CC-5013)
Pomalidomide(CC- 4047)
N
NH
O O
O
NH2
N
NH
O
O O
O
NH2
N
NH
O
O
O
O
Thalidomide


Bortezomib: Mechanisms of action.
Rajkumar et al. J Clin Oncol 2005;23:630
Inhibition NFkB
Activation of caspase
Overcome drug resistance
Inhibits binding myeloma cell to stroma
Inhibits angeiogenesis
Inhibits interactions mediated by cytokines
Microenvironment
Myeloma cell

Structuur van proteasomen.
• Proteasomen:• Cylinder van enzymes
• Aanwezig in cytoplasma en kern van alle eukaryote cellen
• > 30 verschillende proteïnes
19S cap
19S cap
20Score

Proteasomen.
• Verantwoordelijk voor activatie/degradatie van regulerende proteïnes.
• Belangrijk regelmechanisme van:
• Gen expressie
• Celcyclus
• Angiogenese
• Apoptose
• Tumorinteractie met micromilieu
Cell Cycle
Angiogenesis
Apoptosis
Myeloma cell interaction with microenvironment

Proteasome inhibitie: Werkingsmechanisme van bortezomib.
De 26S proteasome is een groot proteïne complex dat eiwitten degradeert
Bortezomibis een reversibeleinhibitor van de chymotrypsine-likeactiviteit van de 26S proteasome
Inhibitie van de 26Sproteasome voorkomtproteolyse van proteïnes, wat kan leiden tot verandering van multipele signaal cascades in de cel.
1
2
3



Velcade: Bijwerkingen.
• Meestal mild tot matig.
• Tijdig vermelden ikv. dosisaanpassing!
• Geen haarverlies.
• Belangrijkste: maagdarm, daling bloedwaarden, vermoeidheid en polyneuropathie.

Velcade: Minder gekende bijwerkingen.
• Tumorlysis => voldoende vochtinname, evtl. allopurinol, ...
• Ortostatisme => hydratatie, evtl. hydrocortisone, …
• Herpes reactivatie => Zovirax !!.

Wat kost dit?
• Velcade 3.5 mg = 1219 €
• Dus: 6 cycli aan + 9.6 mg/cyclus =>
• = 20.061,3 €

•Revival immunotherapie?

Liu T-C et al. (2007) Clinical trial results with oncolytic virotherapy: a century of promise, a decade of progress Nat
Clin Pract Oncol 4: 101–117 doi:10.1038/ncponc0736
Tumor responses following incidental viral infection, vaccination or treatment with non-engineered virus strains
(A) Permission obtained from Elsevier © Bluming AZ and Ziegler JL (1971) Regression of Burkitt's lymphoma in association with measles infection. Lancet 2: 105–106. (B) Permission obtained from American
Medical Association © Hansen RM and Libnoch JA (1978) Remission of chronic lymphocytic leukemia after smallpox vaccination. Arch Intern Med 138: 1137–1138. (C) Reproduced from Kawa A and Arakawa S
(1987) The effect of attenuated vaccinia virus AS strain on multiple myeloma: a case report. Jpn J Exp Med 57: 79–81.

Dendritic Cell Vaccine Immunotherapy for
Aggressive Multiple Myeloma
Donor Derived
Monocytes
GM-CSF+IL-4
Intranodal
Vaccination of Donor
with myeloma loaded
DCs
Myeloma
Protein Immature DCs
CD40L
Mature
myeloma protein
loaded DCs
+Anti-myeloma
CD25+T-cells are
collected and purified
from the donor
Purified anti-myeloma
T-cells are infused into
the patient after
transplant to prevent
relapse


MM behandeling door de jaren.
1846 1960 1970 1980 1990 2000 2004 2009
Melphalan
Combination chemoVincristineDoxorubicin Dexamethasone
Thalidomide
BortezomibLenalidomide
MelphalanGlucocorticoids
(1969)
High-dose chemoStem cell transplantation
Bisphosphonates
Mr.McBean1948
HDAC InhHsP90 InhIGFR InhAplidin
New Imid
New PIImmuno

Dank U!


























![SBR Consistente Presentatie€¦ · SCP-30.5 TIJDELIJKE REGEL] De Consistente Presentatie MOET de waardes van concepten in een totaaltelling met een afwijkende balanceType visueel](https://img.pdfslide.tips/doc/110x75/60078a8f69c52a15702f8af6/sbr-consistente-presentatie-scp-305-tijdelijke-regel-de-consistente-presentatie.jpg)


