Embed Size (px)
Citation preview
Mary L. Bouxsein, PhDCenter for Advanced Orthopedic Studies
Department of Orthopedic Surgery, Harvard Medical School
MIT-Harvard Health Sciences and Technology Program
Boston, MA
14th Annual Osteoporosis Update Meeting
UCSF, July 2017
Denosumab Therapy for Osteoporosis
Disclosures
Consultant / Advisory board: Agnovos Healthcare, Acceleron Pharma, Radius Health
Research funding: Amgen – for an investigator initiated preclinical study
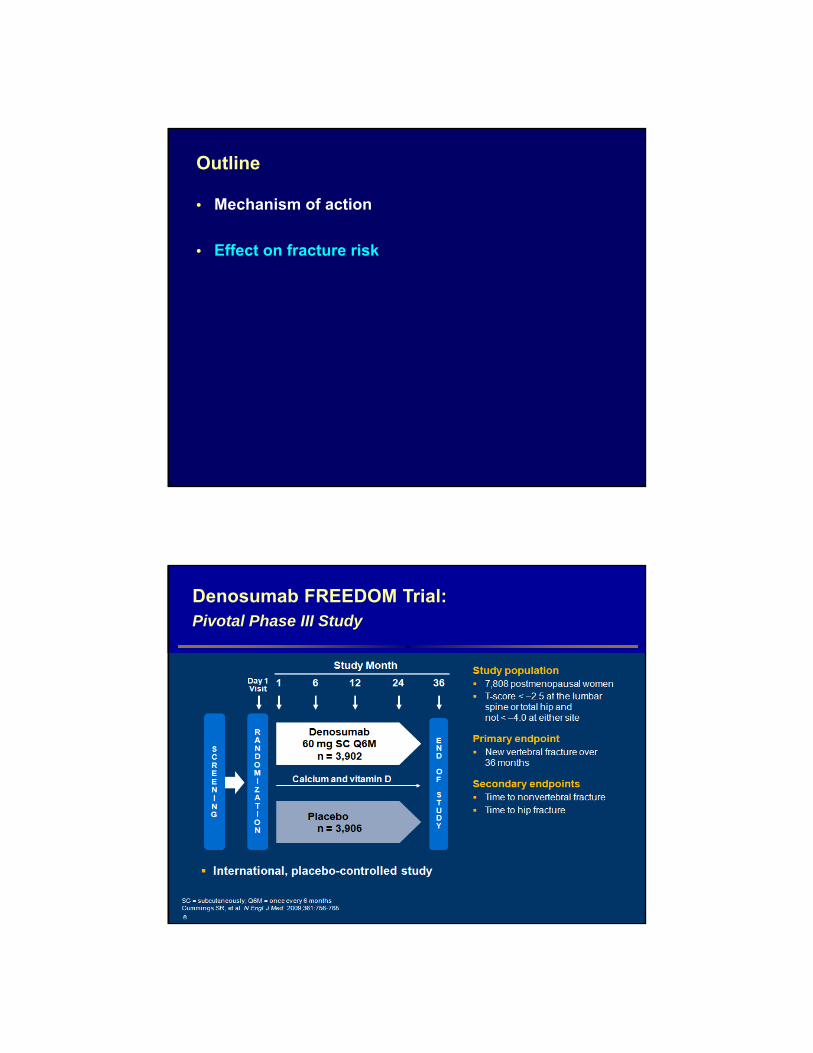
Outline
• Mechanism of action
• Effect on fracture risk
• Effect on bone turnover and BMD
• Long term treatment: BMD and fractures
• Safety & treatment cessastion
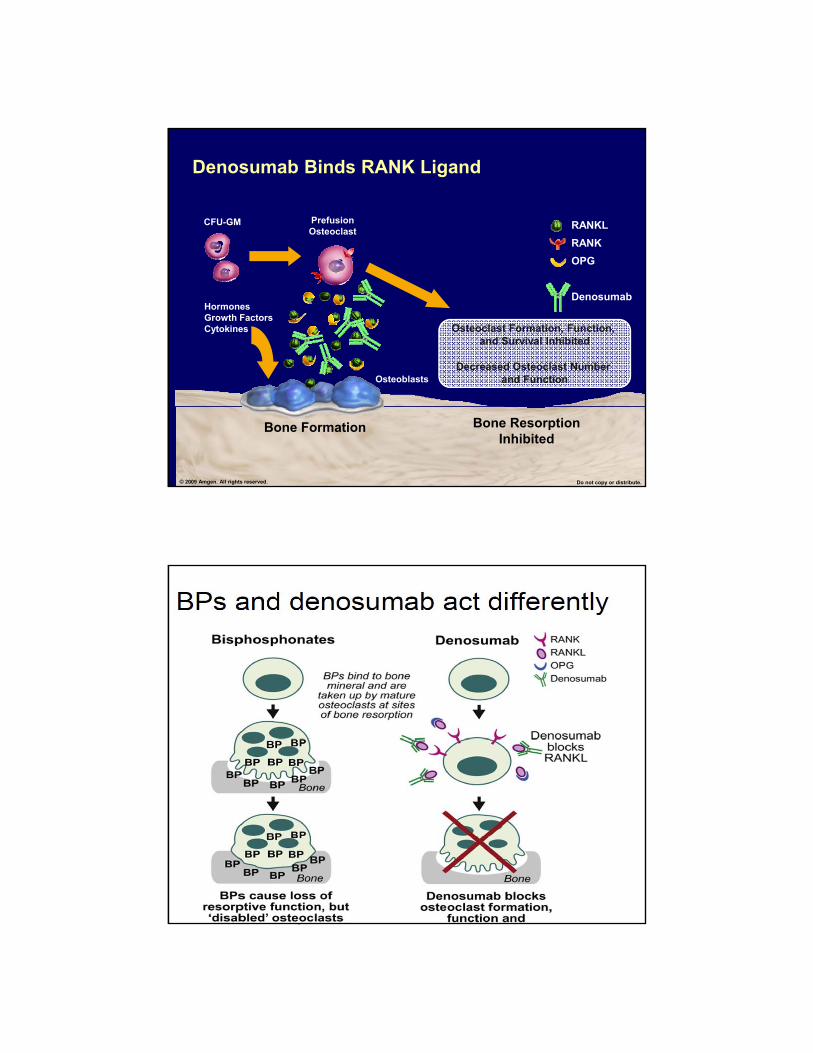
Excess RANK Ligand Increases Bone Resorption
Bone Formation
Bone Resorption
Activated Osteoclast
CFU-GM PrefusionOsteoclast
MultinucleatedOsteoclast
Osteoblasts
Decreased Estrogen Leads to Increased RANK Ligand
Adapted from: Boyle WJ, et al. Nature. 2003;423:337-342.© 2009 Amgen. All rights reserved. Do not copy or distribute.
RANKL
RANK
OPG
RANKL
RANK
OPG
Denosumab
Bone Formation Bone Resorption Inhibited
Osteoclast Formation, Function, and Survival Inhibited
Decreased Osteoclast Number and Function
CFU-GM PrefusionOsteoclast
Osteoblasts
HormonesGrowth FactorsCytokines
© 2009 Amgen. All rights reserved. Do not copy or distribute.
Denosumab Binds RANK Ligand
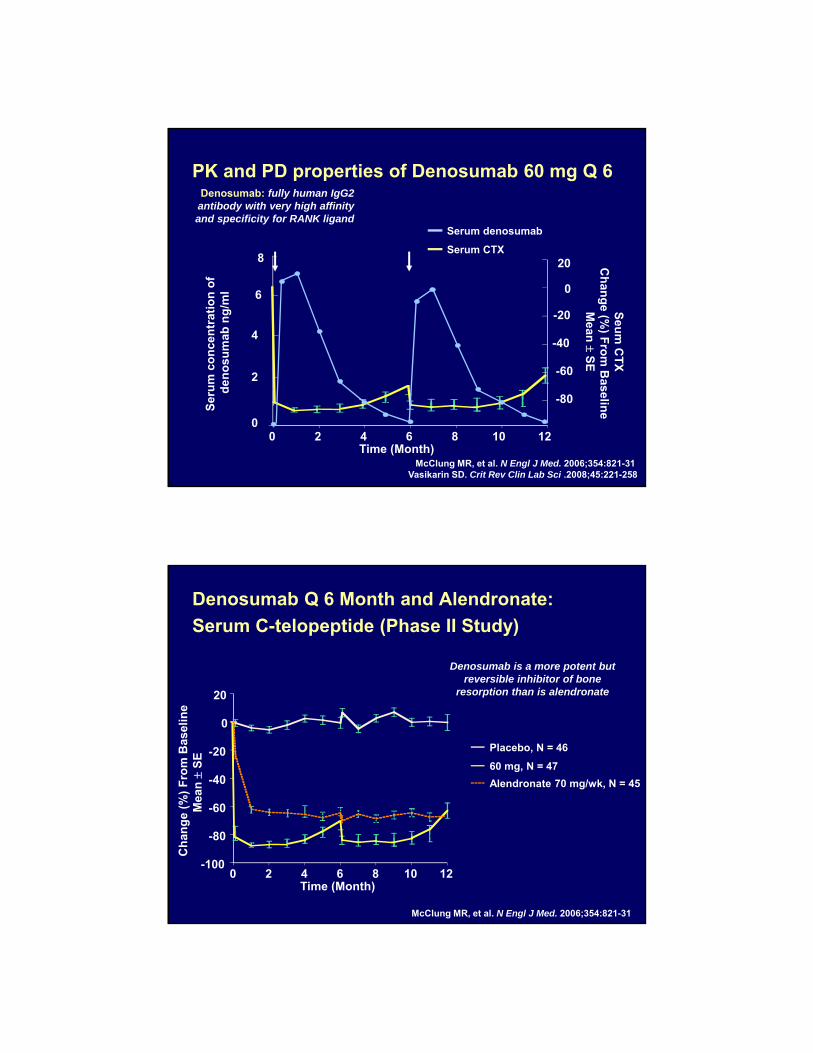
PK and PD properties of Denosumab 60 mg Q 6
Serum denosumab
Serum CTX
Ser
um
co
nce
ntr
atio
n o
f d
eno
sum
ab n
g/m
l
McClung MR, et al. N Engl J Med. 2006;354:821-31 Vasikarin SD. Crit Rev Clin Lab Sci .2008;45:221-258
0
2
4
6
8
0 2 4 6 8 10 12Time (Month)
-80
-60
-40
-20
0
20
Seu
m C
TX
C
han
ge (%
) Fro
m B
aseline
Mean
S
E
Denosumab: fully human IgG2 antibody with very high affinity and specificity for RANK ligand
Denosumab Q 6 Month and Alendronate:
Serum C-telopeptide (Phase II Study)
-100
-80
-60
-40
-20
0
20
0 2 4 6 8 10 12Time (Month)
Placebo, N = 46
60 mg, N = 47
Alendronate 70 mg/wk, N = 45
Ch
ang
e (%
) F
rom
Bas
elin
eM
ean
S
E
McClung MR, et al. N Engl J Med. 2006;354:821-31
Denosumab is a more potent but reversible inhibitor of bone
resorption than is alendronate
Outline
• Mechanism of action
• Effect on fracture risk
Denosumab FREEDOM Trial:Pivotal Phase III Study
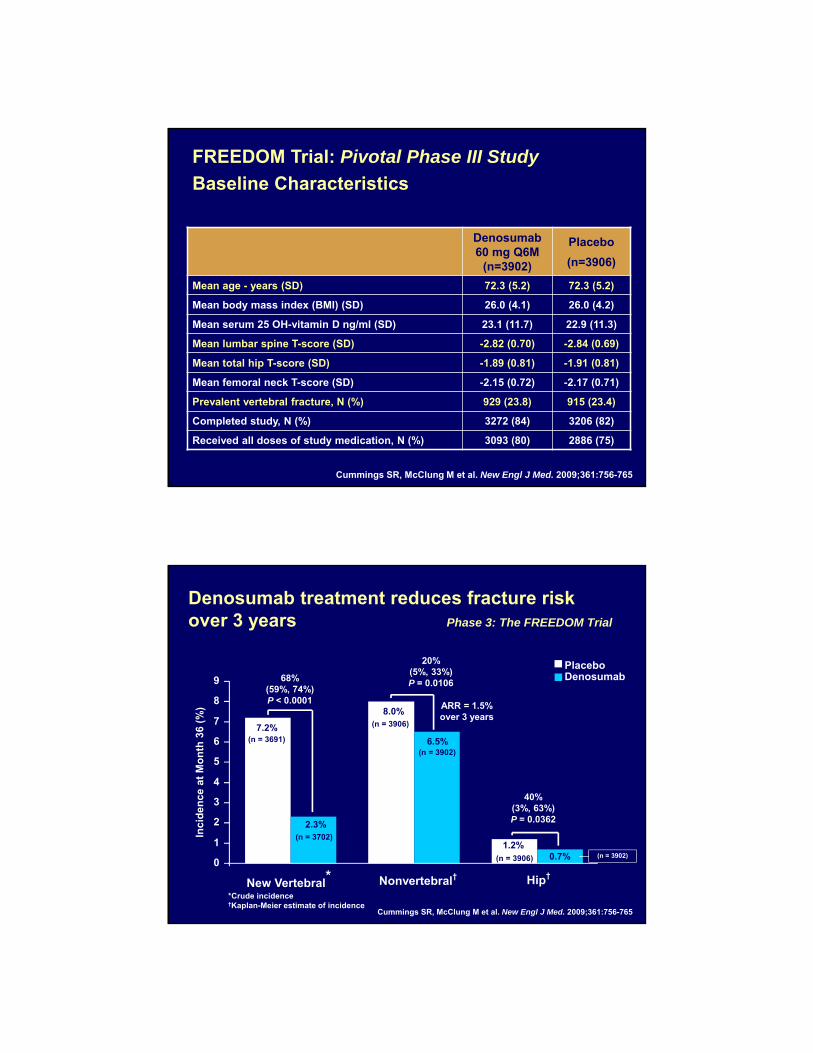
FREEDOM Trial: Pivotal Phase III Study
Baseline Characteristics
Cummings SR, McClung M et al. New Engl J Med. 2009;361:756-765
Denosumab 60 mg Q6M
(n=3902)
Placebo
(n=3906)
Mean age - years (SD) 72.3 (5.2) 72.3 (5.2)
Mean body mass index (BMI) (SD) 26.0 (4.1) 26.0 (4.2)
Mean serum 25 OH-vitamin D ng/ml (SD) 23.1 (11.7) 22.9 (11.3)
Mean lumbar spine T-score (SD) -2.82 (0.70) -2.84 (0.69)
Mean total hip T-score (SD) -1.89 (0.81) -1.91 (0.81)
Mean femoral neck T-score (SD) -2.15 (0.72) -2.17 (0.71)
Prevalent vertebral fracture, N (%) 929 (23.8) 915 (23.4)
Completed study, N (%) 3272 (84) 3206 (82)
Received all doses of study medication, N (%) 3093 (80) 2886 (75)
Denosumab treatment reduces fracture risk over 3 years Phase 3: The FREEDOM Trial
40%(3%, 63%)P = 0.0362
20%(5%, 33%)P = 0.010668%
(59%, 74%) P < 0.0001
7.2%
8.0%
1.2%
6.5%
0.7%
2.3%
0
1
2
3
4
5
6
7
8
9
New Vertebral* Nonvertebral† Hip†
Inci
den
ce a
t M
on
th 3
6 (%
)
*Crude incidence†Kaplan-Meier estimate of incidence
(n = 3691)
(n = 3702)
(n = 3906)
(n = 3902)
(n = 3906) (n = 3902)
PlaceboDenosumab
Cummings SR, McClung M et al. New Engl J Med. 2009;361:756-765
ARR = 1.5% over 3 years
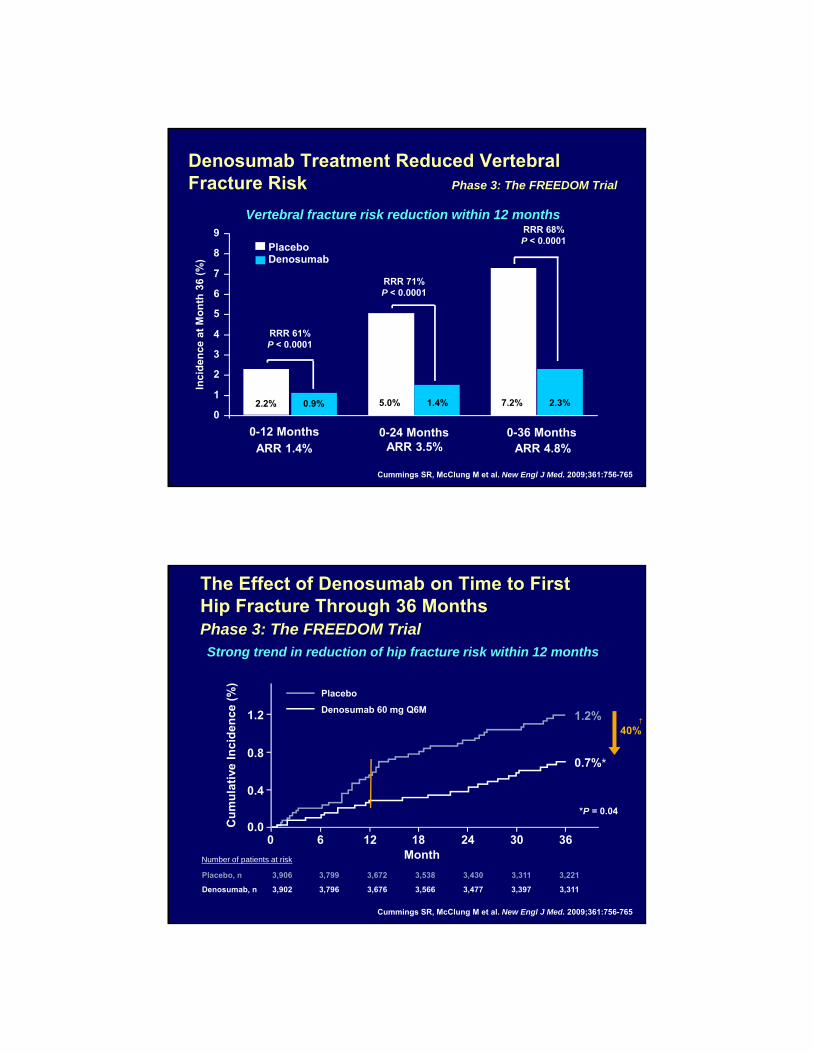
Denosumab Treatment Reduced Vertebral Fracture Risk Phase 3: The FREEDOM Trial
RRR 61%P < 0.0001
2.2% 0.9%0
1
2
3
4
5
6
7
8
9
0-12 Months
Inci
den
ce a
t M
on
th 3
6 (%
)
PlaceboDenosumab
0-24 Months 0-36 Months
5.0% 1.4% 7.2% 2.3%
RRR 71%P < 0.0001
RRR 68%P < 0.0001
ARR 1.4% ARR 3.5% ARR 4.8%
Cummings SR, McClung M et al. New Engl J Med. 2009;361:756-765
Vertebral fracture risk reduction within 12 months
The Effect of Denosumab on Time to First Hip Fracture Through 36 MonthsPhase 3: The FREEDOM Trial
Placebo, n 3,906 3,799 3,672 3,538 3,430 3,311 3,221
Denosumab, n 3,902 3,796 3,676 3,566 3,477 3,397 3,311
Number of patients at risk
Cu
mu
lati
ve I
nci
den
ce (
%)
Month0 6 12 24
0.018 30 36
0.4
0.8
1.2
0.7%*
1.2%
Placebo
Denosumab 60 mg Q6M
40%†
*P = 0.04
Cummings SR, McClung M et al. New Engl J Med. 2009;361:756-765
Strong trend in reduction of hip fracture risk within 12 months
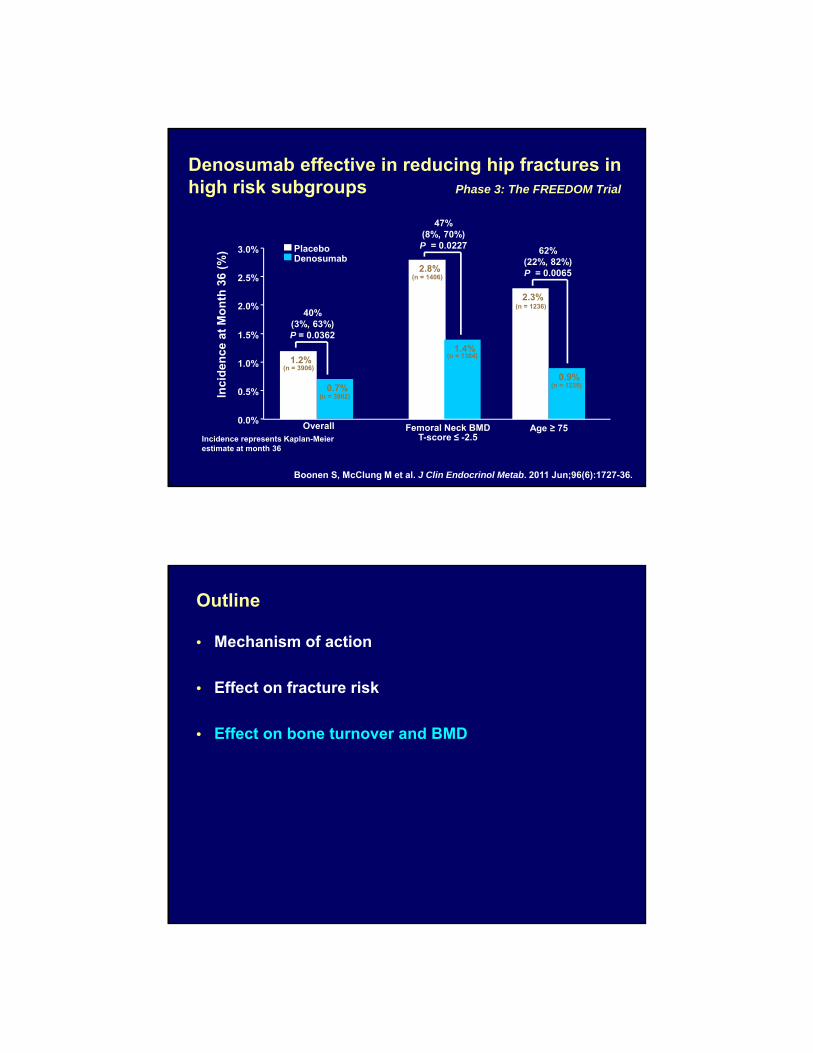
Denosumab effective in reducing hip fractures in high risk subgroups Phase 3: The FREEDOM Trial
Incidence represents Kaplan-Meier estimate at month 36
(n = 1406)2.8%
(n = 1384)
47%(8%, 70%)P = 0.0227
1.4%
(n = 1236)2.3%
62%(22%, 82%)P = 0.0065
(n = 1235)0.9%
40%(3%, 63%)P = 0.0362
(n = 3902)0.7%
(n = 3906)1.2%
Inci
den
ce a
t M
on
th 3
6 (%
)
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0% PlaceboDenosumab
Femoral Neck BMDT-score ≤ -2.5
Age ≥ 75Overall
Boonen S, McClung M et al. J Clin Endocrinol Metab. 2011 Jun;96(6):1727-36.
Outline
• Mechanism of action
• Effect on fracture risk
• Effect on bone turnover and BMD
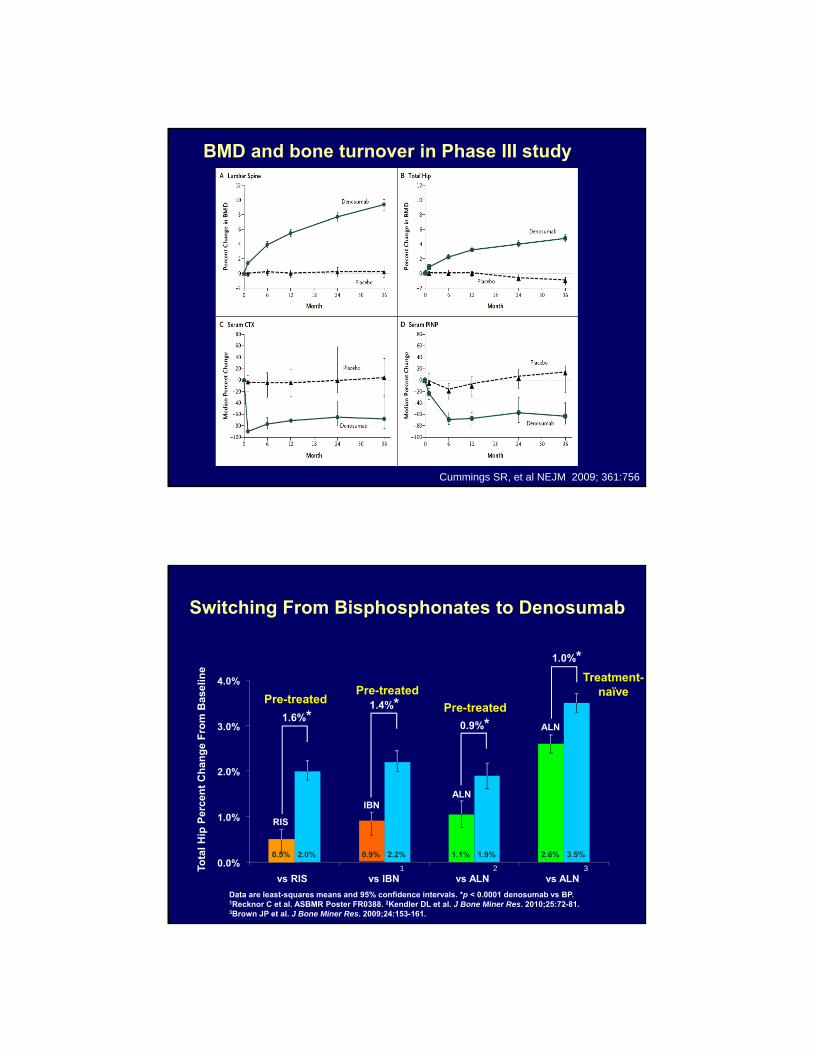
BMD and bone turnover in Phase III study
Cummings SR, et al NEJM 2009; 361:756
Treatment-naïve
Switching From Bisphosphonates to Denosumab
Data are least-squares means and 95% confidence intervals. *p < 0.0001 denosumab vs BP. 1Recknor C et al. ASBMR Poster FR0388. 2Kendler DL et al. J Bone Miner Res. 2010;25:72-81. 3Brown JP et al. J Bone Miner Res. 2009;24:153-161.
IBNALN
ALN
RIS
1.6%*1.4%*
0.9%*
1.0%*
1 2 3
Pre-treated
Pre-treatedPre-treated
Tota
l H
ip P
erce
nt
Ch
ang
e F
rom
Bas
elin
e
0.5% 0.9% 1.1% 2.6%2.0% 2.2% 1.9% 3.5%0.0%
1.0%
2.0%
3.0%
4.0%
vs RIS vs IBN vs ALN vs ALN
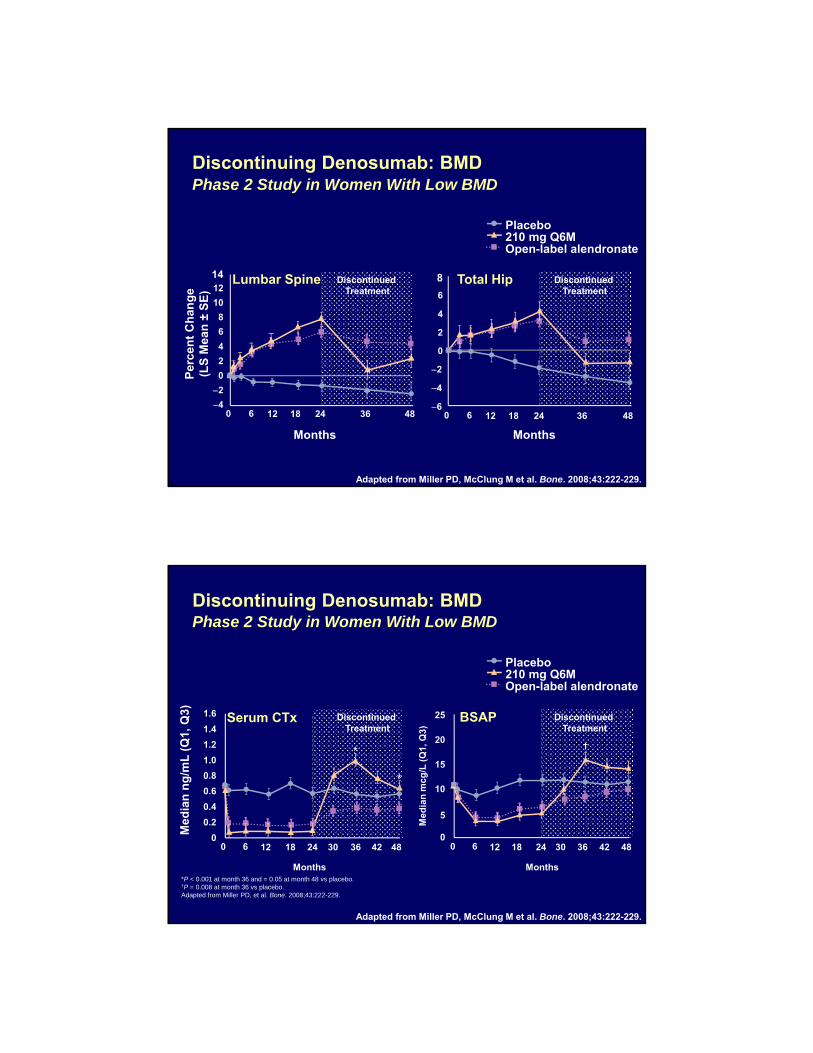
Discontinuing Denosumab: BMDPhase 2 Study in Women With Low BMD
Adapted from Miller PD, McClung M et al. Bone. 2008;43:222-229.
Discontinued Treatment
Discontinued Treatment
Lumbar Spine Total Hip
Per
cen
t C
han
ge
(LS
Mea
n ±
SE
)
Months
6
4
2
0
2
4
6
8
Months
0 6 12 18 24 36 484
2
0
2
4
6
8
10
12
14
0 6 12 18 24 36 48
Placebo210 mg Q6MOpen-label alendronate
*P < 0.001 at month 36 and = 0.05 at month 48 vs placebo.†P = 0.008 at month 36 vs placebo.Adapted from Miller PD, et al. Bone. 2008;43:222-229.
Serum CTx BSAP
0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
0 6 12 18 24 30 36 42 48
Med
ian
ng
/mL
(Q
1, Q
3)
0
5
10
15
20
25
0 6 12 18 24 30 36 42 48
Months Months
Med
ian
mcg
/L (
Q1,
Q3)
*
*
†
Adapted from Miller PD, McClung M et al. Bone. 2008;43:222-229.
Discontinuing Denosumab: BMDPhase 2 Study in Women With Low BMD
Discontinued Treatment
Discontinued Treatment
Placebo210 mg Q6MOpen-label alendronate

Outline
• Mechanism of action
• Effect on fracture risk
• Effect on bone turnover and BMD
• Long term treatment: BMD and fractures
Key Inclusion Criteria for the Extension:• Completed the FREEDOM study (completed the 3-year visit, did not
discontinue investigational product, and did not miss > 1 dose)• Not receiving any other osteoporosis medications
FREEDOM Extension
1 2 3Year 0 5 6 74 8 9 10
1 2 30 6 74Year
RANDOMIZATION
Denosumab 60 mgSC Q6M
(N = 3902)
PlaceboSC Q6M
(N = 3906)
Long-termDenosumabTreatment
Cross-overDenosumabTreatment
Denosumab 60 mgSC Q6M
(N = 2343)
Denosumab 60 mgSC Q6M
(N = 2207)
Calcium and Vitamin D
FREEDOM Extension Study DesignInternational, multicenter, open-label, single-arm study
5
Cross-over DMAb Treatment Extension Subjects
N = 2207
Long-term DMAb Treatment Extension Subjects
N = 2343
FREEDOM Baseline
Extension Baseline
FREEDOM Baseline
ExtensionBaseline
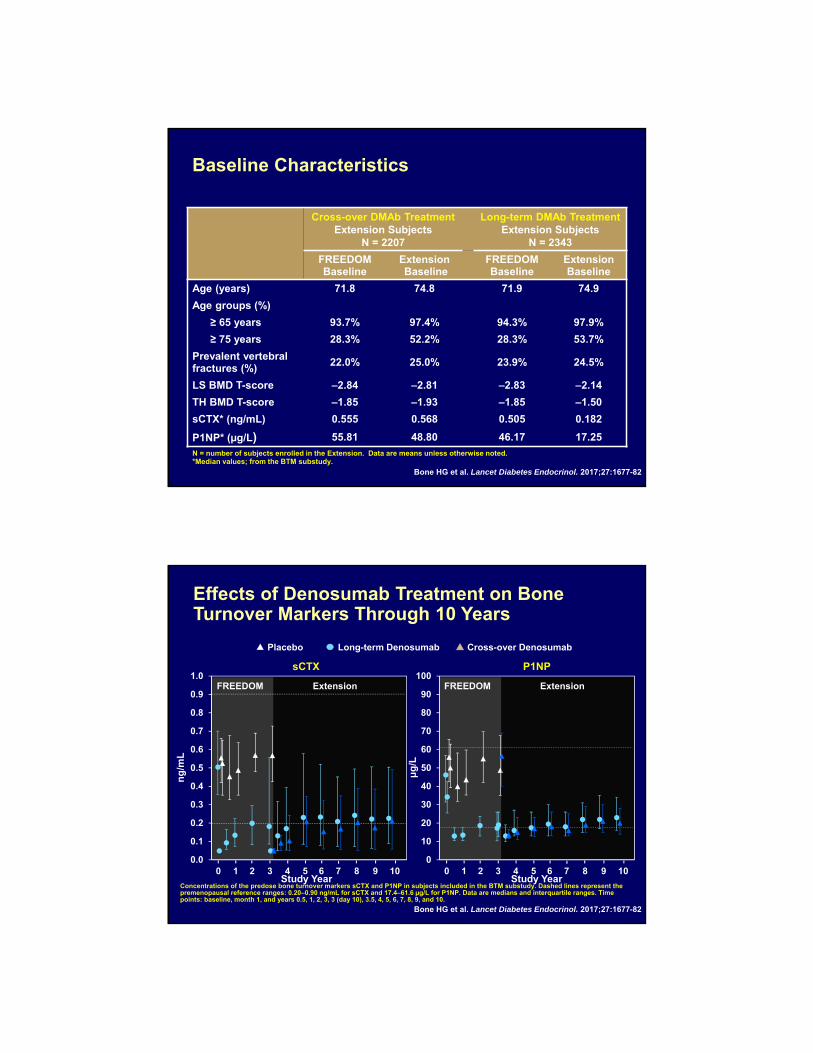
Age (years) 71.8 74.8 71.9 74.9
Age groups (%)
≥ 65 years 93.7% 97.4% 94.3% 97.9%
≥ 75 years 28.3% 52.2% 28.3% 53.7%
Prevalent vertebral fractures (%)
22.0% 25.0% 23.9% 24.5%
LS BMD T-score –2.84 –2.81 –2.83 –2.14
TH BMD T-score –1.85 –1.93 –1.85 –1.50
sCTX* (ng/mL) 0.555 0.568 0.505 0.182
P1NP* (µg/L) 55.81 48.80 46.17 17.25
N = number of subjects enrolled in the Extension. Data are means unless otherwise noted.*Median values; from the BTM substudy.
Baseline Characteristics
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
ExtensionFREEDOM
0
10
20
30
40
50
60
70
80
90
100ExtensionFREEDOM
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
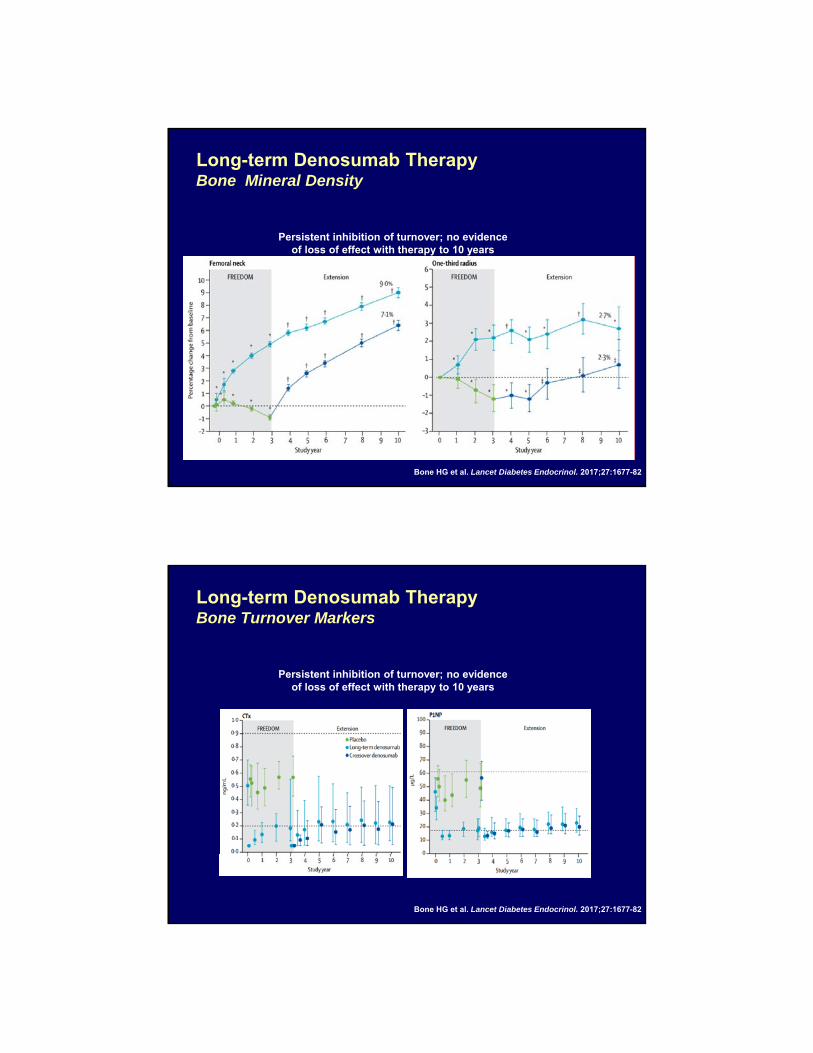
Effects of Denosumab Treatment on Bone Turnover Markers Through 10 Years
Placebo Cross-over DenosumabLong-term Denosumab
sCTX P1NP
Concentrations of the predose bone turnover markers sCTX and P1NP in subjects included in the BTM substudy. Dashed lines represent the premenopausal reference ranges: 0.20–0.90 ng/mL for sCTX and 17.4–61.6 µg/L for P1NP. Data are medians and interquartile ranges. Time points: baseline, month 1, and years 0.5, 1, 2, 3, 3 (day 10), 3.5, 4, 5, 6, 7, 8, 9, and 10.
ng
/mL
0 1 2 3 4 5 6 7 8 9 10Study Year Study Year
0 1 2 3 4 5 6 7 8 9 10
μg
/L
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
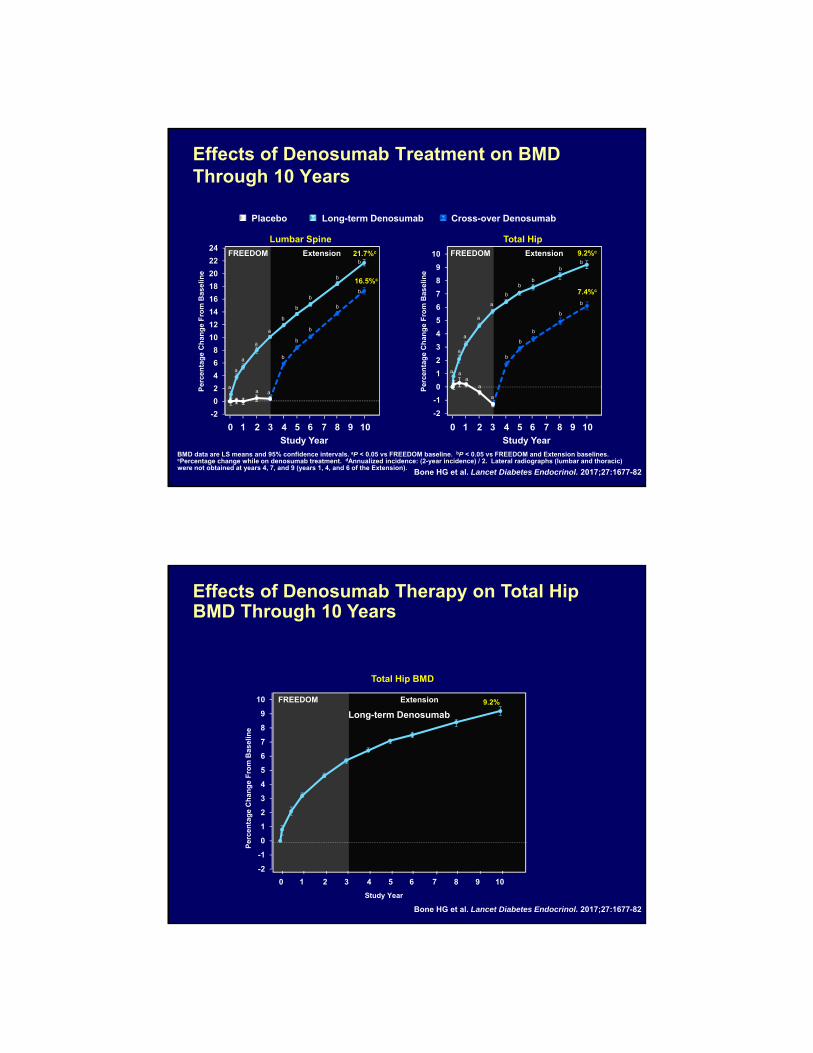
BMD data are LS means and 95% confidence intervals. aP < 0.05 vs FREEDOM baseline. bP < 0.05 vs FREEDOM and Extension baselines. cPercentage change while on denosumab treatment. dAnnualized incidence: (2-year incidence) / 2. Lateral radiographs (lumbar and thoracic) were not obtained at years 4, 7, and 9 (years 1, 4, and 6 of the Extension).
Effects of Denosumab Treatment on BMD Through 10 Years
Placebo Cross-over DenosumabLong-term Denosumab
FREEDOM Extension
-2
-1
0
1
2
3
4
5
6
7
8
9
10
b
bb
b
b
b
b
b
a
a
aa
a
a
a
a
9.2%c
7.4%c
b
b
Per
cen
tag
e C
han
ge
Fro
m B
asel
ine
Study Year
1 2 3 4 50 6 7 8 9 10
Total Hip
a
FREEDOM Extension
-2
0
2
4
6
8
10
12
14
16
18
20
22
24
b
21.7%c
b
b
a
a
a
a
b
b
b
16.5%c
Lumbar Spine
Per
cen
tag
e C
han
ge
Fro
m B
asel
ine
b
b
aa
b
b
Study Year
1 2 3 4 50 6 7 8 9 10
a
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
Effects of Denosumab Therapy on Total Hip BMD Through 10 Years
FREEDOM Extension
-2
-1
0
1
2
3
4
5
6
7
8
9
10 9.2%
Per
cen
tag
e C
han
ge
Fro
m B
asel
ine
Study Year
1 2 3 4 50 6 7 8 9 10
Total Hip BMD
Long-term Denosumab
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
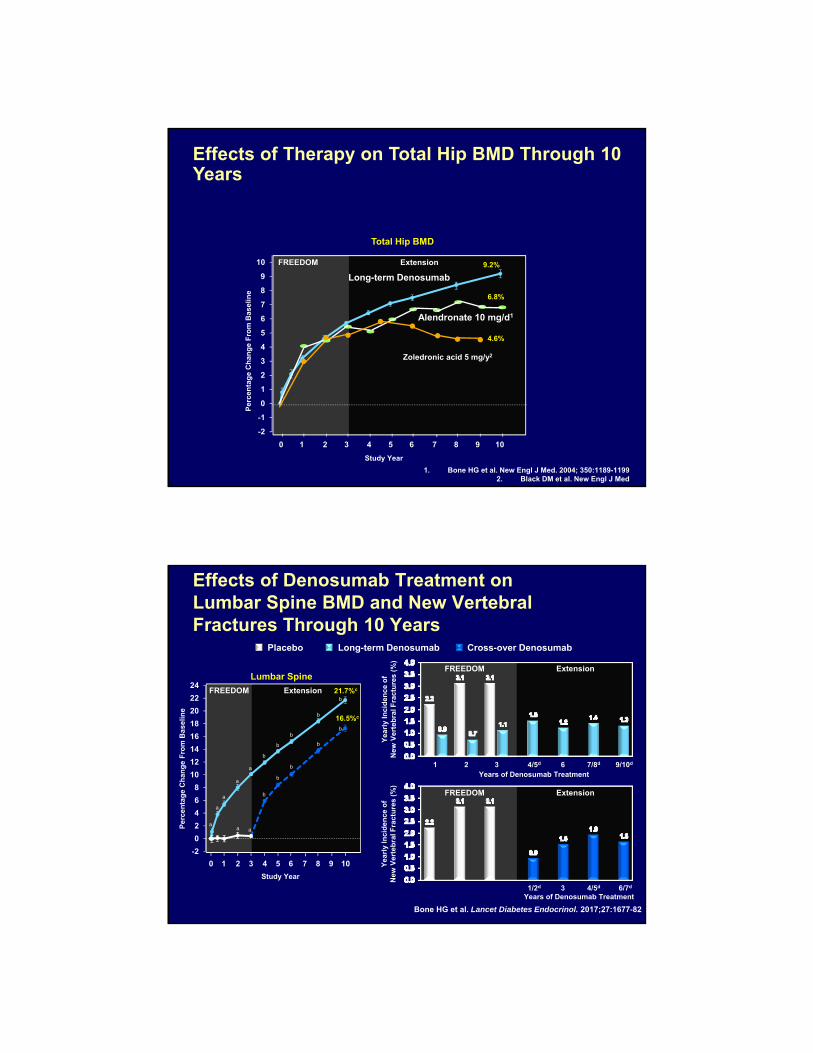
Effects of Therapy on Total Hip BMD Through 10 Years
Long-term DenosumabFREEDOM Extension
-2
-1
0
1
2
3
4
5
6
7
8
9
10 9.2%
6.8%
Per
cen
tag
e C
han
ge
Fro
m B
asel
ine
Study Year
1 2 3 4 50 6 7 8 9 10
Total Hip BMD
4.6%
1. Bone HG et al. New Engl J Med. 2004; 350:1189-11992. Black DM et al. New Engl J Med
Zoledronic acid 5 mg/y2
Alendronate 10 mg/d1
Long-term Denosumab
FREEDOM Extension
-2
0
2
4
6
8
10
12
14
16
18
20
22
24
b
21.7%c
b
b
a
a
a
a
b
b
b
16.5%c
Lumbar Spine
Per
cen
tag
e C
han
ge
Fro
m B
asel
ine
b
b
aa
Effects of Denosumab Treatment on Lumbar Spine BMD and New Vertebral Fractures Through 10 Years
b
b
FREEDOM Extension
FREEDOM Extension
Years of Denosumab Treatment1/2d 4/5d3
1 2 3 4/5d 7/8d6 9/10d
6/7d
Years of Denosumab Treatment
Yea
rly
Inci
den
ce o
fN
ew V
erte
bra
l Fra
ctu
res
(%)
Yea
rly
Inci
den
ce o
fN
ew V
erte
bra
l Fra
ctu
res
(%)
Study Year
1 2 3 4 50 6 7 8 9 10
Placebo Cross-over DenosumabLong-term Denosumab
a
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82

FREEDOM Extension
-2
-1
0
1
2
3
4
5
6
7
8
9
10
Effects of Denosumab Treatment on Total Hip BMD and Nonvertebral Fractures Through 10 Years
b
bb
b
b
b
b
b
a
a
aa
a
a
a
a
9.2%c
7.4%c
b
b
Per
cen
tag
e C
han
ge
Fro
m B
asel
ine
Study Year
1 2 3 4 50 6 7 8 9 10
Total HipFREEDOM Extension
FREEDOM Extension
Yea
rly
Inci
den
ce o
fN
on
vert
ebra
l Fra
ctu
res
(%)
Yea
rly
Inci
den
ce o
fN
on
vert
ebra
l Fra
ctu
res
(%)
1 532 4
1 2 3 4 865 7 9 10
6 7
Years of Denosumab Treatment
Years of Denosumab Treatment
Placebo Cross-over DenosumabLong-term Denosumab
a
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
• A simulation method was used to estimate expected fracture rates in a hypothetical cohort of long-term placebo controls (“virtual twins”) since all subjects in the Extension study received denosumab treatment.1
– Models were developed using actual FREEDOM data on BMD, fracture history, BMI, age, and smoking status for subjects who received placebo during the 3 years of FREEDOM and enrolled in the Extension.
– Models then predicted fracture outcomes for the denosumab-treated women who entered the Extension had they received placebo for 3 years in FREEDOM and 7 years in the Extension (“virtual twins”).
Virtual Twin Placebo
1. Bone HG et al., J Clin Endocrinol Metab 2013;98:4483-4492.
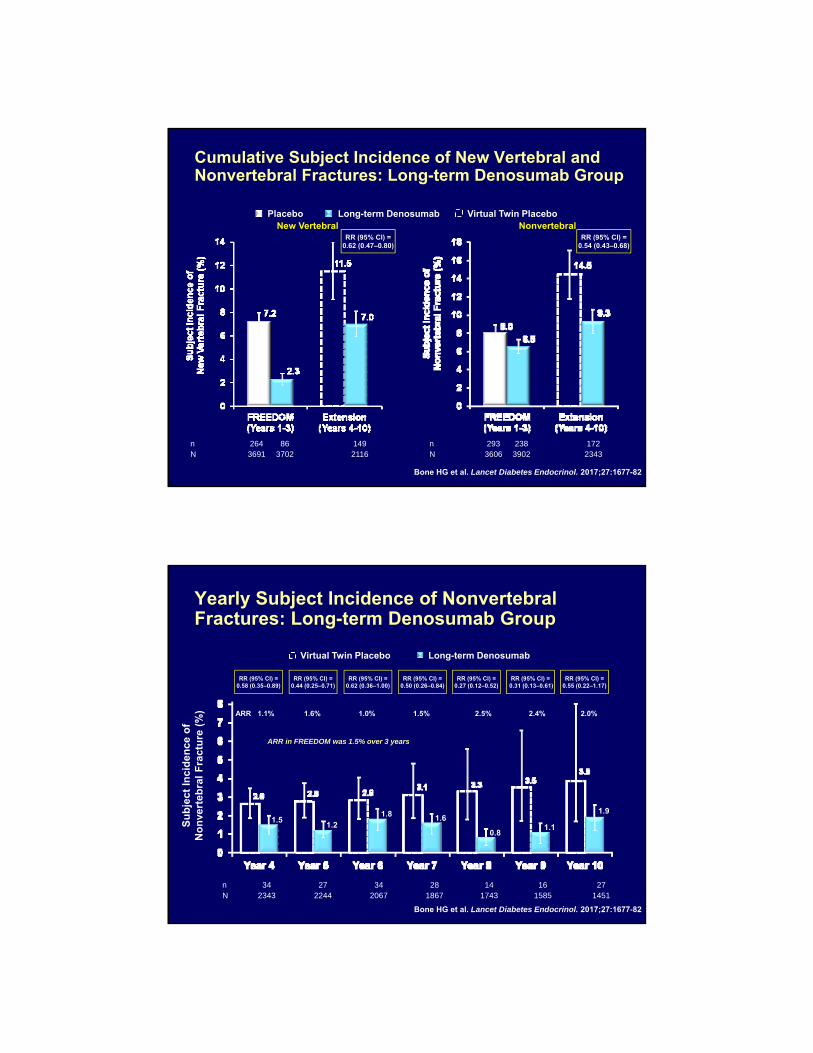
Cumulative Subject Incidence of New Vertebral and Nonvertebral Fractures: Long-term Denosumab Group
Placebo Virtual Twin PlaceboLong-term Denosumab
n 264 86 149N 3691 3702 2116
RR (95% CI) =0.62 (0.47–0.80)
New VertebralRR (95% CI) =
0.54 (0.43–0.68)
Nonvertebral
n 293 238 172N 3606 3902 2343
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
Yearly Subject Incidence of Nonvertebral Fractures: Long-term Denosumab Group
Long-term DenosumabVirtual Twin Placebo
RR (95% CI) =0.58 (0.35–0.89)
RR (95% CI) =0.44 (0.25–0.71)
RR (95% CI) =0.62 (0.36–1.00)
RR (95% CI) =0.50 (0.26–0.84)
RR (95% CI) =0.27 (0.12–0.52)
Su
bje
ct I
nci
den
ce o
fN
on
vert
ebra
l F
ract
ure
(%
)
n 34 27 34 28 14 16 27N 2343 2244 2067 1867 1743 1585 1451
RR (95% CI) =0.31 (0.13–0.61)
RR (95% CI) =0.55 (0.22–1.17)
1.51.2
1.8 1.6
0.81.1
1.9
ARR 1.1% 1.6% 1.0% 1.5% 2.5% 2.4% 2.0%
ARR in FREEDOM was 1.5% over 3 years
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
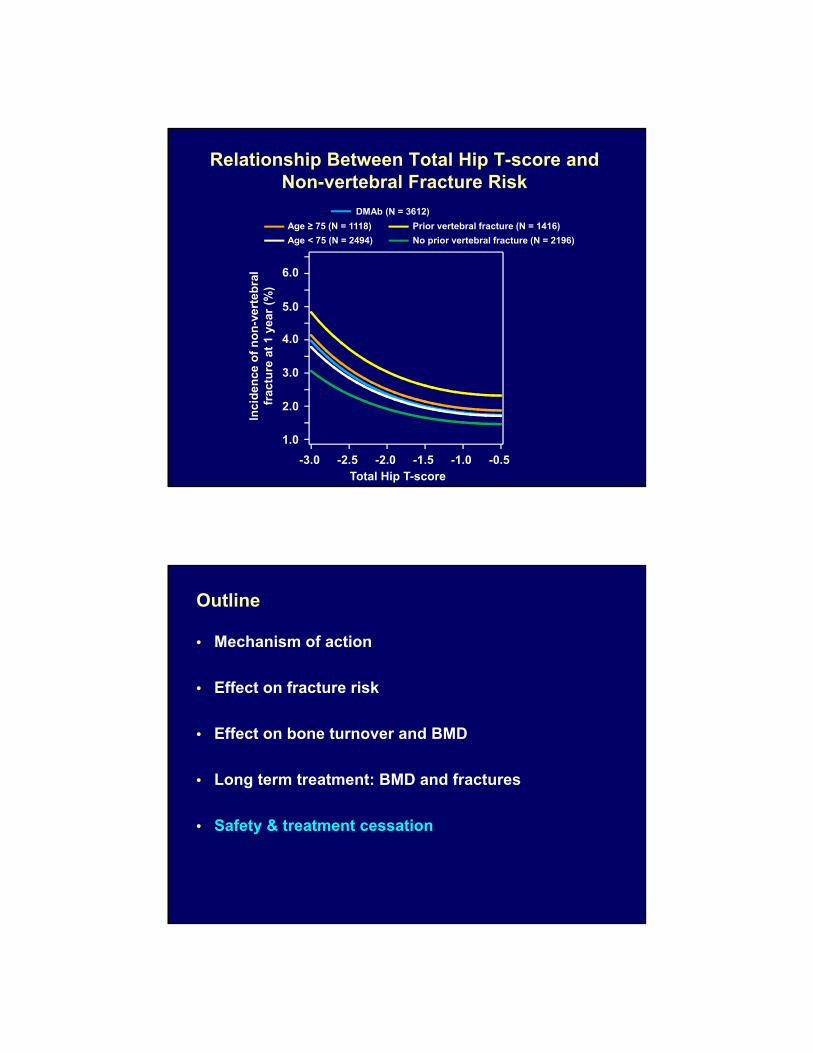
Relationship Between Total Hip T-score and Non-vertebral Fracture Risk
Inci
den
ce o
f n
on
-ver
teb
ral
frac
ture
at
1 ye
ar (
%)
-3.0 -2.5 -2.0 -1.5 -1.0 -0.5
1.0
2.0
3.0
4.0
5.0
6.0
DMAb (N = 3612)
Age ≥ 75 (N = 1118)
Age < 75 (N = 2494)
Prior vertebral fracture (N = 1416)
No prior vertebral fracture (N = 2196)
Total Hip T-score
Outline
• Mechanism of action
• Effect on fracture risk
• Effect on bone turnover and BMD
• Long term treatment: BMD and fractures
• Safety & treatment cessation
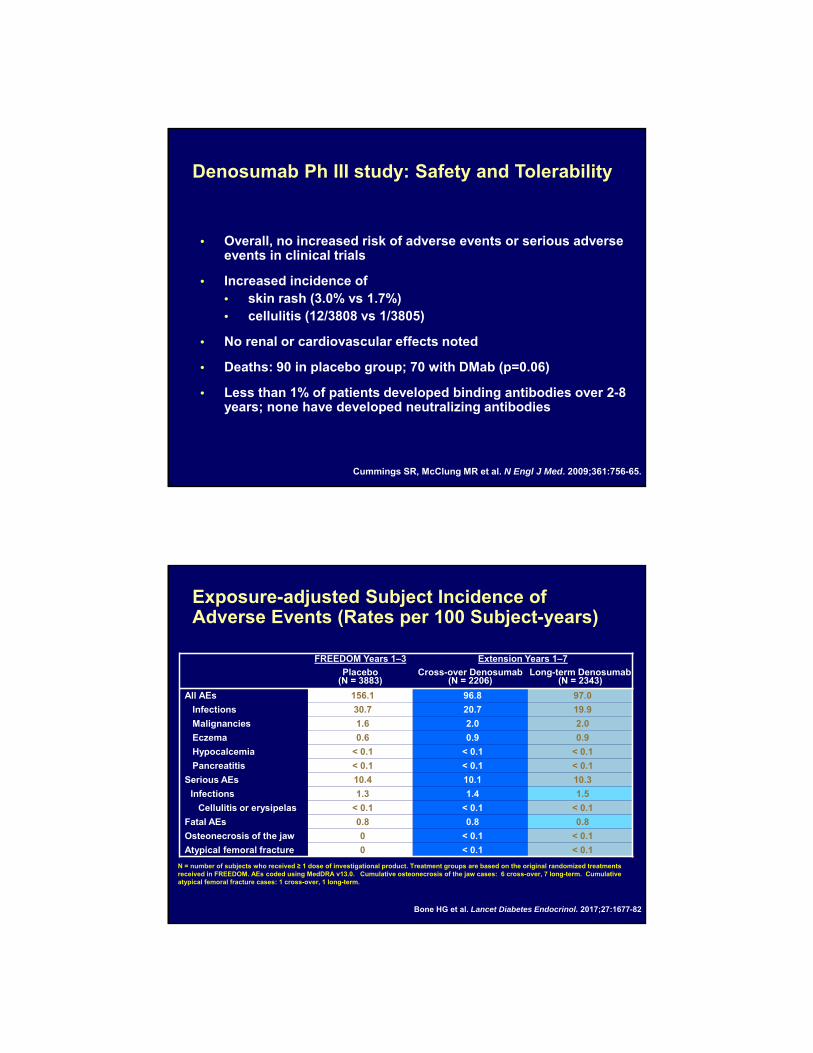
• Overall, no increased risk of adverse events or serious adverse events in clinical trials
• Increased incidence of • skin rash (3.0% vs 1.7%)• cellulitis (12/3808 vs 1/3805)
• No renal or cardiovascular effects noted
• Deaths: 90 in placebo group; 70 with DMab (p=0.06)
• Less than 1% of patients developed binding antibodies over 2-8 years; none have developed neutralizing antibodies
Denosumab Ph III study: Safety and Tolerability
Cummings SR, McClung MR et al. N Engl J Med. 2009;361:756-65.
FREEDOM Years 1–3 Extension Years 1–7
Placebo (N = 3883)
Cross-over Denosumab (N = 2206)
Long-term Denosumab(N = 2343)
All AEs 156.1 96.8 97.0
Infections 30.7 20.7 19.9
Malignancies 1.6 2.0 2.0
Eczema 0.6 0.9 0.9
Hypocalcemia < 0.1 < 0.1 < 0.1
Pancreatitis < 0.1 < 0.1 < 0.1
Serious AEs 10.4 10.1 10.3
Infections 1.3 1.4 1.5
Cellulitis or erysipelas < 0.1 < 0.1 < 0.1
Fatal AEs 0.8 0.8 0.8
Osteonecrosis of the jaw 0 < 0.1 < 0.1
Atypical femoral fracture 0 < 0.1 < 0.1
N = number of subjects who received ≥ 1 dose of investigational product. Treatment groups are based on the original randomized treatments received in FREEDOM. AEs coded using MedDRA v13.0. Cumulative osteonecrosis of the jaw cases: 6 cross-over, 7 long-term. Cumulative atypical femoral fracture cases: 1 cross-over, 1 long-term.
Exposure-adjusted Subject Incidence of Adverse Events (Rates per 100 Subject-years)
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
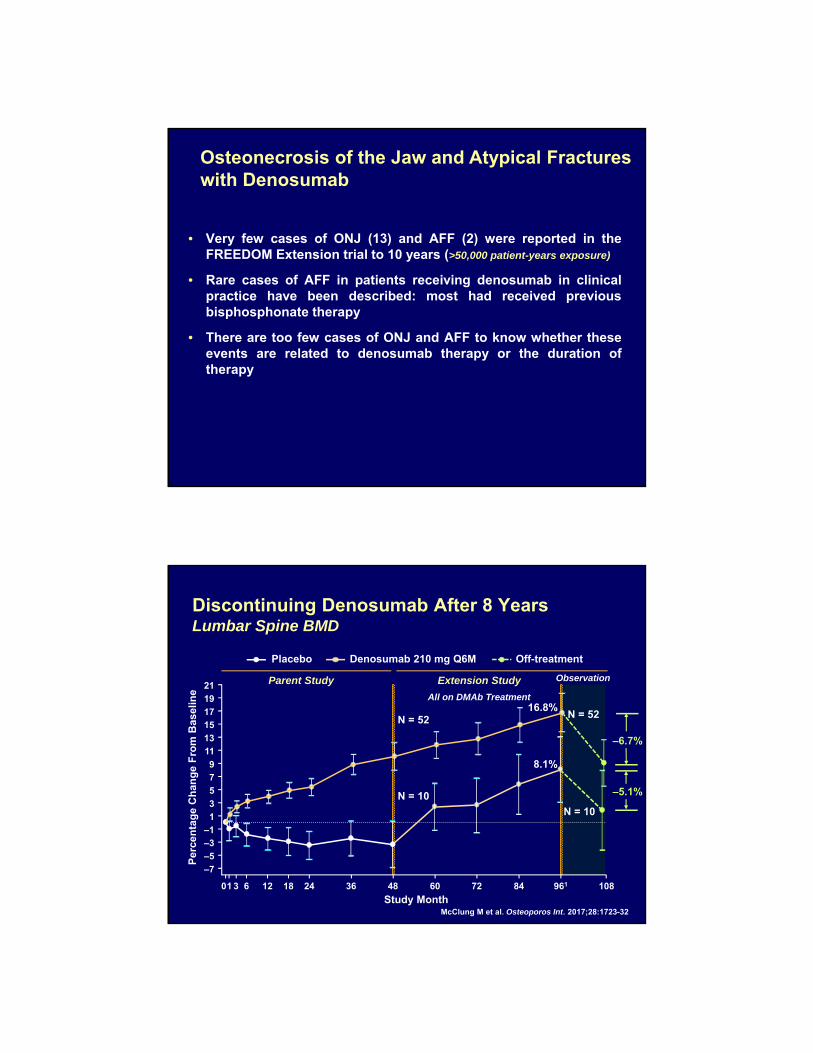
• Very few cases of ONJ (13) and AFF (2) were reported in theFREEDOM Extension trial to 10 years (>50,000 patient-years exposure)
• Rare cases of AFF in patients receiving denosumab in clinicalpractice have been described: most had received previousbisphosphonate therapy
• There are too few cases of ONJ and AFF to know whether theseevents are related to denosumab therapy or the duration oftherapy
Osteonecrosis of the Jaw and Atypical Fractures with Denosumab
–6.7%
–5.1%
N = 10
N = 52
Discontinuing Denosumab After 8 YearsLumbar Spine BMD
Extension StudyParent Study
All on DMAb Treatment
–7
–5
–3
–1
1
3
5
79
11
13
1517
19
21
01 3 6 12 18 24 36 48 60 72 84 961 108
16.8%
8.1%
N = 52
N = 10
McClung M et al. Osteoporos Int. 2017;28:1723-32
Observation
Study Month
Per
cen
tag
e C
han
ge
Fro
m B
asel
ine
Placebo Denosumab 210 mg Q6M Off-treatment

Vertebral Fractures After Discontinuing Denosumab Therapy
• At least 24 patients have been reported who experienced vertebral fractures within 3-18 months after discontinuing denosumab therapy. (1)
• Many or most have had multiple and/or severe fractures
• Raised concern about “rebound” risk of fracture
• Similar to rapid loss of fracture protection when estrogen therapy is discontinued (2,3)
1. Anastasilakis AD et al. J Bone Miner Res. 2017 Feb 272. Heiss G et al. JAMA 299:1036–45
3. McClung MR. Osteoporos Int. 2016;27:1677-82
Case Reports of Clinical Vertebral Fractures Following Denosumab Discontinuation
• Anecdotal Case of Multiple Fractures following discontinuation of denosumab• 51 y.o. PMO 5 yrs. , T score LS -2.5, no vertebral frx
by xray
• 2/2012 Rx Denosumab 60mg q 6 for 3 years., last Rx 8/2014
• 2/2015 T score LS -1.8
• 4/2015 Severe back pain bending to pull drawer of refigerator, 8 months after last dmab Rx
• MRI found 3 incident Vertebral Frxns T12, L1, and L3
Anastasilakis AD, et al OI, (2016): 1929-1930
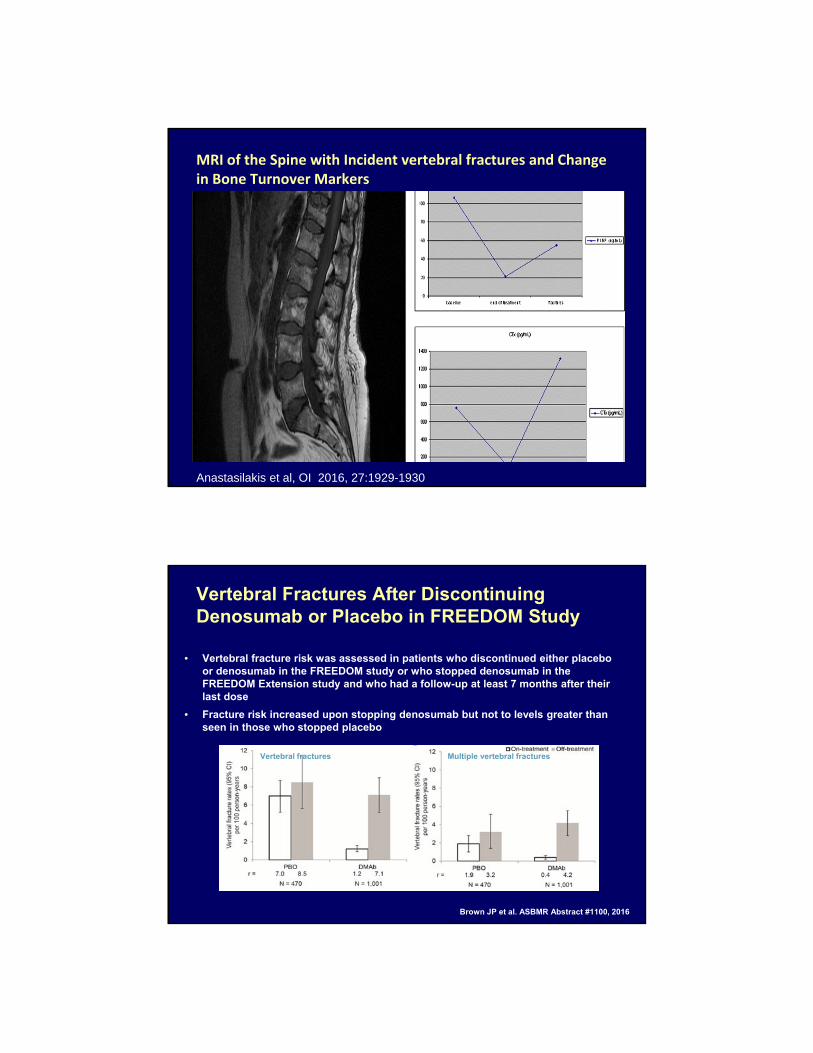
MRI of the Spine with Incident vertebral fractures and Change in Bone Turnover Markers
Anastasilakis et al, OI 2016, 27:1929-1930
Vertebral Fractures After Discontinuing Denosumab or Placebo in FREEDOM Study
• Vertebral fracture risk was assessed in patients who discontinued either placebo or denosumab in the FREEDOM study or who stopped denosumab in the FREEDOM Extension study and who had a follow-up at least 7 months after their last dose
• Fracture risk increased upon stopping denosumab but not to levels greater than seen in those who stopped placebo
Vertebral fractures Multiple vertebral fractures
Brown JP et al. ASBMR Abstract #1100, 2016
• Bone loss and rise in serum CTX is attenuated in patients who stop denosumab but who took bisphosphonates before denosumab therapy.
• Bone loss after stopping denosumab is attenuated in patients who then receive anti-remodeling agents
Discontinuing DenosumabOther Information
Ferrari S et al. ECTS 2016
McClung M et al. Osteoporos Int. 2017;28:1723-32
Recommendations• If treatment with denosumab is discontinued, there may be
an increase in bone turnover, bone mass loss and increased risk of vertebral fracture. Therefore
• Consider switching to another anti‐resorptive agent like a bisphosponate
• Studies with less potent antiresorptive agents may work ( SERM, calcitonin, estrogen) however need to be tested.
• Discuss with the potent patients the risk of increased fracture with discontinuation of treatment

Conclusions
• Mechanism of action• Rapid and potent effect
• Effect on fracture risk• Reduction in fracture risk, greatest effect at the spine
• Effect on bone turnover and density• Greater than oral alendronate
• Long-term effect on bone density• Continued effects to 10 years
• Safety• Cellulitis; a few cases of ONJ, AFF; transient
hypocalcaemia (avoided by administration of calcium and vitamin D supplements), and if discontinuing Denosumab- consider treatment with another anti-resorptive agent for a few years.
• Denosumab treatment for up to 10 years was associated with:
– persistent reduction of bone turnover
– continued increases in BMD without therapeutic plateau
– low incidence of new vertebral and nonvertebral (including hip) fracture
– no evidence of resistance to therapy
– no new adverse events with long-term therapy
Summary
• Long-term therapy to treat patients with osteoporosis is necessary and important for many patients
• Discontinuing therapy results in rapid loss of gains
• There is rarely a need to discontinue denosumab therapy
– Certainly no need for a “drug holiday”
• Denosumab is effective in elderly patients
• The benefit/risk profile for denosumab in an aging population of postmenopausal women remains favorable
Conclusions
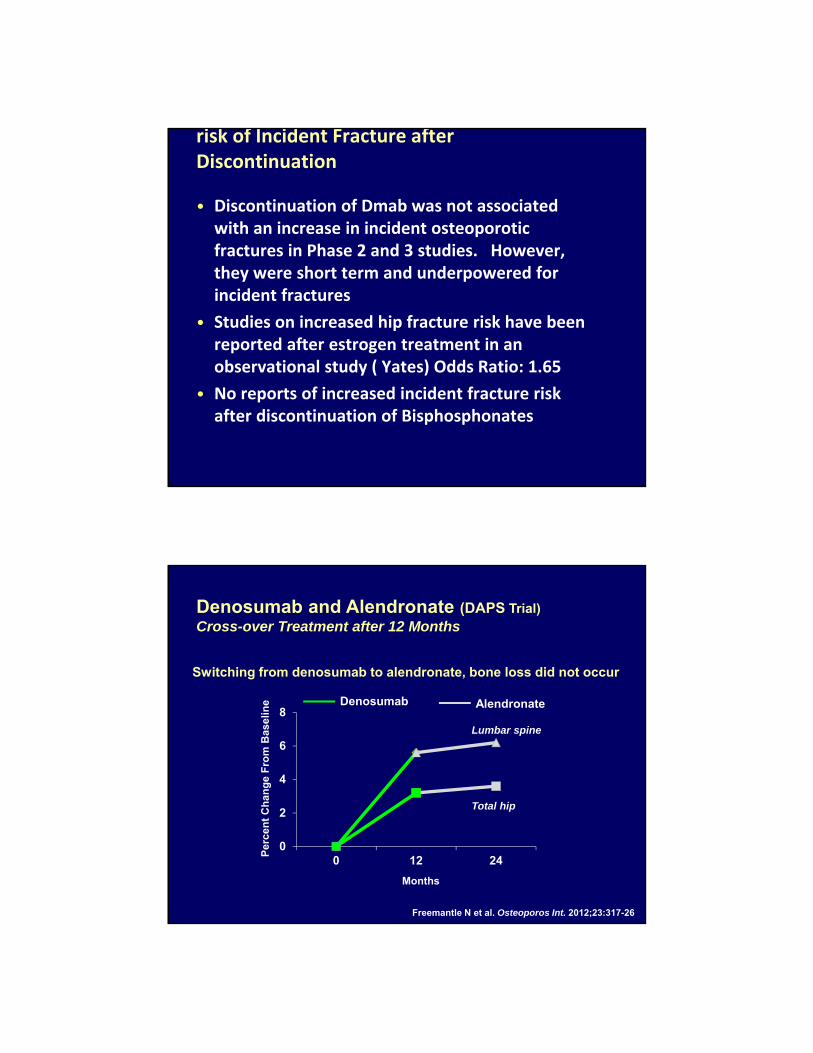
risk of Incident Fracture after Discontinuation
• Discontinuation of Dmab was not associated with an increase in incident osteoporotic fractures in Phase 2 and 3 studies. However, they were short term and underpowered for incident fractures
• Studies on increased hip fracture risk have been reported after estrogen treatment in an observational study ( Yates) Odds Ratio: 1.65
• No reports of increased incident fracture risk after discontinuation of Bisphosphonates
0
2
4
6
8
0 12 24
Denosumab and Alendronate (DAPS Trial)Cross-over Treatment after 12 Months
Freemantle N et al. Osteoporos Int. 2012;23:317-26
Per
cen
t C
han
ge
Fro
m B
asel
ine
Months
Denosumab Alendronate
Switching from denosumab to alendronate, bone loss did not occur
Lumbar spine
Total hip
Discontinuing DenosumabChange in Prescribing Information
• A new caution has been added to Prolia label:
• Multiple vertebral fractures have been reported following Prolia discontinuation.
• Consider transitioning to another antiresorptive agent if Prolia is discontinued.
• There are very few reasons to consider stopping denosumab therapy• intolerance or side effect• reaching a treatment “target”
• If therapy is stopped after a year or more, consider options to prevent rapid bone loss and fracture risk
• At present, the most appealing strategy would be to treat with a bisphosphonate for 1-2 years, re-evaluating the patient at regular intervals
Long-term Denosumab TherapySummary
McClung MR. Cancel the denosumab holiday. Osteoporos Int. 2016;27:1677-82
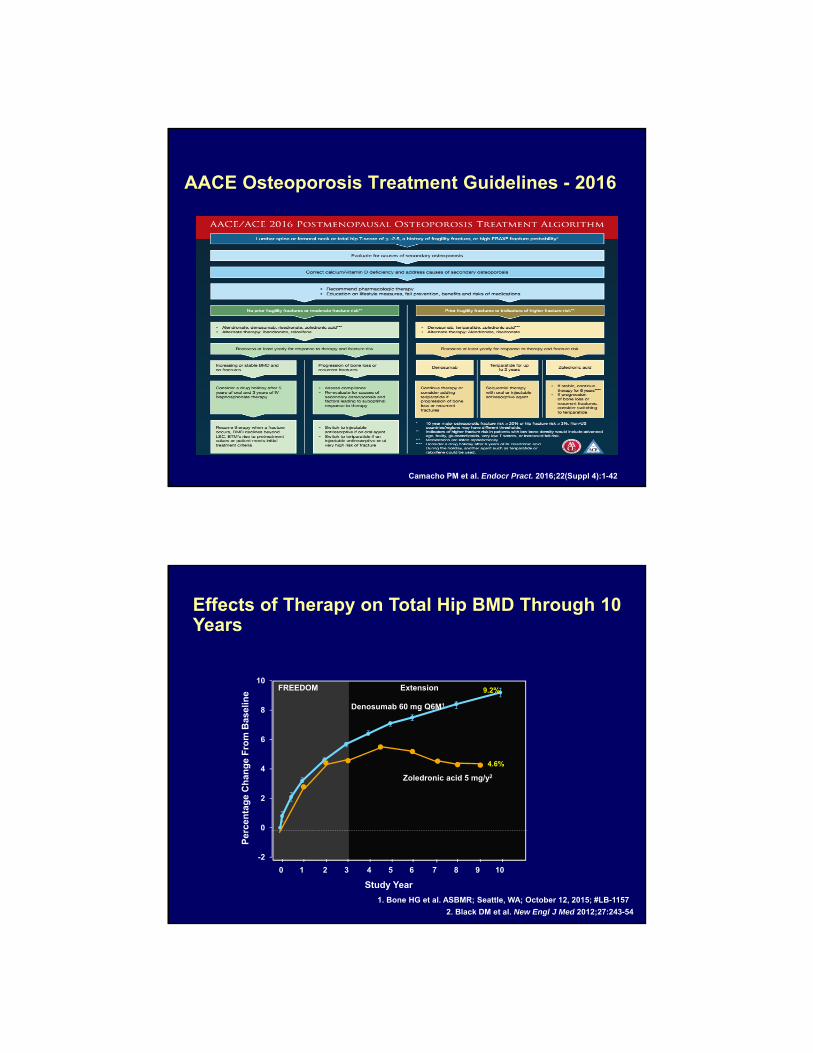
Camacho PM et al. Endocr Pract. 2016;22(Suppl 4):1-42
AACE Osteoporosis Treatment Guidelines - 2016
Effects of Therapy on Total Hip BMD Through 10 Years
Long-term Denosumab
1. Bone HG et al. ASBMR; Seattle, WA; October 12, 2015; #LB-1157
FREEDOM Extension
-2
0
2
4
6
8
109.2%
Per
cen
tag
e C
han
ge
Fro
m B
asel
ine
Study Year
1 2 3 4 50 6 7 8 9 10
4.6%
2. Black DM et al. New Engl J Med 2012;27:243-54
Zoledronic acid 5 mg/y2
Denosumab 60 mg Q6M1
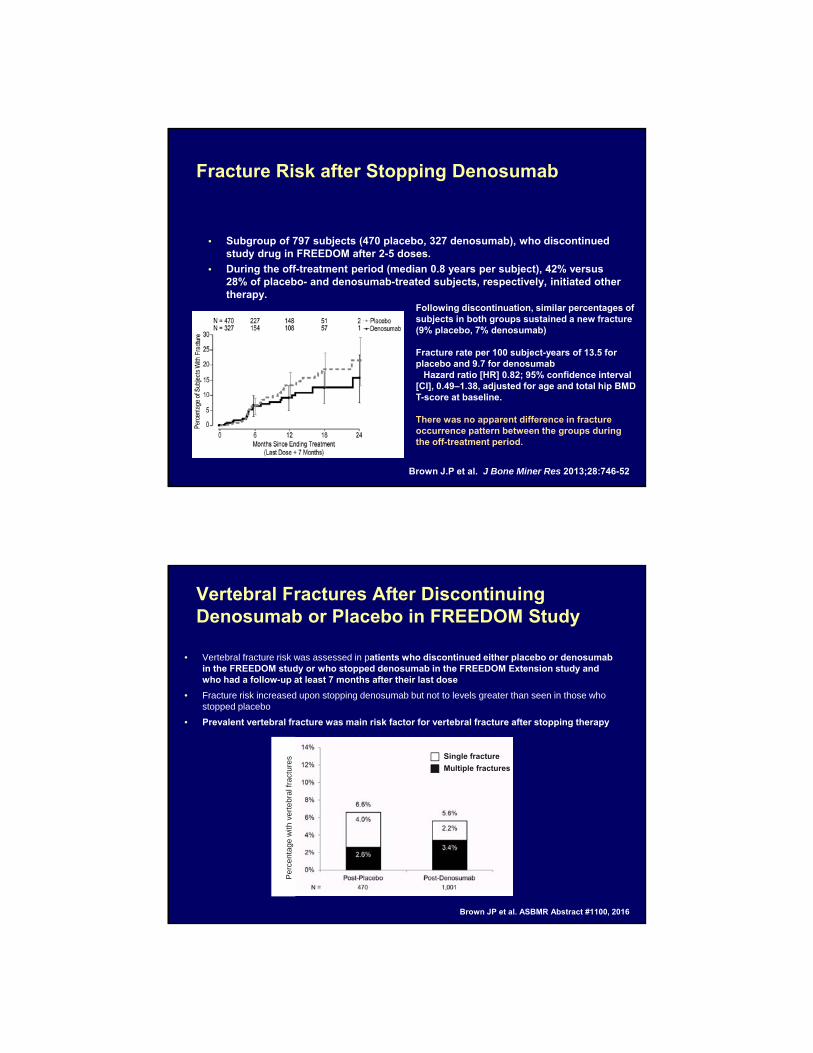
Fracture Risk after Stopping Denosumab
• Subgroup of 797 subjects (470 placebo, 327 denosumab), who discontinued study drug in FREEDOM after 2-5 doses.
• During the off-treatment period (median 0.8 years per subject), 42% versus 28% of placebo- and denosumab-treated subjects, respectively, initiated other therapy.
Brown J.P et al. J Bone Miner Res 2013;28:746-52
Following discontinuation, similar percentages of subjects in both groups sustained a new fracture (9% placebo, 7% denosumab)
Fracture rate per 100 subject-years of 13.5 for placebo and 9.7 for denosumab
Hazard ratio [HR] 0.82; 95% confidence interval [CI], 0.49–1.38, adjusted for age and total hip BMD T-score at baseline.
There was no apparent difference in fracture occurrence pattern between the groups during the off-treatment period.
Vertebral Fractures After Discontinuing Denosumab or Placebo in FREEDOM Study
Brown JP et al. ASBMR Abstract #1100, 2016
• Vertebral fracture risk was assessed in patients who discontinued either placebo or denosumab in the FREEDOM study or who stopped denosumab in the FREEDOM Extension study and who had a follow-up at least 7 months after their last dose
• Fracture risk increased upon stopping denosumab but not to levels greater than seen in those who stopped placebo
• Prevalent vertebral fracture was main risk factor for vertebral fracture after stopping therapy
Single fracture
Multiple fractures
Pe
rce
nta
ge w
ith v
ert
eb
ral f
ract
ure
s
Fracture Risk after Stopping Denosumab• Protection from vertebral fractures is quickly lost upon
stopping denosumab
BUT
• There is no apparent excess or rebound in vertebral fracture risk upon stopping therapy
McClung M. Personal opinion, 2017
• Bone loss and rise in serum CTX is attenuated in patients who stop denosumab but who took bisphosphonates before denosumab therapy.
• Bone loss after stopping denosumab is attenuated in patients who then receive anti-remodeling agents
Discontinuing DenosumabOther Information
Ferrari S et al. ECTS 2016
McClung M et al. Osteoporos Int. 2017;28:1723-32
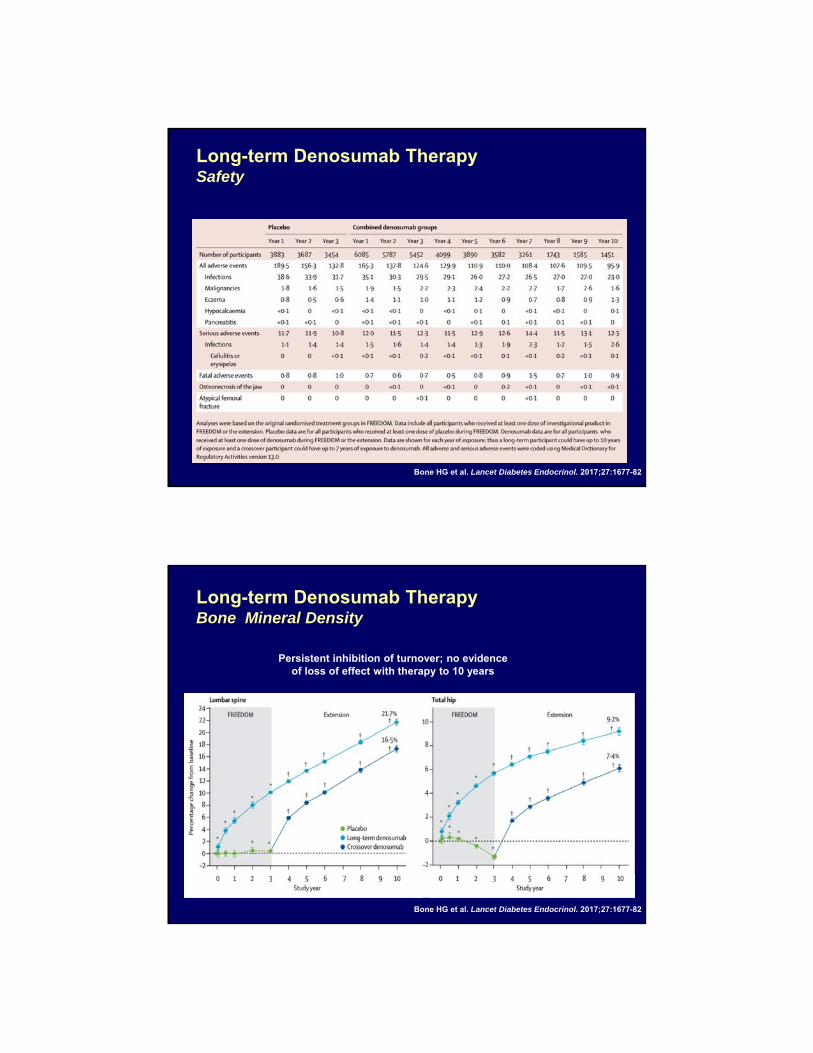
Long-term Denosumab TherapySafety
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
Long-term Denosumab TherapyBone Mineral Density
Persistent inhibition of turnover; no evidence of loss of effect with therapy to 10 years
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
Long-term Denosumab TherapyBone Mineral Density
Persistent inhibition of turnover; no evidence of loss of effect with therapy to 10 years
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
Long-term Denosumab TherapyBone Turnover Markers
Persistent inhibition of turnover; no evidence of loss of effect with therapy to 10 years
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
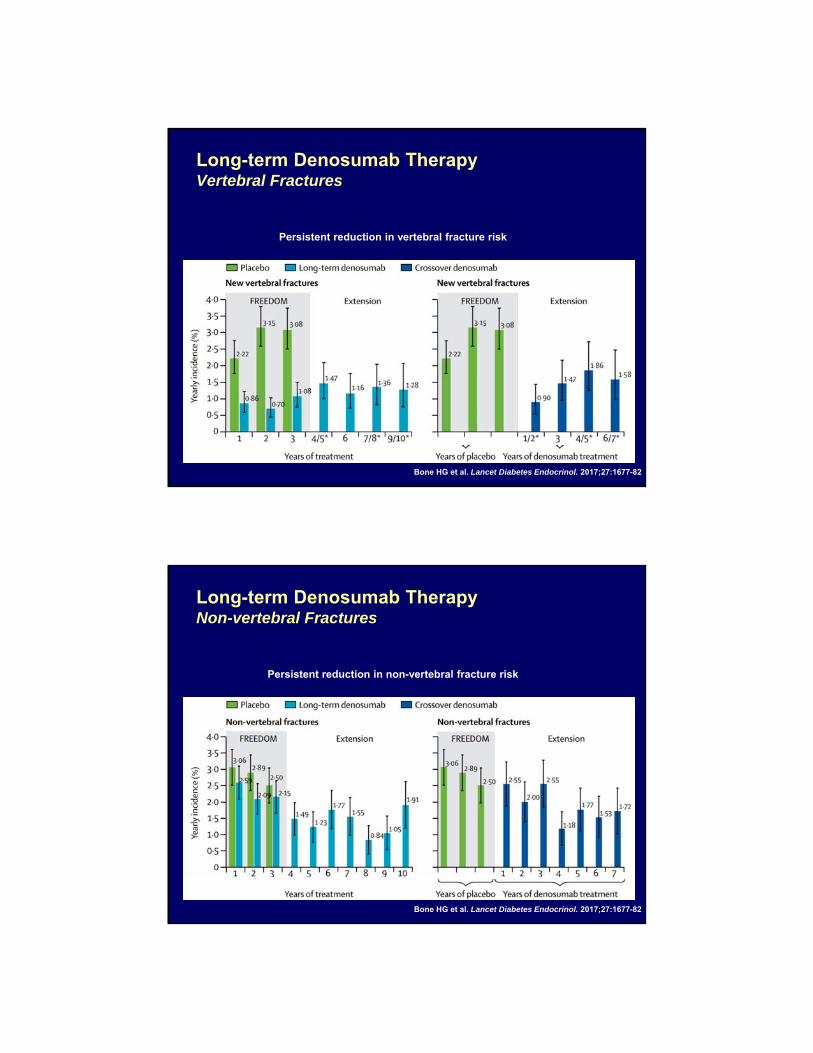
Long-term Denosumab TherapyVertebral Fractures
Persistent reduction in vertebral fracture risk
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
Long-term Denosumab TherapyNon-vertebral Fractures
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
Persistent reduction in non-vertebral fracture risk
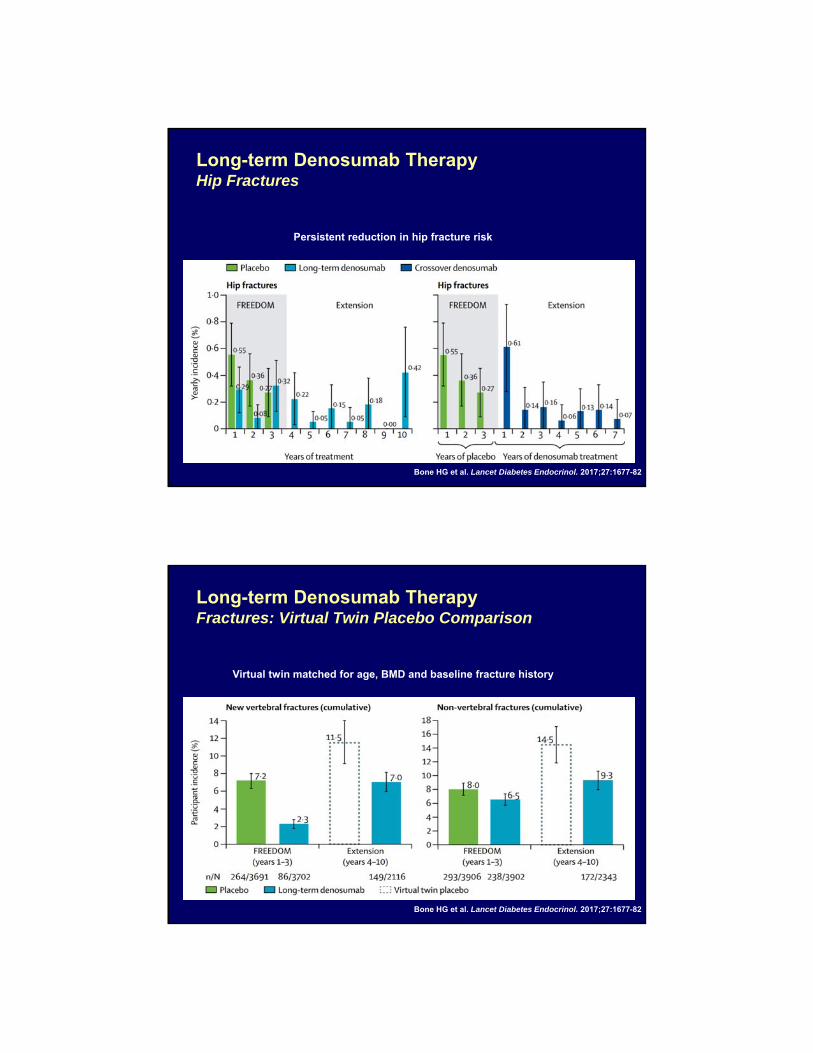
Long-term Denosumab TherapyHip Fractures
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
Persistent reduction in hip fracture risk
Long-term Denosumab TherapyFractures: Virtual Twin Placebo Comparison
Virtual twin matched for age, BMD and baseline fracture history
Bone HG et al. Lancet Diabetes Endocrinol. 2017;27:1677-82
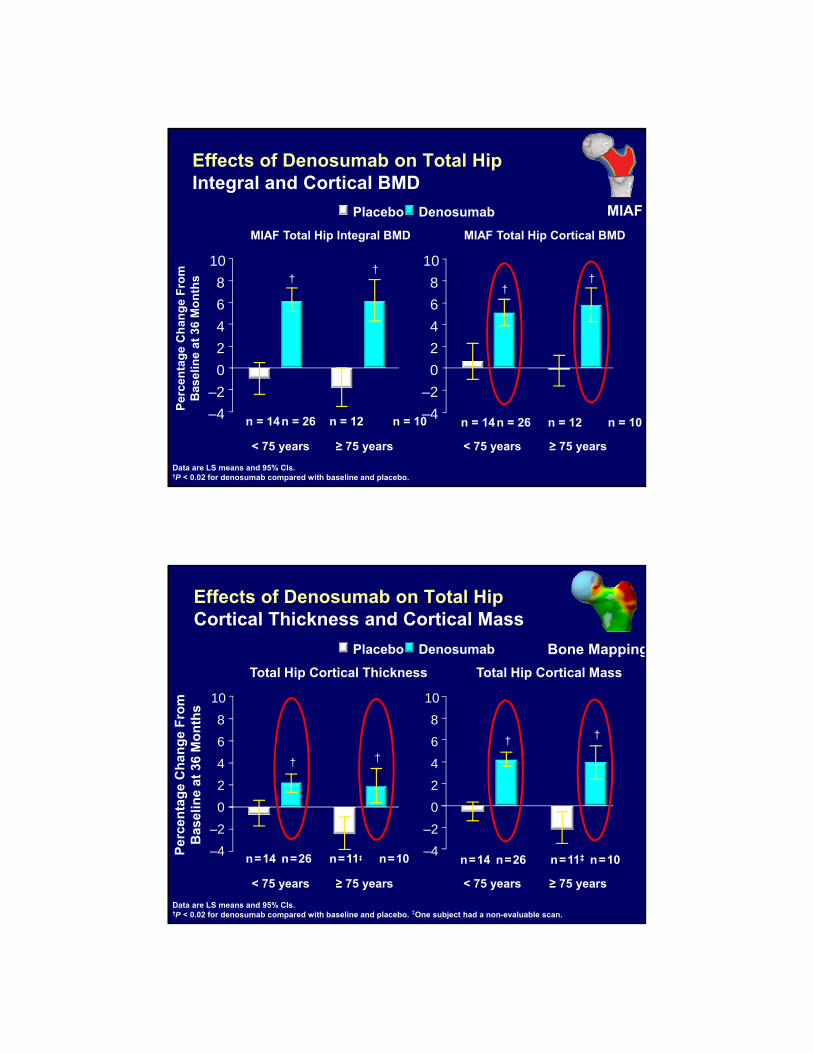
Effects of Denosumab on Total HipIntegral and Cortical BMD
Data are LS means and 95% CIs.†P < 0.02 for denosumab compared with baseline and placebo.
–4
–2
0
2
4
6
8
10†
†
††
Placebo Denosumab
–4
–2
0
2
4
6
8
10
MIAF Total Hip Integral BMD MIAF Total Hip Cortical BMD
≥ 75 years< 75 years ≥ 75 years< 75 years
Per
cen
tag
e C
han
ge
Fro
mB
asel
ine
at 3
6 M
on
ths
n = 14n = 26 n = 12 n = 10 n = 14n = 26 n = 12 n = 10
MIAF
Effects of Denosumab on Total Hip Cortical Thickness and Cortical Mass
Data are LS means and 95% CIs. †P < 0.02 for denosumab compared with baseline and placebo. ‡One subject had a non-evaluable scan.
† †
–4
–2
0
2
4
6
8
10
††
–4
–2
0
2
4
6
8
10
Total Hip Cortical Thickness Total Hip Cortical Mass
Placebo Denosumab
Per
cen
tag
e C
han
ge
Fro
mB
asel
ine
at 3
6 M
on
ths
≥ 75 years< 75 years ≥ 75 years< 75 years
n=14 n=26 n=11‡ n=10 n=14 n=26 n=11‡ n=10
Bone Mapping
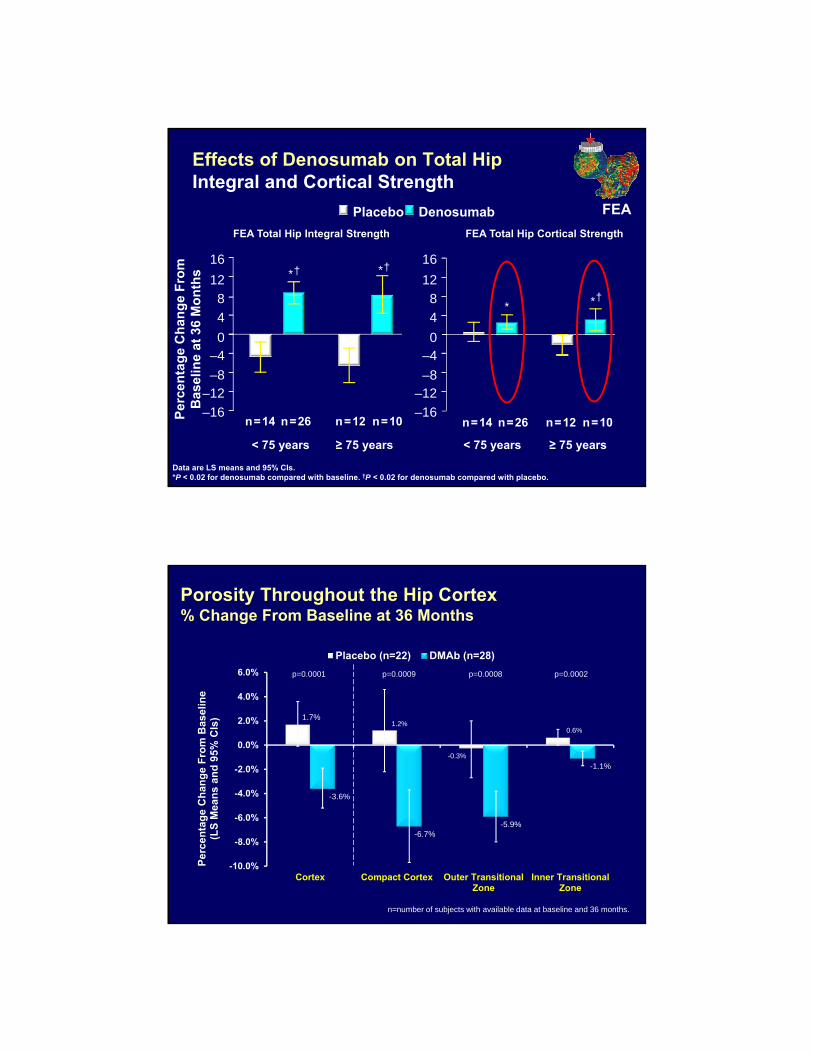
Data are LS means and 95% CIs. *P < 0.02 for denosumab compared with baseline. †P < 0.02 for denosumab compared with placebo.
Effects of Denosumab on Total HipIntegral and Cortical Strength
Placebo Denosumab
* *
**
Per
cen
tag
e C
han
ge
Fro
mB
asel
ine
at 3
6 M
on
ths
–12–8
–40
4
8
12
16
–16
FEA Total Hip Integral Strength FEA Total Hip Cortical Strength
–12–8
–40
4
8
12
16
–16
† †
†
≥ 75 years< 75 years ≥ 75 years< 75 years
n=14 n=26 n=12 n=10 n=14 n=26 n=12 n=10
FEA
Porosity Throughout the Hip Cortex% Change From Baseline at 36 Months
1.7%1.2%
-0.3%
0.6%
-3.6%
-6.7%-5.9%
-1.1%
-10.0%
-8.0%
-6.0%
-4.0%
-2.0%
0.0%
2.0%
4.0%
6.0%
Cortex Compact Cortex Outer TransitionalZone
Inner TransitionalZone
Per
cen
tag
e C
han
ge
Fro
m B
asel
ine
(LS
Mea
ns
and
95%
CIs
)
Placebo (n=22) DMAb (n=28)
p=0.0001 p=0.0009 p=0.0008 p=0.0002
n=number of subjects with available data at baseline and 36 months.