-
Depressive symptoms and regional cerebral blood ow inAlzheimer's
disease
Seishi Terada a,n, Etsuko Oshima a, Shuhei Sato b, Chikako Ikeda
a, Shigeto Nagao a,Satoshi Hayashi a, Chinatsu Hayashibara a, Osamu
Yokota a, Yosuke Uchitomi a
a Department of Neuropsychiatry, Okayama University Graduate
School of Medicine, Dentistry and Pharmaceutical Sciences,2-5-1
Shikata-cho, Kita-ku, Okayama 700-8558, Japanb Department of
Radiology, Okayama University Graduate School of Medicine,
Dentistry and Pharmaceutical Sciences, Okayama, Japan
a r t i c l e i n f o
Article history:Received 31 December 2012Received in revised
form23 October 2013Accepted 9 November 2013Available online 15
November 2013
Keywords:Alzheimer's disease (AD)DepressionDepressive
symptomRegional cerebral blood ow (rCBF)
a b s t r a c t
Depressive symptoms are common in patients with Alzheimer's
disease (AD) and increase the caregiverburden, although the
etiology and pathologic mechanism of depressive symptoms in AD
patients remainunclear. In this study, we tried to clarify the
cerebral blood ow (CBF) correlates of depressive symptomsin AD,
excluding the effect of apathy and anxiety. Seventy-nine
consecutive patients with AD wererecruited from outpatient units of
the Memory Clinic of Okayama University Hospital. The level
ofdepressive symptoms was evaluated using the depression domain of
the Neuropsychiatric Inventory(NPI). The patients underwent brain
SPECT with 99mTc-ethylcysteinate dimer. After removing the
effectsof age, anxiety and apathy scores of NPI, and ve subscales
of Addenbrooke's Cognitive Examination-revised (ACE-R), correlation
analysis of NPI depression scores showed a signicant cluster of
voxels in theleft middle frontal gyrus (Brodmann area 9), similar
to the areas in the simple correlation analysis. Thedorsolateral
prefrontal area is signicantly involved in the pathogenesis of
depressive symptoms in AD,and the area on the left side especially
may be closely related to the depressive symptoms revealedby
NPI.
& 2013 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Alzheimer's disease (AD) is the leading cause of
late-onsetdementia worldwide. Depressive symptoms are common
inpatients with AD and increase the caregiver burden (Akiyamaet
al., 2008; Kataoka et al., 2010). Although the etiology
andpathologic mechanism of depressive symptoms in AD patientsremain
unclear, a biological marker that objectively evaluatesdepressive
symptoms might be useful (Kataoka et al., 2010).
There have been several studies on the relationship of
depressivesymptoms to regional cerebral blood ow (rCBF) or regional
cerebralglucose metabolism in AD (Hirono et al., 1998; Liao et al.,
2003;Holthoff et al., 2005; Lee et al., 2006; Levy-Cooperman et
al., 2008;Akiyama et al., 2008). Data from previous functional
imaging studieshave mainly supported the role of the dorsolateral
prefrontal region(Hirono et al., 1998; Holthoff et al., 2005; Lee
et al., 2006; Levy-Cooperman et al., 2008; Akiyama et al., 2008).
Associations with theanterior cingulate have been described
inconsistently (Hirono et al.,
1998; Liao et al., 2003). However, most of these studies did
notexclude AD patients with apathy or anxiety, although
depressioncommonly coexists with apathy and anxiety (Kataoka et
al., 2010).The presence of apathy is particularly germane as
anterior cingulateand prefrontal hypoperfusion has been associated
with apathysymptoms in AD patients (Lanctt et al., 2007). Moreover,
almostall studies were performed in a cross-sectional setting
(Hirono et al.,1998; Holthoff et al., 2005; Lee et al., 2006;
Levy-Cooperman et al.,2008; Akiyama et al., 2008).
In this study, we tried to identify the cerebral blood
owcorrelates of depressive symptoms in AD without the effect of
apathyand anxiety by correlation analysis. We predicted a
signicantrelationship between depressive symptoms and rCBF in the
dorso-lateral prefrontal regions of AD patients.
2. Methods
2.1. Subjects
Seventy-nine consecutive patients with Alzheimer's disease were
recruitedfrom the outpatient units of the Memory Clinic of Okayama
University Hospitalbetween September 2008 and April 2012 according
to the following criteria. Theyall (i) underwent general physical
and neurological examinations and extensive
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/psychresns
Psychiatry Research: Neuroimaging
0925-4927/$ - see front matter & 2013 Elsevier Ireland Ltd.
All rights
reserved.http://dx.doi.org/10.1016/j.pscychresns.2013.11.002
n Correspondence to: Department of Neuropsychiatry, Okayama
University GraduateSchool of Medicine, Dentistry and Pharmaceutical
Sciences. Tel.: 81 86 235 7242;fax: 81 86 235 7246.
E-mail address: [email protected] (S. Terada).
Psychiatry Research: Neuroimaging 221 (2014) 8691
-
laboratory testing, including thyroid function tests, serum
vitamin B12, and syphilisserology; (ii) took the revised
Addenbrooke's Cognitive Examination (ACE-R)(Yoshida et al., 2012),
the Mini Mental State Examination (MMSE) (Folstein et al.,1975),
the Frontal Assessment Battery (FAB) (Kugo et al., 2007); (iii)
underwentsingle photon emission computed tomography (SPECT) with
99mTc-ethylcysteinatedimer of the brain as well as magnetic
resonance imaging (MRI) of the head; and(iv) were diagnosed with
probable AD according to the criteria formulated bythe NINCDS-ADRDA
(McKhann et al., 1984). The exclusion criteria were(i)
complications from other neurological diseases or illnesses; (ii)
history ofmental illness or substance abuse prior to the onset of
dementia; (iii) evidence offocal brain lesions on head MRI; (iv)
treatment with cholinesterase inhibitors,memantine, antipsychotics,
antidepressants, or anxiolytic drugs; and (v) lefthandedness or
ambidexterity.
The prole of each subject (age, sex, months of disease duration,
and years ofeducation) was obtained. Scores on three subscales
(depression, anxiety, andapathy) of the Neuropsychiatric Inventory
(NPI), Barthel Index, and FunctionalAssessment Questionnaire (FAQ)
were rated by a trained clinical psychologist,based on the
information from family caregivers. The Clinical Dementia
Rating(CDR) (Hughes et al., 1982) score was rated by the chief
clinician.
2.2. Instruments
NPI is a valid and reliable instrument for measuring
non-cognitive symptoms indementia (Cummings et al., 1994; Hirono et
al., 1997). It is a caregiver-based toolthat assesses ten different
domains in dementia. The NPI gives a composite scorefor each
domain, which is the product of frequency multiplied by
severitysubscores: scores from 1 to 4 (with 4 being the most
severe) for the frequencyand from 1 to 3 (with 3 being the most
severe) for the severity of each behavior(Akiyama et al., 2008).
The maximum attainable score was 12. In this study, threesubscales
(depression, anxiety, and apathy) were used.
ACE-R was developed to provide a brief test sensitive to early
stage dementia,and is capable of differentiating between dementia
subtypes including AD,frontotemporal dementia, progressive
supranuclear palsy, and other parkinsoniansyndromes (Mioshi et al.,
2006). ACE-R includes MMSE, but extends it toencompass important
areas not covered by MMSE, such as frontal-executivefunction and
visuospatial skills. For this study, we used the Japanese version
ofACE-R described by Yoshida et al. (2012).
The Barthel Index consists of 10 items that measure a person's
daily function-ing, specically the activities of daily living and
mobility (Wade and Collin, 1988).The total Barthel Index score
ranges from 0 to 100. A higher score indicates a betterperformance.
The Functional Assessment Questionnaire (FAQ) measures
functionalactivities of older adults using the patient's partner as
an informant (Pfeffer et al.,1982). The FAQ consists of ten items,
and the score on each item ranges from 0 to 3.A higher score
indicates more severe impairment.
2.3. Ethics
This study was approved by the Internal Ethical Committee of
OkayamaUniversity Graduate School of Medicine, Dentistry, and
Pharmaceutical Sciences.After a complete description of the study
to the subjects and their relatives, writteninformed consent was
obtained.
2.4. Brain perfusion SPECT imaging
All subjects were examined by brain perfusion SPECT. Patients
were examinedin a comfortable supine position with their eyes
closed in quiet surroundings. Tenminutes after intravenous
administration of 99mTc-ethylcysteinate dimer (ECD,600MBq, Daiichi
Radioisotope Laboratories Ltd., Tokyo, Japan), SPECT images
wereobtained using a triple-head, rotating gamma camera interfaced
to a minicomputer(GCA9300A/ DI; Toshiba, Tokyo, Japan) equipped
with a fanbeam, low-energy,high-resolution collimator. Sixty
projection images over a 3601 angle in a 128128matrix were
acquired. All images were reconstructed using ramp-ltered
back-projection and then three-dimensionally smoothed with a
Butterworth lter (order8, cutoff 0.12 cycles/cm). The reconstructed
images were corrected for gamma rayattenuation using the Chang
method (0.09).
2.5. Data analysis
Spatial reprocessing and statistical analysis of images was
performed on a voxel-by-voxel basis using Statistical Parametric
Mapping 8 (SPM8, Wellcome Departmentof Imaging Neuroscience, UK)
running on MATLAB (The Mathworks, Inc., Natick, MA,USA). All SPECT
images of each subject were normalized to the standard brain of
theMontreal Neurological Institute (MNI), and spatial normalization
was performed with12-parameter afne and non-linear transformations
(Friston et al., 1995). The voxelsizes of the reslice option were 2
mm2 mm2 mm. The non-linear parameterswere set at 25 mm cut-off
basis functions and 16 iterations. All the normalized SPECT
images were then smoothed with an isotropic Gaussian kernel lter
(12 mm full-width at half-maximum).
We applied a simple regression method using SPM8 to obtain the
correlationbetween NPI-dep scores and rCBF imaging data from SPECT
among 79 AD subjects. Theanalysis used a threshold of po0.001
(uncorrected) at the voxel level, and results wereconsidered
signicant at 100 voxels at the cluster level (simple correlation
analysis).Thereafter, to remove the effect of other factors, age,
ve subscale scores of ACE-R andtwo subscale scores (anxiety,
apathy) of NPI were entered into the model as nuisancecovariates,
and we performed a simple regression method using SPM8 to obtain
thecorrelation between NPI-dep and rCBF imaging data from SPECT.
The specic effects ofdepressive symptoms were tested using [1]
t-contrast with an additional zero for thescores of other factors,
assuming that the presence of the symptoms would be
uniquelyassociated with decreased rCBF. In the latter analysis, a
threshold of po0.001(uncorrected) was used at the voxel level, and
results were considered signicant at100 voxels at the cluster
level. In both analyses, global normalization was performed
byproportional scaling with the mean voxel value. Masking was
applied using thethreshold method (0.8 times the global value). In
both analyses, global normalizationwas performed by proportional
scaling with the mean voxel value. Masking was appliedusing the
threshold method (0.8 times the global value).
2.6. Statistical analysis
Statistical analysis was performed using the SPSS 14.0J software
program (SPSSInc., Chicago, IL). The correlation analysis of
NPI-dep scores to other clinicalcharacteristics was done by
Pearson's correlation coefciency. A value of po0.05was accepted as
signicant.
3. Results
3.1. Demographic characteristics
Demographic characteristics are shown in Table 1. Among 79AD
patients, 45 were women and 34 were men. For dementiaseverity, 47
patients had CDR scores 0.5, 31 had CDR 1, and onepatient had CDR
2. On the NPI depression score, 51 patients had ascore of 0, seven
patients scored 1, ten patients scored 2, tenpatients scored 3, and
one patient had a score of 6.
Table 1Clinical characteristics (n79).
Mean S.D. Range
Age (years) 76.2 7.6 4989Duration 28.3 16.6 479Education 11.0
2.5 416NPI-dep 0.8 1.3 06NPI-anxiety 0.2 0.7 04NPI-apathy 2.0 2.8
012MMSE 21.4 4.2 827ACE-R 65.4 13.3 3291Attention 13.7 3.2
318Memory 10.3 5.0 123Fluency 6.4 2.9 013Language 22.0 3.3
1026Visuospatial 12.9 3.0 416
FAB 10.3 2.8 316Barthel 96.9 5.4 80100FAQ 12.0 7.2 027
Duration, disease duration (months);Education, years of
education;NPI-Dep, depression scores of neuropsychiatric
inventory;Duration, duration of disease;Education, years of
education;MMSE, mini mental state examination;ACE-R, revised
Addenbrook's cognitive examination;Attention, attention and
orientation scores of ACE-R;Memory, memory scores of ACE-R;Fluency,
word uency scores of ACE-R;Language, language scores of
ACE-R;Visuospatial, visuospatial scores of ACE-R;FAB, frontal
assessment battery;Barthel. Barthel index;FAQ, functinal assessment
questionnaire.
S. Terada et al. / Psychiatry Research: Neuroimaging 221 (2014)
8691 87
-
Correlation analyses revealed that the NPI-dep score had
nosignicant correlation to demographic characteristics,
cognitivefunctions, or activities of daily living, except for
NPI-anxiety, andNPI-apathy scores (Table 2).
3.2. rCBF
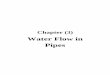
Fig. 1a and Table 3 show the SPM (z) map of signicantcorrelation
between rCBF and NPI-dep scores among AD patients.Simple
correlation analysis showed a signicant cluster of voxelsin the
left middle frontal gyrus (Brodmann area 9). Table 3 showsthe
probability results of the SPM analysis and the location of peakz
scores in terms of MNI coordinates.
After removing the effects of age, anxiety and apathy scores
onNPI, and ve subscales of ACE-R, correlation analysis showed
asignicant cluster of voxels in the left middle frontal
gyrus(Brodmann area 9), similar to the areas in the simple
correlationanalysis (Fig. 1b).
4. Discussion
There have been seven published studies, including this one,
onrCBF or regional cerebral glucose metabolism among AD
patientswith depressive symptoms (Table 4) (Hirono et al., 1998;
Liao et al.,2003; Holthoff et al., 2005; Lee et al., 2006;
Levy-Cooperman et al.,2008; Akiyama et al., 2008).
Among the seven studies, all except one (Liao et al.,
2003),showed that dorsolateral frontal regions are signicantly
related todepressive symptoms in AD. In only the study of Liao et
al. is rCBFin the bilateral anterior cingulate, left posterior
cingulate, and
bilateral precuneus different in AD patients with and
withoutdepression. Their study included more severely impaired
ADpatients (mean MMSE score was 12.9) compared to those in
otherstudies (Table 4). In their study, the severity of cognitive
impair-ment was measured by MMSE scores. MMSE is useful, but
toosimple to validate the similarity of cognitive impairment
betweentwo groups. The difference between cognitive impairments in
ADpatients with and without depression might indicate the
differ-ence of rCBF in the bilateral anterior cingulate, left
posteriorcingulate and bilateral precuneus. Based on the above, we
supposethat the dorsolateral prefrontal area is signicantly related
todepressive symptoms in AD and that depressive symptoms in ADare
due to a specic pathogenesis rather than a reactive phenom-enon
(Liao et al., 2003).
The published ndings on brain lateralization of decreasedrCBF
related to depressive symptoms in AD patients are conict-ing. Lee
et al. (2006) reported a signicant decrease of rCBF in theright
superior frontal region, and Levy-Cooperman et al. (2008)showed a
decrease of rCBF in the right dominant dorsolateral andsuperior
prefrontal regions . In both studies, apathy and anxietycoexisting
with depression were not considered, and the NPI-depscore was not
used to divide positive and negative groups. In theother four
studies, signicantly related regions related to depres-sive
symptoms were the bilateral superior frontal region (Hironoet al.,
1998), left dorsolateral region (Holthoff et al., 2005),
leftprefrontal region (Akiyama et al., 2008), and left middle
frontalgyrus (our study). In the latter four studies, the NPI-dep
score wasused to evaluate depressive symptoms (Table 4).
Additionally,Holthoff et al. (2005) tried to decrease the effect of
coexistingapathy statistically. In the study of Akiyama et al.
(2008), the twogroups (depressive and not depressive) showed
similar scores onapathy and anxiety scales. In our study,
correlation analyses afterremoving the effects of apathy and
anxiety scores revealed asimilar result. Laterality might be caused
by several factors, suchas the inuence of other lesions or the
severity of the disease, or itmight reect sample size, statistical
threshold, or criteria used toscore depressive symptoms (Kataoka et
al., 2010). Although notconclusively, we can say that the left
dorsolateral prefrontal regionis closely related to the depressive
symptoms evaluated by NPI.Many studies have reported that
abnormalities in cortical-limbicor cortical-subcortical circuits
related to emotional regulation areimplicated in the mechanisms
underlying emotional dysfunction(Peng et al., 2012). The middle
frontal gyrus is located in thedorsolateral prefrontal cortex
(DLPFC), and the DLPFC circuit is oneof the prefrontal-subcortical
circuits, some of which are involvedin regulation of affect (Peng
et al., 2012).
Several studies have found that depression is generally
asso-ciated with less left frontal activity and/or more right
frontalactivity (Bell et al., 1998; Minnix et al., 2004). It has
beenhypothesized that relative left frontal activity is related to
positiveemotion and approach motivation, whereas relative right
frontalactivity is related to negative emotion and withdrawal
motivation(Davidson et al., 2000; Minnix et al., 2004). In AD, the
left frontalregion might induce relative right frontal activity and
negativeemotion.
5. Limitations
The results in this study should be interpreted with
somecaution. Firstly, domain scores lower than 4 points of
NPI-depreect behavioral symptoms of mild severity referred to as
asubclinical disturbance (Holthoff et al., 2005). In this study,
almostall patients had scores less than 4 in the NPI-dep
domain.However, the degree of hypoperfusion in the middle frontal
gyruswas correlated with the severity of depressive symptoms in
our
Table 2Correlation analysis of NPI-Dep.
NPI-Dep
Age 0.166Duration 0.001Education 0.015NPI-anxiety 0.487nnn
NPI-apathy 0.340nn
MMSE 0.045ACE-R 0.026Attention 0.023Memory 0.132Fluency
0.189Language 0.142Visuospatial 0.050
FAB 0.121Barthel 0.018FAQ 0.063
NPI-Dep, depression scores of neuropsychiatric
inventory;Duration, duration of disease;Education, years of
education;MMSE, mini mental state examination;ACE-R, revised
Addenbrook's cognitive examination;Attention, attention and
orientation scores of ACE-R;Memory, memory scores of ACE-R;Fluency,
word uency scores of ACE-R;Language, language scores of
ACE-R;Visuospatial, visuospatial scores of ACE-R;FAB, frontal
assessment battery;Barthel. Barthel index;FAQ, functinal assessment
questionnaire;npo0.05.nn po0.01.nnn po0.001.
S. Terada et al. / Psychiatry Research: Neuroimaging 221 (2014)
869188
-
Fig. 1. (a) Correlation. The SPM (z) map of signicant
correlation between rCBF and NPI-dep scores among AD patients.
Upper line, three-way glass view of the area ofsignicant
correlation. Lower line, three-way section of the area of signicant
hypoperfusion. Left, transverse, z30; central, sagittal, x30;
right, coronal, y24.(b) Correlation after removing effects of other
factors. The SPM (z) map of signicant correlation between rCBF and
NPI-dep scores among AD patients after removing theeffects of age,
ve subscale scores of ACE-R, and two subscale scores (anxiety,
apathy) of NPI. Upper line, three-way glass view of the area of
signicant correlation. Lowerline, three-way section of the area of
signicant hypoperfusion. Left, transverse, z34; central, sagittal,
x30; right, coronal, y24.
Table 3Regions signicantly related with NPI-dep scores.
Number of voxels Peak z scores p Coordinates (MNI)
x y z
Region where rCBF signicantly correlate with NPI-dep scores
(Fig. 1a) 107 3.90 o0.001 30 24 303.77 o0.001 28 22 34
Region where rCBF signicantly correlate with NPI-dep scores
afterremoving the effect of other factorsn (Fig. 1b)
151 4.15 o0.001 30 24 34
rCBF, regional cerebral blood ow; NPI-Dep, depression scores of
neuropsychiatric inventory.Voxels, number of voxels; Z scores, peak
Z scores; MNI, Montreal Neurological Institute.
n Other factors are age, ve subscales scores of ACE-R, anxiety
and apathy subscale scores of NPI.
S. Terada et al. / Psychiatry Research: Neuroimaging 221 (2014)
8691 89
-
analysis. Therefore, we suppose that hypoperfusion in the
middlefrontal gyrus was involved in the expression of clinically
depres-sive symptoms in patients with AD. Secondly, although
thethreshold of 0.001 (uncorrected) may be regarded as the
standardthreshold currently, we did not nd any signicant area under
thestrict threshold of 0.01 (corrected).
Acknowledgments
We sincerely thank Ms. Ido, Ms. Horiuchi, Ms. Imai, and Ms.Yabe
for their skillful assistance. This work was supported byGrants
from the Japanese Ministry of Education, Culture, Sports,Science
and Technology (21591517), and the Zikei Institute
ofPsychiatry.
References
Akiyama, H., Hashimoto, H., Kawabe, J., Higashiyama, S., Kai,
T., Kataoka, K.,Shimada, A., Inoue, K., Shiomi, S., Kiriike, N.,
2008. The relationship betweendepressive symptoms and prefrontal
hypoperfusion demonstrated by eZIS inpatients with DAT.
Neuroscience Letters 441, 328331,
http://dx.doi.org/10.1016/j.neulet.2008.06.053.
Bell, I.R., Schwartz, G.E., Hardin, E.E., Baldwin, C.M., Kline,
J.P., 1998. Differentialresting quantitative
electroencephalographic alpha patterns in women withenvironmental
chemical intolerance, depressives, and normals.
BiologicalPsychiatry 43, 376388.
Cummings, J.L., Mega, M., Gray, K., Rosenberg-Thompson, S.,
Carusi, D.A., Gornbein, J.,1994. The Neuropsychiatric Inventory:
comprehensive assessment of psycho-pathology in dementia. Neurology
44, 23082314.
Davidson, R.J., Jackson, D.C., Kalin, N.H., 2000. Emotion,
plasticity, context, andregulation: perspectives from affective
neuroscience. Psychological Bulletin126, 890909.
Folstein, M.F., Folstein, S.E., McHugh, P.R., 1975. "Mini-mental
state". A practicalmethod for grading the cognitive state of
patients for the clinician. Journal ofPsychiatry Research 12,
189198.
Friston, K.J., Ashburner, J., Poline, J.B., Frith, C.D.,
Heather, J.D., Frackowiak, R.S.J.,1995. Spatial realignment and
normalization of images. Human Brain Mapping2, 165189.
Hirono, N., Mori, E., Ikejiri, Y., Imamura, T., Shimomura, T.,
Hashimoto, M.,Yamashita, H., Ikeda, M., 1997. Japanese version of
the NeuropsychiatricInventory: a scoring system for
neuropsychiatric disturbance in dementiapatients. Brain and Nerve
49, 266271. (in Japanese with English abstract).
Hirono, N., Mori, E., Ishii, K., Ikejiri, Y., Imamura, T.,
Shimomura, T., Hashimoto, M.,Yamashita, H., Sasaki, M., 1998.
Frontal lobe hypometabolism and depression inAlzheimer's disease.
Neurology 50, 380383.
Holthoff, V.A., Beuthien-Baumann, B., Kalbe, E., Ldecke, S.,
Lenz, O., Zndorf, G.,Spirling, S., Schierz, K., Winiecki, P.,
Sorbi, S., Herholz, K., 2005. Regionalcerebral metabolism in early
Alzheimer's disease with clinically signicantapathy or depression.
Biological Psychiatry 57, 412421,
http://dx.doi.org/10.1016/j.biopsych.2004.11.035.
Hughes, C.P., Berg, L., Danziger, W.L., Coben, L.A., Martin,
R.L., 1982. A new clinicalscale for the staging of dementia.
British Journal of Psychiatry 140, 566572.
Kataoka, K., Hashimoto, H., Kawabe, J., Higashiyama, S.,
Akiyama, H., Shimada, A.,Kai, T., Inoue, K., Shiomi, S., Kiriike,
N., 2010. Frontal hypoperfusion in depressedpatients with dementia
of Alzheimer type demonstrated on 3DSRT. Psychiatryand Clinical
Neuroscience 64, 293298,
http://dx.doi.org/10.1111/j.1440-1819.2010.02083.x.
Kugo, A., Terada, S., Ata, T., Ido, Y., Kado, Y., Ishihara, T.,
Hikiji, M., Fujisawa, Y., Sasaki, K.,Kuroda, S., 2007. Japanese
version of the Frontal assessment battery for dementia.Psychiatry
Research 153, 6975,
http://dx.doi.org/10.1016/j.psychres.2006.04.004.
Lanctt, K.L., Moosa, S., Herrmann, N., Leibovitch, F.S.,
Rothenburg, L., Cotter, A.,Black, S.E., 2007. A SPECT study of
apathy in Alzheimer's disease. Dementia andGeriatric Cognitive
Disorders 24, 6572, http://dx.doi.org/10.1159/000103633.
Lee, D.Y., Choo, I.H., Jhoo, J.H., Kim, K.W., Youn, J.C., Lee,
D.S., Kang, E.J., Lee, J.S.,Kang, W.J., Woo, J.I., 2006. Frontal
dysfunction underlies depressive syndromein Alzheimer disease: a
FDG-PET study. American Journal of Geriatric Psychia-try 14,
625628, http://dx.doi.org/10.1097/01.JGP.0000214541.79965.2d.
Levy-Cooperman, N., Burhan, A.M., Ra-Tari, S., Kusano, M.,
Ramirez, J., Caldwell, C.,Black, S.E., 2008. Frontal lobe
hypoperfusion and depressive symptoms inAlzheimer disease. Journal
of Psychiatry and Neuroscience 33, 218226.
Liao, Y.C., Liu, R.S., Lee, Y.C., Sun, C.M., Liu, C.Y., Wang,
P.S., Wang, P.N., Liu, H.C.,2003. Selective hypoperfusion of
anterior cingulate gyrus in depressed ADpatients: a brain SPECT
nding by statistical parametric mapping. Dementiaand Geriatric
Cognitive Disorders 16, 238244,
http://dx.doi.org/10.1159/000072808.
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D.,
Stadlan, E.M., 1984.Clinical diagnosis of Alzheimer's disease:
report of the NINCDS-ADRDA WorkGroup under the auspices of
Department of Health and Human Services TaskForce on Alzheimer's
disease. Neurology 34, 939944.
Minnix, J.A., Kline, J.P., Blackhart, G.C., Pettit, J.W., Perez,
M., Joiner, T.E., 2004.Relative left-frontal activity is associated
with increased depression in highreassurance-seekers. Biological
Psychology 67, 145155,
http://dx.doi.org/10.1016/j.biopsycho.2004.03.005.
Mioshi, E., Dawson, K., Mitchell, J., Arnold, R., Hodges, J.R.,
2006. The Addenbrooke'sCognitive Examination Revised (ACE-R): a
brief cognitive test battery fordementia screening. International
Journal of Geriatric Psychiatry 21,
10781085,http://dx.doi.org/10.1002/gps.1610.
Peng, H., Zheng, H., Li, L., Liu, J., Zhang, Y., Shan, B.,
Zhang, L., Yin, Y., Liu, J., Li, W.,Zhou, J., Li, Z., Yang, H.,
Zhang, Z., 2012. High-frequency rTMS treatmentincreases white
matter FA in the left middle frontal gyrus in young patients
Table 4Studies on the cerebral regions related with depressive
symptoms in Alzheimer's disease.
Hirono et al. (1998) Liao et al. (2003) Holthoff et
al.(2005)
Lee et al.(2006)
Levy-Cooperman et al.(2008)
Akiyama et al.(2008)
this study(2013)
Imaging PET SPECT PET PET SPECT SPECT SPECTSoftware ROI SPM99
SPM99 SPM99 SPM2 eZIS SPM8Statistics Comparison Correlation
comparison Comparison Comparison Comparison Comparison
CorrelationNumber 53 43 20 24 56 44 79Two
groups1934 835 1010 1212 2729 1826
Criteria NPI-dep o or 1- SCID NPI-dep o or 4- NIMH criteria CSDD
0-7 or 8- NPI-dep o or 1- NPI-depmean
MMSE21.2 12.9 22.2 nm 23.6 (16.5)n 21.4
Regions bil superior Fr, lt anteriorCin
bil anterior Cin, ltposteriorCin, bil precuneus
lt dorsolateral(preFr)
rt superior Fr dorsolateral &superior preFr (rtZ lt)
lt preFr lt preFr
ROI, manually placed range of interest; SPM, statistical
parametric mapping;eZIS, after eZIS analysis, semiquantitatively
scored from 0 to 2;Number, number of patients with Alzheimer's
disease;Two groups, number of two groups depression positive and
negative;Criteria, criteria for grouping;Regions, areas showing
signicant decrease of regional cerebral blood ow among patients
with depression or areas showing signicant correlation to
depressive symptoms;NPI-dep, depression score of neuropsychiatric
inventory;SCID, structured clinical interview for the Diagnostic
Statistical Manual of mental disorders ed 3 revised;CSDD, Cornell
scale for depression in dementia; MMSE, mini-mental state
examinationn, mean score of the revised Hasegawa Dementia Scale
(full score 30);NIMH, NIMH criteria for depression in Alzheimer's
disease;nm, Not mentioned; bil, bilateral; r, right; lt, left; Fr,
frontal; Cin, cingulate; AchE inhibitors, acetylcholine.
S. Terada et al. / Psychiatry Research: Neuroimaging 221 (2014)
869190
-
with treatment-resistant depression. Journal of Affective
Disorders 136,
249257,http://dx.doi.org/10.1016/j.jad.2011.12.006.
Pfeffer, R.I., Kurosaki, T.T., Harrah, C.H., Chance, J.M.,
Filos, S., 1982. Measurement ofthe functional activities in older
adults in the community. Journal of Gerontol-ogy 37, 323329.
Wade, D.T., Collin, C., 1988. The Barthel ADL Index: a standard
measure of physicaldisability? International Disability Studies 10,
6467.
Yoshida, H., Terada, S., Honda, H., Kishimoto, Y., Takeda, N.,
Oshima, E., Hirayama, K.,Yokota, O., Uchitomi, Y., 2012. Validation
of the revised Addenbrooke'sCognitive Examination (ACE-R) for
detecting mild cognitive impairment anddementia in a Japanese
population. International Psychogeriatrics 24,
2837,http://dx.doi.org/10.1017/S1041610211001190.
S. Terada et al. / Psychiatry Research: Neuroimaging 221 (2014)
8691 91
Depressive symptoms and regional cerebral blood flow in
Alzheimer's
diseaseIntroductionMethodsSubjectsInstrumentsEthicsBrain perfusion
SPECT imagingData analysisStatistical analysis
ResultsDemographic characteristicsrCBF
DiscussionLimitationsAcknowledgmentsReferences