-
7/30/2019 Dermatitis Dr Citra 260907
1/56
DERMATITIS -Eczema
Dr. Citra Cahyarini, SpKK
Department of dermatovenereology
Faculty of medicine YARSI University
-
7/30/2019 Dermatitis Dr Citra 260907
2/56
DERMATITIS -Eczema A common type of inflamation of skin
( epidermo- dermatitis ) which is not caused by micro-organism.
Itching is the most symptom
Some types appear to be due to as yet unidentifiedconstitutional
abnormalities, while others are moreobviously the result of some
external set of circumstance
Constitutional : eg Atopic dermatitis
External : eg Contact dermatitis
-
7/30/2019 Dermatitis Dr Citra 260907
3/56
Eflorescense of Dermatitis-Eczema
ErythemPapuleVesiclePustule
OozingCrust
Squama
-
7/30/2019 Dermatitis Dr Citra 260907
4/56
Several types of Derm- ecz
Atopic dermatitis
Contact dermatitis
Seborrhoic dermatitis Statis dermatitis
Neurodermatitis
Nummular eczema
Dishidrosis
Infective Eczematoid Dermatitis
-
7/30/2019 Dermatitis Dr Citra 260907
5/56
Atopic dermatitis/ EczemaDef :
Acute, subacute, or chronic relapsing skin
disorder that usually begins in infancy and ischaracterized
principally by dry skin and
pruritus.
Often associated with personal or family
history of atopy such as allergic rhinitis,
asthma, and atopic dermatitis (AD)
-
7/30/2019 Dermatitis Dr Citra 260907
6/56
A.Dmay divided into three stages, namely : Infantile ( 2 months
2 years) Childhood ( 2 years 10 years) Adult
Pathogenesis : ???
Complex interaction of skin barrier, genetic,environmental,
pharmacologic and immunologic factors
-
7/30/2019 Dermatitis Dr Citra 260907
7/56
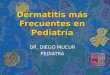
Infantile
Usually begins as an itchy erythema of cheeks followedby
development of vesicle, rupture and produce moistcrusted areas
The eruptions may rapidly extend to other parts of thebody,
chiefly the scalp, the neck, the forehead, the wristand the
extremities
The buttocks and diaper area are often involved
The eruption may become generalized with erythroderma
-
7/30/2019 Dermatitis Dr Citra 260907
8/56
Infantil AD
-
7/30/2019 Dermatitis Dr Citra 260907
9/56
Childhood AD
The lesion to be less exudative, drier, and more papular
The classic locations are the antecubital, and the
poplitealspaces, the wrist, eyelids, and the face and in collarette
about
the neck
The other area, however, are frequently affected
Itching
There is a decrease in the frequency of sensitization to
egg,wheat and milk, but an increase in sensitization to
nonigestedsubstances, particulary wool, cat hair, dog hair, and
pollens
-
7/30/2019 Dermatitis Dr Citra 260907
10/56
Childhood AD
-
7/30/2019 Dermatitis Dr Citra 260907
11/56
Adolescent and adult AD
Usually the eruption involves the antecubital and
poplitealfossae, the front and sides of the neck, the forehead
andthe are about the eyes
Hands dermatitis occurs more frequently in atopicindividuals,
and eczematous lessions of the dorsum areusual
Pruritus : paroxysm, nocturnal, triggered by acute emotional
stress Trigger factors : rough clothing, wool irritation, foods
or
tension.
-
7/30/2019 Dermatitis Dr Citra 260907
12/56
Adolescent and Adult AD
-
7/30/2019 Dermatitis Dr Citra 260907
13/56
Associated features
Cutaneous stigmata : Dennie-Morgan fold, Keratosis pilaris,
and Hertoghes sign
Vascular stigmata : White dermographism
Personality traits : Nervous tension
Ophthamologic abnormalities : cataracts, keratoconus.
-
7/30/2019 Dermatitis Dr Citra 260907
14/56
Susceptibility to infection :
S.aureus, generalized Herpes simplex or vaccinia virusinfections
to produce Kaposis varicelliform eruption
Immunology : elevated serum IgE, decreased T-supressorcells,
decreased chemotaxis and activations of PMNleucocyte.
-
7/30/2019 Dermatitis Dr Citra 260907
15/56
Diagnosis
Hanifin & Rajka , Svenson, SCORAD criterias
Hanifin & Rajka criteria :Major criteria
1. Pruritus
2. Typical morphology and distribution
3. Tendency toward chronics or chronically relapsing
dermatitis4. Personal or family history of atopic diseases (asthma,
allergic
rhinitis, AD)
-
7/30/2019 Dermatitis Dr Citra 260907
16/56
Minor criteria :
1. Xerosis / ichthyosis/ hyperlinear palms
2. Pityriasis alba
3. Keratosis pilaris4. Facial pallor / infraorbital
darkening
5. Elevated serum IgE
6. Keratoconus
7. Tendency to non spesific hand eczema8. Tendency to repeat
cutaneous infections
-
7/30/2019 Dermatitis Dr Citra 260907
17/56
Differential diagnosis
Nummular Dermatitis
Seborrhoic Dermatitis
Contact Dermatitis
Psoriasis
Scabies
-
7/30/2019 Dermatitis Dr Citra 260907
18/56
General management
1. In infancy and childhood
a. It should be avoided :
External irritation
Sudden change of temperature, excessivebathing, insufficient
cleanless especially in thediaper region, local infections
b. Food elimination ( with special attention)
-
7/30/2019 Dermatitis Dr Citra 260907
19/56
b. Antihistamin systemically
c. Olive oil on absorbent cotton may used withgentle patting for
cleansing to avoide rubbing the
affected patrs. Particular attention should be giventhe genitals
and buttocks and the diapers shouldbe changed
d. Weak topical corticosteroid.
-
7/30/2019 Dermatitis Dr Citra 260907
20/56
2. In adults :
a. The emosional stress should be controlled
b. Avoid extremes cold and heat
c. Hydrated xerotic skin
d. Antihistamin
e. Topical steroid ( be ware of the potentiallity)
f. Antiobiotics ( if nedded)
-
7/30/2019 Dermatitis Dr Citra 260907
21/56
Contact Dermatitis (CD)
An exogenous dermatitis which develops as a reaction
of the skin to contact with a foreign substance / an
environmental agent, either a primary irritant ( IrritantCD) or
an allergen (allergic CD)
It may be affected by exposure to UV-light, resulting
into two variant reaction : Photoallergic & Phototoxic
CD
-
7/30/2019 Dermatitis Dr Citra 260907
22/56
A llerg ic Con tact Dermat i t is(ACD)
Occur in predisposed individual
Sensitization occurs within a week after contact with a
substance (allergen), but there are no visible skin changes
Subsequent contact with allergen, even in small amounts,
causes an dermatitis
Once established, sensitivity may persists for months,
years, or even a lifetime
-
7/30/2019 Dermatitis Dr Citra 260907
23/56
Symptom : intense pruritus
Physical exam
acute : erythema & edema
subacute : plaques of mild erythema,dry scales
chronic : plaque of lichenification
Lab : patch test (+)
-
7/30/2019 Dermatitis Dr Citra 260907
24/56
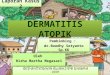
PATCH TEST
-
7/30/2019 Dermatitis Dr Citra 260907
25/56
Irr i tant Con tac t Dermatit is
Occure in any individual provided the chemical irritant
is applied in a potent enough concentration for a
sufficient length of time
Inflamation of the skin develops at the site of contact
There is non allergic mechanism involved, the damageresult from
direct chemical action
-
7/30/2019 Dermatitis Dr Citra 260907
26/56
Irritants:strong irritant severe inflamation at the first
contact
Weak irritants: less toxic substances which requirerepeated or
prolinged contact tocause inflamation (detergent, organicsolvents,
excessive exposure to water)
-
7/30/2019 Dermatitis Dr Citra 260907
27/56
Incidence:
The incidence of cases of ICD (each type)
depending mainly on the degree of exposure andthe causative
agent
In patients with atopic dermatitis there is a
relatively high incidence of ICD
-
7/30/2019 Dermatitis Dr Citra 260907
28/56
acute ICD
Symptom :
- subjective : burning, stinging, smarting
Physical exam :- < 24 h
- erythema vesiculation
* acute : sharply demarcated erythema &superficial edema
vesicles/ blisters
-
7/30/2019 Dermatitis Dr Citra 260907
29/56
chronic ICD
Cumulative ICD: slowly after repeated additiveexposure to mild
irritan
Symptom : stinging & itching, fissure pain
Physical exam :
dryness chapping erythema- hyperkeratosis & scaling fissure
&
crusting
-
7/30/2019 Dermatitis Dr Citra 260907
30/56
Treatment
Preventive :
Once the causative agent has been identified, further
contact should be avoided
Topical therapy :
in acute state : wet dressing : Burowi solution 1/20 1/40,
Permanganate 1/10.000, followed by topical steroid.
in chronic state : moderate topical steroid
Systemic therapy :Antihistamin (severe pruritus) and steroid
(severe /
extensive eruption
-
7/30/2019 Dermatitis Dr Citra 260907
31/56
Contact Dermatitis
-
7/30/2019 Dermatitis Dr Citra 260907
32/56
-
7/30/2019 Dermatitis Dr Citra 260907
33/56
Seborrhoic dermatitis
Two distinct subset of patients :
* The Infantile form *
Characterized by large yellowish scale mainly on the scalp,face,
axilla and napkin rash
May cause confusion with Infantile Atopic Dermatitis
No link between the infantile and adult form
No pruritus eat & sleep well
-
7/30/2019 Dermatitis Dr Citra 260907
34/56
Infantil form Seborrhoeic Dermatitis
-
7/30/2019 Dermatitis Dr Citra 260907
35/56
Cradle Cap
-
7/30/2019 Dermatitis Dr Citra 260907
36/56
* The adult form *
Affect the face, scalp, anterior chest, axilla, sub
mammary fold, groins, external ear
Facial lesion, particularly in the nasolabial fold, in
men, maybe very persistent the scalp is frequently involved
presenting
complaint, esp severe and persistent dandruff
Eyebrow/ eyelid
stickness of the eyelid inearly morning
-
7/30/2019 Dermatitis Dr Citra 260907
37/56
Differential diagnosis :Contact dermatitis, psoriasis and
Pityriasis versicolor
Treatment : Tends to recure whatever treatment is chosen
Topical : imidazol antifungal ketokonazol(cream/shampoo) , weak
potency topical steroid
-
7/30/2019 Dermatitis Dr Citra 260907
38/56
Adult form Seborrhoeic Dermatitis
-
7/30/2019 Dermatitis Dr Citra 260907
39/56
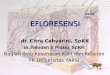
Stasis dermatitis
dermatitis on the lower legs, commonly seen in associationwith
venous insufficiency
many cases seen in obese, female patients have a degree ofvenous
insufficiency
inner aspects of boths lower legs above and around the
medialmalleous are chiefly involved
the skin is shinny, atrophic and large numbers of small
bloodvessels clearly visible, purpura, pigmentation (due
tohaemosiderin)
pruritus may be severe and cause scratch marks which are
slow to heal
Treatment :
treatment of underlying varicose veins, topical steroid
(weak)
be ware of side effects atrophy
-
7/30/2019 Dermatitis Dr Citra 260907
40/56
Stasis Dermatitis
-
7/30/2019 Dermatitis Dr Citra 260907
41/56
Neurodermatitis
(liken simplex chronicus) a well demarcated are of chronic
lichenified dermatitis which is
not due to either external irritants or identified allergens
In predisposed persons, the lesions are induced by continual
scratching or rubbing of a localized area of itching skin stress
/ emotional disturbance pruritic stimulus scratch
itch-scratch-itch cycle stimulate a reactive
hyperplasia,recognized clinically as lichenification
clinically, neurodermatitis are seen as a well-circumscribe,
lichenified, slightly elevated plaque, seen on the nape of
neck,forearm, or the legs
Treatment :Reduce pruritus, topical steroid (ointment/ intra
lesion)
-
7/30/2019 Dermatitis Dr Citra 260907
42/56
Neurodermatitis
-
7/30/2019 Dermatitis Dr Citra 260907
43/56
Dishydrotic
(eczema dishydrosticum)
a very characteristic pattern of intensely itchy vesiclesof the
skin of the hands and occasionally the feet andalso the side of
finger
Deep-seated vesicle ; often easier to feel than to see
The cause is not understood ( contact dermatitis /stress? )
Treatment ; systemic antihistamins ( control the needto scratch)
prevent secondary infection, potenttopical steroid ( a short time)
; for the moist lesioncalamine lot.
-
7/30/2019 Dermatitis Dr Citra 260907
44/56
Dishydrotic
-
7/30/2019 Dermatitis Dr Citra 260907
45/56
Nummular or Discoid dermatitis
a chronic, recurrent pattern of dermatitis with
discretecoin-shape lesions tending to to involve the limbs
Usually affects adults (many of whom will have a pasthistory of
AD) ; The aetiology is unknown
Clinically : subacute with erythema, edema,vesiculation; the
surface may be moist and appearinfected bacterial eczema
Pruritus is variable
Treatment : topical steroid + antibiotic
-
7/30/2019 Dermatitis Dr Citra 260907
46/56
Nummular or Discoid Dermatitis
-
7/30/2019 Dermatitis Dr Citra 260907
47/56
INFECTIVE ECZEMATOID DERMATITIS IED is exogen in nature, can be
defined as fluid/ exudate
which originates from inflammation or disorders such as:
OMP, sinusitis, chronic ulcers, etc
IED is thought as autosensitisation dermatitis which occurs
from skins sensitivity toward chemical substances
originating from tissues/ bacteria in the bodys own exudate
-
7/30/2019 Dermatitis Dr Citra 260907
48/56
Clinical appearances : Erythema & exudation
In a dry state, there is crust. If crust is peeled, we would
see erythema & often pustules on the edgesExamples :
The earlobes of children suffering from OMP.
The area around the nose of maxilaris sinusitis sufferers
-
7/30/2019 Dermatitis Dr Citra 260907
49/56
Therapy :
Rivanol 1/1000, Betadine dressing
When cleared Hidrocortisone 1 % or combination with
antibiotic
-
7/30/2019 Dermatitis Dr Citra 260907
50/56
Infective Eczematoid Dermatitis
-
7/30/2019 Dermatitis Dr Citra 260907
51/56
URTICARIA & AGIOEDEMA Def:
*URTICARIA
is compoused of wheals (transient edematous papules
&plaques, usually pruritic and due to edema of papilary
body). The wheals are superficial, well defined.
*ANGIODEMA
is a large edematous area that involves the dermis and
subcutaneous tissue, is deep and ill defined
-
7/30/2019 Dermatitis Dr Citra 260907
52/56
Therapy
Antihistamin : H1, H1 + H2
Systemic corticosteroid
Adrenalin inj subcutis/ ephedrin tab
-
7/30/2019 Dermatitis Dr Citra 260907
53/56
urticaria
angioedema
-
7/30/2019 Dermatitis Dr Citra 260907
54/56
VasculitisA heterogeneous group of clinical synd
characterized by inflammation of blood vessels
The clinical picture is essensially dependent of size
and extent of vessel involvement purpuraTest : diaskopiTherapy
Systemic corticosteroid
-
7/30/2019 Dermatitis Dr Citra 260907
55/56
-
7/30/2019 Dermatitis Dr Citra 260907
56/56
CC, Sept- 2007