Embed Size (px)
Citation preview

Desafíos del sistema de salud chileno
Thomas Leisewitz
24 Octubre 2013

Elementos para un diagnóstico

Diagnóstico
① Macro indicadores sanitarios buenos, aunque en riesgo② Gasto en salud creciente, equivalente en la actualidad al mundo privado③ Pérdida de productividad④ Excesivo poder del Estado (asegurador, prestador, regulador)⑤ Insatisfacción de los pacientes, y judicialización de la salud
Thomas Leisewitz – 2013 | 3

Problema de Salud Prevalencia (%) ENS 2003
Prevalencia (%)ENS 2009-2010
Tabaquismo (fumador actual) 42 40.6
Sobrepeso 37,8 39,3
Obesidad 23,2 25,1
Diabetes mellitus 6,3 9,4
Sedentarismo 89,4 88,6
Síntomas depresivos en últimoaño 17,5 17,2
Diagnóstico | Buenos macro-indicadores de salud, pero…
Fuente: Encuesta Nacional de Salud, MINSAL, 2011 Thomas Leisewitz – 2013 | 4

Diagnóstico | Gasto creciente
Thomas Leisewitz – 2013 | 5Fuente: DIPRES, 2013. Elaboración propia

Diagnóstico | Gasto creciente
Thomas Leisewitz – 2013 | 6Fuente: OECD, 2010

Diagnóstico | Desacople en el gasto
Thomas Leisewitz – 2013 | 7Fuente: OECD, 2013
0,0%1,0%2,0%3,0%4,0%5,0%6,0%7,0%
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Average OECD health expenditure growth rates in real terms, 2000 to 2011, public and total
Total Health Expenditure Public health expenditureSource: OECD Health Data

Diagnóstico | Gasto en salud sigue creciendo en Chile
Thomas Leisewitz – 2013 | 8Fuente: OECD, 2013
-15%
-10%
-5%
0%
5%
10%
15%
Greec
e Ire
land
Icelan
d Esto
nia
Portug
al Den
mark
Spain
United
King
dom
Sloven
ia
Czech
Rep
ublic
Ita
ly Aus
tria
OECD Fr
ance
Aus
tralia
Mex
ico
Nether
lands
Pola
nd
Belgium
Ger
many
Norway
New Z
ealan
d Can
ada
Finlan
d
United
Stat
es
Hunga
ry Switz
erlan
d
Slovak
Rep
ublic
Swed
en
Israe
l Ja
pan
Chile
Korea
Average annual growth in health spending across OECD countries in real terms, 2000-2011
2000-09 2009-11
Note: Growth rates for Australia, Denmark, Japan, Mexico and Slovak Republic refer to 2009-10 instead of 2009-11 Growth rates for 2009-11 are not available for Luxembourg, and Turkey. Growth rates for Chile calculated using the Consumer Price Index (CPI).
Source: OECD Health Data 2013.

Diagnóstico | La crisis afecta principalmente a la prevención
Thomas Leisewitz – 2013 | 9Fuente: OECD, 2013

Diagnóstico | Gasto per capita, FONASA versus ISAPRE
Thomas Leisewitz – 2013 | 10Fuente: Esrimación propia, en base a datos DIPRES y Superint.endencia de Salud. ISAPRES cerradas usando el 5,5% del 7% de cotización legal.
Año 2012 FONASA ISAPRES
Beneficiarios 13.377.082 2.885.331 Gasto mensual per capita en prestaciones 24.135$ 26.259$ 92%

Diagnóstico | Productividad a la baja
Thomas Leisewitz – 2013 | 11Fuente: El Mercurio, 22 octubre 2013

Diagnóstico | Productividad a la baja (2)
Thomas Leisewitz – 2013 | 12Fuente: Rodrigo Castro, Libertad y Desarrollo, 2005

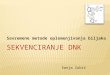
Diagnóstico | “Flat-of-the-curve medicine”?
AUS
AUT
BEL
BRA
CAN
CHL
CHN
CZE
DNK
EST
FIN
FRA
DEU
GRC
HUN
ISL
IND
IDN
IRL
ISR
ITA JPN
KOR
LUX
MEX
NLD NZL NOR
POL
PRT
RUS
SVK
SVN
ESP
SUE CHE
TUR
GBR USA
R² = 0.69 64
68
72
76
80
84
0 2000 4000 6000 8000
Life expectancy in years
Health spending per capita (USD PPP)
Fuente: OECD, 2012 Thomas Leisewitz – 2013 | 13

Diagnóstico | “Flat-of-the-curve medicine”?
• Evidentemente, queda mucho pormejorar
Thomas Leisewitz – 2013 | 14Fuente: OECD, 2013
AustraliaAustriaBelgiumCanadaChileCzech RepublicDenmarkEstoniaFinlandFranceGermanyGreeceHungaryIcelandIrelandIsraelItalyJapanKoreaLuxembourgMexicoNetherlandsNew ZealandNorwayPolandPortugalSlovak RepublicSloveniaSpainSwedenSwitzerlandTurkeyUnited KingdomUnited StatesOECD AVERAGE
Average length of stayMyocardial Infarctio
2011 (or nearest y
Days5.5 8.1 7.2 5.9 7.8 6.8 3.9 9.1 8.1 6.2
10.6 7.0 8.2 6.8 8.0 5.7 7.7
..10.4 5.9 7.2 6.2 8.9 4.0 6.4 7.9 4.8 7.7 7.8 4.7 6.9 4.0 7.8 5.4 6.9
y, for Acuteon (AMI)year)

Diagnóstico | Mercado privado de la Salud poco competitivo
• Excesivo rol del Estado, ¿causa o efecto?
– asegurador
– prestador
• Incertidumbre regulatoria
– Judicialización creciente
– Cambios normativos en discusión (por ejemplo, PGS)
Thomas Leisewitz – 2013 | 15

Diagnóstico | Insatisfacción creciente
Thomas Leisewitz – 2013 | 16Fuente: Superintendencia de Salud, 2012

Diagnóstico | Insatisfacción creciente
Thomas Leisewitz – 2013 | 17Fuente: Superintendencia de Salud, 2012

3 desafíos

Después de 25 años, el sistemarequiere un rediseño.

Distintos modelos: “No silver bullets”
Fuente: OECD (2010), Health Care Systems: Efficiency and Policy Settings, OECD Publishing Thomas Leisewitz – 2013 | 20

Todos los sistemas son igualmente buenos (o igualmente malos…)
“Efficiency estimates vary more withincountry groups sharing similarinstitutional characteristics thanbetween groups. This suggests thatno broad type of health care systemperforms systematically better thananother in improving the populationhealth status in a cost-effectivemanner. Still, within-groupcomparisons allow the spotting ofstrengths and weaknesses for eachcountry and identifying areas whereachieving greater consistency inpolicy settings could yield efficiencygains.”
Fuente: OECD (2010), Health Care Systems: Efficiency and Policy Settings, OECD Publishing Thomas Leisewitz – 2013 | 21

Salud en el mundo del “segundo mejor”
• Mercado: no alcanzanaturalmente los puntos óptimosde eficiencia
• ¿Rol del Estado? Ojo con el Transantiago...
Fuente: : Lipsey RG, Lancaster K. The General Theory of Second Best. The Review of Economic Studies. Vol. 24, No. 1 (1956 - 1957), pp. 11-32 Thomas Leisewitz – 2013 | 22

Fuente: Macinko J, Starfield B, Shi L. The contribution of primary care systems to health outcomes within Organization for Economic Cooperation and Development (OECD) countries, 1970-1998. Health Serv Res 2003; 38(3):831-865. Tomado de Starfield 06/02, 02-126
Rediseño | Empezar por la Atención Primaria
*Predicted PYLL (both genders) estimated by fixed effects, using pooled cross-sectional time series design. Analysis controlled for GDP, percent elderly, doctors/capita, average income (ppp), alcohol and tobacco use. R2(within)=0.77.Year
Low PC Countries*High PC Countries*All Countries*
1970 1980 1990 20000
5000
10000
PYLL
Thomas Leisewitz – 2013 | 23
Primary Care Score and Premature Mortality in 18 OECD Countries

Rediseño | Colocar al paciente al centro
• Implica reconocer que el paciente, su familia y la comunidad debenparticipar de los procesos de decisión respecto a los servicios de salud que recibirán
• Integrar red de prestadores al servicio de los pacientes, con flexibilidad
• Fomentar que el usuario “vote con los pies”
• Estudiar la incorporación de copagos (contingente a los ingresos) diferenciado según el tipo de servicios.
Thomas Leisewitz – 2013 | 24

Rediseño | Dividir para reinar
La oferta actual puede desagregarseen 3 grupos:
1. Prevención Primaria– Screening, controles sanos, vacunas,
supervisión del embarazo, EMP, etc.
2. Prevención Secundaria-Terciaria:– Programas de crónicos:
cardiovascular, respiratorio, etc.
3. Morbilidad aguda: – Compiten todos los niveles de la red
Prevención Primaria
Crónicos
Morbilidad
Thomas Leisewitz – 2013 | 25

Rediseño | Algunos elementos
• Desdibujamiento de los límites entre los niveles primario, secundario y terciario
• El nivel primario se transforma en el articulador de los prestadores, con accesoamplio a servicios de los otros niveles.
• Además de los médicos generales y familiares, se incorporan otrosespecialistas médicos “generalistas” a los equipos de APS: internistas, geriatras, pediatras, gineco-obstetras.
• Se re-ordenan las poblaciones, de manera de generar polos de excelencia en torno a necesidades de los pacientes. Por ejemplo: pacientes crónicos, pacientes en control sano (embarazadas, niños, etc.).
• La prevención y promoción salen del ámbito exclusivamente asistencial, haciael educacional, laboral y comunitario
Thomas Leisewitz – 2013 | 26

Compra de servicios del NivelSecundario
• Se podría permitir comprar exámenes y consultas a diferentes establecimientos públicos (y privados), desde la Atención Primaria.
• Requiere poner la plata en el nivel primario, y comprar “hacia arriba”
Competencia en Morbilidad
• Se podría permitir competir por el pago por atención de morbilidad entre centros y entre el nivel primario y terciario (SAPUs versus SUH)
Thomas Leisewitz –
Rediseño | 2 ejemplos concretos

Rediseño | Incentivos
• Estructura de incentivosMagnitud de la recompensa económica o premio Quién debe soportar el riesgo
• Estructura de incentivos modifica la conducta de personas y organizaciones
• La conducta de las personas y organizaciones tiene consecuencias reales sobre la calidad y el volumen de los servicios de salud (y el gasto en salud).
Thomas Leisewitz – 2013 | 28

Rediseño | Alinear mecanismos de pago
Prevención Primaria
Crónicos
Morbilidad
Per-capita + P4P
Pago por diagnóstico + P4P
Pago por diagnóstico; o Per-capita + FFS
Thomas Leisewitz – 2013 | 29

Rediseño | Alinear mecanismos de pago (2)
Thomas Leisewitz – 2013 | 30
Prevención Primaria
Crónicos
Morbilidad
Per-capita + P4P
Pago por diagnóstico+ P4P
Pago por diagnóstico; o per-capita + FFS
Salarios + bonosde desempeño
FFS

Hay que revisar el “mandato” del seguro

Plan de salud
Thomas Leisewitz – 2013 | 32
GES
MAI
MLE
GES
CAEC
MLE
COMPLE-MENTARIO
FONASA ISAPRE
Man
dato
rioVo
lunt
ario

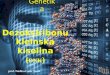
Sistemas de salud | 2 problemas centrales a resolver
¿Qué hacer con las diferencias de costo esperado del gasto en salud de una persona a lo largo de su vida y entre personas?
¿Cómo enfrentar el incremento de costos de la salud?
10.9 8.6
7.5 7.3
6.9 6.3
6.1 5.7
5.2 4.8 4.8
4.4 4.0 4.0 4.0 4.0 3.9
3.7 3.4 3.3 3.3
3.1 2.8 2.8
2.4 2.4
2.2 2.2
2.0 2.0
1.6 1.6 1.5 1.5
0.7
0 4 8 12
Slovak Republic Korea
Estonia Poland Greece Turkey Ireland
Czech Republic Chile
New Zealand United Kingdom
Netherlands Belgium Finland
Spain OECD
Slovenia Canada Sweden
Denmark United States
Mexico Australia Hungary
Japan Norway Austria France
Germany Switzerland
Iceland Italy
Israel Portugal
Luxembourg
Annual average growth rate (%)
Fuente: (1) OIT / STEP 2002, en WB, 2006. Health Financing Revisited. (2) OECD 2011. Annual average growth rate in health expenditure per capita in real terms, 2000-09. Health at a Glance 2011. Thomas Leisewitz – 2013 | 33

Seguro | Reducir el mandato a
Thomas Leisewitz – 2013 | 34
• Un seguro “pobre, pero honrado”, menor al mandato actual
– Amplia cobertura a prevención primaria y secundaria (ojo con Atención Primaria
– Seguro catastrófico grande, que cubre eventos hospitalarios y gastos ambulatorios (incluyo medicamentos), con un deducible importante.
– Cobertura GES
• Un seguro muy bueno para eventos infrecuentes y no prevenibles)
– Uso más importante de copagos y deducibles para eventos ambulatorios y más discrecionales.
– Cuentas de ahorro para la salud para cubrir esos copagos.

Seguro | Temas adicionales
• Seguros suplementarios: muchos, distintos, voluntarios
• Pueden usarse parcialmente como seguro complementario para cubrir copagos y deducibles del seguro mandatorio.
• Hay que revisar potencial “sobre-aseguramiento”, evitando duplicación de coberturas
• Subsidio del Estado: no hay razón para que esté atrapado en el seguro público.
Thomas Leisewitz – 2013 | 35

Podemos incorporar elementos de “inteligencia sanitaria”

“No Toyotas in Healthcare”
• La salud sufre, como describió el profesor William Baumol, del “Cost Disease”, la enfermedad de los costos.
• A diferencia de otras “industrias”, el problema de las nuevas tecnologíassanitarias es que en vez de bajar los costos, generalmente los aumentan.
No ToyotasIn HealthCare:W hy Medical CareHasNot Evolved ToMeet Patients’ NeedsUntil payment policies reward quality improvement, providers willnot place it at thecore of their business strategy.
by Molly Joel Coye
ABSTRACT: The incentives and structure of health care in the United Statesproduce exactly what we should expect in the qualityof care for chronic disease:highly variable patterns of care and widespread failure to implement evidence-based best practices. The persistent inability of providers to improve patterns ofpractice is due in part to the lack of a “business case for quality.” Providerscannot anticipate that quality improvements will result in higher prices, in-creased volume, or decreased costs. However, signs of a business case forquality are emerging, fueled by cost pressures, the increased availability ofdata, informed consumers, and public- and private-sector purchaser initiatives.
The st r uct ur es, i ncent i ves, and f or ces at work in theU.S. health system produceexactly what weshould expect inthequality of carefor chronic disease: highly variablepatterns
of care, widespread failure to implement recognized best practicesand standards of care, and the persistent inability of provider sys-tems to achieve substantive changes in patterns of practice. More-over, after more than two decades of effort to improve clinical caremanagement and to promote the adoption of evidence-based stan-dards, these variations persist. As noted in the recent Institute ofMedicine(IOM) report,ToErr IsHuman, “Thereisabundant evidencethat serious and extensive quality problems exist throughoutAmerican medicineresulting in harm to many Americans.”
Thehealth sector hasbeen exceptionally untouched by thetrans-forming principles of quality management that revolut ionizedmanufacturing and serviceindustries in the1980s.For thosesectors,quality management became acoretask of executive leadership and
Molly Coyeischief executiveofficer of theHealthTechnology Center inSanFrancisco.Aphysician,shehasservedasdirector of theCaliforniaDepartment of HealthServicesandascommissioner of healthfor theStateof NewJersey.
44 CARE &PATIENTS’NEEDS
M e d i c i n e & C h r o n i c I l l n e s s
Thomas Leisewitz – 2013 | 37

Inteligencia sanitaria | Introducir el “Value-for-money”
• Nueva medida: “value-for-money”, entendida como el beneficio que agrega en términos de salud por cadapeso gastado (costoefectividad)
• Implica medir costos y resultados, de manerasistemática, y tomardecisiones acorde a ello.
Thomas Leisewitz – 2013 | 38Fuente: Porter ME, Lee TH. The big idea: The strategy that will fix Health Care. Harvard Business Review, 2013

Inteligencia sanitaria | “Value-for-money”
Thomas Leisewitz – 2013 | 39

Inteligencia sanitaria | Evaluaciones económicas
• “(…) an evidence-based system of pricing and reimbursement for drugs, considering societal willingness-to-pay, is a reasonable policy objective to pursue.”
• Implica: formalizarevaluaciones de tecnologías; y restricciones al libre accesoa ellas
Thomas Leisewitz – 2013 | 40Fuente: Drummond M. Twenty Years of Using Economic Evaluations for Reimbursement Decisions. What Have We
Achieved? CHE Discussion Papers, University of York. 2012

Inteligencia sanitaria | Introducir el “Value-for-money”
• Mezclar instrumentos de pago que permitan poner incentivos acordes a los objetivos
Prevención: per capita, pago por desempeño (P4P)
incremento de prestaciones curativas: pago por prestación (fee for service, FFS)
aumento de calidad: pago por desempeño (P4P)
fomento a la eficiencia (pago por caso, diagnóstico)
Thomas Leisewitz – 2013 | 41

Inteligencia sanitaria | Introducir el “Value-for-money”
• Mezclar instrumentos de pago que permitan poner incentivos acordes a los objetivos
Prevención: per capita, pago por desempeño (P4P)
incremento de prestaciones curativas: pago por prestación (fee for service, FFS)
aumento de calidad: pago por desempeño (P4P)
fomento a la eficiencia (pago por caso, diagnóstico)
Thomas Leisewitz – 2013 | 42

Acceso a nuevas tecnologías | 4 caminos
Volume-price agreements Cap on budget impactCoverage with evidence development Risk-sharing agreements
Source: OECD, 2010.

The way forward | Recommendation
• Rationalize access to new drugs, introducing formal HTA process, at least for public affiliates. That way could at the same time improve the value-for- money achieved, and improve access to better treatments.
• FONASA should avoid decentralized buying definition at hospitals, but could introduce two new mechanisms for covering innovative drugs: Coverage with evidence development, and Risk-sharing agreements.
• Private insurance may be spending too much in innovative medicines. They should be beneficiated also with formal HTA introduction.

Desafíos del sistema de salud chileno
Thomas Leisewitz
24 Octubre 2013

El autor es responsable de toda la información y opiniones presentadas, y no representa necesariamente a lasinstituciones con las cuales está vinculado.