Embed Size (px)
Citation preview
BRIEF REPORT
Does OROS*-methylphenidate improve core symptoms and deficits in executive function? Results of an open-label trial in adults with attention deficit hyperactivity disorderAngelo Fallu a, Caroline richard a, rosanna prinzo b and Carin binder b
a Clinique Woodward, Sherbrooke, Quebec, Canadab Janssen-Ortho Inc., Toronto, Ontario, Canada
Address for correspondence: Angelo Fallu, MD, Clinique Woodward, 685 rue Woodward, Sherbrooke, Quebec, J1G 1W4, Canada. Tel.: +1-819-565-1441; Fax: +1-819-565-2246; email: [email protected]
Key words: Adult attention deficit hyperactivity disorder – Effectiveness – Executive function – OROS-methylphenidate – Safety
0300-7995
doi:10.1185/030079906X154132
All rights reserved: reproduction in whole or part not permitted
CurrENt MEdiCAl rESEArCH ANd OpiNiON®
VOL. 22, NO. 12, 2006, 2557–2566
© 2006 librApHArM liMitEd
Paper 3588 2557
Objective: This pilot, uncontrolled, open-label study evaluated the safety/tolerability and potential effectiveness of OROS-methylphenidate (OROS-MPH) in adult attention deficit hyperactivity disorder (ADHD).
Methods: Adults with DSM-IV-defined ADHD were enrolled in this 38-day study. Retrospective childhood diagnosis was made using the Wender Utah Rating Scale. Eligible patients required a baseline Conners Adult ADHD Rating Scale (CAARS) score ≥24, Clinical Global Impression of Severity (CGI-S) score ≥4 (at least moderate illness), and Montgomery–Asberg Depression Rating Scale (MADRS) score ≤ 16. Safety/tolerability measurements included adverse event reporting, vital signs, electrocardiograms (ECGs), weight, physical examination. Primary effectiveness evaluated changes in CAARS scores. Secondary effectiveness parameters included executive function.
Results: Thirty-two patients formed the safety analysis; however, 30 comprised the effectiveness analysis since two patients did not meet diagnostic inclusion criteria. No serious adverse events were reported and there were no early withdrawals due to adverse events. There
were no clinically significant changes in endpoint ECGs, physical examination, or blood pressure. Mean pulse rate increased by 5.9 beats/min( p = 0.003) and mean body weight decreased by 2.2 kg at endpoint ( p < 0.0001). Total CAARS scores decreased significantly at endpoint as well as the inattention ( p < 0.0001) and hyperactivity/impulsivity symptom subscales ( p < 0.0001) separately. Statistically significant improvements were observed in executive function and all other secondary measures, including the CAARS self report, CGI-S/CGI-I, Subject Satisfaction with treatment and the Sheehan Disability Scale (SDS). Mean dose of OROS-MPH = 52.3 ± 14.0 mg. Modal dose = 54 mg. Study limitations include: the lack of placebo control in the study design leading to potential observer bias, the exclusion of adults with unstable psychiatric and other medical conditions which is less reflective of clinical practice, and the short study duration.
Conclusions: This uncontrolled, open-label trial suggests that OROS-MPH is well tolerated, providing core symptom control with the added benefit of improving executive function. However, future larger, randomized, controlled trials are required.
A B S T R A C T
* OROS is a registered trade name of Alza Corporation, Mountain View, CA, USA
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/2
6/14
For
pers
onal
use
onl
y.

2558 OROS-methylphenidate for ADHD © 2006 librApHArM ltd – Curr Med res Opin 2006; 22(12)
Introduction
Attention deficit hyperactivity disorder (ADHD) has long been known as a childhood disorder characterized by inattention, impulsivity, and motor restlessness, affecting 8–10% of youngsters1. It has only been in the last 30 years that the persistence of ADHD into adulthood has officially been recognized2. As many as two-thirds of children diagnosed with ADHD continue to exhibit ADHD symptoms into adult life3. It is now estimated that 4.4%4 of adults have ADHD, although many remain undiagnosed and untreated5. Adult ADHD is more difficult to diagnose than childhood ADHD because symptoms like overt hyperactivity are less obvious and can also occur as unspecific symptoms of other disorders like bipolar disorder, depression, anxiety or personality disorder among others. As a result, diagnosis requires an accurate, retrospective diagnosis of childhood onset ADHD, which at times is difficult to assess, while differentiating presenting symptoms from other psychiatric disorders6. Stimulant therapy remains the mainstay of pharmacological treatment for children with ADHD. A recent meta-analysis reported strong evidence for the effectiveness of methylphenidate in treating adult ADHD, although relatively few studies have been conducted in this population7. In a recent double-blind, randomized, 6-week, placebo-controlled study, Biederman and colleagues found that treatment with Osmotic Release Oral System (OROS*)-methylphenidate (MPH) at daily doses above 72 mg was effective and well tolerated, with small but statistically significant increases in blood pressure and heart rate8. An open-label study demonstrated similar benefits with OROS-MPH treat-ment in 36 adults with late-onset ADHD/ADHD NOS (initial symptoms occurring later than the required 7 years of age)9.
Previous articles have established well-replicated findings in the neuropsychology of ADHD. This body of work has proposed that symptoms of ADHD arise from a primary deficit in specific domains of executive function, defined as response inhibition, working memory or general weakness in executive control10. This hypothesis is based on the observation that lesions in the prefrontal cortex can produce hyperactivity, distractibility or impulsivity in addition to deficits in executive function. In Seidman’s recent review6, he notes that executive dysfunctions are correlates of ADHD regardless of gender or age.
Despite executive dysfunction becoming the focus of current theories concerning the neuropsychological basis of ADHD, limited research has been conducted to determine neuropsychological functioning in ADHD,
especially in adults over 40 years of age6 and in effects of methylphenidate treatment in these areas.
This pilot study was designed to evaluate the safety, tolerability and potential effectiveness of OROS-MPH for treating adults with ADHD (age 18–65 years) and to assess treatment effect on executive function.
Patients and methodsSubjects
This single-centre, pilot study had no formal sample size calculation but planned to enroll approximately 30 adult subjects (18–65 years of age inclusive) with a diagnosis of ADHD according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition Text Revision (DSM-IV-TR) criteria11 obtained via structured clinical interview12. Retrospective childhood diagnosis was obtained using the Wender Utah Rating Scale13 (WURS) and patients had to have a baseline investigator-rated CAARS, short version ≥ 24, baseline CGI-S ≥ 4 (at least ‘moderate’ disease) and a baseline MADRS ≤ 16. ADHD was not diagnosed if the symptoms revealed during the structured interview were better accounted for by another primary psychiatric disorder (e.g., mood, anxiety, psychotic, personality disorders).
Subjects could not have been treated with any methylphenidate/non-methylphenidate or amphet-amine/non-amphetamine-containing medication within 4 weeks of the screening visit, nor could the subject (or his/her child, if applicable) be a known non-responder (when given a trial of MPH at adequate and recom-mended dose levels, as per manufacturer, would fail to exhibit any improvement of symptoms) to methyl-phenidate. Subjects with marked (i.e., limiting patient’s daily life and overpowering the features of the ADHD diagnosis) anxiety, tension, aggression, agitation, autism, Asperger’s syndrome, or a DSM-IV diagnosis of substance-use disorder (abuse/dependence) within 6 months prior to screening evaluation were excluded (except for nicotine and caffeine dependence), as were subjects with a history of ongoing seizure disorder, glaucoma, uncontrolled hypertension, angina pectoris, cardiac arrhythmias, severe gastrointestinal narrowing or the inability to swallow study medication.
Any psychiatric conditions deemed clinically unstable by the investigator upon completion of a structured interview, including but not limited to acute mood disorder, schizophrenia, bipolar disorder, acute obsessive–compulsive disorder (OCD), and anti-social personality disorder were excluded. Patients were only permitted to treat their ADHD with the study medication and no
* OROS is a registered trade name of Alza Corporation, Mountain View, CA, USA
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/2
6/14
For
pers
onal
use
onl
y.

© 2006 librApHArM ltd – Curr Med res Opin 2006; 22(12) OROS-methylphenidate for ADHD Fallu et al. 2559
new behavioral modification programs could be initiated nor existing ones changed. Use of other psychotropic medications used to treat co-morbidities (not ADHD) was permitted during the study, providing the dose of the medication had remained stable for a minimum of 4 weeks prior to trial entry and was expected to remain stable during the trial.
All patients were enrolled between March 2005 and October 2005 at a single community-based psychiatric practice in Sherbrooke, Quebec, Canada. The study was conducted in accordance with the Declaration of Helsinki and its subsequent revisions, and approved by Research Review Board Inc., Waterloo, Ontario, Canada. Written consent was obtained from each study participant prior to enrolment.
Study treatment
Once deemed eligible, subjects in this open-label study began treatment with OROS-MPH administered by mouth as a single 18-mg tablet daily for 3 days, then titrated up on day 4 to a 36-mg tablet daily for 7 days. Thereafter, depending on response, tolerability, and clinician’s judgment, the dose of OROS-MPH could continue to be titrated up, every 7 days thereafter, first to a 54-mg tablet daily and then to a maximum of 72 mg (2 × 36 mg tablets) once per day, in order to achieve the optimal dose for each subject. The titration period was to last a maximum of 3 weeks. In the latter 2 weeks of the 38-day trial, the subject was expected to stay on the optimal dose achieved during the first 3 weeks of the study. Medication was preferably taken in the morning, before 10:00 a.m.
Assessments
Study visits took place as follows: screening (day –7 to 0), baseline (day 0), day 3, day 10, day 17, day 24, and final visit (day 38). If possible, the same person was to complete the same assessment at all visits.
Safety measures
Safety and tolerability measures included physical examination, height, weight, ECGs, laboratory tests, vital signs including blood pressure and heart rate. Adverse events reported by the subject or noted by the clinician were collected and pregnancy testing in females of childbearing potential was performed.
primary effectiveness measure
The primary measure of effectiveness was based on scores from the investigator-rated Conners Adult ADHD Rating Scale (CAARS)14. This scale includes 18
items corresponding to the core DSM-IV symptoms for ADHD, consisting of two subscales measuring inattention and hyperactivity/impulsivity symptoms, respectively. Responses were rated on a 4-point scale as follows: 0 = not at all, never; 1 = just a little, once in a while; 2 = pretty much, often; 3 = very much, very frequently.
Secondary effectiveness measures
Secondary effectiveness measures included the following: Conners’ Adult ADHD Rating Scale – Self Report, Short Version (CAARS-S:S)14; Montgomery–Asberg Depression Rating Scale (MADRS)15; Stroop Color–Word Test16; Wechsler Adult Intelligence Scale 3rd Edition (WAIS-III) Working Memory Sub-Scale17; Controlled Oral Word Association Test (COWAT)18; Sheehan Disability Scale (SDS)19; Clinical Global Impression-Severity (CGI-S) and Clinical Global Impression-Improvement (CGI-I)20; and Patient Satisfaction with Treatment measured on a 5-point Likert Scale21. All executive function tests (Stroop, Working Memory Subscale, COWAT) were performed by a certified psychologist versed in the administration of these tests.
A post hoc analysis looking at symptomatic remission, as defined as a total score of ≤ 1 on each of the 18 items of the CAARS investigator-rated scale was also conducted.
Statistical methods
Safety, effectiveness and executive function endpoints were summarized by descriptive statistics. All subjects who took at least one dose of OROS-MPH were included in the safety analysis. The number and per-centage of subjects with treatment-emergent adverse events was calculated. Changes in vital signs, ECG, and physical examination, including body weight, were summarized.
All subjects who met eligibility criteria, took at least one dose of OROS-MPH and had both baseline and at least one post-baseline effectiveness assessment were included in the intent-to-treat effectiveness analysis. Descriptive statistics were provided for the changes in all effectiveness endpoints from baseline to each post-baseline visit. The primary analysis used the observed case and last observation carried forward method (LOCF). Change from baseline p-values were calculated using the t-test, except for the CGI scores which used the Wilcoxon signed-rank test.
Results
A total of 32 subjects were recruited into the study between March 2005 and October 2005 and comprised
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/2
6/14
For
pers
onal
use
onl
y.
2560 OROS-methylphenidate for ADHD © 2006 librApHArM ltd – Curr Med res Opin 2006; 22(12)
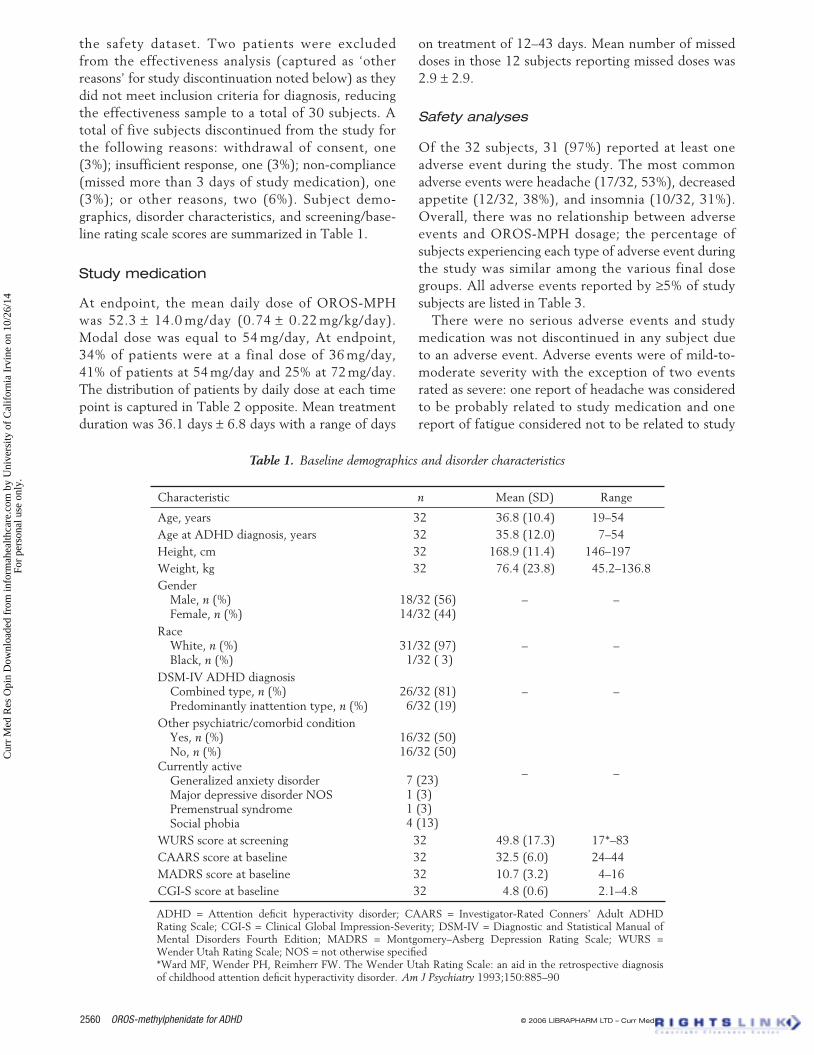
the safety dataset. Two patients were excluded from the effectiveness analysis (captured as ‘other reasons’ for study discontinuation noted below) as they did not meet inclusion criteria for diagnosis, reducing the effectiveness sample to a total of 30 subjects. A total of five subjects discontinued from the study for the following reasons: withdrawal of consent, one (3%); insufficient response, one (3%); non-compliance (missed more than 3 days of study medication), one (3%); or other reasons, two (6%). Subject demo-graphics, disorder characteristics, and screening/base-line rating scale scores are summarized in Table 1.
Study medication
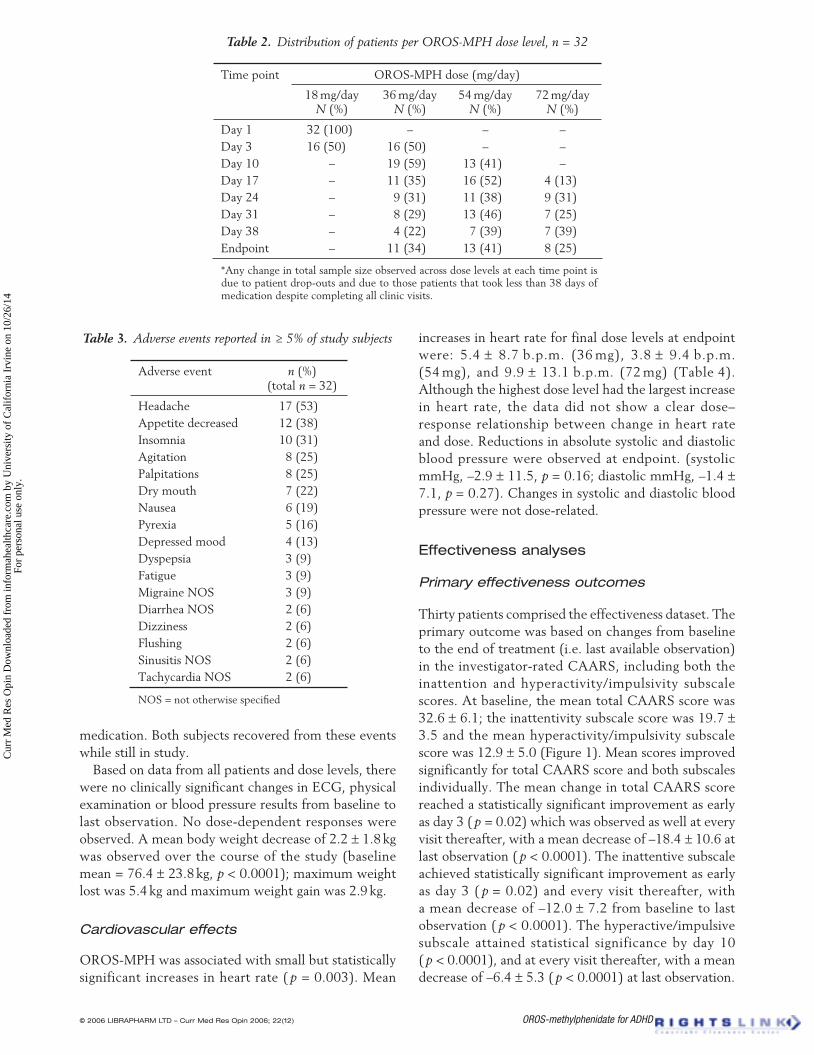
At endpoint, the mean daily dose of OROS-MPH was 52.3 ± 14.0 mg/day (0.74 ± 0.22 mg/kg/day). Modal dose was equal to 54 mg/day, At endpoint, 34% of patients were at a final dose of 36 mg/day, 41% of patients at 54 mg/day and 25% at 72 mg/day. The distribution of patients by daily dose at each time point is captured in Table 2 opposite. Mean treatment duration was 36.1 days ± 6.8 days with a range of days
on treatment of 12–43 days. Mean number of missed doses in those 12 subjects reporting missed doses was 2.9 ± 2.9.
Safety analyses
Of the 32 subjects, 31 (97%) reported at least one adverse event during the study. The most common adverse events were headache (17/32, 53%), decreased appetite (12/32, 38%), and insomnia (10/32, 31%). Overall, there was no relationship between adverse events and OROS-MPH dosage; the percentage of subjects experiencing each type of adverse event during the study was similar among the various final dose groups. All adverse events reported by ≥5% of study subjects are listed in Table 3.
There were no serious adverse events and study medication was not discontinued in any subject due to an adverse event. Adverse events were of mild-to-moderate severity with the exception of two events rated as severe: one report of headache was considered to be probably related to study medication and one report of fatigue considered not to be related to study
Table 1. Baseline demographics and disorder characteristics
Characteristic n Mean (SD) Range
Age, years 32 36.8 (10.4) 19–54 Age at ADHD diagnosis, years 32 35.8 (12.0) 7–54 Height, cm 32 168.9 (11.4) 146–197 Weight, kg 32 76.4 (23.8) 45.2–136.8 Gender Male, n (%) Female, n (%)
18/32 (56) 14/32 (44)
– –
Race White, n (%) Black, n (%)
31/32 (97) 1/32 ( 3)
– –
DSM-IV ADHD diagnosis Combined type, n (%) Predominantly inattention type, n (%)
26/32 (81) 6/32 (19)
– –
Other psychiatric/comorbid condition Yes, n (%) No, n (%) Currently active Generalized anxiety disorder Major depressive disorder NOS Premenstrual syndrome Social phobia
16/32 (50) 16/32 (50)
7 (23) 1 (3) 1 (3) 4 (13)
– –
WURS score at screening 32 49.8 (17.3) 17*–83 CAARS score at baseline 32 32.5 (6.0) 24–44 MADRS score at baseline 32 10.7 (3.2) 4–16 CGI-S score at baseline 32 4.8 (0.6) 2.1–4.8
ADHD = Attention deficit hyperactivity disorder; CAARS = Investigator-Rated Conners’ Adult ADHD Rating Scale; CGI-S = Clinical Global Impression-Severity; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders Fourth Edition; MADRS = Montgomery–Asberg Depression Rating Scale; WURS = Wender Utah Rating Scale; NOS = not otherwise specified *Ward MF, Wender PH, Reimherr FW. The Wender Utah Rating Scale: an aid in the retrospective diagnosis of childhood attention deficit hyperactivity disorder. Am J Psychiatry 1993;150:885–90
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/2
6/14
For
pers
onal
use
onl
y.
© 2006 librApHArM ltd – Curr Med res Opin 2006; 22(12) OROS-methylphenidate for ADHD Fallu et al. 2561
medication. Both subjects recovered from these events while still in study.
Based on data from all patients and dose levels, there were no clinically significant changes in ECG, physical examination or blood pressure results from baseline to last observation. No dose-dependent responses were observed. A mean body weight decrease of 2.2 ± 1.8 kg was observed over the course of the study (baseline mean = 76.4 ± 23.8 kg, p < 0.0001); maximum weight lost was 5.4 kg and maximum weight gain was 2.9 kg.
Cardiovascular effects
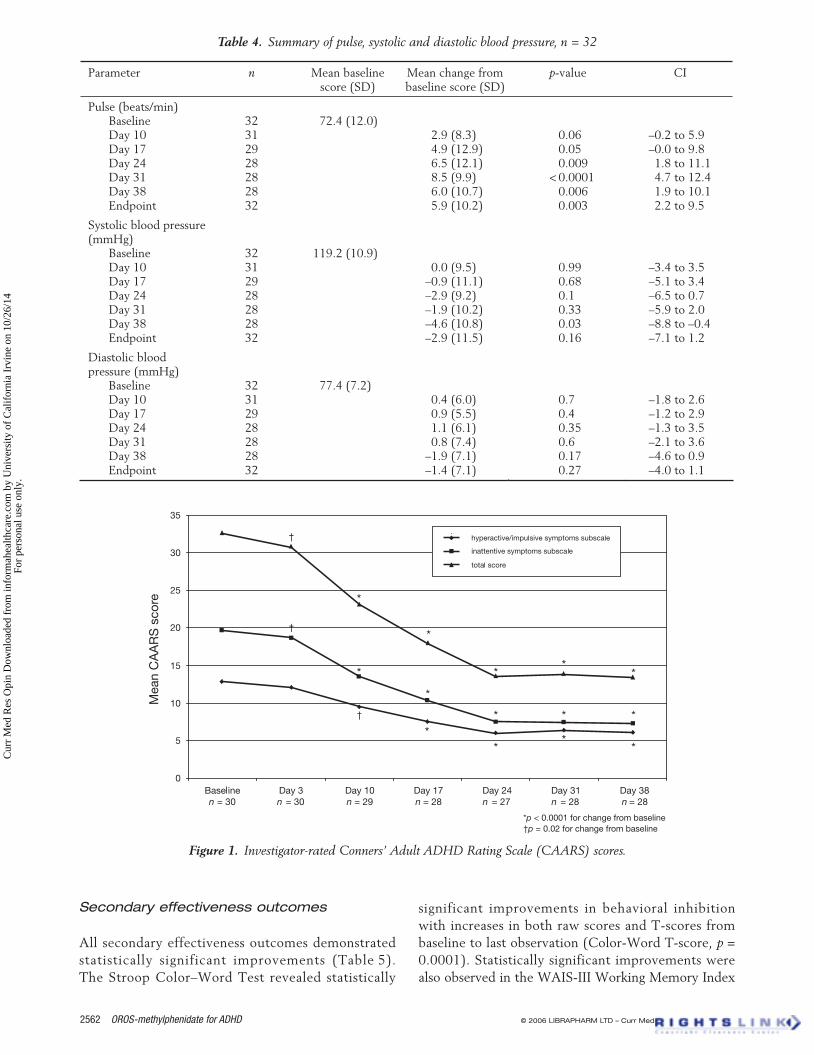
OROS-MPH was associated with small but statistically significant increases in heart rate ( p = 0.003). Mean
increases in heart rate for final dose levels at endpoint were: 5.4 ± 8.7 b.p.m. (36 mg), 3.8 ± 9.4 b.p.m. (54 mg), and 9.9 ± 13.1 b.p.m. (72 mg) (Table 4). Although the highest dose level had the largest increase in heart rate, the data did not show a clear dose–response relationship between change in heart rate and dose. Reductions in absolute systolic and diastolic blood pressure were observed at endpoint. (systolic mmHg, –2.9 ± 11.5, p = 0.16; diastolic mmHg, –1.4 ± 7.1, p = 0.27). Changes in systolic and diastolic blood pressure were not dose-related.
Effectiveness analyses
Primary effectiveness outcomes
Thirty patients comprised the effectiveness dataset. The primary outcome was based on changes from baseline to the end of treatment (i.e. last available observation) in the investigator-rated CAARS, including both the inattention and hyperactivity/impulsivity subscale scores. At baseline, the mean total CAARS score was 32.6 ± 6.1; the inattentivity subscale score was 19.7 ± 3.5 and the mean hyperactivity/impulsivity subscale score was 12.9 ± 5.0 (Figure 1). Mean scores improved significantly for total CAARS score and both subscales individually. The mean change in total CAARS score reached a statistically significant improvement as early as day 3 ( p = 0.02) which was observed as well at every visit thereafter, with a mean decrease of –18.4 ± 10.6 at last observation ( p < 0.0001). The inattentive subscale achieved statistically significant improvement as early as day 3 ( p = 0.02) and every visit thereafter, with a mean decrease of –12.0 ± 7.2 from baseline to last observation ( p < 0.0001). The hyperactive/impulsive subscale attained statistical significance by day 10 ( p < 0.0001), and at every visit thereafter, with a mean decrease of –6.4 ± 5.3 ( p < 0.0001) at last observation.
Table 2. Distribution of patients per OROS-MPH dose level, n = 32
OROS-MPH dose (mg/day) Time point
18 mg/day N (%)
36 mg/day N (%)
54 mg/dayN (%)
72 mg/day N (%)
Day 1 32 (100) – – – Day 3 16 (50) 16 (50) – – Day 10 – 19 (59) 13 (41) – Day 17 – 11 (35) 16 (52) 4 (13) Day 24 – 9 (31) 11 (38) 9 (31) Day 31 – 8 (29) 13 (46) 7 (25) Day 38 – 4 (22) 7 (39) 7 (39) Endpoint – 11 (34) 13 (41) 8 (25)
*Any change in total sample size observed across dose levels at each time point is due to patient drop-outs and due to those patients that took less than 38 days of medication despite completing all clinic visits.
Adverse event n (%) (total n = 32)
Headache 17 (53) Appetite decreased 12 (38) Insomnia 10 (31) Agitation 8 (25) Palpitations 8 (25) Dry mouth 7 (22) Nausea 6 (19) Pyrexia 5 (16) Depressed mood 4 (13) Dyspepsia 3 (9) Fatigue 3 (9) Migraine NOS 3 (9) Diarrhea NOS 2 (6) Dizziness 2 (6) Flushing 2 (6) Sinusitis NOS 2 (6) Tachycardia NOS 2 (6)
NOS = not otherwise specified
Table 3. Adverse events reported in ≥ 5% of study subjects
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/2
6/14
For
pers
onal
use
onl
y.
2562 OROS-methylphenidate for ADHD © 2006 librApHArM ltd – Curr Med res Opin 2006; 22(12)
Secondary effectiveness outcomes
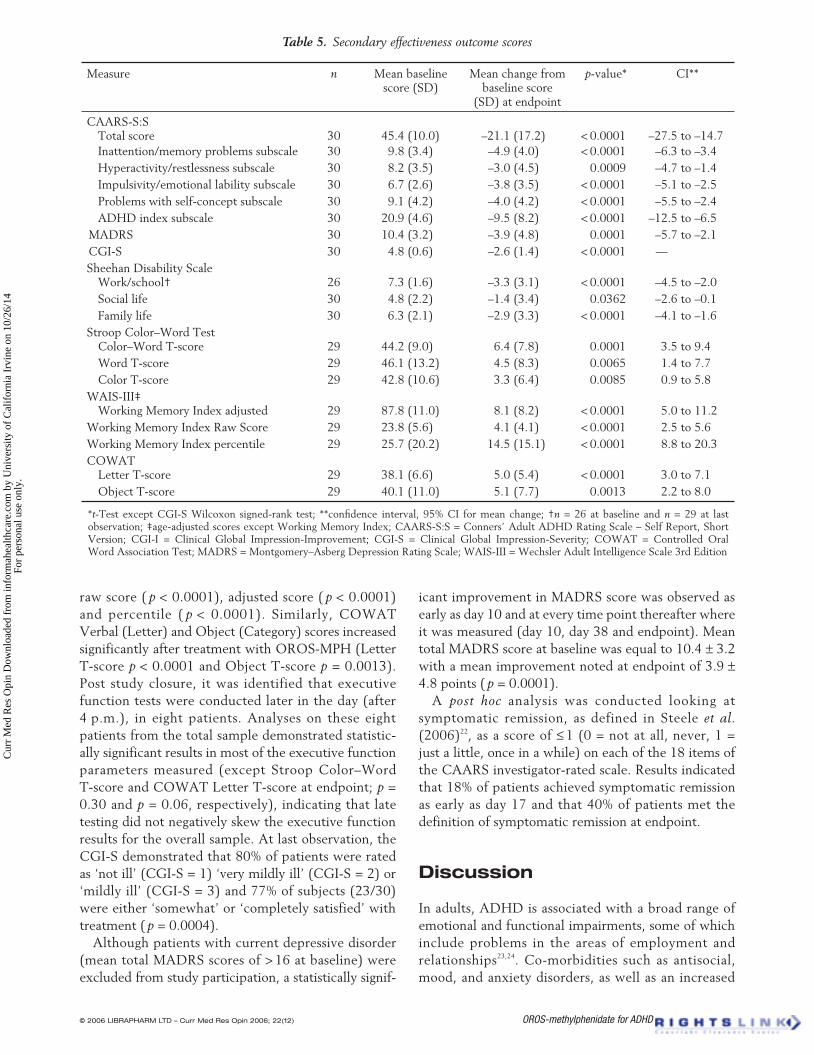
All secondary effectiveness outcomes demonstrated statistically significant improvements (Table 5). The Stroop Color–Word Test revealed statistically
significant improvements in behavioral inhibition with increases in both raw scores and T-scores from baseline to last observation (Color-Word T-score, p = 0.0001). Statistically significant improvements were also observed in the WAIS-III Working Memory Index
Table 4. Summary of pulse, systolic and diastolic blood pressure, n = 32
Parameter n Mean baseline score (SD)
Mean change from baseline score (SD)
p-value CI
Pulse (beats/min) Baseline Day 10 Day 17 Day 24 Day 31 Day 38 Endpoint
32 31 29 28 28 28 32
72.4 (12.0)
2.9 (8.3) 4.9 (12.9) 6.5 (12.1) 8.5 (9.9) 6.0 (10.7) 5.9 (10.2)
0.06 0.05 0.009
< 0.0001 0.006 0.003
–0.2 to 5.9 –0.0 to 9.8 1.8 to 11.1 4.7 to 12.4 1.9 to 10.1 2.2 to 9.5
Systolic blood pressure (mmHg)
Baseline Day 10 Day 17 Day 24 Day 31 Day 38 Endpoint
32 31 29 28 28 28 32
119.2 (10.9)
0.0 (9.5) –0.9 (11.1) –2.9 (9.2) –1.9 (10.2) –4.6 (10.8) –2.9 (11.5)
0.99 0.68 0.1 0.33 0.03 0.16
–3.4 to 3.5 –5.1 to 3.4 –6.5 to 0.7 –5.9 to 2.0 –8.8 to –0.4 –7.1 to 1.2
Diastolic blood pressure (mmHg)
Baseline Day 10 Day 17 Day 24 Day 31 Day 38 Endpoint
32 31 29 28 28 28 32
77.4 (7.2)
0.4 (6.0) 0.9 (5.5) 1.1 (6.1) 0.8 (7.4)
–1.9 (7.1) –1.4 (7.1)
0.7 0.4 0.35 0.6 0.17 0.27
–1.8 to 2.6 –1.2 to 2.9 –1.3 to 3.5 –2.1 to 3.6 –4.6 to 0.9 –4.0 to 1.1
Figure 1. Investigator-rated Conners’ Adult ADHD Rating Scale (CAARS) scores.
†p = 0.02 for change from baseline*p < 0.0001 for change from baseline
n n n n n n n
Mea
n C
AA
RS
sco
re
†
†
†
*
*
**
*
*
**
**
**
*
*
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/2
6/14
For
pers
onal
use
onl
y.
© 2006 librApHArM ltd – Curr Med res Opin 2006; 22(12) OROS-methylphenidate for ADHD Fallu et al. 2563
raw score ( p < 0.0001), adjusted score ( p < 0.0001) and percentile ( p < 0.0001). Similarly, COWAT Verbal (Letter) and Object (Category) scores increased significantly after treatment with OROS-MPH (Letter T-score p < 0.0001 and Object T-score p = 0.0013). Post study closure, it was identified that executive function tests were conducted later in the day (after 4 p.m.), in eight patients. Analyses on these eight patients from the total sample demonstrated statistic-ally significant results in most of the executive function parameters measured (except Stroop Color–Word T-score and COWAT Letter T-score at endpoint; p = 0.30 and p = 0.06, respectively), indicating that late testing did not negatively skew the executive function results for the overall sample. At last observation, the CGI-S demonstrated that 80% of patients were rated as ‘not ill’ (CGI-S = 1) ‘very mildly ill’ (CGI-S = 2) or ‘mildly ill’ (CGI-S = 3) and 77% of subjects (23/30) were either ‘somewhat’ or ‘completely satisfied’ with treatment ( p = 0.0004).
Although patients with current depressive disorder (mean total MADRS scores of > 16 at baseline) were excluded from study participation, a statistically signif-
icant improvement in MADRS score was observed as early as day 10 and at every time point thereafter where it was measured (day 10, day 38 and endpoint). Mean total MADRS score at baseline was equal to 10.4 ± 3.2 with a mean improvement noted at endpoint of 3.9 ± 4.8 points ( p = 0.0001).
A post hoc analysis was conducted looking at symptomatic remission, as defined in Steele et al. (2006)22, as a score of ≤ 1 (0 = not at all, never, 1 = just a little, once in a while) on each of the 18 items of the CAARS investigator-rated scale. Results indicated that 18% of patients achieved symptomatic remission as early as day 17 and that 40% of patients met the definition of symptomatic remission at endpoint.
Discussion
In adults, ADHD is associated with a broad range of emotional and functional impairments, some of which include problems in the areas of employment and relationships23,24. Co-morbidities such as antisocial, mood, and anxiety disorders, as well as an increased
Table 5. Secondary effectiveness outcome scores
Measure n Mean baseline score (SD)
Mean change from baseline score
(SD) at endpoint
p-value* CI**
CAARS-S:S Total score
30
45.4 (10.0)
–21.1 (17.2)
< 0.0001
–27.5 to –14.7
Inattention/memory problems subscale 30 9.8 (3.4) –4.9 (4.0) < 0.0001 –6.3 to –3.4 Hyperactivity/restlessness subscale 30 8.2 (3.5) –3.0 (4.5) 0.0009 –4.7 to –1.4 Impulsivity/emotional lability subscale 30 6.7 (2.6) –3.8 (3.5) < 0.0001 –5.1 to –2.5 Problems with self-concept subscale 30 9.1 (4.2) –4.0 (4.2) < 0.0001 –5.5 to –2.4 ADHD index subscale 30 20.9 (4.6) –9.5 (8.2) < 0.0001 –12.5 to –6.5
MADRS 30 10.4 (3.2) –3.9 (4.8) 0.0001 –5.7 to –2.1 CGI-S 30 4.8 (0.6) –2.6 (1.4) < 0.0001 — Sheehan Disability Scale
Work/school†
26
7.3 (1.6)
–3.3 (3.1)
< 0.0001
–4.5 to –2.0 Social life 30 4.8 (2.2) –1.4 (3.4) 0.0362 –2.6 to –0.1 Family life 30 6.3 (2.1) –2.9 (3.3) < 0.0001 –4.1 to –1.6
Stroop Color–Word Test Color–Word T-score
29
44.2 (9.0)
6.4 (7.8)
0.0001
3.5 to 9.4
Word T-score 29 46.1 (13.2) 4.5 (8.3) 0.0065 1.4 to 7.7 Color T-score 29 42.8 (10.6) 3.3 (6.4) 0.0085 0.9 to 5.8
WAIS-III‡ Working Memory Index adjusted
29
87.8 (11.0)
8.1 (8.2)
< 0.0001
5.0 to 11.2
Working Memory Index Raw Score 29 23.8 (5.6) 4.1 (4.1) < 0.0001 2.5 to 5.6 Working Memory Index percentile 29 25.7 (20.2) 14.5 (15.1) < 0.0001 8.8 to 20.3 COWAT
Letter T-score
29
38.1 (6.6)
5.0 (5.4)
< 0.0001
3.0 to 7.1 Object T-score 29 40.1 (11.0) 5.1 (7.7) 0.0013 2.2 to 8.0
*t-Test except CGI-S Wilcoxon signed-rank test; **confidence interval, 95% CI for mean change; †n = 26 at baseline and n = 29 at last observation; ‡age-adjusted scores except Working Memory Index; CAARS-S:S = Conners’ Adult ADHD Rating Scale – Self Report, Short Version; CGI-I = Clinical Global Impression-Improvement; CGI-S = Clinical Global Impression-Severity; COWAT = Controlled Oral Word Association Test; MADRS = Montgomery–Asberg Depression Rating Scale; WAIS-III = Wechsler Adult Intelligence Scale 3rd Edition
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/2
6/14
For
pers
onal
use
onl
y.

2564 OROS-methylphenidate for ADHD © 2006 librApHArM ltd – Curr Med res Opin 2006; 22(12)
risk of substance abuse and a disruptive family environ-ment, are also associated with adult ADHD25,26,27. Recent studies have demonstrated that adult ADHD is a common and costly workplace condition, affecting 4.2% of workers, and associated with 35.0 days of annual lost work performance28. Individuals with adult ADHD also have significantly higher annual medical costs than matched controls, even after controlling for patient comorbidity29. Barkley et al. (2006) reported on a cohort of hyperactive and community control subjects followed to adulthood. The hyperactive group had lower educational performance leading to a 32% failure rate in completing high school. Adults had been fired from more jobs and demonstrated more employer-rated ADHD and oppositional defiant disorder symptoms and lower job performance than the community control group. Socially, the hyperactive group had fewer friends, trouble keeping friends and more parent-rated social problems30.
This open-label, pilot study of OROS-MPH for the treatment of adults with ADHD suggests that OROS-MPH may offer a well-tolerated and effective treatment option for this population.
Results observed in the investigator-rated CAARS reached a statistically significant improvement as early as day 3 in symptoms of inattention ( p = 0.02) and as early as day 10 in symptoms of hyperactivity/impulsivity ( p < 0.0001), with improvements equal to –12.0 ± 7.2 and –6.4 ± 5.3 at endpoint, respectively. The improvement in symptom control was maintained from day 24 to end of study (Figure 1) which was expected by the authors. Given that stimulants are rapidly-acting and that, as per protocol, patients had already been stabilized on their individualized, optimal dose by day 24 of treatment and achieved a substantial reduction in mean CAARS score, additional improve-ment beyond day 24 was not anticipated. In a recently published open-label study in adult patients with late-onset ADHD conducted by Biederman et al. (2006)9, a statistically significant reduction in symptoms was also observed in inattention (–9.3 ± 6.2) and hyperactiv-ity/impulsivity (–7.2 ± 5.2) on the Adult ADHD Investigator Symptom Report Scale (AISRS), confirm-ing the results presented here.
At endpoint, the mean daily dose of OROS-MPH was 52.3 ± 14.0 mg/day (0.74 ± 0.22 mg/kg/day) which was lower than the mean dose reported by Biederman et al. (2006)9. Though the maximal dose permitted in our study was 72 mg/day, only eight patients achieved this maximal dose at endpoint. It is of interest that, although most patients did not reach this maximum dose, 87% of patients experienced an improvement in symptoms as rated by the CGI-S scale, with no patients having experienced deteriorating symptomatology, and only four patients rated as 0 (‘no change’) at endpoint,
and thus considered non-responders. Improvements in ADHD symptom scales were similar to what has been previously reported in other studies evaluating the same population7,8,31.
Neuropsychological theory of ADHD suggests that its symptoms arise from dysregulation of prefrontal cortical/striatal and cerebellar (PFC) circuits32 leading to behavioral hyperactivity, distractibility or impulsivity, as well as deficits in executive function. Executive function is defined as neurocognitive processes that maintain an appropriate problem-solving set to attain a future goal33 and range from being able to maintain a certain focus of attention to switching attention from one source of information to another, to the ability to suppress ongoing response behavior (response inhibition)33. Specific to ADHD, deficits of response inhibition or attention have been identified as playing a critical role in disorder presentation34. A recent meta-analysis conducted by Willcutt et al. (2005)35, concluded that ADHD is associated with weaknesses in several key executive function domains, most notably in areas of response inhibition, vigilance, spatial working memory and some measures of planning, with effect sizes falling within the moderate range. Aron et al. (2003)36 confirmed prior reports that a response inhibition deficit in adults can be ameliorated by methylphenidate administration.
This study attempted to evaluate the likelihood of improving executive function in adult ADHD patients via analysis of Stroop Color–Word (interfer-ence/response inhibition), Working Memory Index of WAIS-III (working memory, attention) and Controlled Oral Word Association Test (COWAT) Verbal and Category (fluency) tests. It is important to mention, however, that these neuropsychological measures were not originally developed for use in ADHD and as a result may not be sensitive enough to detect improve-ments related to treatment. Nevertheless, results of this trial demonstrated statistically significant improve-ments in all areas of executive function measured (Table 5), consistent with previous studies evaluating executive function in children and adults with ADHD treated with methylphenidate34,37,38. Improvement in executive function may lead to a better ability to focus on tasks in the work, school and home milieu, improve social functioning and assist in maintaining employ-ment. The ability to focus on a task may result in completion of objectives and may translate to increased work and school-related performance. Stimulant therapy has been shown to decrease impulsive actions, characteristic of the disorder, which are not tolerated in the workplace or within the family36. This improve-ment in behavioral inhibition renders the patient in control of his/her impulses, thereby also improving social relations with friends, family and co-workers.
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/2
6/14
For
pers
onal
use
onl
y.

© 2006 librApHArM ltd – Curr Med res Opin 2006; 22(12) OROS-methylphenidate for ADHD Fallu et al. 2565
In addition to the ADHD symptom and executive function improvement observed in this study, the Sheehan Disability Scale (SDS) evaluating quality of life also demonstrated statistically significant improve-ments in work/school, family life and social life domains ( p < 0.0001, p < 0.0001, p = 0.04, respect-ively). At endpoint, a statistically significant improve-ment of 2.6 ± 1.4 was observed in investigator-rated CGI-S ( p < 0.0001)
With regard to cardiovascular effects, a statistically significant change in heart rate was observed with OROS-MPH in this study ( p = 0.004) and there was a reduction in absolute systolic and diastolic blood pressure. Since the mean dose employed by Biederman and colleagues9 was much higher than the mean dose reported in this study, [78.2 ± 29.4 mg/day vs. 52.3 ± 14.0 mg/day], the authors hypothesize that the increase in number of cardiovascular outliers in the Biederman et al. study may be dose-related. In general, these results suggest that monitoring of heart rate and blood pressure may be called for when treating adults with OROS-MPH.
The results of this study must be tempered against its methodological limitations. Since this was an open-label trial without a placebo control, the results were subject to observer bias. Moreover, adverse effects and assessment of tolerability are limited by not having the benefit of a placebo comparator. Adults with unstable psychiatric and medical disorders were excluded from the sample, rendering our sample less reflective of clinical practice. Since this trial involved an approx-imate 5-week study duration, conclusions of effective-ness for longer periods of time cannot be drawn. Longer-term studies are required in order to gauge the continued effect or lack thereof of OROS-MPH. We can hypothesize, however, that the benefits of treatment should also be maintained in the adult population as was demonstrated in the previous long-term OROS-MPH studies conducted in children39.
Conclusion
Despite these limitations, the results of this study replicate the results previously published in adult patients with ADHD by Biederman and colleagues and suggest that once-daily OROS-MPH is a well tolerated and effective treatment for adult ADHD. The results also suggest that OROS-MPH offers an additional benefit of improvement in executive function, in the areas of response inhibition, verbal/category fluency and working memory, previously identified in the literature as having a critical role in adult ADHD. More randomized, controlled trials, however, are needed to evaluate effectiveness and safety in long-term treatment in adults with ADHD.
Acknowledgments
This information was presented at the American Psychiatric Association annual meeting, May 20th–25th, 2006, Toronto, ON, Canada; the Society of Biological Psychiatry meeting, May 18–20, 2006, Toronto, ON, Canada; and the Collegium Internationale Neuropsychopharmacologicum meeting, July 9–13, 2006, Chicago, IL, USA. Publication of a clinical trial registry summary is located on the clinicaltrials.gov website.
Sincere appreciation to Jenny Wang, PhD, president of Covar Inc. for her statistical assistance and to Janice Kramer of Medical Writing Associates for support with medical writing. This study has been registered with the clinicaltrials.gov web-site. As principal investigator for this study, Angelo Fallu, Clinique Woodward, Sherbrooke, Quebec, was reimbursed for patient enrolment by the sponsor of the study, Janssen-Ortho, Canada. Caroline Richard is an employee of Clinique Woodward, Sherbrooke, Quebec. Rosanna Prinzo and Carin Binder are employees of Janssen-Ortho, Canada, sponsor of this study.
References 1. American Academy of Pediatrics, Committee on Quality
Improvement and Subcommittee on Attention-Deficit/Hyper-activity Disorder. Clinical Practice Guideline, Diagnosis and evaluation of the child with attention-deficit/hyperactivity disorder. Pediatrics 2000;105:1158-70
2. Adler LA, Chua HC. Management of ADHD in adults. J Clin Psychiatry 2002;63(Suppl 12):29-35
3. Wender PH, Wolf LE, Wasserstein J. Adults with ADHD. An overview. Ann N Y Acad Sci 2001;931:1-16
4. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. Am J Psychiatry 2006;163:716-23
5. Lamberg L. ADHD often undiagnosed in adults: appropriate treatment may benefit work, family, social life. JAMA 2003;290:1565-7
6. Seidman LJ. Neuropsychological functioning in people with ADHD across the lifespan. Clin Psychol Rev 2006;26: 466-85
7. Faraone SV, Spencer T, Aleardi M, et al. Meta-analysis of the efficacy of methylphenidate for treating adult attention–deficit/hyperactivity disorder. J Clin Psychopharmacol 2004;24:24-9
8. Biederman J, Mick E, Surman C, et al. A randomized, placebo-controlled trial of OROS-methylphenidate in adults with attention–deficit/hyperactivity disorder. Biol Psychiatry 2006;59:829-35
9. Biederman J, Mick E, Spencer T, et al. An open trial of OROS- methylphenidate in adults with late-onset ADHD. CNS Spectr 2006;11:390-6
10. Barkely RA. Behavioural inhibition, sustained attention and executive function: constructing a unified theory of ADHD. Psychol Bull 1997;121:65-94
11. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders Fourth Edition, Text Revision, Washington DA, The American Psychiatric Association, 2000
12. First MB, Spitzer RL, Gibbon M, et al. Structured Clinical Interview for DSM-IV Axis I Disorders, Patient Edition (SCID-P), version 2. New York: New York State Psychiatric Institute, Biometrics Research, 1994
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/2
6/14
For
pers
onal
use
onl
y.

2566 OROS-methylphenidate for ADHD © 2006 librApHArM ltd – Curr Med res Opin 2006; 22(12)
13. Ward MF, Wender PH, Reimherr FW. The Wender Utah Rating Scale: an aid in the retrospective diagnosis of childhood attention deficit hyperactivity disorder. Am J Psychiatry 1993;150: 885-90
14. Conners CK, Erhardt D, Sparrow E. Conners’ Adult ADHD Rating Scales (CAARS): Technical Manual. New York: Multi-Health Systems, 1999
15. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry 1979;134:382–9
16. Golden CJ, Freshwater SM. The Stroop Color and Word Test. Manual for Clinical and Experimental Uses. Wood Dale, IL: Stoelting, 2002
17. Wechsler D. Échelle d’intelligence de Wechsler pour adultes – Troisième édition. Version pour francophones du Canada. Manuel d’administration, Édition de recherche. The Psychological Corporation, 2004
18. Gladsjo JA, Schuman CC, Evans JD, et al. Norms for letter and category fluency: demographic corrections for age, education, and ethnicity. Assessment 1999;6:147-78
19. Sheehan DV, Sajatovic M, Ramirez LF. Sheehan Disability Scale. Rating Scales in Mental Health. 2nd edn. Hudson, OH: Lexi-Comp, 2003:41-2
20. National Institutes of Mental Health (NIMH). CGI (Clinical Global Impression Scale) – NIMH. Psychopharmacol Bull 1985;21:839-43
21. Likert R. A technique for the measurement of attitudes. Arch Psychology 1932;140:52
22. Steele M, Weiss M, Swanson J, et al. A randomized, controlled effectiveness trial of OROS-methylphenidate compared to usual care with immediate-release methylphenidate in ADHD. Can J Clin Pharmacol 2006;13:e50-62
23. Murphy K, Barkley RA. Attention deficit hyperactivity disorder in adults: comorbidities and adaptive impairments. Compr Psychiatry 1996;37:393-401
24. Barkley RA. Major life activity and health outcomes associated with attention–deficit/hyperactivity disorder. J Clin Psychiatry 2002;63(Suppl 12):10-15
25. Biederman J, Faraone SV, Monuteaux MC, et al. Gender effects on attention–deficit/hyperactivity disorder in adults, revisited. Biol Psychiatry 2004;55:692-700
26. Adler L, Cohen J. Diagnosis and evaluation of adults with attention–deficit/hyperactivity disorder. Psychiatr Clin North Am 2004;27:187-201
27. Schoechlin C, Engel R, Neuropsychological performance in adult attention–deficit hyperactivity disorder: meta-analysis of empirical data. Arch Clin Neuropsychol 2005;20:727-44
28. Kessler RC, Adler L, Ames M, et al. The prevalence and effects of adult attention deficit/hyperactivity disorder on work performance in a nationally representative sample of workers. J Occup Environ Med 2005;47:565-72
29. Matza LS, Paramore C, Prasad M. A review of the economic burden of ADHD. Cost Eff Resourc Alloc 2005;3:5
30. Barkley RA, Fischer M, Smallish L. Young adult outcome of hyperactive children: adaptive functioning in major life activities. J Am Acad Child Adolesc Psychiatry 2006;45:192-202
31. Spencer T, Biederman J, Wilens T, et al. A large, double-blind, randomized clinical trial of methylphenidate in the treatment of adults with ADHD. Biol Psychiatry 2005;57:456-63
32. Arnsten A, Dudley AG. Methylphenidate improves prefrontal cortical cognitive function through α2 adrenoceptor and dopamine D1 receptor actions: relevance to therapeutic effects in attention deficit hyperactivity disorder. Behav Brain Funct 2005;1:2
33. Bekker E, Overtoom C, Kooij JJ, et al. Disentangling deficits in adults with attention–deficit/hyperactivity disorder. Arch Gen Psychiatry 2005;62:1129-36
34. Mehta MA, Goodyer MI, Sahakian BJ. Methylphenidate improves working memory and set-shifting in AD/HD: relation-ships to baseline memory capacity. J Child Psychol Psychiatry 2004;45:293-305
35. Willcutt E, Doyle A, Nigg JT, et al. Validity of the executive function theory of attention–deficit/hyperactivity disorder: a meta-analytic review. Biol Psychiatry 2005;57:1336-46
36. Aron A, Dowson JH, Sahakian BJ, et al. Methylphenidate improves response inhibition in adults with attention–deficit/hyperactivity disorder. Biol Psychiatry, 2003;54:1465-8
37. Turner DC, Blackwell AD, Dowson JH, et al. Neurocognitive effects of methylphenidate in adult attention–deficit/hyper-activity disorder. Psychopharmacology (Berl) 2004;178:286-95
38. Schweitzer JB, Lee DO, Hanford RB, et al. Effect of methyl-phenidate on executive functioning in adults with attention–deficit/hyperactivity disorder: normalization of behavior but not related to brain activity. Biol Psychiatry 2004;56:597-606
39. Wilens T, McBurnett K, Stein M, et al. ADHD treatment with once-daily OROS methylphenidate: final results from a long-term open-label study. J Am Acad Child Adolesc Psychiatry 2005;44:1015-23
CrossRef links are available in the online published version of this paper:http://www.cmrojournal.com
Paper CMRO-3588_4, Accepted for publication: 12 October 2006Published Online: 30 November 2006
doi:10.1185/030079906X154132
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/2
6/14
For
pers
onal
use
onl
y.