Embed Size (px)
Citation preview
Idiopathic Thrombocytopenic Purpura
DR BINOD KUMAR SINGH Associate Professor, PMCH, Patna CIAP Executive Board Member 2015 NNF State President-2014
IAP State Secretary ,Bihar 2010-2011 NNF State Secretary , Bihar 2008-2009
Chief Consultant: Shiv Shishu Hospital
K- 208 P C Colony ,Hanuman NagarPatna 800020.
Email- [email protected] web site :- www.shivshishuhospital.com
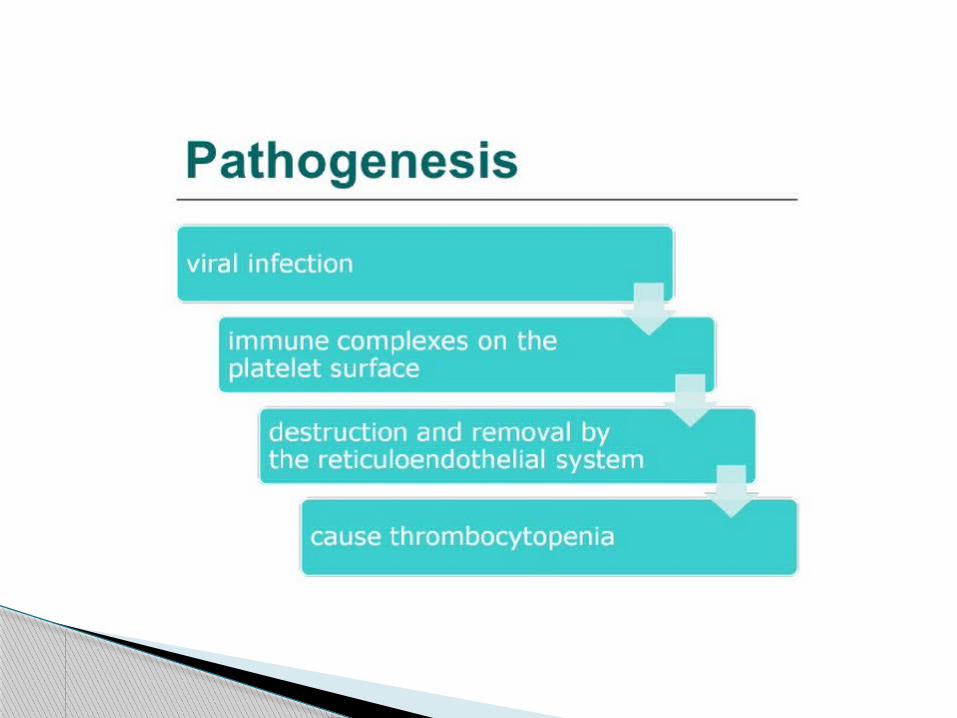
Etiology - still unknown and Pathogenesis -is complex and possibly
depends on - disturbed antigen presentation, -T cell activation and signaling,
-disregulated B cell stimulation and antibodies
production, -unbalanced activation / suppression of complement.
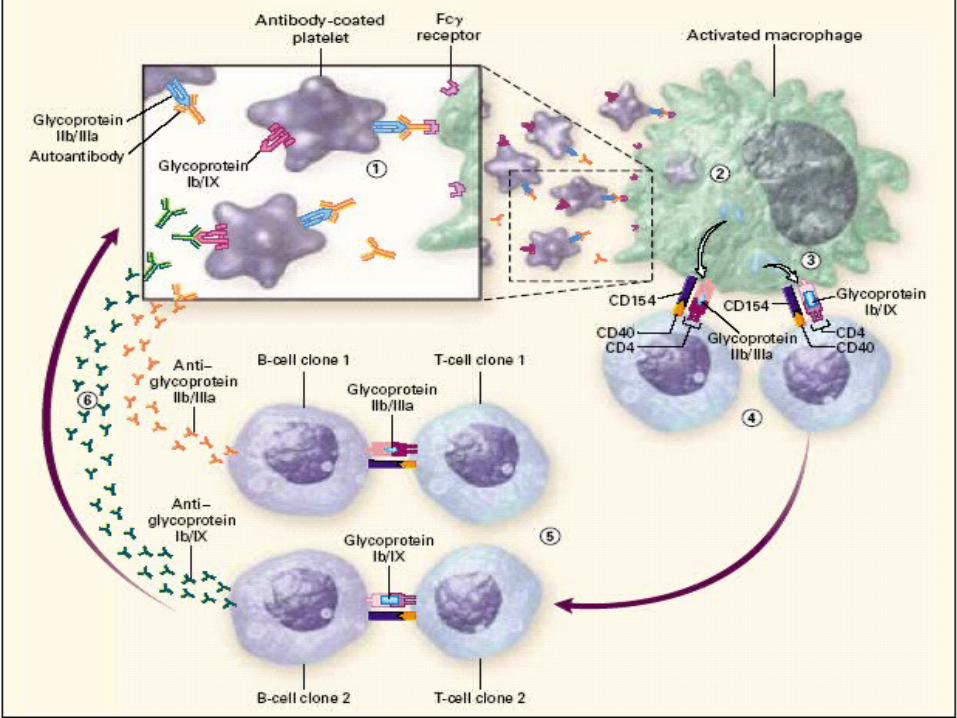
ITP is mediated by IgG autoantibodies.
Glycoprotein IIb/IIa, Ib/Ix, Ia/IIa, IV and V ...
Accelerated clearance through Fcү receptors that are expressed by tissue macrophages.
Pathophysiology




No symptoms Mild symptoms: bruising and
petechiae,occasional minor epistaxis. Moderate: more severe skin and mucosal
lesions,troublesome epistaxis and menorrhagia.
Severe: bleeding episodes requiring transfusion or hospitalisation, symptoms interfering seriously with quality of life.
Clinical Manifestations
DiagnosisDiagnosis should be based ono the infection historyo clinical featureso physical examinationo laboratory test
The diagnosis of ITP remains one of exclusion.
Secondary causes of thrombocytopenia:• Infections - DIC , malaria, kala-azar, DHF,
Hepatitis B & C , HIV, congenital torch infection , Infections ass. with hemophagocytosis syndrome
• Medications – valproate , penicillins, heparin,quinine,digoxin
• Thrombotic microangiopathy : Thrombotic thrombocytopenic purpura, HUS
• Malignancies : leukemia,lymphoma, neuroblastoma
Diagnosis
• Auto immune or related disorders: SLE , Evans Syndrome ,Antiphospholipid syndrome, Neonatal immune thrombocytopenia
• Immunodeficiency: Wiskott aldrich syndrome,HIV/ AIDS
• Bone Marrow failure : TAR , Fanconi anemia, Shwachman-diamond syndrome
• Marrow replacement : Osteopetrosis, Gaucher disease
• Others : Hypersplenism, Kasabach meritt syndrome
Secondary causes of thrombocytopenia contd.
Laboratory studieso White blood cell count and morphology are normal.o Hemoglobin values are normal unless there has been prolonged bleeding.o PT and PTT are normal, bleeding time would be prolonged, but testing is unnecessary.
Laboratory studies
o Peripheral blood smear: an isolated thrombocytopenia with no other abnormalities, platelet count<100 x10⁹/L,the few circulating platelet may be quite large (megathromocytes).
In adolescents with new onset ITP, an antinuclear antibody test for SLE.
HIV test in at risk population. Coomb’s test for unexplained anemia or
before instituting therapy with IV anti-D.
Other Laboratory Tests
Laboratory studieso Measuring antipatelet antibodieso including the measurment of the amount of platelet-associated IgG (PAIgG)and direct assay of specific platelet antibodies.o However , these tests lack both specificity and sensitivity in acute ITP of childhood.
Abnormal WBC count or differential count Unexplained anemia Findings on history and physical
examination suggestive of BM failure syndrome or malignancy.
Indications for bone Marrow Examination
Laboratory studieso Bone marrow:The bone marrow in patient with ITP contains normal or increased numbers of megakaryocytes
Indicating that platelet production is normal and that thrombocytopenia results from increased platelet destruction
- Those without hemorrhage –is managed on an outpatient basis with minimal investigation,
- Short-term therapy in selected cases, - Avoidance of activities that predispose the
patient to trauma and- Avoidance of medications that impair
platelet function.
TREATMENT ITP
Treatment
1. General Treatmento salicylate- containing medications, antihistamines and nonsteroidal drugs
that interfere function and increase the risk of bleeding should be avoided.
Children who have platelet counts >20,000/mm3 and are asymptomatic or have only minor purpura do not require routine treatment.
Children who have platelet counts < 20,000/mm3 and significant mucous membrane bleeding and those who have platelet counts < 10,000/mm3 and minor purpura should receive specific treatment.
Indication for treatment
o Children with active bleeding – IVIG or Rh anti –D immunoglobulin
o Corticosteroids should be adm after malignancy is ruled out by BM examination
o Prednisolone- 1 to 4 mg/kg/ d for 2 to 4 weeks and then tapered
o Dexamethasone – 20 mg/m² over 4 days every three weeks for 4 to 6 courses.
o Serious hemorrhage- platelet transfusion + corticosteroid/IVIG/Rh anti- D Immunoglobulin
Treatment of Acute ITP
o Prednisolone low dose on alternate day o Combinations of the following options:- - Danazol - vincristine - cyclosporine - azathioprineo Rituximab (Anti-CD 20 monoclonal
antibody)o Splenecdomy o Thrombopoietin receptor- binding agents
Chronic ITP
Treatment
2. Intravenous immunoglobulin (IVIG).o Mechanisms:o Blocking Fc receptor of the RE(reticulo= endothelium) phagocyteso Preventing them from binding and destroying IgG antibody-coated
platelets.
DOSE: 0.8 – 1gm/kg/day for 1-2 days. It induces rapid rise in platelet count in 95%
of patients within 48hrs.
Treatment
Treatmento Disadvantages of IVIG:- - it is expensive , -long infusion time of 6 to 8 hours, - allergic reactions, - aseptic meningitis with severe
headache in 10% to 30 %, - 50% to 75% have headache,nausea, vomiting or fever.
Treatment
3. Corticosteroids. Mechanisms:o Reducing capillary fragilityo Inhibiting platelets destruction o Have a rapid, dose dependent action that reduce RE destruction of antibody- coated plateletso Also reduces antibody production slowly.
Treatment
o Children with chronic ITP who have mild or recurrent bleeding are sometimes treated with intermittent courses of IVIG or high dose corticosteroids (interavenous methayl prednisolone 20 ∼ 30 mg/kg/d for 3 days ).
Treatment
4. Intravenous anti –Rh(D) Immunoglobulin for Rh-positive patient.
Mechanisms:o Anti-Rh(D) immunoglobulin produces a mild
hemolytic anemia that saturates the Fc receptors of the phagocytic elements of the
RE system.
Treatmento Permitting increased survival of antibody
coated platelets.o The immediate goal of therapy is to
increase the platelet count to a safe level, usually>
20 x 10⁹/L, in the hope of the reducing the risk of severe hamorrhage.
o Dose:IV Anti-Rh(D) , 50μg to 75μg/kg for 2 days.
Treatment
Merit of Anti Rh(D) immunoglobulin :o less expensive than IVIG but more costly
than steroids,o lower rate of allergic side effects(10%) than
IVIG ando does not cause aseptic meningitis.Disadvantage : cause mild hemolysis with a
transient hemoglobin decrease of 10 to 20%
For children>4yrs with severe ITP and whose symptoms are not controlled with therapy.
When life threatening hemorrhage complicates ITP.
It is associated with risk of infection caused by encapsulated organisms and potential development of pulmonary hypertension in adulthood.
5) SPLENECTOMY
Treatment
6. Other treatment.o ɑ interferon, danazol (a synthetic androgen), ascorbic acid, cyclosporine, and a variety of immunosuppressive drugs including mycophenolate
mofetil ,vincristine (VCR), azathioprine,and cyclophosphamide(CTX).
o No large study of these agents have been described in children with chronic ITP, and they may have immediate and long-term toxicities
.o Adsorption Ab removal has been used with limited
success in refractory cases.
A chimeric monoclonal anti B-cell antibody. Reduces the immune system response. May be considered for children with ITP
who have significant ongoing bleeding. May be considered as an alternative to
splenectomy in children with chronic ITP or who have failed splenectomy.
RITUXIMAB
Eltrombopag (Promacta) Oral thrombopoietin (TPO) receptor agonist. Interacts with transmembrane domain of
human TPO receptor and induces megakaryocyte proliferation and differentiation from bone marrow progenitor cells.
Indicated for thrombocytopenia associated with chronic ITP in patients experiencing inadequate response to corticosteroids, immunoglobulins, or splenectomy.
FDA approved for use in adults, no published data for use in children.
Thrombopoietin agonists
Romiplostim (Nplate) An Fc-peptide fusion protein (peptibody) that
increases platelet production through binding and activation of the thrombopoietin (TPO) receptor.
Indicated for chronic ITP in patients who have had an insufficient response to corticosteroids, immunoglobulins, or splenectomy.
Side effects: headache, joint or muscle pain, dizziness, nausea, vomiting.
Treatment
LifeThreatening Hemorrhage- IVIG +platelet transfusion
o May require concomitant Multimodality Therapyo frequently requires Emergency Splenectomyo sometimes necessary Plasmapheresis
Follow -Up
Spontaneous recovery is the normo 60 % in 3 monthso 80 % in 6 monthso 90 % in 9 monthsThe incidence of significiant bleeding-
related morbidity and mortality is extremely low
o Less than 5 %Of Patients with chronic ITPo 20% will ultimately have spontaneous
resolution of their thrombocytopenia.