-
7/25/2019 Dyslipidemia Harper CHO
1/37
Dyslipidemia
Rene J. Harper, M.D.
Georgia Health Sciences University
October 21, 2012
Dyslipidemia
Definition
Classification
Signs and symptoms
Primary causes
Secondary causes Evaluation
Treatment
-
7/25/2019 Dyslipidemia Harper CHO
2/37
Dyslipidemia
Elevation of plasma cholesterol and/ortryglycerides or a low HDL
level thatcontributes to the development ofatherosclerosis.
Causes may be primary (genetic) orsecondary (most common).
Diagnosis is by measuring plasma levels oftotal cholesterol,
TGs, and individuallipoproteins.
Treatment is dietary changes, exercise, andlipid-lowering
drugs.
Dyslipidemia
There is no natural cutoff between normal andabnormal lipid
levels because lipid measurementsare continuous
A linear relation probably exists between lipid levelsand
cardiovascular risk, so many people with
normal cholesterol levels benefit from achievingstill lower
levels
Consequently, there are no numeric definitions of
dyslipidemia; the term is applied to lipid levels forwhich
treatment has proven beneficial Proof of benefit is strongest for
lowering elevated
LDL levels; it is less strong for lowering elevated TGand
increasing low HDL levels, in part becauseelevated TG and low HDL
levels are more predictiveof cardiovascular risk in women than in
men
-
7/25/2019 Dyslipidemia Harper CHO
3/37
Dyslipidemia
Dyslipidemias have been traditionallyclassified by patterns of
elevation inlipids and lipoproteins (Fredricksonphenotype)
Fredrickson Classification
Lipoprotein Patterns (Fredrickson Phenotypes)
Phenotype Elevated Lipoprotein(s) Elevated LipidsI Chylomicrons
TGsIIa LDL CholesterolIIb LDL and VLDL TGs and
cholesterolIII VLDL and chylomicron remnants TGs and
cholesterolIV VLDL TGs
V Chylomicrons and VLDL TGs andcholesterol
-
7/25/2019 Dyslipidemia Harper CHO
4/37
Classification of
dyslipidemiasA more practical system classifies
dyslipidemias as primary or secondaryand characterizes these by:
increases in cholesterol only (pure or
isolated hypercholesterolemia)
increases in TGs only (pure or isolatedhypertriglyceridemia)
increases in both cholesterol and TGs(mixed or combined
hyperlipidemias)
Signs and symptoms
Dyslipidemias are usually asymptomatic but oftenlead to
atherosclerotic vascular disease
High levels of LDL can cause eyelid xanthelasmaand xanthomas
found at the Achilles, elbow, andknee tendons and over
metacarpophalangeal joints(tendinous) or pressure areas
(tuberous)
Patients with the homozygous form of familial
hypercholesterolemia may have the above findingsand additionally
planar or cutaneous xanthomas
Patients with hypertriglyceridemia may havexanthelasma and
eruptive or planar xanthomas
-
7/25/2019 Dyslipidemia Harper CHO
5/37
Signs and symptoms
Patients with the rare dysbetalipoproteinemia mayhave palmar and
tuberous xanthomas andinvolvement of palmar creases
Patients with severe elevations of TGs can haveeruptive
xanthomas over the trunk, back, elbows,buttocks, knees, hands, and
feet
Severe hypertriglyceridemia (> 2000 mg/dL) maygive retinal
arteries and veins a creamy whiteappearance (lipemia retinalis)
Extremely high lipid levels also give a lactescent
(milky) appearance to blood plasma. High TGs (> 1000 mg/dL)
may cause acute
pancreatitis
Planar xanthoma
-
7/25/2019 Dyslipidemia Harper CHO
6/37
-
7/25/2019 Dyslipidemia Harper CHO
7/37
Tendinous xanthoma
Tendinous xanthoma
-
7/25/2019 Dyslipidemia Harper CHO
8/37
Eruptive xanthoma
Eruptive xanthoma
-
7/25/2019 Dyslipidemia Harper CHO
9/37
Tuberous xanthoma
Palmar xanthoma
-
7/25/2019 Dyslipidemia Harper CHO
10/37
Tuberous xanthoma
Xanthelasma
-
7/25/2019 Dyslipidemia Harper CHO
11/37
Xanthelasma
Lipemia retinalis
-
7/25/2019 Dyslipidemia Harper CHO
12/37
Lipemia retinalis
Arcus corneae
-
7/25/2019 Dyslipidemia Harper CHO
13/37
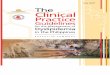
Lipoprotein
Size and BuoyancyCharacteristics ofLipoproteins
-
7/25/2019 Dyslipidemia Harper CHO
14/37
Primary (genetic) causes
Single or multiple genetic mutations that result ineither
overproduction or defective clearance of TGand LDL cholesterol, or
in underproduction orexcessive clearance of HDL.
Primary lipid disorders are suspected when apatient has physical
signs of dyslipidemia, onset ofpremature atherosclerotic disease
(< 60 yr), afamily history of atherosclerotic disease, or
serumcholesterol > 240 mg/dL (> 6.2 mmol/L).
Primary disorders are the most common cause of
dyslipidemia in children, but dont cause a largepercentage of
cases in adults.
Primary (genetic) causes
Familial hypercholesterolemia (FH) Defect in LDL receptor that
leads to diminished
LDL clearance Autosomal dominant inheritance Heterozygotes:
1/500; 5% of AMIs < 60 yr
Tendon xanthomas, xanthelasma, arcus corneaeand premature CAD
(ages 3050)
TC 250500 mg/dL, normal TGL Homozygotes: 1/1 million Tendon
xanthomas, xanthelasma, planar
xanthomas, and premature CAD (< age 18) TC > 500 mg/dL,
normal TGL
-
7/25/2019 Dyslipidemia Harper CHO
15/37
Primary (genetic) causes
Familial defective apo B-100 Defect in Apo B (LDL
receptor-binding
region) that leads to diminished LDLclearance
Autosomal dominant inheritance
1/700
Xanthomas, xanthelasma, and premature
CAD (milder manifestations than FH) TC 250500 mg/dL
Primary (genetic) causes
Polygenic hypercholesterolemia
Unknown genetic defect; likely multipledefects and
mechanisms
Variable inheritance
Common
Premature CAD
TC 250350 mg/dL
-
7/25/2019 Dyslipidemia Harper CHO
16/37
Primary (genetic) causes
LPL deficiency (chylomicronemia) Defect in endothelial LPL that
leads to
diminished chylomicron clearance
Recessive inheritance
Rare
Failure to thrive (infants), eruptivexanthomas, lipemia
retinalis,
hepatosplenomegaly, and pancreatitis TG > 750 mg/dL
Primary (genetic) causes
Apo C-II deficiency Defect in Apo C-II (activating cofactor
for
LPL) leading to functional LPL deficiency
Recessive inheritance
Very rare, frequency < 1/1 million
Pancreatitis in children and young adults,may be associated with
metabolicsyndrome
TG > 750 mg/dL
-
7/25/2019 Dyslipidemia Harper CHO
17/37
Primary (genetic) causes
Familial hypertriglyceridemia Unknown defect, possibly multiple
defects and
mechanisms Autosomal dominant 1/100 (affects 1/2 of first-degree
relatives) Usually no symptoms or findings; obesity and
insulin resistance; occasional eruptivexanthomas or
pancreatitis; low HDL,hyperuricemia
TG 200500 mg/dL; levels increased by dietaryfactors, estrogens,
hypothyroidism and alcohol
Primary (genetic) causes
Familial combined hyperlipidemia Unknown defect
Autosomal dominant
1/50 to 1/100
Premature CAD, 15% of AMIs < 60 yr; obesityand insulin
resistance; low HDL, hyperuricemia
Small, dense LDL; apo B elevated
TC 250500 mg/dL
TG 250750 mg/dL
-
7/25/2019 Dyslipidemia Harper CHO
18/37
Primary (genetic) causes
Familial dysbetalipoproteinemia Defect in Apo E (usually e2/e2
homozygotes);
diminished chylomicron and VLDL clearance
Recessive (more common) or dominant (lesscommon)
1/5000
Xanthomas (especially palmar), yellow palmarcreases, premature
CAD
TC 250500 mg/dL TG 250500 mg/dL
Secondary causes
Most cases of dyslipidemia in adults The most important
secondary cause in developed
countries is a sedentary lifestyle with excessivedietary intake
of saturated fat, cholesterol, andtrans fatty acids (TFAs)
Other common secondary causes: diabetes mellitus alcohol
abuse
chronic renal insufficiency, nephrotic syndrome hypothyroidism
primary biliary cirrhosis and other cholestatic liver
diseases, Drugs: thiazides, -blockers, retinoids,
highly-active
antiretroviral agents, estrogen and progestins,
andglucocorticoids
-
7/25/2019 Dyslipidemia Harper CHO
19/37
Diabetic dyslipidemia
Diabetic patients, in particular DM-2, tend to have
anatherogenic combination of high TGs, high small/denseLDL and low
HDL.
This profile may be a consequence of obesity and/orpoor control
of diabetes, which increases circulatingFFAs, leading to increased
hepatic VLDL production.
TG-rich VLDL then transfers TG and cholesterol to LDLand HDL,
promoting formation of TG-rich, small, denseLDL and clearance of
TG-rich HDL.
Diabetic dyslipidemia is often exacerbated by theincreased
caloric intake and physical inactivity that
characterize the lifestyles of some patients with DM-2. Diabetic
women may be at special risk for cardiac
disease.
-
7/25/2019 Dyslipidemia Harper CHO
20/37
Diagnosis and Screening
Measure serum lipids (lipid profile)
TC, TG, and HDL are measureddirectly
LDL is calculated or measured directly
TC and TG values reflect cholesteroland TG in all circulating
lipoproteins,including chylomicrons, VLDL, IDL,LDL, and HDL.
Diagnosis and Screening
LDL values are often calculated as the amount ofcholesterol not
contained in HDL and VLDL, where
VLDL is estimated by TG 5: LDL = TC [HDL +(TG 5)] (Friedewald
formula); valid only when TGare < 400 mg/dL and patients are
fasting
The calculated LDL value incorporates measures ofall non-HDL,
nonchylomicron cholesterol, includingthat in IDL and Lp(a)
LDL can be measured directly using plasmaultracentrifugation or
by immunoassay Direct measurement may be useful in patients
with
elevated TG to determine if LDL levels are elevated
-
7/25/2019 Dyslipidemia Harper CHO
21/37
Diagnosis and Screening
TC values may vary by 10% and TG by upto 25% even in the absence
of disease
Testing should be postponed until afterresolution of acute
illness, because TGincrease and cholesterol levels decrease
ininflammatory states
Lipid profiles are generally reliable within
the first 24 h after an AMI but then changeafterwards
Diagnosis and Screening
A fasting lipid profile (TC, TG, HDL, and calculatedLDL) should
be obtained in all adults 20 yr andshould be repeated q 5 yr
Assessment of other cardiovascular risk factors atthe time of
initial screening:
DM
Smoking
HTN FH of premature CAD - 1st-degree relative
male before age 55
female before age 65
-
7/25/2019 Dyslipidemia Harper CHO
22/37
Diagnosis and Screening
Indications for screening patients < 20yr Atherosclerotic
risk factors
DM
HTN
Smoking
Obesity
Premature CAD in a parent, grandparent, orsibling
Cholesterol level > 240 mg/dL or knowndyslipidemia in a
parent
Additional testing
Blood tests for secondary causes ofdyslipidemia should be
obtained inpatients with recently diagnoseddyslipidemia, or when a
component ofthe lipid profile has changed for the
worse: FBG, liver enzymes, creatinine, TSH,
urinary protein
-
7/25/2019 Dyslipidemia Harper CHO
23/37
Evaluation
1. Measure fasting lipoproteins2. Identify CAD or CAD
equivalents
Other atherosclerotic disease: peripheral arterial
disease,abdominal aortic aneurysm, symptomatic carotid
arterydisease
Diabetes mellitus
3. Identify major CAD risk factors Cigarette smoking
Hypertension (BP 140/90 oron antihypertensive drug) Low HDL (40
mg/dL
Family history of premature CAD - 1st-degree relativemale <
55 yrfemale < 65 yr
Age (men 45 yr, women 55 yr)
Evaluation
If 2 major risk factors are presentwithout CAD or CAD
equivalent, assess10-yr risk of MI or CAD death usingFramingham
risk tables or electroniccalculation tool
-
7/25/2019 Dyslipidemia Harper CHO
24/37
Estimation of CHD risk*
*Use internet Framingham 10-year risk calculator
Online calculation tools
http://hp2010.nhlbihin.net/atpiii/calculator.asp
http://www.mdcalc.com/framingham-coronary-heart-disease-risk-score-si-units/
http://www.medcalc.com/heartrisk.html
http://reference.medscape.com/calculato
r/framingham-coronary-risk-ldl
-
7/25/2019 Dyslipidemia Harper CHO
25/37
Lipid profile references
TC (mg/dL)
< 200 Desirable
200239 Borderline high
240 High
LDL (mg/dL)
< 100 Optimal
100129 Near optimal/above optimal
130159 Borderline high
160189 High190 Very high
Lipid profile references
HDL (mg/dL)
< 40 Low
60 High
TG (mg/dL)
< 150 Desirable
150199 Borderline high
200499 High500 Very high
-
7/25/2019 Dyslipidemia Harper CHO
26/37
Comparison of LDL Cholesterol andNon-HDL Cholesterol Goals
for
Three Risk Categories
LDL-C Goal
(mg/dL)Risk CategoryNon-HDL-C
Goal (mg/dL)
20%)
-
7/25/2019 Dyslipidemia Harper CHO
27/37
ATP III update
The treatment goal for high-riskpatients is an LDL < 100
mg/dL
Update: There is a therapeutic optionto set the goal at an
LDL
-
7/25/2019 Dyslipidemia Harper CHO
28/37
Drug therapy
Drug treatment options depend on the specific lipidabnormality,
although different lipid abnormalitiesoften coexist.
In some patients, a single abnormality may requireseveral drug
therapies
In others, a single drug treatment may be adequatefor several
abnormalities.
Treatment should always include treatment ofhypertension and
diabetes, smoking cessation, andin those with a 10-yr risk of MI or
death from CAD
of 10% (as determined from the Framinghamtables) low-dose daily
aspirin.
Drug therapy - statins
Statins are the treatment of choice for LDLreduction and
demonstrably reducecardiovascular mortality
Statins inhibit hydroxymethylglutaryl CoAreductase, a key enzyme
in cholesterolsynthesis, leading to up-regulation of LDL
receptors and increased LDL clearance They reduce LDL by up to
60% and produce
small increases in HDL and modestdecreases in TGs
-
7/25/2019 Dyslipidemia Harper CHO
29/37
Drug therapy - statins
Statins also appear to decrease intra-arterialand/or systemic
inflammation by stimulatingproduction of endothelial nitric
oxide
They may also decrease LDL deposition inendothelial macrophages
and decreasecholesterol in inflammatory cell membranes
This anti-inflammatory effect is
antiatherogenic even in the absence ofelevated lipid levels
Drug therapy - statins
Adverse effects are uncommon but include liverenzyme elevations,
and myositis or rhabdomyolysis
Muscle toxicity without enzyme elevation has alsobeen
reported
Adverse effects are more common in older patients,those with
multiple diseases, and those on multipledrugs; changing from one
statin to another orlowering the dose may relieve the problem
Muscle toxicity seems to be most common whensome of the statins
are used with drugs that inhibitcytochrome P3A4 (eg, macrolide
antibiotics, azoleantifungals, cyclosporine) and with
fibrates(especially gemfibrozil)
-
7/25/2019 Dyslipidemia Harper CHO
30/37
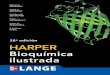
Drug therapy - fibrates
Activate PPAR (peroxisomeproliferator-activated
receptors)especially PPAR
Stimulate endothelial LPL, leading toincreased fatty acid
oxidation in the
liver and muscle and decreasedhepatic VLDL synthesis
Structurally and pharmacologicallyrelated to the
thiazolidinediones (TZD)
-
7/25/2019 Dyslipidemia Harper CHO
31/37
Drug therapy - fibrates
Reduce TGs by up to 50%
Increase HDLs by up to 20%
May cause GI adverse effects,including dyspepsia and
abdominalpain; rarely cause cholelithiasis
Potentiate muscle toxicity when usedwith statins and potentiate
the effectsof warfarin
PPAR -alpha and -gamma pathways.
-
7/25/2019 Dyslipidemia Harper CHO
32/37
Drug therapy - bile acid
sequestrants Block intestinal bile acid reabsorption,
forcing up-regulation of hepatic LDLreceptors to recruit
circulatingcholesterol for bile synthesis.
Proven to reduce cardiovascularmortality.
Usually used with statins or withnicotinic acid to augment
LDLreduction
Drug therapy - bile acidsequestrants
Drugs of choice for children andwomen who are or are planning
tobecome pregnant
Safe, but their use is limited byadverse effects of bloating,
nausea,
cramping, and constipation
They may also increase TGs, so theiruse is contraindicated in
patients withhypertriglyceridemia.
-
7/25/2019 Dyslipidemia Harper CHO
33/37
Drug therapy - bile acid
sequestrants Cholestyramine and colestipol, but not
colesevelam, interfere with absorptionof other drugsnotably
thiazides, -blockers, warfarin, digoxin, andthyroxinean effect that
can beminimized by administration 4 h
before or 1 h after other drugs Lower LDL 15-25%
Drug therapy - niacin
Most effective drug for increasing HDLs
Mechanism of action is unknown, but itappears to both increase
HDL productionand inhibit HDL clearance; it may alsomobilize
cholesterol from macrophages.
Also decreases TGs and, in doses of 1500 to
2000 mg/day, reduces LDLs Lower LDL 15-30%, lower TGs 30-40%
amd
raise HDL 15-25%
-
7/25/2019 Dyslipidemia Harper CHO
34/37
Drug therapy - niacin
Produces flushing, pruritus, and nausea;premedication with
low-dose aspirin mayprevent these adverse effects;
slow-releasepreparations cause these side effects less often
May cause liver enzyme elevations andoccasionally liver failure,
insulin resistance, andhyperuricemia and gout.
In patients with average LDL and below-
average HDL levels, niacin combined with statintreatment may be
effective in preventingcardiovascular disease
Drug therapy - ezetimibe
Inhibits intestinal absorption of cholesteroland phytosterol
Usually lowers LDL by 15-20% and causessmall increases in HDL
and a mild decreasein TGs
Can be used as monotherapy in patientsintolerant to statins or
added to statins for
patients on maximum doses with persistentLDL elevation
Adverse effects are infrequent
-
7/25/2019 Dyslipidemia Harper CHO
35/37
Drug therapy omega-3
fatty acids Omega-3 fatty acids in high doses (1 to 6 g/day
of eicosapentaenoic acid [EPA] anddocosahexaenoic acid [DHA])
can be effectivein reducing TGs
The -3 fatty acids EPA and DHA are the activeingredients in fish
oil or -3 capsules
Adverse effects include eructation and diarrhea;these may be
decreased by giving the fish oil
capsules with meals in divided doses (eg, bid ortid)
Omega-3 fatty acids can be a useful adjunct toother
therapies
Treatment of diabeticdyslipidemia
Treatment of diabetic dyslipidemia shouldalways involve
lifestyle changes, with statinsto reduce LDLs and/or fibrates to
decreaseTGs
Metformin lowers TGs, which may be areason to choose it over
other oralantihyperglycemic drugs when treating
diabetics with dyslipidemia
-
7/25/2019 Dyslipidemia Harper CHO
36/37
Treatment of diabetic
dyslipidemia Thiazolidinediones (TZDs) may increase
both HDLs and LDLs (probably the lessatherogenic large, buoyant
type of LDLs)
TZDs may decrease TGs; however, theseagents should not be chosen
over lipid-lowering drugs to treat lipid abnormalities indiabetic
patients but may be useful adjuncts
Patients with very high TG levels and lessthan optimally
controlled diabetes may havebetter response to insulin than to
oralantihyperglycemic drugs
Targets for dyslipidemiain diabetic patients
LDL
-
7/25/2019 Dyslipidemia Harper CHO
37/37