Embed Size (px)
Citation preview

Original Article
Effects of triple-drug therapy with nitazoxanide, high-doseribavirin and peginterferon-a-2a in patients with chronichepatitis C
P. Patrick Basu,1,2 Krishna Rayapudi,2 Niraj James Shah,2 Nithya Krishnaswamy2 andRobert S. Brown1
1Division of Digestive and Liver Diseases and Center for Liver Disease and Transplantation, Columbia UniversityMedical Center, New York, and 2North Shore University Hospital at Forest Hills, Forest Hills, NY, USA
Aim: The historical standard of care for patients with chronichepatitis C virus (HCV) was peginterferon (PEG IFN) and riba-virin combination therapy, yielding sustained virologicalresponse (SVR) rates of 38–52% in HCV genotype 1 patients.This study evaluated a novel three-drug regimen of nitazox-anide and high-dose ribavirin as lead-in therapy, followed byPEG IFN-a-2a in triple therapy.
Methods: A prospective, open-label pilot study was con-ducted in treatment-naive patients with HCV genotype 1.Patients received nitazoxanide 500 mg twice a day for 2weeks, then nitazoxanide plus ribavirin 1400 mg/day for 2weeks, then nitazoxanide plus ribavirin plus PEG IFN-a-2a180 mg weekly for 12 weeks, followed by ribavirin plus PEGIFN-a-2a for 12 weeks (48 weeks if HCV RNA negative afterweek 24). Primary outcome was SVR. Other outcomesincluded very rapid virological response (VRVR), rapid viro-logical response (RVR), early virological response (EVR), end-of-treatment response (ETR), and safety and tolerability.
Results: Thirty-three patients with a mean age of 46 years,detectable HCV RNA (64% with <600 000 IU/mL), and METAVIRfibrosis scores (F1:F2:F3) of 15%:49%:36% were enrolled. Out-comes were as follows: SVR, 67% (22/33); VRVR, 39% (13/33);RVR, 48% (16/33); EVR, 70% (23/33); and ETR, 67% (22/33). Mostpatients required at least one growth factor. Two patientsdiscontinued because of adverse events.
Conclusion: This three-drug regimen was effective inachieving SVR in patients with HCV genotype 1. No patientsrelapsed, and the toxicity profile was favorable. Furtherstudies on the role of nitazoxanide in the treatment of chronicHCV are warranted.
Key words: hepatitis C virus, interferon, nitazoxanide,ribavirin
INTRODUCTION
CHRONIC HEPATITIS C virus (HCV) infectionis a global public health problem, affecting up to
180 million individuals worldwide.1 Approximately20–30% of chronic carriers of HCV may develop seriouscomplications, including cirrhosis, over a period of10–30 years.2 Among patients with cirrhosis, approxi-mately 1–4% will develop hepatocellular carcinoma onan annual basis.3 Chronic HCV infection is not only theleading indication for liver transplantation, but alsothe leading cause of liver-related deaths in the USA.4 Thevast majority of patients do not spontaneously clear thevirus, but effective treatment is available that has beenshown to reduce serum HCV RNA, improve biochemicalindices of liver function, improve liver histologyand achieve a sustained virological response (SVR) inapproximately half of patients.1,5–7
Correspondence: Dr P. Patrick Basu, North Shore University Hospital,5 Station Square, Forest Hills, NY 11375, USA.Email: [email protected] contribution: P. P. B., principal investigator, patientrecruitment, patient evaluation, data collection and manuscriptpreparation; K. R., data collection, patient evaluation andmanuscript preparation; N. J. S., data collection, patientmanagement and patient follow up; N. K., data collection andpatient evaluation; R. S. B. Jr, manuscript preparation andprotocol design.Financial support: noneConflict of interest: P. P. B. has received educational grants fromSalix Pharmaceuticals and Romark Laboratories, and serves onthe advisory boards for Roche, Vertex Pharmaceuticals andGilead.Received 13 March 2012; revision 19 October 2012; accepted 23October 2012.
bs_bs_banner
Hepatology Research 2013; 43: 589–595 doi: 10.1111/hepr.12013
© 2012 The Japan Society of Hepatology 589

The goal of treatment is to prevent complications anddeath from chronic HCV infection by achieving SVR. Inthis regard, the historical standard of care has been apeginterferon (PEG IFN)-based therapy given in combi-nation with ribavirin using weight-based dosing.8 Anti-viral activity of interferon (IFN) is mediated throughinduction of multiple IFN-stimulated genes, includingdouble-stranded RNases, inhibitors of viral proteintranslation and proteins that destabilize viral messengerRNA.9,10 Additionally, IFN-a activates natural killer cells,promotes maturation of dendritic cells, causes prolifera-tion of memory T cells and prevents T-cell apoptosis. Incontrast to IFN-a, the mechanism of antiviral activity ofribavirin, an oral nucleoside analog, has not been wellestablished. Although ribavirin does not appear to havea direct effect on viral replication, it may deplete intra-cellular guanosine triphosphate and cause lethal muta-tion of virions.11,12
When PEG IFN and ribavirin have been given in com-bination for 48 weeks of treatment, overall rates of SVRhave ranged 54–63%.5–7 SVR rates are lower for patientswith HCV genotype 1 and have ranged 38–52%.1,5–7
Indeed, HCV genotype 1, black race, male sex and HCVRNA levels of more than 600 000 IU/mL are associatedwith lower response rates to PEG IFN plus ribavirincombination therapy.9,13
Various approaches to increasing SVR rates have beenexplored, including increasing the dose of ribavirin. Inone small trial, higher daily doses of ribavirin (e.g.1400–2400 mg) were associated with higher SVR rates,albeit at the expense of greater toxicity.14 Another impor-tant factor in achieving an SVR is the rate of HCV RNAreduction; indeed, the rate of HCV RNA reduction ispredictive of SVR outcomes. In a study assessing theeffect of very rapid virological response (VRVR), definedas undetectable HCV RNA at 2 weeks, an early antiviralresponse was predictive of achieving an SVR.15 As aconsequence, regimens that are highly potent in thetreatment initiation phase may be expected to providegreater efficacy, provided the regimen has an acceptabletoxicity profile.
Nitazoxanide, the first member of the thiazolide classof anti-infectives, has demonstrated antiviral activityagainst HCV.16 The agent inhibits viral protein transla-tion via the phosphorylation of dsRNA-dependentprotein kinase and has also been shown to be an IFNinducer.17 Clinical synergy with PEG IFN and ribavirinhas been demonstrated in patients with chronic HCVgenotype 4.18 In that trial, the combination of nitazox-anide, PEG IFN-a-2a and ribavirin increased the rateof SVR in patients compared with PEG IFN-a-2a plus
ribavirin (79% vs 50%; P = 0.023). The authors reportednitazoxanide was well tolerated with minimal addedtoxicity. In the current study, we hypothesized that thefollowing sequential therapy may increase the incidenceof SVR in patients with chronic HCV genotype 1: initialtherapy with nitazoxanide; followed by nitazoxanideplus high-dose ribavirin; followed by triple therapy withPEG IFN-a-2a, ribavirin and nitazoxanide; and finallyPEG IFN-a-2a plus ribavirin.
METHODS
Study design
THIS WAS A prospective, open-label, single-centerpilot study of triple-drug therapy in treatment-naive
patients with chronic HCV genotype 1 (ERAIS-C trial:Effect of High-Dose Ribavirin, Nitazoxanide [Alinia;Romark Laboratories, Tampa, FL, USA], and PegylatedIFN alfa-2a in Attaining Sustained Virologic Response inTreatment of Chronic Hepatitis C). The protocol wasapproved by the Institutional Review Board at LongIsland Jewish Hospital-Forest Hills and was performedin accordance with the Declaration of Helsinki, theInternational Conference on Harmonization GoodClinical Practice Guidelines, and applicable local lawsand regulations. Signed informed consent was obtainedfor each patient before study enrollment.
Patient populationPatients were eligible if they were 18 years of age orolder, had compensated liver disease with chronic HCVgenotype 1 infection, had detectable plasma HCV RNA,and had not received previous treatment for HCV infec-tion. Patients with uncontrolled diabetes (hemoglobinA1c of >7.5%), decompensated cirrhosis, active use ofillicit drugs, excessive alcohol intake (>40 g/day),comorbid conditions (e.g. severe depression, anemia,thrombocytopenia, HIV infection), pregnancy or poormotivation were excluded.
Triple-drug therapyPatients received 52 weeks of open-label treatment inthe following sequence (Fig. 1): nitazoxanide 500 mgtwice daily for 2 weeks, then nitazoxanide (same dose)plus ribavirin 1400 mg/day for 2 weeks, then nitazox-anide plus ribavirin (same doses) plus PEG IFN-a-2a180 mg weekly (standard dose) for 12 weeks, and thenribavirin plus PEG IFN-a-2a (same doses) for 12 weeks(up to a total of 48 weeks if HCV RNA negative afterweek 24). All patients received the 1400-mg/day dose
590 P. P. Basu et al. Hepatology Research 2013; 43: 589–595
© 2012 The Japan Society of Hepatology
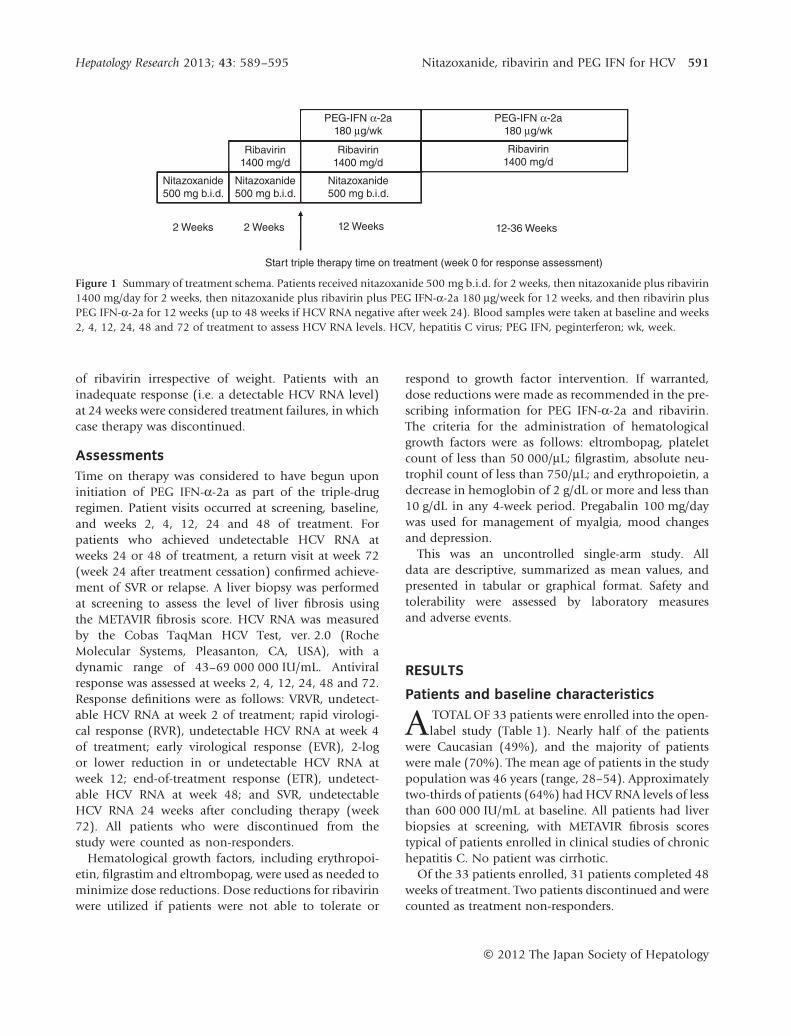
of ribavirin irrespective of weight. Patients with aninadequate response (i.e. a detectable HCV RNA level)at 24 weeks were considered treatment failures, in whichcase therapy was discontinued.
AssessmentsTime on therapy was considered to have begun uponinitiation of PEG IFN-a-2a as part of the triple-drugregimen. Patient visits occurred at screening, baseline,and weeks 2, 4, 12, 24 and 48 of treatment. Forpatients who achieved undetectable HCV RNA atweeks 24 or 48 of treatment, a return visit at week 72(week 24 after treatment cessation) confirmed achieve-ment of SVR or relapse. A liver biopsy was performedat screening to assess the level of liver fibrosis usingthe METAVIR fibrosis score. HCV RNA was measuredby the Cobas TaqMan HCV Test, ver. 2.0 (RocheMolecular Systems, Pleasanton, CA, USA), with adynamic range of 43–69 000 000 IU/mL. Antiviralresponse was assessed at weeks 2, 4, 12, 24, 48 and 72.Response definitions were as follows: VRVR, undetect-able HCV RNA at week 2 of treatment; rapid virologi-cal response (RVR), undetectable HCV RNA at week 4of treatment; early virological response (EVR), 2-logor lower reduction in or undetectable HCV RNA atweek 12; end-of-treatment response (ETR), undetect-able HCV RNA at week 48; and SVR, undetectableHCV RNA 24 weeks after concluding therapy (week72). All patients who were discontinued from thestudy were counted as non-responders.
Hematological growth factors, including erythropoi-etin, filgrastim and eltrombopag, were used as needed tominimize dose reductions. Dose reductions for ribavirinwere utilized if patients were not able to tolerate or
respond to growth factor intervention. If warranted,dose reductions were made as recommended in the pre-scribing information for PEG IFN-a-2a and ribavirin.The criteria for the administration of hematologicalgrowth factors were as follows: eltrombopag, plateletcount of less than 50 000/mL; filgrastim, absolute neu-trophil count of less than 750/mL; and erythropoietin, adecrease in hemoglobin of 2 g/dL or more and less than10 g/dL in any 4-week period. Pregabalin 100 mg/daywas used for management of myalgia, mood changesand depression.
This was an uncontrolled single-arm study. Alldata are descriptive, summarized as mean values, andpresented in tabular or graphical format. Safety andtolerability were assessed by laboratory measuresand adverse events.
RESULTS
Patients and baseline characteristics
A TOTAL OF 33 patients were enrolled into the open-label study (Table 1). Nearly half of the patients
were Caucasian (49%), and the majority of patientswere male (70%). The mean age of patients in the studypopulation was 46 years (range, 28–54). Approximatelytwo-thirds of patients (64%) had HCV RNA levels of lessthan 600 000 IU/mL at baseline. All patients had liverbiopsies at screening, with METAVIR fibrosis scorestypical of patients enrolled in clinical studies of chronichepatitis C. No patient was cirrhotic.
Of the 33 patients enrolled, 31 patients completed 48weeks of treatment. Two patients discontinued and werecounted as treatment non-responders.
PEG-IFN α-2a
180 μg/wk
PEG-IFN α-2a
180 μg/wk
Ribavirin
1400 mg/d
Ribavirin
1400 mg/dRibavirin
1400 mg/d
Nitazoxanide
500 mg b.i.d.
Nitazoxanide
500 mg b.i.d.
Nitazoxanide
500 mg b.i.d.
2 Weeks 2 Weeks 12 Weeks 12-36 Weeks
Start triple therapy time on treatment (week 0 for response assessment)
Figure 1 Summary of treatment schema. Patients received nitazoxanide 500 mg b.i.d. for 2 weeks, then nitazoxanide plus ribavirin1400 mg/day for 2 weeks, then nitazoxanide plus ribavirin plus PEG IFN-a-2a 180 mg/week for 12 weeks, and then ribavirin plusPEG IFN-a-2a for 12 weeks (up to 48 weeks if HCV RNA negative after week 24). Blood samples were taken at baseline and weeks2, 4, 12, 24, 48 and 72 of treatment to assess HCV RNA levels. HCV, hepatitis C virus; PEG IFN, peginterferon; wk, week.
Hepatology Research 2013; 43: 589–595 Nitazoxanide, ribavirin and PEG IFN for HCV 591
© 2012 The Japan Society of Hepatology

Antiviral response ratesVirological response rates, determined from the timeof initiation of triple-drug therapy, are summarized inFigure 2. Two-thirds of patients (67% [22/33]) metthe primary end-point of SVR. SVR was achieved by71% (15/21) of the patients with HCV RNA of lessthan 600 000 IU/mL at baseline compared with 58%(7/12) of the patients with HCV RNA greater than600 000 IU/mL at baseline. Early virological suppres-sion at weeks 2 and 4 of triple-drug therapy wasassociated with an SVR. No patient who achievedundetectable HCV RNA levels at weeks 2 or 4 failed to
achieve an SVR. In general, achievement of an SVR wasindependent of the time of clearance of HCV RNA; HCVRNA was later detected in only one patient among thosewho had achieved an EVR. Notably, no patient whoachieved an ETR relapsed.
TolerabilityOverall, the three-drug regimen was generally well tol-erated, with no unanticipated adverse events. The mostcommon adverse events were hematological abnormali-ties, as expected. Anemia, neutropenia and thrombocy-topenia were common, and most patients required atleast one growth factor. Sixteen patients (48%) requirederythropoietin, and 17 patients (52%) required fil-grastim. Nine patients (27%) required both erythropoi-etin and filgrastim. Thirteen patients (39%) receivedeltrombopag for thrombocytopenia. Macular skin rashwas observed in nine patients (27%). Eleven patients(33%) required pregabalin for myalgia, mood changesand mild depression. Of the 33 patients enrolled, 31(94%) and 31 (94%) were adherent (i.e. received 380%of scheduled doses) to ribavirin and PEG IFN-a-2a treat-ment, respectively.
One patient discontinued because of adverse events(i.e. fatigue, severe anemia, rash and hair loss), and onepatient was lost to follow up.
DISCUSSION
DESPITE HAVING A well-established clinical profilein the treatment of patients with chronic hepatitis
C, historical antiviral responses to standard therapywith PEG IFN given in conjunction with ribavirin aresuboptimal. This study was conducted with the goal ofimproving antiviral response rates achieved with stan-dard therapy through incorporation of nitazoxanide(with a novel mechanism of action) in conjunction withhigh-dose ribavirin and standard-dose PEG IFN-a-2a. Instandard in vitro antiviral assays, nitazoxanide exhibitedpotent inhibition of HCV replication.16 Additionally,pretreatment of HCV replicon–containing cells withnitazoxanide enhanced the subsequent effects of IFN,suggesting potential synergy between the drugs. Thepotential for clinical potentiation was tested and vali-dated in a study of nitazoxanide, PEG IFN-a-2a, andribavirin in patients with HCV genotype 4 infection.18 Inthat study, triple-drug therapy was associated with anSVR of 79%, compared with 50% for standard PEGIFN-a-2a plus ribavirin (P = 0.023).
In the current study of triple-drug therapy in patientswith HCV genotype 1, we observed a higher rate of SVR
Table 1 Baseline demographic and disease characteristics
Parameter Patients (n = 33)
Age, mean (range), years 46 (28–54)Male, n (%) 23 (70)Race, n (%)
White 16 (49)Black 5 (15)Asian 6 (18)Hispanic 6 (18)
BMI, mean (range) 28 (25–31)HCV RNA level, n (%)
<600 000 IU/mL 21 (64)>600 000 IU/mL 12 (36)
METAVIR fibrosis score, n (%)F1 5 (15)F2 16 (49)F3 12 (36)
BMI, body mass 2index; HCV, hepatitis C virus.
100
90
80
70
60
50
40
30
20
10
0VRVR RVR EVR SVRETR
39
48
7067 67
Re
sp
on
se
ra
te,
%
Figure 2 Summary of antiviral responses to triple-drugtherapy. Response rates are shown for 33 patients enrolled inthe study. ETR, end-of-treatment response; EVR, early virologi-cal response; RVR, rapid virological response; SVR, sustainedvirological response; VRVR, very rapid virological response.
592 P. P. Basu et al. Hepatology Research 2013; 43: 589–595
© 2012 The Japan Society of Hepatology

than that in previous studies of standard PEG IFN plusribavirin for patients with chronic hepatitis C genotype1 (67% vs a range of 38%-52%, respectively).1,5–7
However, it may be argued that the higher rate of SVRobserved in our study was due to the use of high-doseribavirin and hematological growth factors rather thanthe addition of nitazoxanide to the treatment regimen.This is unlikely as the SVR rate reported here was higherthan that observed in a previous study of patients withHCV genotype 1 receiving PEG IFN plus high-dose rib-avirin and epoetin (49%).19 Notably, treatment withepoetin in this previous study was not associated withincreased rates of SVR, although the use of high-doseribavirin was.
The benefit of triple-drug therapy reported here isconsistent with that observed in treatment-naivepatients with HCV genotype 418 but higher than ratesobserved in patients with HCV genotype 1 in anotherstudy.20 In the latter study, triple therapy achieved anSVR of 44% compared with 32% for PEG IFN andribavirin; however, this study had problems with enroll-ment, which appeared to significantly impact bothregimens. When the data were analyzed for siteswith customary standard-of-care response rates, tripletherapy achieved an SVR rate of 57% compared with42% for PEG IFN and ribavirin. In this study, the highrate of SVR was associated with a VRVR and an RVR, aspatients who cleared HCV RNA early went on to achievean SVR. Patients who achieved an ETR sustained theresponse at week 72, with no patient relapsing. Thisfinding is unique among trials, which have reported thatapproximately 19% (all genotypes) to 32% (genotype1) of patients who achieved an ETR on PEG IFN plusribavirin went on to relapse during the 24-week post-treatment period.1,5 In a study of patients with HCVgenotype 4, the relapse rate among patients randomizedto triple therapy was 4% (1/23), compared with 33%(10/30) of patients who received standard therapy ofPEG IFN-a-2a plus ribavirin.18 Although the explanationfor the low relapse rate is unclear, it may be related tothe rapid rate of viral elimination and, in part, to thelack of development of HCV resistance to nitazox-anide.21 The ultimate long-term efficacy of this regimenwill be elucidated with subsequent SVR analysis.
The overall side-effect profile appeared to be consis-tent with the use of combination PEG IFN andribavirin,1,5–7 with nitazoxanide yielding no unantici-pated toxicity. Rossignol et al.18 have previously com-mented on a possible explanation for the low toxicity ofnitazoxanide. Briefly, the mechanism of action of nita-zoxanide – protein kinase induction – targets only those
cells infected with HCV, having no effect on uninfectedcells.17 Ultimately, the agent may improve the overallsafety outcomes by reducing the duration of therapyfrom 48 weeks. Further studies are under way to testdifferent treatment durations.
There were several limitations to this study, includinga relatively small population size and the lack of a com-parative study group. In addition, we assessed antiviralresponse rates beginning from the initiation of PEGIFN-a-2a as part of a triple-drug regimen, which doesnot readily align with the assessment schedule forresponse rates reported in the IDEAL study1 and otherstudies of PEG IFN plus ribavirin regimens.6,7,13 In thecurrent study, patients received 4 weeks of antiviraltherapy with nitazoxanide and 2 weeks of high-doseribavirin before the initiation of PEG IFN (week 0 forthe response assessment period). Additionally, becauseof the study design, it was difficult to determine to whatextent high-dose ribavirin and nitazoxanide contributedto the higher apparent SVR. Further, there is littleclinical evidence pertaining to how long nitazoxanideshould be given; patients may have achieved better orworse antiviral activity depending on the duration ofnitazoxanide. In the study by Rossignol et al.,18 nitazox-anide lead-in time before triple-drug therapy was 12weeks compared with 4 weeks in our study. We basedthis 4-week lead-in period on a subsequent study byRossignol et al.22 in which virological response was notfound to be compromised by reducing the lead-inperiod from 12 to 4 weeks. Additionally, in our study,nitazoxanide was given for a total of 16 weeks, a some-what arbitrary and different cut-off compared with otherstudies in which nitazoxanide was continued for theduration of treatment with PEG IFN plus ribavirin.18,22
Finally, we did not examine patients or HCV samples forthe presence of mutations that have been associatedwith response to PEG IFN and ribavirin treatment (e.g.IL-28B locus host mutations and viral mutations in theNS5A IFN sensitivity-determining region, NS5A IFN/ribavirin resistance-determining region and core aminoacids [e.g. amino acid 70]).23
Since the time this study was initiated, two membersof a new class of drugs called serine protease inhibitors(boceprevir [VictrelisT; Schering, Whitehouse Station,NJ, USA] and telaprevir [Incivek; Vertex Pharmaceuti-cals, Cambridge, MA, USA]) have been approved for thetreatment of chronic HCV when combined with PEGIFN and ribavirin.24,25 Clinical trials with these agentsindicate a substantial increase in SVR when used incombination with PEG IFN and ribavirin comparedwith PEG IFN and ribavirin alone. This increase in SVR
Hepatology Research 2013; 43: 589–595 Nitazoxanide, ribavirin and PEG IFN for HCV 593
© 2012 The Japan Society of Hepatology

is also associated with a substantial degree of additionaltoxicity. No in vivo studies with nitazoxanide in combi-nation with either boceprevir or telaprevir have beenperformed. However, in vitro studies indicate that nita-zoxanide is synergistic in combination with proteaseinhibitors (e.g. telaprevir, boceprevir and danoprevir),maintains activity against protease inhibitor-resistantmutants and prevents the emergence of telaprevir-resistant mutants.16,26,27 Based on the known in vitrodata with nitazoxanide and telaprevir,16,26,27 and nitazox-anide’s relatively low toxicity profile,18 clinical studies ofthese agents in combination with PEG IFN and ribavirinshould be considered.
Recognizing these study limitations, clearly this novelregimen requires further investigation in a randomized,multicenter setting. The key findings of a 67% SVR rateand the absence of relapse, without any apparent addedtoxicity, are intriguing. Additionally, potentially reduc-ing the duration of therapy while still maintaining ahigh SVR rate is a goal well worth pursuing.
ACKNOWLEDGMENTS
THE AUTHORS OF this study would like to thankEmmet Keeffe, M.D., and Matthew Bardin, PharmD,
for their guidance and technical assistance. Editorial andwriting assistance was provided by MedThink SciComunder the direction of the authors with support fromSalix Pharmaceuticals.
REFERENCES
1 McHutchison JG, Lawitz EJ, Shiffman ML et al. for theIDEAL Study Team. Peginterferon alfa-2b or alfa-2a withribavirin for treatment of hepatitis C infection. N Engl JMed 2009; 361: 580–93.
2 Thomas DL, Seeff LB. Natural history of hepatitis C. ClinLiver Dis 2005; 9: 383–98. vi.
3 Fattovich G, Stroffolini T, Zagni I, Donato F. Hepatocellu-lar carcinoma in cirrhosis: incidence and risk factors. Gas-troenterology 2004; 127 (5 Suppl 1): S35–50.
4 Kim WR. The burden of hepatitis C in the United States.Hepatology 2002; 36 (5 Suppl 1): S30–4.
5 Fried MW, Shiffman ML, Reddy KR et al. Peginterferonalfa-2a plus ribavirin for chronic hepatitis C virus infec-tion. N Engl J Med 2002; 347: 975–82.
6 Hadziyannis SJ, Sette H, Morgan TR et al. Peginterferon-alpha2a and ribavirin combination therapy in chronichepatitis C: a randomized study of treatment duration andribavirin dose. Ann Intern Med 2004; 140: 346–55.
7 Manns MP, McHutchison JG, Gordon SC et al. Peginter-feron alfa-2b plus ribavirin compared with interferon
alfa-2b plus ribavirin for initial treatment of chronichepatitis C: a randomised trial. Lancet 2001; 358: 958–65.
8 Ghany MG, Strader DB, Thomas DL, Seeff LB. Diagnosis,management, and treatment of hepatitis C: an update.Hepatology 2009; 49: 1335–74.
9 Hoofnagle JH, Seeff LB. Peginterferon and ribavirin forchronic hepatitis C. N Engl J Med 2006; 355: 2444–51.
10 Tilg H. New insights into the mechanisms of interferonalfa: an immunoregulatory and anti-inflammatory cytok-ine. Gastroenterology 1997; 112: 1017–21.
11 Crotty S, Maag D, Arnold JJ et al. The broad-spectrum anti-viral ribonucleoside ribavirin is an RNA virus mutagen. NatMed 2000; 6: 1375–9.
12 Maag D, Castro C, Hong Z, Cameron CE. Hepatitis C virusRNA-dependent RNA polymerase (NS5B) as a mediator ofthe antiviral activity of ribavirin. J Biol Chem 2001; 276:46094–8.
13 Feld JJ, Hoofnagle JH. Mechanism of action of interferonand ribavirin in treatment of hepatitis C. Nature 2005; 436:967–72.
14 Lindahl K, Stahle L, Bruchfeld A, Schvarcz R. High-doseribavirin in combination with standard dose peginterferonfor treatment of patients with chronic hepatitis C. Hepatol-ogy 2005; 41: 275–9.
15 Neumann AU, Pianko S, Zeuzem S et al. Positive and nega-tive prediction of sustained virologic response at weeks 2and 4 of treatment with albinterferon alfa-2b or peginter-feron alfa-2a in treatment-naive patients with genotype 1,chronic hepatitis C. J Hepatol 2009; 51: 21–8.
16 Korba BE, Montero AB, Farrar K et al. Nitazoxanide, tizox-anide and other thiazolides are potent inhibitors of hepa-titis B virus and hepatitis C virus replication. Antiviral Res2008; 77: 56–63.
17 Elazar M, Liu M, McKenna SA et al. The anti-hepatitis Cagent nitazoxanide induces phosphorylation of eukaryoticinitiation factor 2alpha via protein kinase activated bydouble-stranded RNA activation. Gastroenterology 2009;137: 1827–35.
18 Rossignol J-F, Elfert A, El-Gohary Y, Keeffe EB. Improvedvirologic response in chronic hepatitis C genotype 4treated with nitazoxanide, peginterferon, and ribavirin.Gastroenterology 2009; 136: 856–62.
19 Shiffman ML, Salvatore J, Hubbard S et al. Treatment ofchronic hepatitis C virus genotype 1 with peginterferon,ribavirin, and epoetin alpha. Hepatology 2007; 46: 371–9.
20 Bacon BR, Shiffman ML, Lim JK, Berman A, Rustgi VK,Keefe EB. A phase II, randomized, double-blind, placebo-controlled study of nitazoxanide plus peginterferonand ribavirin in naïve patients with chronic hepatitisC genotype 1 infection: final report [AGA abstract].Gastroenterology 2010; 139: e18.
21 Korba BE, Elazar M, Lui P, Rossignol J-F, Glenn JS. Poten-tial for hepatitis C virus resistance to nitazoxanide or tizox-anide. Antimicrob Agents Chemother 2008; 52: 4069–71.
594 P. P. Basu et al. Hepatology Research 2013; 43: 589–595
© 2012 The Japan Society of Hepatology

22 Rossignol JF, Elfert A, Keeffe EB. Treatment of chronichepatitis C using a 4-week lead-in with nitazoxanide beforepeginterferon plus nitazoxanide. J Clin Gastroenterol 2010;44: 504–9.
23 Chayama K, Hayes CN. Hepatitis C virus: how geneticvariability affects pathobiology of disease. J GastroenterolHepatol 2011; 26 (Suppl 1): 83–95.
24 INCIVEK. (telaprevir) Prescribing Information. Cambridge,MA: Vertex Pharmaceuticals, Inc, 2011.
25 VICTRELIS. (boceprevir) Prescribing Information. White-house Station, NJ: Schering Corp, 2011.
26 Korba B, Elazar M, Liu P, Glenn JS, Rossignol J-F. Potentialrole for nitazoxanide in combination with STAT-C agentsfor the inhibition of HCV replication without the develop-ment of resistance [AASLD abstract 115]. Hepatology 2008;48 (Suppl 1): 356A.
27 Korba B, Farrar KE, Yon C. Nitazoxanide exhibits synergywith HCV protease inhibitors and prevents the emergenceof telaprevir-resistant HCV mutants in combination treat-ments in cell culture [AASLD abstract 377]. Hepatology2011; 54 (Suppl 1): 546A.
Hepatology Research 2013; 43: 589–595 Nitazoxanide, ribavirin and PEG IFN for HCV 595
© 2012 The Japan Society of Hepatology





























