Embed Size (px)
Citation preview


SÍNDROME ANTIFOSFOLÍPIDO
Enfermedad autoinmune de afectación multisistémica caracterizada portrombosis vascular (arterial y venosa) y/o complicaciones obstétricas enpresencia de AAF, resultado de la interacción de factores ambientales,hormonales y genéticos (HLA DR4, DRw53, genes IRF5 y STAT4).
AAF+ condición necesaria, pero no suficiente para inducir lasmanifestaciones clínicas, es necesario un factor desencadenante“second-hit model”

Incidencia SAF 5 casos /105/año; prevalencia 40-50 casos/105
SAF catastrófico < 1% de todos los casos de SAF.
Nat Rev Dis Primers. 2018
Enfermedad rara según la definición de Orphanet (1/2000)
Prevalencia de AAF en diferentes situaciones clínicas (%)
Anticoagulante lúpico
Anti- cardiolipina Anti-β2 glicoproteína 1
Sanos 1-5 0.1-5 3
Trombosis venosa 1-16 4-24 5-10
Trombosis arterial 4-18 0.1-24 3-18
Abortos 7-12 3-16 2-8LES 15-34 12-44 10-19
Sexo femenino, edad 30-40 años, 60% no asociado a otra patología, 30 %asociado a LES y 10% a otras entidades (Sjögren, AR, esclerodermia,vasculitis, polimialgia reumática )

1Limper M, et al. RMD Open 2018;0:e000785. doi:10.1136/rmdopen-2018-000785
REVIEW
Antiphospholipid syndrome: state of the art on clinical practice guidelines
Marteen Limper,1 Carlo Alberto Scirè,2 Rosaria Talarico,3 Zahir Amoura,4 Tadej Avcin,5 Martina Basile,6 Gerd Burmester,7 Linda Carli,3 Ricard Cervera,8 Nathalie Costedoat-Chalumeau,9 Andrea Doria,10 Thomas Dörner,7 João Eurico Fonseca,11 Ilaria Galetti,12 Eric Hachulla,13 David Launay,13 Filipa Lourenco,14 Carla Macieira,11 Pierluigi Meroni,15 Carlo Maurizio Montecucco,16 Maria Francisca Moraes-Fontes,14 Luc Mouthon,9 Cecilia Nalli,17 Veronique Ramoni,16 Maria Tektonidou,18 Jacob M van Laar,1 Stefano Bombardieri,19 Matthias Schneider,20 Vanessa Smith,21,22 Ana Vieira,23 Maurizio Cutolo,24 Marta Mosca,3,25 Angela Tincani17
To cite: Limper M, Scirè CA, Talarico R, et al. Antiphospholipid syndrome: state of the art on clinical practice guidelines. RMD Open Published Online First: [please include Day Month Year]. doi:10.1136/rmdopen-2018-000785
Received 1 August 2018Revised 23 August 2018Accepted 28 August 2018
For numbered affiliations see end of article.
Correspondence toAngela Tincani; angela. tincani@ unibs. it
Autoimmunity
© Author(s) (or their employer(s)) 2018. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
ABSTRACTAntiphospholipid syndrome (APS) is a rare disease characterised by venous and/or arterial thrombosis, pregnancy complications and the presence of specific autoantibodies called antiphospholipid antibodies. This review aims to identify existing clinical practice guidelines (CPG) as part of the ERN ReCONNET project, aimed at evaluating existing CPGs or recommendations in rare and complex diseases. Seventeen papers providing important data were identified; however, the literature search highlighted the scarceness of reliable clinical data to develop CPGs. With no formal clinical guidelines in place, diagnosis and treatment of APS is largely based on consensus and expert opinion. Patients’ unmet need refers to the understanding of the disease and its clinical picture and implications, the need of education for patients, family members and healthcare providers, as well as to the development of monitoring pathways involving multiple healthcare providers.
INTRODUCTIONAntiphospholipid syndrome (APS) is a systemic autoimmune disease with the highest prevalence in women of childbearing age, characterised by venous and/or arterial thrombosis, pregnancy complications and the presence of specific autoantibodies called antiphospholipid (aPL) antibodies. APS is a rare disease; although accurate figures for incidence and prevalence are lacking, it is generally considered to fall within the Orphanet definition of rare disease, being a disease not affecting more than 1 person per 2000 (https://www. orpha. net/ consor4. 01/ www/ cgi- bin/ Disease. php? lng= EN). Due to its low prevalence, not many randomised, controlled clinical trials have been under-taken. This review aims to identify all existing
clinical guidelines on APS, to integrate possible recommendations and to identify unmet needs with regard to diagnosis and management of APS. This work has been driven by the ERN ReCONNET team that performed the literature research and assisted the authors during the whole search process. In addition, ERN ReCONNET allowed for the first time, at least to our knowledge, to write a manuscript including both patients and physicians’ opinions about the disease and its management.
METHODSWe carried out a systematic search in PubMed and Embase based on controlled terms (MeSH and Emtree) and keywords of the disease and publication type (clinical prac-tice guidelines (CPG)). We reviewed all the published articles in order to identify existing CPGs on diagnosis, monitoring and treat-ment, according to the Institute of Medi-cine 2011 definition (CPGs are statements that include recommendations intended to optimise patient care that are informed by a systematic review of evidence and an assess-ment of the benefits and harms of alternative care options).
The disease coordinator of the ERN ReCONNET for APS has assigned the work on CPGs to the healthcare providers (HCP) involved. This publication was funded by the European Union’s Health Programme (2014-2020), Framework Partnership Agree-ment number: 739531 – ERN ReCONNET. The content of this publication represents the views of the authors only and it is their
on 18 October 2018 by guest. Protected by copyright.http://rm
dopen.bmj.com
/RM
D Open: first published as 10.1136/rmdopen-2018-000785 on 18 October 2018. Downloaded from
1Limper M, et al. RMD Open 2018;0:e000785. doi:10.1136/rmdopen-2018-000785
REVIEW
Antiphospholipid syndrome: state of the art on clinical practice guidelines
Marteen Limper,1 Carlo Alberto Scirè,2 Rosaria Talarico,3 Zahir Amoura,4 Tadej Avcin,5 Martina Basile,6 Gerd Burmester,7 Linda Carli,3 Ricard Cervera,8 Nathalie Costedoat-Chalumeau,9 Andrea Doria,10 Thomas Dörner,7 João Eurico Fonseca,11 Ilaria Galetti,12 Eric Hachulla,13 David Launay,13 Filipa Lourenco,14 Carla Macieira,11 Pierluigi Meroni,15 Carlo Maurizio Montecucco,16 Maria Francisca Moraes-Fontes,14 Luc Mouthon,9 Cecilia Nalli,17 Veronique Ramoni,16 Maria Tektonidou,18 Jacob M van Laar,1 Stefano Bombardieri,19 Matthias Schneider,20 Vanessa Smith,21,22 Ana Vieira,23 Maurizio Cutolo,24 Marta Mosca,3,25 Angela Tincani17
To cite: Limper M, Scirè CA, Talarico R, et al. Antiphospholipid syndrome: state of the art on clinical practice guidelines. RMD Open Published Online First: [please include Day Month Year]. doi:10.1136/rmdopen-2018-000785
Received 1 August 2018Revised 23 August 2018Accepted 28 August 2018
For numbered affiliations see end of article.
Correspondence toAngela Tincani; angela. tincani@ unibs. it
Autoimmunity
© Author(s) (or their employer(s)) 2018. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
ABSTRACTAntiphospholipid syndrome (APS) is a rare disease characterised by venous and/or arterial thrombosis, pregnancy complications and the presence of specific autoantibodies called antiphospholipid antibodies. This review aims to identify existing clinical practice guidelines (CPG) as part of the ERN ReCONNET project, aimed at evaluating existing CPGs or recommendations in rare and complex diseases. Seventeen papers providing important data were identified; however, the literature search highlighted the scarceness of reliable clinical data to develop CPGs. With no formal clinical guidelines in place, diagnosis and treatment of APS is largely based on consensus and expert opinion. Patients’ unmet need refers to the understanding of the disease and its clinical picture and implications, the need of education for patients, family members and healthcare providers, as well as to the development of monitoring pathways involving multiple healthcare providers.
INTRODUCTIONAntiphospholipid syndrome (APS) is a systemic autoimmune disease with the highest prevalence in women of childbearing age, characterised by venous and/or arterial thrombosis, pregnancy complications and the presence of specific autoantibodies called antiphospholipid (aPL) antibodies. APS is a rare disease; although accurate figures for incidence and prevalence are lacking, it is generally considered to fall within the Orphanet definition of rare disease, being a disease not affecting more than 1 person per 2000 (https://www. orpha. net/ consor4. 01/ www/ cgi- bin/ Disease. php? lng= EN). Due to its low prevalence, not many randomised, controlled clinical trials have been under-taken. This review aims to identify all existing
clinical guidelines on APS, to integrate possible recommendations and to identify unmet needs with regard to diagnosis and management of APS. This work has been driven by the ERN ReCONNET team that performed the literature research and assisted the authors during the whole search process. In addition, ERN ReCONNET allowed for the first time, at least to our knowledge, to write a manuscript including both patients and physicians’ opinions about the disease and its management.
METHODSWe carried out a systematic search in PubMed and Embase based on controlled terms (MeSH and Emtree) and keywords of the disease and publication type (clinical prac-tice guidelines (CPG)). We reviewed all the published articles in order to identify existing CPGs on diagnosis, monitoring and treat-ment, according to the Institute of Medi-cine 2011 definition (CPGs are statements that include recommendations intended to optimise patient care that are informed by a systematic review of evidence and an assess-ment of the benefits and harms of alternative care options).
The disease coordinator of the ERN ReCONNET for APS has assigned the work on CPGs to the healthcare providers (HCP) involved. This publication was funded by the European Union’s Health Programme (2014-2020), Framework Partnership Agree-ment number: 739531 – ERN ReCONNET. The content of this publication represents the views of the authors only and it is their
on 18 October 2018 by guest. Protected by copyright.
http://rmdopen.bm
j.com/
RMD O
pen: first published as 10.1136/rmdopen-2018-000785 on 18 O
ctober 2018. Downloaded from
Limper M, Scirè CA, Talarico R et al. RMD Open. BMJ; 2018;4(Suppl 1)
Áreas de incertidumbre
• Test de laboratorio y su estandarización.• Profilaxis primaria.• Tratamiento trombosis.• Manifestaciones clínicas no incluidas en los
criterios de clasificación.• Manejo de la gestación y sus complicaciones.• SAF catastrófico.
APS ACTION red internacional de investigación (registro on line)

Criterios clínicosTrombosis vascular
• Uno o más episodios clínicos de trombosis arterial, venosa o de pequeño vaso, en algún órgano o tejido.
Patología obstétrica• 1 o más muertes fetales (> 10ª s) con morfología fetal normal (eco o examen directo).• Uno o más prematuros (<34ª s) por eclampsia, pre-eclampsia o insuficiencia placentaria.• 3 o más abortos espontáneos (<10ª s) consecutivos excluyendo anormalidades anatómicas
u hormonales y causas cromosómicas maternas y paternas.
2006
Criterios biológicosAnticoagulante lúpico
• En 2 o más ocasiones, separadas 12 semanas, detectado según las recomendaciones de laISTH.
aCL IgG o IgM• Títulos altos/medios (>40 GPL/MPL o > p 99th) en más de 2 determinaciones al menos
separadas 12 semanas con ELISA estandarizado.Anti-β2GPI IgG o IgM
• (> p 99th) en más de 2 determinaciones separadas 12 semanas con ELISA estandarizado.
Se precisa un criterio clínico y otro biológico)

Ictus (20%) AIT (11%)Amaurosis fugazTrombosis arteria/vena retina
Microinfartos simulando EM Déficitcognitivo, cambios sub-corticales en lasustancia blanca. Sd Guillen-BarréCorea, Migraña (20%) EpilepsiaMielopatía transversa
MANIFESTACIONES CLÍNICAS
Embolismo pulmonar (14.1%)Hipertensión pulmonar Hemorragia pulmonar alveolar
Infarto miocardio, anginaVegetaciones y engrosamiento valvular(11.6%)Trombosis vena/arteria renal.Microangiopatía trombótica. NefropatiaInsuficiencia adrenal por infartohemorrágico
Trombosis portalSíndrome de Budd Chiari
Morbilidad obstétrica
Livedo reticularis (24%),Raynaud
Osteonecrosis,artralgias
Gangrena digital
Trombosis venosa profunda (39%)Tromboflebitis superficial (11.7%)Trombocitopenia (29.6%), AHAI
Ulceras isquémicas, lesionespseudovasculiticas.
Adaptada de Nat Rev Dis Primers. 2018Cervera, R. et al Ann. Rheum. Dis. 74, 1011–1018 (2015).

AUTOIMMUNITY REVIEWS, 14 (5), 2015,
reported complement activation by aPL in arterial thrombosis in both the circulation and the arterial wall for the first time.
The current hypothesis suggests that the classi-cal complement pathway is persistently activated in patients with APS, but is generally halted at comple-ment protein C3 (REF. 46). However, when complement activation is accelerated, usually by second-hit triggers, inhibition is overcome and complement protein C5a is produced. Unfortunately, this model does not answer the question of whether immune complexes contain-ing aPL are the initiators of complement activation. To date, agents able to block complement activation (such as eculizumab, a monoclonal antibody directed against complement protein C5) have only been used in select cases of relapsing and/or refractory APS or catastrophic APS52–54, and in patients with APS who have severe renal involvement55–58. In line with these preliminary positive results, complement inhibition was able to prevent re- thrombosis in a patient with APS following arterial surgery51. Further research is needed to fully elucidate the role of complement activation in thrombotic APS, potentially paving the way for new therapeutic strategies, including use of complement inhibitors35.
Extra-criteria aPLData that have emerged in the past few years suggest that several autoantibodies outside of those included in the APS classification criteria (anticardiolipin (aCL) antibodies, lupus anticoagulant (LAC) and anti- β2GPI antibodies) could be relevant to APS pathogen-esis12. Extra-criteria aPL have a range of specificities,
binding to various targets: domains of β2GPI not tar-geted by classic anti-β2GPI antibodies; plasma proteins involved in the coagulation cascade (such as prothrom-bin or phosphatidylserine– prothrombin complexes); and annexin A5 (REF. 16). The clinical role of extra-criteria aPL, in particular their role in thrombotic risk assessment, is still under debate.
IgA antibody isotypes. IgA isotypes of aPL are not cur-rently part of routine diagnostic testing for APS and the role of IgA as a diagnostic marker for APS is still a matter of debate59–65. The evidence available to support testing for IgA aPL isotypes mainly comprises data from retrospective studies59–65, an important limitation for generating evidence-based recommendations16. Other limitations include the heterogeneity of the study popu-lations, the design of the studies, the assays used and the cut-off values used to define aPL positivity. Furthermore, some of these studies failed to demonstrate enhanced diagnostic accuracy by the addition of testing for IgA aCL antibodies and IgA anti-β2GPI antibodies to the routine tests65, potentially because IgA isotypes coexist with other routinely measured aPL and because of the low prevalence of IgA isotypes.
A study from 2013 (REF. 66) suggested that isolated IgA anti-β2GPI antibodies might be useful in identi-fying patients with clinical features of APS who tested negative for IgG and IgM aPL isotypes. The authors recommended that IgA isotypes could be tested for when patients are negative for other aPL and APS is strongly suspected; however, of the 5,892 patient sam-ples tested in this study, only 57 (<1%) were positive for IgA anti-β2GPI antibodies alone, limiting the usefulness of these recommendations to a very select population of patients. In 2016, results from an observational, multi-centre cohort study revealed the utility of IgG, IgM and IgA assays for aCL antibodies, standard anti-β2GPI anti- bodies and autoantibodies to domain 1 of β2GPI (anti-β2GPI-D1 antibodies) in the diagnosis of APS67. By analysing serum samples from patients with APS (n = 111), patients with SLE but not APS (n = 119) and healthy individuals (n = 200), the authors showed that although assays for all antibody isotypes were specific for APS, IgA anti-β2GPI antibodies had a better speci-ficity for APS than IgM anti-β2GPI antibodies (HR 33.9 (10.5–109.5) and HR 9.2 (4.6–18.4), respectively)67. Variability between assays could account for some of the differences between these studies, as well as for the lack of consensus as to the clinical relevance of IgA test-ing60,68. The lack of well-designed prospective studies raises doubts as to the usefulness of testing for IgA aPL when assessing the risk of thrombosis in patients with APS. Testing for IgA aPL should enhance thrombotic risk assessment only under certain circumstances, such as when clinical signs and symptoms of APS are present (usually in association with SLE), and tests for standard aPL are negative16.
Antiprothrombin antibodies. Antibodies against pro-thrombin represent a novel biomarker for thrombosis and pregnancy morbidity in patients with suspected APS.
Box 2 | Main findings of the aPL Task Force on Clinical Manifestations
Below is a summary of the main findings of a review of the quality of evidence and available data for antiphospholipid antibodies (aPL), as presented at the 14th International Antiphospholipid Congress in Rio de Janeiro in 2014 (REFS 15,16).
Superficial vein thrombosis (SVT)Low overall quality of evidence to support the suggestion that SVT is a result of antiphospholipid antibodies (aPL) or antiphospholipid syndrome (APS), unless other features of APS are present15.
ThrombocytopeniaLow quality of evidence to support the inclusion of thrombocytopenia as a main clinical feature of APS in the classification criteria for APS. Thrombocytopenia does not reduce the risk of future thrombosis15.
aPL-related nephropathyModerate quality of evidence to support the inclusion of biopsy-confirmed aPL-related nephropathy in the classification criteria for APS146,147.
Valvular heart disease (VHD)Moderate quality of evidence to support the inclusion of VHD in the APS classification criteria15.
Livedo reticularisModerate quality of evidence to support the inclusion of livedo reticularis in the APS classification criteria15.
Neurological manifestationsNeurological manifestations such as migraine, myelitis, seizures and chorea were analysed separately by the task force. There was moderate overall quality of evidence to support the suggestion that chorea and longitudinal myelitis, but not migraine or seizures, should be included in the APS classification criteria15.
REV IEWS
552 | SEPTEMBER 2017 | VOLUME 13 www.nature.com/nrrheum
ǟɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ ǟ
ɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ
Livedo reticularis, corea y mielitistransversa, nefropatía y valvulopatíacardiaca.
The relevance of "non-criteria" clinical manifestations of antiphospholipid syndrome: 14th International Congress on Antiphospholipid Antibodies Technical Task Force Report on Antiphospholipid SyndromeClinical Features. Abreu MM1, Danowski A2, Wahl DG3, Amigo MC4, Tektonidou M5, Pacheco MS2, Fleming N6, Domingues V7, Sciascia S8, Lyra JO9, Petri M10, Khamashta M11, Levy RA12.
1Disciplina de Reumatologia, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil. Electronic address: [email protected]. 2Serviço de Reumatologia, Hospital do Servidor Estadual do Rio de Janeiro, Rio de Janeiro, Brazil. 3Vascular Medicine Division and Regional Competence Centre For Rare Vascular and Systemic Autoimmune Diseases, Centre Hospitalier Universitaire (CHU), Nancy, France; Institut Lorrain du Coeur et des Vaisseaux Louis Mathieu, Vandoeuvre-les-Nancy, France; Institut National de la Santé et de la Recherche Médicale (INSERM), U1116, Vandoeuvre-les-Nancy Cedex, France. 4ABC Medical Center, México City, Mexico. 5First Department of Internal Medicine, University of Athens, Athens, Greece. 6Pedro Ernesto University Hospital of the Universidade do Estado do Rio de Janeiro, Rio de Janeiro, Brazil. 7New York Presbyterian Hospital, Weill Cornell Medical College, New York, NY, USA. 8Centro di Ricerche di Immunopatologia e Documentazione su Malattie Rare and Università di Torino, Dipartimento di Scienze Cliniche e Biologiche, Torino, Italy; Graham Hughes Lupus Research Laboratory, King's College London, London, UK. 9Rio de Janeiro Municipality, Rio de Janeiro, Brazil. 10Johns Hopkins University School of Medicine, Baltimore, USA. 11Lupus Research Unit at St Thomas' Hospital, London, UK. 12Discipline of Rheumatology, Universidade do Estado do Rio de Janeiro, Rio de Janeiro, Brazil.
Abstract The purpose of this task force was to critically analyze nine non-criteria manifestations of APS to support their inclusion as
APS classification criteria. The Task Force Members selected the non-criteria clinical manifestations according to
their clinical relevance, that is, the patient-important outcome from clinician perspective. They included superficial vein
thrombosis, thrombocytopenia, renal microangiopathy, heart valve disease, livedo reticularis, migraine, chorea, seizures and
myelitis, which were reviewed by thisInternational Task Force collaboration, in addition to the seronegative APS (SN-APS).
GRADE system was used to evaluate the quality of evidence of medical literature of each selected item. This critical appraisal
exercise aimed to support the debate regarding theclinical picture of APS. We found that the overall GRADE analysis was
very low for migraine and seizures, low for superficial venous thrombosis, thrombocytopenia, chorea, longitudinal myelitis
and the so-called seronegative APS and moderate for APS nephropathy, heart valve lesions and livedo reticularis. The next
step can be a critical redefinition of an APS gold standard, for instance derived from the APS ACTION registry that will
include not only current APS patients but also those with antiphospholipid antibodies not meeting current classification
criteria.
Keywords Antiphospholipid Syndrome;
GRADE system;
Clinical features;
Non-criteria manifestations;
Accuracy

MANIFESTACIONES CLÍNICAS que pueden ser incorporadas como criterios clasificatorios.
Livedo reticularis (16-25%)Patron reticular, coloracion rojiza-azulada. RacemosaSe asocia a mayor prevalencia de ictus, HTA,valvulopatía cardiaca y pérdidas fetales.Puede ser un marcador pronóstico de enfermedadmás grave y factor de riesgo independiente para latrombosis arterial
Valvulopatía cardiaca (30-60%)Engrosamiento focal/difuso mitras/aortico (>3mm).Vegetaciones de Libman-Sacks (1-5%)Se asocia con ictus, migraña y epilepsia.Patogenia desconocida. Se recomienda ecografía atodos los pacientes al diagnóstico del SAF, si espatológico seguimiento periódico.

Afectación renal (2.7-9%)Vasculopatia/microangiopatia trombóticaProteinuria, hematuria e insuficiencia renal progresiva ofallo renal agudo e HTA. Biopsia renal: Microtrombosiso trombosis vascular organizada o fibrinoide sincomponente inflamatorio. DD con nefroangioesclerosis.
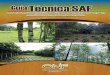
FIGURE 1 | Antiphospholipid syndrome nephropathy histologic lesions. (A) Luminal narrowing due to circumferential myointimal thickening of the wall of one arteriole and one interlobular artery. Glomerulus exhibiting ischemic features with wrinkling of the glomerular capillary basement membranes (PAS 200×). (B) An interlobular artery and an arteriole showing luminal narrowing due to pale mucoid intimal thickening and myointimal cellular proliferation. Additionally, the arteriole reveals fibrin insudation within the wall (black arrows) (Masson trichrome 400×). (C) Arteriole showing luminal thrombus (HE 400×). (D) Arteriole showing TMA with platelet-fibrin thrombus occluding the lumen and nuclear debris in the arterial wall (HE 400×).
3
Tektonidou Kidney in APS
Frontiers in Immunology | www.frontiersin.org May 2018 | Volume 9 | Article 1181
addition to thrombotic microangiopathy, Amigo et al. described a number of chronic renal vascular lesions as a part of kidney involve-ment in APS and in the absence of overt lupus nephritis (31).
Antiphospholipid syndrome nephropathy, a renal small-vessel vasculopathy characterized by acute thrombosis and/or chronic arterial and arteriolar lesions, was first defined as a distinct histological and clinical entity in 1999. After examining 16 renal biopsies of primary APS patients, Nochy et al. suggested that at least one of the following lesions should be detected for the diagnosis of APS nephropathy: thrombotic microangiopathy (acute lesion), interlobular fibrous intimal hyperplasia, arterial and arteriolar recanalizing thrombi, fibrous arterial occlusion, and focal cortical atrophy (32) (Figure 1). The same French group later observed the same histological lesions in patients with SLE-associated APS, over and above lupus nephritis lesions (33). APS nephropathy has been associated with LA, arterial thrombosis, and fetal loss. It was also associated with an higher risk of hypertension, elevated serum creatinine levels, and kidney interstitial fibrosis, all recognized as predictors of worse renal outcomes.
Tektonidou et al. showed that in lupus nephritis biopsy samples, APS nephropathy lesions were much more prevalent in aPL- positive patients (39.5% versus only 4.3% of those with negative aPL) (34). Furthermore, APS nephropathy was found in two-thirds of those meeting APS criteria among those aPL-positive patients with SLE. A strong association with APS nephropathy was also noted in patients with arterial thrombosis and livedo
reticularis. APS nephropathy was characterized by a higher fre-quency of hypertension and elevated creatinine levels on biopsy, but did not predict the risk of decline in kidney function, end-stage renal disease or death at the end of follow-up. The rate of APS-related clinical manifestations, such as arterial thrombosis, was higher in SLE patients with versus without APS nephropathy during a long-term follow-up.
Some years later, Tektonidou et al. examined three different APS groups for acute and chronic APS nephropathy lesions: pri-mary APS, SLE-associated APS, and for the first time, catastrophic APS (35). Thrombotic microangiopathy, the acute lesion, was prominent in catastrophic APS while the prevalence of chronic lesions was similar among all APS groups. In all three APS groups, hypertension, proteinuria (mild to nephrotic syndrome), micro-scopic hematuria, and renal insufficiency (usually mild) were the main clinical features of APS nephropathy.
Further studies confirmed the above findings. However, the impact of APS nephropathy on long-term renal outcomes varied among different studies. In a single cohort from Thailand, APS nephropathy lesions were present in 34% of 150 patients with biopsy-proven lupus nephritis. APS nephropathy was correlated with indices of disease activity and chronicityhypertension, renal failure, severe proteinuria, class III and IV histology, and end-stage renal disease (36). In another study, APS nephropathy was present in 10% of kidney biopsy specimens from 162 Mexican patients with lupus nephritis and was associated with anticar-diolipin antibodies and elevated rates of rapidly progressive
Manifestaciones neurológicasCorea (1.3%) y mielitis transversa (<1%)
MANIFESTACIONES CLÍNICAS que pueden ser incorporadas como criterios clasificatorios.

7 Recomendaciones SER sobre síndrome antifosfolípido primario
Tabla 2. Criterios preliminares para la clasificación del síndrome antifosfolípido catastrófico8
Criterios diagnósticos
1. Evidencia de la afectación de tres o más órganos, sistemas o tejidos. 2. Desarrollo de las manifestaciones de forma simultánea o en menos de una semana. 3. Confirmación histopatológica de la oclusión de pequeño vaso en al menos un órgano o
tejido. 4. Confirmación analítica de la presencia de anticuerpos antifosfolípidos (anticoagulante
lúpico y/o anticuerpos anticardiolipina y/o antiβ2 glicoproteína I).
SAF catastrófico definitivo
- Los cuatros criterios.
SAF catastrófico probable
- Los cuatros criterios, pero solo dos áreas afectadas. - Los cuatro criterios, en ausencia de confirmación analítica. - Criterios 1,2 y 4. - Criterios 1,3 y 4 y el desarrollo de un tercer episodio entre una semana y un mes
después de su presentación, a pesar de anticoagulación; pero menos de un mes, a pesar de la anticoagulación.
SAF definitivo: es la presencia de al menos un criterio clínico y uno de laboratorio. La prueba de laboratorio debe ser positiva en dos o más ocasiones separadas 12 semanas.
SAF CATASTRÓFICO CRITERIOS DE CLASIFICACIÓN
R. Asherson, R. Cervera, P.G. de Groot, Lupus 12 (2003) 530–534.
10th International Congress on aPL in 2002
Microangiopatia trombótica universal y con un componenteasociado de respuesta inflamatoria sistémica y citoquinas queinvolucra al complemento.

SITUACIONES CLÍNICAS DE SOSPECHA DE SAF
• TTPa prolongado. Trombopenia leve. AHAI
• Sujetos jóvenes (habitualmente pero no siempre < 50 años) con ETEV noprovocada, en lugar no habitual, o asociada a enfermedad autoinmune.
• Sujetos jóvenes con Ictus embólico de origen desconocido o ictuscriptogénico o trombosis arterial no explicada y cuando otrasmanifestaciones clínicas están presentes: demencia, livedo reticularis ,epilepsia, enfermedad valvular...
• Recurrencias
• Pérdidas recurrentes del primer trimestre, muerte fetal, preeclampsia-eclampsia, CIR, desprendimiento prematuro de placenta.
• Corea, migraña, pérdida de memoria, enfermedad desmielinizante deetiología no aclarada, neuropatía óptica, amaurosis fugaz, trombosis venasretina, necrosis avascular, úlceras cutáneas…
• Trombosis en varios territorios con fallo multiorgánico, presencia deesquistocitos, trombopenia, coagulopatía...
Internistas, vasculares, neurólogos, cardiólogos, traumatólogos,reumatólogos, digestólogos, dermatólogos, obstetras,intensivistas, nefrólogos, hematólogos.

TRATAMIENTORecomendaciones para la prevención y tratamiento a largo plazo de la trombosis
en pacientes con AAF . Consenso de Galveston 2010Grado de la recomendación
Portadores de AAF• Control estricto de los factores de riesgo vascular en
todos los pacientes con perfil de AAF de alto riesgo*No determinado
• Profilaxis de trombosis con dosis habitual de HBPM ensituaciones de riesgo como cirugía, inmovilizaciónprolongada o puerperio
1C
Tromboprofilaxis Primaria en pacientes con LES y AAF• Hidroxicloroquina (1) y AAS (2) a baja dosis 1B (1) 2B (2)
Tromboprofilaxis Primaria en sujetos con AAF sin LES
• Profilaxis a largo plazo con AAS a baja dosis en pacientescon perfil de AAF de alto riesgo, especialmente enpresencia de otros factores de riesgo de trombosis
2C
Trombosis y AAF positivo solo en una ocasión. Tratamiento igual que la población general.
1B fuerte recomendación. Moderada calidad de la evidencia. 1C fuerte recomendación . Baja o muy baja calidad de la evidencia.2B debil recomendación . Moderada calidad de la evidencia. 2C débil recomendación , baja o muy baja calidad de la evidencia.* AL positivo. Triple positividad. ACA o antiβ-2GPI persistentemente positivos a titulos moderados-alto (40)
Lupus (2011) 20, 206–218.

TRATAMIENTORecomendaciones para la prevención y tratamiento a largo plazo de la trombosis
en pacientes con AAF . Consenso de Galveston 2010Grado de la recomendación
Tromboprofilaxis secundaria• Trombosis venosa AVK (2-3) 1B
• Trombosis arterial AVK (>3) o AVK (2-3) y AAS• Oras opciones con AVK (2-3) o solo AAS podrían ser
adecuadas.• Atención al riesgo de sangrado si se recomienda terapia
dual o anticoagulación de alta intensidad.
No determinado. Ausencia de consenso.
• Los pacientes con SAF no asociado a LES con unaprimera trombosis arterial no cardioembólica y con perfilde AAF de bajo riesgo y presencia de factores de riesgodesencadenantes reversibles podrian ser consideradosde modo individual como candidatos a tratamientoantiagregante
No consenso
Duración del tratamiento• Indefinido• En caso de primer evento trombótico venoso y perfil de
AAF de bajo riesgo y factor desencadenante 3-6 meses
1C
No determinado1B fuerte recomendación. Moderada calidad de la evidencia. 1C fuerte recomendación . Baja o muy baja calidad de la evidencia..Perfil bajo riesgo. ACA o antiβ-2GPII de modo aislado o intermitente a titulos bajos.(20-39)
Lupus (2011) 20, 206–218.

Mujer 58 años. Menopausia temprana. Osteoporosis/artrosisPreoperatorio Prótesis total cadera. TTPa prolongado. Anticoagulantelúpico positivo.
• Profilaxis de ETEV habitual . HBPM 35 dias
• ¿Hacemos algo más?
Prevención Primaria
1. Nos limitamos a dar nota para anestesia para que sea intervenida yrecomendamos profilaxis de ETEV habitual.
2. Remitimos a su medico para seguimiento.
3. Citamos en nuestra consulta para completar estudio .
Riesgo absoluto de una primera trombosis. AAF sin factores de riesgo. <1%/añoAAF perfil de alto riesgo/Enf sistémica/factores de riesgo. 5%/año

Mujer 58 años. Menopausia temprana. Osteoporosis/artrosisPreoperatorio Prótesis total cadera. TTPa prolongado. Anticoagulantelúpico positivo.
Edad, presencia de otros factores de riesgo vascular (tabaco, HTA, diabetes,dislipemia) o enfermedades autoinmunes asociadas. SAF obstétrico.
Prevención Primaria
Sciascia, S.; Bertolaccini, M.L.. Thrombotic risk assessment in APS Lupus (2014) 23, 1286–1287.
The Global APS Score (GAPSS)
Perfil de AAF
Riesgo Alto AL positivo con o sin aCL o anti-β2GPI IgG o IgM a títulos moderados-altos
Riesgo Moderado
AL negativo con aCL o anti-β2GPI IgG o IgM a títulos moderados-altos
Riesgo Bajo AL negativo con aCL o anti-β2GPI IgG o IgM a titulos bajos.
HTA, Dislipemia
Estratificar el riesgo trombótico.
ACA IgG 65 GPL (TTPa prolongadohace 1 año).

15th Congreso Internacional sobre AAF se recomienda usar los modelosde valoración de riesgo de la población general, hasta que no existanmodelos de estratificación específicos validados para individuos con AAF.
Atherosclerotic Cardiovascular Disease 10 Year Risk Score (ASCVD)
>7.5% estatinas >10% AAS . Grado B
Systematic Coronary Risk Estimation(SCORE)
>5% estatinas. No recomiendan AAS sin enfermedad cardiovascular establecida. Clase I
9 estudios con 1044 individuos con AAFpositivos sin trombosis. No suficienteevidencia para recomendar AAS enprevención primaria.Bala MM, Paszek E, Lesniak W, Wloch-Kopec D, Jasinska K, Undas A.2018, Issue 7. Art. No.: CD012534.
Cochrane Database of Systematic Reviews
Antiplatelet and anticoagulant agents for primary preventionof thrombosis in individuals with antiphospholipid antibodies(Review)
Bala MM, Paszek E, Lesniak W, Wloch-Kopec D, Jasinska K, Undas A
Bala MM, Paszek E, Lesniak W, Wloch-Kopec D, Jasinska K, Undas A.
Antiplatelet and anticoagulant agents for primary prevention of thrombosis in individuals with antiphospholipid antibodies.
Cochrane Database of Systematic Reviews 2018, Issue 7. Art. No.: CD012534.
DOI: 10.1002/14651858.CD012534.pub2.
www.cochranelibrary.com
Antiplatelet and anticoagulant agents for primary prevention of thrombosis in individuals with antiphospholipid antibodies (Review)
Copyright © 2018 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cálculo riesgo 2% a los 10 años.

ANTIPHOSPHOLIPID SYNDROME (S ZUILY, SECTION EDITOR)
Primary Thrombosis Prophylaxis in Persistently AntiphospholipidAntibody-Positive Individuals: Where Do We Stand in 2018?
Yu Zuo1 & Medha Barbhaiya2 & Doruk Erkan2
Published online: 10 September 2018# Springer Science+Business Media, LLC, part of Springer Nature 2018
AbstractPurpose of review To update our previous literature review and management recommendations on risk stratification and primarythrombosis prophylaxis in persistently antiphospholipid antibody (aPL)-positive individuals.Recent Findings The estimated annual thrombosis incident rate (ATIR) among aPL-positive individuals with or without systemicautoimmune disease (SAIDx) is 0 to 5.3%, probably very low (< 1%/year) in those with no other SAIDx and thrombosis riskfactors. Risk stratification based on aPL profile, age, additional SAIDx, and traditional cardiovascular disease (CVD) or venousthrombosis risk factors is crucial to determine the risk of first thrombosis in aPL-positive patients. The protective effect of low-dose aspirin for primary thrombosis prophylaxis prevention is not supported by randomized controlled data. Hydroxychloroquineis protective against thrombosis in aPL-positive SLE patients; however, its role in aPL-positive individuals with other SAIDxremains uncertain. Statins downregulate proinflammatory and prothrombotic biomarkers among antiphospholipid syndrome(APS) patients and may have a role in aPL-positive individuals with high CVD risk.Summary The optimal primary thrombosis prevention strategy in patients with clinically significant aPL profiles should include(a) regular screening and elimination of non-aPL thrombosis risk factors, (b) optimal management of concomitant SAIDx, (c)patient counseling and education, and (d) use of CVD risk prediction tools and guidelines to perform risk-benefit calculationsregarding low-dose aspirin, hydroxychloroquine, and/or statin therapy.
Keywords Antiphospholipid antibodies . Antiphospholipid syndrome . Thrombosis . Primary thrombosis prevention .
Thrombosis risk
Introduction
Antiphospholipid syndrome (APS) is an autoimmune multi-system disorder characterized by thrombosis and pregnancymorbidity, and serologically by positive antiphospholipid(aPL) antibodies [1], which consist of a family of heteroge-neous immunoglobulins directed against phospholipid-binding plasma proteins. Antiphospholipid antibodiesincluded in the Sydney APS classification criteria include
the IgG and IgM isotypes of anti-β2-glycoprotein-I antibodies(aβ2GPI), anticardiolipin antibodies (aCL), and a positive lu-pus anticoagulant (LA) test (“criteria aPL tests”) [2].Accumulating evidence suggests a role for “non-criteria”aPL tests, including antibodies against Domain I of β2-glyco-protein-I (anti-Domain I) and phosphatidylserine-dependentantiprothrombin antibodies (aPS/PT). These tests remain lim-ited in their commercial availability, and their clinical signif-icance in predicting thrombosis is debated.
Antiphospholipid antibody-positive patients exist withoutaPL-related thrombosis or pregnancy manifestations, withonly pregnancy morbidity, or with only “non-criteria” aPLmanifestations, e.g., thrombocytopenia, livedo reticularis, orcardiac valve disease. Physicians may order aPL tests for avariety of reasons, including evaluation of a systemic au-toimmune disease, or in the setting of an elevated activatedpartial thromboplastin time (aPTT) or a false positiveVenereal Disease Research Laboratory test. When aPLtesting returns positive, a major challenge in clinical
This article is part of the Topical Collection on AntiphospholipidSyndrome
* Doruk [email protected]
1 Division of Rheumatic Disease, Department of Medicine, UTSouthwestern Medical Center, Dallas, TX, USA
2 Barbara Volcker Center for Women and Rheumatic Diseases,Hospital for Special Surgery, Weill Cornell Medicine, 535 E 70thStreet, New York, NY 10021, USA
Current Rheumatology Reports (2018) 20: 66https://doi.org/10.1007/s11926-018-0775-8
differences in the incidences of stroke, CVmortality, all-causemortality, and total coronary heart disease [69]. Recent 10-year follow-up of Japanese Primary Prevention ofAtherosclerosis with Aspirin for Diabetes trial concluded thatprimary prophylaxis with low-dose aspirin did not affect CVevent risk but increased risk for gastrointestinal bleeding inpatients with type 2 diabetes [70]. Secondary analysis of theWomen’s Health Study concluded that low-dose aspirin treat-ment has no significant effect on venous thromboembolismprevention in healthy women age 45 years or older [71]. TheAmerican College of Cardiology (ACC) and American HeartAssociation (AHA) still endorse low-dose aspirin use for pri-mary CVD prevention among patients who have ≥ 10% 10-year CVD risk [72]. The European Society of Cardiology(ESC) does not recommend antiplatelet therapy for primaryCVD prevention [63].
In summary, whether low-dose aspirin is protective againstincident thrombosis in aPL-positive individuals remains con-troversial due to lack of high quality data. Two meta-analysessuggest the use of aspirin among aPL-positive individuals isassociated with a decreased rate of arterial thrombosis.However, their results are driven mainly by retrospective un-controlled observations and are limited by outcome heteroge-neity of included studies. Furthermore, the protective role ofaspirin against cardiovascular events in the general populationis still under investigation. Any benefit of primary thrombosisprophylaxis with aspirin must also be weighed against the riskof bleeding (10-year average annual rate of 2.37%) [73]. Thus,in the absence of disease-specific prediction tools, we recom-mend the use of general population CVD risk prediction toolsand prevention guidelines (e.g., US Preventative Service TaskForce, ACC/AHA, ESC) that are formulated based on risk-
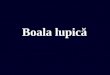
Clinically Significant aPL-Profile
Yes
• Aggressive Disease Control• Hydroxychloroquine if
Indicated for Disease Control(e.g., SLE)
Indication for Daily Low Dose Aspirin and/or Statin Based on General
Population Guidelines (e.g., SCOREor ASCVD)?
Systemic Autoimmune Diseases?
Yes
NoProphylacticMedication
No
• Continuous Assessment / Elimination of Cardiovascular Diseaseand Venous Thrombosis Risks
• Consider Prophylaxis During High Thrombosis Risk Period. (e.g.,surgery, hospitalization.)
• Patient Education
No
Daily Low Dose Aspirinand/or Statin
Fig. 1 Proposed primarythrombosis prophylaxis algorithmfor patients with clinicallysignificant antiphospholipidantibody (aPL) profiles
Curr Rheumatol Rep (2018) 20: 66 Page 7 of 12 66

Recomendaríamos control estricto de factores de riesgo vascular (obesidad,sedentarismo), contraindicada la terapia hormonal sustitutiva, confirmar quetoma estatinas, profilaxis de ETEV ante situaciones de riesgo.
¿Recomendaríamos profilaxis primaria con AAS 100 mg diarios.??????
Mujer 58 años. Menopausia temprana. Osteoporosis/artrosis. HTADislipemia. AAF alto riesgo.
Prevención Primaria
Livedo reticularis

ü Hidroxicloroquina en prevención primaria. Cerrado por falta dereclutamiento. Erkan, 2017 (APS ACTION HCQ TRIAL)
ü Estatinas. Recomendado en pacientes con perfil lipídico aterotrombóticoy por sus efectos antinflamatorios sobre monocitos, linfocitos y sucapacidad de interferir con la activacion del endotelio inducida por losAAF. Ann. Rheum. Dis. 73 (2014) 1176-1180.
ü Suplementos de Vitamina D. Coenzima Q Ann. Rheum. Dis. 70 (2011) 145-150.Thromb. Vasc. Biol. 37 (2017) 1923-1932.
Prevención Primaria

Mujer 30 años. TVP proximal hace 15 meses, Fumadora. IMC >30. Triplepositividad para AAF. Control de INR adecuado con muestra venosa (INR2-3 1B)
SAF trombosis venosa
Tratamiento antitrombótico indefinido. 1C. Si único episodio, asociado afactor desencadenante transitorio y perfil de AAF de bajo riesgo 3-6 meses.Ha dejado de fumar, ha perdido 20 Kg de peso, no tiene Sdpostrombótico. DD menor 250 ( HERDOO2, DASH, Normograma deViena ) pero los AAF persisten positivos.
Can we withdraw anticoagulation in patients with antiphospholipidsyndrome after seroconvertion?
S. Sciascia a,1, E. Coloma-Bazán b,1, M. Radin a, M.L. Bertolaccini c, C. López-Pedrera d, Gerard Espinosa b,P.L. Meroni e,⁎, R. Cervera b,2, M.J. Cuadrado f,2
a Center of Research of Immunopathology and Rare Diseases, Coordinating Center of Piemonte and Valle d'Aosta Network for Rare Diseases, Department of Clinical and Biological Sciences, S.Giovanni Bosco Hospital, University of Turin, Turin, Italyb Department of Autoimmune Diseases, Hospital Clinic, Barcelona, Catalonia, Spainc Academic Department of Vascular Surgery, Cardiovascular Division, King's College London, United Kingdomd Maimonides Institute for Research in Biomedicine of Cordoba (IMIBIC), Reina Sofia University Hospital, University of Cordoba, Cordoba, Spaine Division of Rheumatology, ASST-G Pini, Department of Clinical Sciences & Community Health, University of Milan, Immunorheumatology Research Laboratory, Istituto Auxologico Italiano, Milan, Italyf Louise Coote Lupus Unit, Guy's and St Thomas' NHS Foundation Trust, London, UK
a b s t r a c ta r t i c l e i n f o
Article history:Received 22 July 2017Accepted 27 July 2017Available online 9 September 2017
The current mainstay of treatment in patients with thrombotic antiphospholipid syndrome (APS) is long-termanticoagulation, mainly with Vitamin K antagonist agents. Some recently available studies have created newground for discussion about the possible discontinuation of anticoagulation therapy in patients with a historyof thrombotic APS in whom antiphospholipid antibodies (aPL) are not detected any longer (i.e. aPLseroconversion).We report themainpoints discussed at the last CORAMeeting regarding the issuewhether or not anticoagulationcan be stopped after aPL seroconversion. In particular, we systematically reviewed the available evidence inves-tigating the clinical outcome of APS patients with aPL seroconversion in whom anticoagulation was stoppedwhen compared to those inwhom therapy was continued regardless the aPL profile. Furthermore, themolecularbasis for the aPL pathogenicity, the available evidence of non-criteria aPL and their association with thrombosisare addressed.To date, available evidence is still limited to support the indication to stop oral anticoagulation therapy in patientswith a previous diagnosis of thrombotic APS who subsequently developed a negative aPL profile. The identifica-tion of thewhole risk profile for cardiovascularmanifestations and possibly of a second level aPL testing in select-ed patients with aPL might support the eventual clinical decision but further investigation is warranted.
© 2017 Elsevier B.V. All rights reserved.
Keywords:Antiphosphospholipid syndromeAntiphospholipid antibodiesAnticoagulationThrombosis
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11102. Systematic review of the available evidence on aPL seroconversion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1110
2.1. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11102.2. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1110
2.2.1. Definition of aPL negativization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11102.2.2. Follow up and recurrences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1110
3. Molecular basis for the antiphospholipid antibody pathogenicity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11113.1. Tissue factor and endothelial dysfunction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11113.2. Oxidative stress . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11113.3. Toll like receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1111
Autoimmunity Reviews 16 (2017) 1109–1114
⁎ Corresponding author at: Division of Rheumatology, ASST-G Pini, University of Milan, Italy.E-mail address: [email protected] (P.L. Meroni).
1 Sciascia S, Coloma-Bazán E contributed equally to this work.2 Cervera R, Cuadrado MJ contributed equally to this work.
https://doi.org/10.1016/j.autrev.2017.09.0041568-9972/© 2017 Elsevier B.V. All rights reserved.
Contents lists available at ScienceDirect
Autoimmunity Reviews
j ourna l homepage: www.e lsev ie r .com/ locate /aut rev
3.4. NETosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11123.5. Genomic and epigenetic. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1112
4. Non-classification criteria antiphospholipid antibodies and thrombosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11124.1. Prothrombin/phosphatidylserine complex . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11124.2. Antibodies directed to the domain I of β2GPI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11124.3. IgA aPL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11134.4. Anti-annexin A5 and antivimentin antibodies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1113
5. Conclusions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1113Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1113Disclosure of conflicts of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1113Funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1113References. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1113
1. Introduction
High morbidity and mortality due to recurrence of thrombotic eventsis the main concern in patients with antiphospholipid syndrome (APS)[1]. Current evidence-based guidelines recommend long-term oralanticoagulation (OAC) as prophylaxis of new thrombotic manifestationsof APS. Thedecisionon theduration and intensity of this treatment shouldbe based on the clinical features and immunological profile. According tothe guidelines, patients with definite APS and a first venous thromboticevent should receive long-term OAC to an international normalizedratio (INR) target of 2.0–3.0 (the so called conventional-intensityanticoagulation). On the other side, patients with definite APS and an ar-terial thrombotic event should receive high-intensity anticoagulationtherapy to an INR target between 3.0 and 4.0. However, long-term OAChas also been associated to a wide broad of hemorrhagic complications[2].
Especial attentionhas recently beenpayed to a small subset of patientswho fulfill APS criteria but inwhom aPL become persistently negative [3].
We systematically reviewed the available evidence investigating theclinical outcome of APS patients with aPL seroconversion(negativization) inwhomanticoagulationwas stoppedwhen comparedto those in whom therapy was continued regardless the aPL profile.Moreover, we aim to discuss themolecular basis for the aPL pathogenic-ity and the available evidence of non-criteria aPL and their associationwith thrombosis.
2. Systematic reviewof the available evidence on aPL seroconversion
The aim of this systematic review is to identify the available evi-dence on the clinical experience of thrombotic APS patients with persis-tent negative aPL.We also focused on those caseswhere anticoagulationwas stopped after patients showed persistent negativity to conventionalaPL tests.
2.1. Methods
We performed a systematic review to identify and include in ourstudy articles that reported clinical experience of thrombotic APS pa-tients with persistent aPL seroconversion and patients that werediscontinued anticoagulation for that reason. Key words and subjectterms used in the search included: (“antiphospholipidantibodies”[MeSH Terms] OR “aPL”[All Fields]) AND(“negativization”[All Fields]) AND (“anticoagulation”[All Fields] OR“treatment”[All Fields]) AND “phospholipid”[All Fields]) OR(“antiphospholipid syndrome”[MeSH Terms] OR (“APS” [All Fields]).
The search strategy was applied to Ovid MEDLINE, In-Process andOther Non-Indexed Citation, EMBASE, Cochrane Central Register of Con-trolled Trials and Scopus from 1983 (year when the antiphospholipidsyndrome was firstly described) to present; abstracts from EULAR andACR were also screened. Inclusion criteria included either: a) followup of thrombotic APS patients with persistent aPL seroconversion b)
follow-up of thrombotic APS patients with persistent aPL seroconver-sion that were discontinued anticoagulation therapy. Studies that metthe above-mentioned criteria were systematically analyzed by two in-dependent reviewers (MR and IC). Disagreements were resolved byconsensus; if consensus could not be achieved, a third party (SS) provid-ed an assessment of eligibility. As the data on eligibility were dichoto-mous (eligible: yes/no), inter-rater agreement at both the title andabstract review and the full article review stageswas determined by cal-culation of Cohen's kappa coefficient (k = 0.85).
2.2. Results
Out of 1006 screened studies, a total of four [3–6] met the inclusioncriteria, including 47 thrombotic APS patients with persistently aPL se-roconversion. Three out of four studies, including 23 thrombotic APS pa-tients, described discontinuation of anticoagulation therapy after aPLseroconversion.
Characteristics of retrieved studies are summarized in Table 1.
2.2.1. Definition of aPL negativizationThe definition of aPL seroconversion/negativization was heteroge-
neous among studies. Two studies [4,5] included patientswith 2 consec-utive aPL seroconversion, however one of those studies [5] retestedpatients to confirm aPL disappearance after five years. Two studies [6,7] did not define the aPL negativization, however one study [7], report-ed patients with at least nine negative determinations of criteria aPLtesting. Of note, one study reported patients positive for aCL IgG atlow titer in most cases and one patients positive for LA only but withnegative results in a second determination [4]. Another study includedmainly patients positive for LA only [5]; only one study [6] tested theircohort of patients for non-criteria aPL (anti-annexin A5 antibodies).Anti-beta 2 glycoprotein I (β2GPI) antibodies were not investigated inall the reported studies.
2.2.2. Follow up and recurrencesMedina and colleagues [5], investigated 24 primary APS patients
with aPL seroconversion in a retrospective study, without stoppinganticoagulation therapy. Since aPL disappearance and after 60 monthsof follow up, 11 out of 24 patients (45.8%) presented recurrence ofthrombosis despite the continuation of the anticoagulant treatment.Among these 11 patients, 9 presented a DVT, one experienced an ische-mic stroke and onepatient developed pulmonary artery hypertension. 9out of 24 patients (37.5%) had a past history of arterial thromboticevents (eight strokes and onemesenteric thrombosis) before aPL disap-pearance. This fact could place this group of patients at a higher throm-botic risk category. In addition, other non-thrombotic or non-criteriaAPS manifestations occurred in 6 patients, such as chronic skin ulcersin lower extremities in 4 patients and severe thrombocytopenia intwo. Comarmond and colleagues [6] included 10 APS patients withprolonged disappearance of antiphospholipid antibodies (aPL) inwhom anticoagulation therapy was discontinued. After a median
1110 S. Sciascia et al. / Autoimmunity Reviews 16 (2017) 1109–1114
- Primer evento trombótico no grave.- Presencia de un factor de riesgo precipitante transitorio (fumar, HTA, reciente
cirugía)- Perfil de AAF de bajo riesgo: AAF único que persistentemente es negativo
durante un tiempo prolongado, p.ej 2 años)

Mujer 30 años. TVP hace 15 meses. Fumadora . IMC >30. Triple positividadpara AAF. Control de INR adecuado con muestra venosa.¿Puedo cambiar a una de las nuevas pastillas que no tiene controles?
SAF trombosis venosa
15th International Congress on Antiphospholipid Antibodies Task Forceon Treatment Trends Recommendation: (North Cyprus, September 2016)Insufficient evidence to make recommendations at this time regarding DOACuse in APS.
ClinicalTrials.gov.Identifier: NCT02157272. TRAPS Rivaroxaban 20 mgvs warfarina Cerrado reclutamiento en enero 2018 por 19% de eventostrombóticos en el grupo de Rivaroxaban vs 3% en el grupo de warfarina.Pacientes de alto riesgo.
ClinicalTrials.gov.Identifier: NCT02295475. ASTRO-APS Apixaban 2.5c/12 vs warfarina. Modificación protocolo. Apixaban 5 mg c/12 y solopacientes con ETEV, no incluir pacientes si RNM datos de isquemia oimportantes cambios en sustancia blanca.
¿Recomendaríamos cambiar a ACODs?

Varón 45 años. Ictus isquémico 2 años antes. Fumador y dislipémico. ACAIgG 45 GPL, Antiβ2-GPI 55 U/L Tratamiento con acenocumarol INR 2-3 ycontrol estricto factores de riesgo vascular. Acude a urgencias por AIT. INR2.9. Soplo sistólico. Ecocardiografia: engrosamiento/verrugas válvula mitral.
SAF trombosis arterial y recurrencia
AVK INR (3-4) o tratamiento combinado AVK (INR 2-3) y AAS, aunque otrasopciones como antiagregación solo o AVK (INR 2-3) pueden ser opcionesválidas. No existe consenso
(Consenso de Galveston,2010)
Cochrane Database of Systematic Reviews
Antiplatelet and anticoagulant agents for secondaryprevention of stroke and other thromboembolic events inpeople with antiphospholipid syndrome (Review)
Bala MM, Celinska-Lowenhoff M, Szot W, Padjas A, Kaczmarczyk M, Swierz MJ, Undas A
Bala MM, Celinska-Lowenhoff M, Szot W, Padjas A, Kaczmarczyk M, Swierz MJ, Undas A.
Antiplatelet and anticoagulant agents for secondary prevention of stroke and other thromboembolic events in peoplewith antiphospholipid
syndrome.
Cochrane Database of Systematic Reviews 2017, Issue 10. Art. No.: CD012169.
DOI: 10.1002/14651858.CD012169.pub2.
www.cochranelibrary.com
Antiplatelet and anticoagulant agents for secondary prevention of stroke and other thromboembolic events in people with
antiphospholipid syndrome (Review)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cochrane Database of Systematic Reviews
Antiplatelet and anticoagulant agents for secondaryprevention of stroke and other thromboembolic events inpeople with antiphospholipid syndrome (Review)
Bala MM, Celinska-Lowenhoff M, Szot W, Padjas A, Kaczmarczyk M, Swierz MJ, Undas A
Bala MM, Celinska-Lowenhoff M, Szot W, Padjas A, Kaczmarczyk M, Swierz MJ, Undas A.
Antiplatelet and anticoagulant agents for secondary prevention of stroke and other thromboembolic events in peoplewith antiphospholipid
syndrome.
Cochrane Database of Systematic Reviews 2017, Issue 10. Art. No.: CD012169.
DOI: 10.1002/14651858.CD012169.pub2.
www.cochranelibrary.com
Antiplatelet and anticoagulant agents for secondary prevention of stroke and other thromboembolic events in people with
antiphospholipid syndrome (Review)
Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
No hay suficiente evidencia a favorni en contra del uso de AVK (3-4)comparado con AVK (2-3). Si >riesgo de sangrado .No evidencia suficiente a favor ni encontra de AVK mas AAS o dobleantiagregación comparado con AAS.

SAF MANEJO RECURRENCIASEn estudios prospectivos 3-24% de los pacientes con SAF desarrollan recurrencias incluso durante el tratamiento anticoagulante.• Confirmar INR en rango• Incrementar INR 2-3• HBPM• Añadir AAS o si contraindicada Hidroxicloroquina o clopidogrel.• Estatinas.• Rituximab, Inmunoglobulinas, Eculizumab (receptores de trasplante renal)15th International Congress on APS Task Force on Antiphospholipid Syndrome Treatment Trends Report
Tratamiento manifestaciones cardiacas (Anomalías valvulares) asociadas a AAF
• Sintomáticas (insuficiencia cardiaca, embolismo) o presencia devegetaciones: AVK.
• Asintomáticas (engrosamiento valvular sin repercusión funcional,tromboembolismo, ni factores de riesgo ) AAS
No es necesaria la profilaxis de endocarditis bacteriana y no existe consensoen cuanto al tratamiento con corticoides. 4-6% requieren cirugia
10th Internantional Congress on APS. Comité de expertos en enfermedades cardiacasen SAF recomienda (Lupus,2003)
¿Quien revisa a pacientes como el nuestro?¿Se podría haber evitado ?

570 J. Pardos Gea
TABLA 8. Tratamiento de las complicaciones obstétricas en pacientes AAF/SAF.
Situación clínica Tratamiento
Historia de 3 o más abortos < 10 sem gestación sin trombosis previa
Aspirina 100 mg/día monoterapia o asociada a HBPM profiláctica
Historia de muerte fetal > 10 sem gestación o preeclampsia grave o retraso crecimiento por insuficiencia placentaria
Aspirina 100 mg/día más HBPM profiláctica
SAF con trombosis previa y gestación Aspirina 100 mg/día más HBPM dosis anticoagulante
Paciente AAF sin criterios clínicos SAF definitivo (< 3 abortos < 10 sem gestación, no trombosis) y gestación
Aspirina 100 mg/día
Paciente AAF sin criterios clínicos de SAF definitivo y fecundación in vitro
HBPM profiláctica, mantener en gestación
Todas las pacientes con SAF obstétrico En puerperio alargar tratamiento HBPM 6 semanas y paso posterior aspirina 100 mg/día a largo plazo
HBPM: heparina bajo peso molecular.
TABLA 9. Tratamiento de las manifestaciones clínicas no clasificatorias en SAF.
Manifestación clínica Tratamiento
Livedo reticularis racemosa Medidas físicas, tratamiento enfermedad base
Vasculopatía liveloide atrofia blanca Antiagregación, TIS, pentoxifilina, danazol
Pioderma gangrenoso Antiagregación, anticoagulación, TIS, rituximab
Valvulopatía cardíaca sintomática (insuficiencia, embolismo) o presencia de vegetaciones
anticoagulación oral AVK. Corticoides, TIS no indicado
Engrosamiento valvular sin repercusión funcional, tromboembolismo ni factores de riesgo trombótico)
Antiagregación (Aspirina 100 mg/día)
Todos pacientes con valvulopatía y AAF No requieren profilaxis endocarditis infecciosaManejo anticoagulación óptimo si recambio valvular
Nefropatía asociada a AAF Antiagregación / Anticoagulación
LES con nefropatía asociada a AAF Hidroxicloroquina y Antiagregación / AnticoagulaciónIECAS, ARA-II en todos los pacientes
Corea Neurolépticos, corticoides, TIS
Disfunción cognitiva Antiagregación/anticoagulación
Mielitis/EM-like disease TIS. Rituximab si asociado a LES
Trombocitopenia sintomática o < 50.000 plaquetas
Corticoides, Ig, TIS, rituximab, esplenectomía, eltrombopagEn algún caso respuesta a tratamiento antiagregante
TIS: tratamiento inmunosupresor; Ig: inmunoglobulinas endovenosas.
559
INTRODUCCIÓN. HISTORIAEl síndrome antifosfolípido (SAF) se define
en la actualidad según unos criterios clasifica-torios de consenso[1] que califican de SAF a pa-cientes que aúnen clínica trombótica vascular (arterial/venosa) y/o complicaciones obstétri-cas atribuibles a patología vascular placentaria, junto a la presencia de anticuerpos antifosfolípi-dos (AAF) del tipo anticoagulante lúpico (AL), anticardiolipina (aCL) y/o anti-beta-2-glicopro-teína I (anti-B2 GPI).
La evolución histórica de la entidad se ini-cia en 1952 cuando se describe una elevada prevalencia de serología luética falsamente positiva en pacientes con lupus eritematoso sistémico (LES)[2] y por parte de otros inves-tigadores, la presencia de una inhibición de la coagulación con alargamiento de tiempos de coagulación in vitro que no se corregía con la adición de plasma normal[3], fenómeno más tarde catalogado como “anticoagulante lúpi-co”. Algunos autores a posteriori, describieron la coexistencia de ambos fenómenos en pacientes con LES[4]. A pesar de que inicialmente se aso-ciaron estos hallazgos con clínica hemorrágica, por varios casos de pacientes con LES (en los que presumiblemente se producirían otros fe-nómenos como hemorragia por trombopenia), los siguientes años los estudios clínicos demos-traron su asociación “paradójica” a fenómenos trombóticos[5,6].
A principios de los años 80 se determinó definitivamente que el fenómeno AL se pro-ducía por un conjunto heterogéneo de autoan-
ticuerpos contra fosfolípidos de membrana plaquetar[7]. En ese período varios estudios objetivan en modelo murino de LES que varios anticuerpos monoclonales anti ADN se unen a su vez a fosfolípidos, entre otros la cardiolipina, presentando actividad AL[8].
Es en este contexto cuando Hughes y su grupo de trabajo aúnan por primera vez el con-cepto de SAF al plantearse como una entidad clínica específica la presencia de fenómenos trombóticos, pérdidas fetales, patología neu-rológica y el fenómeno AL[9]. Dentro del mismo grupo de estudio, Harris y Gharavi describirán una nueva técnica de radioinmunoensayo en fase sólida 400 veces más sensible que la sero-logía luética en la detección de los anticuerpos anticardiolipina, que definirá por tanto el pri-mer antígeno demostrable como generador del fenómeno AL y que asociarían directamente al riesgo trombótico en pacientes con LES[10]. El concepto de SAF primario se define por pri-mera vez a finales de los años 80 con un regis-tro de pacientes y sus características clínicas y serológicas[11].
Al inicio de los años 90, varios grupos de investigación[12,13] descubren que el antígeno de los anticuerpos aCL es un fosfolípido de carga negativa junto a la beta-2-glicoproteína I (B2
GPI), un cofactor anticoagulante fisiológico, y por tanto se acuña el término de aCL como an-ticuerpos anticofactor-fosfolípido. La actividad AL sin embargo se descubre no dependiente de B2 GPI, evidenciándose como un grupo de AAF diferentes en parte a aCL.
Síndrome antifosfolípidoJosep Pardos Gea
15.2
EditorasInmaculada Soto Ortega
María Teresa Álvarez Román
Auspiciado por
Sociedad Española de Trombosis y Hemostasia
Inm
acul
ada
Soto
Ort
ega
Mar
ía T
eres
a Á
lvar
ez R
omán
HEMOSTASIA y TROMBOSISen la práct i ca c l ín i ca
HEM
OST
ASIA y TR
OM
BOSI
Se
n l
a p
ráct
ica
clí
nic
a
Patrocinado por
ES/H
/021
8/00
05

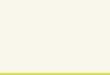
careful bridging between oral anticoagulant to heparin is required.Probably, a multidisciplinary approach with an hemostasis specialist toeach case might be necessary [54]. Additionally, puerperium should beadequately covered for a minimum of 6 weeks with prophylactic dose oflow molecular weight heparin (LMWH).
7.3. Anticoagulation
AC with heparin is the mainstay CAPS treatment. The main reasonfor its use is the inhibition of ongoing clotting and its ability to break upexisting clots that may contribute to the ongoing thrombosis[21,27,55–59]. Moreover, although its pharmacodynamic mechanismsare not completely understood, anti-inflammatory activity of heparinseems to account for its extraordinary usefulness in CAPS [60] and,additionally, heparin seems to inhibit aPL binding to their target on thecell surface [61]. Most CAPS patients are initially treated with
unfractionated heparin because non-fractionated heparin enablesthrowing back its effect in case of requirement. This is often a needduring ICU period either because electively to perform invasive pro-cedures or because of bleeding. Later, non-fractionated heparin can beswitched to LMWH and finally to oral AC. However, physicians shouldnot rush to change heparin to other AC because a long time underheparin treatment favors clot fibrinolysis. A seven to ten days courseunder heparin treatment is recommended. Still, heparin should not bewithdrawn before achieving a correct international normalized ratio(INR) between 2 and 3 with oral AC treatment.
7.4. Glucocorticoids
GC are the most commonly used anti-inflammatory drugs in thetreatment of autoimmune diseases. GC are used to overcome the ex-cessive inflammatory response triggered by multiple blood flow
Fig. 5. Proposed treatment algorithm of catastrophic antiphospholipid syndrome. Abbreviations: aPL: antiphospholipid antibodies; CAPS: catastrophic antipho-spholipid syndrome; ICU: intensive care unit; IVIG: intravenous immunoglobulin; LMWH: low molecular weight heparin; MHA: microangiopathic haemolytic anemia;OAC: oral anticoagulation; PE: plasma exchange; SLE: systemic lupus erythematosus.
R. Cervera et al. -RXUQDO�RI�$XWRLPPXQLW\������������²��
�
Contents lists available at ScienceDirect
Journal of Autoimmunity
journal homepage: www.elsevier.com/locate/jautimm
The diagnosis and clinical management of the catastrophic antiphospholipidsyndrome: A comprehensive reviewRicard Cerveraa,∗, Ignasi Rodríguez-Pintób, Gerard Espinosaaa Department of Autoimmune Diseases, Hospital Clínic, Barcelona, Catalonia, Spainb Systemic Autoimmune Diseases Unit, Department of Internal Medicine, Hospital Mútua de Terrassa, Terrassa, Catalonia, Spain
A R T I C L E I N F O
Keywords:Catastrophic antiphospholipid syndromeTherapeuticsAnticoagulationCorticoidsPlasma exchangeIntravenous immunoglobulinsRituximabEculizumabSirolimus
A B S T R A C T
The catastrophic antiphospholipid syndrome (CAPS) is a life-threating variant of the antiphospholipid syndromecharacterized by the development of multiple thrombosis in a short period of time, usually ending up in thefailure of function of several vital organs. Most CAPS episodes are related to a prothrombotic situation or pre-cipitating factor such as infections, surgical procedures or malignant diseases. In patients with CAPS, the de-velopment of multiple thrombosis leads to an important cytokine release that worsens the already critical pa-tient's situation. The disease usually involves the kidneys, the lungs and the heart, although any organ systemcan be affected. Although occasionally the disease affects large vessels, in the majority of cases it affects smallvessels, leading to a disseminated microangiopathic syndrome resembling thrombotic thrombocytopenic pur-pura. Treatment is based on the administration of anticoagulants, corticosteroids, plasma exchange and/or in-travenous immunoglobulins. Cyclophosphamide is recommended in those CAPS cases associated to systemiclupus erythematosus. Additionally, rituximab and eculizumab have been used in refractory cases. Mortality isstill around 30% despite current treatment.
1. Introduction
The antiphospholipid syndrome (APS) is an autoimmune disordercharacterized by an increased risk of thrombosis and pregnancy lossassociated with antiphospholipid antibodies (aPL) [1]. Persistentlypositive lupus anticoagulant (LAC), moderate to high titers of antic-ardiolipin (aCL) or anti-β2-glycoprotein I (aβ2GPI) antibodies, in iso-lation or in any combination, are the aPL included in the updated re-vised classification criteria for APS [2].
This syndrome is currently considered the most frequent cause ofacquired thrombophilia. In a recent systematic review, the frequency ofaPL in young patients with cerebrovascular events was estimated at17%, increasing to 22% for aCL in patients with stroke [3]. Regardingpregnancy morbidity, myocardial infarction, and deep venous throm-bosis, the overall frequency of aPL was estimated as 6%, 11%, and9.5%, respectively [4]. These figures are of paramount importanceconsidering that APS is not only a frequent disorder but also an effec-tively treatable disease. In general, current consensus is to treat APSpatients with thrombotic manifestations with long-term oral antic-oagulation therapy and those with obstetric features with aspirin or thecombination of aspirin and heparin [5].
Approximately 1% of APS patients develop a severe clinical picture
characterized by multiple thromboses involving mainly small vessels[6]. In the first descriptions of this devastating type of APS, mortalityraised to 50% of patients [7]. Due to this poor prognosis, the term“catastrophic” was introduced to describe this life-threatening form ofAPS [8]. Patients with catastrophic APS (CAPS) have in common: a)clinical evidence of multiple organ involvement (commonly, three ormore organs) developing over a very short period of time; b) histo-pathological evidence of multiple small vessel occlusions, and c) la-boratory confirmation of the presence of aPL, usually in high titers [9].
Therefore, although uncommon, its potentially lethal outcome em-phasizes its importance in clinical medicine today. Most patients withCAPS end up in intensive care units (ICU) with multi-organ failure.Unless the condition is considered in the differential diagnosis by theattending physicians, it may be completely missed, resulting in a dis-astrous outcome for these patients [10].
Due to the rarity of this syndrome, an international registry of pa-tients with CAPS was created in 2000 by the European Forum onAntiphospholipid Antibodies, a network of research groups devoted to thedevelopment of multicenter projects with large populations of APSpatients [11]. This database is named “CAPS Registry” and currentlydocuments the clinical, laboratory and therapeutic data of more than500 patients with CAPS. The periodical analysis of these data has
https://doi.org/10.1016/j.jaut.2018.05.007Received 2 May 2018; Accepted 10 May 2018
∗ Corresponding author. Department of Autoimmune Diseases, Hospital Clínic, Villarroel, 170, 08036, Barcelona, Catalonia, Spain.E-mail addresses: [email protected], [email protected] (R. Cervera).
-RXUQDO�RI�$XWRLPPXQLW\������������²��
$YDLODEOH�RQOLQH����0D\�����������������������3XEOLVKHG�E\�(OVHYLHU�/WG�
7
Contents lists available at ScienceDirect
Journal of Autoimmunity
journal homepage: www.elsevier.com/locate/jautimm
The diagnosis and clinical management of the catastrophic antiphospholipidsyndrome: A comprehensive reviewRicard Cerveraa,∗, Ignasi Rodríguez-Pintób, Gerard Espinosaaa Department of Autoimmune Diseases, Hospital Clínic, Barcelona, Catalonia, Spainb Systemic Autoimmune Diseases Unit, Department of Internal Medicine, Hospital Mútua de Terrassa, Terrassa, Catalonia, Spain
A R T I C L E I N F O
Keywords:Catastrophic antiphospholipid syndromeTherapeuticsAnticoagulationCorticoidsPlasma exchangeIntravenous immunoglobulinsRituximabEculizumabSirolimus
A B S T R A C T
The catastrophic antiphospholipid syndrome (CAPS) is a life-threating variant of the antiphospholipid syndromecharacterized by the development of multiple thrombosis in a short period of time, usually ending up in thefailure of function of several vital organs. Most CAPS episodes are related to a prothrombotic situation or pre-cipitating factor such as infections, surgical procedures or malignant diseases. In patients with CAPS, the de-velopment of multiple thrombosis leads to an important cytokine release that worsens the already critical pa-tient's situation. The disease usually involves the kidneys, the lungs and the heart, although any organ systemcan be affected. Although occasionally the disease affects large vessels, in the majority of cases it affects smallvessels, leading to a disseminated microangiopathic syndrome resembling thrombotic thrombocytopenic pur-pura. Treatment is based on the administration of anticoagulants, corticosteroids, plasma exchange and/or in-travenous immunoglobulins. Cyclophosphamide is recommended in those CAPS cases associated to systemiclupus erythematosus. Additionally, rituximab and eculizumab have been used in refractory cases. Mortality isstill around 30% despite current treatment.
1. Introduction
The antiphospholipid syndrome (APS) is an autoimmune disordercharacterized by an increased risk of thrombosis and pregnancy lossassociated with antiphospholipid antibodies (aPL) [1]. Persistentlypositive lupus anticoagulant (LAC), moderate to high titers of antic-ardiolipin (aCL) or anti-β2-glycoprotein I (aβ2GPI) antibodies, in iso-lation or in any combination, are the aPL included in the updated re-vised classification criteria for APS [2].
This syndrome is currently considered the most frequent cause ofacquired thrombophilia. In a recent systematic review, the frequency ofaPL in young patients with cerebrovascular events was estimated at17%, increasing to 22% for aCL in patients with stroke [3]. Regardingpregnancy morbidity, myocardial infarction, and deep venous throm-bosis, the overall frequency of aPL was estimated as 6%, 11%, and9.5%, respectively [4]. These figures are of paramount importanceconsidering that APS is not only a frequent disorder but also an effec-tively treatable disease. In general, current consensus is to treat APSpatients with thrombotic manifestations with long-term oral antic-oagulation therapy and those with obstetric features with aspirin or thecombination of aspirin and heparin [5].
Approximately 1% of APS patients develop a severe clinical picture
characterized by multiple thromboses involving mainly small vessels[6]. In the first descriptions of this devastating type of APS, mortalityraised to 50% of patients [7]. Due to this poor prognosis, the term“catastrophic” was introduced to describe this life-threatening form ofAPS [8]. Patients with catastrophic APS (CAPS) have in common: a)clinical evidence of multiple organ involvement (commonly, three ormore organs) developing over a very short period of time; b) histo-pathological evidence of multiple small vessel occlusions, and c) la-boratory confirmation of the presence of aPL, usually in high titers [9].
Therefore, although uncommon, its potentially lethal outcome em-phasizes its importance in clinical medicine today. Most patients withCAPS end up in intensive care units (ICU) with multi-organ failure.Unless the condition is considered in the differential diagnosis by theattending physicians, it may be completely missed, resulting in a dis-astrous outcome for these patients [10].
Due to the rarity of this syndrome, an international registry of pa-tients with CAPS was created in 2000 by the European Forum onAntiphospholipid Antibodies, a network of research groups devoted to thedevelopment of multicenter projects with large populations of APSpatients [11]. This database is named “CAPS Registry” and currentlydocuments the clinical, laboratory and therapeutic data of more than500 patients with CAPS. The periodical analysis of these data has
https://doi.org/10.1016/j.jaut.2018.05.007Received 2 May 2018; Accepted 10 May 2018
∗ Corresponding author. Department of Autoimmune Diseases, Hospital Clínic, Villarroel, 170, 08036, Barcelona, Catalonia, Spain.E-mail addresses: [email protected], [email protected] (R. Cervera).
-RXUQDO�RI�$XWRLPPXQLW\������������²��
$YDLODEOH�RQOLQH����0D\�����������������������3XEOLVKHG�E\�(OVHYLHU�/WG�
7
ALGORITMO TERAPÉUTICO EN SAF CATASTRÓFICO

MUCHASGRACIAS
GUIA DE PRACTICA CLINICA PARA EL MANEJO DE SAF. European League Against Rheumatism
Recomendaciones SER sobre síndrome
Antifosfolípido primario