Embed Size (px)
Citation preview

Este, 31 marzo 2012
Lucas G Cavallaro UOC Gastroenterologia Ospedale San Martino, Belluno
EMR – ESD
perché l’endoscopia ?

Quale ruolo dell’endoscopia ?
• Diagnosi
• Resezione mucosa
• Staging EUS
• Trattamento emorragia
• Palliazione

Quale ruolo della resezione mucosa ?
• Diagnosi
• Resezione mucosa
• Staging EUS
• Trattamento emorragia
• Palliazione
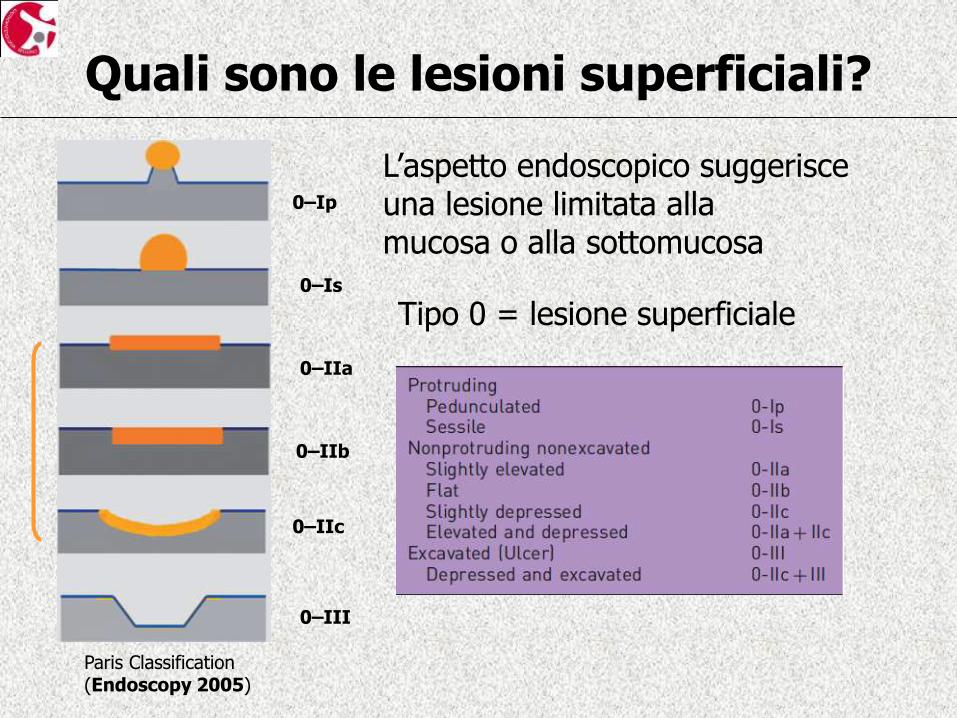
Quali sono le lesioni superficiali?
L’aspetto endoscopico suggerisce una lesione limitata alla mucosa o alla sottomucosa
0–Ip
0–Is
0–IIa
0–IIb
0–IIc
0–III
Paris Classification (Endoscopy 2005)
Tipo 0 = lesione superficiale
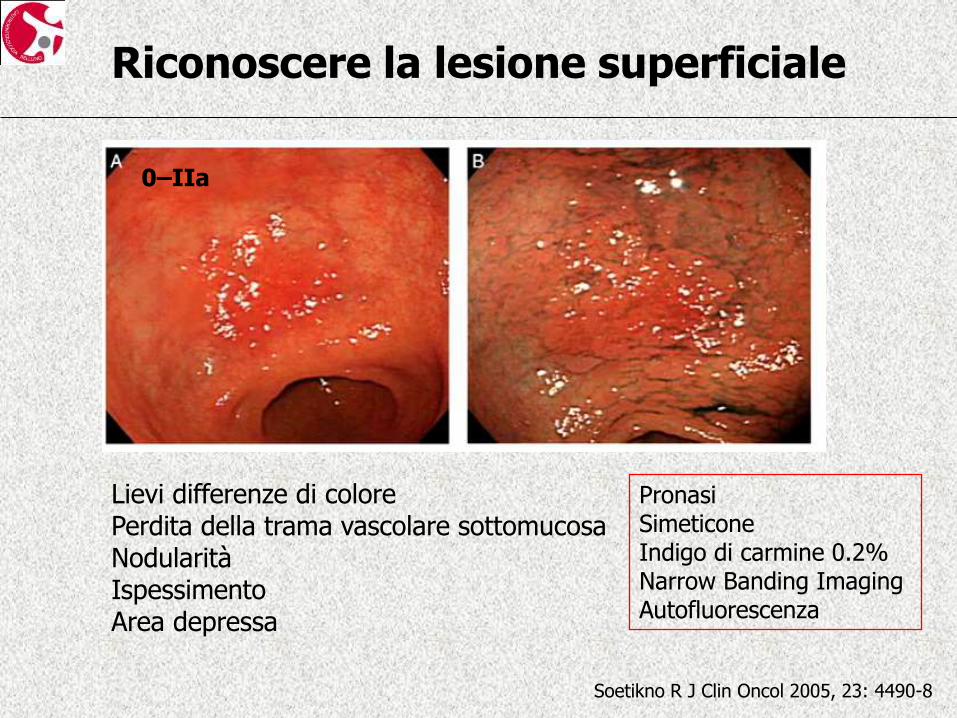
Riconoscere la lesione superficiale
Soetikno R J Clin Oncol 2005, 23: 4490-8
Lievi differenze di colore Perdita della trama vascolare sottomucosa Nodularità Ispessimento Area depressa
Pronasi Simeticone Indigo di carmine 0.2% Narrow Banding Imaging Autofluorescenza
0–IIa
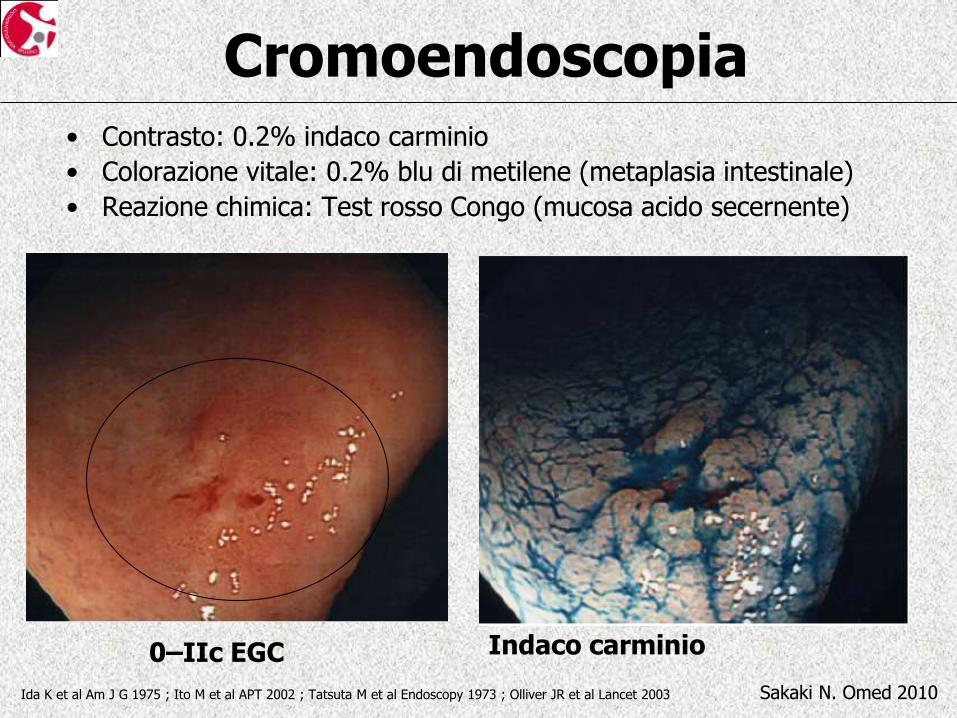
Cromoendoscopia • Contrasto: 0.2% indaco carminio
• Colorazione vitale: 0.2% blu di metilene (metaplasia intestinale)
• Reazione chimica: Test rosso Congo (mucosa acido secernente)
0–IIc EGC
Sakaki N. Omed 2010
Indaco carminio
Ida K et al Am J G 1975 ; Ito M et al APT 2002 ; Tatsuta M et al Endoscopy 1973 ; Olliver JR et al Lancet 2003

Magnificazione
Sakaki N. Omed 2010 Sakaki N et al Gastrointest Endosc 1980
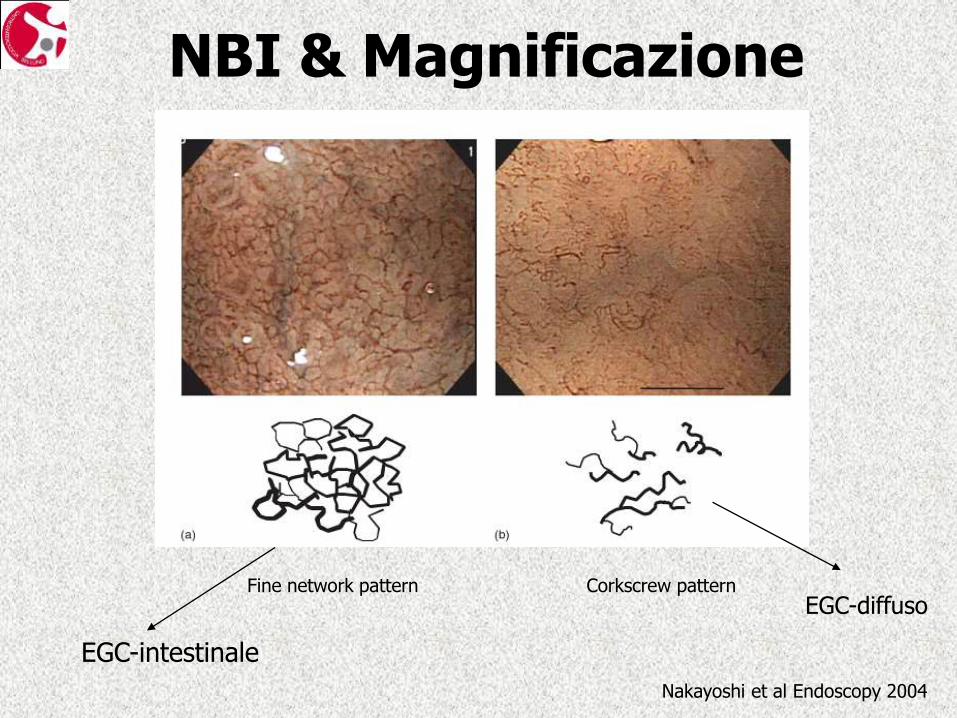
NBI & Magnificazione
Nakayoshi et al Endoscopy 2004
Corkscrew pattern Fine network pattern
EGC-intestinale
EGC-diffuso
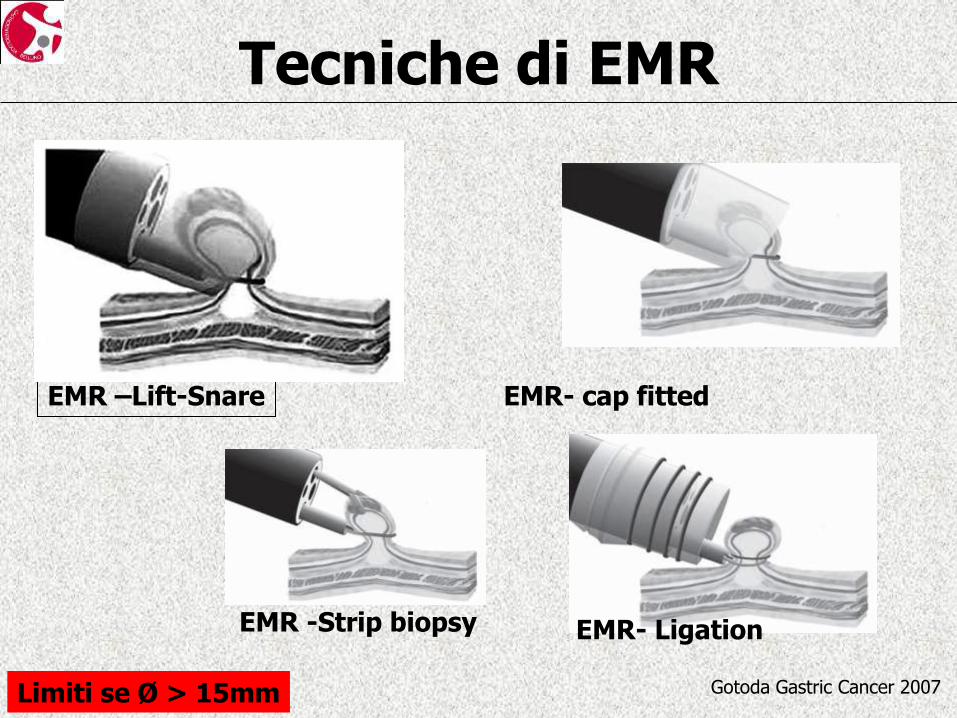
Tecniche di EMR
Gotoda Gastric Cancer 2007
EMR -Strip biopsy EMR- Ligation
EMR- cap fitted
Limiti se Ø > 15mm
EMR –Lift-Snare
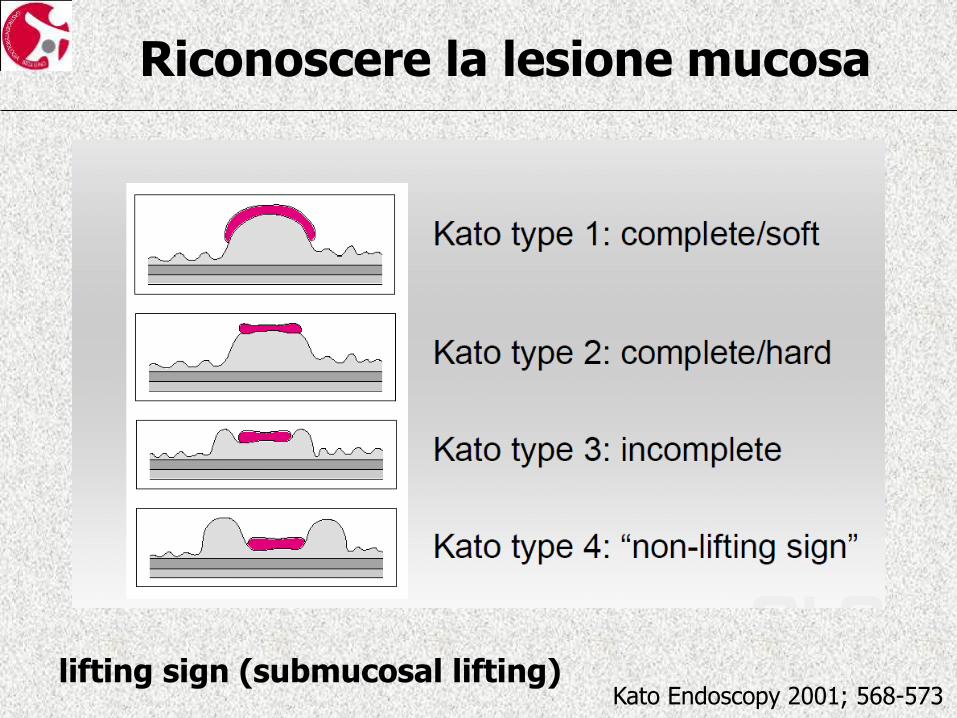
Riconoscere la lesione mucosa
Kato Endoscopy 2001; 568-573 lifting sign (submucosal lifting)
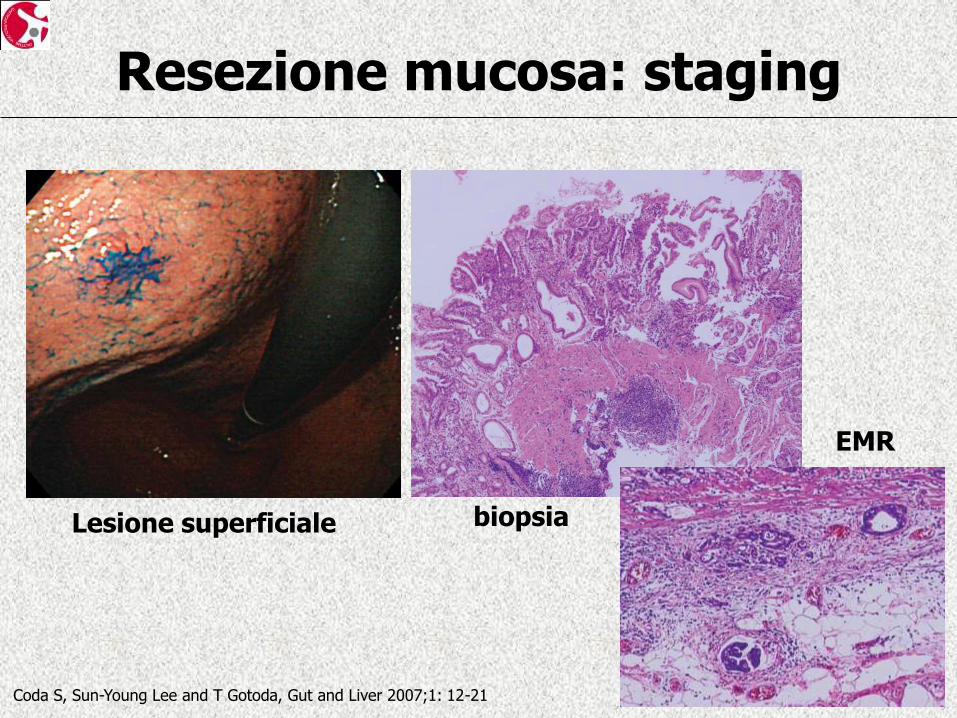
Resezione mucosa: staging
Lesione superficiale biopsia
EMR
Coda S, Sun-Young Lee and T Gotoda, Gut and Liver 2007;1: 12-21
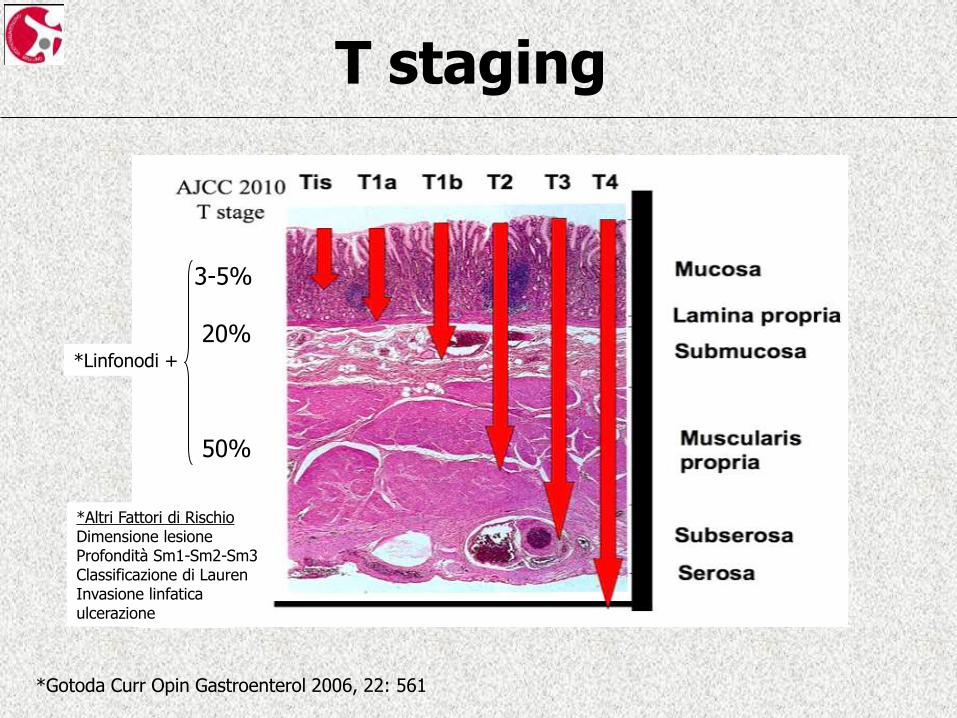
T staging
3-5% 20% 50%
*Linfonodi +
*Gotoda Curr Opin Gastroenterol 2006, 22: 561
*Altri Fattori di Rischio Dimensione lesione Profondità Sm1-Sm2-Sm3 Classificazione di Lauren Invasione linfatica ulcerazione
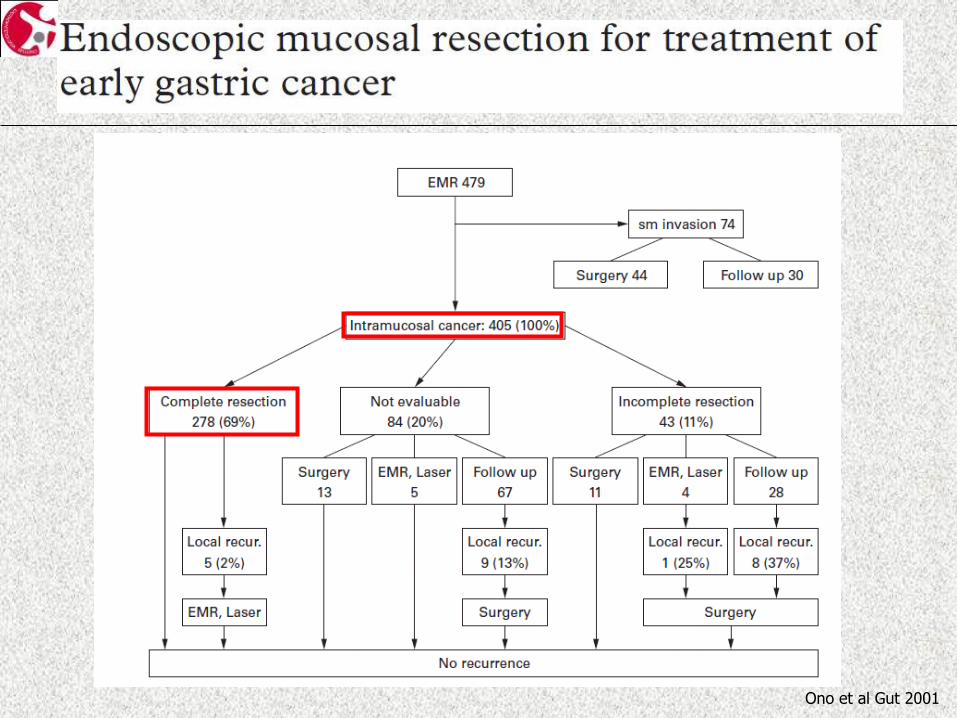
Ono et al Gut 2001
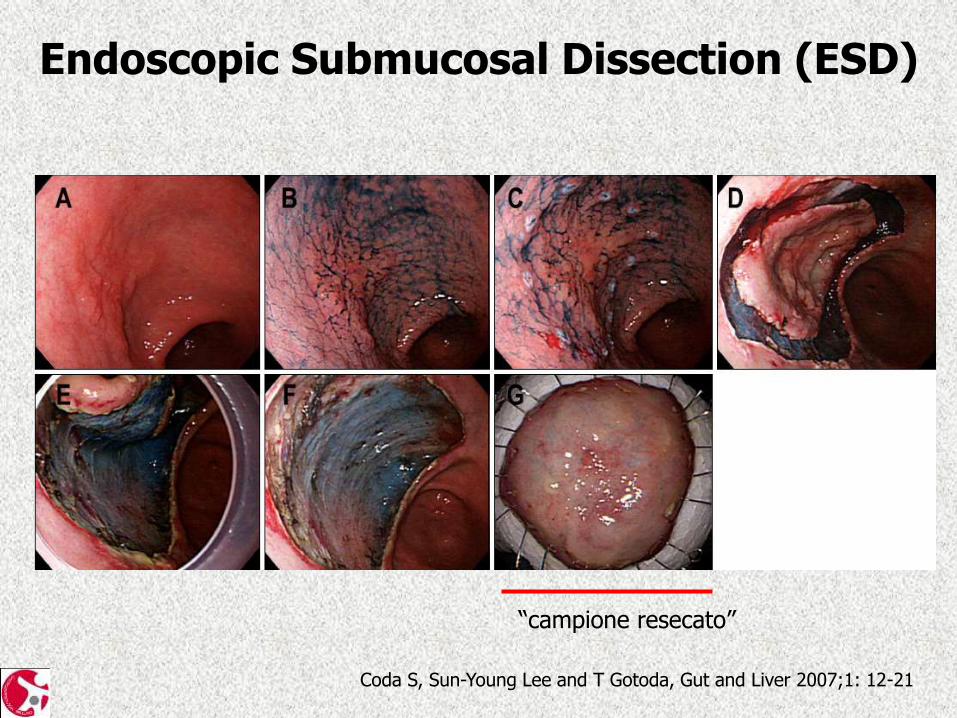
Endoscopic Submucosal Dissection (ESD)
Coda S, Sun-Young Lee and T Gotoda, Gut and Liver 2007;1: 12-21
“campione resecato”
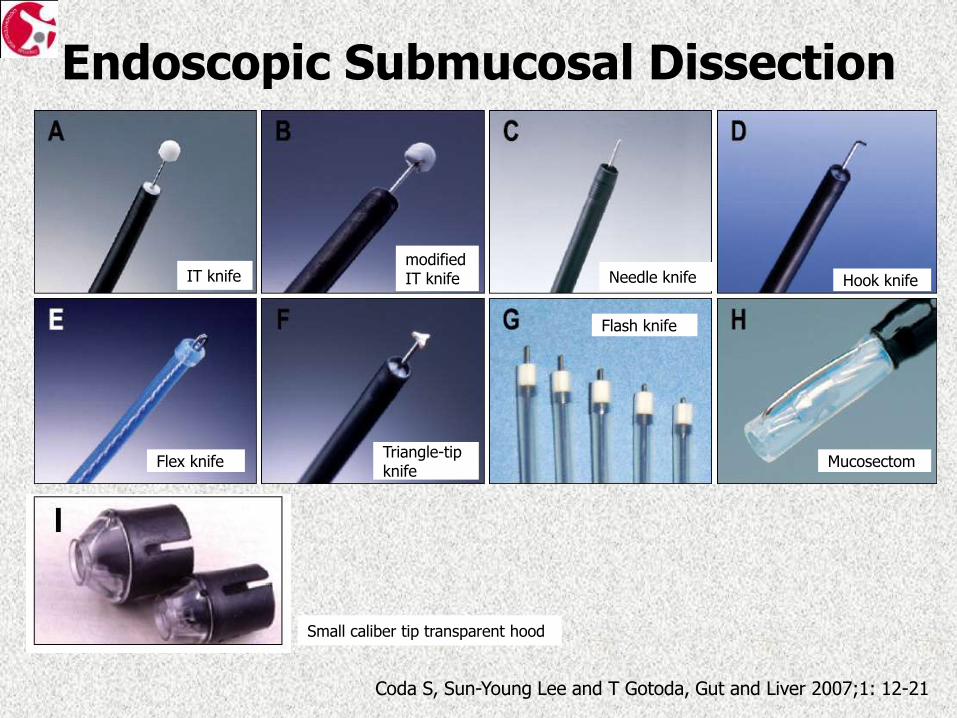
Endoscopic Submucosal Dissection
Coda S, Sun-Young Lee and T Gotoda, Gut and Liver 2007;1: 12-21
IT knife modifiedIT knife Needle knife Hook knife
Flex knife Triangle-tip knife
Flash knife
Mucosectom
Small caliber tip transparent hood
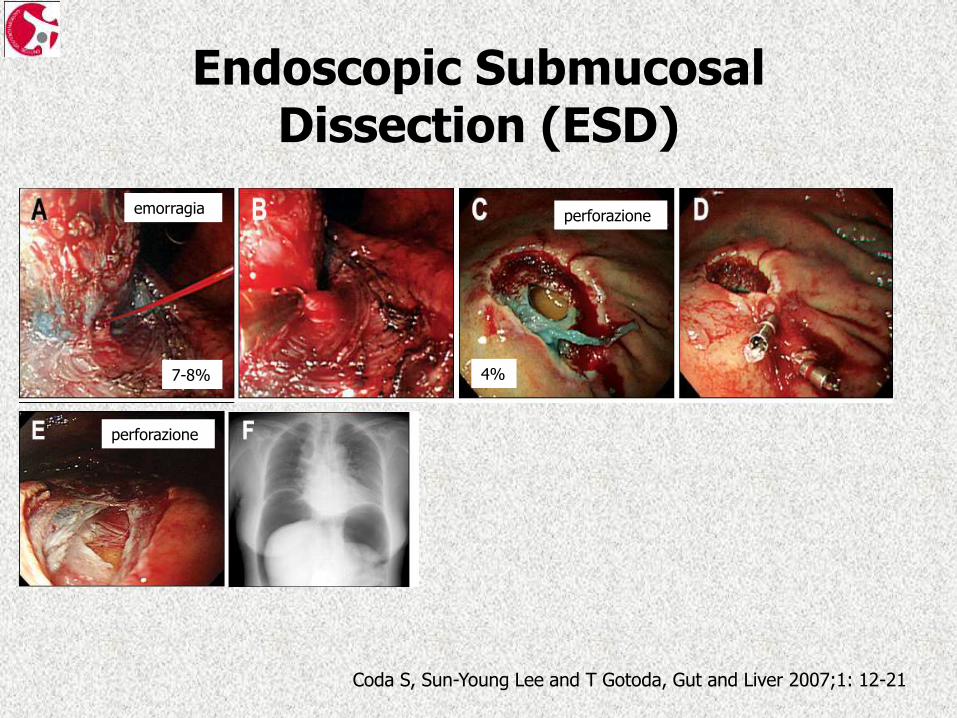
Endoscopic Submucosal Dissection (ESD)
Coda S, Sun-Young Lee and T Gotoda, Gut and Liver 2007;1: 12-21
perforazione
emorragia perforazione
7-8% 4%
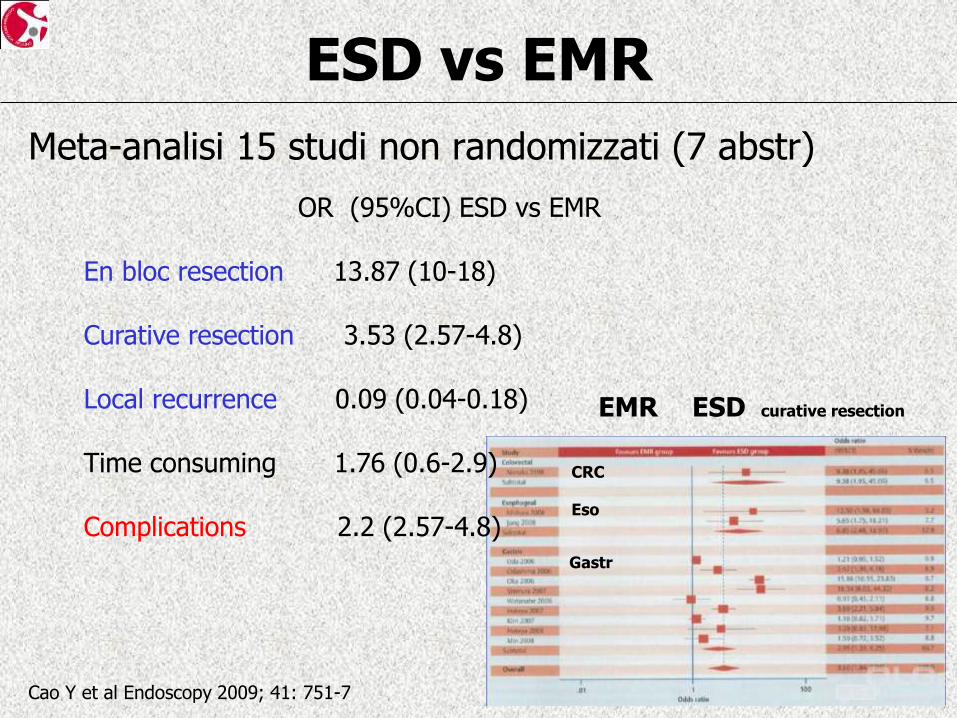
ESD vs EMR
Meta-analisi 15 studi non randomizzati (7 abstr)
Cao Y et al Endoscopy 2009; 41: 751-7
ESD curative resection EMR
CRC
Eso
Gastr
OR (95%CI) ESD vs EMR En bloc resection 13.87 (10-18) Curative resection 3.53 (2.57-4.8) Local recurrence 0.09 (0.04-0.18) Time consuming 1.76 (0.6-2.9) Complications 2.2 (2.57-4.8)
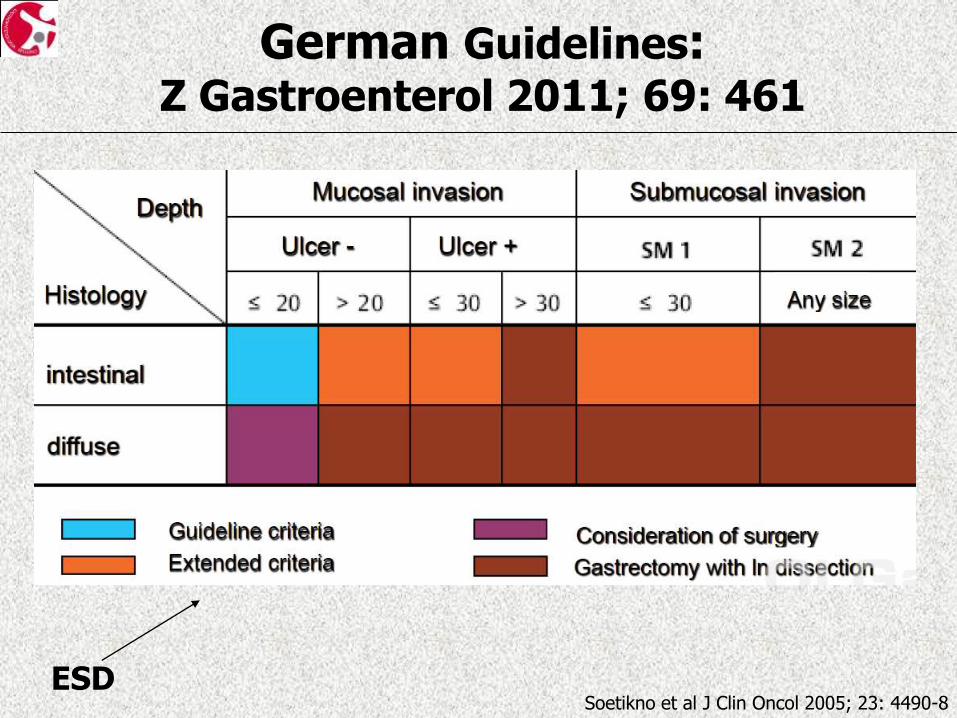
German Guidelines: Z Gastroenterol 2011; 69: 461
Soetikno et al J Clin Oncol 2005; 23: 4490-8 ESD
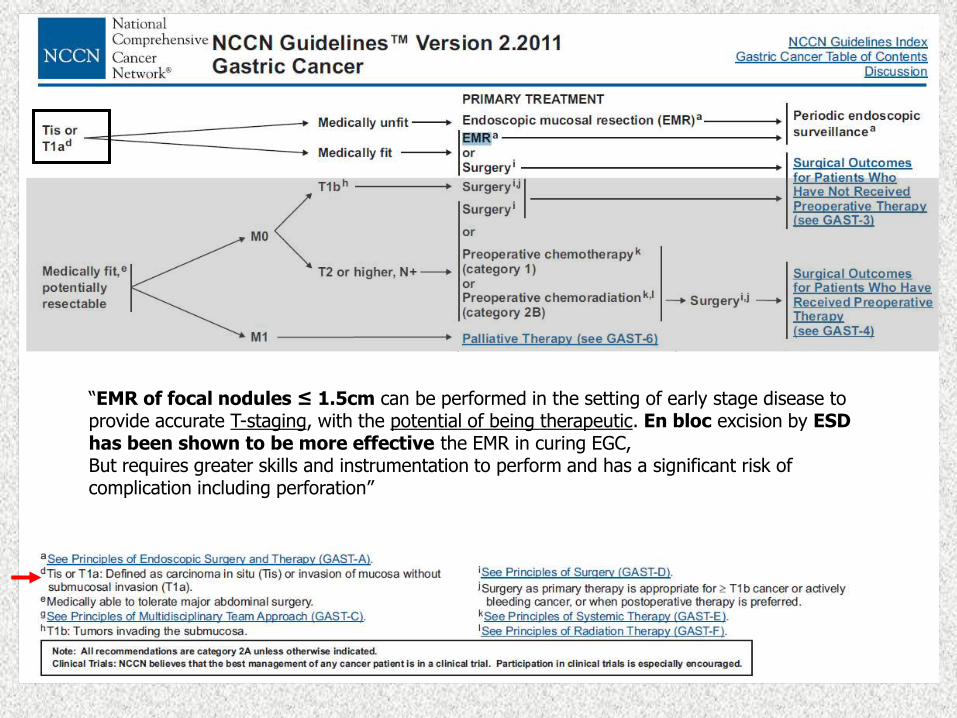
“EMR of focal nodules ≤ 1.5cm can be performed in the setting of early stage disease to provide accurate T-staging, with the potential of being therapeutic. En bloc excision by ESD has been shown to be more effective the EMR in curing EGC, But requires greater skills and instrumentation to perform and has a significant risk of complication including perforation”
Guidelines British Society of Gastroenterology and British Society of Surgical Oncology
Endoscopic adjuncts:
“The most well established…indigo carmine for early cancer in gastric mucosa. With the advent of new endoscopic modalities, these tecniques
may be superseded”
T staging
“EMR is the preferred approach for assessing mucosal and submucosal penetration in small early (T1) cancers” (m-sm)
Treatment: Endoscopy
“EMR and ESD can eradicate early gastro-oesophageal mucosal cancer. EMR should be considered in oesophageal mucosal cancer and both EMR
and ESD should be considered for gastric mucosal cancer”
Allum WH et al Gut 2011; 60: 1449-1472
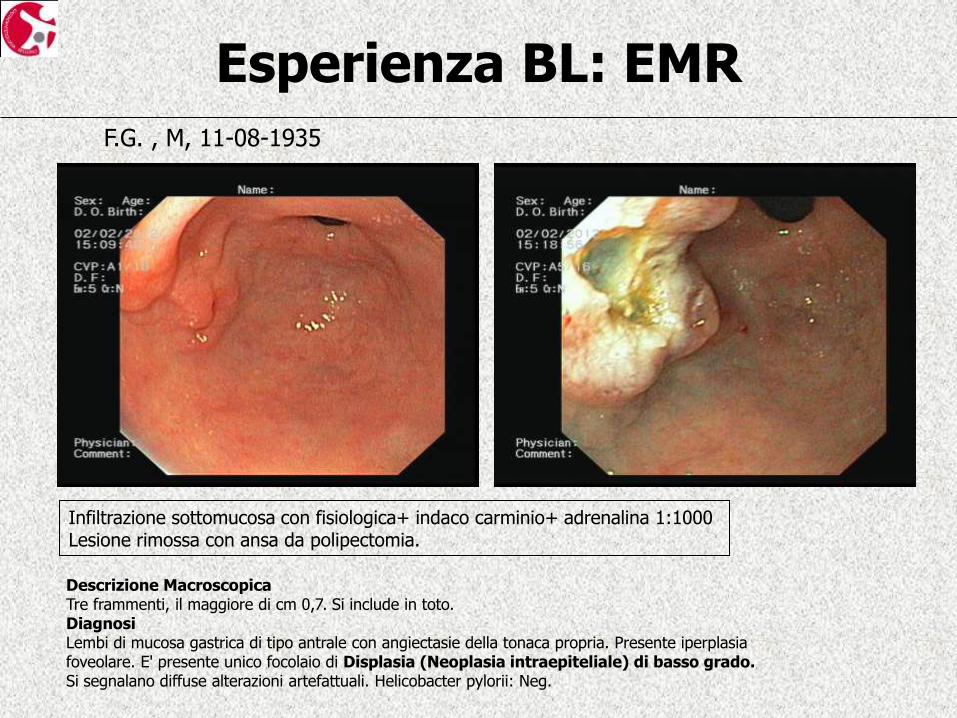
Esperienza BL: EMR
Descrizione Macroscopica Tre frammenti, il maggiore di cm 0,7. Si include in toto. Diagnosi Lembi di mucosa gastrica di tipo antrale con angiectasie della tonaca propria. Presente iperplasia foveolare. E' presente unico focolaio di Displasia (Neoplasia intraepiteliale) di basso grado. Si segnalano diffuse alterazioni artefattuali. Helicobacter pylorii: Neg.
Infiltrazione sottomucosa con fisiologica+ indaco carminio+ adrenalina 1:1000 Lesione rimossa con ansa da polipectomia.
F.G. , M, 11-08-1935