-
CASE REPORT Open Access
Endometrial carcinoma in a gravid uterus: acase report and
literature reviewMayu Shiomi, Shinya Matsuzaki* , Eiji Kobayashi,
Takeya Hara, Satoshi Nakagawa, Tsuyoshi Takiuchi,Kazuya Mimura,
Yutaka Ueda, Takuji Tomimatsu and Tadashi Kimura
Abstract
Background: Endometrial carcinoma (EC) is rarely diagnosed
during pregnancy. Therefore, the histopathologicalfindings,
clinical course, and gross appearance of the resected uterus during
pregnancy are not well known. Wepresent a case of EC diagnosed
during pregnancy. In addition, we reviewed the literature dating
from January 1995to March 2019 for cases of EC diagnosed during
pregnancy and within 15months after pregnancy, and we discussedthis
topic to improve the understanding of this rare condition.
Case presentation: A 35-year-old woman underwent an urgent
cesarean delivery in gestational week 35 due toantepartum bleeding
caused by placenta previa. Hysterectomy was performed with the
diagnosis of placenta accretaspectrum (PAS). Remarkably, the
postoperative gross and histopathological examinations revealed an
endometrioidadenocarcinoma (grade 1). The histopathological
findings revealed a pattern similar to that of EC not related
withpregnancy. Immunohistochemistry revealed an overexpression of
the estrogen and progesterone receptors; however,the p53 expression
was negative. We performed laparoscopic bilateral
salpingo-oophorectomy and pelviclymphadenectomy 102 days after the
cesarean hysterectomy, and confirmed surgical stage IA without
metastases. Ourpatient has had no recurrence in 4 years after the
cesarean delivery.An electronic search of the literature revealed
25 cases of EC (including our case) diagnosed during or after
pregnancy.Sixteen of the 25 patients were diagnosed after abortions
in the first trimester, 9 were diagnosed within 14months
ofchildbirth, and our case was the first with diagnosis from a
surgical specimen of peripartum hysterectomy due to thePAS. In 23
of the 25 cases endometrioid adenocarcinoma grade 1 to 2 was found,
and it seemed to have a goodprognosis.
Conclusion: The present findings suggest that careful
examination of a resected uterus is essential, even when surgeryis
performed for an obstetric indication. Our case is an extremely
rare case of EC during pregnancy; the histopathologicalpattern was
similar to that of typical EC, and no recurrence was noted. The
high levels of estrogen and progesteroneduring pregnancy did not
seem to promote tumor progression in our case.
Keywords: Placenta accreta spectrum, Placenta previa, Pregnancy,
Endometrioid carcinoma endometrial carcinoma,Endometrial cancer
This study presents a case of endometrioid carcinomadiagnosed
during pregnancy. We performed literaturereview and discussed this
topic. We have discussed theeffects of pregnancy on endometrioid
carcinoma in aprevious study. Our present study found the points
listedbelow.
1. Although endometrial carcinoma during pregnancyis extremely
rare, careful observation of the resecteduterus is needed to avoid
a missed diagnosis.
2. In our case, histopathological andimmunohistochemical
findings were consistent withendometrioid adenocarcinoma grade 1.
The patienthas been disease-free for about 4 years aftercesarean
hysterectomy. The high levels of estrogenand progesterone during
pregnancy did not seem topromote tumor progression in our case.
© The Author(s). 2019 Open Access This article is distributed
under the terms of the Creative Commons Attribution
4.0International License
(http://creativecommons.org/licenses/by/4.0/), which permits
unrestricted use, distribution, andreproduction in any medium,
provided you give appropriate credit to the original author(s) and
the source, provide a link tothe Creative Commons license, and
indicate if changes were made. The Creative Commons Public Domain
Dedication
waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies
to the data made available in this article, unless otherwise
stated.
* Correspondence: [email protected] of
Obstetrics and Gynecology, Osaka University Graduate Schoolof
Medicine, 2-2 Yamadaoka, Suita, Osaka 565-0871, Japan
Shiomi et al. BMC Pregnancy and Childbirth (2019) 19:425
https://doi.org/10.1186/s12884-019-2489-y
http://crossmark.crossref.org/dialog/?doi=10.1186/s12884-019-2489-y&domain=pdfhttp://orcid.org/0000-0001-5725-9994http://creativecommons.org/licenses/by/4.0/http://creativecommons.org/publicdomain/zero/1.0/mailto:[email protected]
-
3. Although high levels of estrogen (which has apromoting effect
on endometrioid carcinoma) andprogesterone (which has an anti-tumor
effect onendometrioid carcinoma) were observed, mostauthors
reported that the endometrioid carcinomaassociated with pregnancy
had a good prognosiswith minimal myometrial invasion.
BackgroundEndometrial carcinoma (EC) is the fourth most
commoncancer in women in high-income countries; however, ECcommonly
occurs in peri- or postmenopausal women,and only 5% of women are
diagnosed with adenocarcin-oma before the age of 40 years [1, 2].
Therefore, thecoexistence of EC and pregnancy is rare. Moreover,
ECis rarely detected during pregnancy or within a yearpostpartum
because the tumor can disrupt the preg-nancy. Although a previous
study had already reviewedthe latest 35 reports on EC coexisting
with pregnancyduring the last 80 years [3], the outcome of EC
associ-ated with pregnancy and the effect of pregnancy on ECis not
well known. Previous literature review alsoshowed that there have
been no reports of diagnosingEC during pregnancy in the surgical
specimen ofcesarean hysterectomy. Therefore, we report a case ofEC
diagnosed in a postoperative histopathological exam-ination after
total hysterectomy for placenta accretaspectrum (PAS), and we
additionally present the resultsof a literature review on this
matter.
Case presentationA 35-year-old woman (gravida 2, para 1) was
referred toour hospital due to placenta previa at gestational
week31. Her medical history was unremarkable, and her pre-vious
pregnancy was an uncomplicated, normal vaginal
delivery at gestational week 38. Her current pregnancywas
uncomplicated except for the placenta previa. Shedenied abnormal
genital bleeding before the currentpregnancy. Cervical cytology
performed during earlypregnancy was negative for intraepithelial
lesions. Vagi-nal ultrasonography revealed total placenta previa
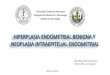
andone lacuna (Fig. 1a). Magnetic resonance imaging (MRI)at
gestational week 31 revealed total placenta previa andloss of the
myometrium between the placenta and blad-der wall (Fig. 1b). Other
MRI findings of PAS such asuterine bulging, heterogenous placenta,
and T2 darkband were not observed. Based on these findings,
wesuspected PAS, and an emergency cesarean delivery wasperformed
owing to antepartum bleeding (approximately100 mL) at gestational
week 35. An abdominal midlineincision was made, and a healthy male
infant weighing2274 g (− 0.42 SD) was delivered with Apgar scores
of 8and 9, at 1 and 5min, respectively. The placenta was
notdelivered within 30min after fetal delivery, thus requir-ing
hysterectomy for PAS. Estimated blood loss was1000 mL. The
postoperative course was uneventful, andthe patient and baby were
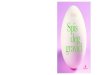
discharged on the 8th postop-erative day.Part of the chorion and
placenta were adhered to the
uterus (Fig. 2a). The resected uterus was divided to 7specimens
in order to perform macroscopic and histo-pathological analyses.
The surgical specimen showed awhite polyp measuring 2 cm, which
parted from theuterine fundus and the lower uterine segment (Fig.
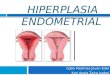
2b).Histopathological examination of the tumor involvingthe lower
uterine segment revealed endometrioid adeno-carcinoma (Grade 1),
with < 50% myometrial invasionand positive expression of
estrogen and progesterone re-ceptors, in addition to PAS (Fig. 3a
and b). Notably, thetumor involving the uterine fundus did not
show
Fig. 1 Images for assessment of placenta accreta spectrum. a
Transvaginal ultrasonography shows total placenta previa with one
lacuna. bMagnetic resonance imaging (MRI) at gestational week 31
revealed total placenta previa, and the placenta was located mainly
on the anteriorside. Although intraplacental T2 dark band, uterine
bulging, and heterogeneous placenta were not observed, we found
myometrial thinning ofthe anterior wall and loss of myometrium
between the placenta and bladder wall. The black arrow indicates
loss of uterine myometriumbetween the placenta and bladder wall.
Based on these findings, we suspected placenta accreta spectrum. No
abnormal finding was observed inthe fetus
Shiomi et al. BMC Pregnancy and Childbirth (2019) 19:425 Page 2
of 9
-
myometrial invasion. Histopathological findings weresimilar in
both tumors located in the uterine lower seg-ment and uterine
fundus. A retrospective review of theMRI images obtained during
pregnancy revealed thetumor involving the uterine fundus, although
involvementof the lower uterine segment was difficult to
detect(Fig. 3c). We performed a laparoscopic bilateral
salpingo-oophorectomy and pelvic lymphadenectomy 102 daysafter
cesarean hysterectomy and confirmed the absence ofmetastases. The
tumor was a stage IA lesion based on theInternational Federation of
Gynecology and Obstetricssystem. Follow-up performed 4 years after
cesareanhysterectomy revealed no recurrence.
Discussion and conclusionOur case demonstrated the gross and
histopathologicalfindings, MRI findings, and clinical course of EC
duringpregnancy. To discuss this rare condition, we performeda
literature review of cases of endometrioid carcinomaassociated with
pregnancy. We defined EC associatedwith pregnancy as diagnosed at
delivery to within 15months after pregnancy. We performed a search
ofPubMed, MEDLINE, and Scopus databases for theperiod between
January 1995 and March 2019, using thefollowing key words:
“endometrial cancer”, “endometrialcarcinoma”, “endometrioid
cancer”, “endometrioid car-cinoma”, “corpus cancer”, “pregnancy”,
“abortion”, and“postpartum” in various combinations. We
excludednon-English articles, discontinued journal and
thosepublished before 1995. We summarized the timing ofdiagnosis,
outcome of EC, symptoms, diagnosis of histo-pathological
examination, surgical stage (base on FIGO
2008) [4], and surgical treatment for EC. We also listedthe
authors’ opinions and discussions about the effect ofpregnancy on
the prognosis of EC.A total of 18 studies with 25 cases of EC
associated
with pregnancy (including our case) have been reported[3, 5–20];
9 cases were identified postpartum up to the14-month; 16 cases were
diagnosed at the time of D&Cfor first-trimester spontaneous or
elective abortion.These results suggest that clinicians should
consider ECafter pregnancy even though abnormal bleeding is
oftenobserved after pregnancy, and EC associated with preg-nancy is
rare. Our literature review revealed that therewere no previous
reports of a diagnosis of EC based onan examination of the resected
uterus following cesareanhysterectomy for PAS [3, 7]. Although our
case is ex-tremely rare, clinicians should check the
macroscopicfinding of the resected uterus carefully regardless of
theindication for hysterectomy.Our literature review showed that
the histopatho-
logical classification was endometrioid adenocarcinomagrade 1–2
in 23 of the 25 cases, unknown grade of endo-metrioid
adenocarcinoma in 1 of the 25 cases, andpoorly differentiated
adenosquamous carcinoma in 1 ofthe 25 cases. Immunohistochemical
(IHC) analysis wasperformed in 9 of the 24 cases and revealed a
typicalstaining pattern as previously reported [21, 22].
Previousreports have shown that women younger than 45 yearsrarely
developed EC, and the most common subtype ofclassification in
younger women was endometrioidadenocarcinoma grade 1–2 [23, 24].
Although the num-ber was limited, these results suggested that
pregnancydid not affect the subtype and IHC staining pattern of
Fig. 2 Macroscopic findings in the surgical specimen. a The
image shows gross findings in the uterus, which was resected due to
placentaaccreta spectrum. The white arrow indicates a white tumor
measuring 3 cm in diameter, involving the lower uterine segment,
which wasdiagnosed as endometrial carcinoma by histopathological
analysis. The tumor involving the uterine fundus is not
identifiable because it iscovered by the placenta. b The image
shows a longitudinal section of the uterus, which was divided into
7 sections. After the placenta wasremoved, a white tumor measuring
2 cm in diameter involving the uterine fundal segment was seen. The
black arrow indicates the 3-cmdiameter tumor which was endometrial
carcinoma involving the lower uterine segment; the white arrow
indicates the tumor involving theuterine fundus. Both tumors were
soft and white, and the macroscopic findings were similar in both
tumors
Shiomi et al. BMC Pregnancy and Childbirth (2019) 19:425 Page 3
of 9
-
EC. We considered that our literature review might bebiased
because we could include only published litera-ture and cases that
made it to the scientific publicationstage and this condition might
be under-reported; thus,this is the limitation of our study.The
case we presented is rare, and this report high-
lights several interesting points, as follows: 1. It
describesthe histopathological analysis of EC during pregnancy;
2.It describes a tumor involving the lower uterine segmentand
simultaneously the uterine fundus; and 3. Itdescribes the MRI
appearance of EC during pregnancy.Histopathological examination of
the specimen re-
vealed EC that presented as a well-differentiated
adeno-carcinoma with a focal cribriform pattern,
back-to-backstructure, and a papillary area. Although IHC
analysisshowed positive expression of estrogen and
progesteronereceptors, our patient did not demonstrate any
metasta-ses, and no recurrence was observed 4 years after
thecesarean hysterectomy. These features resemble those of
typical grade 1 endometrioid adenocarcinoma [25–27].We concluded
that the high-dose estrogen and proges-terone condition during
pregnancy did not promote pro-gression of the EC. As shown in Table
1, most authorsconsidered that pregnancy did not worsen the
prognosisof EC. Further cases are expected to discuss how
thepregnancy affects the prognosis of EC. Moreover,
thehistopathological and IHC findings in our case showedsimilar
pattern to those of typical EC.The reason for the presentation of
separate tumors at
the uterine fundus and lower uterine segment isunknown.
Histopathological analysis of both tumorsshowed similar findings;
thus, we concluded that thetumor presented as 2 separate growths at
the aforemen-tioned sites owing to enlargement of the uterus
duringpregnancy (although this remains speculative).
Otherpossibilities considered were metastasis or multi-site
in-volvement of EC. Myometrial invasion was insignificant;thus, we
excluded metastasis as a possible etiology. The
Fig. 3 Postoperative analysis of histopathological findings,
magnetic resonance imaging, and immunohistochemistry staining. a
The image showsthe histopathological findings in the resected
uterine specimen. Well-differentiated adenocarcinoma with focal
cribriform pattern, back-to-backstructure without intervening
stroma, and a papillary area are observed, and the glands have a
smooth luminal contour. The tumor showspredominant glandular growth
and a < 5% nonsquamous solid component; thus, the tumor was
diagnosed as endometrial cancer grade 1. Thetumor at the lower
uterine segment shows slight myometrial invasion. The white arrow
indicates the tumor in the uterine lower segment whichshows
invasion of the placenta decidua and uterine myometrium. The black
arrow indicates < 50% myometrial invasion (hematoxylin and
eosinstain, × 40.) b Immunohistochemistry analysis showed positive
expression of estrogen and progesterone receptors, and negative
expression ofp53. (Magnification, × 40.) c Retrospectively reviewed
magnetic resonance imaging (MRI) revealed endometrial carcinoma in
the uterine fundus. Asagittal T2-weighted MR image shows
endometrial carcinoma measuring 3 cm in diameter with signal
intensity resembling that of the placenta.The white arrow indicates
endometrial carcinoma involving the uterine fundus
Shiomi et al. BMC Pregnancy and Childbirth (2019) 19:425 Page 4
of 9
-
Table
1Asummaryof
theliteraturereview
finding
sforen
dometrio
idcarcinom
aassociated
with
preg
nancy
Firstauthor
Year
(Referen
cenu
mbe
r)
Age
(years)
Timingof
diagno
sis
Outocom
ePerio
dafter
diagno
sis
Symptom
sTheresults
ofhistop
atho
gical
exam
ination
Immun
ohisotoche
ical
staining
Stage
Surgicaltreatm
ent
Kovács
AG
1996
[5]
35Abo
rtion
NA
NED
1year
Abn
ormalge
nital
bleeding
EAgrade1–2
NA
IABrachytherapy+TA
H+BSO+RT
Theauthorshypo
thesized
that
preg
nancymay
adverselyaffect
thetumor
grow
th;how
ever,itcann
otbe
proven
becauseof
thelim
itednu
mbe
rof
cases.
KodamaJ
1997
[6]
30Po
stpartum
7mon
ths
DOD
8 mon
ths
Abn
ormalge
nital
bleeding
Poorlydifferentiated
aden
osqu
amou
scarcinom
a
NA
IIIC
C
Theauthorsop
ined
that
anim
mature,prog
esterone
-unrespo
nsiveen
dometriu
mcouldbe
thepo
ssiblemechanism
ofallowingen
dometrialcarcino
mato
developin
preg
nancy.
Schammel
DP
1998
[7]
38Abo
rtion
9weeks
NED
58 mon
ths
Infertility
EAgrade1
NA
IARepe
atcurettagewith
prog
esterone
therapy
41Abo
rtion
13weeks
NED
48 mon
ths
Abn
ormalge
nital
bleeding
EAgrade1
NA
IATA
H+BSO
29Abo
rtion
9–10
weeks
NA
NA
Non
eEA
grade1
NA
IANA
34Abo
rtion
13weeks
NED
12 mon
ths
Abn
ormalge
nital
bleeding
EAgrade1
NA
IATA
H+BSO
33Po
stpartum
During
cesarean
delivery
NED
57 mon
ths
Non
eEA
grade1
NA
IARepe
atcurettagewith
prog
esterone
therapy
Theauthorsconsidered
that
thefate
ofthemoreadvanced
-stage
tumorswith
deep
ermyometrialinvasionor
high
-grade
cytologicfeatures
may
beless
subjectto
theprotectiveeffectsof
gestational
prog
esterone
.
Ayhan
A1999
[8]
44Abo
rtion
5weeks
NA
NA
Abn
ormalge
nital
bleeding
EAgrade1
NA
IATA
H+BSO+LN
D+OM
Theauthorscitedaprevious
repo
rtwhich
observed
that
hCGinhibitstheDMBA
-indu
cedbreastcarcinog
enesisin
ratsthroug
han
insulin-like
grow
thfactor-dep
ende
ntmechanism
.
Foersterling
DL
1999
[9]
31Po
stpartum
9weeks
NED
1year
Abn
ormalge
nital
bleeding
EAgrade1
NA
IATA
H+BSO
Theauthorsop
ined
that
inpreg
nancy-associated
endo
metrialcarcino
ma,partof
theliningun
dergoe
sge
stationalchang
e,whe
reas
anothe
rpartbe
comes
neop
lastic.The
portionof
theen
dometriu
mwhich
becomes
neop
lasticmay
besensitive
toestrog
en,yet
unrespon
sive
toprog
esterone
.
Vaccarello
L1999
[10]
35Abo
rtion
9weeks
NED
31 mon
ths
Abn
ormalge
nital
bleeding
EAgrade1
NA
IATA
H+BSO
40Po
stpartum
4mon
ths
NED
6years
Abn
ormalge
nital
bleeding
EAgrade1
NA
IATA
H+BSO
32Po
stpartum
4mon
ths
NED
3.5years
Abn
ormalge
nital
bleeding
EAgrade2
NA
NA
TAH+BSO
They
conclude
dthat
with
concom
itant
secretoryen
dometriu
m,the
malignant
region
smustbe
prog
esterone
refractory.
Mitsushita
J2000
[11]
28Po
stpartum
6mon
ths
NA
NA
Previous
historyof
endo
metrio
idcarcinom
a
EAgrade1
ER:p
ositive
PR:p
ositive
IATA
H
Theauthorsdidno
tdiscusstheassociationbe
tweenpreg
nancyanden
dometrio
idcarcinom
a.
Shiomi et al. BMC Pregnancy and Childbirth (2019) 19:425 Page 5
of 9
-
Table
1Asummaryof
theliteraturereview
finding
sforen
dometrio
idcarcinom
aassociated
with
preg
nancy(Con
tinued)
Firstauthor
Year
(Referen
cenu
mbe
r)
Age
(years)
Timingof
diagno
sis
Outocom
ePerio
dafter
diagno
sis
Symptom
sTheresults
ofhistop
atho
gical
exam
ination
Immun
ohisotoche
ical
staining
Stage
Surgicaltreatm
ent
Kovács
AG
1996
[5]
35Abo
rtion
NA
NED
1year
Abn
ormalge
nital
bleeding
EAgrade1–2
NA
IABrachytherapy+TA
H+BSO+RT
IshiokaS
2000
[12]
25Po
stpartum
14mon
ths
NED
6 mon
ths
Abn
ormalge
nital
bleeding
EAgrade1
ER:p
ositive
PR:neg
ative
p53:ne
gative
IAmRH
+BSO+LN
D
Theauthorsconclude
dthat
theoccurren
ceof
postpartum
ECwas
extrem
elyrare
prob
ablydu
eto
theanti-tumor
effectsof
prog
esterone
.
IchikawaY
2001
[13]
35Po
stpartum
6mon
ths
NED
3.5years
Lower
abdo
minal
pain
EAgrade1
NA
IBTA
H+BSO+LN
D+OM+
App
ende
ctom
y
Theauthorsspeculated
that
high
prog
esterone
levelsdu
ringpreg
nancymay
protectagainstEC
.
ItohK
2004
[14]
39Po
stpartum
6mon
ths
NED
3years
Abn
ormalge
nital
bleeding
EAgrade1
ER:neg
ative
PR:neg
ative
IBTA
H+BSO+LN
D
Theauthorsconclude
dthat
theanticancereffect
ofprog
esterone
durin
gpreg
nancywas
ineffect
inthesetumors.
Hannu
naKY
2009
[3]
34Abo
rtion
12weeks
NED
18 mon
ths
Abo
rtion
EAgrade1–2
ER:p
ositive
PR:p
ositive
CK7:p
ositive
CK20:ne
gative
β-hC
G:neg
ative
E-cadh
erin:p
ositive
EpCAM:p
ositive
Placen
talalkaline
phosph
atase:po
sitive
IAD&C
Theauthorsspeculated
that
thepresen
ceof
ECmight
have
been
relatedto
ahypo
xicdamageof
thechorionicvilli.Itmight
sugg
estacausalcorrelationbe
tweenen
dometrialm
alignancyand
spon
tane
ousabortio
n.
Theauthorsfoun
dthat
mostcase
repo
rtsof
firsttrim
esterEA
arealso
repo
rted
asarisingin
afocallesion.
Terada
T2009
[15]
29Con
curren
ten
dometrial
aden
ocarcino
maandan
early
preg
nancyloss
NA
NA
Abo
rtion
EAgrade2
ER:p
ositive
PR:p
ositive
p53:po
sitive
vimen
tin:positive
CA19–9:focalpo
sitive
CA125:po
sitive
Ki-67:80%
labe
lling
CEA
:neg
ative
PTEN
:neg
ative
p16:ne
gative
NA
Repe
atcurettagewith
out
prog
esterone
therapy
Theauthorsconsidered
that
ECassociated
with
preg
nancyweremostly
instages
IA,and
werehistolog
icallyEA
s.
AkilA
2012
[16]
45Con
curren
ten
dometrial
aden
ocarcino
maandan
early
preg
nancyloss
NA
NA
Abo
rtion
EAgrade1
NA
IATA
H+BSO+LN
D
Theauthorsconclude
dthat
theroutinehistolog
icalexam
inationof
thecurettagespecim
ensforallfirsttrim
esterabortio
ns,ind
epen
dent
oftheageof
thepatient,sho
uldbe
encouraged
.
SaciragicL
2014
[17]
36Abo
rtion
8weeks
NA
NA
Abn
ormalge
nital
bleeding
EAgrade1
Ki67:p
ositive
IATA
H+BSO+LN
D
Shiomi et al. BMC Pregnancy and Childbirth (2019) 19:425 Page 6
of 9
-
Table
1Asummaryof
theliteraturereview
finding
sforen
dometrio
idcarcinom
aassociated
with
preg
nancy(Con
tinued)
Firstauthor
Year
(Referen
cenu
mbe
r)
Age
(years)
Timingof
diagno
sis
Outocom
ePerio
dafter
diagno
sis
Symptom
sTheresults
ofhistop
atho
gical
exam
ination
Immun
ohisotoche
ical
staining
Stage
Surgicaltreatm
ent
Kovács
AG
1996
[5]
35Abo
rtion
NA
NED
1year
Abn
ormalge
nital
bleeding
EAgrade1–2
NA
IABrachytherapy+TA
H+BSO+RT
Theauthorsdiscussedthat
inawom
anwith
prog
esterone
-resistant
endo
metriu
m,d
evelop
men
tof
endo
metrialcarcino
macouldbe
potentiatedby
therelativelyhype
restroge
nicen
vironm
entof
early
preg
nancyandsubseq
uentlyallowed
toproliferate
furthe
rdu
eto
alack
ofrespon
seto
prog
esterone
.
Bayoglu
TekinY
2014
[18]
36Abo
rtionor
ectopic
preg
nancy
NA
NED
1year
Ectopicpreg
nancy
EAgrade1
NA
NA
Curettage
with
prog
esterone
therapy
Theauthorsthou
ghthat
thepresen
ceof
ECmight
have
been
relatedto
thedamageof
thechorionicvilli,sug
gestingacausalcorrelationbe
tweenEC
andspon
tane
ousabortio
ns.
Zhou
F2015
[19]
40Con
curren
ten
dometrial
aden
ocarcino
maandan
early
preg
nancyloss
NA
NA
Abo
rtion
EAgrade1
ER:p
ositive
PR:p
ositive
p53:ne
gative
NA
Repe
atcurettagewith
out
prog
esterone
therapy
33Con
curren
ten
dometrial
aden
ocarcino
maandan
early
preg
nancyloss
NA
NA
Abo
rtion
EAgrade1
ER:p
ositive
PR:p
ositive
p53:ne
gative
NA
Repe
atcurettagewith
out
prog
esterone
therapy
Theauthorsconsidered
that
thecarefulh
istologicalexaminationof
thecurettagespecim
ensforallfirsttrim
esterpreg
nancylosses
shou
ldbe
encouraged
.
RizzutoI
2019
[20]
29Preg
nancyof
7weeks
gestation
NA
NED
8years
Abn
ormalge
nital
bleeding
EANA
NA
Serialend
ometrialb
iopsywith
insertionof
aLevono
rgestrel
intrauterin
ede
vice
Con
servativemanagem
entforEC
inyoun
gwom
enispo
ssibleinclud
ingacase
with
anincide
ntaldiagno
sisin
preg
nancy.
Our
case
2019
35Placen
taaccreta
spectrum
Cesarean
hysterectomy
NED
4years
Non
eEA
grade1
ER:p
ositive
PR:p
ositive
p53:ne
gative
IACesareanhysterectomy
Laparoscop
icBSO+LN
D
List
ofab
breviatio
ns:B
SOBilateralsalping
o-oo
phorectomy,CChe
mothe
rapy
,CK7
Cytok
eratin
7,CK
20Cytok
eratin
20,C
A19–9
Can
ceran
tigen
19–9
,CA125Can
ceran
tigen
125,
CEACarcino
embryo
nican
tigen
,D&C
Dilatatio
nan
dcurettag
e,DODDeadof
disease,
EAEA
,ECen
dometrio
idcarcinom
a,EpCA
MEp
ithelialcella
dhesionmolecule,
EREstrog
enreceptor,β
-hCG
Hum
anchorionicgo
nado
trop
inβ-subu
nit,LN
DLymph
node
dissectio
n,mRH
Mod
ified
radicalh
ysterectom
y,NANot
available,
NED
Noeviden
ceof
disease,
OM
Omen
tectom
y,PR
Prog
esterone
receptor,R
TRa
diationtherap
y,TA
HTran
sabd
ominal
hysterectomy
Shiomi et al. BMC Pregnancy and Childbirth (2019) 19:425 Page 7
of 9
-
possibility of multi-site involvement of EC is difficult
toexclude; however, the estimated frequency of this condi-tion is
low. Therefore, we concluded that the tumor sep-aration could be
attributed to the uterine enlargementduring pregnancy.MRI scans
were retrospectively analyzed after the
cesarean hysterectomy. We observed a lesion in theuterine fundus
measuring approximately 3 cm in diam-eter with signal intensity
similar to that of the placenta.Notably, this lesion was separate
from the placenta. Cli-nicians must consider the possibility of EC
in womenwith MRI scans showing such lesions during pregnancy.In
conclusion, our findings in this case suggest that
careful analysis of MRI findings during pregnancy andgross
examination of the resected uterus (in patientsundergoing
hysterectomy for obstetric complications)are essential, although EC
during pregnancy is extremelyrare. The literature review suggested
that EC associatedwith pregnancy seemed to have a good
prognosis.
AbbreviationsD&C: Dilatation & Curettage; EC:
Endometrial carcinoma;IHC: Immunohistochemical; MRI: Magnetic
resonance imaging; PAS: Placentaaccreta spectrum
AcknowledgementsThe authors thank H. Abe and K. Sakiyama for
administrative assistance inthe preparation of this manuscript.
Authors’ contributionsMS, SM, EK, and YU made substantial
contributions to conception anddesign, collected the clinical data
and drafted as well as revised themanuscript. EK, TH, SN, TTa, TTo,
and KM helped in reviewing the previousstudies and drafting the
manuscript. TK conceived and generally supervisedof this study, and
gave final approval of the version to be published. Allauthors read
and approved the final manuscript.
FundingThere is no source of financial support or funding.
Availability of data and materialsNot applicable.
Ethics approval and consent to participateThis study was
approved by the Institutional Review Board and the EthicsCommittee
of the Osaka University Hospital (approval #15240, approved
onSeptember 10, 2015).
Consent for publicationWritten informed consent was obtained
from the patient for publication ofthis case report and any
accompanying images. A copy of the writtenconsent is available for
review by the Editor of this journal.
Competing interestsShinya Matsuzaki is an Associate Editor for
BMC Pregnancy and Childbirth.The authors declare no conflicts of
interest about this study. All of authorshave no competing
financial interests regarding this study.
Received: 3 June 2019 Accepted: 4 September 2019
References1. Soliman PT, Oh JC, Schmeler KM, Sun CC, Slomovitz
BM, Gershenson DM,
et al. Risk factors for young premenopausal women with
endometrialcancer. Obstet Gynecol. 2005;105:575–80.
2. Jordan SJ, Na R, Johnatty SE, Wise LA, Adami HO, Brinton LA,
et al.Breastfeeding and endometrial Cancer risk: an analysis from
theepidemiology of endometrial Cancer consortium. Obstet Gynecol.
2017;129:1059–67.
3. Hannuna KY, Putignani L, Silvestri E, Pisa R, Angioli R,
Signore F. Incidentalendometrial adenocarcinoma in early pregnancy:
a case report and reviewof the literature. Int J Gynecol Cancer.
2009;19:1580–4.
4. Pecorelli S. Revised FIGO staging for carcinoma of the vulva,
cervix, andendometrium. Int J Gynaecol Obstet. 2009;105:103–4.
5. Kovacs AG, Cserni G. Endometrial adenocarcinoma in early
pregnancy.Gynecol Obstet Investig. 1996;41:70–2.
6. Kodama J, Yoshinouchi M, Miyagi Y, Kobashi Y, Kamimura S,
Okuda H, et al.Advanced endometrial cancer detected at 7 months
after childbirth.Gynecol Oncol. 1997;64:501–6.
7. Schammel DP, Mittal KR, Kaplan K, Deligdisch L, Tavassoli FA.
Endometrialadenocarcinoma associated with intrauterine pregnancy. A
report of fivecases and a review of the literature. Int J Gynecol
Pathol. 1998;17:327–35.
8. Ayhan A, Gunalp S, Karaer C, Gokoz A, Oz U. Endometrial
adenocarcinomain pregnancy. Gynecol Oncol. 1999;75:298–9.
9. Foersterling DL, Blythe JG. Ovarian carcinoma, endometrial
carcinoma, andpregnancy. Gynecol Oncol. 1999;72:425–6.
10. Vaccarello L, Apte SM, Copeland LJ, Boutselis JG, Rubin SC.
Endometrialcarcinoma associated with pregnancy: a report of three
cases and review ofthe literature. Gynecol Oncol.
1999;74:118–22.
11. Mitsushita J, Toki T, Kato K, Fujii S, Konishi I.
Endometrial carcinomaremaining after term pregnancy following
conservative treatment withmedroxyprogesterone acetate. Gynecol
Oncol. 2000;79:129–32.
12. Ishioka S, Sagae S, Saito T, Sugimura M, Akutagawa N,
Nishimura M, et al. Acase of uterine endometrial carcinoma 15
months post-partum. J ObstetGynaecol Res. 2000;26:417–20.
13. Ichikawa Y, Takano K, Higa S, Tanabe M, Wada A, Sugita M, et
al.Endometrial carcinoma coexisting with pregnancy, presumed to
derivefrom adenomyosis: a case report. Int J Gynecol Cancer.
2001;11:488–90.
14. Itoh K, Shiozawa T, Shiohara S, Ashida T, Konishi I.
Endometrial carcinoma inseptate uterus detected 6 months after
full-term delivery: case report andreview of the literature.
Gynecol Oncol. 2004;93:242–7.
15. Terada T. Endometrial adenocarcinoma in spontaneous
abortion. Pathology.2009;41:694–5.
16. Akil A, Kaya B, Karabay A, Kibar Y. Concurrent endometrial
adenocarcinomaand an early pregnancy loss. Arch Gynecol Obstet.
2012;286:1089–90.
17. Saciragic L, Ball CG, Islam S, Fung-Kee-Fung M. Incidental
endometrialcarcinoma diagnosed at first trimester pregnancy loss: a
case report. JObstet Gynaecol Can. 2014;36:1010–3.
18. Bayoglu Tekin Y, Guvendag Guven ES, Sehitoglu I, Guven S.
Tubalpregnancy associated with endometrial carcinoma after in vitro
fertilizationattempts. Case Rep Obstet Gynecol.
2014;2014:481380.
19. Zhou F, Qian Z, Li Y, Qin J, Huang L. Endometrial
adenocarcinoma inspontaneous abortion: two cases and review of the
literature. Int J Clin ExpMed. 2015;8:8230–3.
20. Rizzuto I, Nicholson R, Dickinson K, Juang HJ, MacNab W,
Rufford B. A caseof incidental endometrial adenocarcinoma diagnosed
in early pregnancyand managed conservatively. Gynecol Oncol Rep.
2019;28:101–3.
21. Cancer Genome Atlas Research N, Kandoth C, Schultz N,
Cherniack AD,Akbani R, Liu Y, et al. Integrated genomic
characterization of endometrialcarcinoma. Nature.
2013;497(7447):67–73.
22. Murali R, Soslow RA, Weigelt B. Classification of
endometrial carcinoma:more than two types. Lancet Oncol.
2014;15:e268–78.
23. Reed SD, Newton KM, Clinton WL, Epplein M, Garcia R, Allison
K, et al.Incidence of endometrial hyperplasia. Am J Obstet Gynecol.
2009;200:678 e1–6.
24. Committee on Practice B-G. Practice bulletin no. 128:
diagnosis of abnormaluterine bleeding in reproductive-aged women.
Obstet Gynecol. 2012;120:197–206.
25. Matsuo K, Machida H, Shoupe D, Melamed A, Muderspach LI,
Roman LD,et al. Ovarian conservation and overall survival in young
women with early-stage low-grade endometrial Cancer. Obstet
Gynecol. 2016;128:761–70.
26. Sorosky JI. Endometrial cancer. Obstet Gynecol. 2008;111(2
Pt 1):436–47.27. Guan J, Xie L, Luo X, Yang B, Zhang H, Zhu Q, et
al. The prognostic
significance of estrogen and progesterone receptors in grade I
and IIendometrioid endometrial adenocarcinoma: hormone receptors in
riskstratification. J Gynecol Oncol. 2019;30:e13.
Shiomi et al. BMC Pregnancy and Childbirth (2019) 19:425 Page 8
of 9
-
Publisher’s NoteSpringer Nature remains neutral with regard to
jurisdictional claims inpublished maps and institutional
affiliations.
Shiomi et al. BMC Pregnancy and Childbirth (2019) 19:425 Page 9
of 9
AbstractBackgroundCase presentationConclusion
BackgroundCase presentationDiscussion and
conclusionAbbreviationsAcknowledgementsAuthors’
contributionsFundingAvailability of data and materialsEthics
approval and consent to participateConsent for publicationCompeting
interestsReferencesPublisher’s Note