Embed Size (px)
Citation preview

Surg Today (2001) 31:1–4
Original Articles
Endoscopic Subtotal Thyroidectomy for Patients with Graves’ Disease
Masahide Yamamoto, Akira Sasaki, Hiroshi Asahi, Yutaka Shimada, Nobuhiro Sato, Jun Nakajima,Rie Mashima, and Kazuyoshi Saito
Department of Surgery 1, Iwate Medical University School of Medicine, 19-1 Uchimaru, Morioka, Iwate 020-8505, Japan
We applied this technique to perform subtotal thyroi-dectomy in 12 patients with Graves’ disease, and reportour results herein.
Patients and Methods
Patients
We performed endoscopic subtotal thyroidectomyvia a precordial approach on 12 patients with Graves’disease at Iwate Medical University Hospital betweenNovember 1998 and November 1999. The patientsincluded eight women and four men, aged from 15 to 59years, with a mean age of 27.7 years.
All of the patients expressed concern about cervicalscarring, and elected to undergo the new method.Written informed consent was obtained from eachpatient.
Anesthesia and Body Position
Under general anesthesia with endotracheal intubation,the patient was placed in the supine position, shouldersresting on pillows with the neck extended. To preventsubcutaneous emphysema developing in the face, flowtension pads were placed along the mandible.
Trocar Insertion
The first skin incision, which was 1.5 cm long, was madein the right breast at the height of the nipple. Bluntdigital dissection using dressing forceps, from theprecordial region to the anterior cervical region, wasperformed to create a subcutaneous tunnel. Dissectionwas extended to the superior margin of the thyroidcartilage cranially, and to the external margin of thesternocleidomastoid muscle laterally. A 12-mm trocarwas inserted subcutaneously, and 5mmHg carbon
Abstract Endoscopic thyroidectomy performed via theprecordial approach leaves no scarring of the neck, andthus provided excellent results from a cosmetic view-point. We applied this technique to perform subtotalthyroidectomy in 12 patients with Graves’ disease.Three trocars were inserted in the precordial region,and endoscopic surgery was performed with carbondioxide insufflation. Vessel management and thyroi-dectomy were carried out using ultrasonic coagulationdevices. The mean operative time was 259.8 min, andthe mean blood loss was 90.2ml. There were no post-operative complications such as subcutaneous emphy-sema or hemorrhage, although hypoparathyroidism andrecurrent laryngeal nerve paralysis occurred in onepatient. Cosmetically esthetic results were achieved inall patients. These findings indicate that this surgicaltechnique represents an effective method of treatingGraves’ disease that provides excellent cosmetic results.
Key words Endoscopic thyroidectomy · Graves’ disease ·Subtotal thyroidectomy
Introduction
Thyroid surgery is traditionally performed througha cervical collar incision; however, many patients,especially young ones, are opposed to any scarring inthe cervical region. Ishii et al. developed a method ofperforming endoscopic thyroidectomy via a precordialapproach which leaves absolutely no postoperativescarring in the neck and thus provides a cosmeticallyappealing alternative.1
Reprint requests to: M. YamamotoReceived: February 18, 2000 / Accepted: July 25, 2000

2 M. Yamamoto et al.: Endoscopic Thyroidectomy for Graves’ Disease
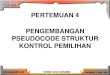
dioxide was insufflated to create a space around thestrap muscles. A flexible endoscope was inserted. Thesecond skin incision was made at the external marginof the left areola cranially, and a 10-mm trocar wasinserted under the scope. The third skin incisionwas made at the external margin of the right areolacranially, and a 5-mm trocar was inserted using the sametechnique (Fig. 1).
Surgical Procedure
An ultrasonic coagulation device (AutoSonix, AutoSuture Japan, Japan) was inserted through the trocar onthe left side for separation, vessel management, andthyroidectomy; no clamps or ligatures were used to con-trol bleeding. With the aid of palpation from the out-side, longitudinal and transverse incisions of the strapmuscles were made. After exposing the thyroid in the
precervical space, the inferior pole of the right lobe wasfreed by blunt dissection. This part was lifted, and theright inferior thyroid vein was cut. The thyroid glandwas cut at the isthmus. The upper part of the right lobewas then separated laterally, and the right superiorthyroid artery and vein were cut. A sponge model of1.0g measuring the residual thyroid volume was placedadjacently, and the thyroid parenchyma was excised incomparison with the thyroid model.2 The right residualthyroid gland was approximately 1.0–2.0g. The speci-men was placed in a plastic bag (Endocatch, AutoSuture Japan), and extracted through the first 1.5-cmaccess. The left lobe was then excised using the sametechnique. The left residual thyroid gland was alsoapproximately 1.0–2.0g. After cleaning the cavity withphysiological saline solution, the strap muscles weresutured. A 3-mm closed suction drain was placed underthe strap muscle through the site of the trocar on theright. The skin incision was sutured intradermally.
Results
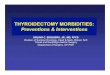
The mean operative time was 259.8min, with a range of175–420min, and the mean blood loss was 90.2ml, witha range of 5–343ml. The mean excised thyroid weightwas 44.1 g, with a range of 18–92g. When the excisedthyroid weight was larger, a tendency toward a longeroperative time and greater blood loss was noted (Table1). The recurrent laryngeal nerves were visualized inthree patients (Fig. 2a) and the parathyroid glands werevisualized and preserved in five patients (Fig. 2b).Subcutaneous emphysema of the face was not seen inany patient during or after surgery. Cardiorespiratorydynamics were stable during surgery, and the end tidalCO2 was normal at 36–38 mmHg. There were nopostoperative complications, such as hemorrhage orsevere pain requiring relief with an analgesic agentsmore than once. Unfortunately, recurrent laryngeal
Fig. 1. Three trocars were inserted in the precordial regionwithout any incision in the anterior cervical region. Carbondioxide was insufflated to 5mmHg to create a space aroundthe strap muscles
Table 1. Clinical details of the 12 patients
Patient Sex/ Thyroid gland Excised thyroid Estimated residualno. age (years) size (cm) weight (g) thyroid weight (g) Operation time (min) Blood loss (ml)
1 F/29 8.0 3 7.0 70.0 2.5 420 2052 M/16 8.0 3 8.0 87.0 2.5 340 743 M31 12.0 3 8.0 92.0 2.0 380 3434 F/52 5.5 3 5.2 30.0 2.0 195 595 F/31 6.0 3 5.5 42.0 2.0 175 456 F/15 6.7 3 6.0 45.7 2.0 240 847 F/20 4.8 3 4.5 17.5 2.5 180 58 F/23 5.0 3 4.5 21.7 2.5 215 109 M/18 6.8 3 4.9 36.1 3.0 245 171
10 M/59 5.3 3 4.3 17.8 4.0 250 1211 F/17 6.1 3 5.8 27.3 3.5 225 3812 F/21 6.1 3 5.8 42.6 4.0 252 36

3M. Yamamoto et al.: Endoscopic Thyroidectomy for Graves’ Disease
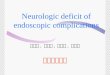
nerve paralysis and hypoparathyroidism developed inone patient. All of the patients were discharged on theseventh postoperative day. The postoperative scarringwas completely hidden by clothing, leaving the patientssatisfied with the cosmetic results (Fig. 3).
Discussion
A number of recent reports have discussed thefeasibility of endoscopic thyroidectomy,1–6 includingIshii et al. who proposed a technique of performingendoscopic thyroidectomy via a precordial approach.Their technique provides excellent cosmetic resultsbecause it leaves no postoperative scarring of the neck,which is difficult to conceal.1 They successfully applied
this endoscopic technique for thyroid adenoma resec-tion without any complications.
Although surgery for Graves’ disease has becomesafer as a result of improvements in preoperativemanagement and surgical techniques, the risk of thyroidbleeding remains. We previously described performingendoscopic thyroidectomy via a precordial approachin a patient with Graves’ disease.2 In this technique,ultrasonic coagulation devices are used, enabling fullseparation as well as easy cutting, in comparison withconventional thyroid surgery. When the thyroid gland isfreed or resected, we operate in close proximity to thethyroid capsule, whereby the recurrent laryngeal nerveand parathyroid gland are inevitably preserved. There-fore, the recurrent laryngeal nerve and parathyroidgland are not necessarily visualized in the operativefield, although when the residual thyroid gland is small,being less than 1.0g, on each side after subtotal thyroi-dectomy, the recurrent laryngeal nerve and parathyroidgland can often be seen. A highly magnified operativefield under endoscopy allows preservation of the recur-rent laryngeal nerve and parathyroid gland; however, inone of our patients, hypoparathyroidism and recurrentnerve paralysis developed, which was likely to havebeen related to thermal stimulation caused by theultrasonic coagulation device. Consequently, this sys-tem should not be used close to Berry’s ligament.
When the goiter is large, controlling the bleedingbecomes difficult, particularly around the superiorthyroid arterial branch, which can prolong the operativetime. Conversely, when the goiter is small, bleeding canbe controlled easily and the surgical procedure becomessimplified. In fact, in one of our patients with 104g ofexcised thyroid gland, coversion to conventional opensurgery was required. Thus, this technique should only
Fig. 2. a The right recurrent laryngeal nerve (arrow) was visualized and preserved (endoscopic view). b The right inferiorparathyroid gland (arrow) was visualized and preserved (endoscopic view)
Fig. 3. Operative scars after 1 years. This technique leavesabsolutely no surgical scarring of the neck
a b

4 M. Yamamoto et al.: Endoscopic Thyroidectomy for Graves’ Disease
be indicated for patients with Graves’ disease having acomparatively small goiter, weighing less than 100g bypreoperative diagnosis, as it provides a better operativefield of vision. For measuring residual thyroid volume,we used the modified sponge thyroid model and com-pared it with the residual tissue.2
In conclusion, endoscopic subtotal thyroidectomyperformed via a precordial approach appears to be auseful surgical technique for Graves’ disease when thegoiter is comparatively small. This approach is feasible,cosmetically appealing, and should be indicated foryoung women in particular.
References
1. Ishii S, Ohgami M, Arisawa Y, Omori T, Noga K, KitajimaM (1998) Endoscopic thyroidectomy with anterior chest wallapproach. Surg Endosc 12:611
2. Yamamoto M, Sasaki A, Asahi H, Shimada Y, Sato N, NakajimaJ, Saito K (1999) Endoscopic subtotal thyroidectomy for Graves’disease (in Japanese with English abstract). Naibunpitsugeka(Endocr Surg) 16:117–121
3. Takami H, Ikeda Y, Sasaki Y, Niimi M (1999) Endoscopic thyroi-dectomy with axillary approach (in Japanese). Naibunpitsugeka(Endocr Surg) 16:243–245
4. Shimizu K, Akira S, Jasmi AY, Kitamura Y, Kitagawa W, AkasuH, Tanaka S (1999) Video-assisted neck surgery: endoscopicresection of thyroid tumor with a very minimal neck wound. J AmColl Surg 188:697–703
5. Hüscher CSG, Chiodini S, Napolitano C, Recher A (1997)Endoscopic right thyroid lobectomy. Surg Endosc 11:877
6. Yeung HC, Ng WT, Kong CK (1997) Endoscopic thyroid andparathyroid surgery. Surg Endosc 11:1135