-
Trastorno hemorrgico del RN, por deficiencia de vitamina k
-
Se afecta produccin neonatal de vit KIngesta inadecuada de LMNO
vit K al nacer
-
VOLUMEN DE INTERCAMBIO =Volumen circulante= peso (kg) x volemia
(80 ml/kg)Catter venoso umbilical alto o bajoCatter arterial
umbilical bajoCatter intravenoso perifricoPlasmanateAlbumina al
5%Solucin fisiolgicaPFC
-
COMPLICACIONES
-
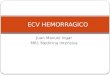
Etapa de HiperplasiaEtapa de HipertrofiaEtapa de Hiperplasia e
Hipertrofia0202840SemanasRCIU simtricoRCIU asimtricoRCIU
intermedioPrenatal diagnosis of deviant fetal growth, 1992Fases del
Crecimiento fetal
-
Es la detencin del crecimiento y desarrollo que origina
hipoplasia o hipotrofia embriofetal, en forma precoz o tarda,
provocado por factores intrnsecos o extrnsecos, generando recin
nacidos con alteraciones en el peso, la talla y permetro cefalico,
que puede conducir a trastornos hipxicos prenatales o neonatales; y
a otros signos postnatales como hipoglucemias, poliglobulias, etc.;
o pudiendo presentar dficit a largo plazo en el plano intelectual y
del aprendizaje.
-
El restriccin del crecimiento intrauterino (RCIU) ocurre cuando
un feto presenta un peso aproximado por debajo del P10 para su EG.
El mismo se haya afectado por una restriccin patolgica en su
capacidad de crecimiento.
Bajo peso al nacer (LBW) significa un nio con un peso al
nacimiento menor de 2500 gr., lo cual puede ser debido a RCIU o a
Prematuridad.
-
RCIU Vs PEGRCIU
CRECIMIENTO ALTERADODISMINUCION DE GRASA SUBCUTANEATAMAO PEQUEO
GENERALMENTE
ESTADO METABLICO ANORMALINDICE PONDERAL BAJOPERIODO POSNATAL
COMPLICADOPEG
CRECIMIENTO NO SIEMPRE ALTERADOGRASA SUBCUTANEA NORMALSIEMPRE ES
PEQUEO
ESTADO METABLICO PUEDE SER NORMAL
INDICE PONDERAL NORMAL PERIODO POSNATAL NORMAL
-
RESTRICCION DEL CRECIMIENTO INTRAUTERINO
La ms aceptada considera el percentil 10 de la curva de peso de
nacimiento-edad gestacional.El ndice ponderal menor a 2 DS. Otros
pases utilizan el percentil 25-5.Recomendacin de la OMS es que la
curva patrn que cada centro perinatal utilice sea reciente y
representativa de su propia poblacin.
-
Incidencia del RCIUEntre el 1 al 20% dependiendo de la definicin
adoptada.50 % se encuentra el diagnstico despus del nacimiento.50%
de los fetos con sospecha de RCIU nacen con pesos normales.Presenta
10% de mortalidad perinatal.50 -80% de los bajos pesos NO son
RCIU.
-
RCIU
RN Normal y con RCIU
Placenta Normal y RCIUJJC
-
Clasificacin RCIU I RCIU II RCIU III
-
- RCIU I - Intrnseco Armnico Simtrico Eutrfico Hipoplsico Precoz
Alteracin Peso, Talla, Permetro Craneal
Frecuencia: 15% al 20%
-
RESTRICCION DEL CRECIMIENTO INTRAUTERINOCLASIFICACION: TIPO
1Causas: intrnseco (gentico) extrnseco (infeccin intrauterina,
drogas, teratgenos)Comienzo temprano: I trimestreN menor de cel.de
tamao normal: HipoplasiaPlacenta normal.Ecografa. Biometra armnica
disminuida.Doppler: Umbilical y ACM S/D aumentado.Crecimiento
Postnatal: Pobre
-
Etiopatogenia: RCIU ICromosomopatas:Tr18-21-Turner-
MosaicismosTeratgenos drogas tabaquismo alcohol.Infecciones: TORCH
Gemelaridad
-
CARACTERSTICAS CLNICASNoxa precoz: afecta el Ncelular e influye
sobre la talla y peso fetales.
Hipoxia crnica.
Desarrollo infantil: perfil bajo
-
Curva de RCIU I
-
- RCIU II -Extrnseco Disarmnico Asimtrico Distrfico Hipotrfico
Tardo Alteracin Peso
Frecuencia: 75% al 85%
- RESTRICCION DEL CRECIMIENTO INTRAUTERINO CLASIFICACION: TIPO
2Causas: Extrnsecas insuficiencia placent.Frecuencia: 80%Comienzo
Tardio: III trimestreN de celulas normal,Tamao menor:
HipotroficoOrganos afectados: Cerebro/Higado R
-
Etiopatogenia RCIU IIAfecciones maternas Endocrinopatas Toxemia
HTA Nefropatas S. Antifosfolipdico
Afecciones placentarias vasculitis Corioangiosis Hipoplasia
placentaria Distopias PlacentariasFACTORES QUE ALTERAN LA
TRANSFERENCIA DE O2 AL FETOMATERNOS
-
CARACTERSTICAS CLNICASNoxa tarda:Afecta el tamao celular e
influye sobre el peso fetal pero no en la talla.
Hipoxia subaguda.
El recin nacido iguala a la media normal en su desarrollo
infantil.
-
Semanas de embarazoCurva del RCIU II
-
RCIU Cuadro comparativo
Tipo I:Simtrico Tipo II:AsimtricoCausas Intrnseco / Extrnseco
ExtrnsecoFrecuencia 20% 80%Comienzo Precoz < 28 sem 3 trimestre
>28 semrganos Afectados
Cerebro/Hgado:NormalCerebro/Hgado:6/1-VN:3/1CaractersticasCelulares
Hipoplasia Tamao normal Hipotrofia N normalCrecimientoPlacentario
Normal DisminudoAnomalas fetales Frecuentes y mltiples
InfrecuentesDBP Pequeo NormalPA Pequeo Pequeo
-
- RCIU III o mixto -Extrnseco Carencial Semiarmnica Hipotrfico
Mal Nutrido Semiprecoz Alteracin Peso y TallaFrecuencia: 5% ?
-
Etiopatogenia CIR III -?-Factores culturales Malnutricin: Se lo
atribuye a hiponutricin materna quepersiste durante todo el
embarazo.
Tabaquismo drogas alcohol
-
CARACTERSTICAS CLNICASCaractersticas ambiguas con predominio de
TIPO I o II
Variable segn el momento y tiempo del impacto de la desnutricin
materna.
-
RCIU*Mecanismos de defensa fetalRedistribucin de flujo hacia los
sitios de mayor importancia Cerebro Corazn SuprarrenalesQuedan con
menor irrigacin Rin Hgado Celular subcutaneoTodo esto provoca
asimetra en el crecimiento clasificarlos en Simtricos o
Asimetricos
RCIU
-
Mecanismos de defensa fetal
-
RCIU: DIAGNOSTICO Clnicos. Ecografa convencional. Ecografa
Doppler.JJC
-
DiagnsticoDe Sospecha (Clnico)
De Presuncin (Ecogrfico)
De Certeza (Neonatolgico)JJC
-
ClnicoHistoria Clnica y Obsttrica. Altura uterina Perimetro
abdominal Curva ponderal maternaEstado nutricional.
JJC
-
Relacin Altura UterinaJJC
-
Ecobiometra Curva de Crecimiento EcogrficoMedicin DBPMedicin
HCMedicin ACMedicin L. Fmur Medicin L. HmeroPeso Fetal ndice
Ponderal = peso (g) / talla (cm) x 100 JJC
-
Diagnstico Bajo ndice ponderal (Wt./Fl).Disminucin del tejido
celular subcutaneo.Presencia / aparicin de - Hipoglucemia,
Hiperbilirrubinemia, Enterocolitis necrotizante, Sindrome de
hiperviscosidad. Neonatal JJC
-
Vigilancia Una vez realizado el diagnstico y comenzado el
tratamiento, el feto debe estar bajo vigilancia.Hay cuatro formas
tiles de vigilancia: -Non-Stress Test, Perfil biofsico, Volumen de
LA, y Doppler de arteria umbilical, cada uno de los cuales valora
distintos aspectos de la salud fetal. La combinacin de los mismos
es mejor que uno aislado. El objetivo es identificar un progreso de
la enfermedad que hiciera peligrar al feto, al punto en que sea
mejor el parto, a que permanezca en tero. JJC
-
Tratamiento:RCIUEl RCIU tiene muchas causas; por lo tanto no hay
un tratamiento nico que siempre funcione. Qu tratamiento es el
adecuado ?JJC
-
TratamientoRIESGO DE PREMATUREZEXISTENCIA EXTRA UTERINA
DIFICIL
RIESGO DE MUERTE INTRAUTERINAAMBIENTE INTRA UTERINO
HOSTILDecidir el momento ptimo para el partoJJC
-
Morbilidad Neonatal
Asfixia perinatal
Alteraciones de la termoregulacin
Hipoglucemia
Policitemia e hiperviscosidad
JJC
-
Morbilidad Neonatal
Encefalopata hipxico-isqumicaSndrome de aspiracin
meconialPersistencia de la circulacin fetalEnterocolitis
necrotizanteIRAEstigmas de anomalas cromosmicasHipocalcemia
JJC
-
*Description There are standards or averages in weight for
unborn babies according to their age in weeks. When the baby's
weight is at or below the 10th percentile for his or her age, it is
called intrauterine growth retardation or fetal growth restriction.
These babies are smaller than they should be for their age. How
much a baby weighs at birth depends not only on how many weeks old
it is, but the rate at which it has grown. This growth process is
complex and delicate. There are three phases associated with the
development of the baby. During the first phase, cells multiply in
the baby's organs. This occurs from the beginning of development
through the early part of the fourth month. During the second
phase, cells continue to multiply and the organs grow. In the third
phase (after 32 weeks of development), growth occurs quickly and
the baby may gain as much as 7 ounces per week. If the delicate
process of development and weight gain is disturbed or interrupted,
the baby can suffer from restricted growth.RCIU*MUCHOS CUESTIONA
QUE EL PESO AL NACIMIENTO SEA UN BUEN INDICADOR DEL FETO CON RCIU.
El ndice ponderal definido como el PESO\TALLA identifica fetos con
masa de tejidos blandos por debajo del desarrollo esqueletico.
Fetos con ndice ponderal menor del dcimo percentil sugiere RCIU.EL
ULTIMO PARMETRO EN ALTERARSE SI ES QUE LLEGA A SUCEDER ES EL
PERIMETRO CEFALICO.Es importante recordar que el diagnostico de
RCIU es por estudios seriados.
*RCIU*RCIU*Este tipo de RCIU presenta el fenmeno de "Proteccin
cerebral" (brain sparing) mediante el cual hay una derivacin
selectiva de la circulacin hacia los tejidos mas sensibles a la
hipoxia (cerebro), sacrificndose la irrigacin esplcnica. Esto se
atribuye a la accin de la sustancia arginina-vasopresina y explica
la importante disminucin en el permetro abdominal que demuestran
estos productos.
*IUGR can be difficult to diagnose and in many cases doctors are
not able to make an exact diagnosis until the baby is born. A
mother who has had a growth restricted baby is at risk of having
another during a later pregnancy. Such mothers are closely
monitored during pregnancy. The length in weeks of the pregnancy
must be carefully determined so that the doctor will know if
development and weight gain are appropriate. Checking the mother's
weight and abdomen measurements can help diagnose cases when there
are no other risk factors present. Measuring the girth of the
abdomen is often used as a tool for diagnosing IUGR. During
pregnancy, the healthcare provider will use a tape measure to
record the height of the upper portion of the uterus (the uterine
fundal height). As the pregnancy continues and the baby grows, the
uterus stretches upward in the direction of the mother's head.
Between 18 and 30 weeks of gestation, the uterine fundal height (in
cm.) equals the weeks of gestation. If the uterine fundal height is
more than 2-3 cm below normal, then IUGR is suspected. Ultrasound
is used to evaluate the growth of the baby. Usually, IUGR is
diagnosed after week 32 of pregnancy. This is during the phase of
rapid growth when the baby should be gaining more weight. IUGR
caused by genetic factors or infection may sometimes be detected
earlier. *Systematic reviews provide strong evidence of benefit
only for the following interventions: balanced protein/energy
supplementation, strategies to reduce maternal smoking, and
antimalarial prophylaxis. In Jamaica, antibiotic administration to
prevent urinary tract infections further reduced an already low
prevalence of IUGR. Improvement of maternal nutrition should be a
priority, especially in developing countries. Unless maternal
undernutrition is severe, the effect of balanced protein/energy
supplementation on birth weight is likely to be modest 100 g).
Reduction in maternal smoking should be encouraged, both by
individual clinicians (using behavioral modification techniques,
for example) and by policy makers (e.g., taxes on cigarettes and
other tobacco products). Antimalarial chemoprophylaxis should be
provided in endemic areas, particularly to primigravidae, although
more research is needed to elucidate the ideal timing of treatment,
combination of agents, and safety for the fetus.*A systematic
review of 126 available randomized controlled trials (RCTs) has
been carried out to summarize the efficacy of 36 prenatal
interventions aimed at reducing IUGR. Strategies include prenatal
care modalities, protein/energy supplementation, treatment of
anemia, vitamin/mineral supplementation, fish oil supplementation,
and prevention and treatment of hypertensive disorders, fetal
compromise, and infection. Based on this review, few statistically
significant reductions in the risk of IUGR have been demonstrated
with these interventions. However, the point estimate (average
effect) associated with some interventions suggests a potential
effect of considerable magnitude; these interventions should be
further evaluated by targeting populations at risk for IUGR,
increasing sample size, and addressing coexisting factors limiting
growth. Studies should be conducted in developed as well as
developing countries.
*