Embed Size (px)
Citation preview

대한내과학회지 : 제 59 권 제 5 호 2000
서 론
비스테로이드성 항염제(이하 NSAIDs : Nonsteroidal
anti- inflammatory drugs)는 류마티스 질환 환자에서의
통증 경감에 가장 기본이 되는 약물이다. 단일 약제로
미국에서 연간 20억 달러 이상의 매출을 기록할 정도로
현재 전 세계에서 가장 많이 팔리는 약물로 모든 종류의
류마티스 질환뿐만 아니라 두통, 월경곤란증(dysmenor-
rhea), 운동손상(sports injuries) 등에도 광범위하게 사
용하고 있다.
지금까지 사용 가능한 NSAIDs의 종류는 매년 새로
개발되어 왔으며 그 약물작용 기전이나 부작용 면에는
약간의 차이가 있다. 그러나 어느 제품이 다른 제품에
비해 더 우수하다고 할 수는 없는 것은 개인에 따라 그
효과와 부작용이 다양하게 나타나기 때문이다. 어쨌든
NSAIDs에 의한 부작용은 이 약제의 사용에 가장 큰 걸
림돌이 되고 있으며 현재 이러한 문제점의 해결에 큰 관
심이 모아지고 있다.
NSAIDs의 작용기전
1. Cyclooxygenase 억제
류마티스 질환에서 보여지는 염증반응은 매우 복잡하
고, 이 중 프로스타글란딘(prostaglandin, 이하 PG)이 매
우 중요한 역할을 담당한다는 것은 잘 알려진 사실이다.
NSAIDs의 주요 작용기전은 cyclooxygenase(이하 COX)
를 억제하여 arachidonic acid로부터 PG의 합성을 차단
함으로써 발열, 부종, 홍반, 백혈구에 대한 화학주성
(chemotaxis), 혈관 투과성 등을 낮춰 항 염증 효과를 발
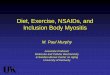
휘하게 되는 것이다1)(Figure 1). 대표적인 약물로 100여
년 전에 알려진 아스피린(acetylated salicylic acid)은
COX를 비가역적으로 억제하는 반면 다른 NSAIDs는
가역적으로 억제한다는 차이가 있다.
최근 COX 효소는 내재적 형태(COX- 1)와 염증성 자
극에 의해 유도되는 형태(COX- 2)의 2가지 동종효소
(isoenzyme)로 존재함이 밝혀졌는데, 전자는 내재적
(constitutively)으로 발현되어 생리적 기능 즉, 위점막의
산 분비를 억제하고, 점액 분비를 촉진하며 위·식도 괄
약근의 긴장을 유지하고 신혈관을 확장하여 체액 감소
시 신혈류량을 유지하는 등의 기능을 수행하는 PG 합성
에 작용하는 것이고, 후자는 언급한대로 염증성 자극에
의해 유도되어 염증을 유발하는 PG 합성에 작용하는 것
이다2, 3)(T able 1). 따라서 NSAIDs와 관련된 부작용은
주로 COX- 1의 억제로 인해 발생되며 항염 효과는
COX- 2의 억제에 기인하리라 생각된다4, 5). 기존에 알려
진 NSAIDs는 대부분 COX- 1과 COX- 2 모두를 억제하
는 반면 최근 연구가 활발히 진행 중인 rofecoxib나
celecoxib 등과 같은 COX- 2 만을 선택적으로 억제할 수
있는 약물은 신독성이나 위장관 부작용을 감소시키는
점에 있어 기존의 NSAIDs에 비해 뛰어난 장점이 있다
고 할 수 있다.
그 외 Nonacetylated salicylates 제제로, salsalate,
choline magnesium trisalicylate 등이 있는데 COX에 대
한 억제 작용은 미약하지만 nonsalicylate NSAIDs 와
임상효과 면에서는 동등하다. NSAIDs의 다른 작용기전
으로 nonprostaglandin- mediated mechanisms of action
이 있는데 이는 L- selectin 감소로 염증부위로의 중성구
이동을 억제하고, Nitric oxide synthase(이하 NOS)의
전사를 막아 염증반응을 억제하는 것이다.
NSAIDs의 효과
1. 항염효과(anti-inflammatory effect)
개인적인 반응의 다양성이 심하므로 현재까지 아스피
린을 비롯한 모든 NSAIDs들의 효과적인 면에서 어느
한 약물이 가장 우수하다고 알려진 것은 없다. 통풍이나
종 설
비스테로이드성 항염제(NS AIDs ) 치료의 최근 경향
가톨릭대학교 의과대학 류마티스내과
박종서·김호연
- 491 -

-Korean Journal of Medicine : Vol. 59, No. 5, 2000 -
척추관절염에서는 경험적으로 indomethacin이 아스피린
이나 다른 NSAIDs보다 선호되는 추세이나 역시 과학적
으로 확실한 근거가 있지는 않다. 다만 부작용 면에서
아스피린 보다 그 이후 개발된 NSAIDs 들이 좀 더 우수
하다는 결과가 있다. 류마티스 관절염에서 항염효과
(T able 2)가 잘 알려져 있고, 임상적으로 관절의 통증,
부종, 뻣뻣함을 감소시킨다. 류마티스 관절염에서 사용
할 때 급성기 반응물질(acute phase reactants) 이나 류
마티스 인자의 역가를 호전시킨다는 제한적인 보고가
있으나 일반적으로는 염증의 지표들의 호전을 가져오지
않는다고 알려져 있다. 그 외에도 널리 쓰이는 경우는
각종의 관절염에서 사용되며 급성 통풍이나 인대염
(tendinitis), 점액낭염(bursitis)에서도 흔히 사용된다. 비
염증성 관절염인 골관절염에서도 NSAIDs가 종종 사용
되는데 임상적인 효과가 항염효과인지 진통효과인지는
불분명하다.
T able 1. Synthes is , function and inhibition of COX1 and COX2
COX- 1 COX- 2Enzymesynthesis
ConstitutiveOnly after induction(IL- 1,TNFα, lipopolysaccharide)
Function Physiologicprotection of the stomach,regulation of platelet aggregation,peripheral vascular res is tance,renal blood flow distribution,sodium excretion
ProinflammatoryPGE2, PGI2 and T XA2 infibroblas ts and macrophages ,and other cells
Inhibitionby NSAIDs
COX- 1 < - - - - - Relative effect favors - - - - - > COX- 2Indomethacin
AspirinPiroxicam
IbuprofenDiclofenac
MeloxicamCelecoxibRofecoxib
Figure 1. Cyclooxygenase/prostaglandin pathway.
T able 2. Proces s es influenced by NSAIDS
Prostaglandin synthes isLeukotriene synthes isSuperox ide radical productionSuperox ide scaveng ingLysosomal enzyme releaseCell membrane activites
EnzymesNADPH oxidasePhospholipaseT ransmembrane anion transportUptake of pros tag landin precurs or
Neutrophil aggregation and adhesionLymphocy te functionRheumatoid factor productionCytokine productionCartilage metabolis mSynthes is of nitric ox ide
- 492 -

- Jong- Seo Park, et al : Current trend of NSAID use -
2. 진통 효과(analgesic effect)
모든 NSAIDs들이 지니는 효과로서 소염효과보다 훨
씬 낮은 용량으로도 진통의 효과가 있다. 중추 신경계를
통해 진통효과를 발휘하는 마약종류와는 달리 NSAIDs
의 진통효과는 말초 신경을 통한 효과로 생각된다. 사용
의 목적이 순수하게 진통의 목적이라면 소염효과를 원
하는 용량의 반 정도면 그 효과를 달성할 수 있지만 우
선은 NSAIDs가 아니고, 부적용이 적은 acetaminophen
같은 약을 먼저 시도하는 것이 바람직하다.
3. 해열 효과(antipyretic effect)
각종 원인의 발열을 완화하는데 효과적이다. 역시 어
느 한 약물이 해열에 가장 우수하다는 증거는 없다.
4. 혈소판 기능억제
NSAIDs는 혈소판의 COX를 억제하여 adenosine di-
phosphate, collagen, epinephrine에 의해 유도되는 혈소
판 응집(platelet aggregation)작용을 억제한다. 아스피린
은 COX를 비가역적으로 아세틸화하여 억제하는 반면
다른 NSAIDs는 가역적으로 억제한다는 차이가 있다.
따라서 출혈성 경향이 있거나 수술예정인 환자에게는
nonacetylated salicylate(diflunisal, salsalate, sodium
salicylate)가 적절한 처방이며, 수술 전에 아스피린은 약
1주전에 중단해야하나 다른 NSAIDs는 반감기에 따라
다소 차이는 있으나 2- 3일전에 중단해도 된다. 혈소판의
COX 생산은 다른 조직에 비해 다량이기 때문에 아스피
린 저용량으로도 항 혈소판 응집 효과를 발휘하며 뇌심
혈관계의 혈전예방에 사용된다.
5. 기타
류마티스 관절염, 골관절염 외에도 강직성 척추염,
인대염, 점액낭염, 통풍, 발열, 두통 등이 적응증 들이며
치주염, 가족성 대장용종(familial polyposis)도 NSAIDs
사용의 적응증이다. NSAIDs는 자궁근 수축을 억제하는
효과가 있기 때문에 월경곤란증(dysmenorrhea)에서도
널리 쓰인다. Indomethacin의 경우 신생아의 동맥관 개
존증(patent ductus arteriosus)의 치료에도 쓰인다. 최근
에는 Alzheimer' s disease 예방에도 효능이 있을 가능성
이 제시되었다.
NSAIDs의 부작용(Table 3)
1. 위장관 부작용6)
소화불량의 증상부터 위장 미란, 소화성 궤양, 천공,
출혈 등이 있으며 환자가 실제 자각증상이 없이도 위장관
병변이 발생하고 위장관의 자각 증상이 있더라도 실제 병
변이 없는 경우도 많으므로 증상만으로 위궤양 등의 합병
증의 여부를 판단하는 것은 매우 불확실하다. 미국의 통계
를 보면 NSAIDs의 위장관 부작용으로 인해 년간 7만 건
의 입원과 7천 명의 사망이 발생하리라 추정되고 있다.
T able 3. Advers e reactions to NSAIDs
Gas trointes tinal
Hepatic
Renal
Hematologic
Cutaneous
Respiratory
Central nervoussystem
Indiges tionGastroesophageal refluxEros ionsPeptic ulcerGastrointestinal hemorrhage and perforation
Small and large bowel ulcerationT ransaminase elevationHepatocellularCholes tas is
T ransient r is e in serum creatinineHyponatremiaAcute renal failureInterstit ial nephritisHyperkalemiaAnalges ic nephropathy
T hrombocytopeniaNeutropeniaRed cell apas iaHemolytic anemia
PhotosensitivityErythema multiformeUrticariaT oxic epidermal necrolys is
BronchospasmPneumonitis
HeadacheDizzinessPersonality chamgeAseptic meningitis
- 493 -

-대한내과학회지 : 제 59 권 제 5 호 통권 제 483 호 2000 -
NSAIDs로 장기간 치료받는 환자의 약 2%에서 만성 궤양
이 발생하며 심각한 위장질환의 발생 위험도도 NSAIDs
를 사용하지 않는 대상에 비해 약 3배 높다. 평상의 대변
잠혈반응 검사는 위장관 합병증을 발견하는데 민감하지
못하여 효과적이지 않다. 따라서 예방이 가장 중요한 수단
이라 하겠다. 예방을 위해서는 단순한 진통의 목적이라면
NSAIDs가 아닌 다른 진통제를 사용한다.
가능하면 최소한의 용량을 사용하며 십이지장궤양이
발생하기 쉬운 위험인자(T able 4)를 가진 경우, 반드시
NSAIDs를 투여해야 한다면, 위장관 합병증을 예방하기
위한 추가적인 처방이 필요하다(T able 5).
NSAIDs의 작용기전의 하나인 PG생성의 억제가 위
장관 부작용 발생에 기여한다고 생각되어 이러한 부작
용의 예방 목적으로 PG 유도체인 misoprostol을 투여하
면 위, 십이지장궤양의 발생을 감소시킨다고 알려져 있
다. 제산제나 ranitidine, cimetidine 제제는 위궤양의 예
방에는 효과적이나 십이지장궤양에는 효과가 없음이 알
려져 있다. NSAIDs에 의한 위장궤양은 보통의 위장 궤
양치료와 동일하며 가능한 한 NSADs의 투여는 중지하
는 것이 바람직 하지만 꼭 사용해야 하는 경우에 위장
궤양 치료와 함께 NSAIDs 투여시 위장관 궤양의 치유를
지연시킨다. 최근에는 omeprazole 이나 famotidine 제제가
NSAIDs와 함께 투여시 위, 십이지장 궤양의 합병증을 예
방해준다는 사실이 알려져 PG 유도체를 복용하지 못하는
경우에 쓸 수 있는 또 다른 방법이다. Helicobactor pylori
에 감염되었을 경우 NSAIDs의 위장궤양의 발생 위험도
를 증가시키지는 않는다고 최근 보고된 바 있다7).
2. 신장계 부작용
신장 질환이 있거나 체액량이 감소 상태, 이뇨제를 복
용중이거나, 간장 질환이 있는 경우에는 위험도가 높으
므로 주의를 요한다. 고혈압 환자에게 투여 시는 기존의
혈압강하제로 혈압이 잘 조절되었다가도 혈압이 상승하
는 경우도 있으므로 전보다 자주 혈압을 측정해 보아야
한다. Metaanalysis에 의하면 평균적으로 이완기 혈압을
5 mmHg 가량 상승시킨다8).
3. 간장 부작용
일시적으로 간 수치의 상승을 유발하지만 대개 투약
을 계속하더라도 정상화되며 심한 간염이 발생하는 경
우는 매우 드물다.
4. 기타
기타 흔한 부작용으로 발진이 발생하는 경우가 있으
나 대개 투약을 중단하면 저절로 소실되고 전신성 홍반
성 루푸스 환자에서 ibuprofen 사용으로 무균성 뇌막염
증상이 발생하는 예가 보고되었다. 비강폴립, 천식, 만성
담마진이 있는 환자는 급성 천식이나 호흡곤란으로 나
타나는 과민성 반응을 보일 위험성이 증가한다.
Cyclooxygenase-2 inhibitor
지난 100년 동안 아스피린은 진통제, 소염제 및 항혈
T able 5. Prophylaxis algorithm for NSAIDs g as trotoxicity
Identify the high risk patientUse the low est poss ible dose of NSAIDs or use non- NSAID analges ic or nonacety lated salicylateT reat “high- risk” patient w ith misoprostol, if concomitat NSAIDs are necessaryIf mis oprostol s ide effects are intolerable, use his tamine- 2 blockers or omeprazolIf patients are not in "high- risk" group, do not treat w ith misoprostol, his tamine- 2 blockers , or omeprazole
prophylactically
T able 4. Ris k for NSAIDs - induced gas troduodenalulcer dis eas e
Elderly people(> 60 years old)History of peptic ulcer disease, with or without NSAIDsHigher dosage of NSAIDsPrevious use of antacids, H2- blockers, or omeprazole for GI
symptoms, with or without NSAIDsHistory of abdominal pain of unclear etiology, with or
without NSAIDsExtent of inflammatory disease for which NSAIDs are
prescribedConcomitant corticosteroid useControversialTobacco useAlcohol use
- 494 -

-박종서 외 1인 : 비스테로이드성 항염제(NSAIDs) 치료의 최근 경향-
전제로서 그 가치가 인정되어 왔다. 그러나 위장장애 문
제를 극복 할 수 있는 보다 안전한 아스피린, 혹은 소염
진통제의 개발이 필요하게 되었고 최근까지 이에 대한
연구와 노력이 꾸준히 이어져 왔다. 과거 COX는 조직
내에서 일정하게 지속적으로 표현되는 것으로 믿고 있
었고 염증이 발생하면 PG 합성이 그 전구 물질에 의해
증가되는 것으로 알고 있었다. 아울러 아스피린이나 여
러 소염 진통제의 COX 효소를 통한 PG 합성 억제가 치
료효과나 부작용 유발의 핵심 이론으로 정립되었다.
1990년 Needleman 연구진이 처음으로 IL- 1 에 의해
자극을 받은 단핵구에서 두 가지의 다른 COX 단백질을
관찰하였다9). 이 두 물질 즉 COX- 1 과 COX- 2 효소는
구조적으로 매우 유사한 머리핀 모양의 길고 좁은 채널
로 되어있다10). COX- 1 효소는 위점막 보호기능이나 신
기능 보전의 역할을 책임지는 "housekeeping" 기능인
PG의 형성을 주로 담당하고 있다. COX- 2 효소는 휴지
기의 세포에서는 거의 발견되지 않는다. 그러나 조직에
염증 반응이 있는 부위에서는 뚜렷이 표현되어 PG 형성
을 증가시키는 "inducible enzyme" 이다5). 이 두 효소는
60% 가량 아미노산 구조가 동일하다. 손상 받은 세포막
에서 유리되는 arachidonic acid가 COX 효소의 길고 좁
은 채널을 통과하면서 산소기를 받아들이고 free radical
이 유리되면서 다섯 개의 carbon ring을 가진 PG을 합
성하게 된다. 이 두 효소는 arachidonic acid에 대한 결
합 장소나 결합 능은 유사하지만 구조나 기능 면에서 중
요한 차이가 있다. 그리고 인체 COX- 2 유전자는 8.3 kb
로 COX- 1 유전자(22 kb)에 비해 작고 glucocorticoid나
IL- 6등과 같은 cytokine과 결합하여 COX- 2 유전자
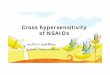
mRNA 표현이 쉽게 조절된다. Figure 2 에서와 같이
NSAIDs는 채널의 중간쯤에서 비선택적으로 결합하여
COX- 1을 억제한다. 이는 arginine 120 위치에서의
hydrogen 결합에 의한 것으로 non- selective binding
site로 생각되어 진다. Arginine 120은 COX- 2에도 존재
한다. 그러나 COX- 1과 COX- 2 효소의 구조적 차이 중
여러 약물들의 selectivity에 결정적 영향을 미치는 것은
단 한 개의 아미노산에서의 상이성 때문으로 바로 523
위치에 각기 존재하고 있는 isoleucine(COX- 1)과
valine(COX- 2)이 그것이다. Valine은 isoleucine 보다 더
입자가 작아 COX- 1 효소에는 존재하지 않는 틈새를
COX- 2 채널에 형성하게 하고 이 틈새는 여러 selective
Figure 2. Prostaglandin synthesis and inhibition by COX- 1 and COX- 212).
- 495 -

-Korean Journal of Medicine : Vol. 59, No. 5, 2000 -
한 약물들로 하여금 side- pocket에의 결합을 가능하게
하는 통로로 작용하는 것이다. 상대적으로 입자가 훨씬
큰 COX- 1의 isoleucine은 이러한 side- pocket으로의 통
로를 차단하게 되어 COX- 2에서와 같은 selectivity를 제
공할 수 없게 된다11, 12).
정상적인 상태에서는 백혈구, 거식세포, 혈관내피세
포 그리고 섬유아세포 등에서 COX 활성화가 관찰되지
않으나 LPS, cytokine이나 growth factor 등에 의한 염
증성 자극을 받게 되면 COX- 2의 작용이 증가하게 된다5).
특히 류마티스 활막 조직에서의 섬유아세포나 혈관내피
세포들은 IL- 1이나 phorbol ester의 자극에 반응하여
COX- 2에 대한 mRNA의 발현이나 PG- E2 형성이 증가
된다. 그리고 glucocorticoid나 어떤 NSAIDs 들은
COX- 2 형성을 억제 시킨다. 선택적으로 inducible
enzyme인 COX- 2를 억제시킨다는 것은 이론적으로 염
증이 있는 부위에만 PG 형성을 억제시켜, 위장관이나
신장 내 PG 형성에 관여하는 내재성 효소인 COX- 1억
제에는 작용하지 않아 부작용을 감소시킬 수 있게된다.
COX- 2 억제제의 개발은 소염진통제의 위장관 안전
성에 근거를 두고 있다. 즉 위점막 내에는 주로 COX- 1
효소에 의해 위를 보호하는 PG이 형성된다. 그 반면
COX- 2는 통증 및 부종과 같은 염증이 있는 부위에서
활성화된다5). 그리고 염증이 없더라도 COX- 2 억제제는
진통제로서 작용하기도 한다.
1. Screening for COX-1 and COX-2 selectivity
COX- 2 inhibitor는 구조적으로 sulphonyl, sulphone
혹은 sulphonamide group등이 COX- 2 side pocket과의
결합 정도에 따라 그 선택정도(selectivity)가 결정된다.
COX- 2 억제는 시간에 따라 달라 보통은 약 15- 30 분
경과 후 COX- 2 선택능이 발생하고 비가역적이다13).
COX- 1 억제는 COX- 2 억제와는 달리 즉시 발생하고
hydrogen 결합에 근거를 둔 것과 같은 경쟁적 가역반응
이다.
약제의 COX- 2 선택능에 대한 검사에는 여러 가지가
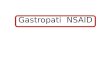
있다14). 그 중 whole blood assay가 널리 이용되고 있고
이는 혈액응고 중 혈소판으로부터 thromboxane 합성을
COX- 1 활성능으로, lipopolysaccharide에 의한 전혈내 세
포(대부분 monocyte)로부터 PGE2 합성을 COX- 2 활성능
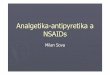
의 지표로 이용하는 것으로서, Figure 3과 Figure 4 에서
볼 수 있듯이, 전혈(whole blood)내 lipopolysaccharide로
유도되어 생산된 PGE2는 사람에서 rofecoxib의 COX- 2
에 대한 selectivity 을 반영하고, 반면 혈액응고 중 전혈
내 thromboxane B2는 혈소판에 대한 COX- 1의 활성을
Figure 3. COX- 2: Lipopolysaccharide- s timulated prostaglandin E2(PGE2) in whole blood.
- 496 -

- Jong- Seo Park, et al : Current trend of NSAID use -
반영하고 있다. 이 assay의 결과, rofecoxib가 COX- 2에
는 강력한 억제제로 작용하나 COX- 1에는 영향을 미치
지 않고 있음을 알 수 있다15).
기타 유전자 재조합 효소나 transfected cell을 이용한
방법들도 단백질의 결합이나 세포벽의 분포 등의 차이
에 따라 다른 결과를 보이고 있어 COX- 2 선택정도를
정확하게 평가할 수 있는 방법은 없지만, human gastric
PG의 억제가 일어나지 않는 정도를 COX- 2 선택정도의
척도로 삼는 것이 가장 표준이라고 인정하고 있다. COX
selectivity는 COX- 1 IC50에 대한 COX- 2 IC50 의 비로
나타내고 있다14)(T able 6). 어떤 약제의 COX selectivity
비가 0.01이면 편의상 COX- 2에 대한 selectivity가 100
배라고 표현한다. 현재 시중에 나와 있는 거의 모든 소
염진통제들은 주로 COX- 1 선택적이다.
Diclofenac은 COX- 1과 COX- 2 에 거의 대등하게 작
용한다.
2. COX-2 preferential inhibitors
기존의 NSAIDs 는 대부분 COX- 1 selectivity가 더
우세한 것들이었으나 그중 두 가지는 어느 정도 COX- 2
selectivity를 갖고 있다. Meloxicam은 piroxicam과 관
련된 enolcarboxamide로16) 여러 연구 결과 약 3- 77배의
COX- 2 selectivity를 갖고 있으며14, 16-18), 이러한 limited
selectivity 때문에 meloxicam은 preferential COX- 2
inhibitor로 불리게 되었다. Meloxicam은 구조적으로 다
른 COX- 2 inhibitors와 상이하며 COX- 2 side- pocket에
결합하기 보다는 COX- 2 channel에서의 다양한 flexibi-
lity를 이용하여 작용한다19). Meloxicam은 약 5- 6 시간
(tmax)에 흡수되고 반감기는 약 20시간으로 하루 한번 투
약이 가능하며 efficacy dose- range는 7.5- 22.5 mg/day
로 알려져 있다16, 20-24).
사람의 위점막에서 PG 형성에 관한 믿을만한 자료는
없지만 한 조사에 따르면 건강한 남성에서 meloxicam
7.5 mg 은 placebo와 비교 시 점막 손상의 정도가 더 심
하지는 않았으나, 고농도(15 mg/day)의 meloxicam을
투여했을 때에는 placebo와 비교 시 점막 손상의 정도가
증가되었고 COX- 2 selectivity 역시 예상치 보다 감소하
는 현상을 관찰할 수 있었다25). Meloxicam 7.5 mg/day
은 efficacy trials와 large- scale tolerability trials 모두
에서 만족할만한 결과를 보여 주었고, 특히 위장관 부작
용에 관해서는 diclofenac 100 mg/day 나 piroxicam
20mg/day 에 비해 더 적은 부작용의 발생을 보여 주였
다26-28)(Table 7). 그러나 meloxicam 7.5 mg은 diclofenac
100 mg/day 나 piroxicam 20 mg/day 에 비해 약물의
Fig ure 4. COX- 1: Serum thromboxane B2(T xB2).
- 497 -

-대한내과학회지 : 제 59 권 제 5 호 통권 제 483 호 2000 -
효과 면에서 상대적으로 낮은 농도였으며 과연 더 높은
농도에서도 이와 같은 안전성이 지속되는지는 아직 확
신할 수 없다.
1985년에 소개된 Nimesulide는29) COX- 2 side- pocket을
통해 작용하며 약 5- 16배의 COX- 2 s electivity를 갖
는다30). 경구 투여 시 흡수는 약 1.2- 3.2 시간(tmax)이면
거의 완전히 이루어지며 약물 반감기는 약 1.6- 5.0 시간
정도이다29).
임상실험에 따르면 nimesulide는 다양한 상황에서 진
통, 소염, 그리고 해열작용을 나타낸다29). 그러나, 위장관
계 부작용에 있어서는 타 NSAIDs에 비해 더 나을 것이
없었고29) 궤양 발생율도 다른 NSAIDs와 비슷한 수준으
로 나타났으며31) 또한, 실제 임상에서 투여되는 용량에
서 COX- 2 selectivity가 사라져 버림으로서 더 이상
COX- 2에 selective 하다고 할 수 없을 것이다. 그외 안
전성이 입증된 NSAIDs로 etodalac32)과 nabumetone33)
이 있으며 이들 역시 COX- 2 selective 하다고 여겨지나
다른 약들에 비해 그 증거가 부족한 상태이다34).
3. Cyclooxygenase-2 specific inhibitors
모든 범위의 용량과 농도에서 COX- 2는 억제하지만
COX- 1에는 아무런 영향이 없는 그런 약물을 우리는
COX- 2 specific inhibitors라 부른다35).
1) Rofecoxib
Rofecoxib는 methylsulphonylphenyl 유도체로서
COX- 1(IC50COX- 1:1.5×10-5mol/L)에 비해 훨씬 높은
COX- 2(IC50COX- 2:1.8×10-8mol/L) selectivity를 갖고
있는 COX- 2 specific inhibitors이다(selectivity ratio
>800)36). 인간에서의 자세한 약물역동은 아직 정립되지
않았으나 rofecoxib는 long- acting 약물로서 하루 한번
투약이 가능하다. Rofecoxib 50 mg 은 placebo보다 우수
하며, 통증 경감 면에 있어서도 최소한 ibuprofen 400
mg 이나 naproxen 550 mg 과 동일한 효과가 있다37,38).
Phase 2 실험을 통해 rofecoxib 하루 용량 12.5- 25 mg
이 5 mg 보다 더 효과적이었음을 알 수 있었고39) 골관
절염 치료를 통한 공인된 자료에 따르면 rofecoxib 하루
T able 6. Differential inhibition of COX- 1 and COX- 2 by various NSAIDs us ing human recombinant enzymesin w hole cell as s ays 14). IC50 values are expres s ed in μmol/ L. Ratios g iven are the ratio of the IC50 ofCOX- 2/ IC50 of COX- 1. All ratios w ere not given in the orig inal publications . 6- MNA is the active metaboliteof nabumetone. T he low es t IC50 values from Ref. 32 repres ented here
Churchill et al30 Cromlesh et al31 Kargman et al32IC50COX- 1 IC50COX- 2 Ratio IC50COX- 1 IC50COX- 2 Ratio IC50COX- 1 IC50COX- 2 Ratio
Aspir inKetoprofenF lurbiprofenIndomethaciNaproxenPirox icamIbuprofen6- MNASulindacSulphideDiclofenacNimesulideMeloxicamFlosulideDuP- 697NS- 398L- 745,337
4.70 16.03 3.4 14.9 5- 70 - 10.0015 0.12 820.0008 0.069 87 0.001 0.002 2
0.019 0.030 1.6 0.0019 0.052 27 0.013 0.016 1.20.33 7.08 21 0.45 6.3 142.03 0.98 0.5 0.8 0.53 0.72.26 15.72 7 2.9 > 50 17 0.472 0.465 18.40 > 300 > 36
0.006 0.29 4.8
0.0026 0.001 0.4 0.003 0.006 2 0.005 0.001 0.21.61 0.36 0.2 5.2 0.87 0.162.24 0.16 0.07
> 18 0.02 0.0010.041 0.002 0.057.7 0.004 0.0005 0.864 0.003 0.003> 93 0.26 0.003 47.6 0.02 0.0004
Differential inhibit ion of COX- 1 and COX- 2 by NSAIDs: a s ummary of results obtained using various tes ts ys tems. Selective COX- 2 inhibitors . Proceedings of a conference held on March 20- 21, 1997 in Cannes , F rance
- 498 -

-박종서 외 1인 : 비스테로이드성 항염제(NSAIDs) 치료의 최근 경향-
용량 12.5- 25 mg 은 ibuprofen 800 mg three times a
day(6주)나 diclofenac 50 mg thrice daily(6- 12 개월)와
같은 효과를 보였다40, 41).
하루 투여용량 250 mg에서 rofecoxib는 비교적 높은
약물 순응도와 COX- 1/COX- 2 selectivity 역시 잘 유지
됨을 보여주었지만, 출혈시간의 연장이나 placebo에 비
해 위점막 손상의 정도가 증가됨 등은 발견할 수 없었
고, 오히려 ibuprofen 2.4 g(over 7 days)보다 더 적은 정
도의 위점막 손상을 보여 주었다42). Indometacin과 비교
하는 in vitro 실험에서 rofecoxib는 위점막의 PGE2 생
성이나 소장에서의 투과성 변화에 미치는 영향이 없음
을 알 수 있었다43). Rofecoxib 각각 25 mg qd와 50 mg
qd, 그리고 ibuprofen 800 mg tid 를 12주 간 투여 후 내
시경으로 각각에 따른 위십이지장 궤양 발생율을
placebo와 비교 조사한 실험에서 Figure 5와 같은 결과
를 보여 rofecxib가 ibuprofen과 같은 기존의 NSAIDs
보다 위장관에 대한 부작용 면에서 월등함을 보여주었
다(Figure 5). 6 개월 이상의 장기간 복용에 따른 궤양
발생율에 대한 자세한 보고는 아직 없으나 이 역시
placebo와 비슷하거나 또는 ibuprofen(2400 mg/day) 보
다는 훨씬 낮은 수준으로 보고있다44).
2) Celecoxib
Celecoxib는 1998년 미국 FDA 공인을 받고 소개된
약으로 1,5- diaryl pyrazole 복합체로 이루어져 있으며45)
COX- 1(IC50 COX- 1:1.5×10-5mol/L)에 비해 훨씬 높은
COX- 2(IC50 COX- 2:4×10-8mol/L) selectivity를 갖고있
는 COX- 2 specific inhibitors이다46). Celecoxib는 COX- 2
에 대한 selectivity가 약 375 배정도 이고46, 47), 600 mg
twice daily로도 혈청 thromboxane이나 platelet 기능에
미치는 영향이 없다48). 약물의 흡수는 약 3 시간(tmax) 정
도로 빠르며 약물 반감기는 약 11.2 시간이다49). 약물의
T able 7. All reported advers e events in global s afety analys is (%)
Melox icam(7.5 mg)(n=893)
Meloxicam(15 mg)(n=3282)
Pirox icam(20 mg)(n=906)
Diclofenac(100 mg)(n=324)
Naproxen(750- 1000 mg)
(n=243)
Patient- yrs ofexposure 172 1146 166 81 78
Gastro-intes t inal 17 18 20 27 37
Centralnervous syst . 8 8 7 7 8
Increase inGOT /GPT 6 7 6 16 10
Skin/appendages 7 6 4 4 8
Res piratorysystem 6 7 4 6 6
Urinary syst . 4 5 5 3 5
Increase incr ./BUN 0.5 0.4 0.9 0.3 0.4
T otal 43 45 44 56 61
Fig ure 5. 12- Week endoscopy studies in patientw withosteoarthritis.
- 499 -

-Korean Journal of Medicine : Vol. 59, No. 5, 2000 -
투여 용량은 류마티스 관절염의 치료 시 100- 200 mg
twice a day로 시작하고, 골 관절염의 치료 시에는 200 mg
once daily 나 100 mg twice daily로 시작하면 된다.
Celecoxib 100 또는 400 mg 단일 용량은 placebo보다
우수한 효과를 보였으며 통증경감에 있어서도 아스피린
만큼 효과적이었다50, 51).
인간의 위 점막에서 PG 생성에 미치는 celecoxib의
효과에 대해서는 아직 공인된 자료가 부족하나, cele-
coxib 200 mg bid 또는 rofecoxib 250 mg qd로 7일간
투여 후 실시한 내시경검사 실험에서 위 점막의 손상정
도를 살핀 결과 placebo실험과는 차이가 없는 반 면
naproxen 500 mg twice a day 와 비교했을 때는 손상
정도에 분명한 감소가 있었고36)(Figure 6), 또한 3- 6 개
월에 걸쳐 실시한 궤양 발생율 조사에서 역시 placebo와
는 비슷했지만, naproxen 이나 diclofenac 보다는 훨씬
낮은 궤양 발생율을 보여주었다52, 53)(T able 8).
4. Alternatives to specific COX-2 inhibitors
1) NO-NSAIDs
PG과 마찬가지로 nitric oxide(이하 NO)도 위점막을
보호한다. 실제로 COX- 1 knock- out mice에서 NO는 위
궤양의 발생을 효과적으로 억제하였으며54), 이는 실제 임
상에서 응용할 수 있는 모델을 제시한 것으로 생각되어진
다. NO- NSAIDs는 일반적인 NSAIDs에 NO를 연결시킨
것으로 이론적으로 위점막에 NO를 공급하여 NSAIDs의
PG에 대한 작용으로 발생하는 손상을 보상하는 것이며
이러한 위장관계에 대한 안전성은 동물실험을 통해 그 효
능이 입증되었다. 한가지 예로 NO- aspirin은 심혈관계 질
환의 예방에 효과적이면서도 매우 안전한 약이 될 것이고
더욱이 aspirin은 non- aspirin NSAIDs 보다 더 중요한 궤
T able 8. Phas e 3 endos copic s afety s tudies w ith celecox ib
Patients Duration T reatment n ulcers(%) Ref
Rheumatoidarthr it is
12 w eeks
PlaceboCelecox ib 100mg bdCelecox ib 200 mg bdCelecox ib 400 mg bdNaproxen 500 mg bd
231240235218221
464626
38
Rheumatoidarthr it is
24 w eeksCelecox ib 200 mg bdDiclofenac SR 75 mg bd
212218
415
39
Fig ure 6. Lack of gastric damage with two specific inhibitors of COX- 2.
- 500 -

- Jong- Seo Park, et al : Current trend of NSAID use -
양 출혈의 원인이 된다는 점에서 그 중요성은 크다 하겠
다55). 이러한 NO- NSAIDs의 사용이 향후 COX- 2 inhibi-
tors를 대신할 수도 있다 하겠으나 실제 임상에서 이용할
수 있기에는 아직 입증된 자료가 부족한 실정이다.
2) Non-selective NSAIDs with protective agent
Misoprostol56)이나 omeprazole57, 58) 같은 proton- pump
inhibitors 등은 NSAID와 연관된 궤양을 예방할 수 있다.
그러나 COX- 2 inhibitors와 비교하여 무엇이 더 우수한
가는 판정하기 아직 어려운 것 같다.
3) Preferential COX-2 inhibitors
Meloxicam은 실험에서 이미 상당히 설득력이 있는
약물 안전성을 보여주었고 더욱이 preferential COX- 2
inhibitors와 specific COX- 2 inhibitors를 비교했던 많은
실험들이 서로 다른 design으로 이루어진 점을 생각할
때 specific과 preferential COX- 2 inhibitors간의 약물
안전성 비교는 그리 간단히 판단될 일이 아닐 것이며 오
직 직접 비교만이 이 문제에 답을 줄 수 있을 것이다.
5. COX-2 inhibitors and their potentia l for inducing
gastrointestinal lesions
COX- 2의 발견이후 사람의 위장관 내에서의 COX- 1
과 COX- 2 발현에 대한 연구가 이루어져왔다. 다양한 위
장관 조직 내에서 COX- 1 단백이 광범위하게 표현됨이
밝혀진 반면, 대부분의 위장관에서 COX- 2의 발현은 관
찰되지 않았다59, 60). 그러나 정상인의 위장관 내에서와는
반대로, 대장암 환자에서 얻어진 조직 내에서는 상당한
정도의 COX- 2 발현을 관찰할 수 있었는데59, 61,62) 이는
대장암의 발생에 대항하는 NSAIDs의 작용이 COX- 2의
억제를 매게 함으로써 이루어짐을 짐작케 한다.
동물실험을 통해 selective prototypic COX- 2 inhi-
bitor는 기존의 다른 NSAIDs에서 볼 수 있는 위장관 부
작용이 없다는 것이 밝혀졌다. 이러한 결과는 selective
COX- 2 inhibitor인 MK- 966을 이용한 인체 실험에서도
관찰할 수 있었는데, 이 실험은 내시경을 이용하여 위장
관 질환이 없다고 밝혀진 건강한 자원자를 대상으로
MK- 966 250 mg qd 와 ibuprofen 800 mg tid, 그리고
aspirin 650 mg qid 및 placebo등을 7일간 투여하여 서
로 비교 관찰하였다63). 관찰결과 ibuprofen과 aspirin은
위장관에 상당한 정도의 궤양 및 미란 등을 유발하였으
나 MK- 966은 placebo와 차이가 없어 기존의 NSAIDs
에 비해 selective COX- 2 inhibitor는 위장관에 미치는
부작용이 거의 없다는 장점이 있음을 확인하였다. 그외
내시경을 이용하여 specific COX- 2 inhibitor인 celecoxib
나 rofecoxib 등이 위장관에 미치는 영향을 naproxen,
ibuprofen, aspirin 및 placebo 등과 비교한 실험(Figure
5)에서도 이와 같은 장점이 확인되었다36).
결 론
COX- 2 inhibitors는 염증과 진통의 조절에 있어 매우
중요한 부분을 차지하는 약물이다. 약물의 사용과 함께 그
들의 장·단점들이 점차 들어 나게 되면서 non- selective
NSAIDs는 misoprostol이나 omeprazole 등과 함께
COX- 2 inhibitors의 alternatives로서의 위치를 가름하
게 될 것으로 생각된다. NO- NSAIDs에 대한 논의는 아
직 이른 감이 있다.
역설적이게도 COX- 2 inhibitors의 급박한 등장은
non- selective NSAIDs를 반드시 처방이 필요한 약물에
서 over- the- counter로 이끄는 결과를 낳고 있고 장차
non- selective NSAIDs나 aspirin의 self- medication에
의한 위장관계 부작용의 증가가 예상되고 있다.
RE F E R E N C E S
1) Kelly WN et al. T extbook of rheum atology. 5th ed.,p.707- 740, P hiladelphia, W .B . Saunders, 1997
2) Dewitt DL, Meade EA, Smith WL. P GH synthaseisoenz yme selectivity: the potential for safernonsteroidal antiinflamm atory drugs. A m J M ed95(Suppl 2A ):40S- 44S , 1993
3) Klippel JH, Dieppe PA. Textbook of rheumatology,2nd ed., vol. 1 section 3.5.1, 1998
4) Vane HR. T owards a better aspirin. N ature. 367:215-216, 1994
5) Pairet M, Engelhardt G. Distinct isoform s (COX - 1and COX - 2) of cyclooxygenase: plssible physiolo-g ical and therapeutic im plications. F und Clin P har-macol 10:1- 15, 1996
6) Pollison R. N onsteroidal anti- inflammatory drugs :P ractical and theoretical considerations in theirselection. A m J M ed 100(Suppl 2A ):31S- 36S, 1996
7) Kim JG, Graham DY. M isoprostol Study Group.H elicobacter pylori infection and development ofgastric or duodenal ulcer in arthritic patients receivingchronic N SA IDs therapy. A m J Gastroenterol89:203- 207, 1994
- 501 -

-대한내과학회지 : 제 59 권 제 5 호 통권 제 483 호 2000 -
8) Johnson AG, Nguyen T V, Day RO. Do nonsteroidalanti- inflammatory drugs affect blood pressure? A nnIntern M ed 121:289- 300, 1994
9) Fu JY, Masferrer JL, Seibert K, Raz A, NeedlemannP. T he induction and suppression of prostaglandinH 2 synthase(cyclooxygenase) in human monocytes. JB iol Chem 265:16737- 16740, 1990
10) Picot D, Loll PJ, Garavito RM. The X - ray crystalstructure of the membrane protein prostaglandin H2synthase- 1. N ature 367:243- 249, 1994
11) Luong C, Miller A, Barnett J, Chow J, Ramasha C,Browner MF. T he structure of human cyclooxy-genase- 2; conservation and flexibility of the N SA IDsbinding site. N at S truct B iol 3:927- 933, 1996
12) Hawkey CJ. COX- 2 inhibitors. Lancet 353(9149):307- 314,1999
13) Gans KR, Galbraith W, Roman RJ, Haber SB, KerrJS, Schmidt WK, Smith C, Hewes WE, AckermanNR. A nti- inflam matory and safety profile of DuP 697,a novel orally effective prostaglandin synthesisinhibition. J P harm acol E xp T her 254:180- 187, 1990
14) Pairet M, van Ryn J, Mauz A, Schierok H, DiederenW, T urck D, Engelhardt G. Differential inhibition ofCOX - 1 and COX - 2 by N SA IDs: a sum mary ofresults obtained using various test systems. In: V aneJ , B otting J , eds. Selective COX - 2 inhibitors:pharmacology, clinical effects and therapeuticpotential. Dordrecht: K luwer A cademic P ublishers,3:27- 46, 1997
15) Ehrich EW, Dalloh A, De Lepeleire I, Van Hecken A,Riendeau D, Yuan W, Porras A, Wittreich J, SeiboldJR, De Schepper P, Mehlisch DR, Gertz BJ. ClinP harm T her 65:336- 347, 1999
16) Noble S, Balfour JA. M eloxicam. Drugs 51:424- 432,1996
17) Jackson LM, Wu K, Mahida YR, et al. COX - 1expression in human gastric mucosa infected withH elicobacter pylori: constitutive or induced?Gastroenterology 114:A 160, 1998
18) Patrignani P, Panara MR, Sciulli MG, Santini G,Renda G, Patrono C. Differential inhibition of humanprostaglandin endoperoxide synthase- 1 and - 2 bynonsteroidal anti- inflammatory drugs. J PhysiolP harmacol 48:623- 631, 1997
19) Gierse J, McDonald J, Hauser S, Rangwala S, SeibertK. A sing le am ino acid difference between cyclooxy-genase- 1 (COX - 1) and - 2 (COX - 2) reverses theselectivity of COX - 2 specific inhibitors. J B iol Chem271:15810- 15814, 1996
20) Goeithe HS, Lund B, Distel MR, Bluhmki E. Adouble- blind, randomized trial to compare meloxicam
15 mg with diclofenac 100 mg in the treatment ofosteoarthritis of the knee. Osteoarthritis Cartilage15:283- 288, 1997
21) Linden B, Distel M, Bluhmki E. A double- blind studyto compare the efficacy and safety of meloxicam 15mg with piroxicam 20 mg in patients with osteoar-thritis of the hip. B r J R heumatol 35(Suppl 1):35- 38,1996
22) Hosie J, Dis tel M, Bluhmki E. M eloxicam inosteoarthritis: a six m onths, double- blind comparisonwith diclofenac sodium . B r J R heumatol 35(Suppl1):39- 43, 1996
23) Hosie J, Dis tel M, Bluhmki E. E fficacy and tolerabilityof m eloxicam versus piroxicam in patients withosteoarthritis of the hip or knee: a six- month double-blind study. Clin Drug Invest 13:175- 184, 1997
24) Wojtulewski JA, Schattenkirchner M, Barcelo P, et al.A six months double- blind trial to com pare theefficacy and safety of meloxicam 7.5 mg daily andnaproxen 750 m g daily in patients with rheumatoidarthritis. B r J R heumatol 35(Suppl 1): 22- 28, 1996
25) Patoia I, Santucci I, Furno P, et al. A four- week,double- blind, parallel- group study to compare thegastrointestinal effects of m eloxicam 7·5 mg,meloxicam 15 mg, piroxicam 20 m g and placebo bymeans of faecal blood loss, endoxcopy and symptomsevaluation in healthy volunteer. B r J R heumatol35:61- 67, 1996
26) Dis tel M, Mueller C, Bluhmki E, Fries J. Globalanalysis of safety of a new N SAIDs, meloxicam. Br JR heumatol 35(Suppl 1):68- 77, 1996
27) Hawkey C, Kahan A, Steinbruck K, Alegre C,Baumelou E, Begaud B, Dequelcer J, Isomaki H,Littlejohn G, Man J, Papazoglou S. Gastrointestinaltolerabability of the COX - 2 inhibitor, meloxicam, inosteoarthritis patients: the m eloxicam large scaleinternatinal study safety assessment (M E LISSA ). B rJ R heumatol 37:937- 945, 1998
28) Dequeker J, Hawkey C, Kahan A, Steinbruck K,Alegre C, Baumelou E, Begand B, Isomaki H,Littlejohn G, Mau J, Papazoglou S. Improvement ingastrointestinal tolerabilityof the selective cyclooxy-genase (COX )- 2 inhibitor, meloxicam, com paredwith piroxicam : results of the safety and efficacylarge- scale evaluation of COX - inhibiting therapies(SELE CT ) trial in osteoarthritis. B r J R heumatol37:946- 951, 1998
29) Davis R, Brogden RN. N imesulide: an update on itspharmacodynamic and pharm acok inetic properties,and therapeutic efficacy. Drugs 48:431- 454, 1994
30) T avares IA, Bishai PM, Bennett A. A ctivity of
- 502 -

-박종서 외 1인 : 비스테로이드성 항염제(NSAIDs) 치료의 최근 경향-
nimesulide on constitutive and inducible cyclooxy-genases. A rz neim ittelforschung 45:1093- 1095, 1995
31) Garcia Rodriguez LA, Cattaruzzi C, T roncon MG,Agostinis L. R isk of hospitalisation for uppergastrointestinal tract bleeding associated with keto-rolac, other nonsteroidal anti- inflammatory drugs,calcium antagonists, and other antihypertensivedrugs. A rch Intern M ed 158:33- 39, 1998
32) Glaser K, Sung ML, O' Neill K, Belfas t M, HartmanD, Carlson R, Kreft A, Kubrak D, Hsiao CL,Weichman B. Etodolac selectively inhibits humanprostaglandin G/ H synthase 2 (P GH S- 2) versushuman P GH S- 1. Eur J Pharmacol 281:107- 111, 1995
33) Hallyar J, Bjarnason I. N SA IDs, COX - 2 inhibitors,and the gut. Lancet 346:521- 522, 1995
34) Cipollone F, Ganci A, Panara MR, Greco A,Cuccurullo F, Patrono C. E ffects of nabum etone onprostanoid synthesis in humans. Clin P harm acol T her58:335- 341. 1995
35) Brooks P, Emery P, Evans J, et al Interpreting theclinical significance of the differential inhibition ofcyclooxygenase- 1 and cyclooxygenase- 2. B r JR heum atol ( in press).
36) Lanza FL, Rack MF, Callison DA, et al. A pilotendoscopic study of the gastroduodenal effects ofSC- 58635, a novel COX - 2- selective inhibitor.Gastroenterology 112(Suppl 4):A 194, 1997
37) Ehrich E, Mehlisch D, Perkins S, et al. Efficacy ofM K - 966, a highly selective inhibitor of COX - 2, inthe treatment of postoperative dental pain. A rthritisR heum 39(Suppl 9):S81, 1996
38) Mehlisch DR, Mills S, Sandler M, et al. E x vivo assayof COX - 2 inhibition predicts analgesic efficacy inpost- surg ical dental pain with M K - 966. ClinP harmacol T her 63:139, 1998
39) Ehrich E, Schnitzer T , Kivitz A, et al. M K - 966, ahighly selective COX - 2 inhibitor, was effective in thetreatment of osteoarthritis (OA ) of the knee and hipin a six- week placebo controlled study. A rthritisR heum 40(Suppl 9):S85, 1997
40) Saag K, Fisher C, McKay J, et al. M K - 0966, aspecific COX - 2 inhibitor, has clinical efficacycomparable to ibuprofen in the treatment of knee andhip osteoarthritis (OA ) in a six- week controlledclinical trial. A rthritis R heum 41(Suppl 9):S84, 1998
41) Cannon G, Caldwell J, Holt P, et al. M K - 0966, aspecific COX - 2 inhibitor, has clinical efficacycomparable to diclofenac in the treatment of kneeand hip osteoarthritis (OA ) in a 26- week controlledclinical trial. A rthritis R heum 41(Suppl 9):S83, 1998
42) Lanza F, Simon T , Quan H, et al. Selective inhibition
of cyclooxygenase- 2 (COX - 2) with M K - 0966 (250mg qd) is associated with less gastroduodenaldamage than aspirin (A SA ) 650 mg qid or ibuprofen(IB U) 800 m g tid. Gastroenterology 112:A 194, 1997
43) Cryer B, Gottesdiener MD, Gertz B, Hsieh P, DallobA, Feldm an M E ffects of a novel cyclooxygenase(COX )- 2 inhibitor on gastric mucosal prostag landin(P G) synthesis in healthy hum ans. A m J Gastroen-terol 93:A 104, 1998
44) Smolen J. Clinical trials of COX - 2 inhibitors. In:V ane J , ed. T he promise of specific COX - 2 inhibitionby novel agents. London, W illiam H arvey P ress,1998
45) Penning TD, Talley JJ, Bertenshaw SR, Carter JS,Collins PW, Docter S, Graneto MJ, Lee LF, Malecha JW,Miyashiro JH, Rogers RS, Rogier DJ, Yu SS, AndersonGD, Burton EG, Cogburm Jn, Gregory SA, Koboldt CM,Perkins WE, Seibert K, Veenhuizen AW, Zhary YY,Isakson PC. Synthesis and biological evaluation of the1,5- diarylpyrazole class of cyclooxygenase- 2 inhibitors:identification of 4- [5- (4- methylphenyl)- 3- (trifluoro-m e thy l) - 1H - py raz ol- 1- y ] be nz e n- e s u lfonam ide(SC- 58635, celecoxib). J M ed Chem 40:1347- 1365,1997
46) Isakson P, Zweifel B, Masferrer J, et al. SpecificCOX - 2 inhibitors: from bench to bedside. In: V aneJ, Botting J , eds. Selective COX - 2 inhibitors: pharma-cology, clinical effects and therapeutic potential.p.127- 133. London, W illiam H arvey P ress, 1997
47) Lipsky PE, Isakson PC. Outcome of specific COX - 2inhibition in rheumatoid arthritis. J R heum atol 24:9- 14, 1997
48) Mengle- Gaw L, Hubbard RC, Karim A, et al. A studyof the platelet effects of SC- 58635, a novel COX - 2-selective inhibitor. A rthritis R heum 40(Suppl 9):S93,1997
49) Celebrex data sheet. Searle, 1999.50) Hubbard RC, Mehlisch DR, et al. SC- 58635, a highly
selective inhibitor of COX - 2, is an effective analgesicin an acute post surg ical pain model. J Invest M ed44:293A , 1996
51) Mehlisch DR, Hubbard RC, et al. A nalgesic efficacyand plasma levels of a highly selective inhibitor ofCOX - 2 (SC- 58635; SC) in patients with post- surgicaldental pain. Clin P harmacol T her 61:195, 1997
52) Geiss GS, Hubbard RC, Callison DA, Yu S, Zhao W.Safety and efficacy of celecoxib, a specific COX - 2inhibitor. R heumatol E ur 27(Suppl 1):118, 1998
53) Geiss GS, Stead H, Morant SV, Nandin R, HubbardRC. E ndoscopic and tolerability, results from a studyof celecoxib, a specific COX - 2 inhibitor, in patients
- 503 -

-Korean Journal of Medicine : Vol. 59, No. 5, 2000 -
with rheumatoid arthritis. R heumatol E ur 27(Suppl1):118, 1998
54) Mahler JF, Davis BJ, Morham SG, Lanenbach R.Disruption of cyclooxygenase genes in mice. ToxicolP athol 24:717- 719, 1997
55) Stack WA, Hawkey GM, Atherton JC, et al. N SA IDsand CagA positive H pylori but not CagA negativeH pylori as independent risk factors for bleedingpeptic ulcers. Gastroenterology 114:A 294, 1998
56) Silverstein FE, Graham DY, Senior JR, Davies HW,Struthers BJ, Bittmrn RM, Geis GS. M isoprostolreduces serious gastrointestinal complications inpatients with rheum atoid arthritis receivingnonsteroidal anti- inflammatory drugs: a randomiz ed,double- blind, placebo- controlled trial. A nn InternM ed 123:241- 249, 1995
57) Hawkey CJ, Jeffrey AK, Szczepanski L, Walker DG,Barlcun A, Swannell AJ, Yeomans ND. A comparisonof omepraz ole and misoprostol for treating andpreventing ulcers associated with non- steroidalanti- inflammatory drugs. N E ngl J M ed 338:727-734, 1998
58)Yeomans ND, T ulassay Z, Juhasz L, Racz I, HowardJM, Van Rensburg CJ, Swannell AJ, Howkey CJ. Acomparison of omepraz ole and ranitidine for treatingand preventing ulcers associated with non- steroidal
anti- inflammatory drugs. N E ngl J M ed 338:719-726, 1998
59) Kargman SL, O' Neill GP, Vickers PJ, Evans JF,Mancini JA, Jothy S. E xpression of prostag landinG/ H synthase- 1 and - 2 protein in human coloncancer. Cancer R es 55:2556- 2559, 1995
60) Kargman S, Charleson S, Cartwright M, et al.P rostaglandin G/ H synthase- 1 and - 2 in rat, dog ,monkey and human gastrointestinal tracts: Localiz a-tion, enz ymatic activity and inhibition by N SA IDs.Gastroenterology. In press.
61) Eberhart CE, Coffey RJ, Radhika A, Giardiello FM,Ferrenbach S, Dubois RN. Upregulation of cyclooxy-genase 2 gene expression in hum an colorectaladenomas and adenocardinomas. Gastroenterology107:1183- 1188, 1994
62) Sano H, Kawahito Y, Wilder RL, Hashiramoto A,Mukai S, Asai K, Kimura S, Kato H, Kondo M, HlaT . E xpression of cyclooxygenase- 1 and - 2 in humancolorectal cancer. Cancer R es 55:3785- 3789, 1995
63) Lanza F, Simon T , quan H et al. Selective inhibitionof cyclooxygenase- 2(COX - 2) with M K - 0966(250mgQ.D.) is associated with less gastrointestinal damagethan aspirin(A SA ) 650mg Q.I.D. or ibuprofen(IB U)800 mg T .I .D. Gastroenterology 112:A 194, 1997
- 504 -

![증 권(일 괄] 신 고 서 · 2020-06-16 · 4 투자실적추이 (연평균 수익률) 종류 최초설정일 최근 1 년 최근 2 년 최근 3 년 최근 5 년 2019/04/25 ~ 설정일이후](https://img.pdfslide.tips/doc/110x75/5fb0cfab7969fe5d983eb8f5/-eoe-e-e-oe-2020-06-16-4-e-e.jpg)
![최근 러시아 경제동향과 2015년 對러 교역여건 전망TF] 최근 러시아... · 2015. 3. 2. · 2 최근 러시아 경제동향과 2015년 對러 교역여건 전망](https://img.pdfslide.tips/doc/110x75/60a4f12fd8a2585baf21b303/oee-eoe-eoeee-2015e-e-ee-e-tf-oee-eoe.jpg)