-
7/27/2019 Etiologi Gea
1/7
10.1128/JCM.43.8.3636-3641.2005.
2005, 43(8):3636. DOI:J. Clin. Microbiol.Gerner-SmidtKrogfelt,
Eskild Petersen, Kre Mlbak and PeterHelms, Flemming Scheutz,
Katharina E. P. Olsen, KarenEthelberg, Peter Schiellerup, Charlotte
Jensen, MortenBente Olesen, Jacob Neimann, Blenda Bttiger,
SteenDenmark: a Case-Control StudyEtiology of Diarrhea in Young
Children in
http://jcm.asm.org/content/43/8/3636Updated information and
services can be found at:
These include:
REFERENCES
http://jcm.asm.org/content/43/8/3636#ref-list-1at:This article
cites 38 articles, 23 of which can be accessed free
CONTENT ALERTS
morearticles cite this article),Receive: RSS Feeds, eTOCs, free
email alerts (when new
http://journals.asm.org/site/misc/reprints.xhtmlInformation
about commercial reprint
orders:http://journals.asm.org/site/subscriptions/To subscribe to
to another ASM Journal go to:
onSe
ptember29,2013byguest
http://jcm.asm.org/
Downloaded
from
onSe
ptember29,2013byguest
http://jcm.asm.org/
Downloaded
from
onSe
ptember29,2013byguest
http://jcm.asm.org/
Downloaded
from
onSe
ptember29,2013byguest
http://jcm.asm.org/
Downloaded
from
onSe
ptember29,2013byguest
http://jcm.asm.org/
Downloaded
from
onSe
ptember29,2013byguest
http://jcm.asm.org/
Downloaded
from
onSe
ptember29,2013byguest
http://jcm.asm.org/
Downloaded
from
http://jcm.asm.org/cgi/alertshttp://jcm.asm.org/cgi/alertshttp://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/http://jcm.asm.org/cgi/alerts
-
7/27/2019 Etiologi Gea
2/7
JOURNAL OF CLINICAL MICROBIOLOGY, Aug. 2005, p. 36363641 Vol.
43, No. 80095-1137/05/$08.000
doi:10.1128/JCM.43.8.36363641.2005Copyright 2005, American Society
for Microbiology. All Rights Reserved.
Etiology of Diarrhea in Young Children in Denmark: aCase-Control
Study
Bente Olesen,1,2* Jacob Neimann,3 Blenda Bottiger,1 Steen
Ethelberg,1 Peter Schiellerup,1
Charlotte Jensen,1 Morten Helms,1 Flemming Scheutz,1 Katharina
E. P. Olsen,1
Karen Krogfelt,1 Eskild Petersen,1 Kre Mlbak,1 and Peter
Gerner-Smidt1
Department of Bacteriology, Mycology, and Parasitology,
Department of Virology, and Department of Epidemiology,Statens
Serum Institut, Artillerivej 5, DK-2300 Copenhagen S, Denmark1;
Department of Clinical Microbiology,
Hillerd Hospital, Helsevej 2, DK-3400 Hillerd, Denmark2; and
Danish Zoonosis Centre, Danish Institutefor Food and Veterinary
Research, Mrkhj Bygade 19, DK-2860 Sborg, Denmark3
Received 17 December 2004/Returned for modification 1 April
2005/Accepted 14 April 2005
Infectious gastroenteritis is one of the most common diseases in
young children. To clarify the infectiousetiology of diarrhea in
Danish children less than 5 years of age, we conducted a 2-year
prospective case-controlstudy. Stools from 424 children with
diarrhea and 870 asymptomatic age-matched controls were examined,
andtheir parents were interviewed concerning symptoms. Rotavirus,
adenovirus, and astrovirus were detected byenzyme-linked
immunosorbent assay, and norovirus and sapovirus were detected by
PCR. Salmonella, ther-motolerant Campylobacter, Yersinia, Shigella,
and Vibrio spp. were detected by standard methods. Shiga
toxin-producing (STEC), attaching-and-effacing (A/EEC),
enteropathogenic (EPEC), enterotoxigenic, enteroinva-sive, and
enteroaggregative Escherichia coli were detected by using colony
hybridization with virulence geneprobes and serotyping. Parasites
were detected by microscopy. Overall, a potential pathogen was
found in 54%of cases. More cases than controls were infected with
rotavirus, Salmonella, norovirus, adenovirus, Campy-
lobacter, sapovirus, STEC, classical EPEC, Yersinia, and
Cryptosporidium strains, whereas A/EEC, althoughcommon, was not
associated with illness. The single most important cause of
diarrhea was rotavirus, whichpoints toward the need for a childhood
vaccine for this pathogen, but norovirus, adenovirus, and
sapoviruswere also major etiologies. Salmonella sp. was the most
common bacterial pathogen, followed by Campylobacter,STEC,
Yersinia, and classical EPEC strains. A/EEC not belonging to the
classical EPEC serotypes was notassociated with diarrhea,
underscoring the importance of serotyping for the definition of
EPEC.
Infectious gastroenteritis is one of the most common dis-
eases in humans, with particularly high morbidity in
childrenyounger than 5 years of age (3). In industrialized
countries,such as Denmark, the associated mortality is low, but the
socialburden and economic costs due to care of ill children
andparents absence from work are substantial because of the
highincidence. Rotavirus is known to be the most common cause
ofsevere acute, watery diarrhea in children under 5 years of agein
industrialized and developing parts of the world (14, 43). Inrecent
decades other new etiologies of diarrhea have beenrecognized,
including noro- and sapovirus, Shiga toxin-produc-ing Escherichia
coli (STEC), and enteroaggregative E. coli(EAggEC). Furthermore,
the incidence of food-borne Campy-lobacter and Salmonella
infections has increased in many in-dustrialized countries.
Several case-control or cohort studies of
enteropathogensassociated with childhood diarrhea have been
conducted indeveloping countries, but only a few analytical studies
coveringa broad range of newly discovered diarrheal agents have
beenundertaken in Europe (5, 8, 25, 35). Many studies have
focusedon either bacterial or viral etiologies of diarrhea (7, 27,
38).The present study, comprising examinations for bacteria,
virus,and parasites, was conducted to clarify the most common
in-
fectious etiologies of diarrhea in Danish children less than
5
years of age.
MATERIALS AND METHODS
Study design. The present study was designed as a prospective
case-controlstudy and was conducted from March 2000 to December
2001. Cases were
consecutively collected among children less than 5 years of age
with stool samplessubmitted for the diagnosis of infectious
diarrhea to Statens Serum Institut that
covered 8 of the 16 Danish counties, corresponding to ca. 45% of
the Danishpopulation. Verbal agreement to participate in the study
was initially receivedfrom patients parents through their
physician. Parents who agreed to participate
were mailed additional information about the study, a consent
form, and aquestionnaire. The parents were requested to review the
questionnaire immedi-
ately and sign and return the consent form by mail. Patients
were excluded fromthe study if the parents were unable to speak
Danish or if the patient had anunderlying malignant illness, did
not have diarrhea, had siblings already enrolled,
or were part of recognized general outbreaks. Controls were
selected from theDanish Civil Registry, which is a complete and
continuously updated populationregister. Controls were individually
matched with cases on gender, week of birth
and county of residence. Eligible controls were mailed a consent
form and aquestionnaire. The aim was to include two controls per
case. If the controls did
not respond after approximately 10 days, new controls were
chosen. Controlswere excluded from the study if they had had
diarrhea or abdominal pain withfever during the preceding month or
if the parents did not speak Danish. The
study was approved by the Danish Scientific Ethical Committee
(KF 01-235/95and 01-148/96).
Stool investigations. Stools were examined for bacteria, virus,
and parasites. Ifmore than one stool sample was submitted from a
case, only the result from theindex sample was included in the
prevalence calculations in order not to intro-
duce a bias in the comparison with the controls.Rotavirus,
adenovirus, and astrovirus. A 10% stool suspension in Parker
199
medium was prepared, and the suspensions were stored at 20C. The
testing for
* Corresponding author. Mailing address: Department of
ClinicalMicrobiology, Hillerd Hospital, Helsevej 2, DK-3400
Hillerd, Den-mark. Phone: 45-48294379. Fax: 45-48294384. E-mail:
[email protected].
3636
-
7/27/2019 Etiologi Gea
3/7
rotavirus, adenovirus, and astrovirus antigens was performed by
using commer-cially available antigen capture tests from Dako
(Taastrup, Denmark): IDEA
Rotavirus (K6020), IDEA Adenovirus (K6021), and Amplified IDEA
Astrovirus
(K6042). The instructions from the manufacturer were followed,
except thatParker 199 was used instead of the supplied sample
buffer.
Norovirus and sapovirus. The stool suspensions described above
were used.
RNA was extracted by QIAamp Viral RNA minikit (QIAGEN GmbH,
Hilden,Germany) according to the manufacturers instructions. The
purified RNA was
kept at 80C until testing. Reverse transcription-PCR (RT-PCR)
for the de-
tection of noroviruses was performed by using slightly modified
JV12/JV13primers (JV12Y, ATACCACTATGATGCAGAYTA; JV13I,
TCATCATCACC
ATAGAAIGAG) (40) and a One-Step RT-PCR kit (QIAGEN). Viral RNA
was
reverse transcribed for 30 min at 50C. The thermocycling
consisted of 40 cyclesof 30 s at 94C, 30 s at 37C, and 30 s at 72C,
with a final extension at 72C for
10 min. RT-PCR for sapoviruses was performed with primers JV33
and SR80
(39) using the same procedure as for noroviruses but with an
annealing temper-ature of 49C.
Bacteria. The SSI enteric medium was used for isolation of
Shigella spp.,
Salmonella spp., Yersinia enterocolitica, and Vibrio spp. (4).
For the isolation ofCampylobacter coli and C. jejuni, the modified
charcoal cefoperazone deoxy-
cholate agar was used (11). Stool samples were examined for
diarrheagenic E.
coli by colony dot blot hybridization of colonies from the
primary plate of the SSI
enteric medium using DNA probes detecting stx1 and stx2 of STEC
(34, 44); eae
of enteropathogenic E. coli (EPEC), attaching-and-effacing E.
coli (A/EEC), and
some STEC strains (13); ipaH of enteroinvasive E. coli (EIEC)
and Shigellastrains (37); and elt, estA, and estB of
enterotoxigenic E. coli (ETEC) (33) and
pCVD432 for detection of EAggEC (2). Single colonies reacting
positively withthe DNA probes were isolated and characterized
further. The strains were
confirmed as being E. coli by using the Minibact E kit (SSI)
(15) and a test for
-glucuronidase production on PGUA plates (SSI) (19). stx1- or
stx2-positivestrains were confirmed by using the Vero cell assay
(18). O:H serotyping was
performed according to the method of rskov and rskov (24).
Non-STEC E.
coli strains reacting with the eae probe belonging to one of the
classical EPECserotypes (O26:H, O26:H11, O26:H34, O55:H, O55:H6,
O55:H7, O86:H,
O86:H34, O111:H, O111:H2, O111:H25, O114:H, O114:H2,
O119:H,O119:H2, O119:H6, O125ac:H, O125ac:H6, O125ac:H21, O126:H-,
O126:H2,
O126:H21, O126:H27, O127:H, O127:H6, O126:H21, O128ab:H,
O128ab:H2, O128ab:H7, O128ab:H12, O142:H, O142:H6, O158:H, and
O158:H23)
(6, 9, 10, 16, 17, 20, 21, 24, 2832) were classified as EPEC;
similar strains notbelonging to these serotypes were classified as
A/EEC.
Parasites. Formalin (10%) was added to the specimen to a total
volume of 20ml. The specimen was then sifted through a gauze mesh,
diluted 2:1 with phos-
phate-buffered saline (pH 7.2), and spun at 1,600 rpm for 2 min.
The pellet wasresuspended in 7 ml of phosphate-buffered saline plus
3 ml of ethyl acetate andcentrifuged for 2 min at 1,600 rpm. Two
drops were placed on a glass slide and
covered before being examined with a 10 objective lens for ova
and a 20objective lens for protozoan cysts after staining with a
drop of 1% iodine in 2%
potassium iodide. A drop from the pellet was spread on a slide,
dried, andZiehl-Neelsen acid fast stained for Cryptosporidium and
Cyclospora spp.
Interviews. The cases were seen initially by a physician, and
clinical informa-
tion was subsequently collected through telephone interviews
with a parentwithout the assistance of a physician. The parents of
cases were questioned aboutclinical symptoms, treatment, and other
relevant clinical information by using the
standard questionnaire sent out when the child was enrolled in
the study. Inorder to facilitate data collection and reduce
interviewer bias, all interviews were
conducted by using a computer-aided telephone interviewing
system. For use ofmedication, the period in question was 4 weeks,
and for foreign travel it was 1week before the onset of
symptoms.
Statistical methods. Pathogenicity was expressed as an odds
ratio (OR), i.e.,the odds of a pathogen-positive specimen being
collected from a child with
diarrhea divided by the odds of a pathogen-positive specimen
being collectedfrom a control. ORs were calculated by multivariate
logistic regression, adjustingfor the matching variables gender,
age group, and season, as well as for foreign
travel. Three age groups (children 1 year old, 1 year old, and 1
year old) and
four seasons (February to April, May to July, August to October,
and Novemberto January) were used. Percent population attributable
risks (PAR%) were
estimated by using the formula by Miettinen (22).
RESULTS
A total of 424 cases and 866 controls were enrolled in thestudy.
Samples were submitted from hospitals for 16% andfrom general
practitioners for 84% of cases. Stools from allcases and 726 of the
controls were examined for bacterialpathogens, but some samples did
not contain enough materialfor viral and parasitic analysis (Table
1). Overall, a potentialpathogen was found in 54% of cases and 22%
of controls, whenonly samples examined for all pathogens were
considered.
TABLE 1. Prevalence and adjusted ORs for diarrheal pathogenicity
for potential enteropathogens acquired in Denmark and abroad
inchildren younger than 5 years olda
Organism
No. positive/no. tested (%)
OR (95% CI)bAcquired in Denmark Acquired through foreign
travel
Cases Controls Cases Controls
Rotavirus 50/357 (14) 1/635 (1) 1/26 (4) 0/14 (0) 96
(13.1700)Norovirus 19/349 (5) 9/629 (1) 1/25 (4) 1/14 (7) 3.7
(1.78.1)
Adenovirus 16/357 (5) 4/633 (1) 0/26 (0) 0/14 (0) 7.7
(2.523)Sapovirus 11/340 (3) 8/619 (1) 0/25 (0) 0/14 (0) 3.0
(1.27.6)
Astrovirus 3/357 (1) 1/635 (1) 0/26 (0) 0/14 (0) 4.7
(0.547)Salmonella sp. 19/396 (5) 4/712 (1) 3/28 (11) 0/14 (0) 9.3
(3.128)Campylobacter sp. 14/396 (4) 3/712 (1) 0/28 (0) 0/14 (0) 8.8
(2.531)Y. enterocolitica 10/396 (3) 1/712 (1) 0/28 (0) 0/14 (0) 19
(2.4150)STEC 11/396 (3) 5/712 (1) 0/28 (0) 0/14 (0) 4.3 (1.513)EPEC
7/396 (2) 5/712 (1) 3/28 (11) 0/14 (0) 3.1 (1.09.4)ETEC 0/396 (0)
1/708 (1) 2/29 (7) 0/14 (0) 2.0 (0.128)EAggEC 7/396 (2) 8/712 (1)
4/28 (14) 0/14 (0) 2.0 (0.85.1)EIEC 1/396 (1) 0/712 (0) 0/28 (0)
0/14 (0) c
A/EEC 44/396 (11) 91/714 (13) 4/28 (14) 0/14 (0) 1.0 (0.71.4)G.
lamblia 2/344 (1) 4/585 (1) 1/25 (4) 0/10 (0) 1.1
(0.25.3)Cryptosporidium 4/327 (1) 0/561 (0) 2/24 (8) 0/10 (0)
B. hominis 2/344 (1) 6/585 (1) 1/25 (4) 2/10 (20) 0.5
(0.12.0)
Ascaris sp. 1/344 (1) 0/585 (0) 0/25 (0) 0/10 (0) a Mixed
infections are included in this table.b ORs were calculated on the
basis of both domestic and imported infections and adjusted for
gender, age, travel, and season. 95% CI, 95% confidence interval.c
, undefined.
VOL. 43, 2005 DIARRHEA IN DANISH CHILDREN 3637
-
7/27/2019 Etiologi Gea
4/7
Among all samples tested, a virus was found in 26% of casesand
3% of controls; a bacterial pathogen was found in 17% ofcases and
4% of controls excluding A/EEC; and a parasite wasfound in in 4% of
cases and 3% of controls. In order ofobserved frequency, rotavirus,
Salmonella, norovirus, adenovi-rus, thermotolerant Campylobacter,
STEC, EPEC, sapovirus,Y. enterocolitica, and Cryptosporidium spp.
were found at
higher prevalences in patients than in controls (Table 1).A/EEC
was equally common among cases (11%) and controls(13%) and thus not
associated with diarrhea. A number ofmicroorganisms were found only
rarely, including astrovirus,ETEC, EIEC, Ascaris spp., Blastocystis
hominis, and Giardialamblia. No Shigella, Vibrio, or Cyclospora
spp. were isolated.The majority of children infected by virus, EPEC
or STECwere under 3 years of age (Table 2).
Rotavirus was by far the most common pathogen detectedand had
the strongest association with disease (OR 96).Consequentially, a
higher proportion of disease (PAR%) wasattributed to this pathogen
(13.2%) than to any other micro-organism (Table 3). The most
frequently isolated bacterialpathogen was zoonotic Salmonella. Five
serotypes were seen:serovars Typhimurium, Enteritidis, Agona,
Hadar, and Bovis-morbificans in 9, 7, 3, 2, and 1 patient,
respectively. The sero-types Typhimurium, Agona, Derby, and
Braenderup werefound in each of four controls. Eleven patients and
five con-trols were infected with STEC. Five patients were infected
withdifferent serotypes, and two each were infected with
STECO157:[H7], O26:H, and O103:H2. Three healthy childrenalso
carried these three serotypes. All STEC isolates were eaepositive
except one serotype O126:H20 strain. Ten and fiveEPEC of classical
O:H serotypes were isolated from cases andcontrols, respectively.
The most common serotype was O55:
[H7], which was found in 6 of the 10 EPEC patients and innone of
the controls. EPEC was only isolated from cases below2 years of age
(Table 2), and was the second most common(4%) bacterial cause of
diarrhea in that age group.
A total of 2% of cases had mixed infections with
pathogensassociated with diarrhea. Two patients were infected with
bothSalmonella and norovirus and single patients with the
following
combinations: rota- and adenovirus, noro- and adenovirus, ro-ta-
and norovirus, EPEC and adenovirus, EPEC and astrovi-rus, and EPEC
and ETEC.
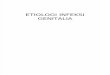
The seasonal prevalence was most prominent for rotavirus,with
most infections seen in the period from January to May.The
bacterial infections tended to occur during summer andfall (Fig.
1).
Clinical data. Selected clinical data on the patients are
givenin Table 4. Overall, the viral infections were characterized
byvomiting. Bloody diarrhea was characteristic for
Campylobacterinfections, but this symptom was also seen among
Salmonella-infected patients, whereas only two of nine patients
infectedwith STEC had bloody diarrhea. None developed
hemolytic-uremic syndrome. Both Salmonella and rotavirus
infectionswere characterized by loss of weight, fever, and high
hospital-ization rates. Antibiotic treatment was given to 21% of
chil-dren infected with Salmonella spp. in contrast to 5% of
chil-dren (P 0.061) with no pathogen identified and 4% ofchildren
(P 0.1) with viral infections. All children survivedtheir
infections.
DISCUSSION
A potential pathogen was detected for 54% of the patients,and an
infectious agent associated with diarrhea was estab-lished for 45%
of the patients in the present study. In spite ofits seasonal
occurrence, rotavirus was the most frequently iso-lated pathogen.
The severity of the rotavirus infections wascomparable to those
caused by Salmonella sp. Norovirus, ad-enovirus, and sapovirus were
also important pathogens ofchildhood diarrhea. Noro- and
sapoviruses have up till nowgenerally not been tested for in
microbiology laboratories, andthe incidence of these pathogens is
therefore probably under-estimated. Astrovirus, a well-known
diarrheagenic pathogen(41), was only identified in a few children
in the present study,which may explain why it was not significantly
linked statisti-cally to diarrhea.
Large case-control studies and cohorts on diarrhea havebeen
conducted in The Netherlands (8), Italy (5), and theUnited Kingdom
(35, 42), and in these studies viruses were
TABLE 2. Age distribution of Danish children with
gastroenteritis caused by the most common pathogensa
Age(yr)
No. (%)
All patientsSalmonella
sp.Campylobacter
sp.Y. enterocolitica STEC EPEC Rotavirus Norovirus Adenovirus
Sapovirus
0 116 (27) 9 (8) 1 (1) 2 (2) 3 (3) 5 (4) 12/103 (12) 3/98 (3)
6/103 (6) 4/112 (4)1 173 (41) 7 (4) 6 (4) 3 (2) 5 (3) 5 (3) 20/159
(13) 14/158 (9) 8/159 (5) 5/155 (3)
2 85 (20) 4 (5) 2 (2) 3 (4) 2 (2) 0 (0) 16/76 (21) 3/76 (4) 1/75
(1) 2/70 (3)3 27 (6) 1 (4) 2 (7) 2 (7) 0 (0) 0 (0) 1/24 (4) 0/76
(0) 0 (0) 0/23 (0)4 23 (5) 1 (4) 3 (13) 0 (0) 1 (4) 0 (0) 2/21 (10)
0/19 (0) 1/20 (1) 0/20 (0)
a Percentages are shown in parentheses. If nothing else is
noted, the denominator is identical to the number of patients.
Mixed infections are included in this table.
TABLE 3. Proportion of disease of enteropathogens with
adjustedORs larger than unity in Danish cases of childhood
diarrheaa
Organism PAR%
Rotavirus..............................................................................................13.2Salmonella
sp.......................................................................................
4.6Norovirus
.............................................................................................
3.9
Adenovirus...........................................................................................
3.6Campylobacter
sp.................................................................................
2.9Y.
enterocolitica....................................................................................
2.2Sapovirus..............................................................................................
2.0STEC
....................................................................................................
2.0EPEC....................................................................................................
1.6EAggEC...............................................................................................
1.3
a Mixed infections are included in this table.
3638 OLESEN ET AL. J. CLIN. MICROBIOL.
-
7/27/2019 Etiologi Gea
5/7
also found to be the leading cause of diarrhea. A number
ofstudies have shown rotavirus to be a leading cause of
gastro-enteritis in children (14, 43). However, English (35), Dutch
(8),and Finnish (26) community studies found the percentage
at-tributable to norovirus to be clearly higher than in our
study,and this is also true for sapovirus (8). The Finnish
studyshowed that norovirus caused milder symptoms than
rotavirus,and thus parents of patients with norovirus infections
will beless likely to seek medical attention. Community studies
aretherefore expected to disclose a higher proportion of
norovirusthan studies involving patients admitted to hospitals or
seen bya physician. The fact that the stool suspensions in our
studyhad been frozen and thawed several times before being
tested
by RT-PCR may also have diminished the sensitivity of
thenorovirus and sapovirus detection. Similarly, astrovirus
causesmilder symptoms than other viruses tested for in the
Finnishstudy (26) and are therefore less likely to be detected
amongsamples from medical facilities. In addition, it has been
shownthat the sensitivity of the enzyme-linked immunosorbent
assayfor astrovirus used here is only 50 to 60% compared to
PCRtests used in other studies (41). With regard to bacterial
causes,our findings are in general agreement with previous
case-con-trol studies. However, in most studies (5, 8, 25, 35),
STEC wasisolated in 1% of cases versus 3% in the present study;
inItaly (5), 19% of stools from cases younger than 10 years oldwere
positive for Salmonella versus 5% in the present study.
FIG. 1. Bubble diagram showing the relative prevalence per month
of the most frequently occurring pathogens among cases.
TABLE 4. Selected clinical data of the most important causes of
gastroenteritis in Danish children under 5 years of agea
Organism No. ofpatients
No. of patients (%) with:Vomiting Bloody diarrhea Fever
Hospitalization Dehydrationb Loss of wt
Rotavirus 45 42 (93) 2 (4) 41 (91) 13 (29) 11 (24) 33
(73)Adenovirus 12 8 (67) 0 (0) 7 (58) 0 (0) 1 (8) 5/9 (56)Norovirus
10 8 (80) 1 (10) 7 (70) 2 (20) 2 (20) 6 (60)Sapovirus 10 6 (60) 0
(0) 5/9 (56) 2 (20) 1 (10) 6/9 (67)Salmonella sp. 19 9 (47) 5 (26)
17 (90) 5 (26) 5 (26) 14/18 (78)Campylobacter sp. 12 2 (17) 11 (92)
11 (92) 2 (17) 2 (17) 4/9 (44)Y. enterocolitica 10 3 (30) 2 (20) 8
(80) 1 (10) 0 (0) 5/9 (56)STEC 9 3 (33) 2 (22) 4 (44) 3 (33) 2 (22)
2 (22)EPEC 7 2 (29) 1 (14) 4 (57) 3 (43) 2 (29) 2/5 (20)No pathogen
183 71/181 (39) 11/181 (6) 99/177 (56) 23/182 (13) 23 (13) 67/158
(42)
a Percentages are shown in parentheses. Mixed and potentially
mixed infections (cases with a secondary bacterial pathogen
isolated within 30 days before and afterthe index pathogen) were
excluded. If nothing else is noted, the denominator is identical to
the number of patients.
b Patients who received treatment with oral or intravenous
fluid.
VOL. 43, 2005 DIARRHEA IN DANISH CHILDREN 3639
-
7/27/2019 Etiologi Gea
6/7
Surveillance data indicate that thermotolerant Campy-lobacter is
the most common bacterial gastrointestinal patho-gen for all ages
in Denmark (1). However, in the present studyof children younger
than 5 years, it was surpassed by Salmo-nella as the most common
bacterial pathogen. Y. enterocoliticawas isolated from 3% of
patients, indicating that this speciescontinues to be an important
pathogen in young children.
Several points of interest relate to diarrheagenic E. coli.Apart
from STEC, only eae gene-positive strains belonging tothe classical
EPEC serotypes were associated with diarrhea.A/EEC, i.e., E. coli
isolates harboring the eae gene but notproducing Shiga toxin or
belonging to the classical EPEC se-rotypes, was the most commonly
isolated potential pathogen inthe present study. However, A/EEC was
isolated at a similarproportion from cases and controls. The
presence of the geneencoding bundle-forming pilus, a recognized
EPEC virulencefactor (23), was neither alone nor in combination
with the eaegene associated with diarrhea (data not shown). Recent
studieshave applied a definition of EPEC where the serotype of
theinfecting strains is not taken into account (25, 27). Had we
defined EPEC by the presence of the eae gene in
stx-negativestrains, we would not have identified EPEC as a
diarrheagenicpathogen. It is, therefore, premature to define EPEC
indepen-dently of the serotype. Until virulence factors that may
becofactors for diarrhea in EPEC infections have been identified,we
recommend including the serotype or at least the O groupfor the
identification of EPEC in young children. ClassicalEPEC was only
isolated from children below 2 years of age andwas the second most
common bacterial pathogen in this agegroup, indicating that this
pathogen is an important cause ofsporadic diarrheal illness in
infants.
Eleven and five STEC strains were isolated from patientsand
controls, respectively. The serotypes O26:H, O103:H3
(both stx1 and eae positive), and O157:H7 (stx2 and eae
posi-tive) were found in both cases and controls. This is
interestingbecause these three serotypes are not only the most
commonbut also among the most virulent STEC types (36).
Althoughmost patients infected with STEC stop excreting the
organismshortly after the acute illness has passed, a substantial
propor-tion may continue to carry the organism for several
months(12, 36). This may partly explain the occurrence of these
patho-gens among the control children in the present study. Very
fewETEC, EAggEC, and EIEC were isolated. ETEC and EIECare
well-known pathogens, but they are uncommon in childrenfrom
industrialized countries. EAggEC was isolated more fre-quently from
cases than controls. However, this difference wasnot statistically
significant.
Parasitic infections were rare in the present study,
thoughcryptosporidia were isolated from 1.7% of cases. A small
num-ber of children were diagnosed with Giardia, explaining why
noassociation with diarrhea was found for this pathogen. In
gen-eral, infections with Giardia lamblia are a minor cause of
di-arrhea in Denmark. In 2004, the rate ofG. lamblia was 1.7%
insamples where examinations for parasites were requested by
aphysician (unpublished data [Maiken Arendrup, Laboratory
ofMycology and Parasitology, Statens Serum Institut, Copenha-gen,
Denmark]).
Only few cases in the present study (6.6%) acquired
theirinfections during foreign travel. Salmonella and EPEC werethe
most common travel related pathogens. Not surprisingly,
Cryptosporidium, ETEC, and EAggEC were also associatedwith
travel. Very few viruses were isolated from cases with atravel
history. In general, there were overlapping signs andsymptoms
between the different etiologic categories. Some typ-ical patterns
were, however, observed. Bloody diarrhea wasreported in 92% of the
Campylobactercases and 20 to 26% ofthe patients with Salmonella, Y.
enterocolitica, and STEC in-fections but rarely among the patients
with a viral infection. Asexpected, vomiting was a more prominent
finding among casesinfected with viruses than bacteria.
In conclusion, rotavirus was confirmed as the most
commonpathogen in childhood diarrhea, especially during winter
andspring in Denmark. This fact, in combination with the severityof
the infections, warrants consideration of a rotavirus vaccinein the
childhood immunization program. The role of diarrhea-genic E. coli
was confirmed for STEC and classical EPEC.A/EEC, i.e.,
attaching-and-effacing E. coli not belonging to theclassical EPEC
serotypes, was commonly identified but was notassociated with
disease. Parasites are only rarely identified inchildren with
diarrhea with the possible exception of patients
who have traveled abroad. Routine examination of stool cul-tures
from children less than 5 years of age should include testsfor
viruses in the colder months and for STEC and classicalEPEC.
Ideally, identification of STEC should be based ondetection of the
Shiga toxins or their genes. As for EPEC,routine examination may be
restricted to children below 2years of age but must include a
combination of detection of theeae gene and the serogroup of the
infecting strain.
ACKNOWLEDGMENTS
We are grateful to Carsten Struve and Andreas Munk Petersen
forhaving contributed to the data collection and to Brita Bruun for
criticalreading of the manuscript. We thank the staff of the
laboratories thattook part in the study.
REFERENCES
1. Anonymous. 2002. Annual Report on Zoonoses in Denmark 2001.
Ministryof Food, Agriculture, and Fisheries, Copenhagen,
Denmark.
2. Baudry, B., S. J. Savarino, P. Vial, J. B. Kaper, and M. M.
Levine. 1990. Asensitive and specific DNA probe to identify
enteroaggregative Escherichiacoli, a recently discovered diarrheal
pathogen. J. Infect. Dis. 161:12491251.
3. Bern, C., J. Z. I. de Martines, and R. I. Glass. 1992. The
magnitude of theglobal problem of diarrhoeal disease: a ten-year
update. Bull. W. H. O.70:705714.
4. Blom, M., A. Meyer, P. Gerner-Smidt, K. Gaarslev, and F.
Espersen. 1999.Evaluation of Statens Serum Institut enteric medium
for detection of entericpathogens. J. Clin. Microbiol.
37:23122316.
5. Caprioli, A., C. Pezzella, R. Morelli, A. Giammanco, S.
Arista, D. Crotti, M.Facchini, P. Guglielmetti, C. Piersimoni, I.
Luzzi, et al. 1996. Enteropatho-gens associated with childhood
diarrhea in Italy. Pediatr. Infect. Dis. J.15:876883.
6. Cravioto, A., R. J. Gross, S. M. Scotland, and B. Rowe. 1979.
An adhesive
factor found in strains ofEscherichia coli belonging to the
traditional infan-tile enteropathogenic serotypes. Curr. Microbiol.
3:9599.
7. Dennehy, P. H., S. M. Nelson, S. Spangenberger, J. S. Noel,
S. S. Monroe,and R. I. Glass. 2001. A prospective case-control
study of the role of astro-virus in acute diarrhea among
hospitalized young children. J. Infect. Dis.184:1015.
8. de Wit, M. A., M. P. Koopmans, L. M. Kortbeek, W. J. Wannet,
J. Vinje, F.van Leusden, A. I. Bartelds, and Y. T. van Duynhoven.
2001. Sensor, apopulation-based cohort study on gastroenteritis in
The Netherlands: inci-dence and etiology. Am. J. Epidemiol.
154:666674.
9. Donnenberg, M. S. 1995. Enteropathogenic Escherichia coli, p.
709726. InM. J. Blaser, P. D. Smith, J. I. Ravdin, H. B. Greenberg,
and R. L. Guerrant(ed.), Infections of the gastrointestinal tract.
Raven Press, Ltd., New York,N.Y.
10. Gomes, T. A., M. A. Vieira, I. K. Wachsmuth, P. A. Blake,
and L. R. Trabulsi.1989. Serotype-specific prevalence of
Escherichia coli strains with EPECadherence factor genes in infants
with and without diarrhea in Sao Paulo,Brazil. J. Infect. Dis.
160:131135.
3640 OLESEN ET AL. J. CLIN. MICROBIOL.
-
7/27/2019 Etiologi Gea
7/7
11. Hutchinson, D. N., and F. J. Bolton. 1984. Improved blood
free selectivemedium for the isolation of Campylobacter jejuni from
faecal specimens.J. Clin. Pathol. 37:956957.
12. Jensen, C., P. Schiellerup, K. E. P. Olsen, F. Scheutz, E.
Petersen, P.Gerner-Smidt, and K. Molbak. Antimicrobial treatment of
asymptomaticcarriers of verocytotoxin-producing Escherichia coli:
an empiric study. Scand.J. Infect. Dis. 37:6163.
13. Jerse, A. E., J. Yu, B. D. Tall, and J. B. Kaper. 1990. A
genetic locus ofenteropathogenic Escherichia coli necessary for the
production of attaching
and effacing lesions on tissue culture cells. Proc. Natl. Acad.
Sci. USA87:78397843.14. Kapikan, A., Y. Hoshino, and R. M. Chanock.
2001. Rotaviruses, p. 1787
1834. In D. M. Knipe and M. J. Hudson (ed.), Fields virology.
Lippincott/TheWilliams & Wilkins Co., Philadelphia, Pa.
15. Kjaeldgaard, P., B. Nissen, N. Lange, and H. Laursen. 1986.
Evaluation ofMinibact, a new system for rapid identification of
Enterobacteriaceae: com-parison of Minibact, Micro-ID, and API 20E
with a conventional method asreference. Acta Pathol. Microbiol.
Immunol. Scand. B 94:5761.
16. Knutton, S., T. Baldwin, P. H. Williams, and A. S. McNeish.
1989. Actinaccumulation at sites of bacterial adhesion to tissue
culture cells: basis of anew diagnostic test for enteropathogenic
and enterohemorrhagic Escherichiacoli. Infect. Immun.
57:12901298.
17. Knutton, S., A. D. Phillips, H. R. Smith, R. J. Gross, R.
Shaw, P. Watson,and E. Price. 1991. Screening for enteropathogenic
Escherichia coli in infantswith diarrhea by the fluorescent-actin
staining test. Infect. Immun. 59:365371.
18. Konowalchuk, J., J. I. Speirs, and S. Stavric. 1977. Vero
response to a
cytotoxin of Escherichia coli. Infect. Immun.18:
775779.19. Lautrop, H., N. Hiby, A. Bremmelgaard, and B.
Korsager. 1979. Bakteri-ologiske undersgelsesmetoder. FADLs Forlag,
Copenhagen, Denmark.
20. Levine, M. M., and R. Edelman. 1984. Enteropathogenic
Escherichia coli ofclassic serotypes associated with infant
diarrhea: epidemiology and patho-genesis. Epidemiol. Rev.
6:3151.
21. Levine, M. M., J. P. Nataro, H. Karch, M. M. Baldini, J. B.
Kaper, R. E.Black, M. L. Clements, and A. D. OBrien. 1985. The
diarrheal response ofhumans to some classic serotypes of
enteropathogenic Escherichia coli isdependent on a plasmid encoding
an enteroadhesiveness factor. J. Infect.Dis. 152:550559.
22. Miettinen, O. S. 1974. Proportion of disease caused or
prevented by a givenexposure, trait, or intervention. Am. J.
Epidemiol. 99:325332.
23. Nataro, J. P., and J. B. Kaper. 1998. Diarrheagenic
Escherichia coli. Clin.Microbiol. Rev. 11:142201.
24. rskov, F., and I. rskov. 1984. Serotyping of Escherichia
coli. MethodsMicrobiol. 14:43112.
25. Pabst, W. L., M. Altwegg, C. Kind, S. Mirjanic, D.
Hardegger, and D. Nadal.2003. Prevalence of enteroaggregative
Escherichia coli among children withand without diarrhea in
Switzerland. J. Clin. Microbiol. 41:22892293.
26. Pang, X. L., S. Honma, S. Nakata, and T. Vesikari. 2000.
Human calicivi-ruses in acute gastroenteritis of young children in
the community. J. Infect.Dis. 181(Suppl. 2):S288S294.
27. Rademaker, C. M., A. C. Fluit, M. Jansze, W. H. Jansen, J.
H. Glerum, andJ. Verhoef. 1993. Frequency of enterovirulent
Escherichia coli in diarrhoealdisease in The Netherlands. Eur. J.
Clin. Microbiol. Infect. Dis. 12:9397.
28. Robins-Browne, R. M. 1987. Traditional enteropathogenic
Escherichia coli ofinfantile diarrhea. Rev. Infect. Dis.
9:2853.
29. Scaletsky, I. C., M. L. Silva, M. R. Toledo, B. R. Davis, P.
A. Blake, and L. R.
Trabulsi. 1985. Correlation between adherence to HeLa cells and
sero-groups, serotypes, and bioserotypes of Escherichia coli.
Infect. Immun. 49:528532.
30. Scotland, S. M., H. R. Smith, T. Cheasty, B. Said, G. A.
Willshaw, N. Stokes,and B. Rowe. 1996. Use of gene probes and
adhesion tests to characteriseEscherichia coli belonging to
enteropathogenic serogroups isolated in theUnited Kingdom. J. Med.
Microbiol. 44:438443.
31. Scotland, S. M., G. A. Willshaw, T. Cheasty, and B. Rowe.
1992. Strains ofEscherichia coli O157:H8 from human diarrhoea
belong to attaching and
effacing class of E. coli. J. Clin. Pathol. 45:10751078.32.
Scotland, S. M., G. A. Willshaw, H. R. Smith, R. J. Gross, and B.
Rowe. 1989.Adhesion to cells in culture and plasmid profiles of
enteropathogenic Esch-erichia coli isolated from outbreaks and
sporadic cases of infant diarrhoea.J. Infect. 19:237249.
33. Sommerfelt, H., K. H. Kalland, P. Raj, S. L. Moseley, M. K.
Bhan, and B.Bjorvatn. 1988. Cloned polynucleotide and synthetic
oligonucleotide probesused in colony hybridization are equally
efficient in the identification ofenterotoxigenic Escherichia coli.
J. Clin. Microbiol. 26:22752278.
34. Thomas, A., H. R. Smith, G. A. Willshaw, and B. Rowe. 1991.
Non-radioac-tively labeled polynucleotide and oligonucleotide DNA
probes, for selec-tively detecting Escherichia coli strains
producing Vero cytotoxins VT1, VT2and VT2 variant. Mol. Cell Probes
5:129135.
35. Tompkins, D. S., M. J. Hudson, H. R. Smith, R. P. Eglin, J.
G. Wheeler,M. M. Brett, R. J. Owen, J. S. Brazier, P. Cumberland,
V. King, and P. E.Cook. 1999. A study of infectious intestinal
disease in England: microbio-logical findings in cases and
controls. Commun. Dis. Public Health 2:108113.
36.Tozzi, A. E., S. Goriette, and A. Caprioli.
2001. Epidemiology of humaninfections by Escherichia coli O157
and other verocytotoxin-producing E.coli, p. 113148. In G. Duffy,
P. Garvey, and D. A. McDowell (ed.), Vero-cytotoxigenic E. coli.
Food & Nutrition Press, Inc., Trumbull, Conn.
37. Venkatesan, M. M., J. M. Buysse, and D. J. Kopecko. 1989.
Use of Shigellaflexneri ipaC and ipaH gene sequences for the
general identification ofShigella spp. and enteroinvasive
Escherichia coli. J. Clin. Microbiol. 27:26872691.
38. Vila, J., A. Gene, M. Vargas, J. Gascon, C. Latorre, and M.
T. Jimenez deAnta. 1998. A case-control study of diarrhoea in
children caused by Esche-richia coli producing heat-stable
enterotoxin (EAST-1). J. Med. Microbiol.47:889891.
39. Vinje, J., H. Deijl, H. R. van der, D. Lewis, K. O. Hedlund,
L. Svensson, andM. P. Koopmans. 2000. Molecular detection and
epidemiology of Sapporo-like viruses. J. Clin. Microbiol.
38:530536.
40. Vinje, J., and M. P. Koopmans. 1996. Molecular detection and
epidemiologyof small round-structured viruses in outbreaks of
gastroenteritis in TheNetherlands. J. Infect. Dis. 174:610615.
41. Walter, J. E., and D. K. Mitchell. 2003. Astrovirus
infection in children. Curr.Opin. Infect. Dis. 16:247253.
42. Wheeler, J. G., D. Sethi, J. M. Cowden, P. G. Wall, L. C.
Rodrigues, D. S.Tompkins, M. J. Hudson, P. J. Roderick, et al.
1999. Study of infectiousintestinal disease in England: rates in
the community, presenting to generalpractice, and reported to
national surveillance. BMJ 318:10461050.
43. Wilhelmi, I., E. Roman, and A. Sanchez-Fauquier. 2003.
Viruses causinggastroenteritis. Clin. Microbiol. Infect.
9:247262.
44. Willshaw, G. A., H. R. Smith, S. M. Scotland, and B. Rowe.
1985. Cloning ofgenes determining the production of Vero cytotoxin
by Escherichia coli.J. Gen. Microbiol. 131(Pt. 11):30473053.
VOL. 43, 2005 DIARRHEA IN DANISH CHILDREN 3641