Embed Size (px)
Citation preview
Farnesoid-X Receptor Agonists: a New Class of Drugs for the Treatment of PBC? An
International Study Evaluating the Addition of Obeticholic Acid (INT-747) to Ursodeoxycholic
Acid An International Study
Andrew Mason, Velimir Luketic, Keith Lindor, Gideon Hirschfield, Stuart Gordon, Marlyn Mayo, Kris Kowdley, Albert Parés, Michael Trauner, Erin
Castelloe, Cathi Sciacca, Tessa Beecher Jones, Mark Pruzanski, David Shapiro
For the Obeticholic Acid [INT‐747] PBC Investigator Group
U. Alberta, Virginia Commonwealth U., Mayo Clinic, U. Toronto, Henry Ford Clinic, U. Texas SW, Virginia Mason Med Center, U. Barcelona, U. Graz, Intercept
Pharmaceuticals.
Disclosure/Conflict of Interest Statement
I have financial relationship(s) within the last 12 months relevant to my presentation:
Full Time Employee with Intercept Pharmaceuticals, Inc.
ANDMy presentation focuses on the investigational use
of:Obeticholic Acid and Placebo
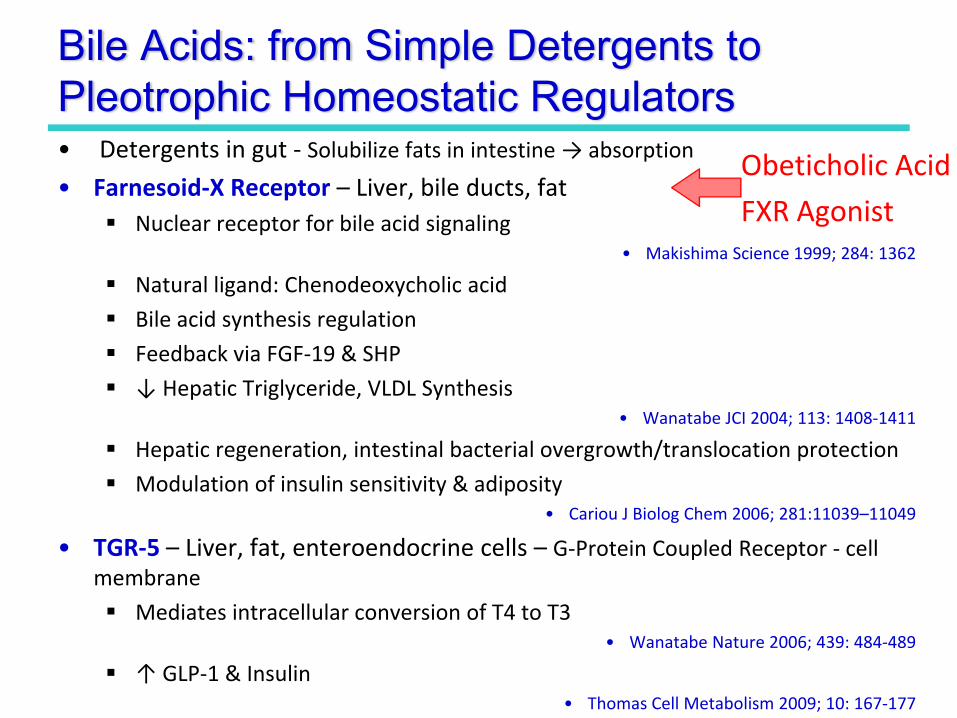
Bile Acids: from Simple Detergents to Pleotrophic Homeostatic Regulators• Detergents in gut ‐ Solubilize fats in intestine → absorption
• Farnesoid‐X Receptor – Liver, bile ducts, fatNuclear receptor for bile acid signaling
• Makishima Science 1999; 284: 1362
Natural ligand: Chenodeoxycholic acid
Bile acid synthesis regulation
Feedback via FGF‐19 & SHP
↓ Hepatic Triglyceride, VLDL Synthesis• Wanatabe JCI 2004; 113: 1408‐1411
Hepatic regeneration, intestinal bacterial overgrowth/translocation protection
Modulation of insulin sensitivity & adiposity• Cariou J Biolog Chem 2006; 281:11039–11049
• TGR‐5 – Liver, fat, enteroendocrine cells – G‐Protein Coupled Receptor ‐ cell membrane
Mediates intracellular conversion of T4 to T3• Wanatabe Nature 2006; 439: 484‐489
↑ GLP‐1 & Insulin• Thomas Cell Metabolism 2009; 10: 167‐177
Obeticholic Acid
FXR Agonist
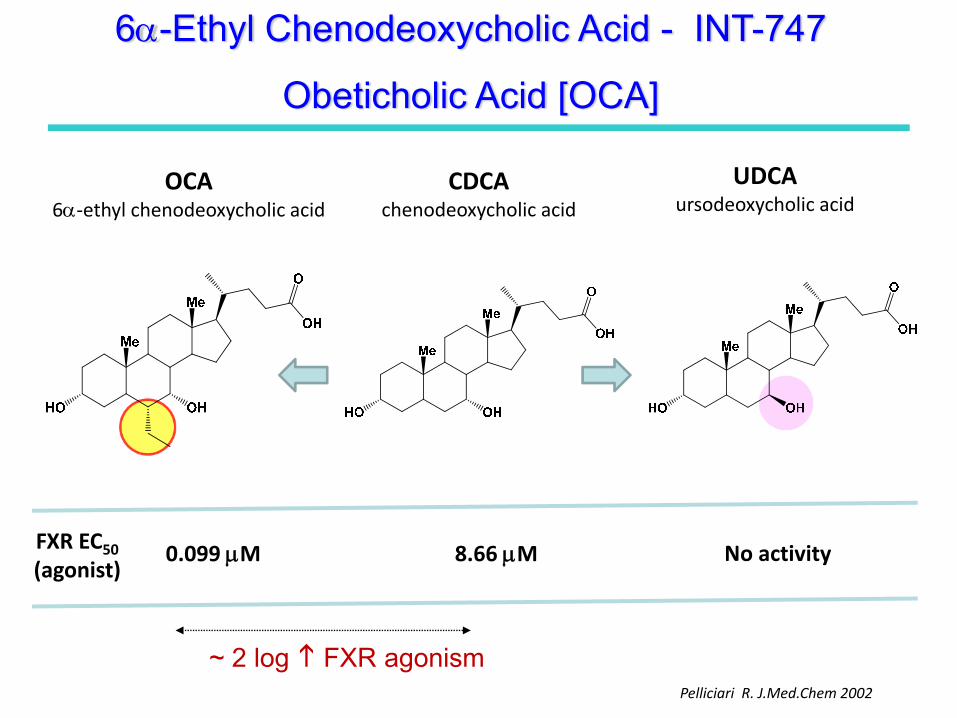
OCA6α‐ethyl chenodeoxycholic acid
CDCAchenodeoxycholic acid
UDCAursodeoxycholic acid
FXR EC50(agonist)
0.099 μM 8.66 μM No activity
Pelliciari R. J.Med.Chem 2002
~ 2 log FXR agonism
6α-Ethyl Chenodeoxycholic Acid - INT-747
Obeticholic Acid [OCA]
6α-Ethyl Chenodeoxycholic Acid - INT-747
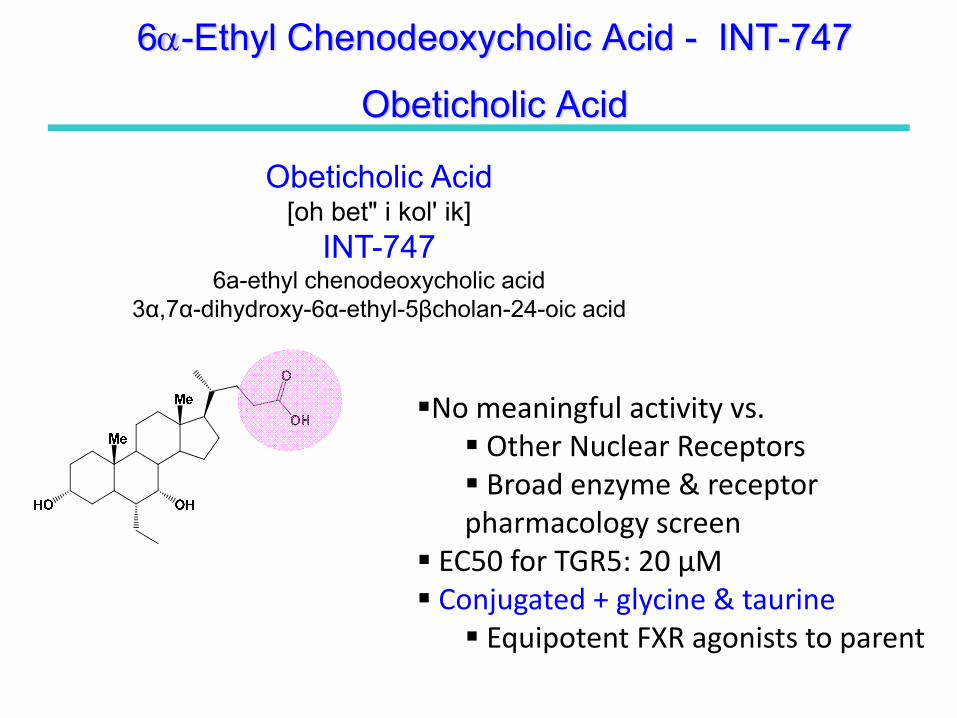
Obeticholic Acid
Obeticholic Acid [oh bet" i kol' ik]
INT-7476a-ethyl chenodeoxycholic acid
3α,7α-dihydroxy-6α-ethyl-5βcholan-24-oic acid
No meaningful activity vs. Other Nuclear ReceptorsBroad enzyme & receptor
pharmacology screen EC50 for TGR5: 20 µMConjugated + glycine & taurine
Equipotent FXR agonists to parent
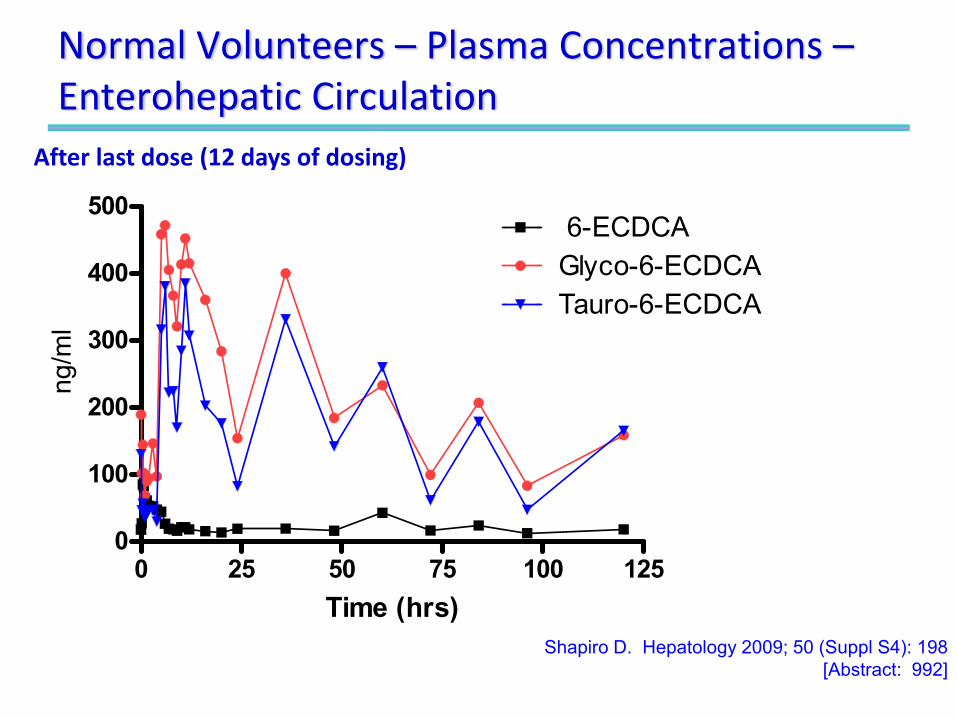
Normal Volunteers – Plasma Concentrations –Enterohepatic Circulation
0 25 50 75 100 1250
100
200
300
400
500
Glyco-6-ECDCATauro-6-ECDCA
6-ECDCA
Time (hrs)
ng/m
l
After last dose (12 days of dosing)
Shapiro D. Hepatology 2009; 50 (Suppl S4): 198 [Abstract: 992]
Preclinical Studies Overview• Numerous animal models evaluated
BDL, estrogen, lithocholic acid, CCl4, ANIT, thioacetamide injuryEffects consistent with FXR agonism• Induced FXR target genes • SHP induction and Cyp7α1 and Cyp8β1 repression
• Cholerectic• Anti‐fibrotic
Changes in α1 collagen, αSMA, TGFβ1, MMP‐2, TIMP‐1, and TIMP‐2Histology ‐ fibrosis, reversal of cirrhosis, Portal hypertension
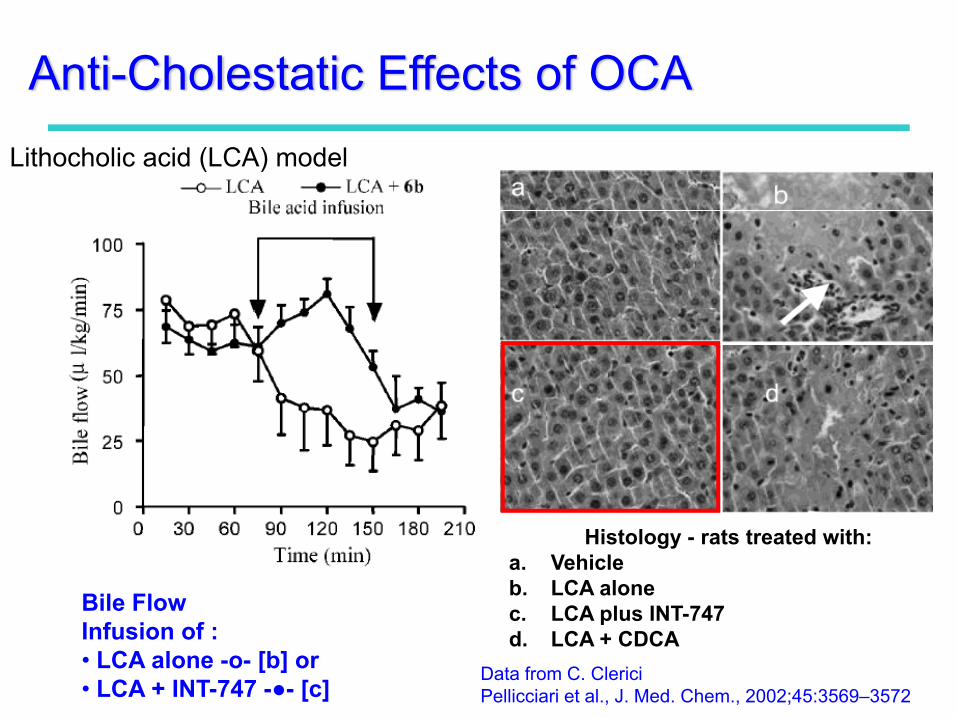
Histology - rats treated with:a. Vehicleb. LCA alonec. LCA plus INT-747d. LCA + CDCA
Bile Flow Infusion of :• LCA alone -o- [b] or • LCA + INT-747 -●- [c]
Data from C. Clerici Pellicciari et al., J. Med. Chem., 2002;45:3569–3572
Anti-Cholestatic Effects of OCALithocholic acid (LCA) model
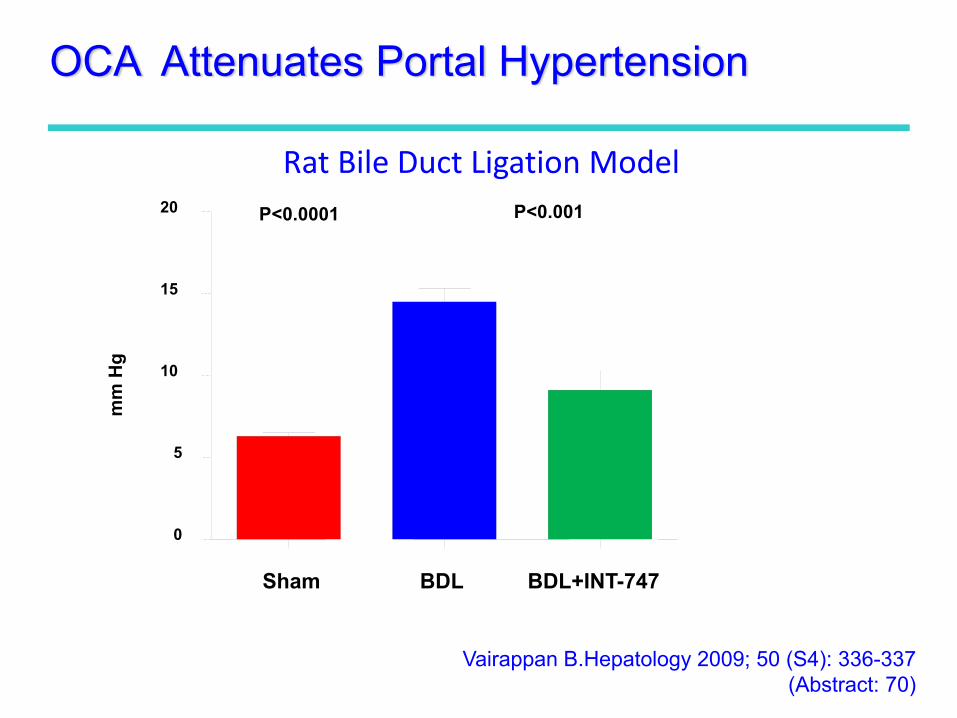
Vairappan B.Hepatology 2009; 50 (S4): 336-337 (Abstract: 70)
Sham BDL BDL+INT-747
0
5
10
15
20
mm
Hg
P<0.0001 P<0.001
Rat Bile Duct Ligation Model
OCA Attenuates Portal Hypertension
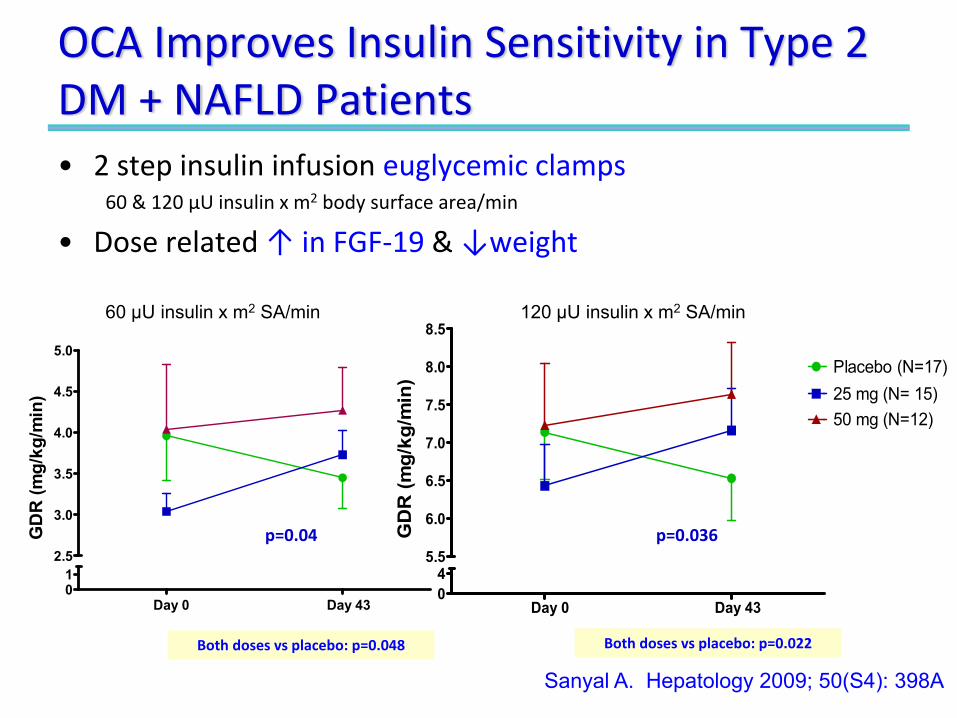
OCA Improves Insulin Sensitivity in Type 2 DM + NAFLD Patients• 2 step insulin infusion euglycemic clamps
60 & 120 µU insulin x m2 body surface area/min
• Dose related ↑ in FGF‐19 & ↓weight
Day 0 Day 4301
2.5
3.0
3.5
4.0
4.5
5.0
GD
R (m
g/kg
/min
)
Day 0 Day 4304
5.5
6.0
6.5
7.0
7.5
8.0
8.5
Placebo (N=17)25 mg (N= 15)50 mg (N=12)
GD
R (m
g/kg
/min
)
Sanyal A. Hepatology 2009; 50(S4): 398A
p=0.04
Both doses vs placebo: p=0.048 Both doses vs placebo: p=0.022
p=0.036
60 µU insulin x m2 SA/min 120 µU insulin x m2 SA/min
PBC Ongoing Medical Needs
• Ursodeoxycholic AcidOnly approved drug for PBC
Therapy has had a clear impact on PBC
But significant proportion of patients have an inadequate response & need better therapy
• Many drugs evaluated, none clearly effective
Poupon R, J Hepatol 2010 52:745-758Silveira M, Lindor K, Clin Liver Dis 2008; 12: 425-443
Kaplan N, Gershwin, E N Engl J Med 2005;353:1261-73
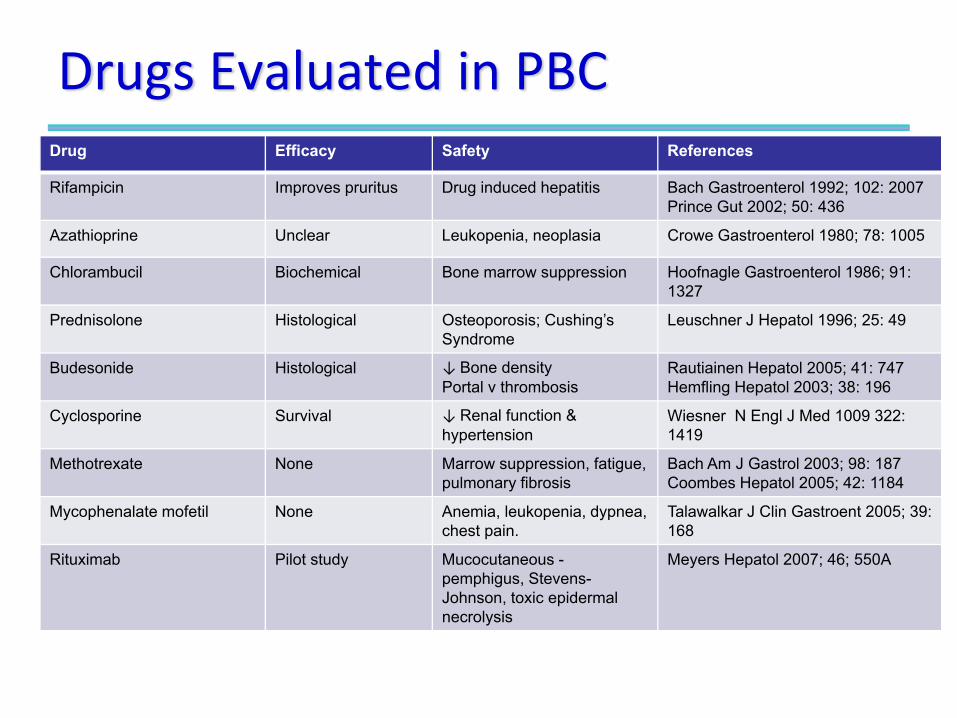
Drugs Evaluated in PBCDrug Efficacy Safety References
Rifampicin Improves pruritus Drug induced hepatitis Bach Gastroenterol 1992; 102: 2007Prince Gut 2002; 50: 436
Azathioprine Unclear Leukopenia, neoplasia Crowe Gastroenterol 1980; 78: 1005
Chlorambucil Biochemical Bone marrow suppression Hoofnagle Gastroenterol 1986; 91: 1327
Prednisolone Histological Osteoporosis; Cushing’s Syndrome
Leuschner J Hepatol 1996; 25: 49
Budesonide Histological ↓ Bone density Portal v thrombosis
Rautiainen Hepatol 2005; 41: 747Hemfling Hepatol 2003; 38: 196
Cyclosporine Survival ↓ Renal function & hypertension
Wiesner N Engl J Med 1009 322: 1419
Methotrexate None Marrow suppression, fatigue, pulmonary fibrosis
Bach Am J Gastrol 2003; 98: 187Coombes Hepatol 2005; 42: 1184
Mycophenalate mofetil None Anemia, leukopenia, dypnea, chest pain.
Talawalkar J Clin Gastroent 2005; 39: 168
Rituximab Pilot study Mucocutaneous -pemphigus, Stevens-Johnson, toxic epidermal necrolysis
Meyers Hepatol 2007; 46; 550A
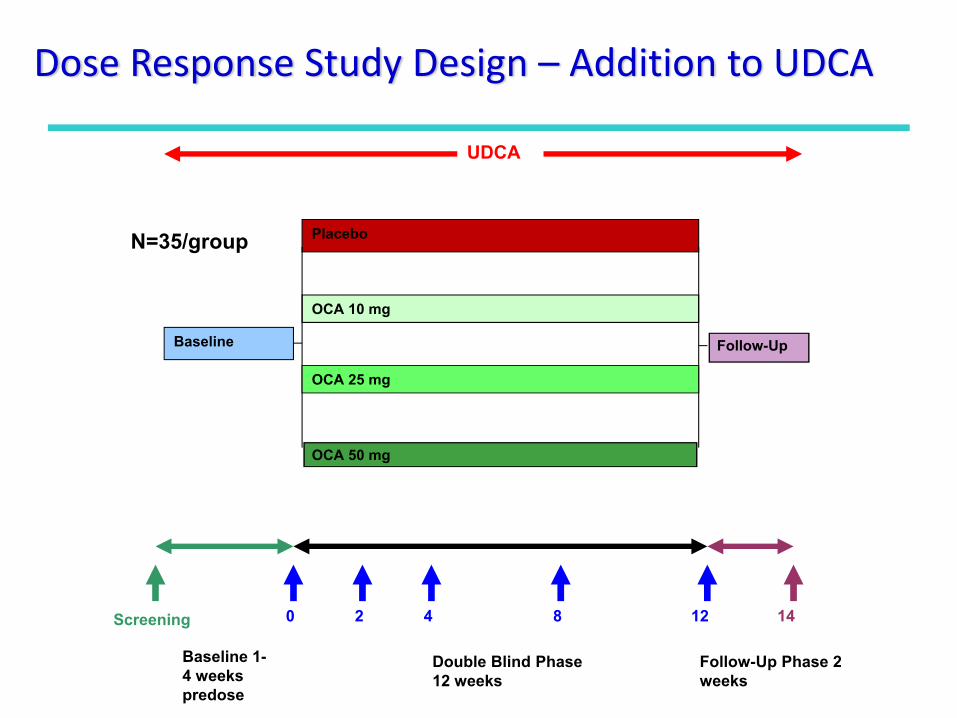
Screening
Baseline 1-4 weeks predose
Double Blind Phase 12 weeks
Follow-Up Phase 2 weeks
Placebo
OCA 10 mg
OCA 50 mg
0 2 4 8 12 14
N=35/group
Baseline Follow-Up
UDCA
OCA 25 mg
Dose Response Study Design – Addition to UDCA
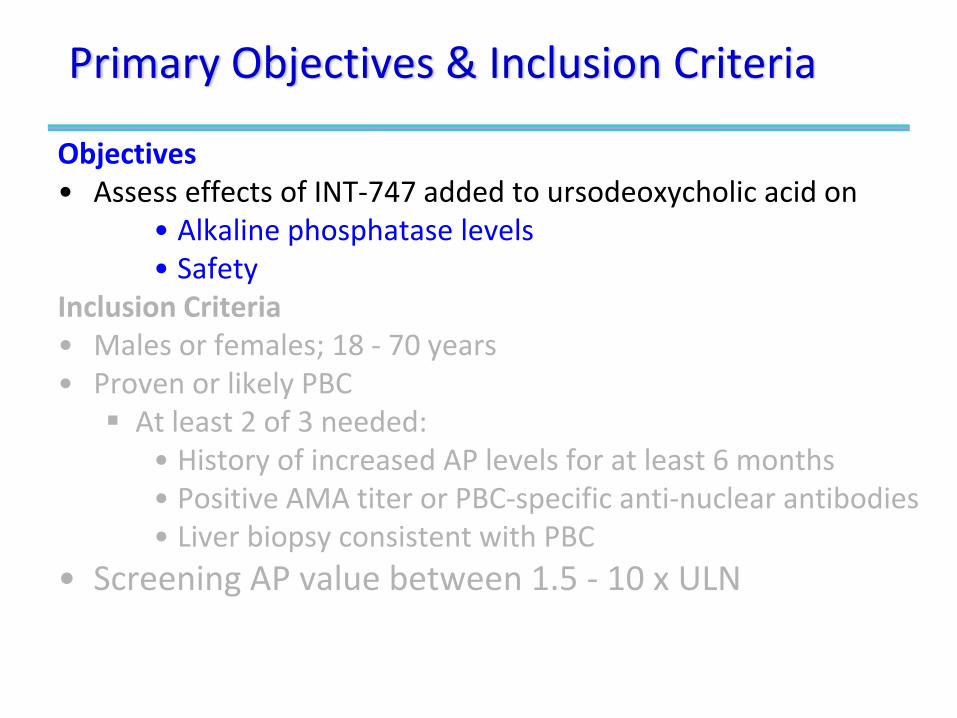
Primary Objectives & Inclusion Criteria
Objectives• Assess effects of INT‐747 added to ursodeoxycholic acid on
• Alkaline phosphatase levels• Safety
Inclusion Criteria• Males or females; 18 ‐ 70 years• Proven or likely PBC
At least 2 of 3 needed:• History of increased AP levels for at least 6 months• Positive AMA titer or PBC‐specific anti‐nuclear antibodies• Liver biopsy consistent with PBC
• Screening AP value between 1.5 ‐ 10 x ULN
Primary Objectives & Inclusion Criteria
Objectives• Assess effects of INT‐747 added to ursodeoxycholic acid on
• Alkaline phosphatase levels• Safety
Inclusion Criteria• Males or females; 18 ‐ 70 yrs• Proven or likely PBC
At least 2 of 3 needed:• History of increased AP levels for at least 6 months• Positive AMA titer or PBC‐specific anti‐nuclear antibodies• Liver biopsy consistent with PBC
• Alkaline Phosphatase: 1.5 ‐ 10 x ULN
Key Medical Exclusion Criteria• Specific drugs in 3 months before screening:
Colchicine, methotrexate, azathioprine, or systemic corticosteroids.
• History or presence of hepatic decompensation (e.g., varicealbleeds, encephalopathy or poorly controlled ascites)
• Screening conjugated bilirubin >2 x ULN• Screening ALT or AST value >5 x ULN• Screening serum creatinine value >1.5 mg/dL (133µmol/L)• Other concomitant liver diseases (HCV, HBV) infection, PSC
and/or other autoimmune liver disease• Pregnancy
Study Centers
•8 Countries, 33 Centers
•165 patients enrolled
•Geography• USA: 56%
• Canada: 26%
• Europe: 18%
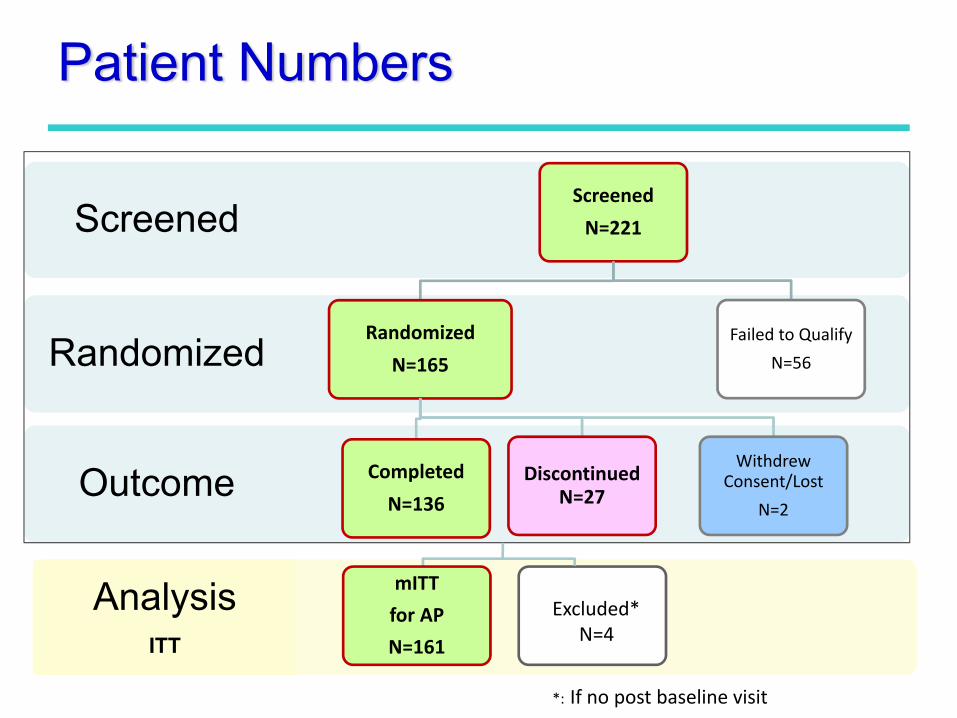
Patient Numbers
Outcome
Randomized
ScreenedScreened
N=221
Randomized
N=165
Completed
N=136Discontinued
N=27
Withdrew Consent/Lost
N=2
Failed to Qualify
N=56
AnalysisITT
mITT
for AP
N=161
Excluded*N=4
*: If no post baseline visit
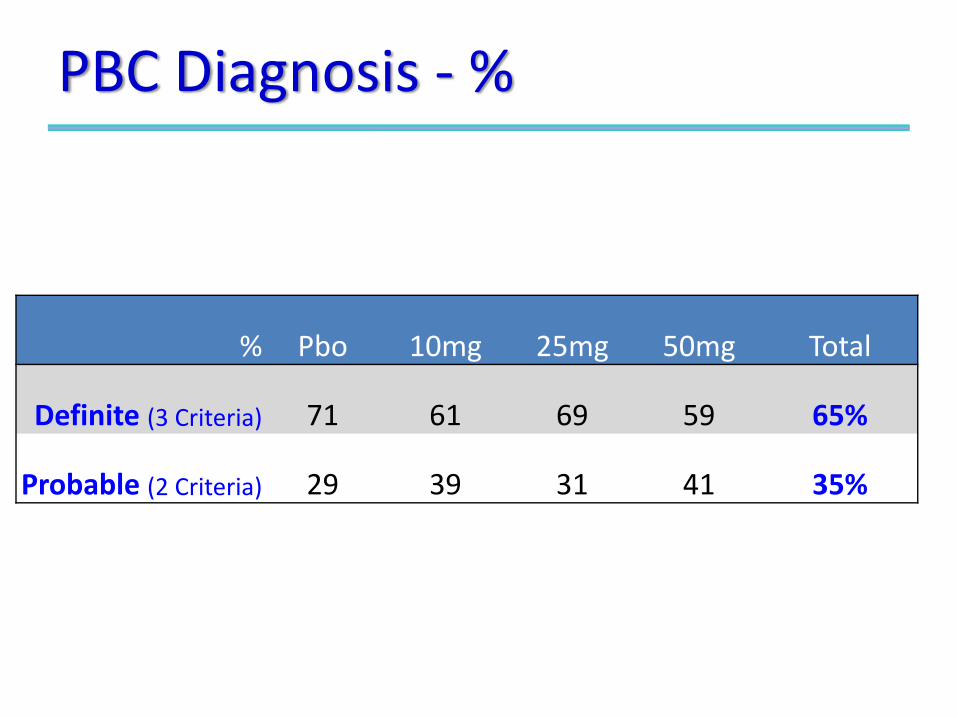
PBC Diagnosis ‐ %
% Pbo 10mg 25mg 50mg Total
Definite (3 Criteria) 71 61 69 59 65%
Probable (2 Criteria) 29 39 31 41 35%
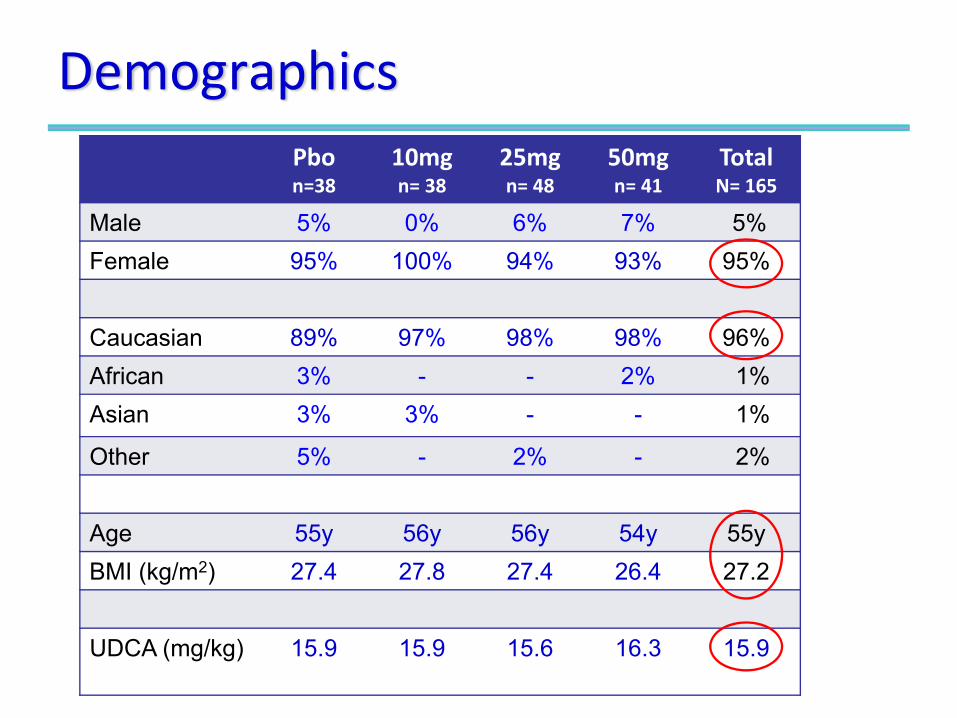
DemographicsPbon=38
10mgn= 38
25mgn= 48
50mgn= 41
TotalN= 165
Male 5% 0% 6% 7% 5%Female 95% 100% 94% 93% 95%
Caucasian 89% 97% 98% 98% 96%African 3% - - 2% 1%Asian 3% 3% - - 1%
Other 5% - 2% - 2%
Age 55y 56y 56y 54y 55yBMI (kg/m2) 27.4 27.8 27.4 26.4 27.2
UDCA (mg/kg) 15.9 15.9 15.6 16.3 15.9
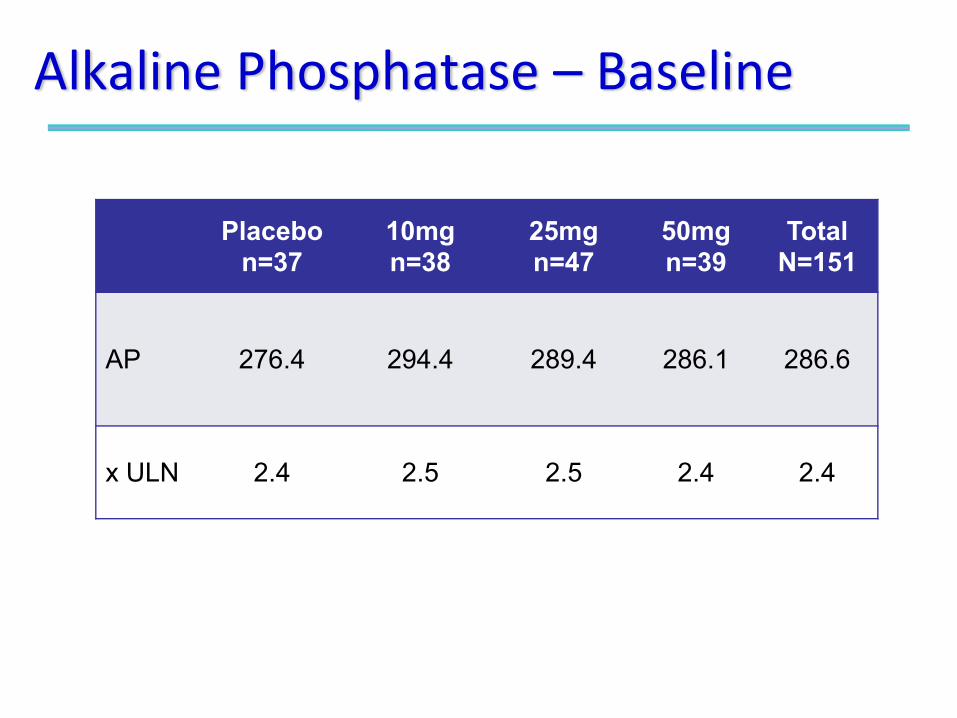
Alkaline Phosphatase – Baseline
Placebon=37
10mgn=38
25mgn=47
50mgn=39
TotalN=151
AP 276.4 294.4 289.4 286.1 286.6
x ULN 2.4 2.5 2.5 2.4 2.4
RESULTS
‐ Efficacy: Alkaline Phosphatase
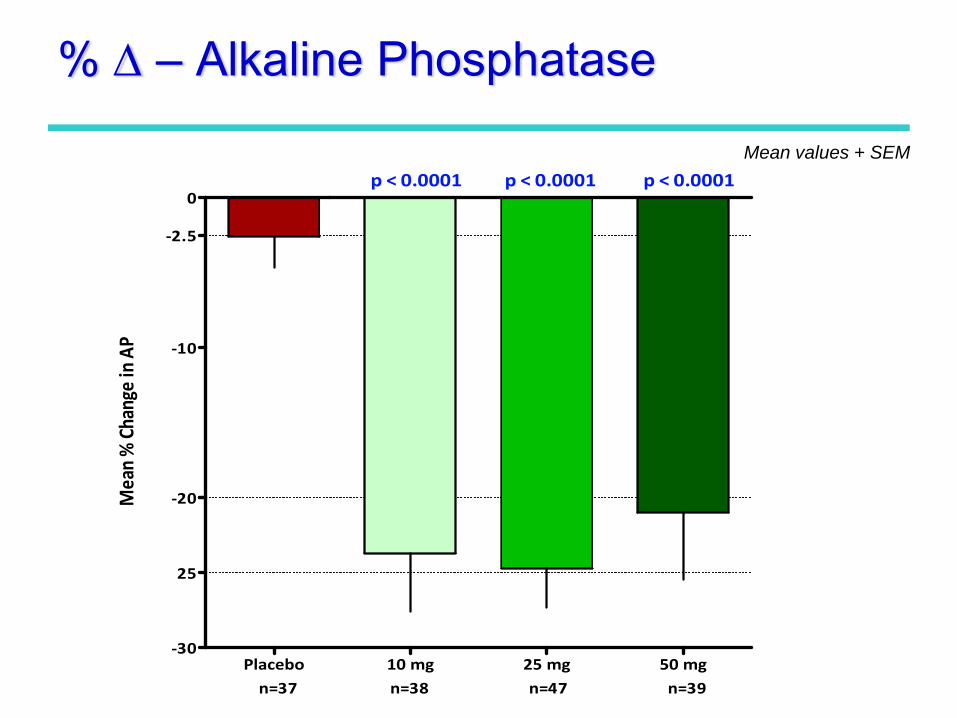
Placebo 10 mg 25 mg 50 mg‐30
‐20
‐10
0
n=37 n=38 n=47 n=39
p < 0.0001 p < 0.0001 p < 0.0001
25
‐2.5
Mean % Change in AP
% Δ – Alkaline Phosphatase
Mean values + SEM
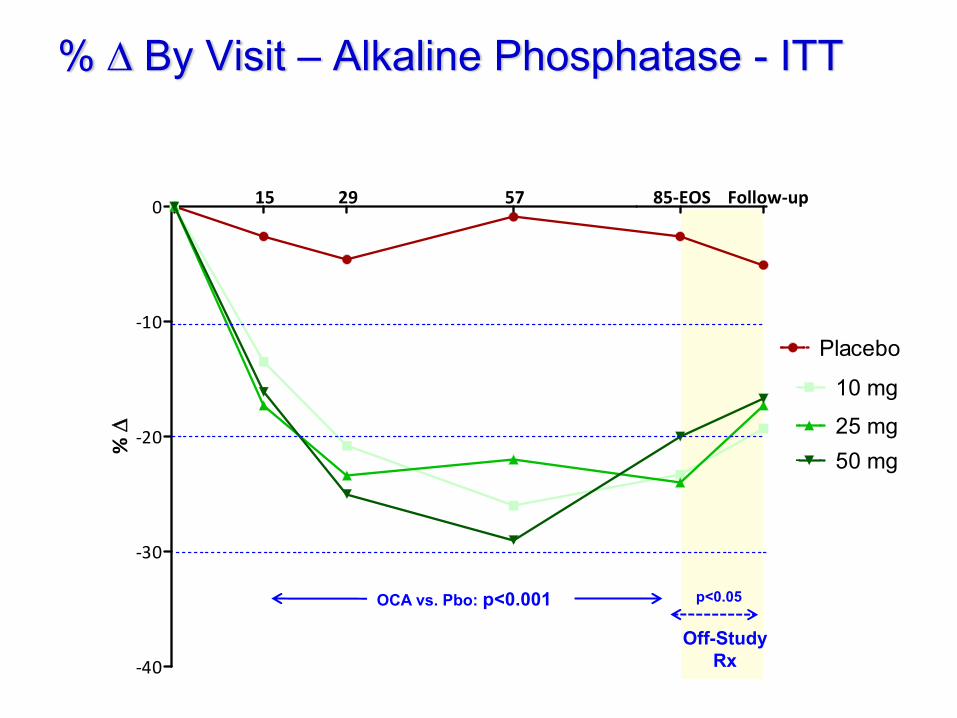
15 29 57 85‐EOS Follow‐up
‐40
‐30
‐20
‐10
0
Placebo
10 mg
25 mg50 mg%
Δ
% Δ By Visit – Alkaline Phosphatase - ITT
Off-StudyRx
OCA vs. Pbo: p<0.001 p<0.05
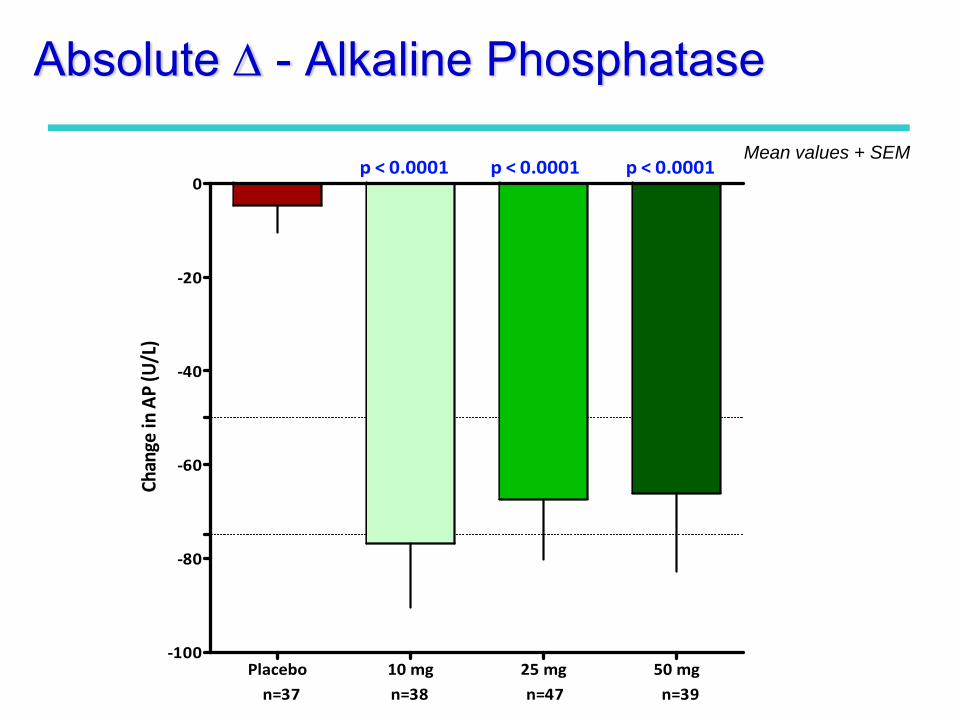
Placebo 10 mg 25 mg 50 mg‐100
‐80
‐60
‐40
‐20
0
n=37 n=38 n=47 n=39
p < 0.0001 p < 0.0001 p < 0.0001Ch
ange
in AP (U/L)
Absolute Δ - Alkaline Phosphatase
Mean values + SEM
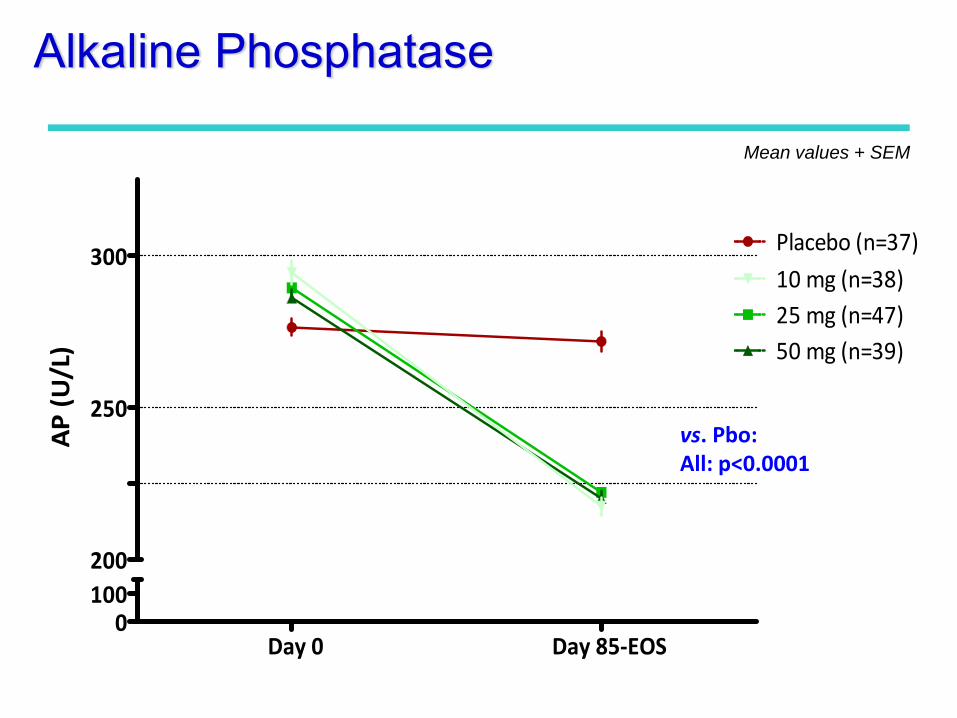
Day 0 Day 85‐EOS0
100200
250
300 Placebo (n=37)
25 mg (n=47)50 mg (n=39)
10 mg (n=38)
AP (U/L)
Alkaline Phosphatase
Mean values + SEM
vs. Pbo:All: p<0.0001
RESULTS
Liver Enzymes
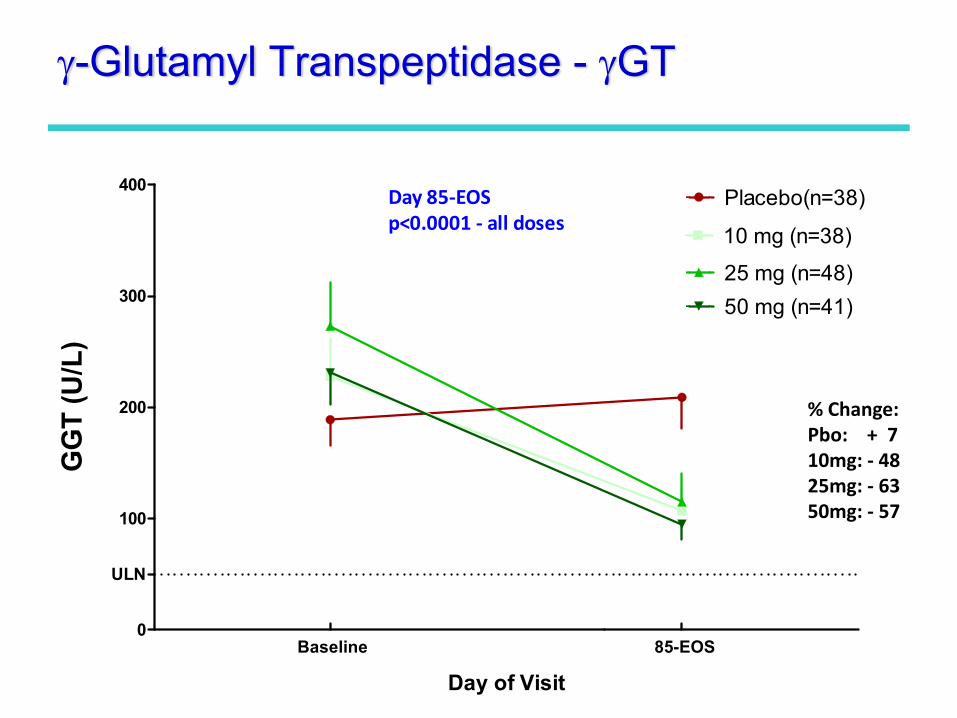
Baseline 85-EOS0
100
200
300
400Placebo(n=38)
10 mg (n=38)
25 mg (n=48)50 mg (n=41)
ULN
Day 85‐EOSp<0.0001 ‐ all doses
Day of Visit
GG
T (U
/L)
γ-Glutamyl Transpeptidase - γGT
% Change: Pbo: + 710mg: ‐ 4825mg: ‐ 6350mg: ‐ 57
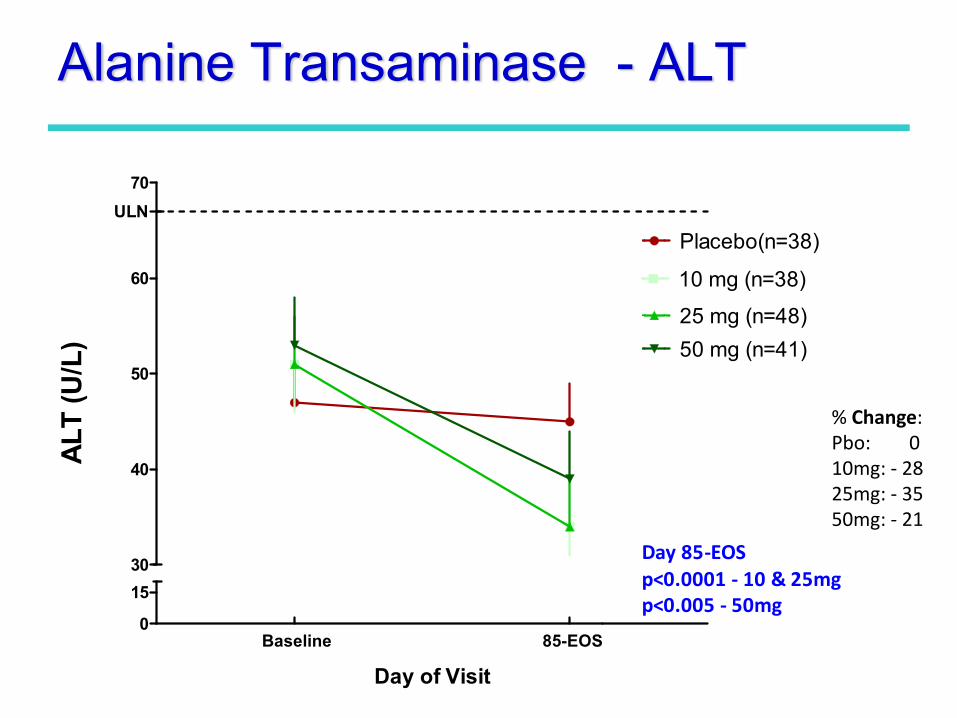
Baseline 85-EOS0
1530
40
50
60
70
Placebo(n=38)
10 mg (n=38)
25 mg (n=48)50 mg (n=41)
ULN
Day 85‐EOSp<0.0001 ‐ 10 & 25mgp<0.005 ‐ 50mg
Day of Visit
ALT
(U/L
)Alanine Transaminase - ALT
% Change: Pbo: 010mg: ‐ 2825mg: ‐ 3550mg: ‐ 21
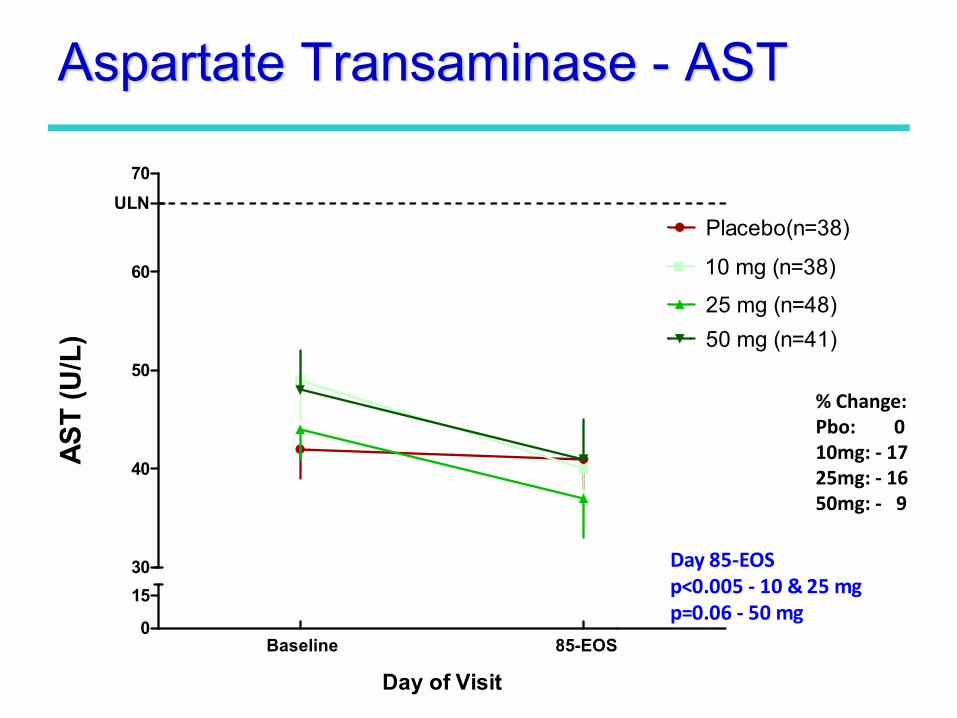
Aspartate Transaminase - AST
% Change: Pbo: 010mg: ‐ 1725mg: ‐ 1650mg: ‐ 9
Baseline 85-EOS0
1530
40
50
60
70
Placebo(n=38)
10 mg (n=38)
25 mg (n=48)50 mg (n=41)
ULN
Day 85‐EOSp<0.005 ‐ 10 & 25 mgp=0.06 ‐ 50 mg
Day of Visit
AST
(U/L
)
Safety & Tolerability
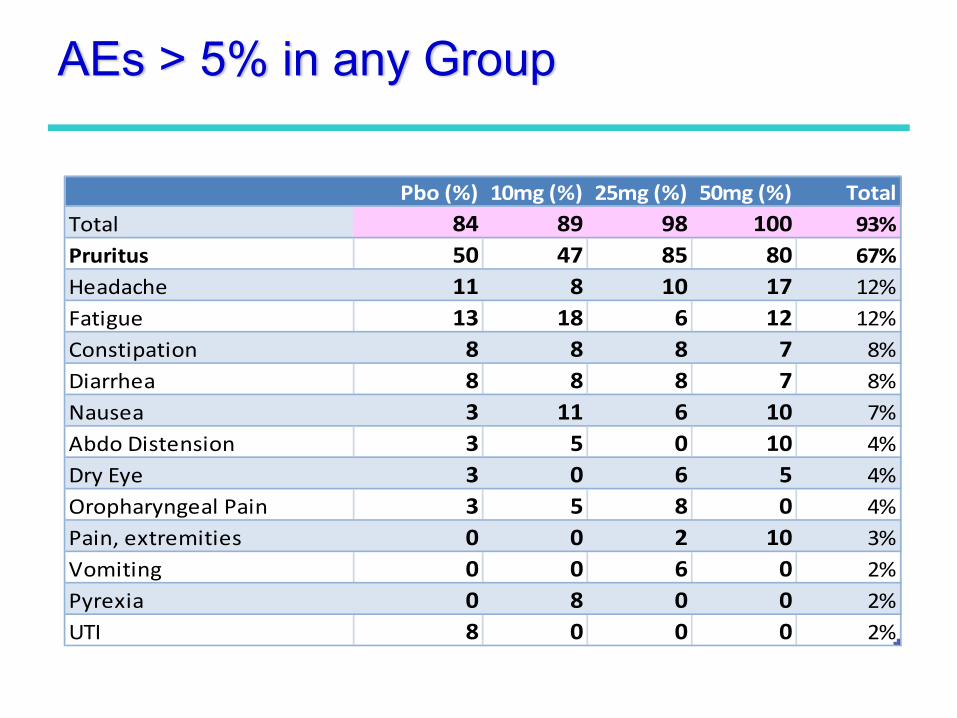
Pbo (%) 10mg (%) 25mg (%) 50mg (%) TotalTotal 84 89 98 100 93%Pruritus 50 47 85 80 67%Headache 11 8 10 17 12%Fatigue 13 18 6 12 12%Constipation 8 8 8 7 8%Diarrhea 8 8 8 7 8%Nausea 3 11 6 10 7%Abdo Distension 3 5 0 10 4%Dry Eye 3 0 6 5 4%Oropharyngeal Pain 3 5 8 0 4%Pain, extremities 0 0 2 10 3%Vomiting 0 0 6 0 2%Pyrexia 0 8 0 0 2%UTI 8 0 0 0 2%
AEs > 5% in any Group
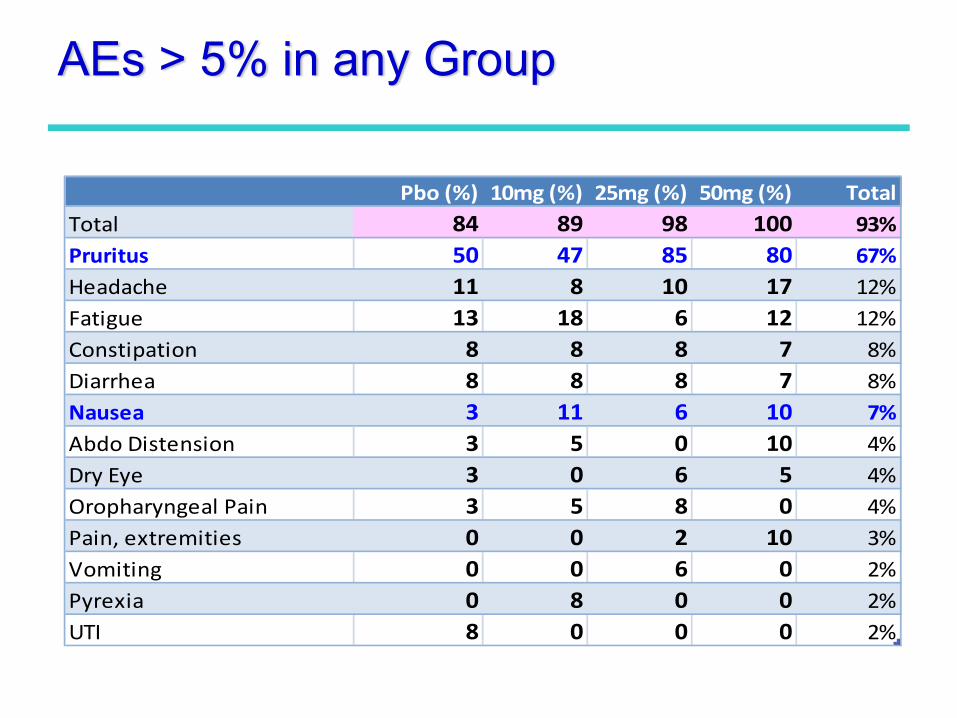
Pbo (%) 10mg (%) 25mg (%) 50mg (%) TotalTotal 84 89 98 100 93%Pruritus 50 47 85 80 67%Headache 11 8 10 17 12%Fatigue 13 18 6 12 12%Constipation 8 8 8 7 8%Diarrhea 8 8 8 7 8%Nausea 3 11 6 10 7%Abdo Distension 3 5 0 10 4%Dry Eye 3 0 6 5 4%Oropharyngeal Pain 3 5 8 0 4%Pain, extremities 0 0 2 10 3%Vomiting 0 0 6 0 2%Pyrexia 0 8 0 0 2%UTI 8 0 0 0 2%
AEs > 5% in any Group
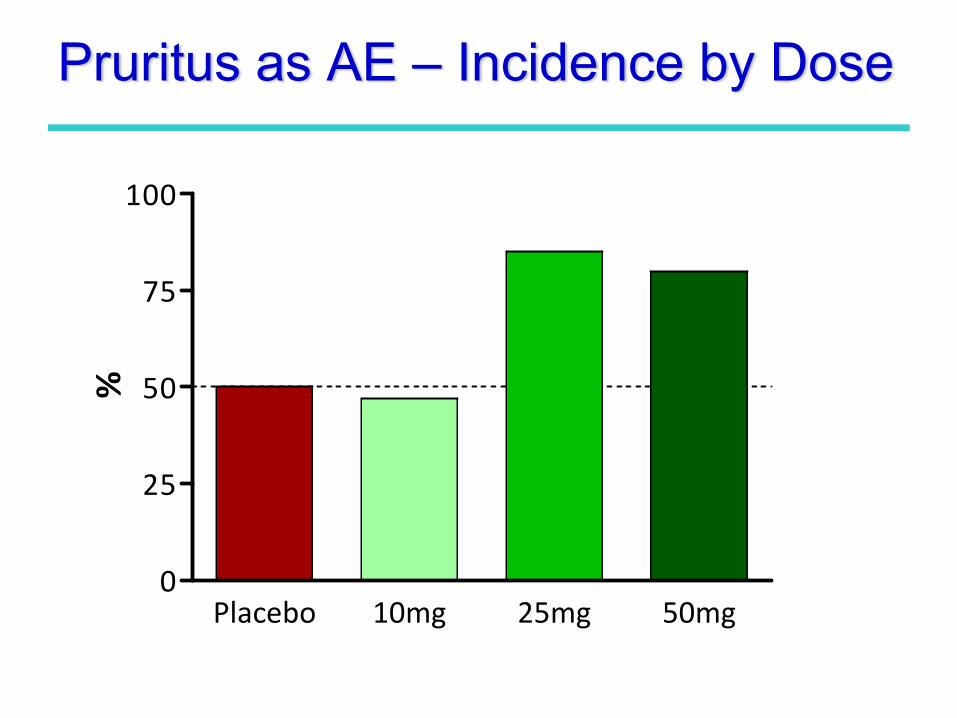
Placebo 10mg 25mg 50mg0
25
50
75
100
%Pruritus as AE – Incidence by Dose
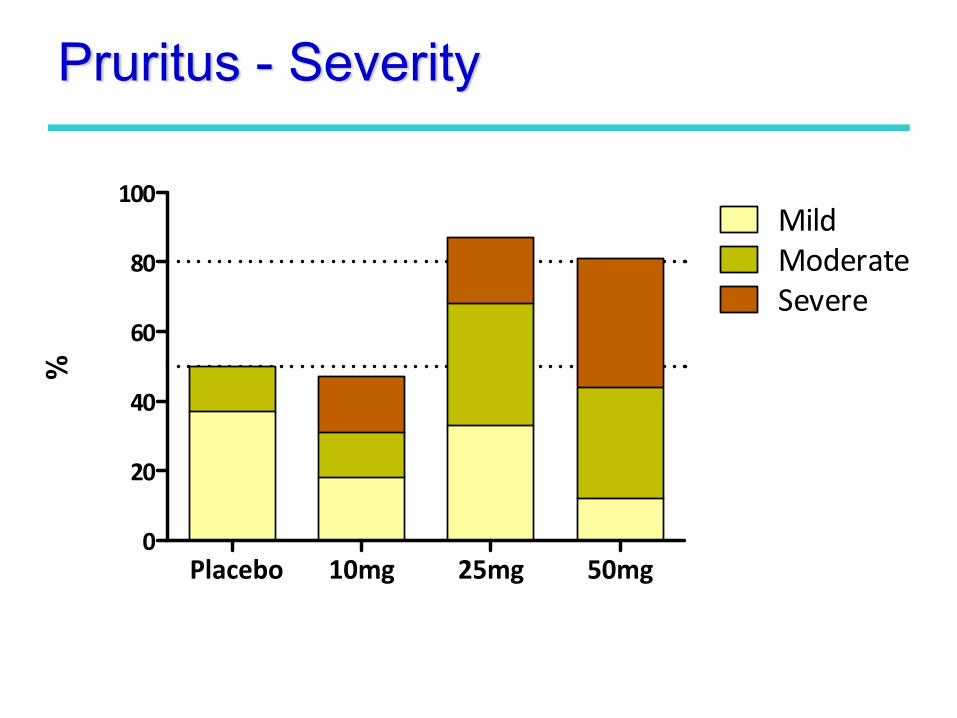
Placebo 10mg 25mg 50mg0
20
40
60
80
100MildModerateSevere
%Pruritus - Severity
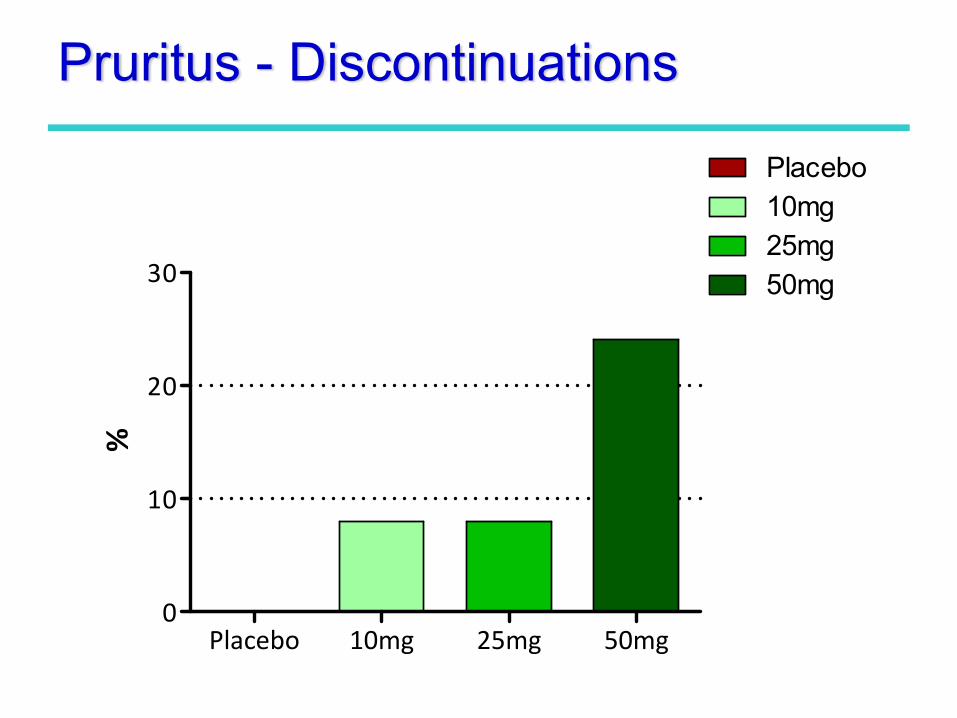
Pruritus - Discontinuations
Placebo 10mg 25mg 50mg0
10
20
30
Placebo10mg25mg50mg
%
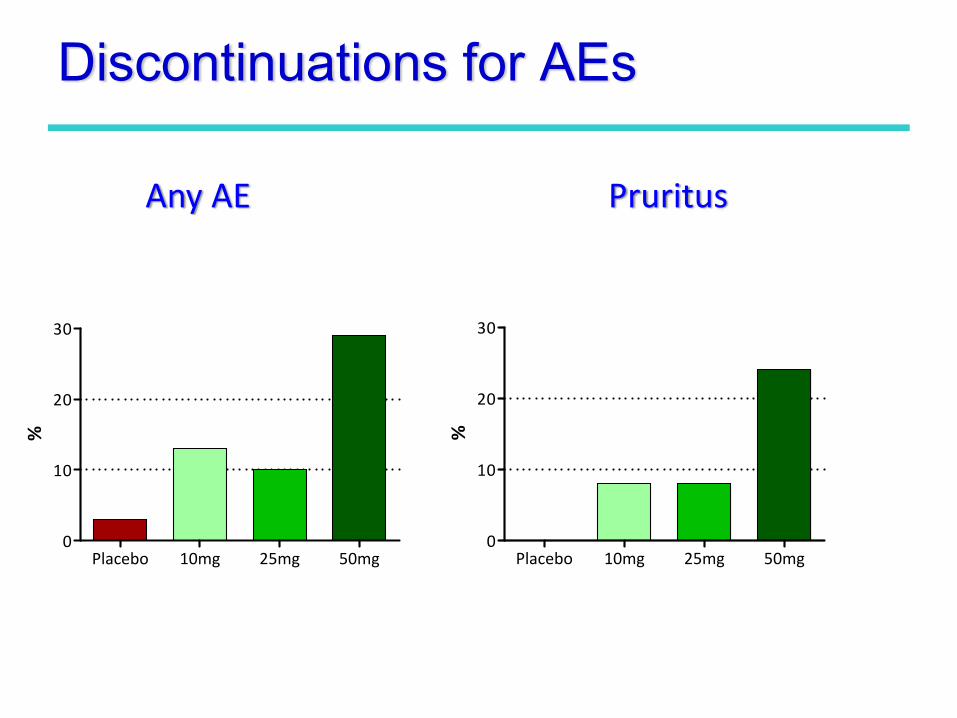
Placebo 10mg 25mg 50mg0
10
20
30
%
Placebo 10mg 25mg 50mg0
10
20
30
%
Discontinuations for AEs
Any AE Pruritus
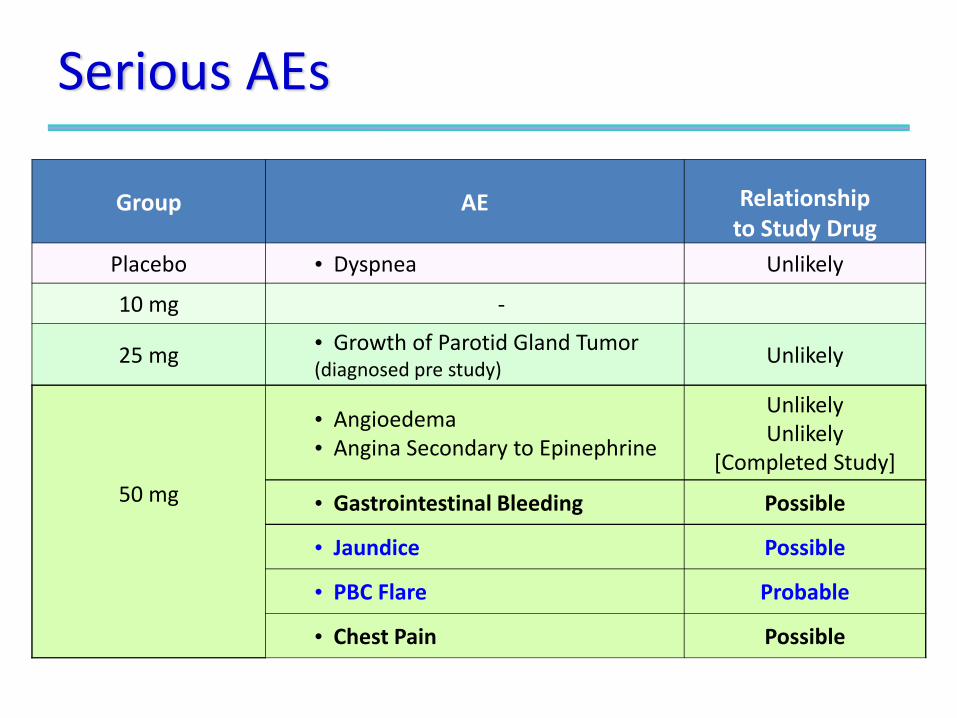
Serious AEs
Group AE Relationship to Study Drug
Placebo • Dyspnea Unlikely
10 mg ‐
25 mg • Growth of Parotid Gland Tumor (diagnosed pre study)
Unlikely
50 mg
• Angioedema• Angina Secondary to Epinephrine
UnlikelyUnlikely
[Completed Study]
• Gastrointestinal Bleeding Possible
• Jaundice Possible
• PBC Flare Probable
• Chest Pain Possible
Conclusions: OCA + UDCA
• Highly significant effects on Alkaline Phosphatase• Significant decreases in: GGT, ALT, AST
• No clear dose response relationship
• Safety & TolerabilityPruritus – Principal AE ‐ shows dose response relationship
• 50mg – unlikely starting dose in PBC
• Ongoing Phase 2 StudiesLong Term Safety Extension
Monotherapy study
• Merits further evaluation – Phase 3 planned
Thank You -Patients & Investigators.
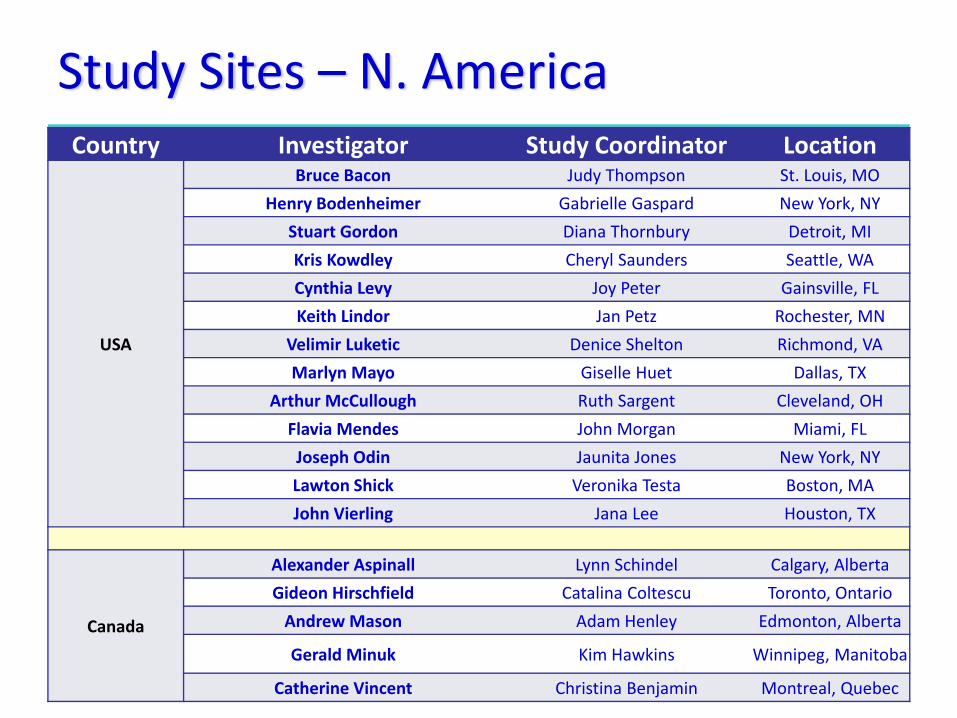
Study Sites – N. AmericaCountry Investigator Study Coordinator Location
USA
Bruce Bacon Judy Thompson St. Louis, MO
Henry Bodenheimer Gabrielle Gaspard New York, NY
Stuart Gordon Diana Thornbury Detroit, MI
Kris Kowdley Cheryl Saunders Seattle, WA
Cynthia Levy Joy Peter Gainsville, FL
Keith Lindor Jan Petz Rochester, MN
Velimir Luketic Denice Shelton Richmond, VA
Marlyn Mayo Giselle Huet Dallas, TX
Arthur McCullough Ruth Sargent Cleveland, OH
Flavia Mendes John Morgan Miami, FL
Joseph Odin Jaunita Jones New York, NY
Lawton Shick Veronika Testa Boston, MA
John Vierling Jana Lee Houston, TX
Canada
Alexander Aspinall Lynn Schindel Calgary, Alberta
Gideon Hirschfield Catalina Coltescu Toronto, Ontario
Andrew Mason Adam Henley Edmonton, Alberta
Gerald Minuk Kim Hawkins Winnipeg, Manitoba
Catherine Vincent Christina Benjamin Montreal, Quebec
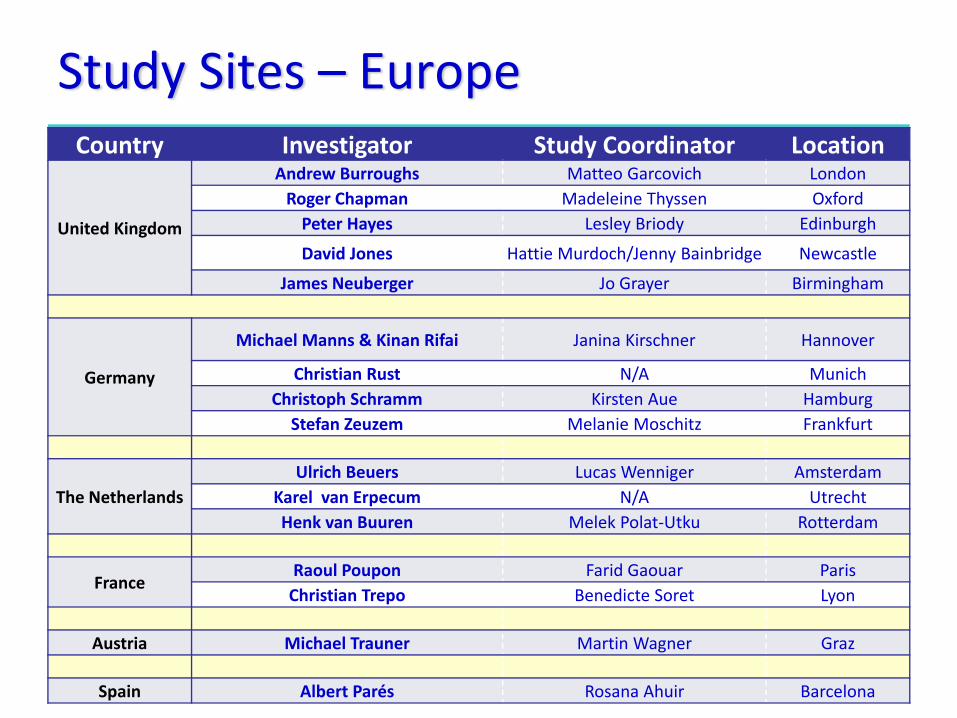
Study Sites – EuropeCountry Investigator Study Coordinator Location
United Kingdom
Andrew Burroughs Matteo Garcovich London Roger Chapman Madeleine Thyssen Oxford Peter Hayes Lesley Briody Edinburgh
David Jones Hattie Murdoch/Jenny Bainbridge Newcastle
James Neuberger Jo Grayer Birmingham
Germany
Michael Manns & Kinan Rifai Janina Kirschner Hannover
Christian Rust N/A Munich Christoph Schramm Kirsten Aue Hamburg
Stefan Zeuzem Melanie Moschitz Frankfurt
The Netherlands Ulrich Beuers Lucas Wenniger Amsterdam
Karel van Erpecum N/A Utrecht Henk van Buuren Melek Polat‐Utku Rotterdam
France Raoul Poupon Farid Gaouar Paris Christian Trepo Benedicte Soret Lyon
Austria Michael Trauner Martin Wagner Graz
Spain Albert Parés Rosana Ahuir Barcelona
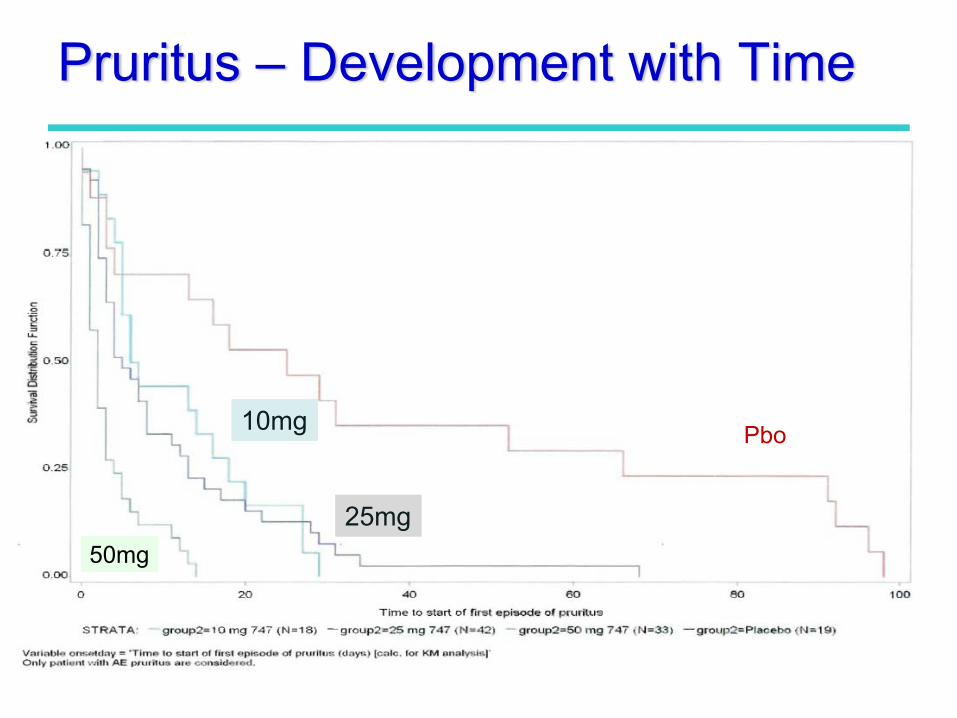
Pruritus – Development with Time
Pbo
50mg
10mg
25mg
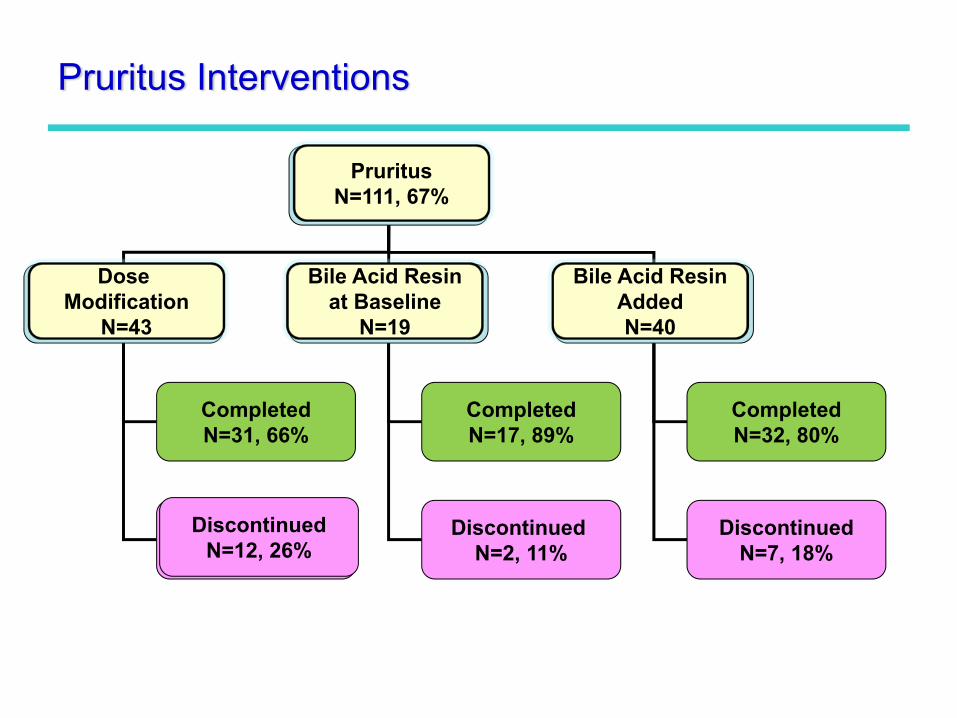
Pruritus Interventions
PruritusN=111, 67%
Dose Modification
N=43
Bile Acid Resinat Baseline
N=19
Bile Acid ResinAddedN=40
CompletedN=32, 80%
DiscontinuedN=7, 18%
CompletedN=17, 89%
Discontinued N=2, 11%
CompletedN=31, 66%
DiscontinuedN=12, 26%
PruritusN=111, 67%
Dose Modification
N=43
Bile Acid Resinat Baseline
N=19
Bile Acid ResinAddedN=40
DiscontinuedN=12, 26%